-
8/7/2019 Acute Myocardium Infarction
1/24
L/O/G/O
STEMI (ST elevation myocardium infarction) / NSTEMI(Non-ST
elevation myocardium infarction)
Acute Myocardium
Infarction
Acute Myocardium
Infarction
-
8/7/2019 Acute Myocardium Infarction
2/24
Risk factors
Abnormal serum lipids (elevated totalcholesterol, high LDL
cholesterol, low
HDL cholesterol), smoking, HPT/HTN,
family history of premature CAD, age(male > 55, female >
65), male sex, and
DM.
-
8/7/2019 Acute Myocardium Infarction
3/24
Management of STEMI (algorithm)
C l i n i c a l f e a t u r e s ,
E C G + / - b i o c h e m i c a l
m a r k e r s s u g g e s t i v e
o f S T E M I
Rapid examination to exclude
hypotension and acute pulmonaryoedema, ECG monitoring, Aspirin
and
clopidogrel, statin, analgesia, sedation,
others.
ReperfusionTherapy Not for reperfusion therapy e
.g > 12hrs, contraindicated for thrombolysis
but primary PCI not available.
Thrombolysis if
no
contraindication
Primary PCI if
available
-
8/7/2019 Acute Myocardium Infarction
4/24
Management of STEMI (algorithm)
Beta blocker if no contraindication, ACE
inhibitor especially anteriorMI, CCF, EF
-
8/7/2019 Acute Myocardium Infarction
5/24
General Management of AMI
RIB for 2-3/7 in uncomplicated case.
ECG monitoring for at least 48hr.
Oxygen at 2-4 L/min for 2-3 hr &
continue thereafter if SaO2 remains
-
8/7/2019 Acute Myocardium Infarction
6/24
General Management of AMI
Patient with recurrent symptoms after SLGTN and morphine should
be started on
IVGTN.
Sedation with small oral doses ofdiazepam or lorazepam if
necessary.
Diet and bowel care for the first day
afterMI, diet should be liquid or soft,stool softners or mild
laxatives are
routinely given.
Potassium level should be maintained at
4-5 mmol/L.
-
8/7/2019 Acute Myocardium Infarction
7/24
Specific Mx to reduce infarct size
and to improve mortality.
1. Thrombolytic therapy. Administration of fibrinolytic agents
can
achieve early reperfusion in 50-70% of
patients (compared with a spontaneousreperfusion rate of
-
8/7/2019 Acute Myocardium Infarction
8/24
Specific Mx to reduce infarct size
and to improve mortality.
a) All patient fulfilling the following criteriawithout CI
should be given thrombolytic
therapy.
i. Clinical:
Chest pain or chest-pain-equivalent
syndrome consistent with acute MI 12 hr
from symptom onset with:
ii. ECG: 1 mm ST elevation in 2 contiguous limb
leads.
2 mm ST elevation in 2 contiguous
precordial leads.
-
8/7/2019 Acute Myocardium Infarction
9/24
Specific Mx to reduce infarct size
and to improve mortality.
New bundle branch block.
True posteriorMI (tall R wave in V1 with
ST depression; exclude other causes of
tall R wave [ e.g RBBB, RVH, WPWsyndrome]; right ventricular
infarction
[ST elevation V4R])
-
8/7/2019 Acute Myocardium Infarction
10/24
Specific Mx to reduce infarct size
and to improve mortality.
iii. Time from onset of symptom: 12 hr : no significant benefit
except inongoing ischemia manifested by persistent
chest pain and ST elevetion on ECG.
-
8/7/2019 Acute Myocardium Infarction
11/24
-
8/7/2019 Acute Myocardium Infarction
12/24
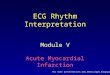
Specific Mx to reduce infarct size
and to improve mortality.
b) Contraindications
i. Absolute CI:
Altered consiousness
Active internal bleeding
Prolonged or traumatic CPR (>10 min)
Known spinal cord or cerebral atriovenous
malformation or tumor.
Recent head trauma
Known previous haemorrhagic
cerebrovascular disease or stroke within
6/12.
-
8/7/2019 Acute Myocardium Infarction
13/24
Specific Mx to reduce infarct size
and to improve mortality.
Intracranial or intraspinal surgery within2/12.
Trauma or surgery within 2/7, which could
result in bleeding in a closed space.
Persistent blood pressure > 200/120 mmHg.
Known bleeding disorder.
Pregnancy.
Suspected aortic dissection.
Previous allergic reaction to streptokinase
or APSAC (or prior use within 1 yr) use
rtPA instead.
-
8/7/2019 Acute Myocardium Infarction
14/24
Specific Mx to reduce infarct size
and to improve mortality.
ii. Relative CI: Chronic uncontrolled HPT/HTN (diastolic
>100 mmHg), treated or untreated.
Ischaemic or embolic stroke in the past (>6month)
Major trauma or surgery > weeks and < 2
month.
Oral anti-coagulation, therapeutic.
Active peptic ulcer disease, or haem-
positive stool.
-
8/7/2019 Acute Myocardium Infarction
15/24
Specific Mx to reduce infarct size
and to improve mortality.
ii. Relative CI: Acute pericarditis, infective endocarditis,
intracardiac thrombus.
Subclavian or intrajugular cannulation.
-
8/7/2019 Acute Myocardium Infarction
16/24
Specific Mx to reduce infarct size
and to improve mortality.
c. Thrombolytic agent: Streptokinase
Recombinant tissue plasminogen activator
(rtPA/Alteplase) Anisoylated plasminogen streptokinase
activator complex (APSAC/Anistreplase)
-
8/7/2019 Acute Myocardium Infarction
17/24
Specific Mx to reduce infarct size
and to improve mortality.
d. Choice of thrombolytic agents. Streptokinase
Recombinant tissue plasminogen activator
(rtPA/Alteplase)e. Monitoring.
Fibrinogen level and PTT should be
monitored 6 hr after the infusion.
Reperfusion is recognized by cessation or
reduction of pain, resolution of ST elevation, or
rapid evolution of ECG to Q waves, reperfusion
arrhythmias, early peak CK (by 12hr)
-
8/7/2019 Acute Myocardium Infarction
18/24
Specific Mx to reduce infarct size
and to improve mortality.
f. Complications of thrombolytic therapy andmanagement.
i. Hypotension during striptokinase infusion.
ii. Allergic reaction to striptokinase.
iii. Uncontrollable bleeding.
iv. Reperfusion arrhythmias.
v. Invasive vascular procedures needed.
-
8/7/2019 Acute Myocardium Infarction
19/24
Specific Mx to reduce infarct size
and to improve mortality.
2. Anti-platlet agents:
Aspirin.
Clopidogrel.
Ticlopidine.
-
8/7/2019 Acute Myocardium Infarction
20/24
Specific Mx to reduce infarct size
and to improve mortality.
3. Beta blockers.
Propanolol.
Atenolol.
4. Nitroglycerin.
5. ACE inhibitors.
6. ARB, angiotensin receptor blocker.
7. Statin therapy.
-
8/7/2019 Acute Myocardium Infarction
21/24
Specific Mx to reduce infarct size
and to improve mortality.
8. Calcium channel blocker.
9. Prophylactic anti-arrhythmics.
10.Anti-coagulants.
11.Primary percutaneous coronary
intervention:
For patients:
i. With CI to thrombolytic therapy.ii. Pressing within 4 hr of a
large anteriorMI.
iii. In whom MI may be due to a vein graft occlusion
iv. With cardiogenic shock.
-
8/7/2019 Acute Myocardium Infarction
22/24
Complications of AMI
1. Cardiac arrhythmias. Ventricular extrasystoles
VT
Vf Af
Sinus Bradycardia
Sinus Tachycardia Various conduction disturbances.
-
8/7/2019 Acute Myocardium Infarction
23/24
Complications of AMI
2. Cardiac failure and cardiogenic shock
3. Thromboembolism.
4. Cardiac rupture.
5. Pericarditis.
6. Post-infarction angina.
7. Left ventricular aneurysm.
8. Other complications.
-
8/7/2019 Acute Myocardium Infarction
24/24
L/O/G/O
Q u e s t i o n a n d A n s w e r S e s s i o n
Finish Anyquestions?
THANK YOU
Finish Anyquestions?
THANK YOU