Ikuo Hirano, MD, FACG
Ikuo Hirano, MDGastroenterology Division
ACG Midwest Postgraduate Course
Eosinophilic EsophagitisGastroenterology DivisionNorthwestern University Medical School
Management of EoE
• Why should I give my patient with suspected E E i l f PPI h ?EoE a trial of PPI therapy?
• How can I best assess disease activity?• What are the pros and cons of drug and diet
therapies?
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
1

Ikuo Hirano, MD, FACG
Case: Patient MH• 18 yo M with 5 year h/o progressive dysphagia
now occurring on a daily basis with monthly, self limited food impactionslimited food impactions
• One ER visit for food impaction• Denies heartburn, refluxate or chest pain• PMH Allergic rhinitis
Case: Patient MH• EGD 3/07: Furrows, edema, exudates, rings.• Path: Marked eosinophilic infiltrate (77 eos/hpf) with
microabscess in both prox and distal esophagus.
• pH study OFF medications: Distal acid exposure 3 7%
What is the patient’s diagnosis?
• pH study OFF medications: Distal acid exposure 3.7%• Allergy evaluation. SPT reactive to sweet potato, peas,
squash, tomato, corn, chicken, rye, wheat, oat, barley. APT negative to same foods. APT equivocal to milk.
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
2

Ikuo Hirano, MD, FACG
Case: Patient MH
•EGD 6/08 lansoprazole 30 mg BID. No dysphagia.•Rings. No exudates.Rings. No exudates.•Path: 6 eos/hpf
•EGD 1/12 lansoprazole 30 mg QD. No dysphagia. 7 eos/hpf
Case: Patient MH
•EGD 6/08 lansoprazole 30 mg BID. No dysphagia.•Rings. No exudates.Rings. No exudates.•Path: 6 eos/hpf
•EGD 1/12 lansoprazole 30 mg QD. No dysphagia. 7 eos/hpf
Does this patient have EoE or GERD?
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
3

Ikuo Hirano, MD, FACG
GERD vs Eosinophilic Esophagitis (EoE): circa 2005
GERD EoE15
GERD vs Eosinophilic Esophagitis (EoE): circa 2005
GERD EoE15Prospective studies have demonstrated a 33-50% histologic response to PPI therapy
in patients with suspected EoE
Ngo Am J Gastro 2006; Dranove J Pediatric 2009; Sayaj J Pediatr Gastro Nutr 2009; Peterson Dig Dis Sci 2009; Molina-Infante Clin Gastro Hep 2011; Francis Aliment Pharm Ther 2012;
Moawad Am J Gastro 2013; DDW 2013
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
4

Ikuo Hirano, MD, FACG
Can GERD cause or contributeto the pathogenesis of EoE?
GERDEoE
Spechler Am J Gastro 2007; 102:1301-1306
?PPI Response = GERD?
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
5

Ikuo Hirano, MD, FACG
PPI Response = GERDGERD vs PPI responsive EoE?? “PPI responsive esophageal eosinophilia
(PPIREE)”
Why patients with suspected EoE should be given a course of PPI therapy1. It works. Reduces symptoms and esophageal
eosinophilia in 30-50% of patients2. PPIs are safe3. pH testing is cumbersome and subject to
significant false positive and negative results4. Experimental evidence that GERD may
contribute to allergic inflammation in EoE (Paterson
Am J Physiol 1998; Rhijn Brendenoord DDW 2013)y ; j )
5. PPIs may have anti-inflammatory properties beyond acid suppression (Cheng,Souza Gut 2013; DDW13)
6. Recommended in current guidelines. Current clinical trials exclude PPIREE (Gastro 2007, JACI 2011,
Am J Gastro 2013)
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
6

Ikuo Hirano, MD, FACG
Management of EoE
• What do I need to know about PPIREE?• How can I best assess disease activity?• What are the pros and cons of drug and diet
therapies?
EoE Disease Outcomes: More than just counting eosinophilsActivity = Inflammation
Esophagealeosinophilia
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
7

Ikuo Hirano, MD, FACG
Are we just scratching the surface?Do the effects of EoE extend beyond the mucosa?
MuscularisPropria
Normal EoE †
Esophageal Subepithelial FibrosisDemonstrated in majority of EoE patients
Normal EoE †Normal EoE †
Straumann et al., Gastroenterology 2003. Aceves J Allergy Clin Immunol 2007 ‡Chehade J Pediatric Gastro NutrLucendo J Allergy Clin Immunol 2011 †
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
8

Ikuo Hirano, MD, FACG
EoE Disease Activity: More than just counting eosinophils!
Activity = Inflammation + Tissue Remodeling
EsophagealEosinophilia
Esophageal Fibrostenosis
Methods to detect esophageal remodeling in EoE
• Endoscopy• Upper GI radiologic examination• Endoscopic ultrasonography (EUS)• Functional luminal imaging (FLIP)• Pathology- subepithelial fibrosis
Bi k f fib i d• Biomarkers of fibrogenesis and remodeling (EMT, TGF B, MBP etc)
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
9

Ikuo Hirano, MD, FACG
Complications of EoE:Narrow caliber esophagus
Vasilopoulos, Murphy, Auerbach, Massey, Shaker, Stewart, Komorowski, Hogan. Gastro Endosc 2002
Classification and grading of endoscopically detected esophageal features in EoEEoE Endoscopic Reference Score (EREFS)
• Edema (pallor)Edema (pallor)• Rings (“trachealization”)• Exudates (plaques)• Furrows (vertical lines)• Stricture
NORMAL
• Mucosal fragility• Narrow caliber esophagus
Hirano Moy Heckman Thomas Gonsalves Achem. Gut. 2012Research supported by CURED.
EoE
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
10

Ikuo Hirano, MD, FACG
Classification and grading of endoscopically detected esophageal features in EoEEoE Endoscopic Reference Score (EREFS)
• Edema (pallor)Edema (pallor)• Rings (“trachealization”)• Exudates (plaques)• Furrows (vertical lines)• Stricture
NORMALInflammatory
Fibrostenotic• Mucosal fragility• Narrow caliber esophagus
Hirano Moy Heckman Thomas Gonsalves Achem. Gut. 2012Research supported by CURED.
EoE
Fibrostenotic
Normal (Grade 0): Distinct vascular markings
Edema (Also referred to as decreased vascular markings, pallor or edema)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
11

Ikuo Hirano, MD, FACG
Normal (Grade 0): Distinct vascular markings
Edema (Also referred to as decreased vascular markings, pallor or edema)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
Decreased (Grade 1) : Loss of clarity or absence of vascular markings
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
Mild (Grade 1): Subtle circumferential ridges seen on esophageal distension
Rings (Also referred to as esophageal rings, corrugated esophagus or trachealization)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
12

Ikuo Hirano, MD, FACG
Mild (Grade 1): Subtle circumferential ridges seen on esophageal distension
Rings (Also referred to as esophageal rings, corrugated esophagus or trachealization)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
Moderate (Grade 2): Distinct rings that do not occlude passage of diagnostic (8-10 mm) endoscope
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
Mild (Grade 1): Subtle circumferential ridges seen on esophageal distension
Rings (Also referred to as esophageal rings, corrugated esophagus or trachealization)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
Moderate (Grade 2): Distinct rings that do not occlude passage of diagnostic (8-10 mm) endoscope
Severe (Grade 3): Distinct rings that do not permit passage of diagnostic (8-10 mm) endoscope
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
13

Ikuo Hirano, MD, FACG
Mild (Grade 1): White lesions involving < 10% of the surface area of the esophagus
Exudates (Also referred to as white exudates, plaques or punctate white spots)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
Mild (Grade 1): White lesions involving < 10% of the surface area of the esophagus
Exudates (Also referred to as white exudates, plaques or punctate white spots)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
Severe (Grade 2): White lesions involving > 10% of the surface area of the esophagus
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
14

Ikuo Hirano, MD, FACG
Furrows (Also referred to as vertical lines or longitudinal furrowing)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
Stricture (Estimate luminal diameter)
EoE Reference Score for Endoscopic Abnormalities (EoE-EREFs)
EoE Endo Atlas NM-IH ver16. Ref: Hirano, Moy Heckman Gut 2012
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
15

Ikuo Hirano, MD, FACG
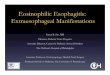
Risk of food impaction correlated with EREFS ring severity score
90
100
n
20
30
40
50
60
70
80%
Foo
d Im
pact
iop<0.05
Nicodeme Clin Gastro Hepatol 2013.
0
10
Ring Score
0 1 2 3
Risk of food impaction correlated with EREFS ring severity score
90
100
n
20
30
40
50
60
70
80
% F
ood
Impa
ctio
p<0.05
EREFS: Allows for uniform characterization Provides information regarding fibrostenosis Complements assessment of therapeutic
0
10
Ring Score
0 1 2 3
Complements assessment of therapeutic outcomes
Nicodeme Clin Gastro Hepatol 2013.
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
16

Ikuo Hirano, MD, FACG
Management of EoE
• What is PPIREE and do I need any?• How can we best assess disease activity?• What are the pros and cons of drug and diet
therapies?
Treatment Options for EoE• Endoscopic Therapy• Medical Therapy
T i l t id– Topical steroids– Systemic steroids– Leukotriene antagonists (montelukast)– Mast cell stabilizers (cromolyn sodium)– Immunomodulators (CRTH2 antagonist, azathioprine)– Biologics (anti IL5, anti IL13, anti TNF, anti IgE)
• Dietary Therapy– Empiric elimination diet– Allergy testing directed elimination diet– Elemental diet
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
17

Ikuo Hirano, MD, FACG
Topical steroids
• Swallowed - not inhaled– Fluticasone 220ug 2-4 puffs BID– Budesonide 0.5-1 mg BID
• Liquid formulations are mixed with substance (sucralose) to increase viscosity
• Patients instructed to fast for 30 minutes after administration
• Mouth rinse after administration to reduce risk thrush may reduce effectiveness
Randomized, Double-Blind Placebo Controlled Trials Budesonide36 Adults with EoE Placebo or budesonide 1 mg BID x 15 days24 Children with EoE: Placebo or budesonide 0.5-1 mg BID x 3 months
Adult Pediatric
4544
noph
ils p
er h
pf
Before After
84
6662 67
80
70
60
50
40
30
90
80
70
60
50
40
30
90
Adult Pediatric
Placebo
Eos
in
Straumann Gastroenterology 2010; 39:1526-1537 Dohil Gastroenterology 2010; 139:418-429
Budesonide PlaceboBudesonide
4 5
30
20
10
0
30
20
10
0
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
18

Ikuo Hirano, MD, FACG
Topical Steroid: Endoscopic Improvement
E1R0E1F1E1R1E2F1
Patient 1 Patient 2 Patient 3E1R2E1F1
Fluticasone
E0R1E0F0 E0R0E0F0 E0R1E0F0
Fluticasone in EoE: What dose?• Konikoff Rothenberg 2006
– 36 Peds; Fluticasone 440 mcg BID x 3 mos vs placebo
– 55% with < 6 eos/hpf • Schaefer Gupta 2008*• Schaefer Gupta 2008
– 80 Peds; RCT fluticasone 220-440 mcg QID vs prednisone x 8 weeks
– 67% with < 6 eos/hpf post fluticasone• Peterson Fang 2009
– 26 Adults; Fluticasone 440 mcg BID vs Esomeprazole x 8 weeks
– 15% with < 5 eos/hpf• Alexander Talley 2012
– 42 Adults; Fluticasone 880 mcg BID x 6 weeks vs placebo42 Adults; Fluticasone 880 mcg BID x 6 weeks vs placebo
– 71% with < 5 eos/hpf• Moawad Wong 2012
– 42 Adults; Fluticasone 440 mcg BID vs esomeprazole x 8 weeks
– 19% with < 7 eos/hpf
*GERD systematically excluded
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
19

Ikuo Hirano, MD, FACG
Eosinophilic Esophagitis:Dietary Treatment
• Elemental diet: Amino acid, carbohydrate, lipid, vitamin/mineral based formula (Kelly Sampson Gastroenterology 1995)
• Directed elimination diet: Exclusion of specific food allergens based on the results of allergy testing (skin prick & patch) (Spergel, Liacouras Ann Allergy Asthma Immunol 2005)
• Non-directed elimination diet: Empiric exclusion of common food allergens (Kagalwalla, Li Clin Gastro Hep 2006)
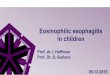
Six Food Elimination Diet (SFED) Prospective Study in Adults (n=50)
6 wk elimination (milk, soy, nuts, eggs, wheat, seafood/shellfish))))
After Diet
Gonsalves, Ritz, Yang, Ditto, Hirano. Gastroenterology 2012
Before Diet
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
20

Ikuo Hirano, MD, FACG
Effect of SFED on Esophageal Eosinophilia
100
Proximal Esophagus Distal Esophagus
30
405060708090
PrePostEos/
hpf
01020
100
Effect of SFED on Esophageal EosinophiliaProximal Esophagus Distal Esophagus
30
405060708090
PrePostEos/
hpf ___ ___* P <0.05
01020
Pre PrePost Post
___ ___* *
Median 34 8 48 13
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
21

Ikuo Hirano, MD, FACG
100
Effect of SFED on Esophageal EosinophiliaProximal Esophagus Distal Esophagus
30
405060708090
PrePostEos/
hpf ___ ___* P <0.0564% achieved histologic response
defined by < 5 eos/hpf
01020
Pre PrePost Post
___ ___* *
Median 34 8 48 13
16
18
Effect of SFED on Dysphagia Score
Pre
4
6
8
10
12
14 Post____
* P <0.01
*2
4
Pre Post
12MedianScore
____
3.5
*
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
22

Ikuo Hirano, MD, FACG
100
Effect of Reintroduction of Foods on Esophageal Eosinophilia
Proximal Esophagus Distal Esophagus
30
405060708090 Pre
Post
Eos/hpf
___ ___
Reintro
01020
Pre Pre
90100
Effect of Reintroduction of Foods on Esophageal Eosinophilia
Proximal Esophagus Distal Esophagus
2030
405060708090 Pre
Post
Eos/hpf
___ ___
Reintro
01020
Pre Pre
___ ___
Post Post
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
23

Ikuo Hirano, MD, FACG
100
Effect of Reintroduction of Foods on Esophageal Eosinophilia
Proximal Esophagus Distal Esophagus
30
405060708090 Pre
Post
Eos/hpf
___ ___
Reintro
___ ___* P <0.01
01020
Pre Pre
___ ___
Post PostReintro Reintro
100
Effect of Reintroduction of Foods on Esophageal Eosinophilia
Proximal Esophagus Distal Esophagus
30
405060708090 Pre
Post
Eos/hpf
___ ___
Reintro
___ ___* P <0.01
Food triggers identified by reintroduction:Wheat (60%), milk(50%), soy (10%), egg (5%)
15% of patients with more than one food trigger
SPT accurately predicted 13% of food triggers
01020
Pre Pre
___ ___
Post PostReintro Reintro
SPT accurately predicted 13% of food triggers.67% of patients with food trigger had negative SPT
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
24

Ikuo Hirano, MD, FACG
Endoscopic improvement with SFED
Pre Diet
E1R1E2F2 E1R0E0F1
Patient 1 Patient 2 Patient 3
E1R0E2F1
Post DietE0R1E1F1 E0R0E0F0 E1R0E0F1
ReintroE1R2E1F1 E1R0E0F1 E1R0E2F1
Empiric Elimination Dietary Treatment for EoE in Adults• Prospective Spanish study of 67 adults with EoE • Diet avoidance of wheat milk egg seafood legumesDiet avoidance of wheat, milk, egg, seafood, legumes,
peanuts, soy, rice, corn for 6 weeks (modified SFED)• Disease remission defined as < 15 eos/hpf• 73% response (48 to 3.5 eos/hpf in responders)• Single food trigger in 36%; 2 foods 31%; 3+ foods 33%• Most common triggers: milk (62%), wheat (29%), egg
(26%), legumes (24%)(26%), legumes (24%)• 2 year follow up in 15 pts. Sustained symptom and
histologic response
Lucendo J Allergy Clin Immunol 2013
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
25

Ikuo Hirano, MD, FACG
Diet therapy in EoE: PROS• No FDA approved medical therapies for EoE
• Many patients would prefer a dietary alternative rather than chronic steroidsrather than chronic steroids
• Conceptual appeal of removing disease trigger rather than suppress inflammatory consequences
• Elimination diets can be a healthy alternative to conventional Western dietsconventional Western diets
• Goal of diet therapy is the identification of specific food trigger(s), not elimination of all potential food groups
Diet therapy in EoE: PROS• No FDA approved medical therapies for EoE
• Many patients would prefer a dietary alternative rather than chronic steroidsrather than chronic steroids
• Conceptual appeal of removing disease trigger rather than suppress inflammatory consequences
• Elimination diets can be a healthy alternative to conventional Western diets
Provides an important proof of concept regarding the role of dietary allergens in
the pathogenesis of EoEconventional Western diets
• Goal of diet therapy is the identification of specific food trigger(s), not elimination of all potential food groups
the pathogenesis of EoE
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
26

Ikuo Hirano, MD, FACG
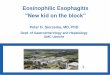
Suggested Algorithm for ManagementOf Eosinophilic Esophagitis
Suspected EoE
PPI x 8 wksSymptom relief &N l hi t l
EGD with Bx
“PPI Responsive Esophageal Eosinophilia” (EoE vs GERD)
Normal histology
EoE
> 15 Eos/hpf
Topical steroidDietary therapy
EGD with BxPersistent Symptoms and Pathology
Elimination diet↑ Dose topicalSystemic steroidBiologic therapy ?
Esophageal dilation
Persistent dysphagiawith stricture
Consider Maintenance Therapy
Symptom relief &Normal histology
• What do I need to know about PPIREE?PPI therapy is a safe and an effective means of recognizing the potential contribution of acid reflux in suspected EoE.
Management of EoE
p p
• How can do I assess disease activity?Symptoms and histology are important but endoscopic findings complement assessment of esophageal remodeling and provides basis for decision for dilation
• What are the pros and cons of drug and diet therapies?Elimination diets are an effective alternative for motivated children and adults
ACG Clinical Guideline: Evidenced Based Approach to the Diagnosis and Management of Esophageal Eosinophilia and Eosinophilic Esophagitis 2013
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
27

Ikuo Hirano, MD, FACG
ACG Regional Postgraduate Course - St. Louis, MO Copyright 2013 American College of Gastroenterology
28
Recommended