
An update on Contraceptionto
the Hillingdon Independent GP Group
18 August 2004
Dr Bela Reed
Family Planning & Reproductive Health Service for Harrow/Hillingdon

The main contraceptive methods in the UKThe main contraceptive methods in the UK•Male condomMale condom•Female condomFemale condom•Diaphragm, caps, spermicidesDiaphragm, caps, spermicides•Natural methodsNatural methods• Combined PillsCombined Pills• Transdermal PatchTransdermal Patch• Vaginal ringVaginal ring• Progestogen only pillsProgestogen only pills•Contraceptive injection(s)Contraceptive injection(s)•Sub-dermal implantSub-dermal implant•Hormonal Emergency Contraception Hormonal Emergency Contraception
Levonelle-2 (Levonelle)Levonelle-2 (Levonelle)•Intra-uterine devicesIntra-uterine devices Intrauterine systems (Mirena)Intrauterine systems (Mirena) Intrauterine implant (GyneFix)Intrauterine implant (GyneFix)•Male and Female sterilisationMale and Female sterilisation

Balancing clinical risks and benefitsBalancing clinical risks and benefits
4 categories of 4 categories of riskrisk (WHO)(WHO):
1.No restriction for use
2.Advantages outweigh risks
3. Risks outweigh advantages
4. Unacceptable health risk

Barrier methods and spermicides
Nonoxynol-9• No evidence that condoms
lubricated with N-9 are more effective in preventing a pregnancy than … silicone. Such condoms should no longer be promoted
• N-9 offers no protection against STI
• N-9 increases the risk of HIV infection when used by women at high risk
• It is better to use a N-9 lubricated condom than no condom at all
WHO 2001

Lactational Amenorrhoea Method (LAM)
The risk of pregnancy is 1% providing …
• Fully or almost fully Fully or almost fully breastfeeding breastfeeding
• AmenorrhoeicAmenorrhoeic• Baby < 6 monthsBaby < 6 months
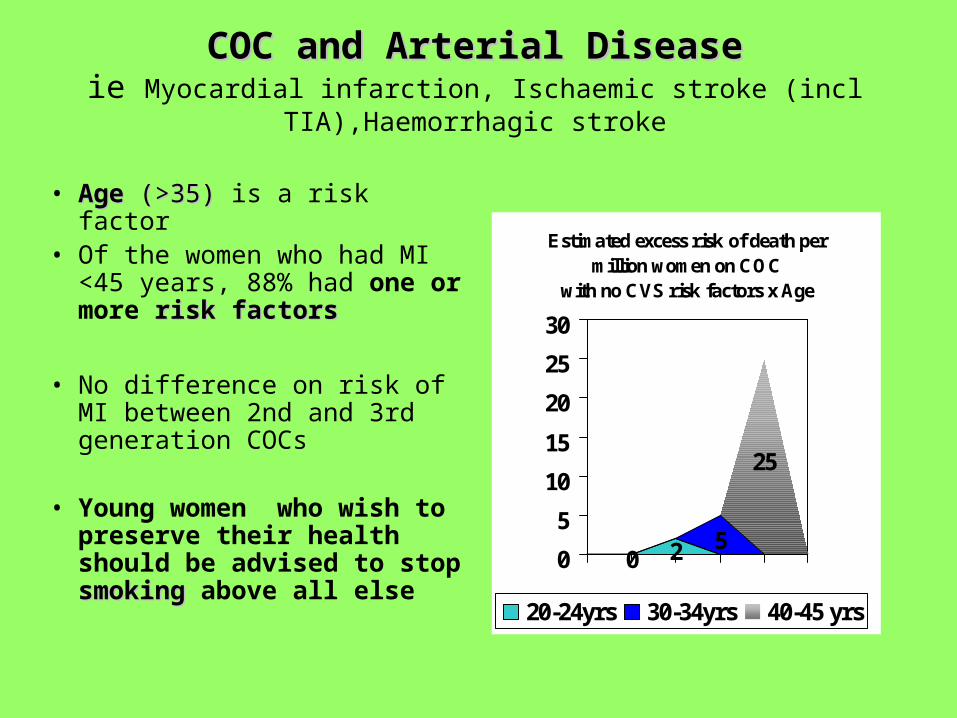
COC and Arterial DiseaseCOC and Arterial Diseaseie Myocardial infarction, Ischaemic stroke (incl TIA),Haemorrhagic stroke
• AgeAge (>35) (>35) is a risk factor• Of the women who had MI
<45 years, 88% had one or more risk factorsrisk factors
• No difference on risk of MI between 2nd and 3rd generation COCs
• Young women who wish to preserve their health should be advised to stop smokingsmoking above all else
Estimated excess risk of death per million women on COC
with no CVS risk factors x Age
0 2 5
25
0
5
10
15
20
25
30
20-24yrs 30-34yrs 40-45 yrs

COC and Cardiovascular disease
• Avoid COC if 2 or more risks apply or if >35 years + 1 risk factor
• Discontinue COC if smoker age >35 years
• Discontinue COC at age 50 years

COC and MigraineRisk of ischaemic stroke
20-25 years – increased 5x
COC contraindicated when
• Migraine with with aura/focal neurological symptoms
• Migraine lasting >72 hours
• Migraine treated with ergot derivatives
• Common migraine but other risk factors for stroke

COC and Migraine
Use COC with caution when
• Migraine or headaches worsening
• First onset of migraine after starting COC
• A history of focal migraine but no recent attacks

COC and VTE• High profile court case
in 2002• Risk of VTE is 25 per
100,000 women per year (cf to 15 with 2nd generation COCs)
• Risk higher in first year of use

COC and VTEGood practice for
prescribing 3rd gen COC
• Screen for risk markers for VTE
• Arrange a thrombophilia screen if first degree relatives had VTE age <45
• Ensure informed consent – that patient aware of this increased risk of VTE
COC and VTERisk markers for VTERisk markers for VTE:• Family history of VTE
age <45 years• BMI > 30 kg/m2
• Severe varicose veins
• Trauma, major surgery, abdominal
or leg surgery, leg in plaster
• Acquired thrombophilia –
chronic disease -anti-phospholipids and lupus factor
• ?long distance travel
• Congenital or valvular heart disease

COC and smoking
• Smoking Smoking in women <35 years<35 years, on COC, increases the risk of CVD from 3.56 to 42.7 per million user years
• SmokingSmoking in women >35 years>35 years, on COC, increases the risk of CVD from 40.4 to 484.6 per million user years
Dunn et al BJFP 1997:23:88-91
• The pill taker who smoked was more likely to suffer a heart attack and more likely to die from it
RCGP studies 1983
COC and obesity• Weight gain on COC due to
– water retention
– Increase in appetite
– Metabolic disturbance
• BMI >30 associated with increase in risk of venous thrombo-embolism and cardio-vascular disease
Avoid COC if other risk markers present
• BMI >39 COC contraindicated

COC and Breast cancerCOC and Breast cancer• Age is most significant risk factor
Breast cancer is rare in women < 40 whether on COCs or notbackground risk increases with age – significant after age 35. The excess risk with users of COC gradually disappear after 10 years
• Duration of use is less important• The possible increase in risk of
breast cancer should be discussed with the user and weighed against the benefits From the meta-analysis of the collaborative group
on hormonal contraceptives in breast cancer. Lancet 1996
• Good practice –discuss breast cancer risks routinely at age 35

The risk of familial breast cancerThe risk of familial breast cancer
• Most women with breast cancer have no positive family history
• Increased risk with a family history– 2 first degree relatives, 13.3%
– 1 first degree relative 5.5%
– Risk grater the younger the affected relative
If women with positive family history do develop breast cancer
- unlikely to get it at a younger age
- does not affect tumour spread nor mortality

COC and Cervical cancer COC and Cervical cancer
• “a causal link between the pill and cervical cancer was likely…increasing risk of cervical cancer and increasing duration of use of OCs”.
• Risk disappears when pill stopped.• taking OCs for up to 5 years – no increase in risk
use OC 5-10 years or more – 3 fold increase use OC >10 years – 4 fold increase of cervical cancer”
The Lancet. March 2002
• “Evidence not sufficiently robust … based on small number of cases
DH March 2002 CEM/CMO/2002/5Further information on www.doh.gov.uk or www.cancerscreening.nhs.uk

Reminder! – Ca Cx is an STI – HPV
– Risk is higher in smokers
– No need to stop COC because of an abnormal smear
– Be scrupulous about cervical cancer screening if used OC >5 years
– Pills are safe and highly effective in preventing pregnancy
What is new/news?What is new/news?
• COCs containing cyproterone acetate (Dianette) have 3.9 times increased relative risk of VTE than on an LNG pill (Microgynon)
(Vasilaakis-Scaramozza C, Jick H. Lancet 2001; 358: 1427-1429)
• Dianette is not licensed as a contraceptive. It is to be used for acne or hirsutism and discontinued 3-4 months after condition has resolved
(CSM/MCA Oct 2002)
Is COC effective for acne?Is COC effective for acne?
• COC usually improves acne.
• Third generation COCs and oestrogen dominant COCs are particularly helpful
• POP and progestogen dominant pills should be avoided
• Dianette is useful but remains a second choice for long term treatment
• ? Yasmin

New COC “Yasmin”30mcg ethinyl oestradiol + 3mg drospirenone
drospirenone –
• “a progestogen resembling natural progesterone”• Anti-mineralocorticoid - prevents sodium retention
– Mean weight below baseline value (2 year data)
– BP both systolic and diastolic lessBP both systolic and diastolic less compared to Marvelon
– Improvement in PMT and PMDD symptomsImprovement in PMT and PMDD symptoms
• Anti-androgenic – Improvement in skin – acne and sebum formation lessImprovement in skin – acne and sebum formation less
– No data on effect on PCO or hirsutism

The contraceptive transdermal patch – Evra®
• Contains ethinyl oestradiol and norelgestromin
• Constant levels of hormones
• Each patch for 7 days effective up to 9 days
• Applied to clean dry skin on buttocks, front/back (not breasts), abdomen, upper arm
• Similar to COC in efficacy, side effects etc

The contraceptive transdermal patch – Evra® ADVANTAGESADVANTAGES
• Better compliance = less failures• ? teenagers• Women who are unable to swallow pills• Gastrointestinal problems• ??? Less VTE (as in HRT studies)
DISADVANTAGESDISADVANTAGES• Local reactionLocal reaction• Patch gets unstuckPatch gets unstuck• ?effectiveness if weight over 90kg?effectiveness if weight over 90kg• Cost Cost (£23.23 for 3 months)
compared to Microgynon 30 at £2.82, Cilest at £6.42

Progestogen only pillsProgestogen only pills• Use in women over 70 Kg (11 stone)?
Possible increase in failure especially in younger women
More effective in older women (>40 effective as COC), breastfeeding women and meticulous pill takers. Use of double dose?? Unlicensed use but consider in women who bleed “regularly” or with nuisance bleeding
• Use in women with PCO?Functional ovarian cysts common (50%) Risk/benefit assessment required in individual cases.
• Increased risk of ectopic pregnancy• Emergency Contraception indicated if pill taking late by >3 hours and UPSI has taken place
from time of missed pill to 48 hours of restarting POP

What is new?CerazetteCerazette - Each tablet
contains 75 mcg desogestrel (metabolised to etonogestrel)
• Inhibits ovulation Efficacy: Pearl index for Cerazette was 0.14 compared to 1.17 for LNG 30 microgram
• Low androgenic activity
• Some ovarian follicular activity present
• Bleeding pattern – early treatment phase (first month) variable bleeding patternlate phase (9-12 months) – bleeding less frequent
• Less dysmenorrhoea• Acne not worse• No weight change • Effective taken up to 12
hours late
“Insufficient evidence that it is more effective than other POPs. Irregular vaginal bleeding similar. ..No compelling reason to use Cerazette instead of a standard POP” DTB Sep 2003

Depo-Provera

Long term DMPALong term DMPA use and effect on bone massuse and effect on bone mass- Review by Olav Meirik IPPF Medical Bulletin 5 Oct 2000
• women in the ‘middle years’women in the ‘middle years’ of reproductive life -effects small and transient. Changes negligible with rapid return to normal
Use DMPAwith caution in• adolescents (<20)adolescents (<20) - process of building up bone mass• perimenopausal yearsperimenopausal years (>45)(>45) - about to lose bone
mass rapidly• women with risk factors for osteoporosisrisk factors for osteoporosis

Risk factors for osteoporosisRisk factors for osteoporosis• genetic - causasians and
asians• Amenorrhoea – athletes,
anorexia• diet - low in calcium or
vitamin D• physical inactivity• smoking• excessive alcohol intake• excess of hormones eg
steroids, thyroid, parathyroid
• lack of oestrogen• BMI <18

IMPLANONA biodegradable single
flexible rod 4cm long x 2mm diameter
Contains 68mg ETONOGESTREL, an active metabolite of desogestrel
Licensed for 3 years – what about women weighing
>70 Kg

Implanon
Release of etonogestrel
60-70ug/day in first 5-6 weeks
35-45ug/day end of year 1
30-40ug/day end of year 2
25-30ug/day end of year 3

Implanon
BenefitsBenefits• reliable long term
contraception• Improvement in
menorrhagia and dysmenorrhoea
• Beneficial effect on acne in 59%
• No adverse effects on bone mass
• No significant effect on lipids, haemostasis or liver function
Adverse side effectsAdverse side effects• Bleeding pattern altered:
Amenorrhoea 20%
Infrequent B-S 26%
Frequent B-S 6%Prolonged BS 12%
• Weight gain of >10% in 21% - no change from reference group
• Hormonal ‘nuisance’ effects eg breast pain, headache, libido decrease, dizziness, nausea
• Other (<2.5%) alopecia,depression,change in libido

How effective is Levonelle-2?How effective is Levonelle-2?
• Overall effectiveness is Overall effectiveness is 85% ie prevents 7 out of 85% ie prevents 7 out of 8 pregnancies8 pregnancies
• Taken within 24hours, it Taken within 24hours, it prevents 95% of prevents 95% of pregnanciespregnancies
• Taken 25-48 hours after Taken 25-48 hours after UPSI, it is 85%UPSI, it is 85%
• Taken 49-72 hours, it is Taken 49-72 hours, it is 58%58%

What are the contraindications?What are the contraindications?
• Pregnancy• previous adverse
reactions• severe liver disease• active pophyria• Current breast cancer
• Certain medical conditions
Special precautionsSpecial precautions• Enzyme inducing medications
Pharmacy
• Under 16
• Gastro-intestinal disease

Levonelle-2Levonelle-2
Does it affect menstruation?Does it affect menstruation?
• Temporary disturbance of menstrual pattern
• menstrual pattern after treatment:
at expected time (57%), a week early (15%) or a week late (15%)
• Any bleeding outside this range should be checked

Levonelle-2Whats new?Whats new?*Change in license – 2 tablets to be taken together asap
within 12 hours and no later than 72 hours after UPSI*Other - FFPRHC Guidance on Emergency Contraception *Other - FFPRHC Guidance on Emergency Contraception
April 2003 – unlicensed useApril 2003 – unlicensed use
• Increase dosage in women taking enzyme inducing drugs – double the first dose
• Interval between tablets can be up to 16 hours• Repeat use in same cycle is safe• Offer L-2 if within 72 hours of UPSI even if referred for
emergency IUD fitted• May be effective up to 5 days after UPSI – small study, IUD better

Levonelle-2Levonelle-2
Advice from the Chief Medical Officer (2002)Advice from the Chief Medical Officer (2002)12 cases of ectopic pregnanciesectopic pregnancies have been reported to the CSM out of a
total of 201 unintended pregnancies
The Committee on Safety of Medicines (CSM) advises• Women should be encouraged to seek treatment as soon as possible
and advised that treatment failure may occur• Women who do not experience a normal period after using Levonelle-
2 should be followed up to exclude pregnancy• The possibility of an ectopic pregnancy should be considered
especially if history of previous ectopic, tubal surgery or PID
NB. High index of suspicion for ectopic pregnancy

Other advice …
• Importance of follow up after 3-4 weeks
• contraceptioncontraception
- interim
- longer term
(starter pack COC)• Risk assessment for
STI

Emergency Contraception -IUD
Indications
• UPSI >72 hours but <120 hours
• UPSI before day 19 of a 28 day cycle
• Multiple episodes UPSI
• Choice as ongoing contraception
• LEI drugs, L-2 contraindicated
Advice• Offer L-2 if <72
hours since UPSI even if IUD to be fitted
• Remove IUD with onset of next menses

INTRA UTERINE CONTRACEPTION
Types of devices:Types of devices:Cu IUDCu IUD
T safe Cu 380AMultiload 375Nova T 380 Flexi-T 300 OtherOtherMultiload Cu 250 Gynefix (IUI)multiload Cu 250 short Mirena

Intra-uterine Contraception
Gyne T 380SGyne T 380S UK gold standard for long
term use in younger women
• Low intra and extra uterine pregnancy rates - Tcu-380A - failure rate 2.2 after 12 years
• Licensed for 8 years use – effective to 10 years
• Discontinued after June 2001

T-Safe CU 380A
• ‘The replacement for Gyne T 380’
• Stem Cu surface area 200sq mm + copper sleeves = total Cu surface area of 380sq mm
• problems with inserting the device into introducer
• Cost 165 euros

Intra-uterine Contraception
MultiloadMultiload• 375 mm2 surface area of
Cu• Useful post-partum and
for repeated expulsion• Low failure rate (2.9)• High rate of removal for
pain and bleeding• Also 250 versions short
and standard

Intra-uterine Contraception
Nova T 380Nova T 380• Increased surface area of
Cu of 380mm2 with silver core
• Effective for 5 years
• Cost £13.50

Intra-uterine Contraception
GyneFix IUI GyneFix IUI - (Belgium 1985)
“frameless and flexible”= less pain and bleeding
Non-biodegradable suture thread 6 Cu tubes (5mmx2.2mm) surface area 330mm2
Special inserting device to anchor knot into fundal myometrium
Suitable for nullips
Expulsion after ToP less than other IUDs
Cost +/- £30

Intra-uterine Contraception
Flexi-T 300Flexi-T 300Size: 2cm wide x 3cmlong
Inserter device 3mm
Surface area of Cu 300mm2
Push in technique
Unplanned pregnancy at end of year three: 2.5
(Pearl index 1.0)
Cost £7.35

Intra-uterine ContraceptionSUMMARYSUMMARY• Devices with surface area
>300mm2 Cu are more effective and reduce ectopic pregnancy rates
• Gyne T 380 is effective for 10 years
• Flexi-T 300 for emergency use only
• After age 40, any IUD may be left in situ till the menopause
CHOICES CHOICES
• T-Safe Cu 380A
• Nova T 380
• Multiload 375
SPECIAL INDICATIONSSPECIAL INDICATIONS
• GyneFix IUI
• Mirena IUS
• Flexi T 300

Intra-uterine ContraceptionIntra-uterine Contraception
ReminderReminder
• InfectionInfection
• Missed pregnancyMissed pregnancy
• Ectopic pregnancy!!Ectopic pregnancy!!
• ExpulsionExpulsion
• perforationperforation

Intra-uterine ContraceptionIntra-uterine ContraceptionLocal Clinical GuidelinesLocal Clinical Guidelines
Sexual historySexual history
RISK MARKERS for RISK MARKERS for ChlamydiaChlamydia
• Age <25 years• New sexual partner in the last 3
months• 2 or more partners in the last 12
months• History of Chlamydia/BV/PID or
NSU in partner
• Symptoms and/or signs of cervicitis/PID

Intra-uterine ContraceptionIntra-uterine ContraceptionLocal Clinical GuidelinesLocal Clinical Guidelines
Chlamydia Screening (contd) Chlamydia Screening (contd)
At high riskAt high risk• Refer for sexual health
screen prior to IUD• In an emergency,i. Take an endocervical swab
ii. prophylactic treatment Azithromycin or Doxycycline
iii. Sexual health screen(7-10 days after insertion)
iv.advise barrier/spermicide
At low riskAt low risk• Routine endocervical swab
for Chlamydia screening
Procedure – Pre-test written information– Inform patient of the result– Treatment and STI screen– Contact tracing

What next?
NEW CHALLENGES
The Male implant

The latest trend in contraception?
Dr Jonathan Healey, West Sussex GP
Recommended

















