C H A P T E R
22
Animal Models of Inflammatory BowelDisease for Drug Discovery
Atsushi Mizoguchi*, Akira Andohy*Department of Pathology, Harvard Medical School, Boston, MA, USA
yDepartment of Mucosal Immunology, Shiga University School of Medicine, Shiga, Japan
A
h
O U T L I N E
Introduction
499Classification of Mouse IBD Models
501Etiology and Mouse IBD Models
501nima
ttp://
The Hygiene Hypothesis 5
01 Appendectomy 5 02 Cigarette Smoking 5 03Classical Therapy and IBD Models
503 Corticosteroids 5 03 Cyclosporine/Tacrolimus 5 04 Nonsteroidal Anti-Inflammatory Drugs 5 04 5-Aminosalicylic Acid 5 05Biological Therapy and IBD Models
505 Anti-TNF-a Therapy 5 05 Anti-Integrin-a4 Therapy 5 06 Anti-Integrin-b7 Therapy 5 07 Anti-Interleukin-12p40 and Anti-Interleukin-23Therapy 5
07499l Models for the Study of Human Disease
dx.doi.org/10.1016/B978-0-12-415894-8.00022-1
Anti-Interleukin-17A Therapy 5
08 Anti-Interleukin-6R Therapy 5 09 Anti-CCR9 Therapy 5 09 Recombinant Interleukin-10 Therapy 5 09 Stem Cell Therapy 5 10 Anti-CTLA4 Therapy 5 11 Anti-CD3 Therapy 5 11 Anti-CD25 Therapy 5 13 Anti-Interferon-Gamma Therapy 5 13 Recombinant GM-CSF Therapy 5 13 Recombinant Interleukin 11 Therapy 5 14 Recombinant Keratinocyte Growth Factor Therapy 5 14 Anti-CD20 Therapy 5 14Conclusion
518Acknowledgments
518References
518INTRODUCTION
Inflammatory bowel disease (IBD) is a chronicrelapsing inflammatory condition that affects over1.5 million Americans.1 The incidence and prevalenceof IBD are increasing with time and in different regionsaround the world, indicating its emergence as a globaldisease.2 IBD is classified into two major forms, Crohn’s
disease (CD) and ulcerative colitis (UC), which aremediated by both common and different mechanismsand have distinct clinical features.3–6 For example, CDis characterized by transmural inflammation affectingthe entire depth of the intestine throughout the digestivetract (frommouth to anus), while UC is characterized bymore focal inflammation restricted to the mucosa of thecolon. A T-helper cell 1 (Th1)-dominant cytokine profile
Copyright � 2013 Elsevier Inc. All rights reserved.

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE500
is often seen in CD, while UC tends to have contribu-tions from the Th2 response.5
The mucosal immune system is distinct from itssystemic counterpart by virtue of its enormous anti-genic exposure (commensal flora, food antigens, path-ogens), making IBD pathogenesis more complicated.7
Indeed, many kinds of knockout (KO) and transgenic(Tg) mouse strains have been shown to develop colitisand/or ileitis spontaneously. So far, at least 69 kindsof animal model are available to study IBD.8 Thesemodels can be classified into four groups dependingon the location of inflammation (Fig. 22.1). The “colitismodel” develops inflammation only in the colon, the“ileitis model” only in the small intestine, the “pan-enterocolitis model” in both colon and small intestine,and the “systemic model” in multiple organsincluding the intestine. Importantly, new therapeuticideas for IBD have been stimulated by preclinicalstudies in the wide variety of animal models ofIBD.9,10
SAMP/YitEpithelial-specific N-cadherin KI
TNFR1-deficient, epithelial-specific TGFβ activation kinase
Src-homology-2-containing inositol 5 phosphatase (SHIP)1 KO
TNF(ARE) KI
CD2-specific TNFS
Epithelial-sp
Epithelial-specific
Runt-related transcription factor RUNX3 KO
Inducible enteric glia KO
Epithelial-specific X-box-binding protein (XBP) 1
Glutathione peroxidase (GPX) 1
Ileitis
OxazolonTNBSCotton-top tamarin
C3H/HeJBir CD3eT
Janus family tyrosine kinase ( T-cell-specific suppressor of cytokine signaling (SOC
Epithelial-specific core 1β1,3-galactosyltransfera
IL-7 Tg
RAG KO treated with anti-CD40
CD45RB IL-10 KO
CD1
TCRα K
Wiskott-Aldrich syndrome protein (WASP) K
Phosphatidyl inositol 3 kinase (PI3K) p110δ KI
CD4-specific phosphoinositide-dependent kinase (PD
T cell-specific B-lymphocyte-induced maturation protein 1
G protein Gαi2 KO
Liver-specific soluble C
CD11c-specific integin β8 KOInducible STAT4 Tg
Myeloid-specific STAT3 KO
Inducible STAT3 KO
24αβ TCR Epithelium polarized sorting factor AP1B KO
IL-6 receptor gp130 KI
Epithelial-specific IκB kinase NEMO KO
T
K
Multiple drug resistanc
RAG KO with deficiency of nuclear factor of activated T ce
RAG KO with deficiency of T-box transcription facto
Colitis
FIGURE 22.1 The different types of IBD models. These include chemspontaneous models (black), congenital models (brown), and genetically einto conventional transgenic models (light blue), conventional knockoutknockout models (pink), knock-in models (orange), and innate models (pu(colitis, red square), small intestine (ileitis, blue square), or multiple orga
VI. URINARY TRACT, K
Over 71 susceptibility loci/genes in CD and over 47 inUC have already been identified in humans.3,11,12 There-fore, one of the current topics in the field of IBD modelsis to identify the biological function of these IBD suscep-tibility genes, and these studies have brought manynovel concepts to further understand IBDpathogenesis.3,11–13 Another topic is to identify thecommensal bacterial composition associated with IBD.The importance of this topic has been highlighted bythe fact that development of colitis was abolished inthe majority of murine IBD models when they weremaintained in a germ-free condition.14 The relevanceof this field to human IBD is supported by recent meta-genome analyses of the human intestinal tract, whichhave identified that CD, UC, and healthy individualsall had distinct bacterial composition patterns.15
Interestingly, Neurath and colleagues have proposed“10” mysteries with IBD, some of which are associatedwith the etiological factors.16 Among them, the hygienehypothesis (probiotics), appendectomy, and cigarette
1-deficient DKO
F15 (TL1A) Tg
ecific IL-15 Tg
Caspase-8 KO
KO
IL-2 KO CD25 KOCD122 KO
TGFβ KO
Dominant negative TGFβR II Tg
Casitas B-lineage lymphoma protein cb1-b KO
Ubiquitin-editing enzyme A20 KO
CD2-specific TNFSF14 (LIGHT) Tg
B-cell-specific CD40L TgEndothelial-specific integrin αV KO
CD4-specific TGFβ KO
Autophagy-related gene (Atg) 5- deficient thymus-implanted nu/nu mice
/2 DKO
DSS
g model
JAK) 3 KOS) 1 Tg
se KO
Mucin 2 KO
32 KO
O
O
K) 1 KO
(Blimp1) KO
D86 Tg
Tg x CD1d Tg
LR5 KO
eratin 8 KO
e (Mdr) 1a KO
lls (NFAT)c2
r T-bet
Systemic Inflammation
ically induced models (dark green), cell-transfer models (light green),ngineered models. Genetically engineered models are further classifiedmodels (red), conditional transgenic models (dark blue), conditionalrple). These models spontaneously develop inflammation in the colonns including the colon and small intestine (systemic, green square).
IDNEY AND BOWEL

ETIOLOGY AND MOUSE IBD MODELS 501
smoking may have potential for IBD therapy. In addi-tion, several conventional and biological drugs havebeen successfully, or unsuccessfully, applied for IBD,or are currently in clinical development.1,17 Therefore,this chapter focuses on these fields (etiological factorsand drugs) that may have immediate therapeutic poten-tial. The authors hope that the datadsummarized in thischapterdwill direct clinicians who are unfamiliar withanimal models of IBD to be familiarized on interpretingdata from IBD models, for the consideration of futureclinical trials of candidate therapies. In addition, thesedata may be helpful for basic researchers to realizesome clinically relevant fields for bridging the gapbetween the bench and the bedside.
CLASSIFICATION OF MOUSE IBDMODELS
In addition to the location of inflammation (seeabove), IBD models can be classified into five majorgroups depending on the method of disease induction(Fig. 22.1)d“chemically induced models” such as thedextran sodium sulfate (DSS) model, in which acutecolitis can be induced by administration of DSS indrinking water; “cell-transfer models,” such as theCD45RB model, in which colitis can be induced inimmunodeficient hosts by adoptive transfer ofCD4þCD45RBhigh naıve T cells from wild-type (WT)donors; “spontaneous models,” such as the cotton-toptamarin (a marmoset native to a small geographic regionof Colombia) that develops colitis presumably throughenvironmental stress when maintained at US; “congen-ital models,” such as SAMP/Yit mice that develop ileitisin a senescence-prone strain derived from 24 genera-tions of siblings from a litter of AKR/J mice; and “genet-ically engineered models” that develop colitis and/orileitis by genetically engineered deletion or overexpres-sion of certain molecules.8,18,19 In addition, geneticallyengineered models are further classified into sixsubgroups.8 “Conventional transgenic” or “conven-tional knockout” mice are genetically engineered tocontinuously overexpress or lack the gene of interest inall cell types, respectively. “Conditional transgenicmice” are genetically engineered using cell-specificpromoters to overexpress the gene of interest in a specificcell type. “Conditional knockout mice” are geneticallyengineered to lack a gene of interest in a specific celltype or to make the gene deletion inducible at anytime. “Knock-in (KI) mice” are genetically engineeredto carry a mutation in the gene of interest. “Innatemodels” are immune-deficient mouse-based systems,such as recombinant activation gene (RAG) KO micethat lack both T and B cells.
VI. URINARY TRACT, K
At least 66 kinds of IBD model had been establishedby early 2011,8 and 3 new genetically engineered IBDmodels have since been established (Fig. 22.1). Amongthe new models, epithelial-cell-specific deletion ofcaspase-8 (under control of the villin promoter) resultedin the spontaneous development of ileitis but not colitisin more than 80% of mice by inducing “necroptosis”.20
Polarity of epithelial cells is, in part, established by anepithelium-specific polarized sorting factor adaptorprotein, AP1B. AP1B KOmice spontaneously developedantibiotic-treatable colitis at 8 weeks of age.21 24ab trans-genic (Tg) mice carry a T-cell receptor (TCR) froma CD1d-reactive natural killer T (NKT) cell line withexpression of TCRVa3.2 and Vb9. When 24ab Tg micewere crossed with CD1d Tg mice, 70% of them devel-oped colitis at 6 months of age.22 The spontaneousdevelopment of colitis was still observed when theywere further crossed with RAG1 KO mice (24ab Tg �CD1d Tg � RAG KO) that had only a mono-associatedT-cell population, TCRVa3.2þ Vb9þ NKT cells.
ETIOLOGY AND MOUSE IBD MODELS
The Hygiene Hypothesis
Environmental factors are essential components ofthe pathogenesis of IBD.23 The hygiene hypothesis hasbeen proposed because of the fact that better livingconditions during childhood have been associatedwith an increased risk of IBD.1,23 North–south gradientsexist within individual countriesdCD is less common inthe southern US and in the south of France.24 Givena more favorable environment (warm temperaturewith high humidity) for microbes in the southern parts,these north–south gradients may support the hygienehypothesis.
Analysis of the recent evolutionary history of humaninterleukin (IL) genes through integrating informationon environmental variables suggested that helminthinfections represent a major selective force of thehygiene hypothesis in IBD.25 In contrast, a large,population-based cohort study suggested that helminthinfections do not reduce the risk for IBD.26 Although theinvolvement of prior helminth infections in the hygienehypothesis of IBD is still controversial, preventive andtherapeutic effects of helminth infections on colitishave been well explored using mouse IBD models.27
Pre-exposure to Schistosoma mansoni eggs, Trichinella spi-ralis, or Hymenolepis diminuta made mice more resistantto Th1-mediated acute colitis induced by trinitroben-zene sulfonic acid (TNBS) or dinitrobenzene sulfonicacid (DNBS).28,29 A therapeutic effect of S. mansoni andAncylostoma caninum extracts has also been reported inthe TNBS colitis model.30 The beneficial effect of
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE502
helminths on colitis may be mediated by suppression ofinterferon gamma (IFN-g) and IL-17 production,enhancement of IL-4, IL-10, and transforming growthfactor beta (TGF-b) production, induction of regulatoryCD8þ T cells, and/or inhibition of macrophageactivation.30–33 TGF-b-signaling in T cells may berequired for the suppression of the Th1 response byhelminthic parasites.34 Different effects of helminths onTh2-mediated colitis in humans versus mice have beenreported. A randomized double-blind placebo-controlled human trial has demonstrated some benefi-cial effect of Trichuris suis ova on UC that has significantcontributions from Th2 responses.35 On the other hand,pre-exposure toH. diminutamademice more susceptibleto Th2-mediated acute colitis induced by oxazolonethrough enhancement of IL-5 production.36
A helminth-independent hygiene hypothesis may besupported by a Th2-mediated chronic colitis model ofTCRa KO mice. Gaskins et al. reported in 1997 thatTCRa KO mice spontaneously developed colitis whenmaintained under specific pathogen-free conditions(SPF), but failed to do so when maintained in a conven-tional facility (CF).37 This observation, although unex-pected, has been confirmed by a subsequent study.38
Enhanced exposure to microorganisms in CF preventedthe development of colitis in TCRa KO mice by stimu-lating the expansion of peritoneal B1 B cells producinglarge amounts of natural IgM that can recognize a broadspectrum of microorganisms. However, no significantdifference in the bacterial colonization pattern betweenSPF and CF TCRa KO mice was found using terminal-fragment-length polymorphism (T-RFLP) analysis,a powerful approach for assessment of diversity ofbacterial flora. In addition, helminth was undetectablein both SPF and CF TCRa KO mice. These findings raisethe possibility that the prevention of colitis in CF ismediated by enhanced exposure to viruses and/orfungi. Indeed, involvement of viruses in the hygienehypothesis has been proposed.39 In addition, adminis-tration of chitin, which is a major component of fungi,has recently been shown to prevent the developmentof colitis in TCRa KO mice by inducing immunetolerance.40
Appendectomy
One of the mysteries with IBD is the negative associ-ation of development of UC, but not CD, with a priorhistory of appendectomy.16 This negative associationwas first demonstrated in 198741 and has since beenconfirmed by many, but not all, case-control studiesand meta-analyses.42–44 Speculations have been raisedto explain the mysterious but consistent finding.A possibility is that the appendix is actively involved
VI. URINARY TRACT, K
in the development of UC. A second possibility is thatpatients who are more susceptible to appendicitis carrygenetic loci protective against UC. A third possibility isthat appendicitis rather than appendectomy serves asthe preventive factor, presumably by generatingimmune tolerance against UC development.45
Accumulating data from mouse models of IBD mayfavor the first possibility. As mice lack an appendixanatomically, resection of cecal patches (analog ofhuman appendix lymphoid follicles) was performed inTCRa KO mice (a model of human UC) as a mimic ofhuman appendectomy. Interestingly, development ofcolitis of TCRa KO mice was suppressed when theappendectomy was done before 3 weeks of age, whereasappendectomy after 3 weeks of age had only minimaleffect on this colitis.46 A similar finding has since beenconfirmed in humans; a stronger negative associationof development of UC with appendectomy wasobserved in patients who underwent appendectomybefore 20 years of age.42,47 A preventive effect of appen-dectomy on DSS-induced acute colitis has also beenreported.48 Cecal patches of TCRa KO mice provideda place for the priming of restricted CD4þ Tcell popula-tions carrying a negatively charged amino acid residueat a specific region within an antigen-recognitiondomain (complementary determinant region 3) ofsome TCRb chains, such as the Vb8.2 chain.49 Interest-ingly, the CD4þ T cells were shown to possess colito-genic ability.49 Indeed, colitogenic CD4þ T cells weredemonstrated in the CD45RB colitis model to firstmigrate into the cecal patch rather than the colon.50
Since the appendix and cecum serve as a major reservoirof commensal microbes that actively participate in thepathogenesis of IBD,14 it is possible that lymphoid folli-cles, such as those of the appendix, and cecal patches inbacteria-rich locations provide a place for the initialpriming of colitogenic CD4þ T cells. The primedCD4þ Tcells may then migrate into the colon to expandthe inflammation. Indeed, an area in the cecum withfocal inflammatory activity surrounding the appendicalorifice, referred to as the “peri-appendical red patch,”has been recognized in 7.9% of patients with distal ulcer-ative colitis, so-called “left-side UC.”51 Similar findingswith much higher incidence have been reported sepa-rately by different group.52–54
In addition to the preventive effect, a potential thera-peutic effect of appendectomy on UC was proposed in2000 by a case report showing the drug-free remissionof a patient with ulcerative proctitis (inflammationrestricted to the rectum) after appendectomy.55 A similartherapeutic effect of appendectomy has since beendescribed in scattered case reports.56,57 In contrast, a clin-ical trial in six patients with refractory UC failed toconfirm the therapeutic effect of appendectomy.58 Inter-estingly, another study showed that appendectomy
IDNEY AND BOWEL

CLASSICAL THERAPY AND IBD MODELS 503
transiently improved endoscopically recognized inflam-mation in five patients with left-side UC, whereasinflammation remained unchanged or was exacerbatedin four patients with pancolitis after appendectomy.59
The effect of appendectomy on left-side UCmay be sup-ported by a recent prospective case series study of30 patients with ulcerative proctitis; 40% patients expe-rienced a complete remission (as judged by a “simpleclinical colitis activity index” score of 0) after appendec-tomy.60 The remission was also paralleled by endoscopicscores. In mouse IBD models, a preventive, but not ther-apeutic, effect of appendectomy has been explored.
Cigarette Smoking
Another mystery with IBD is the different effects ofcigarette smoking on UC versus CD.1,16 Smoking isa risk factor for CD, whereas it serves as a suppressivefactor against UC. Several animal studies have been con-ducted to dissect the mysterious mechanism. One studyproposed an ability of nicotine to induce the differentia-tion of CD4þ T cells into regulatory T cells (Treg)through inhibition of their differentiation into Th17T cells.61 IL-4 induced the expression of a7 nicotinicacetylcholine receptors (a7nAChR) on colonic CD4þ Tcells, and thus pretreatment with nicotine (total dosesof 7.5 mg/k g through subcutaneous (s.c.). injections)enhanced Treg development and simultaneouslyinhibited Th17 development, making mice resistant toTh2-mediated acute colitis induced by oxazolone. Incontrast, IL-12 (an inducer of the Th1 response) sup-pressed the expression of a7nAChR on colonic CD4þT cells, allowing nicotine to exacerbate a Th1-mediatedcolitis induced by TNBS through inhibition of Tregdevelopment.61 Similarly, pre-exposure to cigarettesmoking made rats more susceptible to Th1-mediatedacute colitis induced by TNBS. The increased suscepti-bility was associated with a decreased colonic super-oxide dismutase activity.62 Colonic dorsal rootganglion (DRG) neurons form peripheral afferent path-ways that carry sensory information from the colon tospinal cord. The ability of nicotine to suppress thehyperexcitability of colonic DRG was recently shownin a DSS-induced acute colitis model.63
However, the mechanism of smoking may be morecomplicated. In IL-10 KO mice (another model of CD),administration of nicotine (12.5 mg/ml) in drinkingwater suppressed chronic colitis.64 This suppressionwas associated with an increased production of intes-tinal trefoil factor, which is required for epithelialrepair.65 One component of cigarette smoke is thegaseous molecule carbon monoxide (CO). Exposure ofIL-10 KO mice to 250 ppm CO for 4 weeks improvedchronic colitis, and this improvement was mediated by
VI. URINARY TRACT, K
heme oxygenase (HO)-1-dependent inhibition of IFN-g-induced IL-12p40 expression in macrophages throughIFN regulatory factor (IRF) 8.66 In addition, exposure toCO improved Th2-mediated chronic colitis of TCRa KOmice (a model of UC).67 Treatment with the pharmaco-logical HO-1 inducer cobalt protoporphyrin was alsobeneficial for this colitis. The improvement of the colitiswas associated with enhanced production of IL-10 byCD11bþ cells and of IL-22 by CD11b� cells.
CLASSICAL THERAPY AND IBD MODELS
Corticosteroids
Corticosteroids have been widely but cautiously usedto treat the acute exacerbation of UC and CD.1 As seen inIBD patients, the therapeutic effect of dexamethasone(Dex) has been demonstrated in experimental modelsof both UC and CD. Intraperitoneal administration ofDex (100 mg) for 3 days attenuated the ileitis ofSAMP-1/Yit mice (a model of CD).68 A beneficial effectof Dex has also been shown in Th1-mediated acutecolitis induced by TNBS.69 The glucocorticoid-inducedleucine zipper (GILZ), which can be induced by Dex,was shown to improve chronic colitis of IL-10 KOmice.70 Dex therapy also improved Th2-mediatedchronic colitis of TCRa KO mice71 and Th2-mediatedacute colitis induced by administration of oxazolone.72
In DSS colitis models, the effect of Dex seems todiffer depending upon the disease stage. Dex therapyexacerbated DSS-induced acute colitis, whereas itimproved DSS-induced chronic colitis that was inducedby repeated administrations of DSS.73,74
Although Dex has a strong immune suppressiveeffect, the mechanism has been largely unknown. Anattractive mechanism in this regard has been proposedby IBD models. Combined stimulus with Dex and anactive form of vitamin D3 induced the differentiationof human and mouse naıve T cells to an IL-10-producing CD4þ Tcell subset termed “Tr1.”75 Adop-tive transfer of the in vitro-generated Tr1 was able tosuppress the colitis of a CD45RB model, which wasinduced by effector CD4þ T cells.76 Dendritic cells(DCs) generated in vitro by the same regimen (Dexand vitamin D3) were also reported to possess suppres-sive ability against this colitis.77
Glucocorticoid-induced tumor necrosis factorreceptor (TNFR)-family-related protein (GITR) was firstidentified in 1997 by comparing the gene expressionprofile between Dex-treated versus untreated mouseT-cell hybridoma (3DO) through a differential displayanalysis.78 GITR has since been found to be expressedat high levels by a CD4þCD25þ T cell population thatcontains both recently activated CD25þ effector T cells
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE504
and Foxp3þ regulatory Tcells (Treg).79 Interestingly, theauthors found that the ligation of GITR abolished theimmune suppressive ability of Treg. Consistent withthis observation, GITR deficiency protected mice fromTNBS-induced acute colitis,80 and ligation of GITR byan agonistic antibody led to the exacerbation of thiscolitis.81 Alternatively, a GITRþ, but not GITR�, CD4þT-cell population was shown to suppress the colitis ofa CD45RB model,82 raising the possibility that a GITRþCD4þ T-cell subset serves as a regulatory cell popula-tion when GITR is not activated. An alternative possi-bility has been raised by a recent reportdGITR, whichis expressed by antigen-presenting cells but not by Tcells, was required for the suppression of colitis ina CD45RB model.83 The authors suggested that thesuppressive function of GITR in this colitis may bemedi-ated by the induction of tolerogenic CD103þ PDCA(plasmacytoid marker)þ plasmacytoid DCs that arerequired for the development of Treg.
A therapeutic effect of Dex on colitis/ileitis hasbeen shown in seven kinds of IBD models, includingTh1-mediated chronic and acute colitis, Th2-mediatedchronic colitis, and chronic ileitis. Corticosteroids repre-sent a conventional drug that has been widely used fortreatment of UC and CD.1
Cyclosporine/Tacrolimus
Cyclosporinedwhich serves as an inhibitor ofcalcineurindis effective in hospitalized patientswith severely active UC, but not CD.1 Tacrolimus(FK506)dwhich exhibits similar pharmacological ac-tion to cyclosporinedalso induced rapid clinicalresponse and mucosal healing in hospitalized patientswith steroid-refractory UC.84 The current data, al-though needing further evidence from high-qualityrandomized controlled trials and careful attention tonephrotoxicity, also support the use of tacrolimus inCD that is refractory to conventional therapies.85,86
Calcineurin is required for the activation of nuclearfactor of activated T cells (NFAT) by allowing the trans-location of NFATc into nucleus.87 Deficiency of NFATc2has been shown to suppress Th2-mediated acutecolitis induced by oxazolone.88 Acute colitis in TNBSmodels is mediated by different cytokine responsesdepending upon the mouse strain used. TNBS colitisin the majority of mouse strains, such as SJL, was depen-dent on the Th1 response, whereas TNBS colitis in theBALB/c strain was mediated by an IL-4-dependentTh2 response.89 Treatment with cyclosporine (7.5 mg/kg) suppressed the Th2-mediated TNBS colitis inBALB/c mice.69 In contrast, no therapeutic effect ofcyclosporine on colitis has been proposed in IL-10 KOmice90 or CD45RBmodels.91 Since NFATs have an ability
VI. URINARY TRACT, K
to recruit the transcription factor GATA3 to Th2-typegene promoters such as IL-5,92 this may be one ofreasons why cyclosporine is beneficial to UC and Th2--mediated experimental colitis but not to CD or Th1/Th17-mediated experimental colitis.
Avery rapid therapeutic effect of cyclosporine enemaon DSS-induced acute colitis was shown in 1993,93 anda beneficial effect of intraperitoneal cyclosporine injec-tions on this acute colitis was also demonstrated.94 Theauthors showed the ability of cyclosporine to enhancethe expression of TGF-b, which in turns suppressesepithelial cell apoptosis. Leucine-rich-repeat kinase 2(LRRK2)dwhich is encoded by a major susceptibilitygene for CD3,11,12dwas shown recently to possess anability to serve as a negative regulator of NFAT-driveninnate immune responses in myeloid cells.95 Deficiencyof LRRK2 enhanced nuclear localization of NFAT1 andmade mice more susceptible to DSS-induced acutecolitis.
A beneficial effect of tacrolimus on experimentalcolitis was first proposed in 1995 by Asakura andcolleagues, who utilized a rat DSS colitis.96 Tacrolimusdwhich was entrapped into nanoparticlesdhas sincebeen shown to have a more beneficial effect on rat DSScolitis when it was rectally, rather than orally, adminis-tered.97 In a mouse TNBS colitis model, pretreatmentwith tacrolimus suppressed local inflammation (asjudged by histology of colitis) but not systemic inflam-matory response (as judged by body weight loss).98
Intrarectal administration of tacrolimus had a beneficialeffect on acute colitis in a mouse DSS model and chroniccolitis in IL-10 KO mice, presumably through inductionof apoptosis in activated macrophages.99 In contrast, noeffect of tacrolimuswas shown in chronic colitis that wasinduced in immune-deficient mice by adoptive transferof IL-10-deficient CD4þ T cells.90
The therapeutic potential of cyclosporine and tacroli-mus on colitis has been shown using three kinds of IBDmodels in mice and rats, with some exceptions. Cyclo-sporine and tacrolimus have been used for treatmentof hospitalized patients with severely active UC butnot CD.1
Nonsteroidal Anti-Inflammatory Drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs)dwhich inhibit the production of prostaglandinsand thromboxanes through cyclooxygenase (Cox)-1and 2dhave been reported to aggravate or reactivateIBD.1,100 Enteric commensal bacteria play a major rolein chronic colitis of IL-10 KO mice.14 Development ofcolitis in IL-10 KO mice was abolished or reduced whenthey were maintained under germ-free conditions or inthe absence of Helicobacter species, respectively.14,101
IDNEY AND BOWEL

BIOLOGICAL THERAPY AND IBD MODELS 505
Since the incidence of spontaneous colitis developmentin IL-10 KO mice was low in the absence of Helicobacterspecies, NSAIDs have been used to rapidly and repro-ducibly induce the development of this colitis. Contin-uous administration of piroxicam (200 ppm) in mousechow for 2 weeks induced the rapid development ofcolitis in IL-10 KO mice within 4–6 weeks after termina-tion of piroxicam treatment.100 Administration of eithera selective Cox-1 inhibitor (SC-560) or a selective Cox-2inhibitor (SC-58236 orNS-398) failed to induce the devel-opment of colitis in these mice, but the combination ofthese inhibitors was able to do it.100 Eicosanoidsdwhichare derived from arachidonic aciddinclude both Cox-derived products and 5-lipoxygenase (5-LO)-derivedproducts, also known as leukotrienes. However, 5-LO-derived leukotrienes were not required for thepiroxicam-induced colitis of IL-10 KOmice.102 Enhancedmucosal exposure to enteric bacteria due to the increasedapoptosis of colonic epithelial cells may be responsiblefor the piroxicam-induced colitis.103 An IL-13 decoyreceptor IL-13Ra2dwhich serves as an inhibitor of IL-13 activitydhas been proposed to mediate thepiroxicam-induced colitis by enhancing Th17responses.104 In addition, the rapid and reproducibleinduction of colitis in the piroxicam system has allowedinvestigators to develop a methodology for the assess-ment of colitis. For example, the applicability of2-deoxy-2-[18F]fluoro-D-glucose (FDG) uptake by posi-tron emission tomography (PET) for evaluation of colitiswas demonstrated using a piroxicam-induced colitissystem.105 Activity-based probesdwhich covalentlymodify activated cathepsinsdhave recently been sug-gested as a biomarker of colitis using this system.106
Exacerbation of inflammation by NSAIDs has alsobeen demonstrated in other IBD models. Administra-tion of piroxicam induced the rapid development ofTh2-mediated colitis of TCRa KO mice within 14 daysafter termination of treatment.71 Development of ileitisin SAMP1/Yit mice was elicited by piroxicam treatmentfor 3 weeks.107 In DSS-induced acute colitis, oral admin-istration of a non-selective NSAID (indomethacin) ora combination of Cox-1 (SC-560) and Cox-2 (celecoxib)inhibitors exacerbated the disease.108
NSAIDs have been shown to elicit chronic colitis andileitis in three kinds of chronic IBD models and an acutecolitis model. NSAIDs have been a high-alert drug inIBD patients.
5-Aminosalicylic Acid
5-aminosalicylic acid (5-ASA) preparations are thefirst drugs to be used for UC. This drug, although itsprecise mechanism of action is still unclear, has beensuccessfully applied to treat mild to moderately activeUC and to prevent UC relapse.1
VI. URINARY TRACT, K
Therapy with 500 mg/kg 5-ASA (mesalamine) inmouse chow suppressed epithelial dysplasia withoutaffecting colonic inflammation in piroxicam-treated IL-10 KO mice, while therapy with 1650 mg/kg 5-ASA inmouse chow reduced the dysplasia in conjunction withimproving colonic inflammation.109 Of note, theauthors discovered the ability of 5-ASA to reduce Aktand b-catenin signaling in epithelial cells, particularlywithin middle-to-upper crypts. A nitric-oxide-releasingderivative of mesalamine (NCX-456), but not conven-tional mesalamine, was reported to have a beneficialeffect on TNBS-induced acute colitis.110 The authorsproposed that NCX-456 inhibited the proliferation ofand simultaneously induced the apoptosis of activatedTh1 T cells. A beneficial effect of 5-ASA has also beenreported in DSS-induced and oxazolone-induced acutecolitis models.72,111
A beneficial effect of 5-ASA on colitis has been sup-ported by four kinds of IBD models, and 5-ASA hasbeen widely used for the treatment of UC.
BIOLOGICAL THERAPY ANDIBD MODELS
Anti-TNF-a Therapy
The most successful biological therapy for IBD is thehumanized anti-TNF-a (tumor necrosis factor alpha)antibody infliximab, which has been approved since1998 by the US Food and Drug Administration (FDA)for treatment of IBD.17 Infliximab is effective at inducingremission in moderate to severely active CD, and is usedas a maintenance therapy. This therapy is also effectiveat inducing remission in moderate to severely activeUC outpatients.1
TNF-a is one of the most studied cytokines in IBDmodels. The pathogenic role of TNF-a is well high-lighted by the spontaneous development of ileitis inTNF(ARE)mice, in which TNF-a expression is stabilizedby the absence of functional adenosine-uracil multimers(AU-rich elements, ARE).112 In addition, the pathogenicabilities of TNF-a to initiate and promote intestinalinflammation have been demonstrated using both loss-of-function and gain-of-function approaches in manyIBD models, including Th17-mediated chronic colitisof IL-10 KO mice, Th1-mediated chronic colitis ofCD45RB and CD3ε transgenic models, Th1-mediatedacute colitis of TNBS models, and ileitis of SAMP/Yitmice.8 In contrast, there was no significant beneficialeffect of anti-TNF monoclonal antibody (mAb) on theearly stage of Th2-mediated chronic colitis of TCR-a KO mice,113 but absence of the TNF receptor TNFR2improved this colitis.114 On the other hand, bothTNF-a and TNFR1 were dispensable in the development
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE506
of colitis in A20 KO mice.115 Interestingly, administra-tion of TNF-a ameliorated Th2-mediated acute colitisinduced by oxazolone through induction of extraadrenal glucocorticoid synthesis,116 suggesting a protec-tive role of TNF-a in this acute colitis model. Similarly,TNF-a KO mice were more susceptible to DSS-inducedacute colitis.117,118
Clinical trial data have suggested that 30–40%patients fail to have an initial response if anti-TNFtherapy is introduced after the failure of nonbiologicaltherapies.119 There are also some safety issues withanti-TNF-a therapy, such as an increased risk of infec-tions.119 A two-fold increased risk of hospitalizationwith bacterial infections was seen among patients whoreceived anti-TNF-a therapy as compared to thosewho received methotrexate therapy.120 The ineffective-ness in a subset of patients and increased risk of infec-tions may be causeddin partdby the ability of TNF-ato stimulate both TNFR1 and TNFR2, which may playdistinct biological functions. In DSS-induced acutecolitis, the disease was exacerbated by absence ofTNFR1 but not TNFR2.121 In addition, after DSS chal-lenge, mortality, presumably due to bacterial invasion,was significantly increased in TNFR1-deficient RAG-1(a recombination activating gene) double KO mice lack-ing both T and B cells as compared to TNFR2-deficientRAG-1 double KOmice and RAG-1 KOmice, suggestingthat TNFR1 expressed by innate cells such as epithelialcells plays a protective role against enteric microorgan-isms under an acute intestinal inflammatory condi-tions.122 Indeed, TNFR1 has been shown to promoteepithelial cell survival by protecting TNF-a-inducedapoptosis.123 In addition, a requirement for TNFR2,but not TNFR1, for TNF-a-induced epithelial barrierdysfunction has been demonstrated.124
The roles of TNFR1 versus TNFR2 in colitis have alsobeen explored using TNBS models. TNFR1 KO micedeveloped a more severe form of colitis with increasedmortality after TNBS challenge, while the colitis wasimproved in TNFR2 KO mice.125 Another groupreported that both TNFR1 KO and TNFR2 KO micewere resistant to TNBS-induced acute colitis, buta systemic inflammatory response was seen in TNFR1KO, but not TNFR2 KO, mice after TNBS challenge.126
An interesting observation was made from epithelial-cell-specific TGF-b-activated kinase 1 (TAK1) KOmice. These mice developed very severe epithelialdamage in the small intestine by 3 days of age.127 Theepithelial damage was rescued by absence of TNFR1,but development of ileitis and colitis was in turn eli-cited in TNFR1-deficient epithelial-specific TAK1double KO mice. On the other hand, deficiency ofboth TNFR1 and TNFR2, but not each individually,inhibited the development of ileitis of TNF(ARE)mice.128 In addition, lack of TNFR2 on CD4þ T cells
VI. URINARY TRACT, K
may exacerbate colitis of CD45RB models.129 Takentogether, these findings highlight much a more compli-cated role played by TNFR1 and TNFR2 in IBD thanpreviously predicted.
The pathogenic role of TNF-a in colitis has been sup-ported by many IBD models, with some exceptions. Onthe other hand, some acute colitis models have proposeda protective role of TNFR1 against microbial infections,which may provide a clue to understand how anti-TNF-a therapy increases the risk of infections. Anti-TNF-a therapy has been approved by the FDA fortreatment of IBD.
Anti-Integrin-a4 Therapy
There are at least 18 a-subunits and 8 b-subunits ofintegrins, which link together as heterodimers to formmore than 24 different functional integrin receptors thatallow leukocytes to travel into different tissues.130
Among them, a4 integrin forms heterodimers with b7and b1 integrins. The heterodimer of a4b7 is a pivotalmediator of leukocyte homing into the gastrointestinal(GI) tract through its interaction with mucosal addressincell-adhesion molecule (MAdCAM)-1. On the otherhand, the heterodimer of a4b1 binds to the vascularcell-adhesion molecule (VCAM)-1, which mediatesleukocyte homing into the central nervous system(CNS). The feasibility ofmodulation of leukocyte homingfor IBD therapywas first demonstrated in 1993 by Podol-sky et al.131 They showed that treatment with anti-a4--integrin mAbs attenuated spontaneously developingcolitis in the cotton-top tamarin, a marmoset native toa small geographic region of Colombia.131 This observa-tion has prompted several human trials, and anti-a4--integrin therapy (natalizumab) has been approvedsince 2008 by the FDA for inducing andmaintaining clin-ical response and remission in patients with moderatelyto severely active CDwho had an inadequate response toconventional and anti-TNF therapies.17,132
After the discovery of the beneficial effect of anti-a4-integrin therapy on colitis of cotton-top tamarins, role ofa4 integrin in colitis has been explored in other IBDmodels. A small molecule antagonist against a4 integrinwas shown to have therapeutic potential inDSS-induced acute colitis.133 Interestingly, treatmentwith anti-a4-integrinmAbsalonehadno significant bene-ficial effect on the ileitis of SAMP/Yitmice, but a combina-tion therapy of anti- a4-integrin and anti-ICAM1(intercellular adhesion molecule) mAbs improved theileitis in 70%of thesemice.68 In contrast, a long-term treat-mentwith anti-a4-integrinmAbswasproposed to exacer-bate chronic colitis and increase the risk of cancerdevelopment in Gai2 KO mice (a model of UC).134 Theexacerbationof colitismaybe causedby impairedhomingof Ab-producing B cells into the inflamed colon.134
IDNEY AND BOWEL

BIOLOGICAL THERAPY AND IBD MODELS 507
In addition to anti-a4-integrin therapy, therapeuticmeasures targeting its ligand MAdCAM have alsobeen explored. Anti-MAdCAM therapy improvedTh1-mediated chronic colitis of a CD45RB model,135
and an antisense oligonucleotide capable of inhibitingMAdCAM activity improved Th1-mediated acute colitisinduced by TNBS.136 Preventive and therapeutic effectsof anti-MAdCAM mAbs were also shown inDSS-induced acute colitis.137,138
The therapeutic benefit of targeting the a4 integrin/MAdCAM interaction on colitis/ileitis has been sup-ported by five kinds of animal models, in particular inmodels of CD. Anti-a4-integrin therapy has beenapproved by the FDA for the treatment of moderatelyto severely active CD.1
Anti-Integrin-b7 Therapy
A concern with anti-a4 integrin therapy is the risk ofan unexpected complicationdprogressive multifocalencephalopathy (PML)da serious, often fatal, infectionof the brain caused by reactivation of JC polyomavirus.17,132 This adverse effect is caused by inhibitionof leukocyte recruitment into the CNS through blockageof the a4b1 pathway by anti-a4-integrin therapy.17,132 Inorder to minimize this serious problem, anti-b7-integrintherapy, which blocks the intestine-specific a4b7pathway but not the brain-specific a4b1 pathway, hasbeen under clinical development. A multicenterdouble-blind placebo-controlled trial on 181 patientswith active UC showed that treatment with a mAb(MLN0002) targeting a4b7 heterodimers was effectivefor the induction of clinical and endoscopic remission.139
In addition, a randomized double-blind controlled trialon 185 patients with active CD reported a dose-dependent beneficial effect of MLN0002 (intravenousinfusion of 2 mg/kg Ab at days 1 and 29) on the clinicalremission.140 Of note, worsening of CD was noted as themost common serious adverse effect.140
Administration of an Act-1 mAbdwhich was initiallyreported to recognize CD25 but has subsequently beenidentified to recognize b7 integrin but not CD25dimproved colitis in cotton-top tamarins.141 Adoptivetransfer of b7-integrin-deficient naıve CD4þ T cellswas unable to induce colitis in a severe combinedimmune deficient (SCID) host.142 Similarly, treatmentwith an anti-b7-integrin mAb suppressed the colitisof a CD45RB model.135 Alternatively, this therapy mayhave a preventive, but not therapeutic, effect on thiscolitis.91 Development of ileitis in TNF(ARE) mice wascritically dependent on the integrin b7 pathway.143 Incontrast, the role of b7 integrin in the colitis of IL-2 KOmice did not reach a consensus. One group reportedthat pretreatment with anti-b7-integrin mAb as well as
VI. URINARY TRACT, K
anti-aE-integrin mAb suppressed an antigen (OVA)-induced colitis in IL-2 KO mice.144 In contrast, anothergroup showed that b7-integrin-deficient IL-2 doubleKO mice still developed colitis comparable withthat seen in IL-2 KO mice.142
A novel cell-specific therapy was also tested by tar-geting b7 integrin. An anti-b7-integrin-specific nanopar-ticle approachdwhich was engineered to suppress theproliferation of b7 integrinþ cells through blockage ofcyclin D1dwas shown to improve acute colitis inducedby DSS.145 In addition, the effect of anti-b7-integrintherapy on leukocyte homing to the intestine has beenexplored by several cutting-edge approaches in mouseIBD models. MicroPET imaging of mice with injectionof 64Cu-labeled anti-b7 integrin showed the specificaccumulation of b7 integrinþ cells in the inflamedcolon after challenge with DSS.146 Treatment with anti-b7-integrin mAb improved the colitis of a CD45RBmodel through inhibition of leukocyte homing into thecolon, but this therapy had no effect on experimentalautoimmune encephalomyelitis owing to the lack ofability of this mAb to inhibit leukocyte homing intothe brain.
A potential concern with anti-b7-integrin therapy israised by the observation that some leukocytes were stillable to home into the inflamed colon in a b7-integrin-independent manner.147 Therefore, the therapeutic effectof anti-b7 integrin may be limited as compared to anti-a4-integrin therapy. On the other hand, an attractivepiece of news is that b7-integrin-deficient Treg was stillable to prevent colitis in a CD45RB model, suggestingthat anti-b7-integrin therapy may not affect Treg func-tion, which is well known to contribute to the suppres-sion of colitis.148
The therapeutic potential of anti-b7-integrin therapyin IBD has been supported by four kinds of IBD models,although there is inconsistency in data from IL-2 KOmice. Anti-b7-integrin therapy has been in clinicaldevelopment.17
Anti-Interleukin-12p40 and Anti-Interleukin-23 Therapy
IL-12p40 (p40) is a subunit of the IL-12 family of cyto-kines, which associates with the p35 subunit to form IL-12p70 (IL-12) and with the p19 subunit to form IL-23.IL-12 is a well-known inducer of the Th1 response,and polymorphisms of the IL-23 receptor are negativelyassociated with the development of IBD.3,11,12 A multi-center randomized placebo-controlled double-blindphase II clinical trial in 79 active CD patients reportedthat anti-IL-12p40 therapy (ABT-874/J695, briakinumab)induced a clinical response and remission.149 However,a recent trial with CD patients had a disappointing
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE508
outcome.17,150 Ustekinumab (human IgG1 against p40)has been approved by the FDA for the treatment ofmoderate to severe psoriasis. A double-blind cross-over trial of ustekinumab in 104 patients with moderateto severe CD did not achieve the primary end point.Post-trial analysis, however, found that this therapyinduced a clinical response in patients who had previ-ously received anti-TNF therapy.151
A beneficial effect of anti-p40 mAbs on colitis wasinitially proposed in a Th1-mediated acute colitis ofa TNBS model by Neurath et al.152 and it has sincebeen confirmed in chronic colitis of IL-10 KO mice.153
Anti-p40 therapy was also demonstrated to have bothpreventive and therapeutic effects on colitis ofa CD45RB model.91 Genetically engineered deficiencyof p40 improved the ileitis of TNF(ARE) mice128 andthe colitis of CD3ε transgenic model.154 In contrast, over-expression of p40 in epithelial cells (under the control ofthe T3b promoter) prevented the development of colitisin IL-10 KO mice,155 suggesting a protective role ofectopically expressed p40 in this colitis model.
The ability of p40 to form both IL-12 (p40/p35) and IL-23 (p40/p19) tends to make its function more compli-cated. Indeed, IL-12 and IL-23 may play distinct roles incolitis, depending on the mechanism involved. InTh1-mediated acute colitis of a TNBS model, p35 KOmice lacking IL-12 developed mild inflammation,whereas p40KOmice lacking both IL-12 and IL-23 devel-oped a more exacerbated form of inflammation.156 Simi-larly, TNBS colitis was exacerbated in IL-23 (p19) KOmice.157 These findings suggest a pathogenic role of IL-12p70 and a protective role of IL-23 in TNBS-inducedcolitis. In contrast, a pathogenic role of IL-23 and aprotec-tive role of IL-12 has been shown in the chronic colitis ofIL-10 KO mice.158 IL-12 (p35)-deficient IL-10 double KOmice developed colitis at an earlier age as compared toIL-10 KO mice, while IL-23 (p19)-deficient IL-10 doubleKO mice were still colitis-free at 12 months of age. Inaddition, a pathogenic role of IL-23 and its receptor hasbeen well documented in Th1-mediated chronic colitisof a CD45RB model,159,160 and in innate-immune-mediated acute colitis that can be induced in RAG KOmice by anti-CD40 mAb administration.161 Similarly,both preventive and therapeutic effects of anti-IL-23(p19) mAb were demonstrated in the colitis that wasinduced by a colitogenic bacterial-antigen-specificCD4þ T-cell subset.162 In addition, deficiency of p19dramatically improved the colitis of CD4þ T-cell-specifictransgenic mice of dominant negative TGFbRII.163 Acontribution of IL-23 in the development of intestinalgranulomas (a specific feature of CD) has also beenproposed.164 In Th2-mediated chronic colitis of TCRaKOmice, IL-12 (p35) has been proposed to play a protec-tive role.165 On the other hand, IL-12 may play no role inTh2-mediated acute colitis induced by oxazolone.166
VI. URINARY TRACT, K
Mouse IBD models have suggested differing roles(inflammatory versus protective) of IL-12 (p40/p35)versus IL-23 (p40/p19) in colitis, depending on thefundamental mechanism involved. Anti-IL-12p40 andanti-IL-23 therapies for IBD are currently under clinicaldevelopment.
Anti-Interleukin-17A Therapy
IL-17 is a cytokine that stimulates the recruitment ofneutrophils and monocytes into inflamed areas. In theinflamed colon, IL-17A is produced primarily by a T-cellsubset termed Th17, and by innate lymphoid cells (ILC)that are characterized by the expression of Thy1, stemcell antigen (SCA)1, retinoic-acid-related orphanreceptor (ROR)g, and IL-23R.167,168 Although Th17 Tcells were initially believed to produce IL-17 but notIFN-g, and to differentiate from the same precursor ofTreg, more complicated biology with Th17 has recentlybeen unveiled. CD4þ T cells expressing both IL-17Aand IFN-g were detectable in the inflamed colon of CDpatients,169 and CD4þ T cells expressing both IL-17Aand Foxp3 (a marker of Treg) also appeared in theinflamed colon of IBD patients.170,171 In addition, recentstudies suggest that Th17 T cells are an immediateprecursor of IFN-g-producing Th1 cells.172 These find-ings suggest more complicated functions of IL-17 inIBD. A double-blind placebo-controlled proof-of-concept clinical study in 59 patients with moderate tosevere CD showed anti-IL-17A therapy (secukinumab)exacerbated the disease in a subset of patients.173
Anti-IL-17 mAb together with anti-IL-6 mAb signifi-cantly improved the chronic colitis of IL-10 KOmice.158 IL-17 receptor KO mice were protected fromTNBS-induced acute colitis.174 In response to a colito-genic bacterial antigen, a more potent ability of IL-17-producing effector CD4þ T cells was demonstratedwhen compared to IFN-g-producing effector CD4þ Tcells.175 On the other hand, the role of IL-17 inDSS-induced acute colitis is still controversial. A protec-tive role of IL-17 in DSS colitis was initially suggested bythe exacerbation of colitis after administration of anti-IL-17 mAb.176 In contrast, a beneficial effect of anti-IL-17mAb was shown in the DSS colitis that was induced inCX3CR1 KO mice,177 and resistance of IL-17A KO miceto DSS colitis was also proposed.178 In addition, IL-17may play a more complicated role in the Th1-mediatedchronic colitis of a CD45RB model. Since IL-23dwhichis required for the maintenance of Th17 cellsdcausedthe development of colitis in a CD45RB model, a patho-genic role of IL-17 and Th17 in this colitis was initiallyassumed.179 However, the IL-23-dependent colitis ofthe CD45RB model did not require IL-17 secretion byCD4þ T cells.180 Indeed, adoptive transfer of CD4þ Tcells from IL-17F KO mice or from IL-17A-deficient
IDNEY AND BOWEL

BIOLOGICAL THERAPY AND IBD MODELS 509
and IL-17F-deficient double KO mice still inducedsevere colitis in recipient RAG KO mice.181,182 In addi-tion, a protective role of CD4þ T-cell-derived IL-17Ain this colitis has been demonstrated.183 Deficiency ofIL-17A did not affect the severity of colitis in transgenicmice in which TGF-b signaling was impaired specificallyin CD4þ T cells.163 Similarly, administration of anti-IL-17A mAb did not improve Th2-mediated chronic colitisof TCRa KO mice.165
Therapeutic potential of anti-IL-17 therapy in colitishas been supported by some IBD models, but a criticalconcern has also been raised by other IBD models.Anti-IL-17 therapy is currently under clinical develop-ment but an initial clinical trial has had an unfavorableoutcome.
Anti-Interleukin-6R Therapy
IL-6 activates various cell types carrying themembrane-bound IL-6R/gp130 heterodimer receptors(classical IL-6 signaling) as well as IL-6R� gp130þ cellsvia the soluble IL-6R (IL-6 trans signaling). A pilotrandomized clinical trial on 36 patients with active CDshowed that bi-weekly treatments with a humanizedmAb to the IL-6 receptor normalized the acute phaseresponse and induced clinical, but not endoscopic orhistological, remission in 20% of patients.184
A proinflammatory role of IL-6 in colitis has been welldocumented in several IBD models. Blockage of IL-6trans signaling had a therapeutic effect on theTh1-mediated colitis of a CD45RB model.185 Like theCD45RB model, a single transfer of CD44low CD62Lþnaıve CD8þ T cells from WT mice induced colitis inrecipient RAG2 KO mice. This colitis development wasabolished by the absence of IL-6.186 Anti-IL-6 therapysignificantly improved the chronic colitis of IL-10 KOmice,158 and IL-6 KO mice were resistant to TNBS-induced acute colitis.187 In addition to Th1-mediatedcolitis models, IL-6 was essential for Th2-mediated acutecolitis of an oxazolone model,88 and deficiency of IL-6improved Th2-mediated chronic colitis of TCRa KOmice.114 In contrast, inconsistent findings with thesusceptibility of IL-6 KO mice to DSS-induced acutecolitis have been reported;8 some groups have proposedsusceptibility of IL-6 KOmice to DSS colitis, while othersbelieve IL-6 KO mice are resistant to such treatment.
A concern with anti-IL-6 therapy is raised by theability of IL-6 to serve as a strong activator of signal trans-ducer and activator of transcription 3 (STAT3). Absenceof STAT3 in CD4þ T cells abolished the development ofTh1-mediated colitis in a CD45RB model.188 In contrast,absence of STAT3 in innate immune cells such as macro-phages induced the spontaneous development ofcolitis.189 Similarly, absence of STAT3 in epithelial cellsdelayed the recovery from DSS-induced acute colitis.190
VI. URINARY TRACT, K
Consistent with these findings, gp130 knock-in (KI)mice, which carry a mutated gp130 lacking all STAT3binding sites, spontaneously developed ulceration inthe anorectal region.191 These findings may suggestopposite roles of STAT3 in colitis, depending on the celltypes (e.g., adaptive versus innate) targeted.
A pathogenic role of IL-6 in colitis has been supportedby six kinds of IBD models, but these models have alsosuggested a “double-edged sword” function of STAT3(a downstream event in IL-6 signaling) in colitis. Anti-IL-6 therapy is currently under clinical development.17
Anti-CCR9 Therapy
Interactions of chemokines and their receptors are crit-ical for leukocyte accumulation, including that of Tcells,B cells, eosinophils, and macrophages in the intestinesduring inflammation.192 Among 47 chemokines and 19chemokine receptors, CCL25 (also called Teck) is selec-tively chemotactic for the small, but not the large, intes-tine.193 Ligation of CCR9 by CCL25 results inconformational changes in another intestine-specifichoming receptor pair (integrin a4b7), leading to firmadhesion of a4b7 to its ligand MAdCAM1.193 TheProspective Randomized Oral Therapy Evaluation inCD trial demonstrated the effectiveness of a small mole-cule CCR9 inhibitor (CCX282-B) in maintaining theremission of CD patients over 36 weeks.194
CCL25-deficient TNF(ARE) mice and CCR9-deficientTNF(ARE) mice both developed ileitis, suggesting thatCCL25/CCR9 is dispensable in the ileitis of TNF(ARE)mice.143 On the other hand, pretreatment with a CCR9antagonist (CCX282-B) was reported to suppress thedevelopment of ileitis in TNF(ARE) mice.195 In anotherileitis model of SAMP1/Yit mice, preventive administra-tion (before onset of disease) of neutralizing anti-CCR9or anti-CCL25 mAbs inhibited the development ofileitis, while therapeutic administration of these mAbs(after onset of disease) failed to improve the ileitis.196
Interestingly, a recent report suggested that expressionof CCL25 and CCR9, which is generally undetectablein normal colon, is elicited in the inflamed colon in thecontext of DSS challenge.197 The authors showed thatCCR9 KO mice were more susceptible to DSS-inducedacute colitis than WT control mice, suggesting a protec-tive role of ectopically expressed CCR9 in colitis.
A concern with anti-CCR9 therapy in CD has beenraised by two kinds of ileitis models and an acute colitismodel. CCR9-antagonist therapy in human CD iscurrently under clinical development.
Recombinant Interleukin-10 Therapy
IL-10 is an immune regulatory cytokine that repre-sents a major IBD susceptibility gene.3,11,12
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE510
Polymorphisms within IL-10 receptor genes (IL-10R1and IL-10R2) are also associated positively with thedevelopment of both CD and UC.198 In addition, loss-of-function mutations within the genes of IL-10, IL-10R1, or IL-10R2 are closely associated with early-onset IBD,199 in particular with a very-early-onsetUC.200 Multicenter prospective randomized double-blind placebo-controlled and sequential-escalating-dose trials in 95 patients with Crohn’s disease activityindex (CDAI) scores between 200 and 250 and in 329therapy-refractory patients with CD reported thatsubcutaneous daily administrations of recombinanthuman IL-10 for 28 days did not achieve the primaryend point.201,202
In contrast to the situation in humans, a protective roleof IL-10 in colitis has been reproducibly demonstrated byseparate groups usingmanydifferent kinds of IBDmodels.Genetically engineered deficiency of IL-10 induced thespontaneous development of colitis in mice.203 IL-10served as a protective factor in Th1-mediated acute colitisof a TNBS model.204 Similarly, a protective role of IL-10has been well documented in Th1-mediated chronic colitisof a CD45RB model.205,206 Interestingly, deficiency of IL-10R conferred the ability on Foxp3þ Treg to cause thecolitis of a CD45RBmodel.207 Impaired regulatory functionof Foxp3þ Treg by absence of Wiskott–Aldrich syndromeprotein (WASP) also represented a causative factor ofTh2-mediated chronic colitis in WASP KO mice.208 Th2-mediated chronic colitis of TCRaKOmicewas also exacer-bated by genetic deletion of IL-10.209 In addition, IL-10 KOmice exhibited an increased susceptibility to DSS-inducedacute colitis.210 Mice that are genetically engineered tocarry a point mutation in the P110d gene locus spontane-ously developed focal inflammation restricted to therectum and cecum,211 and this colitis was exacerbated byabsence of IL-10.212 Similarly, deficiency of IL-10 exacer-bated the colitis developing in toll-like receptor (TLR5)KO mice213 and in mucin (Muc2) KO mice.214
Although many IBD models have reacheda consensus regarding the protective role of IL-10 incolitis, clinical trials of subcutaneous recombinant IL-10 injections in CD had a disappointing outcome. Thereare several possibilities to explain these distinctoutcomes between mice and humans.17 The first possi-bility is that the biological function of IL-10 differsbetween mice and humans. However, this possibilitymay be unlikely because in vitro systems using humanand mouse materials generally tend to exhibit similarpatterns of immune responses. A second possibility isan impaired response of IBD patients to IL-10 due topolymorphisms within IL-10 receptors. Since a recentstudy showed that the majority of IBD patients can nor-mally respond to IL-10,215 this possibility may berestricted to a subset of IBD patients. On the otherhand, very attractive observations with a hope for future
VI. URINARY TRACT, K
IBD therapy have recently been reported. Allogeneictransplantation of hematopoietic stem cells with intactIL-10 and IL-10R genes improved CD in a patientcarrying a mutation within the IL-10R gene.198 In addi-tion, among 66 patients with early-onset IBD (< 5 yearsof age), 16 patients carried loss-of-function mutationswithin the IL-10 or IL-10R genes; 3 patients had an IL-10 mutation, 5 patients an IL-10R1 mutation, and8 patients an IL-10R2 mutation.199 Among them,5 patients were subjected to allogeneic hematopoieticstem cell transplantation carrying intact IL-10 signaling.Of note, sustained clinical remission (so far, for 2 years)was seen in all of these 5 patients.199 A third possibility isthat the therapeutic efficacy of recombinant IL-10ddelivered by subcutaneous injectiondis limited byits poor bioavailability to intestinal tissues.17 This possi-bility is supported by the short half-life and instability ofrecombinant cytokines as compared to antibodies thathave been successfully used for IBD therapy. Forexample, recombinant IL-4dwhich was subcutaneouslyinjected or continuously delivered to the subcutaneousspace through an osmotic pumpddid not alter theimmune response in the colon. The problem was over-come when IL-4 was continuously delivered into theperitoneal cavity through an osmotic pump.216 In orderto clarify this possibility, delivery of IL-10 into the intes-tinal lumen through Lactococcus lactis genetically engi-neered to produce human recombinant IL-10 wasconfirmed in a phase I trial to be safe, but the efficacyhas not been reported.217
Stem Cell Therapy
Stem cell therapy is an emerging and promising area ofresearch that has potential to open a new avenue for IBDtherapy. Mesenchymal stromal/stem cells (MSCs) arenon-hematopoietic stromal cells exhibiting multi-lineagedifferentiation capacity and ability to mediate immuno-suppressive and anti-inflammatory effects.218 A phase Iclinical trial of MSC therapy has been conducted in ninepatients with refractory CD. After infusion of ex vivoexpanded autologous bone marrow (BM)-derived MSCs,three patients exhibited an improved clinical response(CDAI decrease > 70) without reaching remission, andanother three patients required surgery owing to diseaseworsening.219
The therapeutic potential of systemic infusion withnot only syngeneic but also allogeneic adipose-derivedmesenchymal stem cells (ASCs) was shown in Th2--mediated acute colitis that was induced in BALB/cmice by TNBS.220 The therapeutic effect may be medi-ated by several mechanisms, including downregulationof the Th1 response, upregulation of IL-10 expression,and induction of Treg expansion through interactionwith macrophages.220 In addition, infusion of human
IDNEY AND BOWEL

BIOLOGICAL THERAPY AND IBD MODELS 511
umbilical-cord-derived MSCs was reported to improvea Th2-mediated acute colitis that was induced inBALB/c mice by TNBS.221 In Th1-mediated acute colitisthat was induced in C57BL/6 mice by TNBS, infusion ofBM-derived MSCs before TNBS challenge had a preven-tive effect.222 Removal of splenic CD11bþ cells resultedin the loss of the beneficial effect of MSC therapy onthis colitis, suggesting that interactions between MSCsand CD11bþ cells may be necessary to fully elicit thebeneficial effect of MSCs.222
A dose-dependent therapeutic effect of human ASCinfusion was proposed in acute colitis that was inducedinmice byDSS.223 In contrast, ASCdidnot have apreven-tive effect on this colitis when ASC infusion was per-formed before challenge with DSS, suggestinga transient effect of ASC therapy. A transient effect isalso supported by a study using a near-infrared in vivoimaging system. MSCs accumulated in the inflamedcolon rapidly after the infusion, but they disappearedfrom all tissues (colon, lung, spleen, and lymphnodes) within 3 days after infusion.222 Interestingly,MSCs that were coated with anti-VCAM-1 mAb throughpalmitated protein G (PPG) showed a more enhancedability to home into the inflamed colon of aDSSmodel.224
Repeated injections of BM-derivedMSCs (days 0, 2, and 4after DSS challenge)were proposed to allow the accumu-lation of MSCs in the inflamed colon and have a thera-peutic effect on DSS-induced acute colitis in rats.225
Busulphan-induced hypoplasia of bone marrow exacer-bated DSS-induced acute colitis, and MSC transplanta-tion ameliorated the disease exacerbation.226 Theauthors proposed that this beneficial effect may bemedi-ated by restoration of epithelial barrier integrity, but notfrom immune response. The ability of MSC therapy toenhance healing of wounds from DSS-induced acutecolitis in rats was also proposed.227 In contrast, a recentstudy suggested no significant effect of MSCs on theprevention of DSS-induced or TNBS-induced acutecolitis.228 The authors proposed that pretreatment ofMSCs with IFN-g is required to elicit their immunesuppressive ability to effectively prevent these forms ofcolitis. A clinically useful observation has also beenmadedMSC phenotype and function were not alteredby drugs that have been used for IBD therapy, includingazathioprine, methotrexate, 5-ASA, and anti-TNFmAb.229
In addition to MSCs, a novel method has recentlybeen established to allow a long-term expansionof leucine-rich-repeat-containing G-protein-coupledreceptor (Lgr)-5-expressing colonic epithelial stemcells.230 The authors demonstrated that intrarectal injec-tion of ex vivo-generated epithelial stem cells was able tocover the colonic ulcerations in a DSS model.
The therapeutic effect ofMSCs on colitis has been sup-ported only by acute colitis models, and there are some
VI. URINARY TRACT, K
inconsistencies in the data published. An initial pilotstudy in human IBD showed an unfavorable outcome,suggesting the existence of many steps to be overcometo successfully apply stem cells to IBD therapy.
Anti-CTLA4 Therapy
Cytotoxic T-lymphocyte-associated molecule 4(CTLA4) is a co-stimulatory molecule that interactswith CD80 and CD86. Anti-CTLA4 antibody (ipilimu-mab) was approved in 2011 by the FDA for treatmentof stage IV melanoma. Development of colitis has beendocumented as one of the serious adverse effects ofanti-CTLA4 therapy.231,232 Abatacept is a geneticallyengineered fusion protein that chimerizes CTLA4 tothe Fc portion of IgG to block the co-stimulatorysignaling. Four placebo-controlled trials in 451 CDpatients and 490 UC patients showed that abatacept isnot efficacious for the treatment of moderate to severeCD or UC.9,233
Constitutive expression of CTLA4 among CD4þTcells is restricted primarily to Treg cells.234 The protec-tive role of CTLA4 in colitis has beenwell explored usingTh1-mediatedcolitis of aCD45RBmodel, andaconsistentoutcome has been reported separately by independentgroups. CTLA4-deficient Treg failed to suppress colitisin a CD45RB model,235 and also in Helicobacter-inducedinnate colitis.236 In addition, administration of anti-CTLA4 mAbs exacerbated the colitis in a CD45RBmodel,237–239 and treatment with a CTLA4 agonist sup-pressed this colitis.240 In contrast, anti-CTLA4 therapysuppressed Th1-mediated acute colitis of a TNBS modelby inducing IL-10-producing inducible T-cell co-stimulator (ICOSþ) regulatory Tcells.241
Different effects of CTLA4 on colitis have beenproposed in CD45RB versus TNBS models. In humans,anti-CTLA4 therapy induced the development of colitisin a subset of patients.
Anti-CD3 Therapy
CD3 is a surface molecule expressed by T-cell popula-tions, including CD4þ T cells, CD8þ T cells, TCRgdT cells, and NKT cells. A randomized double-blindplacebo-controlled clinical trial on 127 corticosteroid-refractoryUCpatients showed that anti-CD3 therapy (vis-ilizumab) was not effective and was associated withincreased cardiac and vascular adverse effects.242Anotherphase I clinical trialwithanti-CD3 therapy (NI-0401) failedto improve moderate to severe CD.243
A requirement for CD4þ T cells for the induction ofcolitis has been well documented using CD4þ T-cell-transfer systems. For example, development ofTh1-mediated colitis in a CD45RB model was inducedby adoptive transfer of CD4þ CD45RBhigh naıve CD4þ
IDNEY AND BOWEL

Treg
CD4+ T cells
TTreegggggFoxp3
Th2
Tfh
Tr1
Th9
Th3
IFN-γIL-10
IL-9
IL-4
?Th17/Treg
TTre
1IL-10
T
reggg
1
Th17Th22
Th1
?Th1/Tr1
IL-17
IL-17
IL-22IL-22
IFN-γIL-10
TGF-β
IL-21
?Th17/Th1
1 ?Tfh/Th1
IL-10
IL-4
Foxp3
IFN-γIL-21
IFN-γIL-17
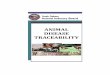
FIGURE 22.2 There are functionally different CD4D T-cell
subsets, depending on their cytokine profiles. Some subsets maydifferentiate from other subsets as indicated by the blue lines. UniqueCD4þ T-cell subsets have been identified to specifically appear in theinflamed intestine, including Foxp3þ IL-17þ CD4þ (CD4þ T cellssharing Treg and Th17 phenotype), IL-17þ IFN-gþ CD4þ (CD4þ Tcells sharing Th17 and Th1 phenotype), and IFN-gþ IL-21þ CD4þ(CD4þ T cells sharing Th1 and Tfh phenotype) T-cell subsets.
22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE512
T cells from WT mice.244 Adoptive transfer of CD4þT cells from WASP KO mice induced Th2-mediatedcolitis in immunodeficient hosts,245 and flagellin-specific CD4þ T cells also had the ability to induce thedevelopment of colitis.246
Genetic deletion of some T-cell subsets has been repro-ducibly demonstrated to abolish the development ofcolitis and ileitis in many IBD models. Absence ofCD4þ T cells failed to elicit the development of chroniccolitis in IL-10 KO mice.247 Colitis development in IL-2KO mice was abolished by genetic deletion of CD4þTCRabþ T cells, but not of CD8þ TCRabþ T cells orTCRgdþ T cells.248,249 Deficiency of CD4þ T cells due toabsence of major histocompatibility complex (MHC)class II abolished the development of Th2-mediatedchronic colitis of TCRaKOmice.49 In addition, deficiencyof CD8þ T cells improved the ileitis of TNF(ARE)mice.128 Furthermore, deficiency of TCRgd T cells im-proved the colitis in phosphoinositide-dependent kinase(PDK1) KO mice.250 Interestingly, mice that were geneti-cally engineered to develop aberrant type II NKT cellsspontaneously developed colitis.22 Genetic modificationof T-cell functions also caused colitis and ileitis. CD4þT-cell-specific overexpression of dominant negativeTGF-b receptor type II led to spontaneous developmentof multi-organ inflammation, including colitis.251 T-cell-specific depletion of Blimp-1 induced the spontaneousdevelopment of colitis.252 Ectopic overexpression ofTNFSF15 in Tcells also caused the spontaneous develop-ment of transmural inflammation in the small, but notlarge, intestine.253
The data from adoptive T-cell transfer and geneticallyengineered mouse models of IBD clearly indicate thatsomeT-cell subsets arenecessary for the inductionof colitisand ileitis.However, these IBDmodels have also identifiedfunctionally different T-cell subsets. For example, theCD4þ T-cell population can be classified into at least 13different subsets, primarily depending on the profile ofcytokines, which play an inflammatory versus protectiverole in colitis/ileitis (Fig. 22.2). Therefore, a critical concernmay be raised when all T cells are depleted by anti-CD3therapy. Among the CD4þ T-cell population, CD25þFoxp3þ Treg, IL-10-producing Tr1, and TGF-b-producingTh3 subsets have been well confirmed to possess a strongability to suppress colitis and ileitis in many IBDmodels.5,254 Regulatory Treg and effector Th17 T-cellsubsets differentiate reciprocally from the same precursorcells, depending upon the cytokine environment. Interest-ingly, several unique CD4þ T-cell subsets have beendemonstrated to develop specifically in the inflamedmucosa of IBD patients. A CD4þ T-cell subset sharingboth Th1 (IFN-g production) and Th17 (IL-17A produc-tion) functions appeared in the inflamed colon of CDpatients.169 Another CD4þ T-cell subset expressing bothIL-17A and Foxp3 also appeared in the inflamed colon of
VI. URINARY TRACT, K
IBD patients.170,171 This CD4þ T-cell subset, although itproduced IL-17A, had immune suppressive abilityin vitro.170 T-follicular-helper CD4þ T cells (termedTfh)dwhich produce IL-21 and IL-4dstimulate B cells ingerminal centers to produce antibodies. Interestingly, theTfh subset was proposed to expand in the inflamedmucosa particularly in CD patients and acquire the abilityto produce IFN-g.255 A novel CD4þ T-cell subset (termedTh9)dwhich produces both regulatory cytokine IL-10and effector cytokine IL-9dwas shown to cause colitis ina CD45RB model.256 In addition to CD4þ T cells, someCD8þ T cells also possess suppressive ability in colitis.CD8þ T-cell subsetsdwhich are characterized by expres-sionofCD11cor by lowexpressionofCD28dhada regula-tory ability to suppress colitis in a CD45RBmodel.257,258 Inaddition, an intraepithelial lymphocyte (IEL) subsetdwhich expressed CD8aa homodimer (not CD8ab hetero-dimer)andalsoCD4dwasproposed to suppress the colitisof a CD45RB model through production of IL-10.259
Furthermore, an NKT-cell subset expressing TCR variableregion a14 may have contributed to the improvement ofacute colitis induced by DSS.260
A requirement for some T-cell subsets for the induc-tion of colitis/ileitis has been well demonstrated in
IDNEY AND BOWEL

BIOLOGICAL THERAPY AND IBD MODELS 513
many IBD models, while they have also identified theexistence of different T-cell subsets, some of whichcontribute to the suppression of colitis/ileitis. Clinicaltrials of anti-CD3 therapy capable of depleting allT-cell subsets had an unfavorable outcome.
Anti-CD25 Therapy
IL-2 is recognized by a heterotrimeric receptorcomposed of IL-2Ra (CD25), IL-2Rb (CD122), andcommon g chain (CD132). CD25 is a potentialCD-susceptibility gene, and the IL-2 gene is locatedwithinan IBD-susceptibility locus.3,11,12Ananti-CD25mAb (basi-liximab) has been approved since 1998 by the FDA forprevention of acute rejection after organ transplantation.Some initial uncontrolled pilot studies demonstrated thepotential effectiveness of anti-CD25 therapy (daclizumab)in fulminatingUC.261However, a subsequent randomizeddouble-blind placebo-controlled dose-ranging trial in 159patients with moderately active UC showed that anti-CD25 therapy rather decreased the remission andresponse, with increased adverse events including naso-pharyngitis and pyrexia.262 Since the ability of IL-2(together with IL-4) to render lymphocytes steroid-resistant has been reported,263 a randomized placebo-controlled trial was also performed on patients withsteroid-refractory UC. However, in the trial, on 149patients with moderate to severe UC despite treatmentfor at least 14 days with oral prednisone, anti-CD25therapy did not increase the effect of steroid on the induc-tion of remission.264
A protective role of IL-2 in IBD has been highlighted bythe spontaneous development of colitis in IL-2KOmice265
and CD25 KOmice.266 A regulatory role of CD25 in colitishas also been supported by the constitutive expression ofCD25 on Treg capable of suppressing colitis and by therequirement of IL-2 for maintaining the regulatory func-tion of Treg.267 Although CD25 can be transientlyexpressed on effector T cells, inherent and continuousexpression of CD25 is seen on the Treg.268 On the otherhand, the therapeutic effect of anti-CD25 mAbs on colitishas been largely unexplored in IBD models. Only onestudy proposed that anti-CD25 therapy had no effect onTh1-mediated acute colitis of a TNBS model.269
A protective role of CD25 in colitis has been sup-ported by the spontaneous development of colitis inCD25-deficient mice, but the effectiveness of anti-CD25therapy has been largely unexplored in IBD models.Clinical trials on active UC had an unfavorable outcome.
Anti-Interferon-Gamma Therapy
CD is generally characterized by an enhanced IFN-g-producing Th1 response, while UC tends to exhibit anenhanced Th2 (e.g., IL-5) response.10 A dose-escalating
VI. URINARY TRACT, K
placebo-controlled double-blind, single- and multiple-dose safety and tolerability clinical trial of anti-IFN-gtherapy (fontolizumab) in 133 patients with CDAI scoresbetween 250 and 450 showed no statistically significantdifference in theprimaryendpointsbetween fontolizumaband placebo groups.270 However, patients receiving twodosesof fontolizumabexhibited adoubling in the responserate at day 56. A recent randomized double-blind placebo-controlled multiple-dose phase II clinical trial in 201patients with CDAI scores between 250 and 450 showedthat fontolizumab, although reducing C-reactive proteinlevels, induced no strong clinical response.271
A series of studies has indicated that development ofcolitis in CD45RB models depends on the Th1 responseassociated with IFN-g production.244 Development ofcolitis in B7.2 Ig Fc transgenic mice was abolishedwhen they were crossed with IFN-gKOmice.272 In addi-tion, deficiency of IFN-g improved the ileitis inTNF(ARE) mice.128 Similarly, CD4þ T cells producingIFN-g were responsible for the development of ileitisin SAMP1/Yit mice.273 Interestingly, deficiency of IFN-g improved a Th2-mediated acute colitis of an oxazolonemodel.274 Taken together, these mouse models supportthe inflammatory role of IFN-g in IBD.
Colitis of IL-10 KOmice has generally been referred toas“Th1-mediated” colitis.However, IFN-gmayplaymorea complicated role in this colitis model. Anti-IFN-gadministration improved Helicobacter hepaticus-inducedcolitis in IL-10 KO mice.275 In contrast, IFN-g may playno role, or a protective role, in the inherent colitis of IL-10 KO mice. The lack of a role of IFN-g in sustaining thecolitis of IL-10 KO mice was initially proposed in 1998by Rennick and colleagues.153 In addition, IFN-g-deficientand IL-10-deficient double KO mice developed a moreexacerbated form of colitis as compared to IL-10 KOmice.276 Similarly, the lack of an obvious role of IFN-g incolitis has been found in some IBD models. Absence ofIFN-g still induced the development of severe colitis ina CD3ε transgenic mouse model.154 WT mice and IFN-g-receptor KO mice exhibited a comparable susceptibilityto TNBS colitis,156 and administration of anti-IFN-gmAbs also had no effect on this colitis.277 Deficiency ofIFN-g did not affect the severity of Th2-mediated chroniccolitis of TCRa KOmice.216
Some IBDmodels have supported a proinflammatoryrole of IFN-g in colitis/ileitis, but other IBDmodels havefound no role, or a protective role, of IFN-g in colitis.Clinical trials of anti-IFN-g therapy did not achieve theprimary end point.
Recombinant GM-CSF Therapy
Granulocyte macrophage colony-stimulating factor(GM-CSF) is a hematopoietic growth factor that contrib-utes in promoting myeloid cell development,
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE514
maturation, and survival. The therapeutic potential ofrecombinant GM-CSF (sargramostim) has been testedin CD patients in several human trials.17,278 Initial find-ings from a small number of patients suggested a benefi-cial effect of GM-CSF therapy on moderate to severeCD,279 but a subsequent randomized double-blindplacebo-controlled trial in 129 patients with moderateto severe CD did not achieve the primary end point.280
Interestingly, a recent study found that expression ofCD116 (receptor of GM-CSF) on granulocytes andmono-cytes was decreased in the context of intestinal inflam-mation, and that the reduced expression was moreprominent in UC,281 raising the possibility that the lowlevel of CD116 expression makes GM-CSF therapyinsufficient.
In a preclinical setting, the therapeutic effect ofGM-CSF on colitis has only been assessed using aDSS-induced acute colitis model. Daily administrationof pegylated GM-CSF promoted wound healing inDSS-induced acute colitis, presumably by enhancingBM-derived CD11cþ myeloid cells.282 An improvementof DSS-induced colitis by GM-CSF treatment was alsoseen in RAG1 KO mice, lacking both T and B cells, sug-gesting that the therapeutic effect is independent of theadaptive immune response.283 A specific plasmacytoidDC subset expressing 440c (a sialic-acid-binding Ig-likelectin) was shown to mediate the improvement of thiscolitis. In addition, GM-CSF KO mice developeda more exacerbated form of colitis after challenge withDSS as compared to WT mice.284
A beneficial effect of GM-CSF therapy on IBD hasonly been supported using a DSS-induced acute colitismodel, and clinical trials have had an unfavorableoutcome.
Recombinant Interleukin 11 Therapy
IL-11 is a thrombopoietic growth factor that stimu-lates the proliferation of megakaryocyte progenitors.Recombinant IL-11 has been used to restore the numberof platelets in patients after certain kinds of chemo-therapy. A randomized double-blind controlled trial in51 patients with CD showed that subcutaneous injec-tions (once weekly for 12 weeks) of recombinant IL-11were significantly inferior when compared to predniso-lone therapy for the induction of remission in activeCD.285
Subcutaneous injection of recombinant IL-11 hasbeen shown to improve inflammation in the jejunumand colon of a rat UCmodel (humanHLA-B27 transgenicrats), suggesting an anti-inflammatory effect of IL-11on colitis.286,287 A preventive and therapeutic effect ofrecombinant IL-11 on acute colitis was also shown usinga TNBS colitis model in rats.288,289 The preventive effectmay have a contribution from amassive release of mucus
VI. URINARY TRACT, K
fromgoblet cells.288 Interestingly, the colonwith improvedinflammation still exhibited high levels of arachidonicacid derivatives, such as PGE2 and LTB4.289
A therapeutic effect of recombinant IL-11 has beensupported only by rat models of IBD, and clinical trialson CD have had an unfavorable outcome.
Recombinant Keratinocyte Growth FactorTherapy
Keratinocyte growth factor 1 (KGF1, also known asFGF7) and KGF2 (FGF10)dwhich belong to the familyof fibroblast growth factors (FGFs)dinteract with oneof the FGF receptors expressed particularly by epithelialcells, and may serve as a protective factor for epithelialtissues. A randomized double-blind placebo-controlleddose-escalation (1–50 mg/kg) clinical trial of intravenousinjection of a truncated recombinant KGF2 in 88 patientswith active UC showed no evidence of therapeuticeffectiveness.290
A preventive and therapeutic effect of recombinantKGF2 was shown in acute colitis induced byDSS,291–293 and KGF2 therapy also enhanced thewound healing in this acute colitis.293 In addition, KGFKO mice were more susceptible to DSS-induced acutecolitis, and recovery from this colitis was impaired inKGF KO mice.294 TCRgd T cells, which located in closeproximity to the area of intestinal damage, primarilyproduced the KGF.
The therapeutic potential of KGF2 in IBD has onlybeen supported by an acute colitis model, and clinicaltrials on UC patients have had an unfavorable outcome.
Anti-CD20 Therapy
IBD, and particularly UC, are characterized byincreased production of autoantibodies such as anti-neutrophil cytoplasmic antigens with a perinuclearstaining pattern (pANCA) and anti-tropomyosin, bothof which are produced in response to entericmicrobes.295 B-cell-depletion therapy through rituximab(a chimeric monoclonal antibody against CD20) hasbeen approved since 1997 by the FDA for the treatmentof non-Hodgkin’s B-cell lymphoma, and has also beensuccessfully applied for the treatment of some autoim-mune diseases. A double-blind randomized controlledtrial in 24 patients with steroid-resistant moderatelyactive UC showed no significant effect of rituximab ininducing remission,296 although no severe adverseeffects were reported. A case report showed an improve-ment of colitis associated with active systemiclupus erythematosus after rituximab therapy.297 Incontrast, an exacerbation of UC with decreased IL-10production after rituximab therapy has been
IDNEY AND BOWEL

BIOLOGICAL THERAPY AND IBD MODELS 515
reported.298 Among ten patients with Graves’ diseasewho were treated with rituximab, one patient rapidlydeveloped UC by 68 days after treatment and anotheracquired a low-grade colonic inflammation.299 A pedi-atric patient with nephritic syndrome developed severeUC at 42 days after treatment with rituximab.300 Rituxi-mab treatment also induced the development of UC ina rheumatoid arthritis patient within 10 weeks aftertreatment.301 Interestingly, a patient with bullous lupusdeveloped appendicitis and then UC-like colitis after rit-uximab therapy.302
Since the specific function of B cells is the productionof immunoglobulin (including autoantibodies), themajor function of B cells has generally been believed tobe mediated by the immunoglobulin. However, it isbecoming increasingly apparent that B cells havea much broader spectrum of immune functions; theycan produce a broad array of cytokines, including the re-gulatory cytokine IL-10, and can serve as a second lineof antigen-presenting cells to induce the expansionof Treg.303,304 Therefore, functions of B cells may bemuch more complicated than previously and evencurrently predicted. Indeed, a growing body of evidencefrom IBD models has unveiled different roles (protec-tive, inflammatory, or no role) of B cells, dependingupon several factors such as the fundamental mecha-nism and the location of inflammation.
Autoantibodies were initially thought to cause theTh2-mediated colitis in TCRa KO mice because of theclose correlation between colitis severity and productionof autoantibodies.305 However, subsequent studiesfound that deficiency of B cells resulted in the exacerba-tion of colitis in TCRa KO mice, suggesting a protectiverole of B cells in this colitis model.306 Three major mech-anisms for the B-cell-mediated protective function havebeen proposed. One mechanism depends on immuno-globulin that may enhance the clearance of apoptoticepithelial cells to prevent the consequent activation ofeffector CD4þ T cells.306 This possibility may be sup-ported by a finding that intake of infected orTLR-ligand-carrying apoptotic epithelial cells by macro-phages stimulated the effector immune response.307 Asecond mechanism is operated by an inducible regula-tory B-cell population (called “Breg”) that appears inthe mesenteric lymph nodes (MLN) only in the contextof inflammation and improves the ongoing colitisthrough production of IL-10.209,304 A third mechanismmay be mediated by another inducible B-cell population(called “B12”) that appears in the inflamed colon,produces IL-12 but not IL-10 in response to bacterialDNA CpG, and consequently improves Th2-mediatedchronic colitis of TCRa KO mice.165,308
Deletion of B cells by a single administration of anti-CD20 mAb induced the rapid development of colitiswithin 15 days in young IL-10 KO mice at 6 weeks of
VI. URINARY TRACT, K
age.309 B cells in this colitismodelmay control the homeo-stasis of Treg tomaintain the immune tolerance.Aprotec-tive role of B cells in Th1-mediated chronic colitis ofa CD45RBmodel has been demonstrated,310 and a recentstudy also found a protective ability of B cells carryingagalactosyl IgG in this colitis model.311 B10 is anotherregulatory B-cell subset that expands initially in thespleen, expresses CD5 and high levels of CD1d, andproduces large amounts of IL-10.312 B10 cells that werestimulated with enterobacterial extract were shown tosuppress Th1-mediated chronic colitis of a CD45RBmodel.313 In another colitis model, Gai2 KOmice, B cellscontributed to the suppression of colitis by facilitatingexpansion of CD4þ CD8aþ intraepithelial T cells andCD3þ CD4� NKT cells with immune regulatoryability.314 MHC-class-I-mediated antigen presentationwas required for this B-cell-mediated induction of a regu-latory CD8þ T-cell subset capable of controlling colitisthrough production of perforin.315 CD4þ T-cell-specificoverexpression (under control of the CD4 promoter) ofdominant negative TGF-b receptor type II led to sponta-neous development of multi-organ inflammation,including colitis. B cells played a protective role in thiscolitis as indicated by the exacerbation of colitis afterdepletion of B cells by anti-CD20 administration.316
NFATc2 KO mice did not develop colitis, but doubleKO mice deficient in both NFATc2 and RAG2 (lacking Tand B cells) spontaneously developed colitis. Adoptivetransfer of B cells, but not Tcells, fromWTmice improvedthis colitis in an IL-10-independent manner.317 Thesemouse IBD models support the protective role of B cellsin colitis.
The role of B cells per seversus bacterial-specific IgG inDSS-induced acute colitis may vary. Deficiency of CD19(B cells) made mice more susceptible to DSS-inducedacute colitis, and this exacerbation was improved byadoptive transfer of regulatory B10 B cells.312 Similarly,CD19-specific deletion of MyD88 rendered mice highlysusceptible to DSS-induced acute colitis.318 In contrast,a subset of IgG contributed to the exacerbation of thisacute colitis. Administration of IgG specific for a colito-genic bacterial antigen (flagellin) exacerbatedDSS-induced colitis by enhancing FcRn-dependentantigen presentation.319 IgE was also proposed to serveas a causative factor in Th2-mediated acute colitisinduced by oxazolone.320
An inflammatory or dispensable role of B cells hasbeen demonstrated in some IBD models, particularlyin ileitis and systemic inflammatory models. B cellswere required for the exacerbation of ileitis in SAMP/YitFc mice by cooperating with colitogenic CD4þT cells,321 and expression of b7 integrin on B cells wasindispensable for eliciting their inflammatory ability.322
Interestingly, development of IL-10-producing regula-tory B cells was impaired in the SAMP1/Yit mice,
IDNEY AND BOWEL

TABLE 22.1 Effects of Therapeutic Agents on Mouse IBD Models
CD models UC models
Colitis Ileitis Colitis Colitis
Acute Chronic Chronic Acute Chronic Acute
Therapy TNBS CD45 IL10 SAMP TNF OXA TCR
DSS Injury
model
Other
models Mouse model score
Hygiene hypothesis SUP SUP X SUP 4 In clinical development
Cigarette smoking SUP SUP SUP SUP SUP 32 Suppressive effect onUC but not CD
Steroid SUP SUP SUP SUP SUP SUP ? 62 Conventional therapyfor IBD
Cyclosporine SUP X X SUP SUP 2 Effective in severe UC,not CD, patients
Tacrolimus SUP X ? SUP SUP(2) 8 Effective in steroid-refractory UC
NSAID* WOR WOR WOR WOR �81 Alert in the use for IBD
5-ASA SUP SUP SUP SUP 16 Effective in IBD
Anti-TNFa SUP SUP SUP SUP SUP WOR SUP WOR SUP(1) 55 Approved by FDA forIBD therapy
Anti-a4 SUP SUP SUP SUP SUP(1) 32 Approved by FDA forCD therapy
Anti-IL-6R SUP SUP SUP SUP SUP WOR SUP(1)WOR(2)
37 In clinical development
Anti-IL23 WOR SUP SUP SUP(2) 13 In clinical development
Anti-b7 ? SUP SUP SUP(1) 9 In clinical development
Mesenchymal stemcellsy
SUP SUP 4 In clinical development
Anti-IL12p40 SUP SUP WOR SUP X WOR SUP(1) 1 In clinical development
VI.
URIN
ARYTRACT,KID
NEYAND
BOW
EL
22.ANIM
ALMODELSOFIN
FLAMMATORYBOWELDISEASE
516

Anti-IL17A SUP ? SUP X ? SUP(1) 0 In clinical development
Anti-CCR9z X ? WOR �4 In clinical development
Anti-CD20* WOR WOR SUP X SUP WOR WOR SUP(2)WOR(3)
�56 In clinical development
rIL-10 SUP SUP SUP SUP SUP SUP(3) 128 No longer in clinicaldevelopment
Anti-IFNg X SUP WOR SUP SUP SUP X SUP SUP(1)X(1)
5 No longer in clinicaldevelopment
rIL-11y SUP(2) 4 No longer in clinicaldevelopment
rGM-CSFy SUP 2 No longer in clinicaldevelopment
rKGFy SUP 2 No longer in clinicaldevelopment
Anti-CD3 ? ? ? ? ? ? 0 No longer in clinicaldevelopment
Anti-CD25y X ? WOR(1) �3 No longer in clinicaldevelopment
Anti-CTLA4* SUP WOR WOR(2) �25 No longer in clinicaldevelopment
* Alert pattern,y insufficient pattern,z unfavorable pattern.The models include TNBS (TNBS), CD45RB (CD45), IL-10 KO (IL10), SAMP/Yit (SAMP), TNF(ARE) (TNF), oxazolone (OXA), TCRa KO (TCR), and DSS (DSS). Data from other IBDmodels are listed in the column
“Other models.” SUP, suppressive effect was observed; WOR, inflammation was worsened; X, no effect was seen; ?, data did not reach a consensus. Numbers in parentheses are the number of mouse models in
other IBD models that exhibited suppressive or exacerbating effect. Score: probability index of likelihood of success of the therapy in mice.
The clinical status is based on review articles.1,17
VI.
URIN
ARYTRACT,KID
NEYAND
BOW
EL
BIO
LOGIC
ALTHERAPYAND
IBD
MODELS
517

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE518
suggesting that the pathogenic function of B cells in thismodel may be promoted by the absence of regulatory Bcells.323 B cells were also proposed to participate in theinduction of small intestinal inflammation characterizedby villus atrophy.324 In addition, induced ectopic overex-pression of gp39 on B cells caused the development ofcolitis and ileitis.325 On the other hand, absence of B cellsdid not affect the severity of ileitis in TNF(ARE) mice.128
IL-2 KO mice spontaneously develop a systemicautoimmune disease including colitis,265 and a compa-rable severity of colitis was seen when IL-2 KO micewere crossed with B-cell-deficient mice, suggesting norole of B cells in this colitis.248
A functional difference between large and smallintestinal B cells is suggested by a recent meta-analysisof more than one million mouse IgA repertoires. ManyIgA variable region of heavy chains (VH) sequencesabundantly present in the small intestine were infre-quent or undetectable in the colon.326 Interestingly, themajority of “colitis” models, except the oxazolonemodel, suggest a protective role of B cells, whereas themajority of “ileitis” models propose an inflammatoryrole for B cells. These results, if true, suggest thatB-cell depletion may be a more favorable therapy forCD (ileitis) rather than UC (colitis). However, a casereport showed ineffectiveness of rituximab therapy ina patient with CD.327
Coexistence of inflammatory and regulatory B-cellpopulations in IBD has been confirmed in IBD models.B-cell-depletion therapy for UC is currently under clin-ical development, but an alert has been raised by fivecase reports.
CONCLUSION
Although mouse models of IBD cannot fully reflectthe pathogenesis of human IBD, they may be used tohelp the preclinical evaluation of some candidate thera-pies. There are recognizable patterns when comparingthe findings from IBD models to the outcome fromsome clinical trials (Table 22.1). An “alert” pattern ariseswhen a majority of IBD models raise concern on theexacerbation of disease by therapy. An “unfavorable”pattern is expressed when many (but not just one ortwo) IBD models fail to support therapeutic benefits.An “insufficient” pattern is raised when the potentialtherapeutic effect has been evaluated based on onlyone or two IBD models. Clinical trials targeting mole-cules categorized into these three patterns may showa tendency to have an unfavorable outcome. As seenin anti-TNF-a and steroid therapies, a consensus froma majority of IBD models, including “chronic” colitis/ileitis models, may be necessary to provide a sufficientrationale for the consideration of future clinical trials.
VI. URINARY TRACT, K
Further accumulation of data from both IBD modelsand clinical trials may help generate a platform forcomputational analysis to determine the likelihood ofsuccess of future therapies in IBD and to developpersonalized therapy depending on the genetic patternof IBD-susceptibility genes and environmental factors.
Acknowledgments
The authors would like to thank Emiko Mizoguchi and HirotsuguImaeda for helpful advice and Cindy W. Lau for nice editorialassistance.
References
1. Talley NJ, Abreu MT, Achkar JP, Bernstein CN, Dubinsky MC,Hanauer SB, et al. An evidence-based systematic review onmedical therapies for inflammatory bowel disease. Am J Gas-
troenterol 2011;106:S2–25.2. Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M,
Chernoff G, et al. Increasing incidence and prevalence of theinflammatory bowel diseases with time, based on systematicreview. Gastroenterology 2012;142:46–54.
3. Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med
2009;361:2066–78.4. Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med 2012;365:
1713–25.5. Kaser A, Zeissig S, Blumberg RS. Inflammatory bowel disease.
Annu Rev Immunol 2010;28:573–621.6. Xavier RJ, Podilsky DK. Unravelling the pathogenesis of
inflammatory bowel disease. Nature 2007;448:427–34.7. Rabinowitz K, Mayer L. Working out mechanisms of
controlled/physiologic inflammation in the GI tract. ImmunolRes 2012;54:14–24.
8. Mizoguchi A. Animal models of inflammatory bowel disease.Prog Mol Biol Transl Sci 2012;105:263–320.
9. Mayer L, Kaser A, Blumberg RS. Dead on arrival: under-standing the failure of CTLA4-immunoglobulin therapy ininflammatory bowel disease. Gastroenterology 2012;143:13–7.
10. Strober W, Fuss I, Mannon P. The fundamental basis ofinflammatory bowel disease. J Clin Invest 2007;117:514–21.
11. Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis ofinflammatory bowel disease. Nature 2011;474:307–17.
12. Lees CW, Barrett JC, Parkes M, Satsangi J. New IBD genetics:common pathways with other diseases. Gut 2011;60:1739–53.
13. Mizoguchi A, Mizoguchi E. Animal models of IBD: linkage tohuman disease. Curr Opin Pharmacol 2010;10:578–87.
14. Sartor RB. Microbial influences in inflammatory bowel diseases.Gastroenterology 2008;134:577–94.
15. Qin J, Li R, Raes J, Arumugam M, Burgdorf KS, Manichanh C,et al. A human gut microbial gene catalogue established bymetagenomic sequencing. Nature 2010;464:59–65.
16. Colombel JF, Watson AJ, Neurath MF. The 10 remainingmysteries of inflammatory bowel disease. Gut 2008;57:429–33.
17. Plevy SE, Targan SR. Future therapeutic approaches forinflammatory bowel diseases. Gastroenterology 2011;140:1838–46.
18. Elson CO, Sartor RB, Tennyson GS, Riddell RH. Experimentalmodels of inflammatory bowel disease. Gastroenterology1995;109:1344–67.
19. Strober W, Fuss IJ, Blumberg RS. The immunology of mucosalmodels of inflammation. Annu Rev Immunol 2002;20:495–549.
IDNEY AND BOWEL

CONCLUSION 519
20. Gunther C, Martini E, Wittkopf N, Amann K, Weigmann B,Neumann H, et al. Caspase-8 regulates TNF-a-induced epithe-lial necroptosis and terminal ileitis. Nature 2011;477:335–9.
21. Takahashi D, Hase K, Kimura S, Nakatsu F, Ohmae M,Mandai Y, et al. The epithelial-specific membrane traffickingfactor AP-1B controls gut immune homeostasis in mice.Gastroenterology 2011;141:621–32.
22. Liao CM, Zimmer MI, Shanmuganad S, Yu HT, Cardell SL,Wang CR. Dysregulation of CD1d-restricted type II naturalkiller T cells leads to spontaneous development of colitis inmice. Gastroenterology 2012;142:326–34.
23. Danese S, Sans M, Fiocchi C. Inflammatory bowel disease: therole of environmental factors. Autoimmun Rev 2004;3:394–400.
24. Kappelman MD, Rifas-Shiman SL, Kleinman K, Ollendorf D,Bousvaros A, Grand RJ, et al. The prevalence and geographicdistribution of Crohn’s disease and ulcerative colitis in theUnited States. Clin Gastroenterol Hepatol 2007;5:1424–9.
25. Fumagalli M, Pozzoli U, Cagliani R, Comi GP, Riva S, Clerici M,et al. Parasites represent a major selective force for interleukingenes and shape the genetic predisposition to autoimmuneconditions. J Exp Med 2009;206:1395–408.
26. Bager P, Vinkel Hansen A, Wohlfahrt J, Melbye M. Helminthinfection does not reduce risk for chronic inflammatory diseasein a population-based cohort study. Gastroenterology 2012;142:55–62.
27. Elliott DE, Weinstock JV. Helminthic therapy: using worms totreat immune-mediated disease. Adv Exp Med Biol 2009;666:157–66.
28. Elliott DE, Li J, Blum A, Metwali A, Qadir K, Urban Jr JF, et al.Exposure to schistosome eggs protects mice fromTNBS-induced colitis. Am J Physiol 2003;284:G385–91.
29. Khan WI, Blennerhasset PA, Varghese AK, Chowdhury SK,Omsted P, Deng Y, et al. Intestinal nematode infectionameliorates experimental colitis in mice. Infect Immun 2002;70:5931–7.
30. Ruyssers NE, De Winter BY, De Man JG, Loukas A, Pearson MS,Weinstock JV, et al. Therapeutic potential of helminth solubleproteins in TNBS-induced colitis in mice. Inflamm Bowel Dis
2009;15:491–500.31. Elliott DE, Metwali A, Leung J, Setiawan T, Blum AM, Ince MN,
et al. Colonization with Heligmosomoides polygyrus suppressesmucosal IL-17 production. J Immunol 2008;181:2414–9.
32. Johnston MJ, Wang A, Catarino ME, Ball L, Pha VC,MacDonald JA, et al. Extracts of the rat tapeworm, Hymenolepisdiminuta, suppress macrophage activation in vitro and alleviatechemically induced colitis in mice. Infect Immun
2010;78:1364–75.33. Metwali A, Setiawan T, Blum AM, Urban J, Elliott DE, Hang L,
et al. Induction of CD8þ regulatory T cells in the intestine byHeligmosomoides polygyrus infection. Am J Physiol Gastrointest
Liver Physiol 2006;291:G253–9.34. Ince MN, Elliott DE, Setiawan T, Metwali A, Blum A, Chen HL,
et al. Role of T cell TGF-beta signaling in intestinal cytokineresponses and helminthic immune modulation. Eur J Immunol
2009;39:1870–8.35. Summers RW, Elliott DE, Urban Jr JF, Thompson RA,
Weinstock JV. Trichuris suis therapy for active ulcerative colitis:a randomized controlled trial. Gastroenterology 2005;128:825–32.
36. Hunter MM, Wang A, McKay DM. Helminth infection enhancesdisease in a murine TH2 model of colitis. Gastroenterology
2007;132:1320–30.37. Gaskins HR, Vondrak-Juergens GL, McCracken BA,
Woolsey JH. Specific-pathogen-free conditions enhance inflam-matory bowel disease in T-cell receptor knockout, but not C3H/HeJBir mice. Lab Anim Sci 1997;47:650–5.
VI. URINARY TRACT, K
38. Shimomura Y, Mizoguchi E, Sugimoto K, Kibe R, Benno Y,Mizoguchi A, et al. Regulatory role of B-1 B cells in chroniccolitis. Int Immunol 2008;20:729–37.
39. Rook GA. Hygiene hypothesis and autoimmune diseases. ClinRev Allergy Immunol 2012;42:5–15.
40. Nagatani K, Wang S, Llado V, Lau CW, Li Z, Mizoguchi A,et al. Chitin microparticles for the control of intestinalinflammation. Inflamm Bowel Dis 2012;18:1698–710.
41. Gilat T, Hacohen D, Lilos P, Langman MJ. Childhood factors inulcerative colitis and Crohn’s disease: An international coop-erative study. Scand J Gastroenterol 1987;22:1009–24.
42. Andersson RE, Olaison G, Tysk C, Ekbom A. Appendectomyand protection against ulcerative colitis. N Engl J Med 2001;344:808–14.
43. Koutroubakis IE, Vlachonikolis IG. Appendectomy and thedevelopment of ulcerative colitis: results of a metaanalysis ofpublished case-control studies. Am J Gastroenterol
2000;95:171–6.44. Rutgeerts P, D’Haens G, Hiele M, Geboes K, Vantrappen G.
Appendectomy protects against ulcerative colitis. Gastroenter-ology 1994;106:1251–3.
45. Frisch M, Pedersen BV, Andersson RE. Appendicitis, mesentericlymphadenitis, and subsequent risk of ulcerative colitis: cohortstudies in Sweden and Denmark. BMJ 2009;338:b716.
46. Mizoguchi A, Mizoguchi E, Chiba C, Bhan AK. Role ofappendix in the development of inflammatory bowel disease inTCR-alpha mutant mice. J Exp Med 1996;184:707–15.
47. Naganuma M, Iizuka B, Torii A, Ogihara T, Kawamura Y,Ichinose M, et al. Appendectomy protects against the develop-ment of ulcerative colitis and reduces its recurrence: results ofa multicenter case-controlled study in Japan. Am J Gastroenterol
2001;96:1123–6.48. Krieglstein CF, Cerwinka WH, Laroux FS, Grisham MB,
Schurmann G, Bruwer M, et al. Role of appendix and spleen inexperimental colitis. J Surg Res 2001;101:166–75.
49. Mizoguchi A, Mizoguchi E, Saubermann LJ, Higaki K,Blumberg RS, Bhan AK. Limited CD4 T-cell diversity associatedwith colitis in T-cell receptor alpha mutant mice requires a Thelper 2 environment. Gastroenterology 2000;119:983–95.
50. Farkas SA, Hornung M, Sattler C, Steinbauer M, Anthuber M,Obermeier F, et al. Preferential migration of CD62L cells into theappendix in mice with experimental chronic colitis. Eur Surg Res2005;37:115–22.
51. Rubin DT, Rothe JA. The peri-appendiceal red patch in ulcera-tive colitis: review of the University of Chicago experience. Dig
Dis Sci 2010;55:3495–501.52. D’Haens G, Geboes K, Peeters M, Baert F, Ectors N, Rutgeerts P.
Patchy cecal inflammation associated with distal ulcerativecolitis: a prospective endoscopic study. Am J Gastroenterol 1997;92:1275–9.
53. Hokama A, Ihama Y, Chinen H, Kishimoto K, Kinjo F, Fujita J.Appendiceal orifice inflammation in ulcerative colitis. Dig DisSci 2010;55:1189.
54. Matsushita M, Tanaka T, Fukui Y, Fukata N, Wakamatsu T,Okazaki K. Peri-appendiceal red patch and pathogenesis of theappendix in ulcerative colitis. Dig Dis Sci 2011;56:2207.
55. Okazaki K, Onodera H, Watanabe N, Nakase H, Uose S,Matsushita M, et al. A patient with improvement of ulcerativecolitis after appendectomy. Gastroenterology 2000;119:502–6.
56. Kim SW, Lee ST, Lee SO, Choi SC. Clinical improvement ofsevere ulcerative colitis after incidental appendectomy: a casereport. Korean J Gastroenterol 2006;47:463–6.
57. Noh CH, Cheung DY, Kim TH, Jun EJ, Lee IK, Kim JI, et al.Remission of ulcerative colitis after appendectomy: a casereport. Korean J Gastroenterol 2010;56:201–4.
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE520
58. Jarnerot G, Andersson M, Franzen L. Laparoscopic appendec-tomy in patients with refractory ulcerative colitis. Gastroenter-ology 2001;120:1562–3.
59. Jo Y, Matsumoto T, Yada S, Nakamura S, Yao T, Hotokezaka M,et al. Histological and immunological features of appendix inpatients with ulcerative colitis. Dig Dis Sci 2003;48:99–108.
60. Bolin TD, Wong S, Crouch R, Engelman JL, Riordan SM.Appendicectomy as a therapy for ulcerative proctitis. Am J
Gastroenterol 2009;104:2476–82.61. Galitovskiy V, Qian J, Chernyavsky AI, Marchenko S, Gindi V,
Edwards RA, et al. Cytokine-induced alterations of a7 nicotinicreceptor in colonic CD4 T cells mediate dichotomous responseto nicotine in murine models of Th1/Th17- versusTh2-mediated colitis. J Immunol 2011;187:2677–87.
62. Guo X, Wang WP, Ko JK, Cho CH. Involvement of neutrophilsand free radicals in the potentiating effects of passive cigarettesmoking on inflammatory bowel disease in rats. Gastroenterology1999;117:884–92.
63. Abdrakhmanova GR, AlSharari S, Kang M, Damaj MI,Akbarali HI. a7-nAChR-mediated suppression of hyperexcit-ability of colonic dorsal root ganglia neurons in experimentalcolitis. Am J Physiol 2010;299:G761–8.
64. Eliakim R, Fan QX, Babyatsky MW. Chronic nicotine adminis-tration differentially alters jejunal and colonic inflammation ininterleukin-10 deficient mice. Eur J Gastroenterol Hepatol
2002;14:607–14.65. Mashimo H, Wu DC, Podolsky DK, Fishman MC. Impaired
defense of intestinal mucosa in mice lacking intestinal trefoilfactor. Science 1996;274:262–5.
66. Hegazi RA, Rao KN, Mayle A, Sepulveda AR, Otterbein LE,Plevy SE. Carbon monoxide ameliorates chronic murine colitisthrough a heme oxygenase 1-dependent pathway. J Exp Med
2005;202:1703–13.67. Sheikh SZ, Hegazi RA, Kobayashi T, Onyiah JC, Russo SM,
Matsuoka K, et al. An anti-inflammatory role for carbonmonoxide and heme oxygenase-1 in chronic Th2-mediatedmurine colitis. J Immunol 2011;186:5506–13.
68. Burns RC, Rivera-Nieves J, Moskaluk CA, Matsumoto S,Cominelli F, Ley K. Antibody blockade of ICAM-1 and VCAM-1ameliorates inflammation in the SAMP-1/Yit adoptive transfermodel of Crohn’s disease in mice. Gastroenterology 2001;121:1428–36.
69. Lahat G, Halperin D, Barazovsky E, Shalit I, Rabau M,Klausner J, et al. Immunomodulatory effects of ciprofloxacin inTNBS-induced colitis in mice. Inflamm Bowel Dis 2007;13:557–65.
70. Cannarile L, Cuzzocrea S, Santucci L, Agostini M, Mazzon E,Esposito E, et al. Glucocorticoid-induced leucine zipper isprotective in Th1-mediated models of colitis. Gastroenterology2009;136:530–41.
71. Nishiyori A, Nagakura Y, Ichikawa K. Piroxicam acceleratesdevelopment of colitis in T-cell receptor alpha chain-deficientmice. Eur J Pharmacol 2009;615:241–5.
72. Kojima R, Kuroda S, Ohkishi T, Nakamaru K, Hatakeyama S.Oxazolone-induced colitis in BALB/C mice: a new method toevaluate the efficacy of therapeutic agents for ulcerative colitis.J Pharmacol Sci 2004;96:307–13.
73. Kojouharoff G, Hans W, Obermeier F, Mannel DN, Andus T,Scholmerich J, et al.Neutralizationof tumournecrosis factor (TNF)but not of IL-1 reduces inflammation in chronic dextran sulphatesodium-induced colitis in mice. Clin Exp Immunol 1997;107:353–8.
74. van Meeteren ME, Meijssen MA, Zijlstra FJ. The effect ofdexamethasone treatment on murine colitis. Scand J Gastroenterol2000;35:517–21.
75. Barrat FJ, Cua DJ, Boonstra A, Richards DF, Crain C,Savelkoul HF, et al. In vitro generation of interleukin
VI. URINARY TRACT, K
10-producing regulatory CD4(þ) T cells is induced by immu-nosuppressive drugs and inhibited by T helper type 1 (Th1)-and Th2-inducing cytokines. J Exp Med 2002;195:603–16.
76. Groux H, O’Garra A, Bigler M, Rouleau M, Antonenko S, deVries JE, et al. A CD4þ T-cell subset inhibits antigen-specificT-cell responses and prevents colitis. Nature 1997;389:737–42.
77. Pedersen AE, Schmidt EG, Gad M, Poulsen SS, Claesson MH.Dexamethasone/1alpha-25-dihydroxyvitamin D3-treateddendritic cells suppress colitis in the SCID T-cell transfermodel. Immunology 2009;127:354–64.
78. Nocentini G, Giunchi L, Ronchetti S, Krausz LT, Bartoli A,Moraca R, et al. A new member of the tumor necrosis factor/nerve growth factor receptor family inhibits T cell receptor-induced apoptosis. Proc Natl Acad Sci USA 1997;94:6216–21.
79. Shimizu J, Yamazaki S, Takahashi T, Ishida Y, Sakaguchi S.Stimulation of CD25(þ)CD4(þ) regulatory T cells through GITRbreaks immunological self-tolerance. Nat Immunol
2002;3:135–42.80. Santucci L, Agostini M, Bruscoli S, Mencarelli A, Ronchetti S,
Ayroldi E, et al. GITR modulates innate and adaptive mucosalimmunity during the development of experimental colitis inmice. Gut 2007;56:52–60.
81. Lee SK, Choi BK, Kim YH, KangWJ, Kim KH, Sakaguchi S, et al.Glucocorticoid-induced tumour necrosis factor receptor family-related receptor signalling exacerbates hapten-induced colitisby CD4þ T cells. Immunology 2006;119:479–87.
82. Uraushihara K, Kanai T, Ko K, Totsuk T, Makita S, Iiyama R,et al. Regulation of murine inflammatory bowel disease byCD25þ and CD25� CD4þ glucocorticoid-induced TNF receptorfamily-related geneþ regulatory T cells. J Immunol 2003;171:708–16.
83. Liao G, Detre C, Berger SB, Engel P, de Waal Malefyt R,Herzog RW, et al. Glucocorticoid-induced tumor necrosisfactor receptor family-related protein regulates CD4(þ)T cell-mediated colitis in mice. Gastroenterology 2012;142:582–91.
84. Ogata H, Kato J, Hirai F, Hida N, Matsui T, Matsumoto T, et al.Double-blind, placebo-controlled trial of oral tacrolimus(FK506) in the management of hospitalized patients withsteroid-refractory ulcerative colitis. Inflamm Bowel Dis 2012;18:803–8.
85. McSharry K, Dalzell AM, Leiper K, El-Matary W. Systematicreview: the role of tacrolimus in the management of Crohn’sdisease. Aliment Pharmacol Ther 2011;34:1282–94.
86. Tamaki H, Nakase H, Matsuura M, Inoue S, Mikami S, Ueno S,et al. The effect of tacrolimus (FK-506) on Japanese patients withrefractory Crohn’s disease. J Gastroenterol 2008;43:774–9.
87. Greenblatt MB, Aliprantis A, Hu B, Glimcher LH. Calcineurinregulates innate antifungal immunity in neutrophils. J Exp Med
2010;207:923–31.88. Weigmann B, Lehr HA, Yancopoulos G, Valenzuela D,
Murphy A, Stevens S, et al. The transcription factor NFATc2controls IL-6-dependent T cell activation in experimental colitis.J Exp Med 2008;205:2099–110.
89. Dohi T, Fujihashi K, Rennert PD, Iwatani K, Kiyono H,McGhee JR. Hapten-induced colitis is associated with colonicpatch hypertrophy and T helper cell 2-type responses. J Exp Med
1999;189:1169–80.90. Ikenoue Y, Tagami T, Murata M. Development and validation of
a novel IL-10 deficient cell transfer model for colitis. Int Immu-
nopharmacol 2005;5:993–1006.91. Lindebo Holm, T, Poulsen SS, Markholst H, Reedtz-Runge S.
Pharmacological evaluation of the SCID T cell transfer model ofcolitis: as a model of Crohn’s disease. Int J Inflam
2012;2012:412178.
IDNEY AND BOWEL

CONCLUSION 521
92. Klein-Hessling S, Bopp T, Jha MK, Schmidt A, Miyatake S,Schmitt E, et al. Cyclic AMP-induced chromatin changessupport the NFATc-mediated recruitment of GATA-3 to theinterleukin 5 promoter. J Biol Chem 2008;283:31030–7.
93. Murthy SN, Cooper HS, Shim H, Shah RS, Ibrahim SA,Sedergran DJ. Treatment of dextran sulfate sodium-inducedmurine colitis by intracolonic cyclosporin. Dig Dis Sci1993;38:1722–34.
94. Satoh Y, Ishiguro Y, Sakuraba H, Kawaguchi S, Hiraga H,Fukuda S, et al. Cyclosporine regulates intestinal epithelialapoptosis via TGF-beta-related signaling. Am J Physiol2009;297:G514–9.
95. Liu Z, Lee J, Krummey S, Lu W, Cai H, Lenardo MJ. The kinaseLRRK2 is a regulator of the transcription factor NFAT thatmodulates the severity of inflammatory bowel disease. Nat
Immunol 2011;12:1063–70.96. Takizawa H, Shintani N, Natsui M, Sasakawa T, Nakakubo H,
Nakajima T, et al. Activated immunocompetent cells in ratcolitis mucosa induced by dextran sulfate sodium and notcomplete but partial suppression of colitis by FK506. Digestion
1995;56:259–64.97. Lamprecht A, Yamamoto H, Takeuchi H, Kawashima Y. Nano-
particles enhance therapeutic efficiency by selectively increasedlocal drug dose in experimental colitis in rats. J Pharmacol Exp
Ther 2005;315:196–202.98. van Dieren JM, Lambers ME, Kuipers EJ, Samsom JN, van der
Woude CJ, Nieuwenhuis EE. Local immune regulation ofmucosal inflammation by tacrolimus. Dig Dis Sci 2010;55:2514–9.
99. Yoshino T, Nakase H, Honzawa Y, Matsumura K, Yamamoto S,Takeda Y, et al. Immunosuppressive effects of tacrolimus onmacrophages ameliorate experimental colitis. Inflamm Bowel Dis
2010;16:2022–33.100. Berg DJ, Zhang J, Weinstock JV, Ismail HF, Earle KA, Alila H,
et al. Rapid development of colitis in NSAID-treated IL-10-deficient mice. Gastroenterology 2002;123:1527–42.
101. Matharu KS, Mizoguchi E, Cotoner CA, Nguyen DD, Mingle B,Iweala OI, et al. Toll-like receptor 4-mediated regulation ofspontaneous Helicobacter-dependent colitis in IL-10-deficientmice. Gastroenterology 2009;137:1380–90.
102. Narushima S, DiMeo D, Tian J, Zhang J, Liu D, Berg DJ.5-Lipoxygenase-derived lipid mediators are not required for thedevelopment of NSAID-induced inflammatory bowel disease inIL-10�/� mice. Am J Physiol 2008;294:G477–88.
103. Hale LP, Gottfried MR, Swidsinski A. Piroxicam treatment of IL-10-deficient mice enhances colonic epithelial apoptosis andmucosal exposure to intestinal bacteria. Inflamm Bowel Dis
2005;11:1060–9.104. Wilson MS, Ramalingam TR, Rivollier A, Shenderov K,
Mentink-Kane MM, Madala SK, et al. Colitis and intestinalinflammation in IL10�/� mice results from IL-13Ra2-mediated attenuation of IL-13 activity. Gastroenterology 2011;140:254–64.
105. Brewer S, McPherson M, Fujiwara D, Turovskaya O, Ziring D,Chen L, et al. Molecular imaging of murine intestinal inflam-mation with 2-deoxy-2-[18F]fluoro-D-glucose and positronemission tomography. Gastroenterology 2008;135:744–55.
106. Cattaruzza F, Lyo V, Jones E, Pham D, Hawkins J, Kirkwood K,et al. Cathepsin S is activated during colitis and causes visceralhyperalgesia by a PAR2-dependent mechanism in mice.Gastroenterology 2011;141. 1864–674.
107. Matsunaga H, Hokari R, Higashiyama M, Kurihara C, Okada Y,Watanabe C, et al. Cilostazol, a specific PDE-3 inhibitor,ameliorates chronic ileitis via suppression of interaction ofplatelets with monocytes. Am J Physiol 2009;297:G1077–84.
VI. URINARY TRACT, K
108. Tanaka K, Suemasu S, Ishihara T, Tasaka Y, Arai Y,Mizushima T. Inhibition of both COX-1 and COX-2 and result-ing decrease in the level of prostaglandins E2 is responsible fornon-steroidal anti-inflammatory drug (NSAID)-dependentexacerbation of colitis. Eur J Pharmacol 2009;603:120–32.
109. Brown JB, Lee G, Managlia E, Grimm GR, Dirisina R,Goretsky T, et al. Mesalamine inhibits epithelial beta-cateninactivation in chronic ulcerative colitis. Gastroenterology
2010;138:595–605.110. Santucci L, Wallace J, Mencarelli A, Farneti S, Morelli A,
Fiorucci S. Different sensitivity of lamina propria T-cell subsetsto nitric oxide-induced apoptosis explains immunomodulatoryactivity of a nitric oxide-releasing derivative of mesalamine inrodent colitis. Gastroenterology 2005;128:1243–57.
111. Hayashi Y, Aoyagi K, Morita I, Yamamoto C, Sakisaka S. Oraladministration of mesalazine protects against mucosal injuryand permeation in dextran sulfate sodium-induced colitis inrats. Scand J Gastroenterol 2009;44:1323–31.
112. Kontoyiannis D, Pasparakis M, Pizarro TT, Cominelli F,Kollias G. Impaired on/off regulation of TNF biosynthesisin mice lacking TNF AU-rich elements: implications for jointand gut-associated immunopathologies. Immunity 1999;10:387–98.
113. Mizoguchi E, Mizoguchi A, Bhan AK. Role of cytokines in theearly stages of chronic colitis in TCR alpha-mutant mice. LabInvest 1997;76:385–97.
114. Mizoguchi E, Mizoguchi A, Takedatsu H, Cario E, de Jong YP,Ooi CJ, et al. Role of tumor necrosis factor receptor 2 (TNFR2) incolonic epithelial hyperplasia and chronic intestinal inflamma-tion in mice. Gastroenterology 2002;122:134–44.
115. Lee EG, Boone DL, Chai S, Libby SL, Chien M, Lodolce JP, et al.Failure to regulate TNF-induced NF-kappaB and cell deathresponses in A20-deficient mice. Science 2000;289:2350–4.
116. Noti M, Corazza N, Mueller C, Berger B, Brunner T. TNFsuppresses acute intestinal inflammation by inducing localglucocorticoid synthesis. J Exp Med 2010;207:1057–66.
117. Naito Y, Takagi T, Handa O, Ishikawa T, Nakagawa S,Yamaguchi T, et al. Enhanced intestinal inflammation inducedby dextran sulfate sodium in tumor necrosis factor-alpha defi-cient mice. J Gastroenterol Hepatol 2003;18:560–9.
118. Xu Y, Hunt NH, Bao S. The correlation between proin-flammatory cytokines, MAdCAM-1 and cellular infiltration inthe inflamed colon from TNF-alpha gene knockout mice.Immunol Cell Biol 2007;85:633–9.
119. Reinisch W, van Assche G, Befrits R, Connell W, D’Haens G,Ghosh S, et al. Recommendations for the treatment of ulcerativecolitis with infliximab: a gastroenterology expert groupconsensus. J Crohns Colitis 2012;6:248–58.
120. Curtis JR, Patkar N, Xie A, Martin C, Allison JJ, Saag M, et al.Risk of serious bacterial infections among rheumatoid arthritispatients exposed to tumor necrosis factor alpha antagonists.Arthritis Rheum 2007;56:1125–33.
121. Stillie R, Stadnyk AW. Role of TNF receptors, TNFR1 andTNFR2, in dextran sodium sulfate-induced colitis. Inflamm
Bowel Dis 2009;15:1515–25.122. Mizoguchi E, Hachiya Y, Kawada M, Nagatani K, Ogawa A,
Sugimoto K, et al. TNF receptor type I-dependent activation ofinnate responses to reduce intestinal damage-associatedmortality. Gastroenterology 2008;134:470–80.
123. Edelblum KL, Goettel JA, Koyama T, McElroy SJ, Yan F,Polk DB. TNFR1 promotes tumor necrosis factor-mediatedmouse colon epithelial cell survival through RAF activation ofNF-kappaB. J Biol Chem 2008;283:29485–94.
124. Wang F, Schwarz BT, GrahamWV, Wang Y, Su L, Clayburgh DR,et al. IFN-gamma-induced TNFR2 expression is required for
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE522
TNF-dependent intestinal epithelial barrier dysfunction.Gastroenterology 2006;131:1153–63.
125. Ebach DR, Riehl TE, Stenson WF. Opposing effects of tumornecrosis factor receptor 1 and 2 in sepsis due to cecal ligationand puncture. Shock 2005;23:311–8.
126. Yang Y, Wang H, Dou Y, Wang Y, Han G, Wang R, et al. Col-itogenic role of tumour necrosis factor (TNF) receptors in tri-nitrobenzene sulphonic acid colitis: TNF-R1 ablation does notaffect systemic inflammatory response. Clin Exp Immunol
2011;165:372–82.127. Kajino-Sakamoto R, Inagaki M, Lippert E, Akira S, Robine S,
Matsumoto K, et al. Enterocyte-derived TAK1 signalingprevents epithelium apoptosis and the development of ileitisand colitis. J Immunol 2008;181:1143–52.
128. Kontoyiannis D, Boulougouris G, Manoloukos M, Armaka M,Apostolaki M, Pizarro T, et al. Genetic dissection of the cellularpathways and signaling mechanisms in modeled tumornecrosis factor-induced Crohn’s-like inflammatory boweldisease. J Exp Med 2002;196:1563–74.
129. Dayer Schneider, J, Seibold I, Saxer-Sekulic N, Paredes BE,Saurer L, Mueller C. Lack of TNFR2 expression by CD4(þ) T cellsexacerbates experimental colitis. Eur J Immunol 2009;39:1743–53.
130. Yonekawa K, Harlan JM. Targeting leukocyte integrins inhuman diseases. J Leukoc Biol 2005;77:129–40.
131. Podolsky DK, Lobb R, King N, Benjamin CD, Pepinsky B,Sehgal P, et al. Attenuation of colitis in the cotton-top tamarin byanti-alpha 4 integrin monoclonal antibody. J Clin Invest
1993;92:372–80.132. Ghosh S, Panaccione R. Anti-adhesion molecule therapy for
inflammatory bowel disease. Therap Adv Gastroenterol 2010;3:239–58.
133. Murphy CT, Moloney G, Macsharry J, Haynes A, Faivre E,Quinlan A, et al. Technical Advance: Function and efficacy of ana4-integrin antagonist using bioluminescence imaging to detectleukocyte trafficking in murine experimental colitis. J Leukoc Biol2010;88:1271–8.
134. Bjursten M, Bland PW, Willen R, Hornquist EH. Long-termtreatment with anti-alpha 4 integrin antibodies aggravatescolitis in G alpha i2-deficient mice. Eur J Immunol 2005;35:2274–83.
135. Picarella D, Hurlbut P, Rottman J, Shi X, Butcher E,Ringler DJ. Monoclonal antibodies specific for beta 7 integrinand mucosal addressin cell adhesion molecule-1 (MAdCAM-1) reduce inflammation in the colon of SCID mice recon-stituted with CD45RBhigh CD4þ T cells. J Immunol
1997;158:2099–106.136. Goto A, Arimura Y, Shinomura Y, Imai K, Hinoda Y. Antisense
therapy of MAdCAM-1 for trinitrobenzenesulfonic acid-induced murine colitis. Inflamm Bowel Dis 2006;12:758–65.
137. Farkas S, Hornung M, Sattler C, Edtinger K, Steinbauer M,Anthuber M, et al. Blocking MAdCAM-1 in vivo reducesleukocyte extravasation and reverses chronic inflammation inexperimental colitis. Int J Colorectal Dis 2006;21:71–8.
138. Kato S, Hokari R, Matsuzaki K, Iwai A, Kawaguchi A, Nagao S,et al. Amelioration of murine experimental colitis by inhibitionof mucosal addressin cell adhesion molecule-1. J Pharmacol Exp
Ther 2000;295:183–9.139. Feagan BG, Greenberg GR, Wild G, Fedorak RN, Pare P,
McDonald JW, et al. Treatment of ulcerative colitis witha humanized antibody to the alpha4beta7 integrin. N Engl J Med
2005;352:2499–507.140. Feagan BG, Greenberg GR, Wild G, Fedorak RN, Pare P,
McDonald JW, et al. Treatment of active Crohn’s disease withMLN0002, a humanized antibody to the alpha4beta7 integrin.Clin Gastroenterol Hepatol 2008;6:1370–7.
VI. URINARY TRACT, K
141. Hesterberg PE, Winsor-Hines D, Briskin MJ, Soler-Ferran D,Merrill C, Mackay CR, et al. Rapid resolution of chronic colitisin the cotton-top tamarin with an antibody to a gut-homingintegrin alpha 4 beta 7. Gastroenterology 1996;111:1373–80.
142. Sydora BC, Wagner N, Lohler J, Yakoub G, Kronenberg M,Muller W, et al. Beta7 Integrin expression is not required for thelocalization of T cells to the intestine and colitis pathogenesis.Clin Exp Immunol 2002;129:35–42.
143. Apostolaki M, Manoloukos M, Roulis M, Wurbel MA,Muller W, Papadakis KA, et al. Role of beta7 integrin and thechemokine/chemokine receptor pair CCL25/CCR9 in modeledTNF-dependent Crohn’s disease. Gastroenterology 2008;134:2025–35.
144. Ludvıksson BR, Strober W, Nishikomori R, Hasan SK,Ehrhardt RO. Administration of mAb against alpha E beta 7prevents and ameliorates immunization-induced colitis in IL-2�/� mice. J Immunol 1999;162:4975–82.
145. Peer D, Park EJ, Morishita Y, Carman CV, Shimaoka M. Systemicleukocyte-directed siRNA delivery revealing cyclin D1 as ananti-inflammatory target. Science 2008;319:627–30.
146. Dearling JL, Park EJ, Dunning P, Baker A, Fahey F, Treves ST,et al. Detection of intestinal inflammation by MicroPET imagingusing a (64)Cu-labeled anti-beta(7) integrin antibody. Inflamm
Bowel Dis 2010;16:1458–66.147. Forbes E, Hulett M, Ahrens R, Wagner N, Smart V, Matthaei KI,
et al. ICAM-1-dependent pathways regulate colonic eosino-philic inflammation. J Leukoc Biol 2006;80:330–41.
148. Denning TL, Kim G, Kronenberg M. CD4þCD25þ regulatory Tcells impaired for intestinal homing can prevent colitis.J Immunol 2005;174:7487–91.
149. Mannon PJ, Fuss IJ, Mayer L, Elson CO, Sandborn WJ,Present D, et al. Anti-interleukin-12 antibody for active Crohn’sdisease. N Engl J Med 2004;351:2069–79.
150. Panaccione R, Sandborn W, Gordon G. Briakinumab (anti-interleukin 12/23p40, ABT874) for treatment of Crohn’s disease.Am J Gastroenterol 2010;105:S1245.
151. Sandborn WJ, Feagan BG, Fedorak RN, Scherl E, Fleisher MR,Katz S, et al. A randomized trial of Ustekinumab, a humaninterleukin-12/23monoclonal antibody, in patientswithmoderate-to-severe Crohn’s disease. Gastroenterology 2008;135:1130–41.
152. Neurath MF, Fuss I, Kelsall BL, Stuber E, Strober W. Antibodiesto interleukin 12 abrogate established experimental colitis inmice. J Exp Med 1995;182:1281–90.
153. Davidson NJ, Hudak SA, Lesley RE, Menon S, Leach MW,Rennick DM. IL-12, but not IFN-gamma, plays a major role insustaining the chronic phase of colitis in IL-10-deficient mice.J Immunol 1998;161:3143–9.
154. Simpson SJ, Shah S, Comiskey M, de Jong YP, Wang B,Mizoguchi E, et al. T cell-mediated pathology in two modelsof experimental colitis depends predominantly on the inter-leukin 12/Signal transducer and activator of transcription(Stat)-4 pathway, but is not conditional on interferon gammaexpression by T cells. J Exp Med 1998;187:1225–34.
155. ShirakiM,AiharaH,Kinouchi Y, Takahashi S,OkiM,NoguchiM,et al. IL-12 p40 prevents the development of chronic enterocolitisin IL-10-deficient mice. Lab Invest 2004;84:1491–500.
156. Camoglio L, te Velde AA, de Boer A, ten Kate FJ, Kopf M, vanDeventer SJ. Hapten-induced colitis associated with maintainedTh1 and inflammatory responses in IFN-gamma receptor-deficient mice. Eur J Immunol 2000;30:1486–95.
157. Becker C, Dornhoff H, Neufert C, Fantini MC, Wirtz S,Huebner S, et al. IL-23 cross-regulates IL-12 production in Tcell-dependent experimental colitis. J Immunol 2006;177:2760–4.
158. Yen D, Cheung J, Scheerens H, Poulet F, McClanahan T,McKenzie B, et al. IL-23 is essential for T cell-mediated colitis
IDNEY AND BOWEL

CONCLUSION 523
and promotes inflammation via IL-17 and IL-6. J Clin Invest
2006;116:1310–6.159. Ahern PP, Schiering C, Buonocore S, McGeachy MJ, Cua DJ,
Maloy KJ, et al. Interleukin-23 drives intestinal inflammationthrough direct activity on T cells. Immunity 2010;33:279–88.
160. Kullberg MC, Jankovic D, Feng CG, Hue S, Gorelick PL,McKenzie BS, et al. IL-23 plays a key role in Helicobacterhepaticus-induced T cell-dependent colitis. J Exp Med 2006;203:2485–94.
161. Uhlig HH, McKenzie BS, Hue S, Thompson C, Joyce-Shaikh B,Stepankova R, et al. Differential activity of IL-12 and IL-23 inmucosal and systemic innate immune pathology. Immunity
2006;25:309–18.162. Elson CO, Cong Y, Weaver CT, Schoeb TR, McClanahan TK,
Fick RB, et al. Monoclonal anti-interleukin 23 reverses activecolitis in a T-cell-mediated model in mice. Gastroenterology
2007;132:2359–70.163. Ando Y, Yang GX, Tsuda M, Kawata K, Zhang W, Nakajima T,
et al. The immunobiology of colitis and cholangitis in IL-23p19and IL-17A deleted dnTGFbRII mice. Hepatology
2012;56:1418–26.164. Mizoguchi A, Ogawa A, Takedatsu H, Sugimoto K,
Shimomura Y, Shirane K, et al. Dependence of intestinal gran-uloma formation on unique myeloid DC-like cells. J Clin Invest
2007;117:605–15.165. Sugimoto K, Ogawa A, Shimomura Y, Nagahama K,
Mizoguchi A, Bhan AK. Inducible IL-12-producing B cellsregulate Th2-mediated intestinal inflammation. Gastroenterology2007;133:124–36.
166. Boirivant M, Fuss IJ, Chu A, Strober W. Oxazolone colitis: Amurine model of T helper cell type 2 colitis treatable withantibodies to interleukin 4. J Exp Med 1998;188:1929–39.
167. Buonocore S, Ahern PP, Uhlig HH, Ivanov II, Littman DR,Maloy KJ, et al. Innate lymphoid cells drive interleukin-23-dependent innate intestinal pathology.Nature 2010;464:1371–5.
168. Nishida A, Lau CW, Zhang M, Andoh A, Shi HN, Mizoguchi E,et al. Themembrane-boundmucinmuc1 regulates T helper 17-cellresponses and colitis in mice. Gastroenterology 2012;142:865–74.
169. Annunziato F, Cosmi L, Santarlasci V, Maggi L, Liotta F,Mazzinghi B, et al. Phenotypic and functional features of humanTh17 cells. J Exp Med 2007;204:1849–61.
170. Hovhannisyan Z, Treatman J, Littman DR, Mayer L. Charac-terization of interleukin-17-producing regulatory T cells ininflamed intestinal mucosa from patients with inflammatorybowel diseases. Gastroenterology 2011;140:957–65.
171. Kryczek I, Wu K, Zhao E, Wei S, Vatan L, Szeliga W, et al. IL-17þregulatory T cells in the microenvironments of chronic inflam-mation and cancer. J Immunol 2011;186:4388–95.
172. Hirota K, Duarte JH, Veldhoen M, Hornsby E, Li Y, Cua DJ, et al.Fate mapping of IL-17-producing T cells in inflammatoryresponses. Nat Immunol 2011;12:255–63.
173. Hueber W, Sands BE, Vandemeulebroecke M, Reinisch W,Higgins PDR, Wehkamp J, et al. Inhibition of IL-17A by secu-kinumab is ineffective for Crohn’s disease (CD). J Crohns Colitis2011;5:S7.
174. Zhang Z, Zheng M, Bindas J, Schwarzenberger P, Kolls JK.Critical role of IL-17 receptor signaling in acute TNBS-inducedcolitis. Inflamm Bowel Dis 2006;12:382–8.
175. Feng T, Qin H, Wang L, Benveniste EN, Elson CO, Cong Y. Th17cells induce colitis and promote Th1 cell responses through IL-17 induction of innate IL-12 and IL-23 production. J Immunol
2011;186:6313–8.176. Ogawa A, Andoh A, Araki Y, Bamba T, Fujiyama Y. Neutrali-
zation of interleukin-17 aggravates dextran sulfate sodium-induced colitis in mice. Clin Immunol 2004;110:55–62.
VI. URINARY TRACT, K
177. Medina-Contreras O, Geem D, Laur O, Williams IR, Lira SA,Nusrat A, et al. CX3CR1 regulates intestinal macrophagehomeostasis, bacterial translocation, and colitogenic Th17responses in mice. J Clin Invest 2011;121:4787–95.
178. Ito R, Kita M, Shin-Ya M, Kishida T, Urano A, Takada R, et al.Involvement of IL-17A in the pathogenesis of DSS-inducedcolitis in mice. Biochem Biophys Res Commun 2008;377:12–6.
179. Do JS, Visperas A, Dong C, Baldwin 3rdWM, Min B. Generationof colitogenic Th17 CD4 Tcells is enhanced by IL-17þ gd Tcells.J Immunol 2011;186:4546–50.
180. Izcue A, Hue S, Buonocore S, Arancibia-Carcamo CV, Ahern PP,Iwakura Y, et al. Interleukin-23 restrains regulatory T cellactivity to drive T cell-dependent colitis. Immunity
2008;28:559–70.181. Leppkes M, Becker C, Ivanov II, Hirth S, Wirtz S, Neufert C,
et al. RORgamma-expressing Th17 cells induce murine chronicintestinal inflammation via redundant effects of IL-17A and IL-17F. Gastroenterology 2009;136:257–67.
182. Noguchi D, Wakita D, Tajima M, Ashino S, Iwakura Y, Zhang Y,et al. Blocking of IL-6 signaling pathway prevents CD4þ T cell-mediated colitis in a T(h)17-independent manner. Int Immunol
2007;19:1431–40.183. O’Connor Jr W, Kamanaka M, Booth CJ, Town T, Nakae S,
Iwakura Y, et al. A protective function for interleukin 17A inT cell-mediated intestinal inflammation. Nat Immunol 2009;10:603–9.
184. Ito H, Takazoe M, Fukuda Y, Hibi T, Kusugami K, Andoh A,et al. A pilot randomized trial of a human anti-interleukin-6receptor monoclonal antibody in active Crohn’s disease.Gastroenterology 2004;126:989–96.
185. Atreya R, Mudter J, Finotto S, Mullberg J, Jostock T, Wirtz S,et al. Blockade of interleukin 6 trans signaling suppresses T-cellresistance against apoptosis in chronic intestinal inflammation:evidence in Crohn disease and experimental colitis in vivo. Nat
Med 2000;6:583–8.186. Tajima M, Wakita D, Noguchi D, Chamoto K, Yue Z, Fugo K,
et al. IL-6-dependent spontaneous proliferation is required forthe induction of colitogenic IL-17-producing CD8þ T cells. J ExpMed 2008;205:1019–27.
187. Gay J, Kokkotou E, O’Brien M, Pothoulakis C, Karalis KP.Interleukin-6 genetic ablation protects from trinitrobenzenesulfonic-acid-induced colitis in mice: Putative effect of antiin-flammatory cytokines. Neuroimmunomodulation 2006;13:114–21.
188. Durant L, Watford WT, Ramos HL, Laurence A, Vahedi G,Wei L, et al. Diverse targets of the transcription factor STAT3contribute to T cell pathogenicity and homeostasis. Immunity
2010;32:605–15.189. Takeda K, Clausen BE, Kaisho T, Tsujimura T, Terada N,
Forster I, et al. Enhanced Th1 activity and development ofchronic enterocolitis in mice devoid of Stat3 in macrophagesand neutrophils. Immunity 1999;10:39–49.
190. Pickert G, Neufert C, Leppkes M, Zheng Y, Wittkopf N,Warntjen M, et al. STAT3 links IL-22 signaling in intestinalepithelial cells to mucosal wound healing. J Exp Med 2009;206:1465–72.
191. Ernst M, Inglese M, Waring P, Campbell IK, Bao S, Clay FJ, et al.Defective gp130-mediated signal transducer and activator oftranscription (STAT) signaling results in degenerative jointdisease, gastrointestinal ulceration, and failure of uterineimplantation. J Exp Med 2001;194:189–203.
192. Shang L, Thirunarayanan N, Viejo-Borbolla A, Martin AP,Bogunovic M, Marchesi F, et al. Expression of the chemokinebinding protein M3 promotes marked changes in the accumu-lation of specific leukocyte subsets within the intestine. Gastro-enterology 2009;137:1006–18.
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE524
193. Hart AL, Ng SC, Mann E, Al-Hassi HO, Bernardo D, Knight SC.Homing of immune cells: role in homeostasis and intestinalinflammation. Inflamm Bowel Dis 2010;16:1969–77.
194. Eksteen B, Adams DH. GSK-1605786, a selective small-moleculeantagonist of the CCR9 chemokine receptor for the treatment ofCrohn’s disease. IDrugs 2010;13:472–781.
195. Walters MJ, Wang Y, Lai N, Baumgart T, Zhao BN, Dairaghi DJ,et al. Characterization of CCX282-B, an orally bioavailableantagonist of the CCR9 chemokine receptor, for treatment ofinflammatory bowel disease. J Pharmacol Exp Ther 2010;335:61–9.
196. Rivera-Nieves J, Ho J, Bamias G, Ivashkina N, Ley K,Oppermann M, et al. Antibody blockade of CCL25/CCR9ameliorates early but not late chronic murine ileitis. Gastroen-terology 2006;131:1518–29.
197. Wurbel MA, McIntire MG, Dwyer P, Fiebiger E. CCL25/CCR9interactions regulate large intestinal inflammation in a murinemodel of acute colitis. PLoS One 2011;6:e16442.
198. Glocker EO,KotlarzD, BoztugK,Gertz EM, SchafferAA,NoyanF,et al. Inflammatory bowel disease and mutations affecting theinterleukin-10 receptor. N Engl J Med 2009;361:2033–45.
199. Kotlarz D, Beier R, Murugan D, Diestelhorst J, Jensen O,Boztug K, et al. Loss of Interleukin-10 signaling and infantileinflammatory bowel disease: implications for diagnosis andtherapy. Gastroenterology 2012;143:347–55.
200. Moran CJ, Walters TD, Guo CH, Kugathasan S, Klein C,Turner D, et al. IL-10R polymorphisms are associated withvery-early-onset ulcerative colitis. Inflamm Bowel Dis
2013;19:115–23.201. Fedorak RN, Gangl A, Elson CO, Rutgeerts P, Schreiber S,
Wild G, et al. Recombinant human interleukin 10 in the treat-ment of patients with mild to moderately active Crohn’sdisease. The Interleukin 10 Inflammatory Bowel DiseaseCooperative Study Group. Gastroenterology 2000;119:1473–82.
202. Schreiber S, Fedorak RN, Nielsen OH, Wild G, Williams CN,Nikolaus S, et al. Safety and efficacy of recombinant humaninterleukin 10 in chronic active Crohn’s disease. Gastroenterology2000;119:1461–72.
203. Kuhn R, Lohler J, Rennick D, Rajewsky K, Muller W. Inter-leukin-10-deficient mice develop chronic enterocolitis. Cell1993;75:263–74.
204. Foligne B, Dessein R, Marceau M, Poiret S, Chamaillard M,Pot B, et al. Prevention and treatment of colitis with Lactococcus
lactis secreting the immunomodulatory Yersinia LcrV protein.Gastroenterology 2007;133:862–74.
205. Asseman C, Mauze S, Leach MW, Coffman RL, Powrie F. Anessential role for interleukin 10 in the function of regulatoryT cells that inhibit intestinal inflammation. J Exp Med1999;190:995–1004.
206. MuraiM, TurovskayaO,KimG,MadanR,KarpCL,CheroutreH,et al. Interleukin 10 acts on regulatory T cells to maintainexpression of the transcription factor Foxp3 and suppressivefunction in mice with colitis. Nat Immunol 2009;10:1178–84.
207. Chaudhry A, Samstein RM, Treuting P, Liang Y, Pils MC,Heinrich JM, et al. Interleukin-10 signaling in regulatory T cellsis required for suppression of Th17 cell-mediated inflammation.Immunity 2011;34:566–78.
208. Maillard MH, Cotta-de-Almeida V, Takeshima F, Nguyen DD,Michetti P, Nagler C, et al. The Wiskott–Aldrich syndromeprotein is required for the function of CD4(þ)CD25(þ)Foxp3(þ)regulatory T cells. J Exp Med 2007;204:381–91.
209. Mizoguchi A, Mizoguchi E, Takedatsu H, Blumberg RS,Bhan AK. Chronic intestinal inflammatory condition generatesIL-10-producing regulatory B cell subset characterized by CD1dupregulation. Immunity 2002;16:219–30.
VI. URINARY TRACT, K
210. Pils MC, Bleich A, Prinz I, Fasnacht N, Bollati-Fogolin M,Schippers A, et al. Commensal gut flora reduces susceptibilityto experimentally induced colitis via T-cell-derived interleukin-10. Inflamm Bowel Dis 2011;17:2038–46.
211. Okkenhaug K, Bilancio A, Farjot G, Priddle H, Sancho S,Peskett E, et al. Impaired B and T cell antigen receptor signalingin p110delta PI 3-kinase mutant mice. Science 2002;297:1031–4.
212. Uno JK, Rao KN, Matsuoka K, Sheikh SZ, Kobayashi T, Li F,et al. Altered macrophage function contributes to colitis in micedefective in the phosphoinositide-3 kinase subunit p110d.Gastroenterology 2010;139:1642–53.
213. Vijay-Kumar M, Sanders CJ, Taylor RT, Kumar A, Aitken JD,Sitaraman SV, et al. Deletion of TLR5 results in spontaneouscolitis in mice. J Clin Invest 2007;117:3909–21.
214. van der Sluis M, Bouma J, Vincent A, Velcich A, Carraway KL,Buller HA, et al. Combined defects in epithelial and immuno-regulatory factors exacerbate the pathogenesis of inflammation:mucin 2-interleukin 10-deficient mice. Lab Invest 2008;88:634–42.
215. Begue B, Verdier J, Rieux-Laucat F, Goulet O, Morali A,Canioni D, et al. Defective IL10 signaling defining a subgroup ofpatients with inflammatory bowel disease. Am J Gastroenterol
2011;106:1544–55.216. Mizoguchi A, Mizoguchi E, Bhan AK. The critical role of
interleukin 4 but not interferon gamma in the pathogenesis ofcolitis in T-cell receptor alpha mutant mice. Gastroenterology
1999;116:320–6.217. Braat H, Rottiers P, Hommes DW, Huyghebaert N, Remaut E,
Remon JP, et al. A phase I trial with transgenic bacteriaexpressing interleukin-10 in Crohn’s disease. Clin GastroenterolHepatol 2006;4:754–9.
218. Aggarwal S, Pittenger MF. Human mesenchymal stem cellsmodulate allogeneic immune cell responses. Blood 2005;105:1815–22.
219. DuijvesteinM,VosAC, RoelofsH,WildenbergME,Wendrich BB,Verspaget HW, et al. Autologous bone-marrow-derived mesen-chymal stromal cell treatment for refractory luminal Crohn’sdisease: results of a phase I study. Gut 2010;59:1662–9.
220. Gonzalez MA, Gonzalez-Rey E, Rico L, Buscher D, Delgado M.Adipose-derived mesenchymal stem cells alleviate experi-mental colitis by inhibiting inflammatory and autoimmuneresponses. Gastroenterology 2009;136:978–89.
221. Liang L, Dong C, Chen X, Fang Z, Xu J, Liu M, et al. Humanumbilical cord mesenchymal stem cells ameliorate mice trini-trobenzene sulfonic acid (TNBS)-induced colitis. Cell Transplant2011;20:1395–408.
222. Parekkadan B, Upadhyay R, Dunham J, Iwamoto Y,Mizoguchi E, Mizoguchi A, et al. Bone marrow stromal celltransplants prevent experimental enterocolitis and require hostCD11bþ splenocytes. Gastroenterology 2011;140:966–75.
223. Gonzalez-Rey E, Anderson P, Gonzalez MA, Rico L, Buscher D,Delgado M. Human adult stem cells derived from adiposetissue protect against experimental colitis and sepsis. Gut2009;58:929–39.
224. Ko IK, Kim BG, Awadallah A, Mikulan J, Lin P, Letterio JJ, et al.Targeting improves MSC treatment of inflammatory boweldisease. Mol Ther 2010;18:1365–72.
225. Tanaka F, Tominaga K, Ochi M, Tanigawa T, Watanabe T,Fujiwara Y, et al. Exogenous administration of mesenchymalstem cells ameliorates dextran sulfate sodium-induced colitisvia anti-inflammatory action in damaged tissue in rats. Life Sci2008;83:771–9.
226. Yabana T, Arimura Y, Tanaka H, Goto A, Hosokawa M,Nagaishi K, et al. Enhancing epithelial engraftment of ratmesenchymal stem cells restores epithelial barrier integrity.J Pathol 2009;218:350–9.
IDNEY AND BOWEL

CONCLUSION 525
227. Tanaka H, Arimura Y, Yabana T, Goto A, Hosokawa M,Nagaishi K, et al. Myogenic lineage differentiated mesenchymalstem cells enhance recovery from dextran sulfate sodium-induced colitis in the rat. J Gastroenterol 2011;46:143–52.
228. Duijvestein M, Wildenberg ME, Welling MM, Hennink S,Molendijk I, van Zuylen VL, et al. Pretreatment with interferon-genhances the therapeutic activity ofmesenchymal stromal cells inanimal models of colitis. Stem Cells 2011;29:1549–58.
229. Duijvestein M, Molendijk I, Roelofs H, Vos AC, Verhaar AP,Reinders ME, et al. Mesenchymal stromal cell function is notaffected by drugs used in the treatment of inflammatory boweldisease. Cytotherapy 2011;13:1066–73.
230. Yui S, Nakamura T, Sato T, Nemoto Y, Mizutani T, Zheng X, et al.Functional engraftment of colon epithelium expanded in vitrofrom a single adult Lgr5(þ) stem cell. Nat Med 2012;18:618–23.
231. Cranmer LD, Hersh E. The role of the CTLA4 blockade in thetreatment of malignant melanoma. Cancer Invest 2007;25:613–31.
232. Phan GQ, Yang JC, Sherry RM, Hwu P, Topalian SL,Schwartzentruber DJ, et al. Cancer regression and autoimmu-nity induced by cytotoxic T lymphocyte-associated antigen 4blockade in patients with metastatic melanoma. Proc Natl Acad
Sci USA 2003;100:8372–7.233. Sandborn WJ, Colombel JF, Sands BE, Rutgeerts P, Targan SR,
Panaccione R, et al. Abatacept for Crohn’s disease and ulcera-tive colitis. Gastroenterology 2012;143:62–9.
234. Read S, Malmstrom V, Powrie F. Cytotoxic T lymphocyte-associated antigen 4 plays an essential role in the function ofCD25(þ)CD4(þ) regulatory cells that control intestinal inflam-mation. J Exp Med 2000;192:295–302.
235. Sojka DK, Hughson A, Fowell DJ. CTLA-4 is required byCD4þCD25þ Treg to control CD4þ T-cell lymphopenia-induced proliferation. Eur J Immunol 2009;39:1544–51.
236. Watanabe K, Rao VP, Poutahidis T, Rickman BH, Ohtani M,Xu S, et al. Cytotoxic-T-lymphocyte-associated antigen 4blockade abrogates protection by regulatory T cells in a mousemodel of microbially induced innate immune-driven colitis.Infect Immun 2008;76:5834–42.
237. Liu H, Hu B, Xu D, Liew FY. CD4þCD25þ regulatory T cellscure murine colitis: the role of IL-10, TGF-beta, and CTLA4.J Immunol 2003;171:5012–7.
238. Liu Z, Geboes K, Hellings P, Maerten P, Heremans H,Vandenberghe P, et al. B7 interactions with CD28 and CTLA-4control tolerance or induction of mucosal inflammation inchronic experimental colitis. J Immunol 2001;167:1830–8.
239. Read S, Greenwald R, Izcue A, Robinson N, Mandelbrot D,Francisco L, et al. Blockade of CTLA-4 on CD4þCD25þ regu-latory T cells abrogates their function in vivo. J Immunol
2006;177:4376–83.240. Davenport CM, McAdams HA, Kou J, Mascioli K, Eichman C,
Healy L, et al. Inhibition of pro-inflammatory cytokine genera-tion by CTLA4-Ig in the skin and colon of mice adoptivelytransplanted with CD45RBhi CD4þ T cells correlates withsuppression of psoriasis and colitis. Int Immunopharmacol
2002;2:653–72.241. Coquerelle C, Oldenhove G, Acolty V, Denoeud J, Vansanten G,
Verdebout JM, et al. Anti-CTLA-4 treatment inducesIL-10-producing ICOSþ regulatory T cells displayingIDO-dependent anti-inflammatory properties in a mouse modelof colitis. Gut 2009;58:1363–73.
242. Sandborn WJ, Colombel JF, Frankel M, Hommes D, Lowder JN,Mayer L, et al. Anti-CD3 antibody visilizumab is not effective inpatients with intravenous corticosteroid-refractory ulcerativecolitis. Gut 2010;59:1485–92.
243. van der Woude CJ, Stokkers P, van Bodegraven AA, vanAssche G, Hebzda Z, Paradowski L, et al. Phase I, double-blind,
VI. URINARY TRACT, K
randomized, placebo-controlled, dose-escalation study of NI-0401 (a fully human anti-CD3 monoclonal antibody) inpatients with moderate to severely active Crohn’s disease.Inflamm Bowel Dis 2010;16:1708–16.
244. Powrie F, Leach MW, Mauze S, Menon S, Caddle LB,Coffman RL. Inhibition of Th1 responses prevents inflammatorybowel disease in SCID mice reconstituted with CD45RBhiCD4þ T cells. Immunity 1994;1:553–62.
245. Nguyen DD, Maillard MH, Cotta-de-Almeida V, Mizoguchi E,Klein C, Fuss I, et al. Lymphocyte-dependent and Th2 cytokine-associated colitis in mice deficient in Wiskott–Aldrich syndromeprotein. Gastroenterology 2007;133:1188–97.
246. Feng T, Wang L, Schoeb TR, Elson CO, Cong Y. Microbiotainnate stimulation is a prerequisite for T cell spontaneousproliferation and induction of experimental colitis. J Exp Med
2010;207:1321–32.247. Davidson NJ, Leach MW, Fort MM, Thompson-Snipes L,
Kuhn R, Muller W, et al. T helper cell 1-type CD4þ T cells, butnot B cells, mediate colitis in interleukin 10-deficient mice. J ExpMed 1996;184:241–51.
248. Ma A, Datta M, Margosian E, Chen J, Horak I. T cells, but not Bcells, are required for bowel inflammation in interleukin2-deficient mice. J Exp Med 1995;182:1567–72.
249. Nagahama K, Ogawa A, Shirane K, Shimomura Y, Sugimoto K,Mizoguchi A. Protein kinase C theta plays a fundamental role indifferent types of chronic colitis.Gastroenterology 2008;134:459–69.
250. Park SG, Mathur R, Long M, Hosh N, Hao L, Hayden MS, et al.T regulatory cells maintain intestinal homeostasis by suppress-ing gd T cells. Immunity 2010;33:791–803.
251. Gorelik L, Flavell RA. Abrogation of TGFbeta signaling in Tcellsleads to spontaneous T cell differentiation and autoimmunedisease. Immunity 2000;12:171–81.
252. Martins GA, Cimmino L, Shapiro-Shelef M, Szabolcs M,Herron A, Magnusdottir E, et al. Transcriptional repressorBlimp-1 regulates T cell homeostasis and function. Nat Immunol
2006;7:457–65.253. Meylan F, Song YJ, Fuss I, Villarreal S, Kahle E, Malm IJ, et al.
The TNF-family cytokine TL1A drives IL-13-dependent smallintestinal inflammation. Mucosal Immunol 2011;4:172–85.
254. Izcue A, Coombes JL, Powrie F. Regulatory T cells suppresssystemic and mucosal immune activation to control intestinalinflammation. Immunol Rev 2006;212:256–71.
255. Sarra M, Monteleone I, Stolfi C, Fantini MC, Sileri P, Sica G, et al.Interferon-gamma-expressing cells are a major source ofinterleukin-21 in inflammatory bowel diseases. Inflamm Bowel
Dis 2010;16:1332–9.256. Dardalhon V, Awasthi A, Kwon H, Galileos G, Gao W, Sobel RA,
et al. IL-4 inhibits TGF-beta-induced Foxp3þ T cells and,together with TGF-beta, generates IL-9þ IL-10þ Foxp3(�)effector T cells. Nat Immunol 2008;9:1347–55.
257. Pomie C, Vicente R, Vuddamalay Y, Lundgren BA, van derHoek M, Enault G, et al. Autoimmune regulator (AIRE)-defi-cient CD8þCD28 low regulatory T lymphocytes fail to controlexperimental colitis. Proc Natl Acad Sci USA 2011;108:12437–42.
258. Vinay DS, Kim CH, Choi BK, Kwon BS. Origins and functionalbasis of regulatory CD11cþCD8þ T cells. Eur J Immunol
2009;39:1552–63.259. Poussier P, Ning T, Banerjee D, Julius M. A unique subset of
self-specific intraintestinal T cells maintains gut integrity. J ExpMed 2002;195:1491–7.
260. Ueno Y, Tanaka S, Sumii M, Miyake S, Tazuma S, Taniguchi M,et al. Single dose of OCH improves mucosal T helper type 1/Thelper type 2 cytokine balance and prevents experimental colitisin the presence of valpha14 natural killer Tcells in mice. Inflamm
Bowel Dis 2005;11:35–41.
IDNEY AND BOWEL

22. ANIMAL MODELS OF INFLAMMATORY BOWEL DISEASE526
261. van Assche G, Dalle I, Noman M, Aerden I, Swijsen C,Asnong K, et al. A pilot study on the use of the humanized anti-interleukin-2 receptor antibody daclizumab in active ulcerativecolitis. Am J Gastroenterol 2003;98:369–76.
262. van Assche G, Sandborn WJ, Feagan BG, Salzberg BA, Silvers D,Monroe PS, et al. Daclizumab, a humanised monoclonal anti-body to the interleukin 2 receptor (CD25), for the treatment ofmoderately to severely active ulcerative colitis: a randomised,double blind, placebo controlled, dose ranging trial. Gut
2006;55:1568–74.263. Kam JC, Szefler SJ, Surs W, Sher ER, Leung DY. Combination IL-
2 and IL-4 reduces glucocorticoid receptor-binding affinity andT cell response to glucocorticoids. J Immunol 1993;151:3460–6.
264. Sands BE, Sandborn WJ, Creed TJ, Dayan CM, Dhanda AD, vanAssche GA, et al. Basiliximab does not increase efficacy ofcorticosteroids in patients with steroid-refractory ulcerativecolitis. Gastroenterology 2012;143:356–64.
265. Sadlack B, Merz H, Schorle H, Schimpl A, Feller AC, Horak I.Ulcerative colitis-like disease in mice with a disruptedinterleukin-2 gene. Cell 1993;75:253–61.
266. Willerford DM, Chen J, Ferry JA, Davidson L, Ma A, Alt FW.Interleukin-2 receptor alpha chain regulates the size and contentof the peripheral lymphoid compartment. Immunity
1995;3:521–30.267. Malek TR. The biology of interleukin-2. Annu Rev Immunol
2008;26:453–79.268. Dieckmann D, Plottner H, Berchtold S. Ex vivo isolation and
characterization of CD4þCD25þ T cells with regulatory prop-erties from human blood. J Exp Med 2001;193:1303–10.
269. Pfister K, Wittig BM, Jungling B, Ecker KW, Barth S, Huhn M,et al. The in vitro anti-inflammatory effects of recombinant anti-CD25 immunotoxin on lamina propria T cells of patients withinflammatory bowel disease are not sufficient to cure experi-mental colitis in mice. Int J Colorectal Dis 2002;17:77–84.
270. Hommes DW, Mikhajlova TL, Stoinov S, Stimac D, Vucelic B,Lonovics J, et al. Fontolizumab, a humanised anti-interferongamma antibody, demonstrates safety and clinical activity inpatients with moderate to severe Crohn’s disease. Gut
2006;55:1131–7.271. Reinisch W, de Villiers W, Bene L, Simon L, Racz I, Katz S, et al.
Fontolizumab in moderate to severe Crohn’s disease: a phase 2,randomized, double-blind, placebo-controlled, multiple-dosestudy. Inflamm Bowel Dis 2010;16:233–42.
272. Kim G, Turovskaya O, Levin M, Byrne FR, Whoriskey JS,McCabe JG, et al. Spontaneous colitis occurrence in transgenicmice with altered B7-mediated costimulation. J Immunol
2008;181:5278–88.273. Kosiewicz MM, Nast CC, Krishnan A, Rivera-Nieves J,
Moskaluk CA, Matsumoto S, et al. Th1-type responses mediatespontaneous ileitis in a novel murine model of Crohn’s disease.J Clin Invest 2001;107:695–702.
274. Iijima H, Neurath MF, Nagaishi T, Glickman JN,Nieuwenhuis EE, Nakajima A, et al. Specific regulation of Thelper cell 1-mediated murine colitis by CEACAM1. J Exp Med
2004;199:471–82.275. Kullberg MC, Ward JM, Gorelick PL, Caspar P, Hieny S,
Cheever A, et al. Helicobacter hepaticus triggers colitis in specific-pathogen-free interleukin-10 (IL-10)-deficient mice through anIL-12- and gamma interferon-dependent mechanism. InfectImmun 1998;66:5157–66.
276. Sheikh SZ, Matsuoka K, Kobayashi T, Li F, Rubinas T, Plevy SE.IFN-gamma is a negative regulator of IL-23 in murine macro-phages and experimental colitis. J Immunol 2010;184:4069–73.
277. Tozawa K, Hanai H, Sugimoto K, Baba S, Sugimura H, Aoshi T,et al. Evidence for the critical role of interleukin-12 but not
VI. URINARY TRACT, K
interferon-gamma in the pathogenesis of experimental colitis inmice. J Gastroenterol Hepatol 2003;18:578–87.
278. Egea L, Hirata Y, Kagnoff MF. GM-CSF: a role in immune andinflammatory reactions in the intestine. Expert Rev Gastroenterol
Hepatol 2010;4:723–31.279. Dieckgraefe BK, Korzenik JR. Treatment of active Crohn’s
disease with recombinant human granulocyte-macrophagecolony-stimulating factor. Lancet 2002;360:1478–80.
280. Korzenik JR, Dieckgraefe, Korzenik BK, Valentine JF,Hausman DF, Gilbert MJ. Sargramostim for active Crohn’sdisease. N Engl J Med 2005;352:2193–201.
281. Goldstein JI, Kominsky DJ, Jacobson N, Bowers B, Regalia K,Austin GL, et al. Defective leukocyte GM-CSF receptor (CD116)expression and function in inflammatory bowel disease.Gastroenterology 2011;141:208–16.
282. Bernasconi E, Favre L, Maillard MH, Bachmann D, Pythoud C,BouzoureneH, et al. Granulocyte-macrophage colony-stimulatingfactor elicits bone marrow-derived cells that promote efficientcolonic mucosal healing. Inflamm Bowel Dis 2012;16:428–41.
283. Sainathan SK, Hanna EM, Gong Q, Bishnupuri KS, Luo Q,Colonna M, et al. Granulocyte macrophage colony-stimulatingfactor ameliorates DSS-induced experimental colitis. InflammBowel Dis 2008;14:88–99.
284. Xu Y, Hunt NH, Bao S. The role of granulocyte macrophage-colony-stimulating factor in acute intestinal inflammation. CellRes 2008;18:1220–9.
285. Herrlinger KR, Witthoeft T, Raedler A, Bokemeyer B,Krummenerl T, Schulzke JD, et al. Randomized, double blindcontrolled trial of subcutaneous recombinant humaninterleukin-11 versus prednisolone in active Crohn’s disease.Am J Gastroenterol 2006;101:793–7.
286. Greenwood-van Meerveld B, Tyler K, Keith Jr JC. Recombinanthuman interleukin-11 modulates ion transport and mucosalinflammation in the small intestine and colon. Lab Invest
2000;80:1269–80.287. Peterson RL, Wang L, Albert L, Keith Jr JC, Dorner AJ. Molec-
ular effects of recombinant human interleukin-11 in theHLA-B27 rat model of inflammatory bowel disease. Lab Invest
1998;78:1503–12.288. Pfeiffer CJ, Sato S, Qiu BS, Keith JC, Evangelista S. Cellular
pathology of experimental colitis induced by trini-trobenzenesulphonic acid (TNBS): protective effects of recombi-nant human interleukin-11. Inflammopharmacology 1997;5:363–81.
289. Qiu BS, Pfeiffer CJ, Keith Jr JC. Protection by recombinanthuman interleukin-11 against experimental TNB-induced colitisin rats. Dig Dis Sci 1996;41:1625–30.
290. Sandborn WJ, Sands BE, Wolf DC, Valentine JF, Safdi M, Katz S,et al. Repifermin (keratinocyte growth factor-2) for the treat-ment of active ulcerative colitis: a randomized, double-blind,placebo-controlled, dose-escalation trial. Aliment Pharmacol
Ther 2003;17:1355–64.291. Egger B, Procaccino F, Sarosi I, Tolmos J, Buchler MW,
Eysselein VE. Keratinocyte growth factor ameliorates dextransodium sulfate colitis in mice. Dig Dis Sci 1999;44:836–44.
292. Greenwood-van Meerveld B, Venkova K, Connolly K. Efficacyof repifermin (keratinocyte growth factor-2) against abnormal-ities in gastrointestinal mucosal transport in a murine model ofcolitis. J Pharm Pharmacol 2003;55:67–75.
293. Miceli R, Hubert M, Santiago G, Yao DL, Coleman TA,Huddleston KA, et al. Efficacy of keratinocyte growth factor-2 indextran sulfate sodium-induced murine colitis. J Pharmacol Exp
Ther 1999;290:464–71.294. Chen Y, Chou K, Fuchs E, Havran WL, Boismenu R. Protection
of the intestinal mucosa by intraepithelial gamma delta T cells.Proc Natl Acad Sci USA 2002;99:14338–43.
IDNEY AND BOWEL

CONCLUSION 527
295. Targan SR, Karp LC. Defects in mucosal immunity leading toulcerative colitis. Immunol Rev 2005;206:296–305.
296. Leiper K, Martin K, Ellis A, Subramanian S, Watson AJ,Christmas SE, et al. Randomised placebo-controlled trial of ritux-imab (anti-CD20) in active ulcerative colitis. Gut 2011;60:1520–6.
297. Tayal V, Chiu YH, George E, Mane S. Colitis associated withactive systemic lupus erythematosus successfully treated withrituximab. J Clin Rheumatol 2011;17:79–82.
298. Goetz M, Atreya R, Ghalibafian M, Galle PR, Neurath MF.Exacerbation of ulcerative colitis after rituximab salvagetherapy. Inflamm Bowel Dis 2007;13:1365–8.
299. El Fassi D, Nielsen CH, Junker P, Hasselbalch HC,Hegedus L. Systemic adverse events following rituximabtherapy in patients with Graves’ disease. J Endocrinol Invest2011;34:e163–7.
300. Ardelean DS, Gonska T, Wires S, Cutz E, Griffiths A, Harvey E,et al. Severe ulcerative colitis after rituximab therapy. Pediatrics2010;126:e243–6.
301. Bhalme M, Hayes S, Norton A, Lal S, Chinoy H, Paine P.Rituximab-associated colitis. Inflamm Bowel Dis 2013;19:E41–3.
302. Sekkach Y, Hammi S, Elqatni M, Fatihi J, Badaoui M, Elomri N,et al. Ulcerative colitis: exceptional consequence after rituximabtherapy. Ann Pharm Fr 2011;69:265–9.
303. Mauri C, Bosma A. Immune regulatory function of B cells. AnnuRev Immunol 2012;30:221–41.
304. Mizoguchi A, Bhan AK. A case for regulatory B cells. J Immunol2006;176:705–10.
305. Mizoguchi A, Mizoguchi E, Chiba C, Spiekermann GM,Tonegawa S, Nagler-Anderson C, et al. Cytokine imbalance andautoantibody production in T cell receptor-alpha mutant micewith inflammatory bowel disease. J Exp Med 1996;183:847–56.
306. Mizoguchi A, Mizoguchi E, Smith RN, Preffer FI, Bhan AK.Suppressive role of B cells in chronic colitis of T cell receptoralpha mutant mice. J Exp Med 1997;186:1749–56.
307. Torchinsky MB, Garaude J, Martin AP, Blander JM. Innateimmune recognition of infected apoptotic cells directs T(H)17cell differentiation. Nature 2009;458:78–82.
308. Shimomura Y, Ogawa A, Kawada M, Sugimoto K, Mizoguchi E,Shi HN, et al. A unique B2 B cell subset in the intestine. J ExpMed 2008;205:1343–55.
309. Ray A, Basu S, Williams CB, Salzman NH, Dittel BN. A novelIL-10-independent regulatory role for B cells in suppressingautoimmunity by maintenance of regulatory T cells via GITRligand. J Immunol 2012;188:3188–98.
310. Ostanin DV, Pavlick KP, Bharwani S, D’Souza D, Furr KL,Brown CM, et al. T cell-induced inflammation of the small andlarge intestine in immunodeficient mice. Am J Physiol
2006;290:G109–19.311. Shinzaki S, Iijima H, Fujii H, Kuroki E, Tatsunaka N, Inoue T,
et al. Altered oligosaccharide structures reduce colitis inductionin mice defective in b-1,4-galactosyltransferase. Gastroenterology2012;142:1172–82.
312. Yanaba K, Yoshizaki A, Asano Y, Kadono T, Tedder TF, Sato S.IL-10-producing regulatory B10 cells inhibit intestinal injury ina mouse model. Am J Pathol 2011;178:735–43.
313. Schmidt EG, Larsen HL, Kristensen NN, Poulsen SS,Claesson MH, Pedersen AE. B cells exposed to enterobacterialcomponents suppress development of experimental colitis.Inflamm Bowel Dis 2012;18:284–93.
314. Wei B, Velazquez P, Turovskaya O, Spricher K, Aranda R,Kronenberg M, et al. Mesenteric B cells centrally inhibit CD4þT cell colitis through interaction with regulatory T cell subsets.Proc Natl Acad Sci USA 2005;102:2010–5.
315. McPherson M, Wei B, Turovskaya O, Fujiwara D, Brewer S,Braun J. Colitis immunoregulation by CD8þ T cell requires
VI. URINARY TRACT, K
T cell cytotoxicity and B cell peptide antigen presentation. Am J
Physiol Gastrointest Liver Physiol 2008;295:G485–92.316. Moritoki Y, Lian ZX, Lindor K, Tuscano J, Tsuneyama K,
Zhang W, et al. B-cell depletion with anti-CD20 amelioratesautoimmune cholangitis but exacerbates colitis in transforminggrowth factor-beta receptor II dominant negative mice.Hepatology 2009;50:1893–903.
317. Gerth AJ, Lin L, Neurath MF, Glimcher LH, Peng SL. An innatecell-mediated, murine ulcerative-colitis-like syndrome in theabsence of nuclear factor of activated T cells. Gastroenterology2004;126:1115–21.
318. Kirkland D, Benson A, Mirpuri J, Pifer R, Hou B, DeFranco AL,et al. B cell-intrinsic MyD88 signaling prevents the lethaldissemination of commensal bacteria during colonic damage.Immunity 2012;36:228–38.
319. Kobayashi K, Qiao SW, Yoshida M, Baker K, Lencer WI,Blumberg RS. An FcRn-dependent role for anti-flagellinimmunoglobulin G in pathogenesis of colitis in mice. Gastroen-terology 2009;137:1746–56.
320. Hoving JC, Kirstein F, Nieuwenhuizen NE, Fick LC,Hobeika E, Reth M, et al. B cells that produce immunoglobulinE mediate colitis in BALB/c mice. Gastroenterology 2012;142:96–108.
321. Olson TS, Bamias G, Naganuma M, Rivera-Nieves J, Burcin TL,Ross W, et al. Expanded B cell population blocks regulatoryT cells and exacerbates ileitis in a murine model of Crohndisease. J Clin Invest 2004;114:389–98.
322. Gorfu G, Rivera-Nieves J, Hoang S, Abbott DW, Arbenz-Smith K, Azar DW, et al. Beta7 integrin deficiency suppresses Bcell homing and attenuates chronic ileitis in SAMP1/YitFc mice.J Immunol 2010;185:5561–8.
323. Mishima Y, Ishihara S, Aziz MM, Oka A, Kusunoki R, Otani A,et al. Decreased production of interleukin-10 and transforminggrowth factor-beta in Toll-like receptor-activated intestinal Bcells in SAMP1/Yit mice. Immunology 2010;131:473–87.
324. Dohi T, Fujihashi K, Koga T, Shirai Y, Kawamura YI, Ejima C,et al. T helper type-2 cells induce ileal villus atrophy, goblet cellmetaplasia, and wasting disease in T cell-deficient mice.Gastroenterology 2003;124:672–82.
325. Kawamura T, Kanai T, Dohi T, Uraushihara K, Totsuka T,Iiyama R, et al. Ectopic CD40 ligand expression on B cellstriggers intestinal inflammation. J Immunol 2004;172:6388–97.
326. Lindner C,Wahl B, Fohse L, SuerbaumS,MacphersonAJ, Prinz I,et al. Age, microbiota, and T cells shape diverse individual IgArepertoires in the intestine. J Exp Med 2012;209:365–77.
327. Papadakis KA, Rosenbloom B, Targan SR. Anti-CD2O chimericmonoclonal antibody (rituximab) treatment of immune-mediated thrombocytopenia associated with Crohn’s disease.Gastroenterology 2003;124:583.
328. Camoglio L, Juffermans NP, Peppelenbosch M, te Velde AA, tenKate FJ, van Deventer SJ, et al. Contrasting roles of IL-12p40 andIL-12p35 in the development of hapten-induced colitis. Eur JImmunol 2002;32:261–9.
329. Patton DT, Garden OA, Pearce WP, Clough LE, Monk CR,Leung E, et al. The phosphoinositide 3-kinase p110 delta iscritical for the function of CD4þCD25þFoxp3þ regulatoryT cells. J Immunol 2006;177:6598–602.
330. Stefanich EG, Danilenko DM, Wang H, O’Byrne S, Erickson R,Gelzleichter T, et al. A humanized monoclonal antibody tar-geting the b7 integrin selectively blocks intestinal homing of Tlymphocytes. Br J Pharmacol 2009;162:1855–70.
331. Yanaba K, Bouaziz JD, Haas KM, Poe JC, Fujimoto M,Tedder TF. A regulatory B cell subset with a uniqueCD1dhiCD5þ phenotype controls T cell-dependent inflamma-tory responses. Immunity 2008;28:639–50.
IDNEY AND BOWEL
Recommended








![Clinical Trials Glossary - EURORDIS · Animal model [Pharmacology]: An animal with the same or a similar disease in humans. Animal models are used to study the development and progression](https://img.dokumen.tips/doc/110x75/5b5f54e57f8b9a415d8e08bd/clinical-trials-glossary-eurordis-animal-model-pharmacology-an-animal-with.jpg)