-
A Close Look at Therapeutic TouchLinda Rosa, BSN, RN; Emily
Rosa; Larry Sarner; Stephen Barrett, MD
Context.Therapeutic Touch (TT) is a widely used nursing practice
rooted inmysticism but alleged to have a scientific basis.
Practitioners of TT claim to treatmany medical conditions by using
their hands to manipulate a human energy fieldperceptible above the
patients skin.
Objective.To investigate whether TT practitioners can actually
perceive ahuman energy field.
Design.Twenty-one practitioners with TT experience from 1 to 27
years weretested under blinded conditions to determine whether they
could correctly identifywhich of their hands was closest to the
investigators hand. Placement of the inves-tigators hand was
determined by flipping a coin. Fourteen practitioners were tested10
times each, and 7 practitioners were tested 20 times each.
Main Outcome Measure.Practitioners of TT were asked to state
whether theinvestigators unseen hand hovered above their right hand
or their left hand. Toshow the validity of TT theory, the
practitioners should have been able to locate theinvestigators hand
100% of the time. A score of 50% would be expected throughchance
alone.
Results.Practitioners of TT identified the correct hand in only
123 (44%) of 280trials, which is close to what would be expected
for random chance. There was nosignificant correlation between the
practitioners score and length of experience(r=0.23). The
statistical power of this experiment was sufficient to conclude
that ifTT practitioners could reliably detect a human energy field,
the study would havedemonstrated this.
Conclusions.Twenty-one experienced TT practitioners were unable
to detectthe investigators energy field. Their failure to
substantiate TTs most fundamen-tal claim is unrefuted evidence that
the claims of TT are groundless and that furtherprofessional use is
unjustified.
JAMA. 1998;279:1005-1010
THERAPEUTIC TOUCH (TT) is awidely used nursing practice rooted
inmysticism but alleged to have a scientificbasis. Its
practitioners claim to heal orimprove many medical problems
bymanual manipulation of a human energyfield (HEF) perceptible
above the pa-tients skin. They also claim to detect ill-nesses and
stimulate recuperative pow-ersthroughtheir
intentiontoheal.Thera-peutic Touch practice guides1-6 describe
3basic steps, none of which actually re-quires touching the
patients body. Thefirst step is centering, in which the prac-
titionerfocusesonhisorherintenttohelpthe patient. This step
resembles medita-tion and is claimed to benefit the practi-tioner
as well. The second step is assess-ment, in which the practitioners
hands,from a distance of 5 to 10 cm, sweep overthe patients body
from head to feet, at-tuning to the patients condition by be-coming
aware of changes in sensorycues in the hands. The third step is
in-tervention, in which the practitionershands repattern the
patients energyfield by removing congestion, replen-ishing depleted
areas, and smoothing outill-flowing areas. The resultant
energybalance purportedly stems disease andallows the patients body
to heal itself.7
Proponents of TT state that they haveseen it work.8 In a 1995
interview, TTsfounder said, In theory, there should beno limitation
on what healing can be ac-complished.9 Table 1 lists some
claimsmade for TT in published reports.
BACKGROUNDProfessional Recognition
Proponents state that more than100 000 people worldwide have
beentrained in TT technique,38 including atleast 43 000 health care
professionals,2
and that about half of those trained ac-tually practice it.39
Therapeutic Touch istaught in more than 100 colleges and
uni-versities in 75 countries.5 It is said to bethe most recognized
technique used bypractitioners of holistic nursing.40 Con-sidered a
nursing intervention, it is usedbynurses inat least80hospitals
inNorthAmerica,33 often without the permissionor even knowledge of
attending physi-cians.41-43 The policies and proceduresbooks of
some institutions recognizeTT,44 and it is the only treatment for
theenergy-field disturbance diagnosisrecognized by the North
AmericanNursing Diagnosis Association.45 RN,one of the nursing
professions largestperiodicals, has published many
articlesfavorable to TT.46-52
Many professional nursing organiza-tions promote TT. In 1987,
the 50 000-member Order of Nurses of Quebec en-dorsed TT as a bona
fide nursing skill.32The National League for Nursing,
thecredentialing agency for nursing schoolsin the United States,
denies having anofficial stand on TT but has promoted itthrough
books and videotapes,3,53,54 andthe leagues executive director and
a re-cent president are prominent advo-cates.55 The American Nurses
Associa-tion holds TT workshops at its
nationalconventions.Itsofficial journalpublishedthe premier
articles on TT56-59 as well as arecent article designated for
continuingeducation credits.60 The associations im-mediate past
president has written edi-torials defending TT against
criticism.61The American Holistic Nursing
Associa-tionofferscertificationinhealingtouch,a TT variant.62 The
Nurse Healers andProfessional Associates Cooperative,which was
formed to promote TT, claimsabout 1200 members.39
The TT HypothesisTherapeutic Touch was conceived in
theearly1970sbyDoloresKrieger,PhD,RN, a faculty member at New
York Uni-versitys Division of Nursing. Althoughoften presented as a
scientific adapta-tion of laying-on of hands,63-68 TT is im-bued
with metaphysical ideas.
Krieger initially identified TTs activeagent as prana, an
ayurvedic, or tradi-tional Indian, concept of life force.
Shestated,
Health is considered a harmonious relation-ship between the
individual and his total envi-ronment. There is postulated a
continuing in-
From the Questionable Nurse Practices Task Force,National
Council Against Health Fraud Inc (Ms L. Rosa),and the National
Therapeutic Touch Study Group (MrSarner), Loveland, Colo; and
Quackwatch Inc, Allen-town, Pa (Dr Barrett). Ms E. Rosa is a
sixth-gradestudent at Loveland, Colo.
Ms E. Rosa designed and conducted the tests andtabulated her
findings. Mr Sarner did the statisticalanalysis. He and Ms L. Rosa
recruited the test subjects,performed the literature analysis, and
drafted this re-port. Dr Barrett added background material and
editedthe report for publication.
Corresponding author: Stephen Barrett, MD, PO Box1747,
Allentown, PA 18105 (e-mail: [email protected]).
Reprints: Larry Sarner, National Therapeutic TouchStudy Group,
711 W Ninth St, Loveland, CO 80537(e-mail: [email protected]).
JAMA, April 1, 1998Vol 279, No. 13 A Close Look at Therapeutic
TouchRosa et al 1005
1998 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Universidad
de Chile User on 08/16/2014
-
teracting flow of energies from within
theindividualoutward,andfromtheenvironmentto the various levels of
the individual. Healing,it is said, helps to restore this
equilibrium inthe ill person. Disease, within this context,
isconsideredanindicationofadisturbance inthefree flow of the pranic
current.68
Krieger further postulated that thispranic current can be
controlled by thewill of the healer.
When an individual who is healthy touches anill person with the
intent of helping or healinghim, he acts as a transference agent
for theflow of prana from himself to the ill person. Itwas this
added input of prana . . . that helpedthe ill person to overcome
his illness or to feelbetter, more vital.68
Others associate all this with the Chi-nese notion of qi, a life
energy allegedto flow through the human body throughinvisible
meridians. Those inspired bymystical healers of India describe
thisenergy as flowing in and out of sites ofthe body that they call
chakras.
Soon after its conception, TT becamelinked with the westernized
notions ofthe late Martha Rogers, dean of nursingat New York
University. She assertedthat humans do not merely possess en-ergy
fields but are energy fields and con-stantly interact with the
environmentalfield around them. Rogers dubbed herapproach the
Science of Unitary Man,69which later became known as the
moreneutral Science of Unitary Human Be-ings. Her nomenclature
stimulated thepursuit of TT as a scientific practice.Almost all TT
discussion today is based
on Rogers concepts, although Easternmetaphysical terms such as
chakra2,70and yin-yang71 are still used.
The HEF postulated by TT theoristsresemblesthemagnetic
fluidoranimalmagnetism postulated during the 18thcentury by Anton
Mesmer and his follow-ers. Mesmerism held that illnesses arecaused
by obstacles to the free flow of thisfluid and that skilled healers
(sensi-tives) could remove these obstacles bymaking passes with
their hands. Someaspectsofmesmerismwererevivedinthe19th century by
Theosophy, an occult re-ligion that incorporated Eastern
meta-physical concepts and underlies manycurrentNewAgeideas.72
DoraKunz,whois considered TTs codeveloper, waspresident of the
Theosophical Society ofAmerica from 1975 to 1987. She collabo-rated
with Krieger on the early TT stud-ies and claims to be a
fifth-generationsensitive and a gifted healer.20
Therapeutic Touch is set apart frommany other alternative
healing modali-ties, as well as from scientific medicine,by its
emphasis on the healers intention.Whereas the testing of most
therapiesrequires controlling for the placebo ef-fect (often
influenced by the recipientsbelief about efficacy), TT theorists
sug-gest that the placebo effect is irrelevant.According to
Krieger,
Faith on the part of the subject does not makea significant
difference in the healing effect.Rather, the role of faith seems to
be psycho-logical, affecting his acceptance of his illness
orconsequent recovery and what this means tohim. The healer, on the
other hand, must havesome belief system that underlies his actions,
ifone is to attribute rationality to his behavior.65
Thus, the TT hypothesis and the en-tire practice of TT rest on
the idea thatthe patients energy field can be de-tected and
intentionally manipulated bythe therapist. With this in mind,
earlypractitioners concluded that physicalcontact might not be
necessary.13 Thethesis that the HEF extends beyond theskin and can
be influenced from severalcentimeters away from the bodys sur-face
is said to have been tested by JanetQuinn, PhD, and reported in her
1982dissertation.14 However, that studymerely showed no difference
betweengroups of patients who did or did nothave actual contact
during TT. AlthoughQuinns work has never been substanti-ated,
nearly all TT practitioners todayuse only the noncontact form of
TT.
As originally developed by Krieger, TTdid involve touch,
although clothes andother materials interposed between
prac-titioner and patient were not consideredsignificant.56
ItwasnamedTTbecausetheaboriginal term laying-on of hands
wasconsidered an obstacle to acceptance by
curriculum committees and other
insti-tutionalbulwarksoftodayssociety.66
Themysticismhasbeendownplayed,andvari-ous scientific-sounding
mechanisms havebeen proposed. These include the thera-peutic value
of skin-to-skin contact, elec-tron transfer resonance, oxygen
uptakeby hemoglobin, stereochemical similari-ties of hemoglobin and
chlorophyll, elec-trostatic potentials influenced by healerbrain
activity, and unspecified conceptsfrom quantum theory.66,67
Therapeutic Touch is said to be in thevanguard of treatments
that allowhealing to take place, as opposed to thecuring
pejoratively ascribed to main-stream medical practice.
TherapeuticTouch supposedly requires little train-ing beyond
refining an innate ability tofocus ones intent to heal; the
patientsbody then does the rest.5 Nurses whoclaim a unique
professional emphasis oncaring are said to be specially situated
tohelp patients by using TT.56,59 Nonethe-less, proponents also
state that nearlyeveryone has an innate ability to learnTT, even
small children and juvenile de-linquents on parole.2,17,32
Proponents describe the HEF as realand perceptible. Reporting on
a pilotstudy, Krieger claimed that 4 blind-folded men with
transected spinal cordscould tell exactly where the nurseshands
were in their HEFs during theTherapeutic Touch interaction.5 In
or-dinary TT sessions, practitioners gothrough motions that
supposedly inter-act with the patients energy field, in-cluding
flicking excess energy fromtheir fingertips.3
Therapeutic Touch is claimed to haveonly beneficial effects.39
However, someproponents warn against overly lengthysessions or
overtreating certain areas ofthe body. This caution is based on
thenotion that too much energy can be im-parted to a patient,
especially an infant,which could lead to hyperactivity.5,73,74
Literature AnalysisAlthough TT proponents refer to a vo-
luminous and growing body of valid re-search,63,75,76 few
studies have been welldesigned. Some clinical studies,
mostlynursing doctoral dissertations, have re-ported positive
results, principally withheadache relief, relaxation, and
woundhealing.* However, the methods, cred-ibility, and significance
of these studieshave been seriously questioned.41,87-95One
prominent proponent questions thevalidity of the typical placebo
controlused in these studies.96
Twooftheauthors(L.R.andL.S.)haveconducted extensive literature
searchescovering the years 1972 through 1996.
*References 5, 13, 14, 23, 24, 26, 28, 30, 68, 77-86
Table 1.Claims Made for Therapeutic Touch
Calms colicky infants,9 hospitalized infants,10 womenin
childbirth,11 trauma patients,12 and hospitalizedcardiovascular
patients13,14
Promotes bonding between parents and infants15Increases milk let
down in breast-feeding mothers16Helps children make sense of the
world17Protects nurses from burnout18 and effects changes
in their lifestyle19Helps to evaluate situations where diagnosis
is
elusive9Relieves acute pain,20 especially from burns21Relieves
nausea,22,23 diarrhea,5 tension headaches,24
migraine headaches,21 and swelling in edematouslegs and
arthritic joints7
Decreases inflammation25Breaks fever21Remedies thyroid
imbalances5Helps skin grafts to seed9Promotes healing of decubitus
ulcers7Alleviates psychosomatic illnesses5Increases the rate of
healing for wounds, bone and
muscle injuries, and infections26Relieves symptoms of Alzheimer
disease,27 acquired
immunodeficiency syndrome,5 menstruation,28 andpremenstrual
syndrome21
Is an innovative means of social communication29Is effective
with the aged,30,31 asthmatic or autistic
children, stroke patients, and coma patients9Supports people
with multiple sclerosis and Raynaud
disease32Treats measles33 and many different forms of
cancer34Comforts the dying35-37Helps to bring some dead back to
life2
1006 JAMA, April 1, 1998Vol 279, No. 13 A Close Look at
Therapeutic TouchRosa et al
1998 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Universidad
de Chile User on 08/16/2014
-
Using key words such as therapeutictouch, touch therapies, human
energyfield, quackery, and alternative medi-cine, we have searched
MEDLINE, In-dex Medicus, CINAHL,
DissertationAbstracts,MastersAbstracts,ScienceCi-tation Index,
Government PublicationsIndex, Books in Print, National
UnionCatalog, Readers Guide to PeriodicalLiterature, and
Alternative Press Index.Weattemptedtoobtainafull
copyofeachpublication and every additional publica-tion cited in
the ones we subsequentlycollected. During 1997, we continued
tomonitor the journals most likely to con-tain material about
TT.
These methods have enabled us toidentify and obtain 853 reports
(or ab-stracts), of which 609 deal specificallywith TT, 224 mention
it incidentally, and20 discuss TT predecessors. Ninety-seven other
cited items were either non-published or were published in
obscuremedia we could not locate. Only 83 of the853 reports
described clinical research orother investigations by their
authors.Nine of these studies were not quanti-tative. At most, only
1 (the study byQuinn14)ofthe83mayhavedemonstratedindependent
confirmation of any positivestudy.97 (That study was conducted by
acloseassociateoftheoriginalresearcher.)To our knowledge, no
reported study at-tempted to test whether a TT practition-er could
actually detect an HEF.
Of the 74 quantitative studies, 23 wereclearly unsupportive.
Eight reported nostatisticallysignificantresults,16,58,98-103
3ad-mittedtohavinginadequatesamples,22,56,1042 were
inconclusive,11,105 and 6 had nega-tive findings.106-111 Four
attempted inde-pendent replications but failed to sup-port the
original findings.112-115 To ourknowledge, no attempt to conduct
experi-ments to reconcile any of these unsup-portive findings has
been reported.
In 1994, the University of ColoradoHealth Sciences Center
(UCHSC), Den-ver, empaneled a scientific jury in re-sponse to a
challenge to TT in its nursingcurriculum. After surveying
publishedresearch, the panel concluded thatthere is not a
sufficient body of data,both in quality and quantity, to
establishTT as a unique and efficacious healingmodality.116
A few months later, a University ofAlabama at Birmingham
research teamdeclared that their own imminent study(financed by a
$335 000 federal grant)would be the first real scientific evi-dence
for TT.117,118 This project com-pared the effects of TT and sham TT
onthe perception of pain by burn patients.The final report to the
funding agencynoted statistically significant differ-ences in pain
and anxiety in 3 of 7 sub-jective measurements, but there was
no
difference in the amount of pain medica-tion requested.119
With little clinical or quantitative re-search to support the
practice of TT,proponents have shifted to qualitativeresearch,
which merely compiles anec-dotes.120 This approach, which
involvesaskingsubjectswhattheyfeelanddraw-ing conclusions from
their descrip-tions,17,43,121-128 was sharply criticized byUCHSCs
scientific panel.116
Both TT theory and technique requirethatanHEFbefelt
inordertoimpartanytherapeuticbenefittoasubject.Thus,thedefinitivetestofTTisnotaclinical
trialofits alleged therapeutic effects, but a testof whether
practitioners can perceiveHEFs, which they describe, in print andin
our study, with such terms as tingling,pulling, throbbing, hot,
cold, spongy, andtactile as taffy. After doing its own sur-vey, the
UCHSC panel declared that noone had even any ideas about how
suchresearch might be conducted.115 Thisstudy fills that void.
METHODSIn 1996 and 1997, by searching for ad-
vertisements and following other leads,2ofus (L.R.andL.S.)
located25TTprac-titioners in northeastern Colorado, 21 ofwhom
readily agreed to be tested. Ofthose who did not, 1 stated she was
notqualified, 2 gave no reason, and 1 agreedbut canceled on the day
of the test.
The reported practice experience ofthose tested ranged from 1 to
27 years.There were 9 nurses, 7 certified massagetherapists, 2
laypersons, 1 chiropractor, 1medical assistant, and 1 phlebotomist.
Allbut 2 were women, which reflects the sex
ratio of the practitioner population. Onenurse had published an
article on TT in ajournal for nurse practitioners.
There were 2 series of tests. In 1996,15 practitioners were
tested at theirhomes or offices on different days for aperiod of
several months. In 1997, 13practitioners, including 7 from the
firstseries, were tested in a single day.
The test procedures were explainedby 1 of the authors (E.R.),
who designedthe experiment herself. The first seriesof tests was
conducted when she was 9years old. The participants were in-formed
that the study would be pub-lished as her fourth-grade
science-fairproject and gave their consent to betested. The
decision to submit the re-sults toascientific
journalwasmadesev-eral months later, after people whoheard about
the results encouraged pub-lication. The second test series was
doneat the request of a Public BroadcastingService television
producer who hadheard about the first study. Participantsin the
second series were informed thatthe test would be videotaped for
pos-sible broadcast and gave their consent.
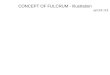
During each test, the practitionersrested their hands, palms up,
on a flatsurface,approximately25to30cmapart.To prevent the
experimenters handsfrom being seen, a tall, opaque screenwith
cutouts at its base was placed overthe subjects arms, and a cloth
towel wasattached to the screen and draped overthem (Figure 1).
Each subject underwent a set of 10trials. Before each set, the
subject waspermitted to center or make any othermental preparations
deemed necessary.
Figure 1.Experimenter hovers hand over one of subjects hands.
Draped towel prevents peeking. Draw-ing by Pat Linse, Skeptics
Society.
JAMA, April 1, 1998Vol 279, No. 13 A Close Look at Therapeutic
TouchRosa et al 1007
1998 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Universidad
de Chile User on 08/16/2014
-
The experimenter flipped a coin to de-termine which of the
subjects handswould be the target. The experimenterthen hovered her
right hand, palm down,8 to 10 cm above the target and said,Okay.
The subject then stated whichof his or her hands was nearer to
theexperimenters hand. Each subject waspermitted to take as much or
as littletime as necessary to make each deter-mination. The time
spent ranged from 7to 19 minutes per set of trials.
To examine whether air movement orbody heat might be detectable
by the ex-perimental subjects, preliminary testswere performed on 7
other subjects whohad no training or belief in TT. Four
werechildren who were unaware of the pur-pose of the test. Those
results indicatedthat the apparatuspreventedtactilecuesfrom
reaching the subject.
The odds of getting 8 of 10 trials cor-rect by chance alone is
45 of 1024 (P=.04),a levelconsideredsignificant inmanyclini-cal
trials. We decided in advance that anindividual would pass by
making 8 ormore correct selections and that thosepassing the test
would be retested, al-though the retest results would not be
in-cluded in the group analysis. Results forthe group as a whole
would not be con-sidered positive unless the average scorewas above
6.7 at a 90% confidence level.
RESULTSInitial Test Results
If HEF perception through TT waspossible, the experimental
subjectsshould have each been able to detect theexperimenters hand
in 10 (100%) of 10trials. Chance alone would produce anaverage
score of 5 (50%).
Before testing, all participants
saidtheycoulduseTTtosignificanttherapeu-tic advantage. Each
described sensorycues they used to assess and manipulatethe HEF.
All participants but 1 certifiedmassage therapist expressed high
confi-
dence in their TT abilities, and even theaforementioned
certified massage thera-pist said afterward that she felt she
hadpassed the test to her own satisfaction.
In the initial trial, the subjects statedthe correct location of
the investigatorshand in 70 (47%) of 150 tries. The numberof
correct choices ranged from 2 to 8.Only 1 subject scored 8, and
that samesubject scored only 6 on the retest.
After each set of trials, the results werediscussed with the
participant. Becauseall but 1 of the trials could have been
con-sidered a failure, the participants usu-ally chose to discuss
possible explana-tions for failure. Their rationalizationsincluded
the following: (1) The experi-menter left a memory of her hand
be-hind, making it increasingly difficult insuccessive trials to
detect the real handfrom the memory. However, the first at-tempts
(7 correct and 8 incorrect) scoredno better than the rest.
Moreover, prac-titioners should be able to tell whether afield they
are sensing is fresh. (2) Theleft hand is the receiver of energy
andthe right hand is the transmitter.Therefore, it can be more
difficult to de-tect the field when it is above the righthand. Of
the 72 tests in which the handwas placed above the subjects right
hand,only 27 (38%) had correct responses. Inaddition, 35 (44%) of
80 incorrect an-swers involved the allegedly more recep-tive left
handconsistent with
random-ness.Moreover,practitionerscustomarilyuse both hands to
assess. (3) Subjectsshould be permitted to identify the
ex-perimenters field before beginning ac-tual trials. Each subject
could be givenan example of the experimenter hover-ing her hand
above each of theirs and toldwhich hand it is. Since the effects of
theHEF are described in unsubtle terms,such a procedure should not
be neces-sary, but including it would remove a pos-sible post hoc
objection. Therefore, we didso in the follow-up testing. (4) The
ex-perimenter should be more proactive,centering herself and/or
attemptingto transmit energy through her own
intentionality. This contradicts the fun-damental premise of TT,
since the ex-perimenters role is analogous to that ofa patient.
Only the practitioners inten-tionality and preparation (centering)
aretheoretically necessary. If not so, theearly experiments (on
relatively unin-volved subjects, such as infants and bar-ley
seeds), cited frequently by TT advo-cates, must also be discounted.
(5) Somesubjects complained that their hands be-came so hot after a
few trials that theywere no longer able to sense the experi-menters
HEF or they experienced dif-ficulty doing so. This explanation
clasheswith TTs basic premise that practition-ers can sense and
manipulate the HEFwith their hands during sessions thattypically
last 20 to 30 minutes. If
practi-tionersbecomeinsensitiveafteronlybrieftesting, the TT
hypothesis is untest-able. Those who made this complaintdid so
after they knew the results, notbefore. Moreover, only 7 of the 15
firsttrials produced correct responses.
Follow-up Test ResultsThe 1997 testing was completed in 1
day and videotaped by a professional filmcrew. Each subject was
allowed to feeltheinvestigatorsenergyfieldandchoosewhich hand the
investigator would usefor testing. Seven subjects chose her
lefthand, and 6 chose her right hand.
Thetestresultsweresimilartothoseofthe first series. The subjects
correctly lo-cated the investigators hand in only 53(41%) of 130
tries. The number of correctanswers ranged from 1 to 7. After
learn-ing of their test scores, one participantsaid he was
distracted by the towel overhishands,anothersaidthatherhandshadbeen
too dry, and several complained thatthe presence of the television
crew hadmade it difficult to concentrate and/oradded to the stress
of the test. However,we do not believe that the situation wasmore
stressful or distracting than the set-tings in which many hospital
nurses prac-ticeTT(eg, intensivecareunits).Figure2shows the
distribution of test results.
Our null hypothesis was that the ex-perimental results would be
due tochance (=5). Our alternative hypoth-esis was that the
subjects would per-form at better than chance levels. The
tstatistic of our data did not exceed theupper critical limit of
the Student t dis-tribution (Table 2). Therefore, the
nullhypothesis cannot be rejected at the .05level of significance
for a 1-tailed test,whichmeansthatoursubjects,withonly123 of 280
correct in the 2 trials, did notperform better than chance.
Our data also showed that if the prac-titioners could reliably
detect an HEF 2of 3 times, then the probability that ei-ther test
missed such an effect would be
Table 2.Statistical Analysis
StatisticalFunction
Initial Test(n = 15)
Follow-up Test(n = 13)
Mean (95%confidenceinterval)
4.67 (3.67-5.67) 4.08 (3.17-4.99)
SD 1.74 1.44a (1-tailed test) .05 .05t statistic 0.7174
2.222Upper critical limit
of Student tdistribution
1.761 1.782
Alternativehypothesis, = 6.67
0.9559 0.9801
Alternativehypothesis, = 7.50
0.999644 0.999953
No.
of S
ubje
cts
0
1
3
2
5
4
7
6
8
0 1 2 3 4 5 6 7 8 9 10No. of Correct Results (Mean = 4.4)
Figure 2.Distribution of test results.
1008 JAMA, April 1, 1998Vol 279, No. 13 A Close Look at
Therapeutic TouchRosa et al
1998 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Universidad
de Chile User on 08/16/2014
-
less than .05. If the practitioners true de-tection rate was 3
of 4, then the probabil-ity that our experiment missed it wouldbe
less than 3 in 10 000. However, if TTtheory is correct,
practitioners should al-ways be able to sense the energy field
oftheir patients. We would also expect ac-curacyto
increasewithexperience.How-ever, there was no significant
correlationbetween the practitioners scoresandthelength of time
they had practiced TT(r=0.23). We conclude on both statisticaland
logical grounds that TT practitionershave no such ability.
COMMENTPractitioners of TT are generally re-
luctant to be tested by people who arenot proponents. In 1996,
the JamesRandi Educational Foundation offered$742 000 to anyone who
could demon-strate an ability to detect an HEF underconditions
similar to those of our study.Although more than 40 000
Americanpractitioners claim to have such an abil-ity, only 1 person
attempted the demon-stration. She failed, and the offer, nowmore
than $1.1 million, has had no fur-ther volunteers despite extensive
re-cruiting efforts.129
We suspect that the present authorswere able to secure the
cooperation of 21practitioners because the person con-ducting the
test was a child who dis-played no skepticism.
CONCLUSIONTherapeutic touch is grounded on the
concept that people have an energy fieldthat is readily
detectable (and modifi-able) by TT practitioners. However,
thisstudy found that 21 experienced practi-tioners, when blinded,
were unable totell which of their hands was in the
ex-perimentersenergyfield.Themeancor-rect score for the 28 sets of
10 tests was4.4, which is close to what would be ex-pected for
random guessing.
To our knowledge, no other objective,quantitative study
involving more thana few TT practitioners has been pub-lished, and
no well-designed study dem-onstrates any health benefit from
TT.These facts, together with our experi-mental findings, suggest
that TT claimsare groundless and that further use
ofTTbyhealthprofessionals isunjustified.
The television program Scientific AmericanFrontiers showed
excerpts from the second testseries on November 19, 1997.
Lisa Feldman Barrett, PhD, Department of Psy-chology, Boston
College, graciously helped with ourstatistical analyses.
References1. Boguslawski M. The use of Therapeutic Touch
innursing. J Continuing Educ Nurs. 1979;10(4):9-15.2. Krieger D.
Therapeutic Touch Inner Workbook.Santa Fe, NM: Bear; 1997:162.
3. Quinn JF. Therapeutic Touch: Healing ThroughHuman Energy
Fields: Theory and Research [vid-eotapes and study guide]. New
York, NY: NationalLeague for Nursing; 1994:42-248542-2487,
42-2493.4. Krieger D. Living the Therapeutic Touch: Heal-ing as a
Lifestyle. New York, NY: Dodd Mead; 1987.5. Krieger D. Accepting
Your Power to Heal: ThePersonal Practice of Therapeutic Touch.
Santa Fe,NM: Bear; 1993.6. Chiappone J. The Light Touch: An Easy
Guide toHands-on Healing. Lake Mary, Fla: Holistic Re-flections;
1989:14.7. Quinn JF, Strelkauskas AJ. Psycho immunologiceffects of
Therapeutic Touch on practitioners andrecently bereaved recipients:
a pilot study. ANSAdv Nurs Sci. 1993;15(4):13-26.8. Jarboux D.
Nurse knows Therapeutic Touchworks. Boulder Sunday Camera. January
2,1994:3E.9. Putnam ZE. Using consciousness to heal. Mas-sage Ther
J. Fall 1995:47-48, 50, 52, 54, 56, 58, 60.10. Leduc E. Therapeutic
Touch. Neonat Network.1987;5(6):46-47.11. Krieger D. Therapeutic
Touch during childbirthpreparation by the Lamaze method and its
relationto marital satisfaction and state anxiety of the mar-ried
couple. In: Krieger D. Living the TherapeuticTouch: Healing as a
Lifestyle. New York, NY: DoddMead; 1987:157-187.12. Glazer S. The
mystery of Therapeutic
Touch.WashingtonPost.December19-26,1995;Healthsec-tion:16-17.13.
Heidt PR. Effect of Therapeutic Touch on anxi-ety level of
hospitalized patients. Nurs Res. 1981;30(1):32-37.14. Quinn JF. An
Investigation of the Effects ofTherapeutic Touch Done Without
Physical Contacton State Anxiety of Hospitalized
CardiovascularPatients [dissertation]. New York: New York
Uni-versity; 1982.15. Thayer MB. Touching with intent: using
Thera-peutic Touch. Pediatr Nurs. 1990;16(1):70-72.16.
MersmannCA.TherapeuticTouchandMilkLetDown in Mothers of Non-nursing
Preterm Infants[dissertation]. New York: New York
University;1993.17. France NEM. The childs perception of the hu-man
energy field using Therapeutic Touch. J Holis-tic Nurs.
1993;11:319-331.18. Meehan MTC. The Science of Unitary HumanBeings
and theory-based practice: TherapeuticTouch. In: Barrett EAM, ed.
Visions of Rogers Sci-ence-Based Nursing. New York, NY:
NationalLeague for Nursing; 1990:67-81. Publication15-2285.19.
Peters PJ. The Lifestyle Changes of SelectedTherapeutic Touch
Practitioners: An Oral History[dissertation]. Minneapolis, Minn:
Walden Univer-sity; 1992.20. Boguslawski M. Therapeutic Touch: a
facilita-tor of pain relief. Top Clin Nurs. 1980;2(1):27-37.21.
SatirF.Healinghands.Olympian.July19,1994.22. Brown PR. The Effects
of Therapeutic Touch onChemotherapy-induced Nausea and Vomiting:
APilot Study [masters thesis]. Reno: University ofNevada; 1981.23.
Sodergren KA. The Effect of Absorption andSocial Closeness on
Responses to Educational andRelaxation Therapies in Patients With
Anticipa-tory Nausea and Vomiting During Cancer Chemo-therapy
[dissertation]. Minneapolis: University ofMinnesota; 1993.24.
DollarCE. EffectsofTherapeuticTouchonPer-ception of Pain and
Physiological MeasurementsFrom Tension Headache in Adults: A Pilot
Study[masters thesis]. Jackson: University of MississippiMedical
Center; 1993.25. Quinn JF. Holding sacred space: the nurseas
healing environment. Holistic Nurs Pract.1992;6(4):26-36.26. Wirth
DP. The effect of non-contact Therapeu-tic Touch on the healing
rate of full thickness dermalwounds. Subtle Energies.
1990;1(1):1-20.27. Woods DL. The Effect of Therapeutic Touch
onDisruptive Behaviors of Individuals With Demen-
tia of the Alzheimer Type [masters thesis]. Seattle:University
of Washington; 1993.28. Misra MM. The Effects of Therapeutic Touch
onMenstruation. [masters thesis]. Long Beach: Cali-fornia State
University; 1993.29. Putnam ZE. The woman behind TherapeuticTouch:
Dolores Krieger, PhD, RN. Massage Ther J.Fall 1995:50, 52.30.
Simington JA, Laing GP. Effects of TherapeuticTouch on anxiety in
the institutionalized elderly.Clin Nurs Res. 1993;2:438-450.31.
Quinn JF. The Seniors Therapeutic Touch Edu-cation Program.
Holistic Nurs Pract. 1992;7(1):32-37.32. Krieger D. Therapeutic
Touch: two decades ofresearch, teaching and clinical practice.
Imprint.1990;37:83, 86-88.33. Fiely D. Field of beams. Columbus
Dispatch.August 20, 1995:1B-2B.34. Calvert R. Dolores Krieger, PhD,
and her Thera-peutic Touch. Massage Magazine. 1994;47:56-60.35.
Mueller Jackson ME. The use of TherapeuticTouch in the nursing care
of the terminally ill per-son. In: Borelli MD, Heidt PR, eds.
TherapeuticTouch: A Book of Readings. New York, NY:Springer;
1981:72-79.36. Brunjes CAF. Therapeutic Touch: a healing
mo-dalitythroughoutlife.TopClinNurs.1983;5(2):72-79.37. Messenger
TC, Roberts KT. The terminally ill:serenity nursing interventions
for hospice clients.J Gerontol Nurs. 1994;20(11):17-22.38. Maxwell
J. Nursings new age? Christianity To-day. 1996;40(3):96-99.39.
KauffoldMP.TT:healingorhokum?debateoverenergy medicine runs hot.
Chicago Tribune Nurs-ing News. November 19, 1995:1.40.
KeeganL.Holisticnursing.JPostAnesthNurs.1989;4(1):17-21.41.
Bullough VL, Bullough B. Therapeutic Touch:why do nurses believe?
Skeptical Inquirer. 1993;17:169-174.42. Dr Quinn studies
Therapeutic Touch. Universityof Colorado School of Nursing News.
May 1989:1.43. Cabico LL. A Phenomenological Study of
theExperiences of Nurses Practicing TherapeuticTouch [masters
thesis]. Buffalo, NY: DYouvilleCollege; 1992.44. Rosa LA. When
magic gets to play science.Rocky Mountain Skeptic.
1993;10(6):10-12.45. Carpenito LJ, ed. Nursing Diagnosis:
Applica-tion to Clinical Practice. 6th ed. Philadelphia,
Pa:Lippincott; 1995:355-358.46. Sandroff R. A skeptics guide to
TherapeuticTouch. RN. 1980;43(1):24-30, 82-83.47. Raucheisen ML.
Therapeutic Touch: maybetheres something to it after all. RN.
1984;47(12):49-51.48. Haddad A. Acute care decisions: ethics in
ac-tion. RN. 1994;57(11):21-22, 24.49. Swackhamer AH. Its time to
broaden our prac-tice. RN. 1995;58(1):49-51.50. Schmidt CM. The
basics of Therapeutic Touch.RN. 1995;58(6):50, 52, 54.51. Ledwith
SP. Therapeutic Touch and mastec-tomy: a case study. RN.
1995;58(7):51-53.52. Keegan L, Cerrato PL. Nurses are
embracingholistic healing. RN. 1996;59(4):59.53. Moccia P, ed. New
Approaches to Theory Devel-opment. New York, NY: National League
for Nurs-ing; 1986;15-1992.54. Barrett EAM, ed. Visions of Rogers
Science-Based Nursing. New York, NY: National Leaguefor Nursing;
1990;15-2285.55. Moccia P. Letter to the editor. Time.
1994;144(24):18.56. Krieger D. Therapeutic Touch: the imprimaturof
nursing. Am J Nurs. 1975;75:784-787.57. Krieger D, Peper E, Ancoli
S. TherapeuticTouch: searching for evidence of physiologicalchange.
Am J Nurs. 1979;79:660-662.58. Macrae JA. Therapeutic Touch in
practice. AmJ Nurs. 1979;79:664-665.59. Quinn JF. One nurses
evolution as a healer. AmJ Nurs. 1979;79:662-664.60. Mackey RB.
Discover the healing power of
JAMA, April 1, 1998Vol 279, No. 13 A Close Look at Therapeutic
TouchRosa et al 1009
1998 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Universidad
de Chile User on 08/16/2014
-
Therapeutic Touch. Am J Nurs. 1995;95(4):27-33.61. Joel LA.
Alternative solutions to health prob-lems. Am J Nurs.
1995;95(7):7.62. Hover-Kramer D. Healing Touch certificateprogram
continues to bring the human dimension tothe nations nurses.
Beginnings. 1992;12(2):3.63. Cowens C, Monte T. A Gift for Healing:
HowYou Can Use Therapeutic Touch. New York, NY:Crown Publishing
Group; 1996.64. Krieger D. The response of in-vivo human
he-moglobin to an active healing therapy by direct lay-ing on of
hands. Human Dimensions. Autumn 1972:12-15.65. Krieger D.
Therapeutic Touch and healing en-ergies fromthe layingonofhands.
JHolisticHealth.1975;1:23-30.66. Krieger D. Therapeutic Touch: an
ancient, butunorthodox nursing intervention. J N Y State NursAssoc.
1975;6(2):6-10.67. Krieger D. Healing by the laying-on of hands asa
facilitator of bio-energetic change: the response ofin-vivo human
hemoglobin. Int J PsychoenergySyst. 1976;1(1):121-129.68. Krieger
D. The relationship of touch, with in-tent to help or to heal, to
subjects in-vivo hemoglo-bin values: a study in personalized
interaction. In:Proceedings of the Ninth ANA Nurses
ResearchConference. New York, NY: American Nurses As-sociation;
1973:39-59.69. Rogers ME. An Introduction to the TheoreticalBasis
of Nursing. Philadelphia, Pa: Davis; 1970.70. Karagulla S, Kunz D.
The Chakras and the Hu-man Energy Field: Correlations Between
MedicalScience & Clairvoyant Observation. Wheaton,
Ill:Theosophical Publishing House; 1989.71. Randolph GL. The yin
and yang of clinical prac-tice. Top Clin Nurs. 1979;1(1):31-42.72.
BriertonTD.EmployersNewAgetrainingpro-grams fail to alter the
consciousness of the EEOC.Lab Law J. 1992;43:411-420.73. Emery CE.
Therapeutic Touch: healing tech-nique or New Age rite? Providence
Sun Journal-Bulletin. November 27, 1994:A1, A24.74. Knaster M.
Dolores Kriegers TherapeuticTouch. East/West. 1989;19(8):54-57, 59,
79-80.75. Colorado State Board of Nursing. Subcommit-tee to
Investigate the Awarding of Continuing Edu-cation Units to Nurses
for the Study of TherapeuticTouch and Other Non-traditional and
Complemen-tary Healing Modalities. Recommendations. Den-ver:
Colorado State Board of Nursing; 1992.76. Mulloney SS,
Wells-Federman C. TherapeuticTouch: a healing modality. J
Cardiovascul Nurs.1996;10(3):27-49.77. Brown CC, Fischer R, Wagman
AMI, HorromN, Marks P. The EEG in meditation and Therapeu-tic Touch
healing. J Altered States Conscious. 1977;3:169-180.78. Quinn JF.
Therapeutic Touch as energy ex-change: testing the theory. Adv Nurs
Sci. 1984;6(1):42-49.79. Guerrero MA. The Effects of Therapeutic
Touchon State-Trait Anxiety Level of Oncology Patients[masters
thesis]. Galveston: University of Texas;1985.80. Keller EAK, Bzdek
VM. Effects of TherapeuticTouch on tension headache pain. Nurs Res.
1986;35(2):101-106.81. Meehan MTC. Theory development. In:
BarrettEAM, ed. Visions of Rogers Science-Based Nurs-ing. New York,
NY: National League for Nursing;1990;15-2285:197-207.82. Kramer NA.
Comparison of Therapeutic Touchand Casual Touch in stress reduction
of hospitalizedchildren. Pediatr Nurs. 1990;16:483-485.83. Shuzman
E. The Effect of Trait Anxiety andPatient Expectation of
Therapeutic Touch on theReduction in State Anxiety in Preoperative
Pa-tients Who Receive Therapeutic Touch [disserta-tion]. New York:
New York University; 1993.
84. Sies MM. An Exploratory Study of RelaxationResponse
inNursesWhoUtilizeTherapeuticTouch[masters
thesis].EastLansing:MichiganStateUni-versity; 1993.85. Wirth DP,
Richardson JT, Eidelman WS,OMalley AC. Full thickness dermal wounds
treatedwith Therapeutic Touch: a replication and exten-sion.
Complementary Ther Med. 1993;1:127-132.86. Gagne D, Toye RC. The
effects of TherapeuticTouch and relaxation therapy in reducing
anxiety.Arch Psych Nurs. 1994;8:184-189.87. Schlotfeldt RM.
Critique of: Krieger D. The re-lationship of touch, with intent to
help or heal, tosubjects in-vivo hemoglobin values: a study in
per-sonalized interaction. In: Proceedings of the NinthANA Nurses
Research Conference. New York, NY:American Nurses Association;
1973:59-65.88. Walike BC, Bruno P, Donaldson S, et al. . .
.[A]ttempts to embellish a totally unscientific pro-cess with the
aura of science. . . . Am J Nurs. 1975;75:1275, 1278, 1292.89.
Levine ME. The science is spurious. . . . Am JNurs.
1979;79:1379-1380.90. ClarkPE,ClarkMJ.TherapeuticTouch: is therea
scientific basis for the practice? Nurs Res. 1984;33(1):38-41.91.
Meehan MTC. Therapeutic Touch. In:
BulechekGM,McCloskeyJC,eds.NursingInterventions:Es-sential Nursing
Treatments. 2nd ed. Philadelphia,Pa: Saunders; 1992:201-212.92.
Fish S. Therapeutic Touch: can we trust thedata? J Christian Nurs.
1993;10(3):6-8.93. Meehan MTC. Therapeutic Touch and postop-erative
pain: a Rogerian research study. Nurs Sci Q1993;6(2):69-78.94.
Bandman EL, Bandman B. Critical Thinking inNursing. Norwalk, Conn:
Appleton & Lange; 1995.95. Meehan MTC. Quackery and
pseudo-science.Am J Nurs. 1995;75(7):17.96. Meehan MTC. . . . And
still more on TT. ResNurs Health. 1995;18:471-472.97. Rosa LA.
Survey of Therapeutic Touch
Re-search.Loveland,Colo:FrontRangeSkeptics;1996.98. Tharnstrom CAL.
The Effects of Non-contactTherapeutic Touch on the Parasympathetic
Ner-vousSystemasEvidencedbySuperficialSkinTem-peratureandPerceivedStress
[masters thesis].SanJose, Calif: San Jose State University;
1993.99. Parkes BS. Therapeutic Touch as an Interven-tion to Reduce
Anxiety in Elderly Hospitalized Pa-tients [dissertation]. Austin:
University of Texas;1985.100. Mueller Hinze ML. The Effects of
TherapeuticTouch and Acupressure on Experimentally-In-duced Pain
[dissertation]. Austin: University ofTexas; 1988.101. Bowers DP.
The Effects of Therapeutic Touchon State Anxiety and Physiological
Measurementsin Preoperative Clients [masters thesis]. San
Jose,Calif: San Jose State University, 1992.102. Olson M, Sneed NV.
Anxiety and TherapeuticTouch. Issues Ment Health Nurs.
1995;16:97-108.103. Fedoruk RB. Transfer of the Relaxation
Re-sponse: Therapeutic Touch as a Method for Reduc-tion of Stress
in Premature Neonates [dissertation].Baltimore: University of
Maryland; 1984.104. Hogg PK. The Effects of Acupressure on
thePsychological and Physiological Rehabilitation ofthe Stroke
Patient [dissertation]. Alameda: Califor-nia School of Professional
Psychology; 1985.105. Snyder M, Egan EC, Burns KR. Interventionsfor
decreasing agitation behaviors in persons withdementia. J Gerontol
Nurs. 1995;21(7):34-40, 54-55.106. Schweitzer SF. The Effects of
TherapeuticTouch on Short-term Memory Recall in the
AgingPopulation: A Pilot Study [masters thesis]. Reno:University of
Nevada; 1980.107. Randolph GL. Therapeutic and physical
touch:physiological response to stressful stimuli. NursRes.
1984;33(1):33-36.
108. Nodine JL. The Effects of Therapeutic
TouchonAnxietyandWell-beinginThirdTrimesterPreg-nant Women [masters
thesis]. Tucson: Universityof Arizona; 1987.109. Post NW. The
Effects of Therapeutic Touch onMuscle Tone [masters thesis]. San
Jose, Calif: SanJose State University; 1990.110. Straneva JAE.
Therapeutic Touch and InVitro Erythropoiesis [dissertation].
Bloomington:Indiana University; 1992.111. Bush AM, Geist CR.
Testing electromagneticexplanations for a possible psychokinetic
effect ofTherapeutic Touch in germinating corn seed. Psy-cholog
Rep. 1992;70:891-896.112. Edge H. The effect of laying on of
handson an enzyme: an attempted replication. Paper pre-sented at:
22nd Annual Convention of the Parapsy-chology Association; August
15-18, 1979; Moraga,Calif.113. MeehanMTC.
TheEffectofTherapeuticTouchon the Experience of Acute Pain in
PostoperativePatients [dissertation]. New York: New York
Uni-versity; 1985.114. Hale EH. A Study of the Relationship
BetweenTherapeutic Touch and the Anxiety Levels of Hos-pitalized
Adults [dissertation]. Denton: TexasWomens University; 1986.115.
Quinn JF. Therapeutic Touch as energy ex-change: replication and
extension. Nurs Sci Q. 1989;2(2):79-87.116. Claman HN, Freeman R,
Quissel D, et al. Re-port of the Chancellors Committee on
TherapeuticTouch. Denver: University of Colorado Health Sci-ences
Center; 1994.117.
ButgereitB.TherapeuticTouch:UABtostudycontroversial
treatmentforPentagon.BirminghamNews. November 17, 1994:1A, 10A.118.
Turner JG. Tri-Service Nursing ResearchGrant Proposal [revised
abstract]. 1994. Grant No.MDA905-94-Z-0080.119. Turner JG. The
Effect of Therapeutic Touch onPain & Anxiety in Burn Patients
[grant final re-port]. Tri-Service Nursing Research Program;
No-vember 14, 1996. Grant No. N94020.120. Lionberger HJ.
Therapeutic Touch: a healingmodality or a caring strategy. In:
Chinn PL, ed.Nursing Research Methodology: Issues and
Imple-mentation. Rockville, Md: Aspen Publishers; 1986:169-180.121.
Lionberger HJ. An Interpretive Study ofNurses Practice of
Therapeutic Touch [disserta-tion]. San Francisco: University of
California; 1985.122. Polk SH. Clients Perceptions of
ExperiencesFollowing the Intervention Modality of Therapeu-tic
Touch [masters thesis]. Tempe: Arizona StateUniversity; 1985.123.
Hamilton-Wyatt GK. Therapeutic Touch: Pro-moting and Assessing
Conceptual Change AmongHealthCareProfessionals
[dissertation].EastLan-sing: Michigan State University, 1988.124.
Heidt PR. Openness: a qualitative analysis ofnurses and patients
experiences of TherapeuticTouch. Image J Nurs Sch.
1990;22:180-186.125. Thomas-Beckett JG. Attitudes Toward
Thera-peutic Touch: A Pilot Study of Women With BreastCancer
[masters thesis]. East Lansing: MichiganState University; 1991.126.
Clark AJ, Seifert P. Client perceptions ofTherapeutic Touch. Paper
presented at: Third An-nual West Alabama Conference on Clinical
NursingResearch; 1992.127. Samarel N. The experience of receiving
Thera-peutic Touch. J Adv Nurs. 1992;17:651-657.128. Hughes PP. The
Experience of TherapeuticTouch as a Treatment Modality With
AdolescentPsychiatric Patients [masters thesis]. Albuquer-que:
University of New Mexico; 1994.129. James Randi Educational
Foundation. Avail-able at: http://www.randi.org. Accessed March
15,1997.
1010 JAMA, April 1, 1998Vol 279, No. 13 A Close Look at
Therapeutic TouchRosa et al
1998 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Universidad
de Chile User on 08/16/2014