Bare Metal Stents vs. DrugBare Metal Stents vs. Drug--Eluting Stents for STEMI:Eluting Stents for STEMI:
Is it Settled? Is it Settled?
Ajay J. Ajay J. KirtaneKirtane, MD, SM, MD, SM
Columbia University Medical Center /Columbia University Medical Center /New York Presbyterian HospitalNew York Presbyterian Hospital

Conflict of Interest DisclosureConflict of Interest Disclosure
•• Ajay J. KirtaneAjay J. Kirtane
–– In the last 12 months, I have received In the last 12 months, I have received honoraria/consultancy fees from Abbott honoraria/consultancy fees from Abbott Vascular, Boston Scientific, and Vascular, Boston Scientific, and Medtronic CardioVascularMedtronic CardioVascular
–– OffOff--label use will be discussedlabel use will be discussed

DES vs. BMS in STEMI:Why the Debate?
•• STEMI patients have the highest thrombotic STEMI patients have the highest thrombotic risk (potential for worse safety)risk (potential for worse safety)•• Worsened healing response after stenting?Worsened healing response after stenting?•• Greater potential for malapposition and/or Greater potential for malapposition and/or
underexpansionunderexpansion•• Highest ST rates, meeting patient “under Highest ST rates, meeting patient “under
the gun”the gun”•• STEMI lesions have lower restenosis rates STEMI lesions have lower restenosis rates
(potential for less DES efficacy)(potential for less DES efficacy)•• Less plaque, ISR less manifestLess plaque, ISR less manifest
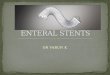
Distinction between AMI andDistinction between AMI andNonNon--AMI LesionsAMI Lesions
Culprit siteCulprit site
Neointima
NC
Rupture siteNeointima
NC
Fibroatheroma culprit site (control)
AMI lesionAMI lesionPost stentPost stent
Stable lesionStable lesionPost stentPost stent
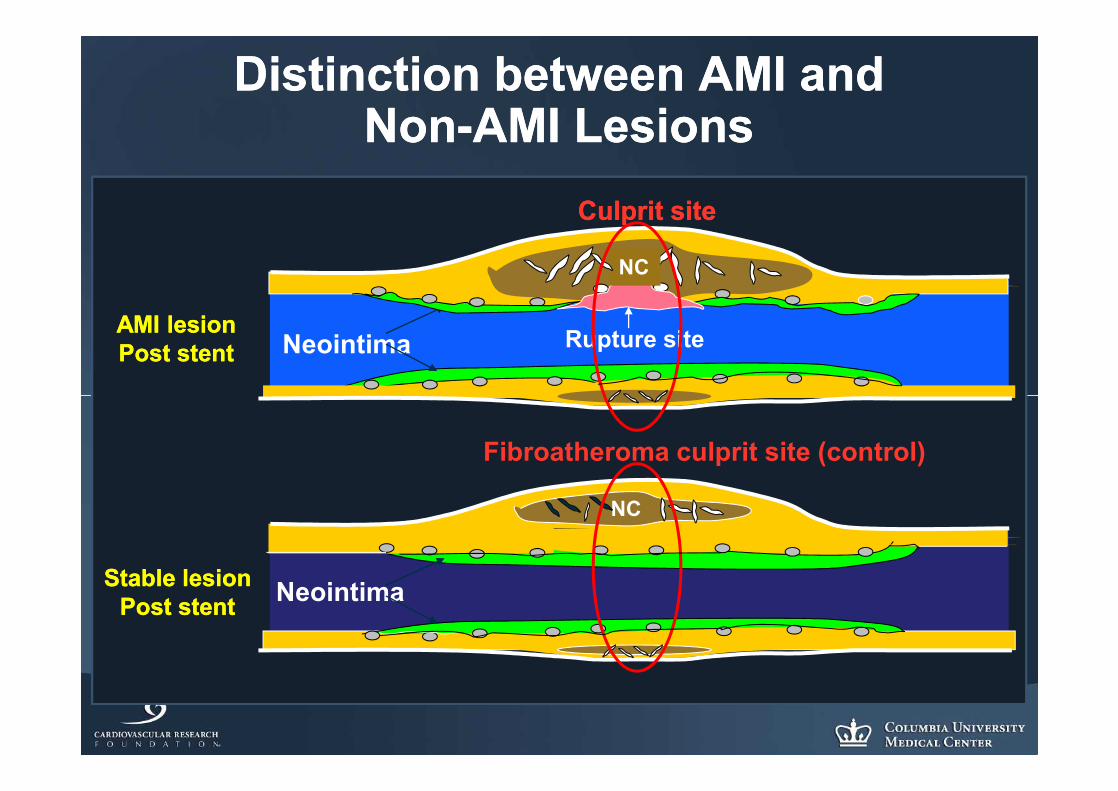
Delayed Arterial Healing with DES in AMI
Persistent fibrin deposition and uncovered struts in AMI compared to stable lesions treated with DES
Nakazawa and Virmani et al. Circulation 2008

AMIwith rupture
(n=17)
Stable with FA(n=18)
p valueAMI vs. Stable
Neointimal thickness, Neointimal thickness, mmmm
0.04(0.02, 0.09)
0.11(0.07, 0.21)
0.008
Strut with fibrin Strut with fibrin deposition, %deposition, % 63 ± 28 36 ± 27 0.008
Strut with Strut with inflammation, %inflammation, % 35 (27, 49) 17 (7, 25) 0.003
Uncovered strut, %Uncovered strut, % 49 (16, 96) 9 (0, 39) 0.01
Pathologic Assessment at Culprit SitePathologic Assessment at Culprit Site(AMI vs. Stable patients)(AMI vs. Stable patients)
Nakazawa and Virmani et al., Circulation 2008

HORIZONSHORIZONS--AMI IVUS SubstudyAMI IVUS Substudy
Post-Stent Follow-up
PES
BMS
• PES reduced net volume obstruction compared to BMS
• PES was associated with more late malapposition compared to BMS (29.6% vs. 7.9%, p<0.001)
402 patients, 446 lesions with serial IVUS data
Maehara A et al, Circulation 2009
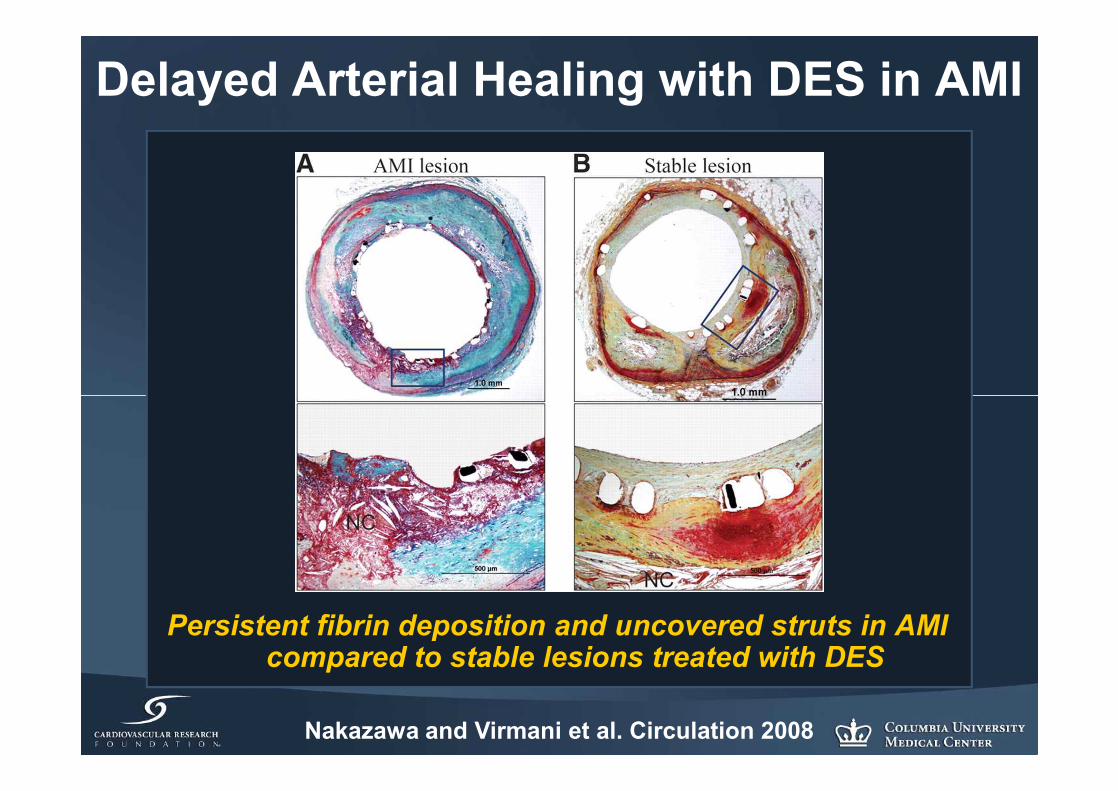
Stent ThrombosisPatient, Procedure, DevicePatient, Procedure, Device
StentStentThrombosisThrombosisProcedure
• Lesion pre/post• Stent Expansion• Flow/Runoff
Patient Factors• Higher Risk (Syndrome, Comorbidities)• Adjunctive therapies• AP Adherence and/or Responsiveness
Device•• Polymer Polymer • Drug• Surface

HR (95% CI)HR (95% CI) P valueP value
LateLate
STEMISTEMI 5.5 (3.55.5 (3.5––7.6)7.6) <0.0001 <0.0001
LADLAD 3.0 (2.03.0 (2.0––4.4)4.4) <0.0001 <0.0001
Stent length (per mmStent length (per mm)) 1.07 (1.051.07 (1.05––1.09)1.09) <0.0001<0.0001
The Spanish ESTROFA RegistryThe Spanish ESTROFA Registry23,500 pts treated w/DES at 20 Spanish hospitals from 200223,500 pts treated w/DES at 20 Spanish hospitals from 2002––06; 63% 06; 63%
PES, 37% SES. Dual antiplatelet Rx for PES, 37% SES. Dual antiplatelet Rx for 8 8 ±± 3 months. 3 months. 1.3% ST rate at median FU 22 (11, 32) mos ; 2.0% ST at 3 yrs1.3% ST rate at median FU 22 (11, 32) mos ; 2.0% ST at 3 yrs
Multivariate Predictors of Stent Thrombosis (n=14,120)Multivariate Predictors of Stent Thrombosis (n=14,120)
de la Torre Hernandez JM et al. de la Torre Hernandez JM et al. JACCJACC 2008;51:9862008;51:986--9090

Impact of Thrombus Burden with DES in AMIImpact of Thrombus Burden with DES in AMI792 STEMI Patients with DES
Follow-Up (months)
Large Thrombus Burden
Small Thrombus Burden
Total Population
12
8.2%
3.2%
1.3%
9
6
3
0
0 1 3 6 9 12 15 18 21 24
Sianos G et al, J Am Coll Cardiol 2007; 50:573-83
Rate of IRA-STSmall Large
Final TIMI 3 94.9% 83.6%*
TMPG-3 53.2% 35.4%*
No-reflow 0.5% 4.0%*
Distal Embol. 3.5% 17.3%*
*P<0.001

Stent Thrombosis at 5 yearsStent Thrombosis at 5 yearsARC definite, probable, possibleARC definite, probable, possible
0 200 400 600 800 1000 1200 1400 1600 1800 2000
Days after Randomization
40
30
20
10
0
Pro
bab
ility of A
RC
Sten
t Th
rom
bo
sis (%)
Tirofiban-SES Abciximab-BMS
Hazard Ratio 1.13[95% CI: 0.44-2.9]; p=0.78
8%8%7%7%
J Am Coll Cardiol in pressJ Am Coll Cardiol in press

TwoTwo--Year Stent ThrombosisYear Stent Thrombosis(ARC Definite or Probable)(ARC Definite or Probable)
p= 0.99p= 0.99
HR [95%CI]=HR [95%CI]=1.00 [0.66, 1.51]1.00 [0.66, 1.51]
4.1%4.1%4.1%4.1%
Sten
t Thr
ombo
sis
(%)
Sten
t Thr
ombo
sis
(%)
00
11
22
33
44
55
66 TAXUS DES (n=2257)TAXUS DES (n=2257)EXPRESS BMS (n=749)EXPRESS BMS (n=749)
00 33 66 99 1212 1515 1818 2121 2424
22382238 21082108 20612061 19981998 16611661744744 696696 681681 661661 547547
Number at riskNumber at riskTAXUS DESTAXUS DESEXPRESS BMSEXPRESS BMS
MonthsMonths

0.0 2.0 4.0 6.0 8.0
CYPHER (n=251)
BMS (n=250)
Early (0 to 30 days) Very Late (> 1yr)
11(4.4%)
Stent Thrombosis (%)
12(4.8%)
9(3.6%)
6(2.4%)
3(1.2%)
5 (2.0%)
TYPHOON: ARC Definite/Probable Stent TYPHOON: ARC Definite/Probable Stent Thrombosis at 4 YearsThrombosis at 4 Years
P = 0.83

PES N=310
BMS N=309
HR (95% CI) P
Definite ST30 days – 1 year 1 (0.3%) 0 (0.0%)
1 year – 5 years 7 (2.5%) 2 (0.7%)
Total 8 (2.9%) 2 (0.8%) 3.95 (0.81 – 18.61) 0.06
Definite or Probable ST30 days – 1 year 2 (0.7%) 0 (0.0%)
1 year – 5 years 7 (2.5%) 3 (1.1%)
Total 9 (3.2%) 3 (1.1%) 2.97 (0.80 – 12.97) 0.09
5-Year LST and VLST
Incidences were estimated from the Kaplan-Meier curves
Vink, ACC/I2 2010

Impact of premature thienopyridine discontinuation: The PREMIER registry
500 pts with AMI undergoing primary PCI with DES at 19 U.S. medical centers, alive and well at 30 days
Spertus JA et al. Circulation 2006;113:2803Spertus JA et al. Circulation 2006;113:2803--9.9.Spertus JA et al. Circulation 2006;113:2803Spertus JA et al. Circulation 2006;113:2803--9.9.
68 (13.6%) were no longer taking 68 (13.6%) were no longer taking prescribed thienopyridines at 30 daysprescribed thienopyridines at 30 days
7.5
0.70
2
4
6
8
10
1 Ye
ar M
orta
lity
(%) D/C thienopyridine at 30 days
Taking thienopyridine at 30 days
P<0.0001P<0.0001Propensity Propensity adjusted for adjusted for
reasons to d/c reasons to d/c thien: HR = thien: HR = 9.02 9.02 (1.3(1.3--60.660.6), P=), P=0.020.02

Death/MI Related to Delays in Filling Clopidogrel Prescription after DES
Of 7,402 patients, 16% did not fill a clopidogrel prescription on day of discharge (median delay of 3 days)
Ho et al, Circ Cardiovasc Qual Outcomes 2010Ho et al, Circ Cardiovasc Qual Outcomes 2010Ho et al, Circ Cardiovasc Qual Outcomes 2010Ho et al, Circ Cardiovasc Qual Outcomes 2010
Delay
No Delay
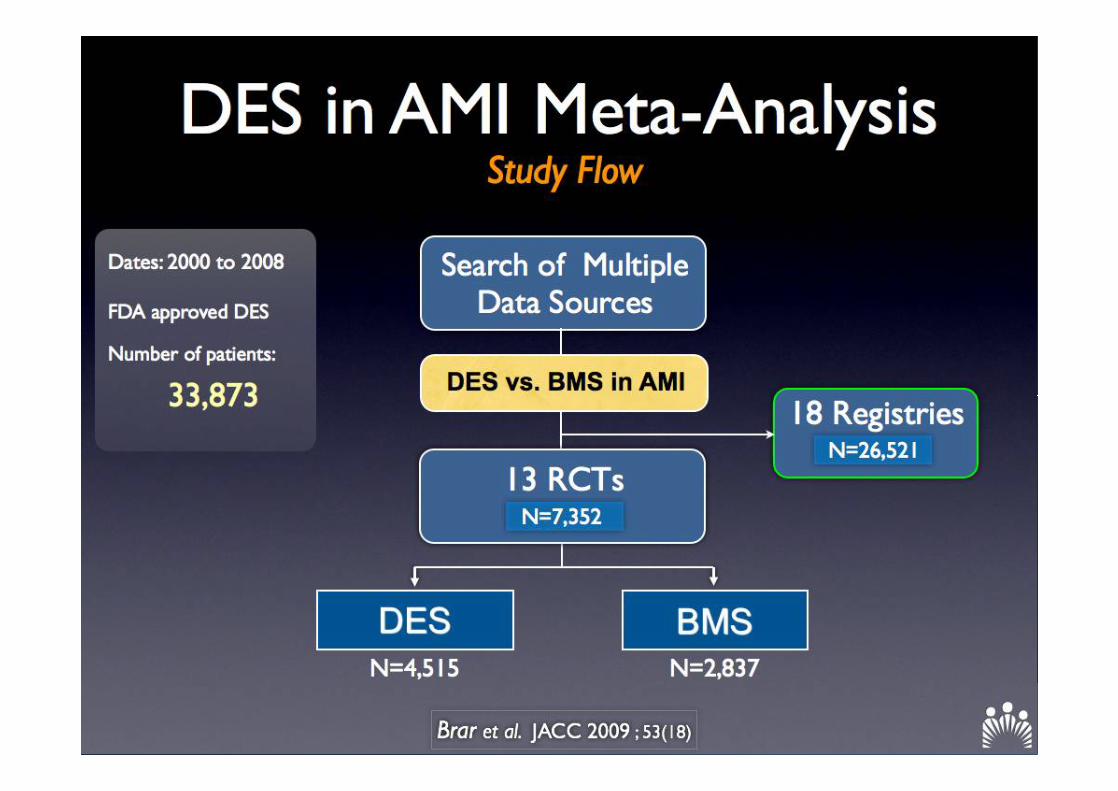
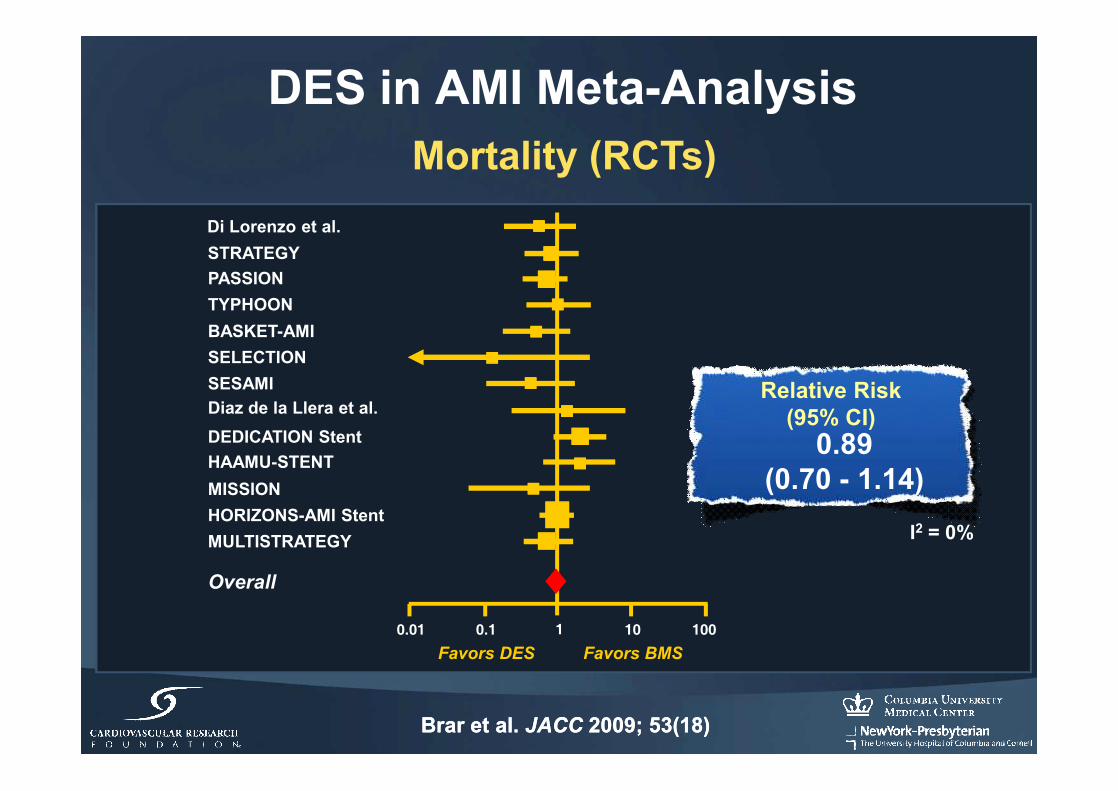
DES in AMI Meta-Analysis
1 10 1000.10.01
Mortality (RCTs)Di Lorenzo et al.STRATEGYPASSIONTYPHOONBASKET-AMISELECTIONSESAMIDiaz de la Llera et al.DEDICATION StentHAAMU-STENTMISSIONHORIZONS-AMI StentMULTISTRATEGY
Overall
Favors DES Favors BMS
Relative Risk (95% CI)
0.89 (0.70 - 1.14)
I2 = 0%
Brar et al. JACC 2009; 53(18)Brar et al. JACC 2009; 53(18)

1 10 1000.10.01
Stent Thrombosis (RCTs)
Di Lorenzo et al.STRATEGYBASKET-AMIPASSIONTYPHOONDEDICATION StentHAAMU-STENTMISSIONSELECTIONDiaz de la Llera et al.HORIZONS-AMI StentMULTISTRATEGY
Overall
Favors DES Favors BMS
Relative Risk (95% CI)
0.97 (0.73 - 1.28)
I2 = 0%
Brar et al. JACC 2009; 53(18)Brar et al. JACC 2009; 53(18)
DES in AMI Meta-Analysis


Massachusetts State RegistryMassachusetts State Registry
Mauri L et al. Mauri L et al. NEJMNEJM 2008;359:13302008;359:1330--4242
22--year mortality (propensity adjusted) in 1298 matched pairs year mortality (propensity adjusted) in 1298 matched pairs (2596 pts) with STEMI at 21 hospitals between 4/03(2596 pts) with STEMI at 21 hospitals between 4/03––9/049/04
11.6%11.6%8.5%8.5%
P=0.008P=0.008
DrugDrug--Eluting StentEluting StentNo. at riskNo. at risk 12981298 12891289 12501250 12271227 12131213Cum. incidence (%)Cum. incidence (%) 0.70.7 3.73.7 5.55.5 6.56.5 8.58.5
BareBare--Metal StentMetal StentNo. at riskNo. at risk 12981298 12921292 12231223 11941194 11731173Cum. incidence (%)Cum. incidence (%) 0.50.5 5.85.8 8.08.0 9.69.6 11.611.6
Days after Initial ProcedureDays after Initial Procedure
Dea
th (a
djus
ted)
(%)
Dea
th (a
djus
ted)
(%)
3030
2020
1010
0000 3030 180180 365365 730730
BMS (n=1298)BMS (n=1298)
DES (n=1298)DES (n=1298)
1% mortality difference at 2 days1% mortality difference at 2 days2.1% mortality2.1% mortality difference at 30 daysdifference at 30 days

DES vs. BMS in STEMI:Case Closed?
•• Despite higher theoretical risks of Despite higher theoretical risks of delayed healing, malapposition, and delayed healing, malapposition, and other potential risks…other potential risks…•• Overall rates of ST and other clinical Overall rates of ST and other clinical
safety outcomes have been similar for safety outcomes have been similar for BMS and DESBMS and DES
•• So what about efficacy?So what about efficacy?

1 10 1000.10.01
Target Vessel Revascularization (RCTs)Di Lorenzo et al.STRATEGYBASKET-AMIPASSIONTYPHOONSELECTIONSESAMIDiaz de la Llera et al.DEDICATION StentHAAMU-STENTMISSIONHORIZONS-AMI StentMULTISTRATEGY
Overall
Favors DES Favors BMS
Relative Risk (95% CI)
0.44 (0.35 - 0.55)
56%REDUCTION
p < 0.001
I2 = 26%
Brar et al. JACC 2009; 53(18)Brar et al. JACC 2009; 53(18)
DES in AMI Meta-Analysis

TYPHOON4-Year Follow-Up of SES vs. BMS for AMI
Conclusion:Conclusion: At 4 years, SES still maintain their initial At 4 years, SES still maintain their initial advantage in terms of revascularization rates over BMS.advantage in terms of revascularization rates over BMS.
Spaulding C. Presented at: EuroPCR 2009.May 19-22, 2009.
4-Year Outcomes
Cyphern = 251
BMSn = 250 P Value
TLR (%) 7.2 15.2 0.005
MI (%) 4.8 4.0 0.83
Death (%) 4.0 6.4 0.23

22572257 21322132 20982098 20692069 18681868749749 697697 675675 658658 603603
Number at riskNumber at riskTAXUS DESTAXUS DESEXPRESS BMSEXPRESS BMS
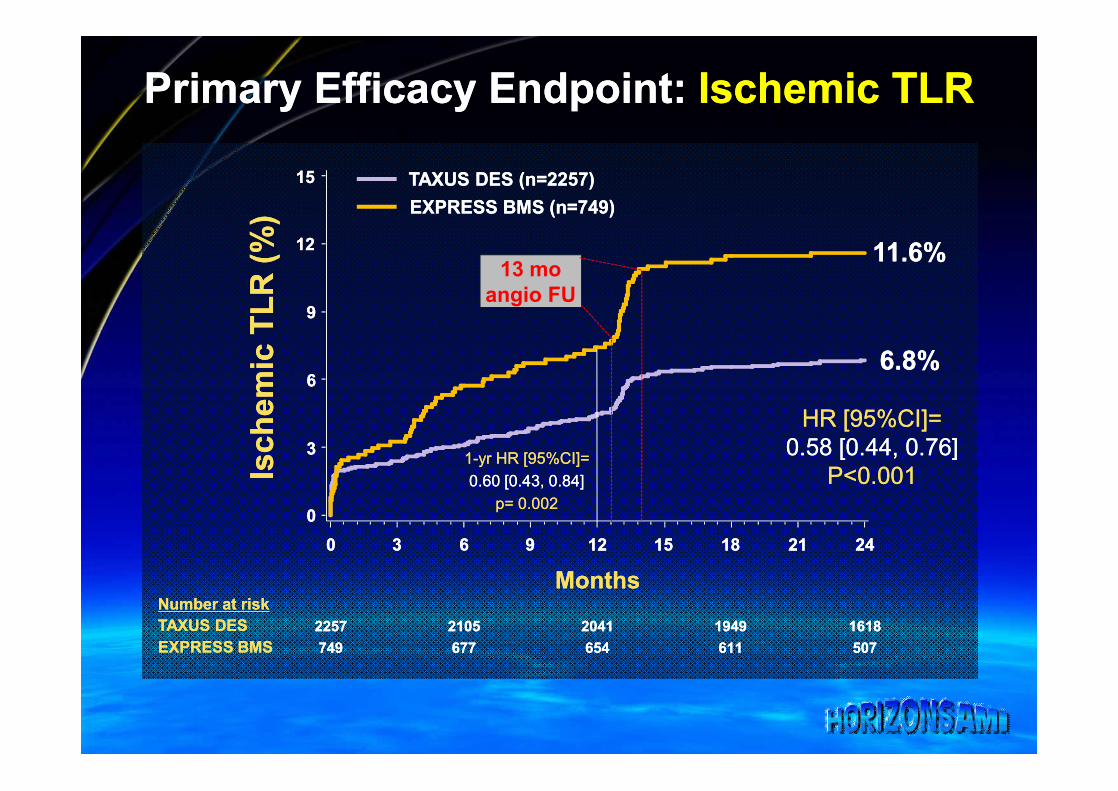
Primary Efficacy Endpoint: Primary Efficacy Endpoint: Ischemic TLRIschemic TLR
Isch
emic
TLR
(%)
Isch
emic
TLR
(%)
00
11
22
33
44
55
66
77
88
99
1010
Time in MonthsTime in Months00 11 22 33 44 55 66 77 88 99 1010 1111 1212
7.5%7.5%
4.5%4.5%
Diff = Diff = --3.0%3.0%HR = HR = 0.590.59P=0.002P=0.002
TAXUS DES (n=2257)TAXUS DES (n=2257)EXPRESS BMS (n=749)EXPRESS BMS (n=749)
Which is more impressive?
1. 41% reduction in ischemic TLR
2. Need to treat 33 patients with DES vs. BMS to prevent one TLR event

Primary Efficacy Endpoint: Primary Efficacy Endpoint: Ischemic TLRIschemic TLR
P<0.001P<0.001
HR [95%CI]=HR [95%CI]=0.58 [0.44, 0.76]0.58 [0.44, 0.76]
6.8%6.8%
11.6%11.6%Is
chem
ic T
LR (%
)Is
chem
ic T
LR (%
)
00
33
66
99
1212
1515 TAXUS DES (n=2257)TAXUS DES (n=2257)EXPRESS BMS (n=749)EXPRESS BMS (n=749)
22572257 21052105 20412041 19491949 16181618749749 677677 654654 611611 507507
00 33 66 99 1212 1515 1818 2121 2424
Number at riskNumber at riskTAXUS DESTAXUS DESEXPRESS BMSEXPRESS BMS
MonthsMonths
Primary Efficacy Endpoint: Primary Efficacy Endpoint: Ischemic TLRIschemic TLR
22572257 21052105 20412041 19491949 16181618749749 677677 654654 611611 507507
P<0.001P<0.001
HR [95%CI]=HR [95%CI]=0.58 [0.44, 0.76]0.58 [0.44, 0.76]
6.8%6.8%
11.6%11.6%Is
chem
ic T
LR (%
)Is
chem
ic T
LR (%
)
00
33
66
99
1212
1515
00 33 66 99 1212 1515 1818 2121 2424
TAXUS DES (n=2257)TAXUS DES (n=2257)EXPRESS BMS (n=749)EXPRESS BMS (n=749)
Number at riskNumber at riskTAXUS DESTAXUS DESEXPRESS BMSEXPRESS BMS
MonthsMonths
p= 0.002p= 0.002
11--yr HR [95%CI]=yr HR [95%CI]=0.60 [0.43, 0.84]0.60 [0.43, 0.84]
13 mo angio FU
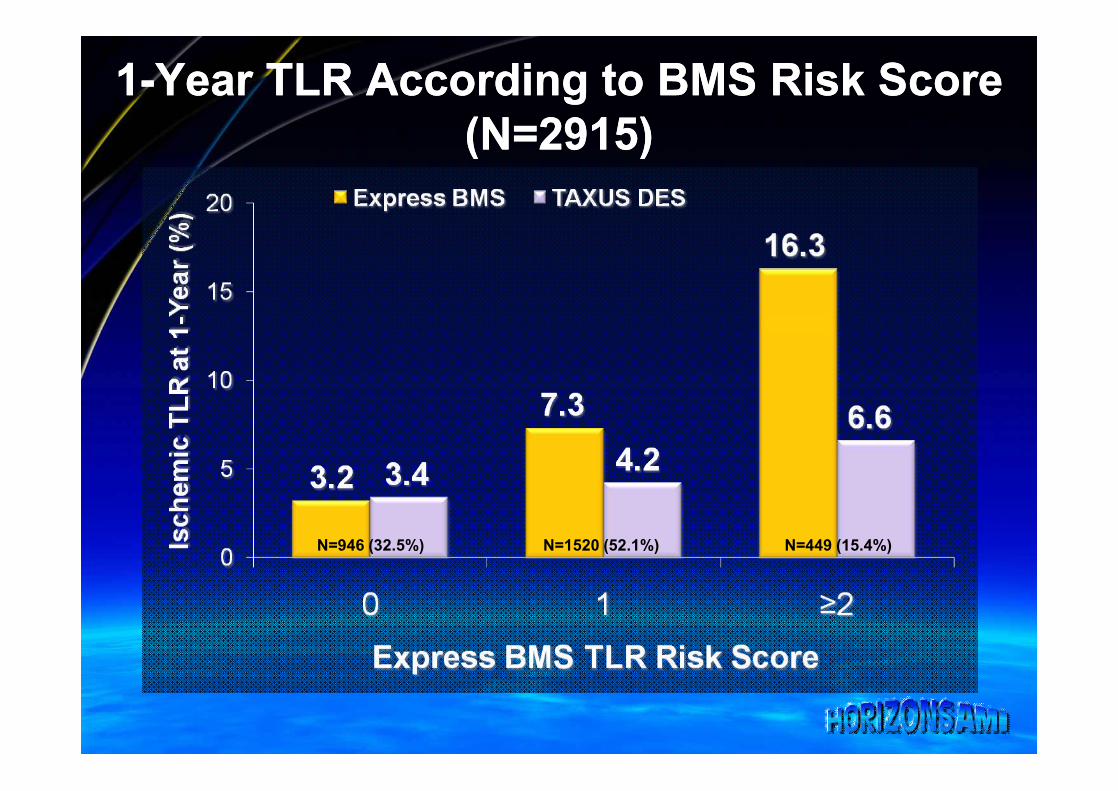
11--Year TLR According to BMS Risk ScoreYear TLR According to BMS Risk Score(N=2915)(N=2915)
N=946 (32.5%) N=1520 (52.1%) N=449 (15.4%)

Safety of DES vs. BMS in STEMI:Case Closed?
•• Despite higher theoretical risks of delayed Despite higher theoretical risks of delayed healing, malapposition, and other potential healing, malapposition, and other potential safety risks…safety risks…•• Overall ST and other safety outcomes Overall ST and other safety outcomes
(mortality, MI) have been similar for BMS (mortality, MI) have been similar for BMS and DESand DES
•• Continued longContinued long--term FU and investigation term FU and investigation of newer DES systems is neededof newer DES systems is needed
•• Issues of DAPT adherence are critical in the Issues of DAPT adherence are critical in the clinical settingclinical setting

Efficacy of DES vs. BMS in STEMI:Case Closed?
•• Because of lower absolute event rates Because of lower absolute event rates of TLR, careful attention to absolute of TLR, careful attention to absolute risk reductions (and number needed to risk reductions (and number needed to treat) rather than relative risk treat) rather than relative risk reductions is neededreductions is needed•• An estimation of baseline restenotic An estimation of baseline restenotic
risk should be performed in order to risk should be performed in order to determine the potential benefit of DES determine the potential benefit of DES in an individual patient!!in an individual patient!!
Recommended