
Dr Matthew BrickOrthopaedic Surgeon
Anterior CruciateLigament Injuries
A.C.L Function
The cruciate ligaments and thecollateral ligaments provide stabilityto the joint by holding the bonestogether. Of those ligaments, theanterior cruciate is important in that itholds the knee together duringtwisting type activities. Duringeveryday walking and in straight linerunning, the ACL is hardly used. Assoon as any twisting is performedhowever, this ligament is essential.Without it the knee twists further thanit is designed to, giving a feeling thatthe knee comes out of joint. It is thisfeeling of coming apart that givesrise to the instability or loss ofconfidence in the knee that is seenwhen the ACL is torn. As it is arotatory instability, it occurs whentwisting or sidestepping is attempted,or when uneven ground isencountered. If major, it may occurin everyday activities. In somehowever, it occurs only on thesporting field, where it is hard toconcentrate on protecting the kneeand where sudden twisting andturning occurs.
Meniscal Cartlilage and Articular(Lining) Cartilage:
Figure 1: The lateral and medialmenisci attach near the centre ofthe tibia.The menisci function as space fillersto spread the load between thesurfaces of the femur and tibia. Theends of these bones are not thesame shape and thus the menisciare needed to make up for thatincongruity. The end of the femur isround and the top of the tibia is flat.They primarily function somewhatlike shock absorbers but they alsohave a secondary role to enhancelubrication and nutrition of thearticular or lining cartilage. They aremade of springy cartilage, a little likeyour ears.
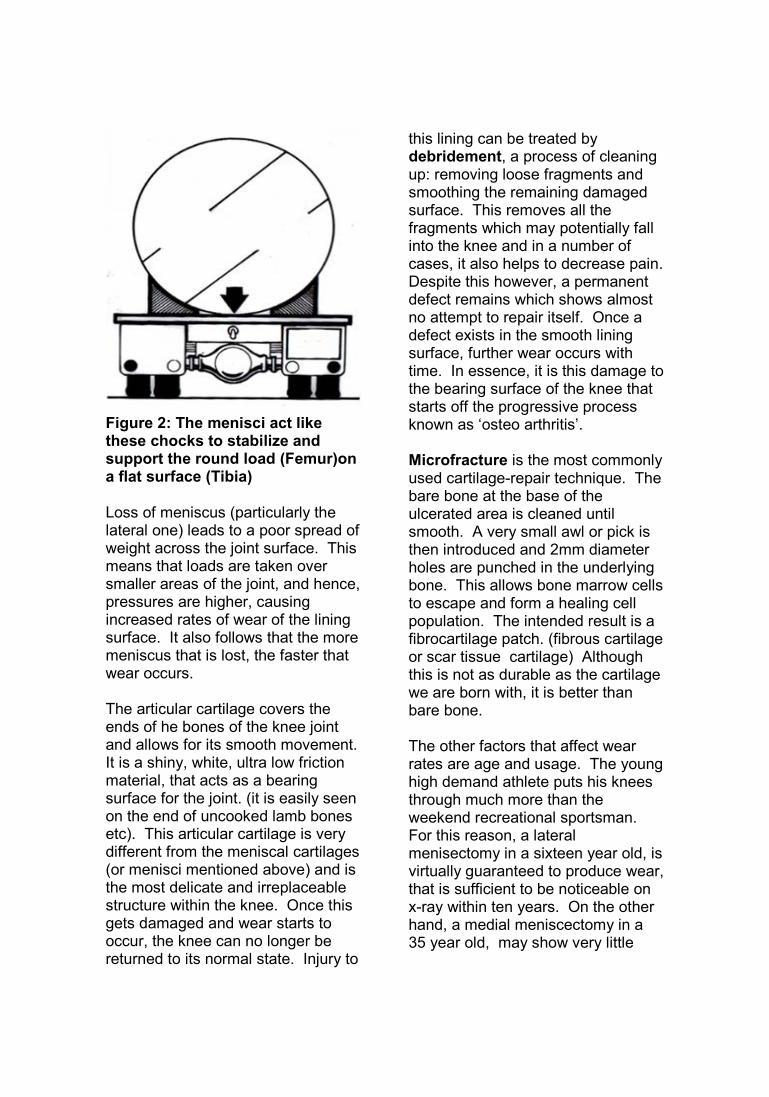
Figure 2: The menisci act likethese chocks to stabilize andsupport the round load (Femur)ona flat surface (Tibia)
Loss of meniscus (particularly thelateral one) leads to a poor spread ofweight across the joint surface. Thismeans that loads are taken oversmaller areas of the joint, and hence,pressures are higher, causingincreased rates of wear of the liningsurface. It also follows that the moremeniscus that is lost, the faster thatwear occurs.
The articular cartilage covers theends of he bones of the knee jointand allows for its smooth movement.It is a shiny, white, ultra low frictionmaterial, that acts as a bearingsurface for the joint. (it is easily seenon the end of uncooked lamb bonesetc). This articular cartilage is verydifferent from the meniscal cartilages(or menisci mentioned above) and isthe most delicate and irreplaceablestructure within the knee. Once thisgets damaged and wear starts tooccur, the knee can no longer bereturned to its normal state. Injury to
this lining can be treated bydebridement, a process of cleaningup: removing loose fragments andsmoothing the remaining damagedsurface. This removes all thefragments which may potentially fallinto the knee and in a number ofcases, it also helps to decrease pain.Despite this however, a permanentdefect remains which shows almostno attempt to repair itself. Once adefect exists in the smooth liningsurface, further wear occurs withtime. In essence, it is this damage tothe bearing surface of the knee thatstarts off the progressive processknown as ‘osteo arthritis’.
Microfracture is the most commonlyused cartilage-repair technique. Thebare bone at the base of theulcerated area is cleaned untilsmooth. A very small awl or pick isthen introduced and 2mm diameterholes are punched in the underlyingbone. This allows bone marrow cellsto escape and form a healing cellpopulation. The intended result is afibrocartilage patch. (fibrous cartilageor scar tissue cartilage) Althoughthis is not as durable as the cartilagewe are born with, it is better thanbare bone.
The other factors that affect wearrates are age and usage. The younghigh demand athlete puts his kneesthrough much more than theweekend recreational sportsman.For this reason, a lateralmenisectomy in a sixteen year old, isvirtually guaranteed to produce wear,that is sufficient to be noticeable onx-ray within ten years. On the otherhand, a medial meniscectomy in a35 year old, may show very little
change on x-ray for 20 years. In theyoung therefore, menisci should berepaired whenever possible and thisis particularly so in the case of thelateral meniscus which seems to bemore important that its medialcounterpart. Family history is alsoimportant as osteoarthritis has aninherited component. An athletewho has a strong family history ofosteoarthritis is especially at risk ifhe or she loses a meniscus.
Injury Mechanism
Injuries to the anterior cruciateligament occur most often in athleticactivities (especially twisting andturning sports, such as football andnetball) but may be ruptured in workinjuries and non-athletic activities.The injury usually occurs withoutcontact and often is associated witha sudden change in direction (egside stepping) or a sudden change inspeed (a deceleration injury). It mayalso occur with the body falling overa fixed leg or with a hyper-extension(over straightening) injury to theknee.The athlete often describes theincident “My knee went one way andmy body went the other.”
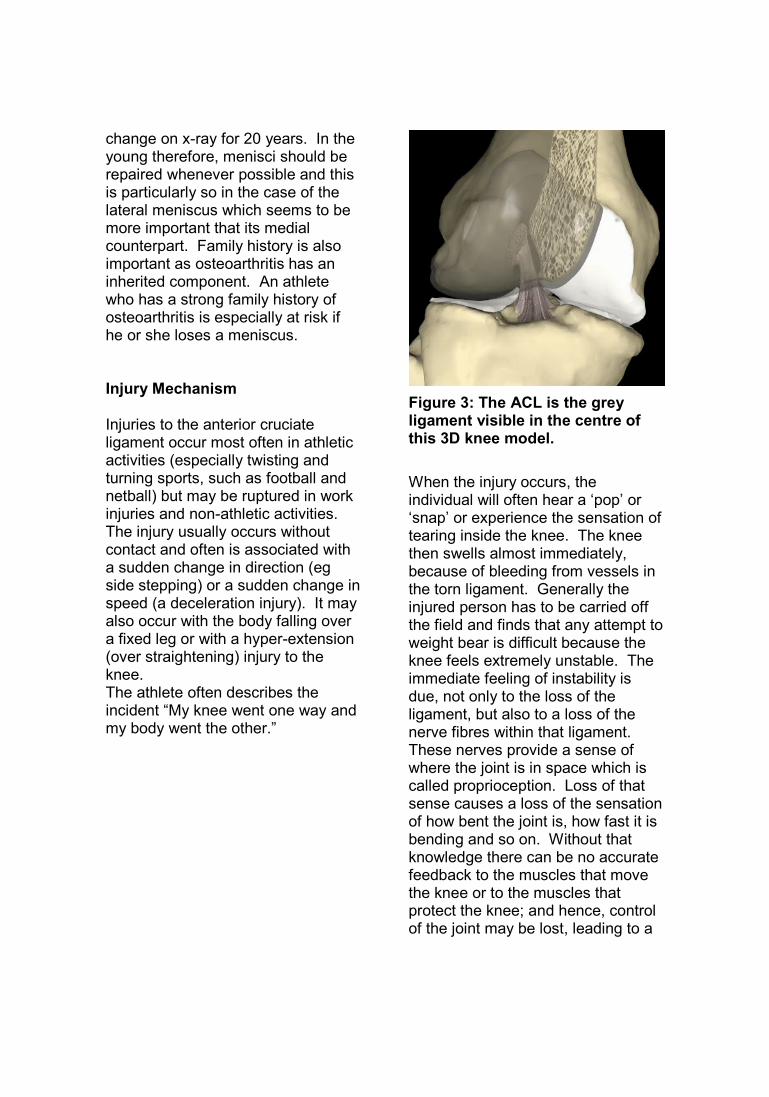
Figure 3: The ACL is the greyligament visible in the centre ofthis 3D knee model.
When the injury occurs, theindividual will often hear a ‘pop’ or‘snap’ or experience the sensation oftearing inside the knee. The kneethen swells almost immediately,because of bleeding from vessels inthe torn ligament. Generally theinjured person has to be carried offthe field and finds that any attempt toweight bear is difficult because theknee feels extremely unstable. Theimmediate feeling of instability isdue, not only to the loss of theligament, but also to a loss of thenerve fibres within that ligament.These nerves provide a sense ofwhere the joint is in space which iscalled proprioception. Loss of thatsense causes a loss of the sensationof how bent the joint is, how fast it isbending and so on. Without thatknowledge there can be no accuratefeedback to the muscles that movethe knee or to the muscles thatprotect the knee; and hence, controlof the joint may be lost, leading to a
feeling of instability or loss ofconfidence.
With time the feeling ofproprioception improves. This isbecause the nerve fibres in the otherligaments attempt to make up for theloss of sensation from the nervefibres in the anterior cruciateligament. This situation is neverquite as good as the original but, ifthe demands on the knee are low, itmay be sufficient to get by.
After the Injury
What happens after injury to theanterior cruciate ligament is asudden loss of control of the knee,which gradually returns. In mostpeople, it takes about two months toreach a level where they can thinkabout playing sport again. Thosewho seem to get back to sportwithout surgery (about 30%) oftenonly have partial tears of theligament. Whilst the injured knee inthis group may be looser thannormal, it is thought that functionmay be satisfactory because someof the proprioceptive nerve fibresremain intact. These are thought toprovide enough feedback to themuscles around the knee, to enablethose muscles to compensatesomewhat for the partial loss of theligament.
Even for those with a completerupture, the feeling of stability doesgradually improve over a 2-3 monthperiod. If by that time however, fullconfidence in the knee has not beenrestored, then that knee will probablynever be able to perform a twisting,turning sport again without ACL
reconstruction. If a return to thosesports is made, then a repeat injuryis likely, due to the ongoinginstability. From then on, every timethat the knee gives way, moredamage is done. Sooner or later,that damage will include injury to thearticular lining cartilage, which isirreparable. This may herald an endto impact loading type activities andin essence, represents osteoarthritis,which will progressively worsen withtime. Because of this risk it is nowconsidered preferable to reconstructthe unstable knee early on, thushopefully, preventing recurrent injury.Our studies show that the athletewho undergoes reconstruction in thefirst 6 months before many instabilityepisodes does better long term thansomeone who has the operation 2-3years later after multiple episodes ofgiving way.
In general patients with ACL injuriesmay be put into one of three roughlyequal size groups:
The first group contains people whodo well and return to their sportwithout too much trouble. In thisgroup the re-injury rate is not all thathigh and, as suggested above, themajority in this group, have partialtears only. Essentially, the re-injuryrate, over a two year period, isthought to roughly equal thepercentage tear of the ligament. Itcould be said that a 30% tearprobably has a 30% chance of goingon to complete rupture within twoyears if normal sporting activity iscontinued.
The second group contains peoplewith a complete ACL tear who seem
to do well until they play ademanding sport. They may evendo well at training but, on taking tothe field, a re-injury soon occurs.This group otherwise copes well inday to day life and thus, onlyrequires surgery if a return to twistingtype sports is desired. Sports suchas netball and football demand goodACL function and for people wantingto play these sports, even at lowlevels, reconstruction of a completelytorn ligament is recommended.
The third group contains peoplewhose knees feel frankly unstable ineveryday life. This group all requiresurgery to give their knee a feeling ofstability. That stability then protectsagainst further injury and furtherdamage to the knee.
Who Warrants Surgery?
Overall, it may be seen that a largenumber of people who injure theiranterior cruciate ligament mighteventually benefit from surgery. Theexact number is uncertain butcurrently it is thought that some 50%or more would be helped. As withmeniscal injury, this is somewhatage dependent and the requirementfor surgery does decrease with age.This is not only because thedemands placed on the kneedecrease with advancing age butalso because the number of partialtears increase with age and theability to cope with proprioceptiveloss improves with age. Theopposite situation occurs in theyoung age group (under 18) wherealmost all tears are complete and themajority tend to be verysymptomatic. In this group
therefore, almost all patients willdevelop enough instability to warrantsurgery.
Those who sustain injuries to otherligaments of the knee, in addition toa tear of the anterior cruciateligament are more likely to fall intothe third group. Virtually all of thesepeople are better off consideringsurgery.
Those with suspected meniscaltears, which may be repairable, mayalso be better off consideringsurgery. It is not possible to knowwhether a meniscal tear will berepairable or not until the knee islooked into but nevertheless if theinjury seems major and suggests thispossibility, then surgery may be abetter long term alternative.
It is possible to repair a meniscusand leave a torn ACL alone, but thebreakdown rate of meniscal repairsin an unstable knee is more thandouble the failure rate in stableknees. For this reason, isolatedmeniscal repair without ACLreconstruction is rarely performed. Ifa meniscal tear is symptomatic andrequires treatment and, for reasonsof time or employment, areconstruction cannot be performed,then partial menisectomy isundertaken. This situation isregarded as a compromise to hastenreturn to work and is not a substitutefor reconstructive surgery. Twisting,turning sports then need to beavoided, until such time as the kneeis made stable.

Conservative Treatment
Treatment for injuries of the anteriorcruciate ligament cannot bestandardized because of individualdifferences in injury patterns andbecause of different expectations ofpatients in regard to return tosporting activities. In the patient whosees sport purely as recreation andwho would consider giving it up if itmeant that an operation could beavoided, a hamstring re-educationand rehabilitation programme mayprovide a satisfactory knee foreveryday use. This type of exerciseprogramme however, is not asubstitute for ACL reconstructionbecause the ligament itself neverheals. What it achieves is bettercontrol over the knee, by improvingstrength and by improving thefeedback from the other ligaments(proprioceptive training). This type ofprogramme is supervised by yourphysiotherapist and involves hardwork that can only be done by you.Given adequate provocation,however, the knee will still give wayand further injury may occur.
Patients with an old anterior cruciateligament rupture need to avoidrecurrent giving way and buckling. Ifthese episodes are associated withpain and swelling and are frequent,the knee will develop progressivewear and tear arthritis (osteoarthritis). Patients in this situationneed to either consider the option ofsurgical reconstruction or change thedemands that they are placing ontheir knee.
For those patients who are athleticand who do not wish to considergiving up sporting activities, it maybe that a surgical procedure toreconstruct the ligament will providethe best chance of returning to areasonable level of performance.
Anterior Cruciate LigamentReconstruction
Reconstruction of the anteriorcruciate ligament is a complexsurgical procedure and there aremany different ways to go about it.The preferred method is to use aportion of tendon from elsewhere asa graft. In most case this meansusing two of the hamstring tendons(semi-tendinosis and gracilis) butother tendons can be used. Anothergraft is the middle one third of thepatellar tendon.
Choice of Graft
The two most common graft choicesare the hamstring graft and thepatellar tendon graft. Each hasadvantages and disadvantages andeach has excellent long term results.
Twenty years ago the patellar tendonwas the most commonly used graft.Today around 85% of sports kneespecialists will use the hamstringtendons as their first choice. This isbecause using the hamstringscauses fewer problems. Themajority of the tendons grow backand strength deficits in the harvestedleg vary between 3 and 15% oneyear after surgery. The major loss is“terminal flexion torque”. This is thehamstring power in the last fewdegrees of flexion. This range is
infrequently used by most athletes. Iwould hesitate to use a hamstringgraft in a track sprinter as even a tinyloss of top end speed could makethe athlete uncompetitive. (I wouldsuggest delaying surgery until thetrack career is over.) Nonethelesshamstring ACL grafts have returnedAll Blacks and Silver Ferns to theirformer level.
Patellar tendon grafts also havebeen successfully used for athletesat the highest level for many years.The main problems that concern usis many patients complain of kneecap pain, the inability to kneel andthe loss of the last 3-5 degrees ofextension. (I can’t quite straightenmy knee doc!) Follow up also showsa worrying incidence of early arthritisof the knee cap within 7 years or so.
The technique for reconstructing theanterior cruciate ligament hasimproved significantly in recent yearsand can now be done in anarthroscopically aided manner. Thisdoes not mean that there are noincisions, however, because the graftstill has to be taken in a standardopen type manner. The incisionscan be kept to around 3cm thoughby using the scope. The knee jointitself is usually not opened as all thework in the joint can be done via thearthroscope. This causes less painand a shorter hospital stay andallows for an earlier and better rangeof knee motion. It also means lesswasting of the muscles postoperatively and an earlier return tonormal knee function.
Surgical Technique
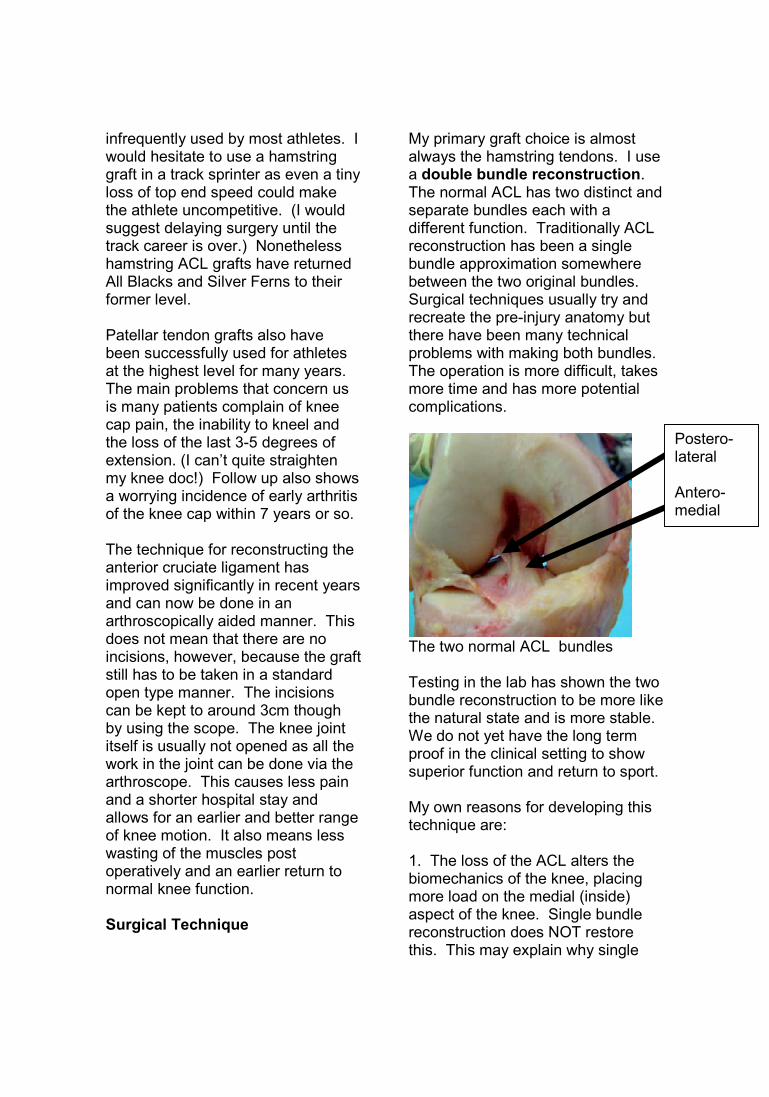
My primary graft choice is almostalways the hamstring tendons. I usea double bundle reconstruction.The normal ACL has two distinct andseparate bundles each with adifferent function. Traditionally ACLreconstruction has been a singlebundle approximation somewherebetween the two original bundles.Surgical techniques usually try andrecreate the pre-injury anatomy butthere have been many technicalproblems with making both bundles.The operation is more difficult, takesmore time and has more potentialcomplications.
The two normal ACL bundles
Testing in the lab has shown the twobundle reconstruction to be more likethe natural state and is more stable.We do not yet have the long termproof in the clinical setting to showsuperior function and return to sport.
My own reasons for developing thistechnique are:
1. The loss of the ACL alters thebiomechanics of the knee, placingmore load on the medial (inside)aspect of the knee. Single bundlereconstruction does NOT restorethis. This may explain why single
Postero-lateral
Antero-medial
bundle reconstruction makes nodifference to the long-term arthritisrate suffered by patients who rupturetheir ACL. Fully 50% eventuallydevelop arthritis whether or notthey have their ACLreconstructed. It is my hope that bymaking biomechanics (forces acrossthe knee) more normal (and doublebundle reconstruction does) this latearthritis rate might be reduced.
2. Few patients with a single bundlereconstruction will describe theirknee as “normal”. Yes, it is goodenough to return to sport but not fullynormal. More patients with a wellperformed double bundle ACL willdescribe their knee as normal. Myown patients with a previous singlebundle in one side and a doublebundle in the other side prefer theirdouble bundle knee every time so farwith no prompting. It is my hope toget a better functional result asnature almost always does knowbest!
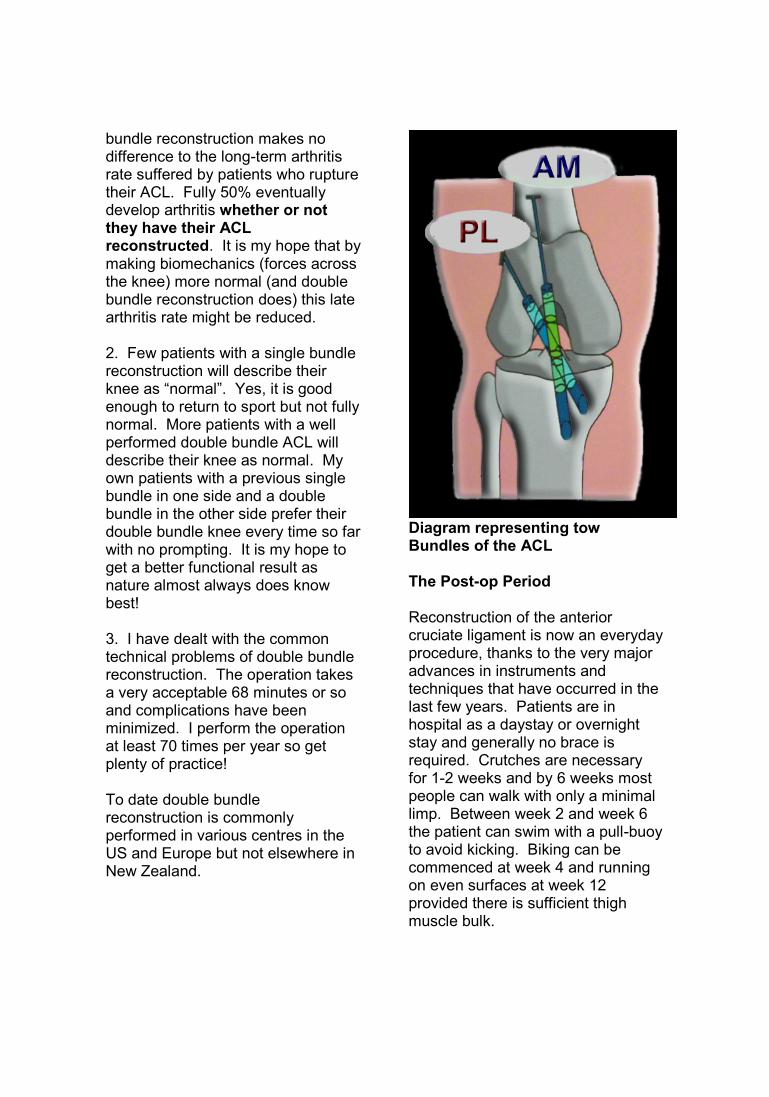
3. I have dealt with the commontechnical problems of double bundlereconstruction. The operation takesa very acceptable 68 minutes or soand complications have beenminimized. I perform the operationat least 70 times per year so getplenty of practice!
To date double bundlereconstruction is commonlyperformed in various centres in theUS and Europe but not elsewhere inNew Zealand.
Diagram representing towBundles of the ACL
The Post-op Period
Reconstruction of the anteriorcruciate ligament is now an everydayprocedure, thanks to the very majoradvances in instruments andtechniques that have occurred in thelast few years. Patients are inhospital as a daystay or overnightstay and generally no brace isrequired. Crutches are necessaryfor 1-2 weeks and by 6 weeks mostpeople can walk with only a minimallimp. Between week 2 and week 6the patient can swim with a pull-buoyto avoid kicking. Biking can becommenced at week 4 and runningon even surfaces at week 12provided there is sufficient thighmuscle bulk.
When first put into the knee, the graftitself is dead. Over a period of time,however, it gains a new bloodsupply, comes back to life andstrengthens. Whilst this processprobably takes some two years tofully complete, it is thought that bythree months some running can becommenced, and by six monthstraining for sport can be started.Actually getting back to full sportdepends on individual progress atthat stage, including the regaining ofproprioception in the knee. Thismeans a return of the ability to runaround corners and to twist and turnon the knee. Exercises to promotethis ability are essential to decreasethe risk of re-injury and areencouraged when running is wellprogressed. You will work closelywith your physiotherapist who willassess your progress. A return tosport can be undertaken anywherefrom six to nine months post-op.
Return to sport is not determined byhow much time has passed but bywhen you have completed a seriesof tests. The “Return to Sport”protocol is a four stage programmewhere progress to the next level isallowed when specific goals havebeen met. Passing the level fourtests is the signal that sport can becommenced. Your physiotherapistor trainer will determine when youhave passed these tests. Aprofessional athlete will almostalways achieve this in six monthsfrom operation. With work andfamily commitments most patientstake 7-9 months.
Because recovery is now muchquicker and easier than previously a
home exercise program is themainstay of post operative treatment.At your one week check you will beprovided with a post operativeprogram. After discharge thatexercise program is continuedwithout change for six weeks. At thesix week mark, most people arehelped by a visit to a sportsphysiotherapist. At that stage anupgraded program can be organizedand, if necessary, supervised. Ifextra therapy is specifically needed,it is easily arranged, and therapistswith particular expertise in this areaof surgery can be recommended.
Another time that most people findtherapy helpful is at the four to sixmonth mark, when they are juststarting to jog or run on the knee. Arehabilitation program here can bemost helpful, particularly to regainproprioception, which is essential fora safe return to sport.
Patients who may benefit from earlytherapy are those who have tightknees and who are having moretrouble than usual getting motionback. This includes the patient withrepairs of other ligaments and thepatient with a meniscal repair whoseknee is tight due to the stitches in thecapsule around the joint.
Time off work
Students can generally return at 7-10days provided that the amount oftime spent on their feet is limited.They may also wish to use theircrutches for a longer period of time.
People in a sit down job can usuallyreturn in two weeks. If the job
involves prolonged standing, thenfour weeks may be more realistic.A job requiring plenty of walking anddriving such as a sales personusually requires six weeks off.
If there is any heavy work to be donethen two months is probably theearliest that a return can be madewith light duties. Jobs requiringprolonged squatting and bendingmay also take at least this long.Heavy manual labour may take fourto five months. Jobs requiring theability to run are the most demandingand these may require six or moremonths for adequate recovery toensue.
Problems of surgery
Overall the number of people whohave problems following ACLreconstruction is small.Nevertheless problems do occur andthese need some consideration.
Bruising in the immediate postoperative period is the commonestproblem. Obviously everybody hassome bruising, but occasionally, it issuch that the knee becomes swollenand sore and the normal milddiscoloration that extends to the footbecomes very obvious. This givesdiscomfort particularly when standingup and may last two weeks. To adegree this can be avoided by notwalking around too much when firstallowed home from hospital. Somepeople however, do bruise moreeasily than others.
D.V.T’s (deep vein thromboses)also occur but are uncommon (lessthan 5%). These represent clots in
the deep veins of the leg, usually thecalf. They probably occur at the timeof surgery and then get slowly biggerover several days. Because of thisthey may not be felt in the first fewdays. If noticeable, it is usually asan ache in the calf at the back of theleg. If this is thought to be occurring,then a Doppler (ultrasound) scan canbe used to detect it and appropriatetreatment organized.
If a patient is at risk for thiscomplication (eg those on a highdoes of oestrogen supplement orhigh dose ‘pill’) then someprophylactic thinning of the bloodcan be performed. This doesincrease bruising and bleedinghowever, and thus, is not regardedas routine treatment.
The concern of having clots in thevein is always that they may spreadto the lungs (pulmonary embolismor PE). This is a rare event but doesrepresent the one major and seriouscomplication of this and other lowerlimb surgery. In the majority ofcases, like DVT’s themselves, it istreatable by thinning of the blood.This prevents new clot from formingand allows the body to slowlydissolve the clot that is present.
Deep infection is uncommon andoccurs in about 1 in every 200cases. Almost all such infectionscan be treated without loss or failureof the graft. Nevertheless, the graftis threatened by this problem whichrequires prompt treatment, includingarthroscopic washout of the kneeand antibiotics. Early diagnosis isvery important to avoid damage tothe rest of the knee joint.
Loss of full extension of the kneeis the most common medium to longterm problem encountered. Some10% of people who undergo ACLreconstruction have a scarring andtightening reaction to that surgery.The reason for this is unknown, but itdoes lead to a general tightening ofthe knee as a whole. This meansslower initial progress, the kneebeing stiffer and more painful. At theend of the day, however, theligament in this group remains tightand strong, and, as the motion isregained, excellent stability can beexpected.
In almost all cases some loss ofextension is common at threemonths following surgery. Most thengo on to regain that motion and atone year less than 5% have anyresidual loss. For that group, thereare procedures that can beundertaken to help this problem andif necessary, these can beperformed. With the newertechniques of reconstruction,however, this type of secondarysurgery is becoming less and lessnecessary. Los of extension is morecommon with the patellar tendongraft than with the hamstring graft.
Graft loosening and failure mayalso occur. Just as there is a 10%group at the tight extreme, so thereis a 10% group who seem toprogressively loosen with time. Thisgroup regains motion early andeasily and as a consequence, theirknees are not particularly sore.Accordingly, they tend to return toactivity early and tend not to protectthe knee as much as perhaps is
ideal. In some instances this cancause early failure of the graft.
A cause of late failure (6-12 months)is where the graft fails to get a newblood supply and thus fails to comeback to life. It is not understood howthis process works, why it works, andwhy, in some instances it does notwork. If the graft remains dead,however, it does not have thecapacity to heal and hence everydaystresses will eventually lead toprogressive rupture of the fibres.Revision reconstruction may then benecessary and is usually successful.
Graft re-rupture can and doesoccur. No graft is as strong as anormal ligament and hence a bigenough injury can cause damage toit. As it turns out however, rupture ofthe ACL in the other leg is morecommon than rupture of the graft.This is not because a graft isstronger than a normal ACL butrather that a large percentage ofpeople who rupture this ligament,have a weaker than normal ligamentin the first place. This may also beseen in some families where severalgenerations all rupture their ACLs.
Patello-femoral pain or ache underthe kneecap (patella) is commononce activity has begun. This ismostly due to the muscles beingwasted and weak and thereforeresponds well to exercise,particularly of the VMO muscle.Physiotherapy at this stage can bevery helpful to reeducate this muscleand to improve patello-femoral jointfunction. This is more common infemale patients who usually haveless thigh muscle to begin with.

Patello-femoral pain can also occurfrom damage to the articular lining ofthe patella itself. This happens inabout 10% of ACL injuries andunfortunately, it can prove relativelydifficult to treat. Nevertheless thisproblem is generally minor andusually does not interfere withsporting activities to any greatextent.
Patella tendonitis or ache from theremaining patella tendon, is notuncommon at some stage duringrecovery when using a patellartendon graft. Fortunately, this tendsto be transient and tends to settleover a 1-2 month period. In mostpeople this occurs when running iscommenced and it represents stresson the remaining smaller patellatendon. This stress then stimulatesthe tendon to get bigger and stronger(hypertrophy) until it is able to cope.As such therefore, with time thetendon usually settles down andstops aching when used. On the fewoccasions when this does nothappen, steroid ionto-phoresis canhelp. This is where cortisone (astrong anti-inflammatory agent) isdriven across the skin and into thetendon electrically (without having toinject it).
Ultimately most knees settle downover a 12 to 15 month period oftime and by that stage most peopleare no longer conscious of theirknee. Ache from the fixation screwis not all that uncommon, butfortunately is rarely bad enough torequire treatment. If the screw isprominent enough to interfere with
kneeling, however, then removalmay well be warranted.
Graft Malposition is a surgical errorwhen the new graft is not placedexactly where the original ACL wassited. The graft only needs to be afew millimeters away from thecorrect site to cause problems likepersistent instability and loss ofmotion. I urge patients to make suretheir surgeon performs this operationfrequently as “practice makesperfect”. I believe ACLreconstruction is not an easyoperation that can be performedaccurately by the occasional surgeon
Summary
The anterior cruciate ligament is amajor and important ligament in theknee which is commonly injured.Treatment depends on the age of thepatient, the exact nature of the injury,the nature of any associated injuries,the lifestyle of the patient and theirfuture sporting aspirations. In thosepatients who are willing to alter theirlifestyle a rehabilitation programmemay be adequate but for the keenathlete who is wanting to return totwisting and turnings sports, areconstruction may be the betteralternative. With the advent of betteroperative procedures to reconstructthis ligament, such as have beendeveloped in the last few years, theproblems that use to be associatedwith this form of surgery are lesscommon and the functional resultsare better. In general 90% of thoseundergoing reconstruction will beable to return to their previous sport
and more than 70% will be able tocompete at their previous level.
Nowadays, an ability to return tosport at the pre-injury level is rarelydue to loss of the anterior cruciateligament: reconstruction of thatligament being generally successful.Rather, it is more usually due toirrepairable damage that has beencaused to other parts of the knee atthe time of the initial injury or insubsequent injuries. (CollateralDamage) It is known that earlyreconstruction with intact menisciand articular cartilage has a betterlong-term outcome than latereconstruction, when repeatedepisodes of instability have damagedthese structures.
What do I do now?
The decision to proceed with surgeryis one that can only be made by you.You should not feel pushed in anyone direction. I see my role asanswering all of the questions youcan think of and helping you makethe decision you believe is best foryour future.
There is no rush to make a decision.If the notes above have raisedquestions for you, you are welcometo email me at [email protected]
If you wish to proceed with surgeryyou need to let my office know sothat I can make an application toACC for funding for your surgery.This process is supposed to take nomore than 21 days but unfortunatelydelays are common. As soon asACC writes to you with an approval
for surgery you can get in touch withRose or Bridget at my office to plan atime for surgery that suits you. Mylists are usually booked up for about6 weeks and your ACC approvalremains valid for 6 months. (It canusually be renewed if necessary.)
Rose and Bridgetphone 09 477 2080email:[email protected]
Recommended

















