FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Acute Compartment Acute Compartment SyndromeSyndrome
Dipak RajDipak Raj
Consultant Orthopaedic SurgeonConsultant Orthopaedic Surgeon
Pilgrim Hospital, BostonPilgrim Hospital, Boston

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Definition:An increased pressure within enclosed
osteofascial space that reduces capillary perfusion below level necessary for tissue viability; the underlying mechanism is:
increased volume within space decreased space for contents combination of both

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
HistoryHistory
1881-Volkman 1881-Volkman described contracted state described contracted state believed due to ischemic musclebelieved due to ischemic muscle
1884-Lesser 1884-Lesser developed clinical modeldeveloped clinical model 1888-Peterson 1888-Peterson felt due to nerve compromisefelt due to nerve compromise 1906-Hildebrand 1906-Hildebrand coined “Volkman’s ischemic coined “Volkman’s ischemic
contracture”contracture” 1914-Murphy 1914-Murphy recommended fasciotomy to recommended fasciotomy to
prevent contractureprevent contracture 1940-Griffiths 1940-Griffiths ‘4 Ps’‘4 Ps’ 1966-Seddon 1966-Seddon emphasized lower extremityemphasized lower extremity 1967-Whiteside 1967-Whiteside stressed 4 compartment stressed 4 compartment
fasciotomyfasciotomy

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
DemographicsDemographics
Incidence:Incidence:Men Men 7.3/100,0007.3/100,000WomenWomen 0.7/100,0000.7/100,000
69% due to trauma69% due to trauma36% fx tibia36% fx tibia9.8% distal radius9.8% distal radius23% soft tissue injury without fx23% soft tissue injury without fx
10% on anticoagulants10% on anticoagulantsHigh energy = low energy incidenceHigh energy = low energy incidence

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
EtiologyEtiology
Trauma with bleeding/swellingTrauma with bleeding/swellingBleeding disordersBleeding disordersBurnsBurnsTight wrapsTight wrapsTractionTractionSurgical positioningSurgical positioningPneumatic antishock garmentPneumatic antishock garmentReprefusion swellingReprefusion swelling

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Casting & WrapsCasting & Wraps
Casting increases pressure 3-7 timesCasting increases pressure 3-7 timesPositioning may effect pressurePositioning may effect pressure
Leg best position 0-37° plantar flexionLeg best position 0-37° plantar flexion
Elevation of extremity changes A-V Elevation of extremity changes A-V gradientgradient

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
TractionTraction
Pressure increases linear with increasing Pressure increases linear with increasing weightweightPosterior compartment of leg most effectedPosterior compartment of leg most effected1 kg added weight1 kg added weight
5% increase in posterior compartment5% increase in posterior compartment<2% increase in anterior compartment<2% increase in anterior compartment
Calcaneal traction increases dorsiflexionCalcaneal traction increases dorsiflexion

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
PositioningPositioning
Lithotomy positionLithotomy positionElevation of legElevation of legPressure on posterior compartmentPressure on posterior compartmentCircumferential inflated devicesCircumferential inflated devicesWraps Wraps

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Tibial FracturesTibial Fractures
Don’t use tractionDon’t use tractionBoth reamed & unreamed nails increase Both reamed & unreamed nails increase
pressurepressureLow threshold for prophylactic Low threshold for prophylactic
fasciotomiesfasciotomiesRevascularizationRevascularizationLong procedureLong procedureUnresponsive patientUnresponsive patient

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Pathophysiology:Increased compartment pressure
leadsto increased venous pressure which decreases AV gradient resulting in muscle and nerve ischemia.
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Variables to ConsiderVariables to Consider
Vascular toneVascular toneBlood pressureBlood pressureDuration of elevated pressureDuration of elevated pressureMetabolic demand of tissueMetabolic demand of tissueLowered ischemic threshold of damaged Lowered ischemic threshold of damaged
musclemuscle

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
MyoglobinemiaMyoglobinemia
Released in high levels at reperfusionReleased in high levels at reperfusionToxic to glomeruliToxic to glomeruliMetabolic acidosis & hperkalemiaMetabolic acidosis & hperkalemiaTogether lead to:Together lead to:
Renal failureRenal failureCardiac arrhythmia & failureCardiac arrhythmia & failureHypothermiaHypothermiaShockShock

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
DiagnosisDiagnosis
HistoryHistoryClinical exam:Clinical exam: the Psthe PsCompartment pressuresCompartment pressuresLaboratory testsLaboratory tests
CPKCPKUrine myoglobinUrine myoglobin
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Clinical DiagnosisClinical Diagnosis
The six ‘Ps’:The six ‘Ps’:PressurePressurePainPainParesthesiaParesthesiaParalysisParalysisPallorPallorPulselessnessPulselessness

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
PressurePressure
Early findingEarly findingOnly objective findingOnly objective findingRefers to palpation of compartment and its Refers to palpation of compartment and its
tension or firmness tension or firmness
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
PainPain
Classically out of portion to injuryClassically out of portion to injuryExaggerated with passive stretch of the Exaggerated with passive stretch of the
involved muscles in compartmentinvolved muscles in compartmentEarliest symptom but inconsistentEarliest symptom but inconsistentNot available in obtunded patientNot available in obtunded patient

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
ParesthesiaParesthesia
Also early signAlso early signPeripheral nerve tissue is more sensitive than Peripheral nerve tissue is more sensitive than
muscle to ischemiamuscle to ischemiaPermanent damage may occur in 75 minutesPermanent damage may occur in 75 minutes
Difficult to interpretDifficult to interpretWill progress to anesthesia if pressure not Will progress to anesthesia if pressure not
relievedrelieved

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
ParalysisParalysis
Very late findingVery late finding Irreversible nerve and muscle damage presentIrreversible nerve and muscle damage present
Paresis may be present earlyParesis may be present earlyDifficult to evaluate because of painDifficult to evaluate because of pain

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Pallor & PulselessnessPallor & Pulselessness
Rarely presentRarely present Indicates direct damage to vessels rather Indicates direct damage to vessels rather
than compartment syndromethan compartment syndromeVascular injury may be more of Vascular injury may be more of
contributing factor to syndrome rather than contributing factor to syndrome rather than resultresult
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Compartment PressureCompartment Pressure
When?When? Confirm clinical examConfirm clinical exam Obtunded patient with tight compartmentsObtunded patient with tight compartments Regional anestheticRegional anesthetic Vascular injuryVascular injury
TechniqueTechnique Whiteside infusionWhiteside infusion Stic technique: side port needleStic technique: side port needle Wick catheterWick catheter Slit catheterSlit catheter
*most common technique?*most common technique?

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Whiteside TechniqueWhiteside Technique
Simple techniqueSimple techniqueReadily available suppliesReadily available suppliesWith 18 gauge needle least accurateWith 18 gauge needle least accurateMore accurate if use side port needleMore accurate if use side port needle

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Slit CatheterSlit Catheter
Developed by RorabeckDeveloped by RorabeckConsidered ‘gold standard’Considered ‘gold standard’Need the catheterNeed the catheterCan use the measuring unit for Stic Can use the measuring unit for Stic
systemsystemCan leave indwelling for continuous Can leave indwelling for continuous
monitoringmonitoring
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
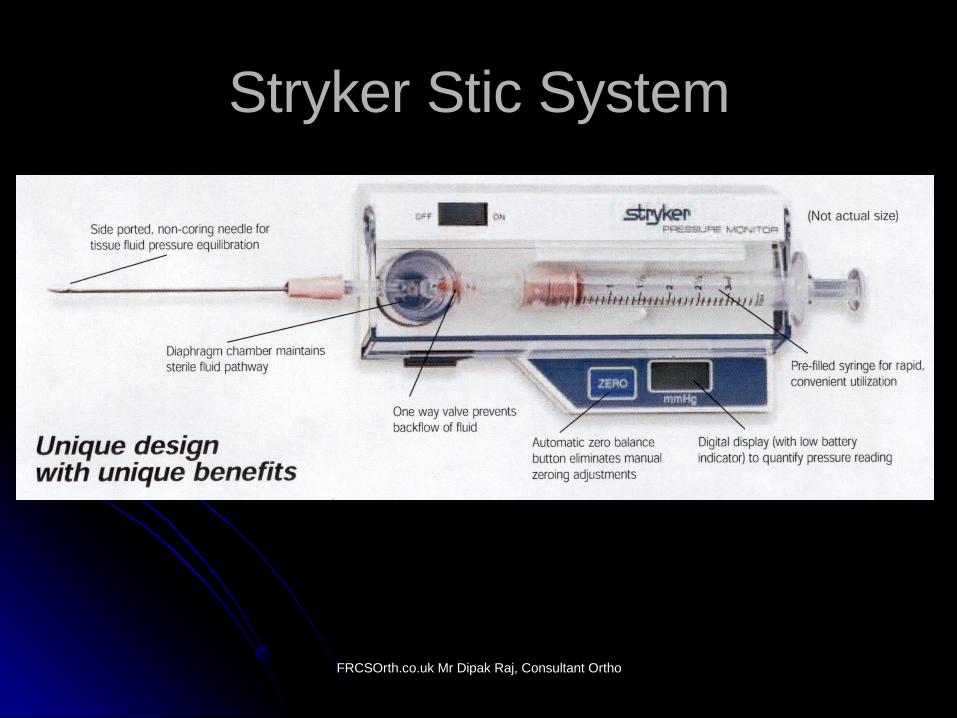
Stryker Stic SystemStryker Stic System
Easy to useEasy to useCan check multiple compartmentsCan check multiple compartmentsDifferent areas in one compartmentDifferent areas in one compartment
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
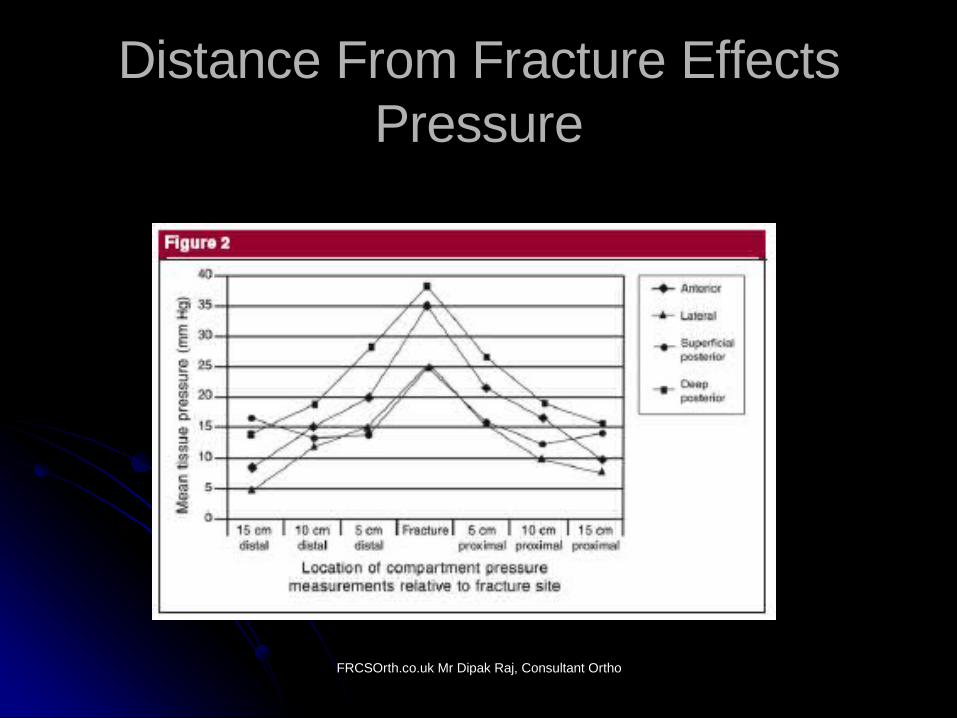
Distance From Fracture Effects Distance From Fracture Effects PressurePressure

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
What is Critical Pressure?What is Critical Pressure?
>30 mm Hg as absolute number >30 mm Hg as absolute number (Roraback)(Roraback)
>45 mm Hg as absolute number (Matsen)>45 mm Hg as absolute number (Matsen)<30 mm Hg for ∆p (where ∆p =diastolic <30 mm Hg for ∆p (where ∆p =diastolic
pressure – compartment pressure, pressure – compartment pressure, McQueen)McQueen)
<40 mm Hg for ∆P (where ∆P mean <40 mm Hg for ∆P (where ∆P mean arterial pressure* – compartment arterial pressure* – compartment pressure, Heppenstall)pressure, Heppenstall)
**mean arterial pressure is diastolic mean arterial pressure is diastolic pressure plus 1/3 of pulse pressurepressure plus 1/3 of pulse pressure

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Decision MakingDecision Making
Fractures in Adults, 5th edition Skeletal Trauma, 3rd edition

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
TreatmentTreatment
Lower leg to level of the heartLower leg to level of the heartRemove castRemove castSplit all dressings down to skinSplit all dressings down to skinFasciotomy if continued clinical findings Fasciotomy if continued clinical findings
and/or elevated compartment pressureand/or elevated compartment pressure

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
CompartmentsCompartments
Most commonMost commonForearmForearmLegLeg
Other compartmentsOther compartmentsHandHandFingerFingerGluteal Gluteal ThighThighFootFoot

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
ForearmForearm
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Leg AnatomyLeg Anatomy

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Leg AnatomyLeg Anatomy
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
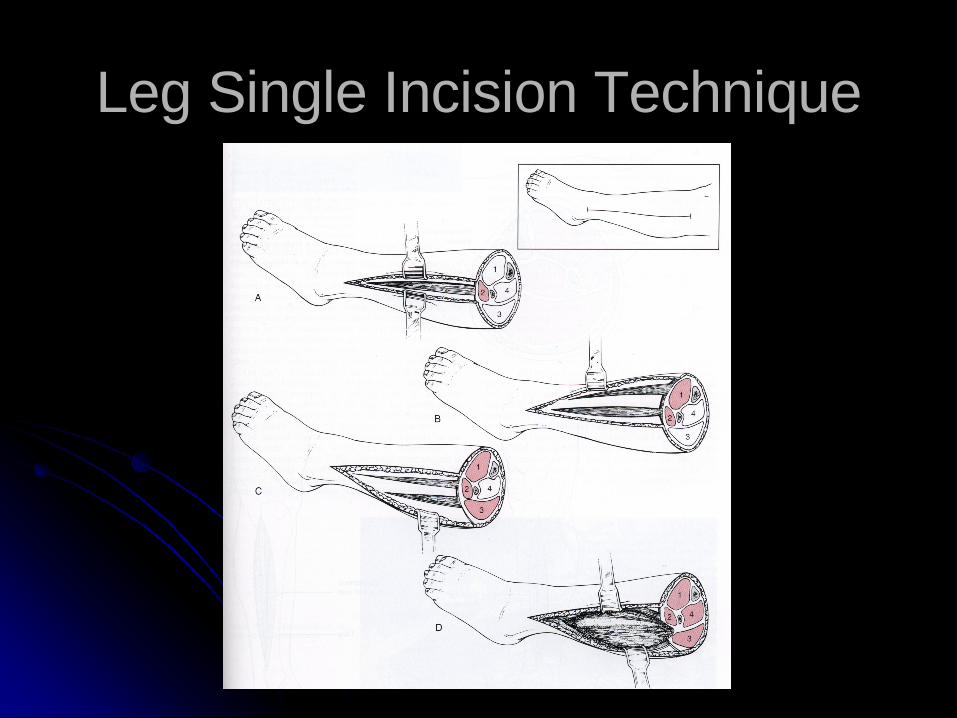
Leg Single Incision TechniqueLeg Single Incision Technique
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
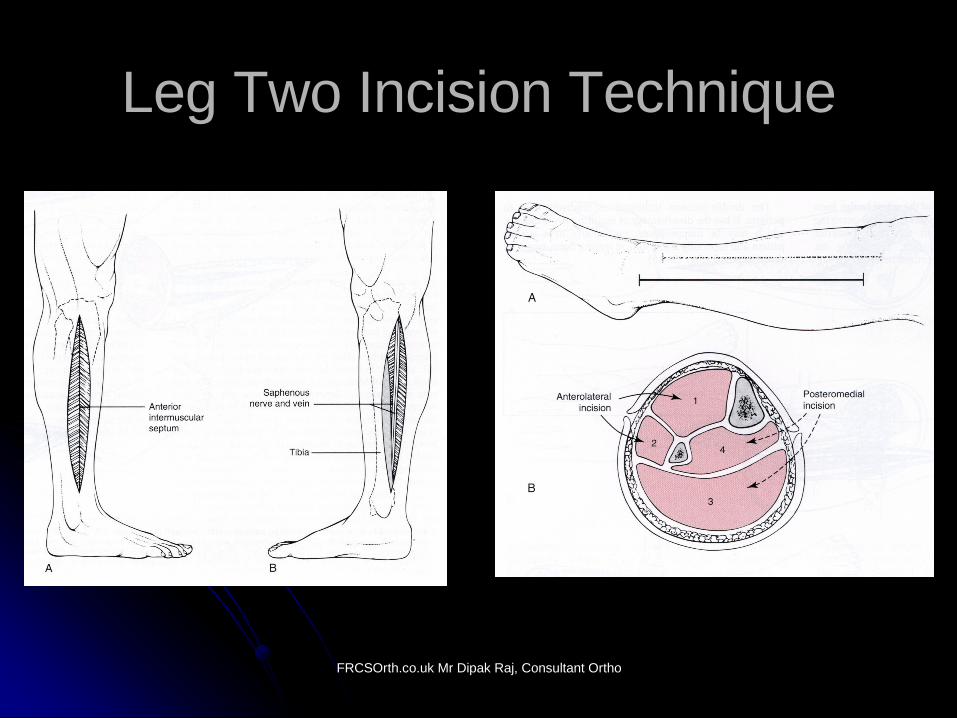
Leg Two Incision TechniqueLeg Two Incision Technique
FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Hand CompartmentsHand Compartments

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Hand CompartmentsHand Compartments

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Foot CompartmentsFoot Compartments

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Foot CompartmentsFoot Compartments

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Wound CareWound Care
Soft tissue coverage by 5-7 daysSoft tissue coverage by 5-7 daysDelayed closureDelayed closure
Vascular loop ‘lace technique’Vascular loop ‘lace technique’
Split thickness skin graftSplit thickness skin graftFlaps or free tissue transferFlaps or free tissue transfer
Although specific clinical parameters reflect an early increased rate of functional recovery in association with computer-assisted minimally invasive total knee arthroplasty within the first postoperative month, the main advantage of this technique over conventional total knee arthroplasty is improved postoperative radiographic alignment without increased short-term complications.

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
ReferencesReferences Acute compartment syndrome WHO IS AT RISK? M. M. McQueen, P. Gaston, C. M. Court-Brown From the Royal Infirmary of Edinburgh, Scotland J Bone J Surg. VOL. 82-B, NO. 2, MARCH 2000.
ACUTE COMPARTMENT SYNDROME IN TIBIAL DIAPHYSEAL FRACTURES. M. M. MCQUEEN, J. CHRISTIE, C. M. COURT-BROWN. J Bone J Surg. VOL. 78-B, NO. 1, JANUARY 1996 95.
COMPARTMENT MONITORING IN TIBIAL FRACTURES. THE PRESSURE THRESHOLD FOR DECOMPRESSION. M. M. MCQUEEN, C. M. COURT-BROWN. J Bone J Surg. .VOL. 78-B, NO. 1, JANUARY 1996

FRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UKFRCSOrth.co.uk Mr Dipak Raj, Consultant Orthopaedic Surgeon, Boston UK
Thank youThank you
FRCSOrth.co.ukFRCSOrth.co.uk
Recommended