-
8/13/2019 yufi nakal
1/13www.thelancet.com/oncology Vol 13 March 2012 e103
Review
Lancet Oncol2012; 13: e10315
Department of Gynaecological
Surgery (Prof P Morice MD,
C Uzan MD, S Gouy MD),
Department of Pathology
(P Duvillard MD), and INSERM
U 10-30 (Prof P Morice, C Uzan),
Institut Gustave Roussy,
Villejuif, France;Universit
Paris-Sud, Le Kremlin Bictre,
France (Prof P Morice);
Department of Obstetrics andGynaecology, CHU Amiensand
INSERM ERI-12, Universit de
Picardie Jules Vernes, Amiens,
France (R Fauvet MD); and
Department of Obstetrics and
Gynaecology, Hpital Tenon,
INSERM UMRS 938, and
Universit Pierre et Marie Curie,
Paris, France(Prof E Darai MD)
Correspondence to:
Prof P Morice, Department of
Gynaecological Surgery, Institut
Gustave Roussy, 114 rue Edouard
Vaillant, 94805 Villejuif Cedex,
France
[email protected]
Borderline ovarian tumour: pathological diagnostic dilemma
and risk factors for invasive or lethal recurrencePhilippe
Morice, Catherine Uzan, Raffaele Fauvet, Sebastien Gouy, Pierre
Duvillard, Emile Darai
By comparison with ovarian carcinomas, borderline ovarian
tumours are characterised clinically by superior overallsurvival,
even in women with peritoneal spread. In this Review, we aimed to
clarify the histological and clinical factorspotentially defining a
high-risk group in whom disease is likely to evolve to invasive
disease. Invasive peritoneal implants(in serous borderline ovarian
tumours) and residual disease after surgery were the two factors
clearly identified. Otherfactors are controversial owing to
increased risk of invasive recurrence: micropapillary patterns in
serous borderlineovarian tumour, intraepithelial carcinoma in
mucinous lesions, stromal microinvasion in serous lesions, and use
ofcystectomy in mucinous borderline ovarian tumours. The
pathologist has a pivotal role in assessment of the
borderlinenature of ovarian tumours and in identification of
high-risk criteria, most of which are histological. But,
reproducibilityof the histological interpretation of some of these
potential criteriaeg, classification of peritoneal implants
(particularly
in desmoplastic subtype), stromal microinvasion, micropapillary
patterns, and intraepithelial carcinoma in mucinousborderline
ovarian tumoursremains unclear, and should be investigated.
IntroductionBorderline ovarian tumours differ from ovarian
carcinomaby absence of stromal invasion. Classifications for
theselesions have been modified extensively over past
decades.Borderline ovarian tumours were reported initially in1929
as semi-malignant disease. In 1961 and 1971, theInternational
Federation of Gynecology and Obstetrics(FIGO) proposed the term low
malignant potential. In1973, FIGO and WHO suggested creation of a
group oftumours with morphological criteria (in particular,
absence
of stromal invasion), which differentiated them fromcarcinoma.
In this same year, WHO adopted the synonymborderline, which is
still used in the current (2003)classification.1 WHO thereafter
defined extra-ovarianperitoneal disease as implants (and not
metastases)because of their indolent nature. In 1988, Bell
andcolleagues2proposed classification of peritoneal
implants(invasive vs non-invasive lesions) according to
theirmorphological features.
The most frequent borderline ovarian tumours areserous lesions,
representing two-thirds to three-quarters ofthese tumours.3However,
in a Danish register-based cohortstudy, mucinous tumours
represented 50% of borderlineovarian tumours and serous tumours
comprised 44%.4
The ratio in Asia is different, with an equivalent or higherrate
of mucinous borderline ovarian tumours.5
The true incidence of borderline ovarian tumoursremains unknown.
1520% of serous tumours are judgedborderline.6 Data from the SEER
(surveillanceepidemiology and end results) programme showed
anincidence of 25 per 100 000 women-years in the USA.7Compared with
carcinoma, borderline ovarian tumour ischaracterised clinically by
a younger age at diagnosis(10 years earlier) and better overall
survival, even withperitoneal spread. 5-year and 10-year survival
rates forstage I, II, and III disease are 99% and 97%, 98% and90%,
and 96% and 88%, respectively.8 Despite thesefavourable data, some
patients relapse or succumb todisease.
Borderline ovarian tumours can be unilateral or
bilateral.Similar to carcinoma, they can spread to the
peritoneumand, eventually, to lymph nodes. High-risk
borderlineovarian tumour has not been defined by
consensus,therefore, identification of risk factors for
invasiverecurrence or disease-related death is pivotal.
In this Review we aimed to analyse prognostic factors
forinvasive recurrence and death from disease for serous
andmucinous borderline ovarian tumours. We have notincluded rare
entities such as endometrioid, Brenner, orclear-cell borderline
ovarian tumours because of their verylow incidence (
-
8/13/2019 yufi nakal
2/13
e104 www.thelancet.com/oncology Vol 13 March 2012
Review
serous borderline ovarian tumours devoid of micro-
papillary patterns (now designated atypical proliferativeserous
tumours), non-invasive micropapillary low-gradeserous carcinoma,
invasive low-grade serous carcinoma(invasive micropapillary serous
carcinoma), and high-grade serous carcinoma. The overriding issue
was toascertain whether patients with serous borderlineovarian
tumours with micropapillary patterns should beincluded in a high
risk-group and their disease bedeemed low-grade carcinoma.
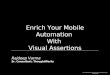
Molecular data seem toconfirm this viewpoint.18,21 May and
co-workers18compared RNA from epithelial cells of serous
borderlineovarian tumours, serous lesions with
micropapillarypatterns, and invasive low-grade serous carcinoma
andnoted that the gene-expression profile of serous lesions
with micropapillary patterns was similar to that ofinvasive
low-grade serous carcinoma but distinct fromthat of serous
borderline ovarian tumours, with candidategenes implicated in the
MAPK pathway. These datareinforce the notion that invasive
low-grade serouscarcinoma develops in a stepwise fashion from
benigncystadenofibroma to classic invasive low-grade
serouscarcinoma via transformations to serous borderlineovarian
tumour (or, atypical proliferative seroustumours)22 and serous
lesions with micropapillarypattern (figure 2).18
Findings suggest that epithelium from the fallopiantube could
become implanted on the ovary, initiatinghigh-grade serous
tumours.28In patients with low-gradeserous disease, mutations in
KRAS, BRAF, andoccasionally HER2 and PIK3CAhave been
characterised.TP53 mutations are rare in this subgroup and
areencountered more frequently in individuals with high-grade
disease.28
Peritoneal implants
The outlook for patients with serous borderline ovariantumours
and peritoneal disease is better than for womenwith ovarian
carcinoma and peritoneal spread. Therefore,peritoneal disease from
borderline ovarian tumours isreferred to as implants and not
metastases. Suggestionsabout pathogenesis of implants include
implantation ofcells detached from the ovarian surface (which
accordswith the high frequency of implants in case of
exophyticvegetations) and formation of implants independently
ofovarian tumours.25 Molecular data lend support toarguments for
both theories but, to date, none of thempredominates.25
Implants can be non-invasive (nearly 85% of implants)or
invasive.29Non-invasive implants are defined as a serous-
type epithelial proliferation that affects peritoneal
surfacesand shows no invasion.2,26 Non-invasive implants
aredesmoplastic or epithelial, and prognosis of these twosubtypes
is similar. However, recognition of potentialinvasion of underlying
tissue is more complex in thedesmoplastic than in the epithelial
subtype.2,6 Invasiveimplants are defined as a serous-type
epithelial pro-liferation affecting peritoneal surfaces and
invadingadjacent or underlying tissue.2,6Morphologically, aspects
ofthese invasive implants are similar to those of invasive
low-grade serous carcinoma, but we should remember that
thediagnosis of borderline ovarian tumour is based on
ovarianhistological features.
The pathologist must harvest suffi cient tissue to be ableto
discriminate non-invasive from invasive implants, byassessment of
the junction between implants and adjacentnormal tissue.27However,
Bell and colleagues29report that25% of implant biopsy specimens
have no underlyingtissue. Surgeons go to tremendous effort to
removeimplants as widely as possible to guarantee resection
ofsurrounding tissue. Subsequently, Bell and colleagues29suggested
use of additional morphological criteria otherthan invasion of
surrounding tissue to classify invasiveand non-invasive implants
(micropapillary architectureand solid epithelial nests surrounded
by clefts).
The skill of the pathologist is also important.26,27Even
forexpert pathologists, some implants remain too ambiguous
to be classified and are categorised as indeterminate
forinvasion.30 To optimise histological analysis and tominimise
interobserver variability, serous borderlineovarian tumours with
implants could benefit fromsystematic review by a reference
pathologist.
To assess the effect of peritoneal implants and to limitrisk of
bias attributable to small series, we analysed reportsincluding at
least 50 patients with serous borderlineovarian tumours with
peritoneal implants (table 1).Longacre and colleagues34 reported
that the soleindependent prognostic factor for overall survival was
theimplant subtype (eight of 14 patients with invasive
implantsrelapsed). Seidman and Kurman36noted that the mortalityrate
for patients with non-invasive and invasive implantswas 47% and
34%, respectively (p
-
8/13/2019 yufi nakal
3/13
www.thelancet.com/oncology Vol 13 March 2012 e105
Review
prognosis for serous borderline ovarian tumours withinvasive
implants is poor, it is better than that for
authenticcarcinoma.23,25 Nevertheless, it is noteworthy that
thenumber of cases of invasive implants and follow-updiffered
widely between series, which could constitutepotential biases.27
Furthermore, proportions of patientswith residual disease and with
micropapillary patternswere not always mentioned. Gershenson and
colleagues32,33recorded very similar rates of progressive and
recurrentdisease (nearly 30%) in patients with non-invasive
andinvasive implants.
These important data should be used to extend follow-upin
advanced-stage borderline ovarian tumours. Silva
andco-workers37suggested that rates of recurrence and
overallsurvival in women with serous borderline ovarian tumoursand
non-invasive implants are time dependent. Of35 relapsing patients,
eight developed recurrent diseasewithin fewer than 5 years of
follow-up, 15 recurrencesarose between 5 and 10 years, eight
between 10 and15 years, and four after 15 years of follow-up.
Patients withinvasive implants relapsed more rapidly than did
thosewith non-invasive implants. The true effect on rate
ofrecurrence (and survival) of implant subtypes should be
assessed in series with prolonged follow-up of more than10
years.2,25,37
Micropapillary patternsFindings of several studies indicate that
serous borderlineovarian tumours with micropapillary patterns have
poorerprognosis than do lesions without this
histologicalfeature.19,34,3840 Nevertheless, the true prognostic
value ofmicropapillary patterns continues to fuel
debate.20Indeed,serous borderline ovarian tumours with
micropapillarypatterns without implants (stage I) or with
non-invasiveimplants (stage IIIII) have the same prognosis as
doserous borderline ovarian tumours without micropapillarypatterns
(or, atypical proliferative serous tumours).22Somefindings indicate
that architecture of micropapillary
patterns does not exert a substantial effect on overallsurvival
when peritoneal implants are controlled for.21,34Decreased survival
of patients with micropapillary patternscould perhaps be linked to
the increased rate of invasiveperitoneal implants and not to
presence of micropapillarypatterns itself.19,38 As a result, some
researchers suggestthat serous borderline ovarian tumours with
micropapillarypatterns without invasive implants should be
classified asserous borderline ovarian tumours and not as
invasivelow-grade serous carcinoma.27,30 Figure 2 shows
theevolution of (but also discrepancies in) these classificationsof
serous borderline ovarian tumours, with morphologicaldescription of
implants and micropapillary patterns.
The main issue for patients with serous borderlineovarian
tumours with micropapillary patterns is toascertain whether the
micropapillary pattern is a feature ofa high-risk group likely to
develop an invasive recurrenceand have disease-related mortality.
In a series with medianfollow-up of 4 years, Shih and colleagues3
noted thatthe micropapillary pattern was associated with
lowdisease-free survival of 759% (95% CI 556878),compared with 943%
(884973) for patients without amicropapillary pattern. However,
patients with and without
invasive implants were not distinguished from those witha
micropapillary pattern. Diffi culties arose in this Reviewwhen we
tried to ascertain whether some recurrences werelinked to the
micropapillary pattern or to invasive peritonealimplants (table 2).
In eight series (n=144)16,17,19,4044showingcorrelations between
overall rate of recurrence, rate ofinvasive recurrence, and rate of
disease-related deathassociated with micropapillary patterns, 56
patients hadrecurrence (39%). 54% (30 of 56) of recurrences
wereinvasive at recurrence and 10% of deaths were related
todisease. Moreover, in seven of eight series
(n=107)16,17,19,40,41,44with information on the nature of
peritoneal implants,29 patients initially had invasive implants
(table 2). Ofthese 29 women, 11 had recurrence in the form
ofcarcinoma or invasive recurrence.16,17,19 The behaviour of
Figure :Evolution of and discrepancies in current
classifications of serous borderline ovarian tumoursSizes of
divisions do not correlate with frequency of each subtype. AFIP=Air
Forces Institute of Pathology. NCI=National Cancer Institute.
NIH=National Institutes of Health. MPSC=micropapillary
serous carcinoma. APST=atypical proliferative serous tumour.
LGSC=low-grade serous carcinoma. HGSC=high-grade serous carcinoma.
*Without micropapillary pattern.
Carcinoma1973: WHO classification23
1980s: implant characterisation2
1996: description of micropapillarypattern16,17
2005 to present: Kurman (2005)22
2003 to present: AFIP (1996),24
WHO (2003),1
NCI/NIH workshop (2004)2527
Evolution of classifications
Proposed current classifications
Borderline
Carcinoma
Carcinoma
Carcinoma
Carcinoma
Stage I borderlineNon-invasive
implantsInvasiveimplants
Stage I borderlineNon-invasive
implants*Invasive
implants*Micropapillary
pattern
Non-invasiveimplants*
Invasiveimplants*
APST HGSCLGSCMPSC
Borderline
CarcinomaBorderline
Stage I borderlineNon-invasive
implantsInvasiveimplants
Micropapillarypattern
-
8/13/2019 yufi nakal
4/13
e106 www.thelancet.com/oncology Vol 13 March 2012
Review
serous borderline ovarian tumours with micropapillarypatterns
seems to be more related to presence of invasiveimplants rather
than to this particular histologicalfeature.25
Stromal microinvasionStromal invasion is more frequently seen in
serous than inmucinous borderline ovarian tumours. Analysis of
theeffect of microinvasion on the rate of invasive recurrencesand
disease-related death is especially diffi cult because ofpotential
confounding factors, such as micropapillarypatterns and presence of
peritoneal implants for serousborderline ovarian tumours.
In 12 series of serous borderline ovarian tumours
withmicroinvasion (n=133), 20 patients had recurrence
(15%),including 35% (seven of 20) with invasive disease
atrecurrence (table 3). Rate of disease-related death was 6%(eight
of 133; table 3).
In accordance with findings of previous studies, our
dataindicate that microinvasion is a prognostic factor for
serousborderline ovarian tumours.34,42Further studies are neededto
establish whether microinvasion is a prognostic factorindependent
of peritoneal implants or micropapillarypatterns.
Histological features of mucinous borderlineovarian
tumoursMucinous borderline ovarian tumours are a complex groupof
lesions, the classifications for which have been revisedseveral
times. Historically, they were mixed with peritonealpseudomyxoma,
but this entity is now known to resultfrom intraperitoneal spread
of non-ovarian adenomatousmucinous neoplasm, most typically from
the appendix,
and should therefore be excluded from mucinousborderline ovarian
tumours.1,27,54
Mucinous borderline ovarian tumours are divided intotwo
subtypes, intestinal (comprising 8590%) andmullerian (or
endocervical) lesions. The intestinal subtypeis more frequently
unilateral, whereas bilateral intestinalmucinous borderline ovarian
tumours should excludeprimary gastrointestinal
carcinoma.1Immunostaining forcytokeratins CK7, CK20, and CDX2, and
oestrogen andprogesterone receptor status, are both useful
fordistinguishing primary ovarian tumours from
metastaticdisease.Moreover, intestinal mucinous borderline
ovariantumour is associated with extraovarian spread in only 2%of
patients. The endocervical or mullerian subtype isbilateral in as
many as 40% of cases. It coexists withipsilateral ovarian or pelvic
endometriosis in 2030% ofpatients, including a serous component
(also calledseromucinous borderline ovarian tumour), which could
be
associated with invasive or non-invasive peritonealimplants such
as serous borderline ovarian tumours.1,55Mucinous borderline
ovarian tumours are thought torepresent an intermediate stage in
the progression toinvasive carcinoma.56 This orderly progression
accountsfor why benign lesions, borderline ovarian tumours,
andinvasive tumour coexist in the same specimen.56 From abiological
viewpoint, mucinous borderline ovariantumours express a
KRASmutation in more than 60% ofcases. The increasing frequency of
KRAS mutation hasbeen described in adenoma, borderline ovarian
tumours,and carcinoma in 3386% of cases.57,58 In addition toabsence
of stromal invasion, mucinous borderline ovariantumours that show
either striking overgrowth of atypicalepithelial cells, more than
three layers of cell stratification,
Patients
(n)
Non-invasive
implants (n)
Invasive
implants (n)
Indeterminate
implants (n)
Duration of follow-up Recurrences in the form of
carcinoma (n)
Deaths related to disease (n)
Bell (1988)2 56 50 6 .. Mean 66 years, median 6 years Not
reported 3 (non-invasive implants);
5 (invasive implants)
Seidman
(1996)1765 52 (with
1 micropapillary
patterns)
13 (with
10 micropapillary
patterns)
.. For micropapillary patterns, median
76 months; for non-invasive
implants, median 99 months
2 (non-invasive implants);
7 or 8* (invasive implants)
1 (non-invasive implants);
6 (invasive implants, 4 of which
were micropapillary patterns)
Zanetta (2001)31 53 28 16 9 Median 70 months 3 0
Gershenson
(1998)32,33112 73 39 .. Median 103 years (non-invasive
implants); median 93 years
(invasive implants)
14 (non-invasive implants);
9 (invasive implants)
6 (non-invasive implants);
6 (invasive implants)
Longacre
(2005)34113 85 14 14 >5 years 3 (non-invasive implants);
4 (invasive implants);
3 (indeterminate implants)
2 (non-invasive implants);
5 (invasive implants);
3 (indeterminate implants)
Kane (2009)15 168 21 9 Mean 57 months 10 in non-invasive
implants
4 in invasive implants
2 (non-invasive implants);
3 (invasive implants)
Shih (2011)35
80 60 19 1 Median 48 years 11 (implant subtypes unknown) 4
(implant subtypes unknown)Total 458 348 87 23 .. 23 (83%)
[non-invasive];
24 or 25 (29%) [invasive]
14 (36%; non-invasive);
23 (25%; invasive)
In case of repeat publications by the same team on a similar
topic, the series with the largest number of patients was reported.
*One patient with vaginal recurrence died of the disease but the
histological
subtype of recurrence was unknown. Series including serous and
mucinous borderline tumours. Recurrences from serous disease.
Including recurrences after conservative treatment. Includes data
from
series reporting initial implant subtypes in patients who
relapsed or died.15,17,3234
Table :Series including 50 or more patients with stage II and
III serous borderline ovarian tumours
-
8/13/2019 yufi nakal
5/13
www.thelancet.com/oncology Vol 13 March 2012 e107
Review
cribriform intraglandular proliferations, or finger-like
projections of solid cellular masses devoid of connectivetissue
are judged intraepithelial carcinoma. However,definition of
intraepithelial carcinoma differs betweenstudies. For some
investigators, tumours with any of thesefeatures alone or in
combination are defined asintraepithelial carcinoma.55A few
pathologists also regardcomplex intraglandular growth patternssuch
ascribriform areas or stroma-free papillae, even withoutsevere
atypiato correspond with a diagnosis ofintraepithelial
carcinoma.54,59 One of the major issues inmucinous borderline
ovarian tumours, particularly inthose showing intraepithelial
carcinoma, is that numeroussampling and more tissue sections should
be obtained torule out invasive carcinoma.56
Intestinal mucinous borderline ovarian tumour istypically
discovered at FIGO stage I, therefore, prognosis isusually
excellent. However, findings have suggested thatmucinous borderline
ovarian tumours (excludingperitoneal pseudomyxoma) could be
associated with a lateand lethal invasive recurrence inside or
outside theabdomen.52,53In a study of mucinous lesions by Koskas
andcolleagues,52 rate of invasive recurrence 10 years
aftertreatment was 13%. Similarly, Khunamornpong
andco-workers53reported a 42% recurrence rate (three of six
patients died of recurrence).Four of the six patients with
recurrence had microinvasion.
53
Of the six patients whorecurred, four had invasive recurrence
and one had nohistological features of recurrence (but had
peritoneal andliver metastases); the remaining woman had
borderlinemucinous disease with intraepithelial and
microinvasivecarcinoma at the time of histological analysis of the
firstrecurrence, but she died from progression 14 months
afterinitial surgery.53These data could be accounted for by
thecontinuum of (benign to frankly invasive) lesions in thesame
specimen and the frequently associated presence ofintraepithelial
carcinoma, which makes differentiationfrom an invasive component
diffi cult. Moreover,researchers have reported that the prognosis
of mucinousinvasive carcinoma is worse than that of other
epithelial
cancers, with diminished chemosensitivity to platinum-based and
paclitaxel-based regimens and overall poorprognosis, particularly
in stage II or III disease.60,61
Intraepithelial carcinomaDefinition of intraepithelial carcinoma
for mucinousborderline ovarian tumours is controversial.54Presence
ofsevere cytological atypia was the only diagnostic criterionon
which a consensus was reached for diagnosis ofintraepithelial
carcinoma. Seidman and Kurman36reported
Total
SBOT
(n)
SBOT with micropapillary patterns Mean follow-up
(months)
Total
(n)
Implants
(n)
Non-invasive
implants (n)
Invasive
implants (n)
Recurrences
(n)
% invasive
recurrence (n)
Deaths related to disease
(n [implant subtypes])
Burks (1996)16 17 10 10 4 6 4 50% (2) 2 (invasive) 732
Seidman (1996)17 65 11 11 1 10 7 71% (5) 4 (invasive) 95
Eichhorn(1999)S1 84 40 11 8 3 4 .. 2 (invasive) ..
Goldstein (2000)41 7 7 3 3 0 2 100% (2) 2 (invasive) 996
Deavers (2002)19 99* 18 18 15 3 14 79% (11) 5 (2 invasive, 3
non-invasive) 125
Prat (2002)39 137 18 13 12 1 2 .. 0 84
Slomovitz (2002)40 57 14 0 0 0 3 33% (1) 0 433
Ayhan(2005)S2 54 11 .. .. .. .. 0 0
Longacre (2005)34 276 23 10 4 5 .. .. (3) 5 (3 invasive, 1
non-invasive
implants, 1 stage I)
76
Cusid (2007)S3 208 29 .. .. .. .. .. .. 883
Silva (2006)37 80 11 .. .. .. 9 .. .. 1884 (median)
Hogg (2007)42 46 13 .. .. .. 2 100% (2) 1 (non-invasive) 678
Chang (2008)S4 85 18 .. .. .. .. .. .. 41
Laurent(2008)43 15 15 9 8 1 11 9% (1) 1 (non-invasive) 63
(median)
Ren (2008)S5 101 20 .. .. .. .. .. 0 40
De Iaco (2009)S6 102 7 .. .. .. .. 0 0 605
Uzan (2011)44 168* 56 56 46 9 13 46% (6) 1 (non-invasive) 57
(median)
Kane (2010)S7 18 8 .. .. .. .. .. 1 (non-invasive) 38
(median)
Shih (2011)3 196 36 .. .. .. .. .. .. 444 (median)
Total 144 56 (39%) 21% (30) 14 (10%)
Supplementary references (S) are listed in the appendix.
SBOT=serous borderline ovarian tumour. *With implants. Only series
providing correlations with overall rate of
recurrence, rate of invasive recurrence, and disease-related
death associated with micropapillary pattern were included in this
calculation.S5,16,17,19,4044
Table :Prognostic effect of micropapillary patterns in SBOT
See Online for appendix
-
8/13/2019 yufi nakal
6/13
e108 www.thelancet.com/oncology Vol 13 March 2012
Review
290 cases of stage I intraepithelial carcinomas with18
disease-related deaths. Of 13 patients with advanced-stage disease,
nine deaths were disease-related. Sincepublication of that report,
findings of five series (n=559)with mucinous borderline ovarian
tumours and clearhistological criteria for diagnosis of
intraepithelialcarcinoma showed presence of intraepithelial
carcinomain 35% of cases (n=197).47,48,52,53,59 Of these
patients,431 (including 153 showing intraepithelial carcinoma)
werefollowed up.47,48,52,53,59 Nine (6%) of the 153 women
hadrecurrence, with three cases of invasive disease at
recurrence. All patients with invasive recurrence died ofthe
disease. In 278 patients without intraepithelialcarcinoma, 11 (4%)
recurred. In the series by Seidman andKurman,36 the overall rate of
death associated withintraepithelial carcinoma was estimated at 6%.
This fairlyhigh rate of death, and the well-known continuum
ofbenign, borderline, and invasive components in the samespecimen,
should encourage pathologists to increase thenumber of tissue
sections examined to rule out anyassociation with invasive
carcinoma.
Stromal microinvasionTable 3 presents data for mucinous
borderline ovariantumours with stromal micronvasion. In eight
series(n=116), no patients developed invasive recurrence and
none died in relation to disease.4549,5153Microinvasion doesnot
seem to be a prognostic factor for mucinous borderlineovarian
tumours.
Preoperative assessment of patients withhigh-risk borderline
ovarian tumoursFrom an epidemiological point of view, borderline
ovariantumours and carcinoma share very close characteristics.Thus,
distinguishing a high-risk group of women withborderline ovarian
tumours is diffi cult. Clinical exam-ination could be helpful for
detection of a high-risk group,
by looking for clinical ascites, suspicious nodes (in thegroin,
axillary, or cervical nodes), or peritoneal lesions inDouglas
pouch, but such findings could also be discoveredin authentic
carcinoma.
The relevance of serum tumour markers in patients withborderline
ovarian tumours is controversial. Van Calsterand colleagues62showed
that amounts of CA125 in serumoverlapped between patients with
borderline ovariantumours and early-stage ovarian carcinoma.
Abnormalconcentrations in serum of CA125 were noted in about40% of
patients with stage I borderline ovarian tumoursand reached 83% in
women with advanced-stage disease.63With the exception of
advanced-stage borderline ovariantumours, no data are available to
support the relevance ofserum tumour markers (eg, CA125, CA199,
carcino-
Histological
type
Borderline ovarian tumour with microinvasion Mean follow-up
(months)
Number Recurrences (n) % invasive recurrence (n)* Deaths related
to disease (n)*
Katzenstein (1978) S8 SBOT 7 0 0 0 131
Bell (1990)S9 21 SBOT 21 1 0 0 624
Casey (1993)S10 SBOT 2 0 0 0 175
Hanselaar (1993) S11 SBOT 9 0 0 0 54
Tan (1994)S12 SBOT 2 1 0 0 264
Siriaunkgul (1995)45 54 MBOT 7 0 0 0
Kennedy (1996)S13 76 SBOT 4 0 0 0 99
Nayar (1996)S14 126 SBOT 7 0 0 0 96
Seidman (1996)17 65 SBOT 4 0 0 0 95
Hoerl (1998)46 49 MBOT 14 0 0 0 71
Eichhorn (1999)S1 84 SBOT 9 1 0 0 744
Riopel (1999)47 73 MBOT 8 0 0 0 33
Lee (2000)48 171 MBOT 7 0 0 0
Nomura (2000)49 25 MBOT 4 0 0 0 85
McKenney (2006)50 SBOT 50 9 67% (6) 7 924
Kim (2007)51 118 MBOT 37 0 0 0 604
Laurent (2009)S15 10 SBOT 10 5 0 0 62
Kane (2009)15 18 SBOT 8 3 33%|| 1|| 38 (median)
Koskas (2011)52 97 MBOT 8 0 0 0 48
Khunamornpong (2011)53 171 MBOT 31 4 0 0 168
Total .. 249 24 (10%) 3% (7) 8 (3%)
Supplementary references (S) are listed in the appendix.
SBOT=serous borderline ovarian tumour. MBOT=mucinous borderline
ovarian tumour. *Implant subtypes during
initial management. With lymph-node involvement.2 indeterminate,
1 invasive, 1 invasive and micropapillary pattern, 2 microinvasion
only .2 indeterminate, 1 invasive,
1 invasive and micropapillary pattern, 1 micropapillary pattern,
2 microinvasion only. With implants. ||1 micropapillary pattern and
non-invasive.
Table :Prognostic effect of stromal microinvasion on SBOT and
MBOT
-
8/13/2019 yufi nakal
7/13
www.thelancet.com/oncology Vol 13 March 2012 e109
Review
embryonic antigen) for identification of a high-risk group
of borderline ovarian tumours.Pelvic ultrasound is a key
procedure for detection andassessment of ovarian tumours. Some
scales or scoringsystems have been defined to assess objectively
the degreeof suspicion for malignant disease in these
lesions.However, those scales are used to gauge so-called risk
ofmalignancy before a potential surgical procedure but, atpresent,
no ultrasound criterion can identify a high-riskgroup of borderline
ovarian tumours.
Findings of radiological studies underline the contri-bution of
perfusion-weighted and diffusion-weighted MRIsequences for
differentiation of benign lesions, borderlineovarian tumours, and
ovarian cancer.64 In a series of12 benign, 13 borderline, and 16
invasive ovarian tumours,64
early tumour enhancement on dynamic contrast-enhancedMRI images
was helpful to distinguish between thesetypes of tumours. MRI
findings correlated with angiogenicstatus of the tumour, which was
ascertained afterhistopathological analysis of VEGF receptor
expression inparaffi n-embedded specimens.64 Correlation of
suchradiohistological findings could perhaps be of futureinterest
to help identify a high-risk group of borderlineovarian tumours.
Yet, since pathological analysis of thetumour specimen (ovary and
peritoneum) is key foridentification of potentially invasive
lesions, establishing ahigh-risk group before surgery seems
uncertain.
Clinical management and effect on rate ofinvasive recurrence and
survivalSurgeryStandard surgical treatment for borderline
ovariantumours is based on bilateral salpingo-oophorectomy, withor
without hysterectomy. Staging surgery is also used,which includes
peritoneal staging procedures with orwithout nodal staging
methods.
Conservative treatment and risk of invasive
recurrenceConservative treatment (defined as preservation of
theuterus and at least a part of one ovary) is important foryoung
patients with borderline ovarian tumours. Thisoption is appropriate
even for serous lesions with non-
invasive implants.31,65 Nearly 2000 cases of
conservativetreatment have been reported in published work.
Fertility-sparing surgery is associated with a higher rate of
recurrencethan is bilateral salpingo-oophorectomy, but it has no
effecton survival because most recurrences are borderline
lesionsthat are cured readily by a second surgical
procedure(possibly conservative).15,31,65Nevertheless, the main
issue isto assess risk of invasive recurrence.
We analysed 47 cases of progression to invasivecarcinoma,
including 21 published since 2009, underliningthe possibility of
publication bias (table 4). Risk ofprogression to invasive
carcinoma was estimated as 23%.Of 47 recurrences, 20 were recorded
in patients with serousborderline ovarian tumours, 24 had mucinous
borderlineovarian tumours, and three were of an unknown
histological subtype. Mean time to progression to
carcinoma was 75 months (range 11310) for serousborderline
ovarian tumours and 33 months (582) formucinous borderline ovarian
tumours. Eight of the20 recurrences of serous borderline ovarian
tumours wererecorded in patients with peritoneal implants. 18
womenhad follow-up data available; six died of the disease andeight
were alive without evidence of disease (table 4). Ofthe 24
recurrences of mucinous borderline ovariantumours, 23 initially had
FIGO stage I disease. Of 21 withfollow-up data, 13 died of disease
and only three were alivewithout disease (table 4).
In patients with serous borderline ovarian tumourstreated by
cystectomy, five of 11 were alive without diseasecompared with one
of nine who had mucinous borderline
ovarian tumours (table 4). Women with recurrence ofinvasive
mucinous lesions had a higher rate ofextra-abdominal metastasis as
the first site of recurrence(four in pleura, lung, or bone) whereas
no extra-abdominalmetastases arose in patients with recurrence of
invasiveserous borderline ovarian tumours.
These differing data do not question the validity ofconservative
treatment. Such recurrences also arise inpatients treated by
bilateral salpingo-oophorectomy forborderline ovarian tumours.
Nevertheless, they suggestthat the rate of death is higher in women
with recurrentmucinous borderline ovarian tumours than in those
withserous lesions with transformation to invasive carcinoma,which
then takes place earlier. Furthermore, a recomm-endation of initial
unilateral salpingo-oophorectomy formucinous borderline ovarian
tumours rather thancystectomy seems logical, whereas in the case of
serouslesions, no clear recommendations can be made.52,66
Role of laparoscopyThe role of laparoscopy is relevant because
of potentialrisks of ruptured cysts, intraperitoneal cell
dissemination,tumour metastasis in trocar incisions, and
recurrence.Findings of previous studies have shown the rate of
cystrupture is higher for laparoscopy than for laparotomy,
andlaparoscopy has a potentially higher risk of
recurrence.67However, risk of cyst rupture was associated most with
a
high rate of conservative surgery (cystectomy).63Similarly,rate
of recurrence after laparoscopy was related toconservative
treatment, but no association was reportedbetween laparoscopic
treatment and risk of invasiverecurrence.
Only eight cases of trocar implantation metastasis havebeen
reported after laparoscopy for borderline ovariantumours;68 five
arose in patients with peritoneal implantsbut none died of the
disease. This finding underlines theneed to recall use of
systematic protected extraction foradnexal tumours.68
Peritoneal staging for identification of high-risk
patientsAdequate staging, including careful inspection of
theperitoneum, is crucial for identification of high-risk
-
8/13/2019 yufi nakal
8/13
e110 www.thelancet.com/oncology Vol 13 March 2012
Review
patients who are likely to develop invasive recurrence and
die of disease. Findings of studies indicate a low rate (38%)of
complete staging (at least peritoneal cytological
analysis,omentectomy, and peritoneal biopsy) during initial
surgery,even when the borderline nature of the lesion could be
assessed by intraoperative histological analysis.69,70
Fauvet
and colleagues
70
reported a 46% rate of complete stagingby laparoscopy during
initial surgery, 214% afterconversion to open surgery, and 254% by
laparotomy. Linand co-workers69recorded a 12% rate of complete
staging
Borderline tumours (n) Details of initial treatment Location*
Details of recurrence(s) Outcomes
Initial
stage
Surgical treatment Histological subtypes Interval
(months)
Histology
Serous tumours
Chambers (1988)S16 11 SBOT IA Cystectomy SBOT Ipsilateral ovary
12 Serous adenocarcinoma
grade 1
..
Morris (2000)S17 26 SBOT Unknown USO and cystectomy SBOT
Ipsilateral ovary 147 Not reported DOD
Morris (2000)S17 11 SBOT IA USO and staging SBOT Contralateral
ovary 39 Serous adenocarcinoma
grade 2
DOD
Zanetta (2001)31 156 stage I SBOT IA Cystectomy SBOT Ovaries,
peritoneum,
nodes
39 Serous adenocarcinoma
grade 3
NED
Zanetta (2001)31 156 stage I SBOT IC USO and CC SBOT Ovary ..
Serous adenocarcinoma
grade 1
..
Donnez (2003)S18 37 SBOT stage IIII I (probably) USO and CC SBOT
At least ovary 12 Invasive (probably) NED
Longacre (2005)34 53 SBOT stage I IA .. SBOT Colon and
gallbladder 288 Low-grade serous
adenocarcinoma
AWD
Longacre (2005)34 53 SBOT stage I IA .. SBOT, SMI Axillary nodes
310 Low- grade serous
adenocarcinoma
NED
Romagnolo (2006)S19 75 SBOT stage IIII IA USO SBOT Contralateral
ovary 36 - DOD
Yokoyama (2006)5 23 SBOT IA Cystectomy SBOT Contralateral ovary
107 Serous adenocarcinoma NED
Suh-Burgmann
(2006)S20109 SBOT stage IIII IC USO SBOT Peritoneum 27 Serous
adenocarcinoma
grade 1
NED
Ji (2010)S21 Case report IC USO and staging SBOT, SMI Ovary and
peritoneum 17 Invasive implants DOD
Zanetta (2001)31
51 SBOT stage IIIII IIB Cystectomy SBOT Contralateral ovaryand
nodes
50 Invasive carcinoma grade 1 NED
Prat (2002)39 40 SBOT stage IIII II USO SBOT, invasive implants
.. .. .. DOD
Attar (2004)S22 Case report IIIC USO, CC, and staging SBOT, MPP,
positive
nodes
Peritoneum 18 Serous adenocarcinoma AWD
Wong (2007)S23 65 SBOT stage IIII IIC Cystectomy SBOT
Ipsilateral ovary .. Invasive implants NED
Vigan (2010)S24 10 SBOT IIIII .. SBOT .. .. Invasive implants
NED
Uzan (2010)65 41 SBOT stage IIIII II Cystectomy and
staging
SBOT, MPP, non-invasive
implants
Ovary and peritoneum 42 Invasive ..
Uzan (2010)65 41 SBOT stage IIIII III Cystectomy and
staging
SBOT, MPP, non-invasive
implants
Ovary and peritoneum 56 Invasive DOD
Uzan (2010)65 41 SBOT stage IIIII III USO SBOT, SMI,
invasive
implants
Peritoneum 11 Invasive ..
Mucinous tumours
Ji (1996)S25 45 MBOT stage I IC Cystectomy MBOT .. .. Not
reported DOD
Gotlieb (1998)S26 23 MBOT stage I IA USO MBOT Contralateral
ovary 5 Endometrioid
adenocarcinoma
NED
Zanetta (2001)31 117 MBOT stage I IC Cystectomy MBOT Pelvis and
abdomen 10 Mucinous adenocarcinoma
grade 3
DOD
Zanetta (2001)31 117 MBOT stage I IA Cystectomy MBOT Ipsilateral
ovary 55 Mucinous adenocarcinoma
grade 1
NED
Lee (2000)48 136 MBOT stage IIII
intestinal
IC USO and staging MBOT, IEC, grade 3
nuclei
Peritoneum 12 Mucinous adenocarcinoma
grade 2
DOD
Suh-Burgmann
(2006)S2081 MBOT stage IIII IC USO MBOT Peritoneum Mucinous
adenocarcinoma
grade 3
DOD
Wong (2007)S23 169 MBOT stage IIII IA USO MBOT Contralateral
ovary
and peritoneum
Invasive carcinoma DOD
Wu (2009)S27 157 MBOT stage IIII IC Cystectomy MBOT Colon serosa
and
trocar site
82 Invasive carcinoma DOD
(Continues on next page)
-
8/13/2019 yufi nakal
9/13
www.thelancet.com/oncology Vol 13 March 2012 e111
Review
by laparotomy, 7% for general surgeons, and 50% for
oncological surgeons. Study data suggest that incompletestaging
has no effect on survival and rate of recurrence.69,71
However, Seidman and Kurman36noted a recurrence rateof 17% in
patients with complete staging versus 99% inthose with incomplete
staging. Similarly, Camatte andcolleagues71reported no recurrence
after complete stagingcompared with a rate of 8% after incomplete
staging.
Despite these data, surgery to restage a patient iscontroversial
because it has little effect on managementfor those with borderline
ovarian tumours. In fact, the onlyway to modify management of women
with apparentstage I borderline ovarian tumours is if invasive
implantsare found at microscopic examination and the patient
isupstaged (in such cases, adjuvant treatment could bediscussed).
If non-invasive implants are identified in a
woman with a macroscopically normal peritoneal cavity,
further treatment (surgery or adjuvant treatment) is
notnecessary. Nevertheless, only a few cases (n=2) ofmicroscopic
invasive implants (with an apparently normalperitoneum at surgical
staging) have been noted duringmicroscopic examination
only.72,73Thus, systematic surgicalstaging for identification of
patients in whom adjuvanttreatment should be delivered (microscopic
invasiveimplants) is limited. However, features that argue in
favourof restaging surgery include mucinous borderline
ovariantumours treated by cystectomy, micropapillary
pattern,microinvasion, incomplete excision of peritoneal
implants,and the indeterminate nature of peritoneal
implants,attributable to absence of adjacent and underlying
tissue.
Conventional complete surgical staging for mucinousborderline
ovarian tumours includes appendectomy to
Borderline tumours (n) Details of initial treatment Location*
Details of recurrence(s) Outcomes
Initial stage Surgical treatment Histological subtypes
Interval
(months)
Histology
(Continued from previous page)
Wu (2009)S27 157 MBOT stage IIII IIB USO and staging MBOT
Peritoneum and nodes 11 Invasive carcinoma
Park (2009)S28 139 MBOT stage IIII IA USO and cystectomy MBOT
Lung 82 Mucinous invasive
carcinoma
DOD
Chiesa (2010)S29 Case reported in the
Discussion
IC USO and staging MBOT intestinal Peritoneum 70 Adenocarcinoma
grade 1
Koskas (2011)52 74 MBOT stage I IA Cystectomy MBOT intestinal
Contralateral ovary,
peritoneum, bones
57 Invasive carcinoma AWD
Koskas (2011)52 74 MBOT stage I IA Cystectomy MBOT intestinal
Ipsilateral ovary 27 Invasive carcinoma AWD
Koskas (2011)52 74 MBOT stage I IC USO and staging MBOT
intestinal Peritoneum and nodes 10 Invasive carcinoma DOD
Koskas (2011)52 74 MBOT stage I IA Cystectomy MBOT mixed At
least ovary 7 Invasive carcinoma AWD
Koskas (2011)52 74 MBOT stage I IA Cystectomy MBOT endocervical
Peritoneum Invasive carcinoma DOD
Koskas (2011)52 74 MBOT stage I IA USO and staging MBOT
intestinal, IEC Pleura Invasive carcinoma DOD
Khunamornpong
(2011)5360 MBOT stage I
intestinal
I .. MBOT intestinal, IEC,
SMI
Contralateral ovary 17 Invasive disease in nodes NED
Khunamornpong
(2011)5360 MBOT stage I
intestinal
IC .. MBOT intestinal, IEC,
SMI
Contralateral ovary
and nodes
36 Invasive carcinoma DOD
Khunamornpong
(2011)5360 MBOT stage I
intestinal
IC .. MBOT intestinal Contralateral ovary
and peritoneum
36 Invasive carcinoma DOD
Khunamornpong
(2011)5360 MBOT stage I
intestinal
IC .. MBOT intestinal .. .. Invasive carcinoma ..
Ha (2011)S30 7 conservative
treatment
.. USO and staging MBOT endocervical and
IEC
.. 25 Carcinoma DOD
Ha (2011)S30 7 conservative
treatment
.. USO MBOT, IEC Contralateral ovary,
bone, lung
23 Not reported, but
progression with
metastasis
AWD
Song (2011)S31 106 MBOT IA .. .. Contralateral ovary 26 Invasive
carcinoma AWD
Unknown subtype
Fort (1989)S32 8 stage III I or II USO Not reported
Contralateral ovary 60 Serous adenocarcinoma NED
Kehoe (1996)S33 54 stage III I (probably) USO Not reported
Contralateral ovary 12 Invasive carcinoma DOD
Maneo (2004)S34 61 stage I by
laparoscopy
IA Laparoscopy Not reported Ipsilateral ovary and
omentum
44 Invasive carcinoma grade 2 ..
In case of repeat publications by the same team on a similar
topic, the series with the last updated outcomes or largest number
of patients was reported. Supplementary references (S) are listed
in the appendix.
AWD=alive with disease. CC=contralateral cystecomy. DOD=died of
disease. IEC=intraepithelilal carcinoma. MBOT=mucinous borderline
ovarian tumour. MPP=micropapillary pattern. NED=no evidence of
disease. SBOT=serous borderline ovarian tumour. SMI=stromal
microinvasion. USO=unilateral salpingo-oophorectomy. *Of first
invasive recurrence. Details on the invasive recurrence (some
patients had a
previous history of borderline recurrence before invasive
recurrence). Number treated conservatively and radically.
Table :Cases of progression to invasive carcinoma after c
onservative treatment of borderline ovarian tumours
-
8/13/2019 yufi nakal
10/13
e112 www.thelancet.com/oncology Vol 13 March 2012
Review
exclude synchronous or primitive appendiceal tumour(mucocele).
However, in a study focusing on the histologicalinterest of
appendectomy, no disease was reported in theappendix in 57 patients
with early-stage ovarian tumourswho underwent surgical staging for
mucinous tumours(15 were borderline).74
Effect of lymphadenectomy and lymph-nodeinvolvement on
survivalLymph-node involvement is recorded in about 25% ofpatients
with advanced-stage borderline ovarian tumours(FIGO stage III or
IV).75 Lymph-node involvement issometimes associated with
lymph-node endosalpingiosis.
Molecular and histological data suggest that most nodalimplants
are metastases from synchronous ovarianneoplasms, but a few arise
from de novo nodal
endosalpingiosis.76 Pathways by which nodal metastasesproceed in
non-invasive neoplasms are unclear. Fadare andcolleagues77 showed
no difference in lymphatic vesseldensity between node-positive and
node-negative tumours,suggesting that these lesions might have a
predilection forperitoneal rather than lymphatic spread.
Several researchers have reported no effect of lymph-node
involvement on survival of patients with borderlineovarian
tumours.34,36,77,78 In a series of 123 patients,including 68 with
complete surgical staging, Kanat-Pektasand colleagues78recorded no
difference between disease-free and overall survival. Data from our
institution andfrom the SEER database accord with these findings
andshow that survival correlates with FIGO stage irrespectiveof
nodal status.75The rate of invasive implants seems to
be higher in patients with lymph-node involvement than
in those without nodal spread.
50,79
Djordjevic and Malpica
79
reported rates of invasive implants of 25% (nine of 36)
inpatients with lymph-node involvement versus 3% (one of36) in
those without involvement. Lymph-node dissectioncould be discussed
for treatment of peritoneal implantsassociated with gross nodal
disease during surgicalexploration and in women with invasive
implants.
Residual diseaseResidual disease is a prognostic factor for
borderlineovarian tumours.29,32,34,35 In addition to the
potentialtherapeutic effect, complete removal of peritoneal
implantsallows for comprehensive histological analysis. In a
seriesof 168 patients with serous borderline ovarian tumours
(FIGO stage II and III), 5-year disease-free survival was75% in
patients with no residual disease, 76% in those withresidual
disease less than or equal to 2 cm, and 56% inthose with residual
disease greater than 2 cm (p
-
8/13/2019 yufi nakal
11/13
www.thelancet.com/oncology Vol 13 March 2012 e113
Review
Moreover, Lesieur and co-workers75recorded no effect of
adjuvant chemotherapy on disease-free survival in patientswith
lymph-node involvement.Concern persists for patients with invasive
implants.
Most teams currently propose chemotherapy as treatment,although
the proven effectiveness of this option continuesto be debated. If
undertaken, the chemotherapy regimen issimilar to that used in
ovarian cancer (a platinum-basedregimen with paclitaxel).
Different pathways (particularly the MAPK signallingpathway)
have been identified in the carcinogenesis ofserous borderline
ovarian tumours with micropapillarypatterns and low-grade
carcinoma, suggesting that targetedtreatments could be used in
these diseases.18,21,84May andcolleagues18suggested that inhibition
of PARP1 could be a
target. A trial has started to test a MEK inhibitor in
recurrentlow-grade serous carcinoma with the poorest response
toconventional chemotherapy compared with high-gradecarcinoma
(ClinicalTrials.gov identifier NCT00551070).
Follow-up to detect invasive recurrencesSeveral researchers have
described outcomes of patientswith borderline ovarian tumours,
including advanced-stage disease, but very few have focused on
usefulmethods for detection of recurrences.67,85,86
Transvaginalultrasonography is the most effective procedure
forconservative management of early-stage disease. In aseries of
five patients with invasive recurrence afterconservative treatment
for early-stage borderline ovariantumours,85all had abnormal
findings on ultrasound andabnormal amounts of CA125. Uzan and
colleagues86confirmed the importance of imaging
(abdominopelvicultrasonography) for detection of recurrence (422%)
inwomen with stage II or III serous borderline ovariantumours who
were treated conservatively. A raised levelof CA125 in serum formed
part of the initial diagnosis inonly 156% of all recurrences, but
this marker was themost frequent method for diagnosis of recurrent
invasivelesions (six of 13 patients relapsed with
carcinoma).86Thus, a combination of follow-up proceduresie,
bothimaging and determination of CA125 in serumseemsto be an
adequate option, particularly in patients
with invasive implants. For conservative
treatment,abdominopelvic ultrasound is needed. AbdominopelvicCT or
MRI could be proposed for women treated forstage II or III disease
with abnormal or inconclusivefindings on ultrasound (due to complex
previoussurgeries or obesity). Nevertheless, very few series
havebeen published on this specific topic, and the combinationof
blood markers and imaging has not had an effect onoverall survival
in this context. Potential prognosticfactors for invasive
recurrence in borderline ovariantumours are presented in the
panel.
ConclusionsThe pathologist has a pivotal role in assessment of
theborderline nature of ovarian tumours and in identifica-
tion of high-risk criteria for invasive recurrences andpossible
death from disease. We have identified twofactors that are
important for recurrence of invasivedisease. First is invasive
peritoneal implants (in serousborderline ovarian tumours), and
second is residualdisease after surgery. Other factors are
controversialowing to increased risk of invasive recurrence,
forexample, presence of micropapillary patterns in serousborderline
ovarian tumours, presence of intraepithelialcarcinoma in mucinous
lesions, presence of stromalmicroinvasion in serous tumours, and
use of cystectomyin mucinous borderline ovarian tumours.
Variability in rates of recurrence and survival betweenseries
depends not only on pathological criteria used toclassify entities
but also on how published materialwas gathered. Population-based
studies from academicinstitutions, data obtained over several
decades, cohortstudies, or collection of specimens by one
pathologist allrepresent potential biases.20 Publication bias
cannot beignored because it can lead to overestimation of risk
forpoor prognosis. To avoid such biases, all studies shouldverify
the quality of tissue collection and sampling forhistological
analysis to enable centralised uniformpathological review
(particularly important in multicentreseries) with suffi cient
patients and prolonged follow-up,which will allow relevant
conclusions to be drawn for
routine practice.21At present, the only pragmatic way to better
identify
patients at high risk of invasive recurrence is
pathologicalreview of tumour slides by a skilled pathologist (or a
panelof pathologists) for patients in at-risk situationseg,
thosewith borderline ovarian tumours with implants (to
clearlydistinguish invasive from non-invasive implants),
withmicropapillary patterns (associated with a higher rate
ofimplants), with intraepithelial carcinoma, stromalmicroinvasion,
or both (could ultimately be diagnosed asinvasive carcinoma), and
mucinous borderline ovariantumours (pathological classification of
this tumour isarduous). In some countries, centralised
pathologicalreviews (or registries) are being organised to decrease
therare but potentially lethal risk of invasive recurrences.
Search strategy and selection criteria
Data for this Review were identified from searches of Medline,
Current Contents, PubMed,
and references in relevant articles, with the terms borderline
ovarian tumours, low-
malignant potential ovarian tumours, recurrence, implants,
micropapillary, stromal
microinvasion, intraepithelial carcinoma, mucinous ovarian
tumours, and serous
ovarian tumours. We did not include abstracts and reports from
meetings. We searched
for articles published in English or French (with abstracts in
English) between 1985 and
May, 2011. Because many studies have been published on
borderline ovarian tumours, the
papers we selected were based on the description of invasive
recurrences (with respect to
different factors analysed for clinical management) and on their
relevance for our
discussion of histopathology and pathological prognostic
factors. Thus, we included series
reporting particular histopathological patterns for the first
time or series reporting the
largest number of patients or the most complete results (in
terms of variables studied).
-
8/13/2019 yufi nakal
12/13
e114 www.thelancet.com/oncology Vol 13 March 2012
Review
Contributors
PM and ED had the idea for the Review. All authors contributed
to theliterature search, analysis of data, and writing of the
Review.
Conflicts of interest
We declare that we have no conflicts of interest.
References1 Tavassoli FA, Devilee P. World Health Organization
classification
of tumours: pathology and geneticstumours of the breast
andfemale genital organs. Lyon: IARC Press, 2003.
2 Bell DA, Weinstock MA, Scully RE. Peritoneal implants of
ovarianserous borderline tumors: histologic features and
prognosis.Cancer1988; 62:221222.
3 Shih KK, Zhou Q, Huh J, et al. Risk factors for recurrence of
ovarianborderline tumors. Gynecol Oncol2011; 120:48084.
4 Hannibal CG, Huusom LD, Kjaerbye-Thygesen A, Tabor A, Kjaer
SK.Trends in incidence of borderline ovarian tumors in
Denmark19782006. Acta Obstet Gynecol Scand2011; 90:30512.
5 Yokoyama Y, Moriya T, Takano T, et al. Clinical outcomes and
riskfactors for recurrence in borderline ovarian tumours. Br J
Cancer
2006; 94:158691.6 Hart WR. Borderline epithelial tumors of the
ovary. Mod Pathol2005;
18:S3350.
7 Mink P, Sherman ME, Devesa S. Incidence patterns of invasive
andborderline ovarian tumors among white women and black women
inthe United States: results from the SEER program, 19781997.
Cancer2002; 95:238089.
8 Trimble CL, Kosary C, Trimble EL. Long-term survival and
patterns ofcare in women with ovarian carcinoma: a population-based
analysis.Gynecol Oncol2002; 86:3437.
9 Bell DA, Scully RE. Atypical and borderline
endometrioidadenofibromas of the ovary: a report of 27 cases. Am J
Surg Pathol1985; 9:20514.
10 Snyder RR, Norris HJ, Tavassoli F. Endometrioid proliferative
andlow malignant potential tumors of the ovary: a clinicopathologic
studyof 46 cases. Am J Surg Pathol1988; 12:66171.
11 Bell KA, Kurman RJ. A clinicopathologic analysis of
atypicalproliferative (borderline) tumors and
well-differentiated
endometrioid adenocarcinomas of the ovary. Am J Surg Pathol
2000;24:146579.
12 Roth LM, Emerson RE, Ulbright TM. Ovarian endometrioid
tumorsof low malignant potential: a clinicopathologic study of 30
cases withcomparison to well-differentiated endometrioid
adenocarcinoma.Am J Surg Pathol2003; 27:125359.
13 Kao GF, Norris HJ. Unusual cystadenofibromas:
endometrioid,mucinous, and clear cell types. Obstet Gynecol1979;
54:72936.
14 Roth LM, Langley FA, Fox H, Wheeler JE, Czernobilsky B.
Ovarianclear cell adenofibromatous tumors: benign, of low
malignantpotential, and associated with invasive clear cell
carcinoma.Cancer1984; 53:115663.
15 Kane A, Uzan C, Rey A, et al. Prognostic factors in patients
withovarian serous low malignant potential (borderline) tumors
withperitoneal implants. Oncologist2009; 14:591600.
16 Burks R, Sherman M, Kurman R. Micropapillary serous carcinoma
ofthe ovary: a distinctive low-grade carcinoma related to
serous
borderline tumors. Am J Surg Pathol1996; 20:131930.17 Seidman
JD, Kurman RJ. Subclassification of serous borderlinetumors of the
ovary into benign and malignant types:a clinicopathologic study of
65 advanced stage cases.Am J Surg Pathol1996; 20:133145.
18 May T, Virtanen C, Sharma M, et al. Low malignant
potentialtumors with micropapilllary features are molecularly
similar tolow-grade serous carcinoma of the ovary. Gynecol
Oncol2010;117:917.
19 Deavers MT, Gershenson DM, Tortolero-Luna G, Malpica A, Lu
KH,Silva E. Micropapillary and cribriform patterns in ovarian
seroustumors of low malignant potential: a study of 99 advanced
stage cases.Am J Surg Pathol2002; 26:112941.
20 Prat J. Serous tumors of the ovary (borderline tumors
andcarcinomas) with and without micropapillary features.Int J
Gynecol Pathol2003; 22:2528.
21 Shih IM. Ovarian serous low malignant potential (borderline)
tumor:does micropapillary matter? Gynecol Oncol2010; 117:13.
22 Kurman RJ, Seidman JD, Shih IM. Serous borderline tumours of
theovary. Histopathology2005; 47:31015.
23 Serov SF, Scully RE, Sobin LH. International
histologicalclassification and staging of tumours: histologic
typing of ovarian
tumors. Geneva: World Health Organization, 1973.24 Scully RE,
Young RH, Clement PB. Atlas of tumor pathology: tumors
of the ovary, maldeveloped gonads, fallopian tube, and
broadligament. Washington: Air Forces Institute of Pathology,
1996.
25 Bell DA, Longacre TA, Kohn EC, et al. Serous borderline
(lowmalignant potential, atypical proliferative) ovarian tumors:
workshopperspectives. Hum Pathol 2004; 35:93448.
26 Seidman JD, Soslow RA, Vang R, et al. Borderline ovarian
tumors:diverse contemporary viewpoints on terminology and
diagnosticcriteria with illustrative images. Hum Pathol2004;
35:91833.
27 Silverberg SG, Bell DA, Kurman RJ, et al. Borderline ovarian
tumors:key points and workshop summary. Hum Pathol2004;
35:91017.
28 Kurman RJ, Shih IM. Molecular pathogenesis and extraovarian
originof epithelial ovarian cancer: shifting the paradigm. Hum
Pathol2001;42:91831.
29 Bell KA, Smith Sehdev AE, Kurman RJ. Refined diagnostic
criteria forimplants associated with atypical proliferative serous
tumours
(borderline) and micropapillary serous carcinoma. Am J Surg
Pathol2001; 25:41932.
30 Longacre T, Kempson RL, Hendrickson MR. Serous tumours of
lowmalignant potential (serous borderline tumours): moving
towarddtente. Histopathology 2005; 47:31518.
31 Zanetta G, Rota S, Chiari S, et al. Behavior of borderline
tumors withparticular interest to persistence, recurrence, and
progression toinvasive carcinoma: a prospective study.J Clin
Oncol2001;19:265664.
32 Gershenson DM, Silva EL, Tortolero-Luna G, et al. Serous
borderlinetumors of the ovary with noninvasive peritoneal implants.
Cancer1998; 83:215763.
33 Gershenson DM, Silva EG, Levy L, Burke TW, Wolf JK, Tornos
C.Ovarian serous borderline tumors with invasive peritoneal
implants.Cancer1998; 82:1096103.
34 Longacre TA, McKenney JK, Tazelaar HD, et al. Ovarian
seroustumors of low malignant potential (borderline
tumors):outcome-based study of 276 patients with long-term
(>5-year)
follow up. Am J Surg Pathol2005; 29:70723.35 Shih KK, Zhou QC,
Aghajanian C, et al. Patterns of recurrence and
role of adjuvant chemotherapy in stage IIIV serous
ovarianborderline tumors. Gynecol Oncol 2011; 120: 48084.
36 Seidman JD, Kurman RJ. Ovarian serous borderline tumors: a
criticalreview on the literature with emphasis on prognostic
factors.Hum Pathol2000; 31:52957.
37 Silva EG, Gershenson DM, Malpica A, et al. The recurrence and
theoverall survival rates of ovarian serous borderline neoplasms
withnoninvasive implants is time dependent. Am J Surg
Pathol2006;30:136771.
38 Bristow RE, Gossett DR, Shook DR, et al. Recurrent
micropapillaryserous ovarian carcinoma. Cancer 2002; 95:791800.
39 Prat J, De Nictolis M. Serous borderline tumors of the
ovary:a long-term follow-up study of 137 cases, including 18 with
amicropapillary pattern and 20 with microinvasion. Am J Surg
Pathol2002; 26:111128.
40 Slomovitz BM, Caputo TA, Gretz HF III, et al. A
comparativeanalysis of 57 serous borderline tumors with and without
anoninvasive micropapillary component. Am J Surg
Pathol2002;26:592600.
41 Goldstein NS, Ceniza N. Ovarian micropapillary serous
borderlinetumors: clinicopathologic features and outcome of seven
surgicallystaged patients. Am J Clin Pathol2000; 114:38086.
42 Hogg R, Scurry J, Kim SN, Friedlander M, Hacker N.
Microinvasionlinks ovarian serous borderline tumor and grade 1
invasivecarcinoma. Gynecol Oncol2007; 106:4451.
43 Laurent I, Uzan C, Gouy S, Pautier P, Duvillard P, Morice P.
Resultsafter conservative treatment of serous borderline tumors of
the ovarywith a micropapillary pattern. Ann Surg Oncol2008;
15:356166.
44 Uzan C, Kane A, Rey A, et al. Prognosis and prognostic
factors of themicropapillary pattern in patients treated for stage
II and III serousborderline tumors of the ovary. Oncologist2011;
16:18996.
45 Siriaunkgul S, Robbins KM, McGowan L, Silverberg SG.
Ovarianmucinous tumors of low malignant potential: a
clinicopathologic
study of 54 tumors of intestinal and mllerian type.Int J Gynecol
Pathol1995; 14:198208.
-
8/13/2019 yufi nakal
13/13
Review
46 Hoerl HD, Hart WR. Primary ovarian
mucinouscystadenocarcinomas: a clinicopathologic study of 49 cases
with
long-term follow-up. Am J Surg Pathol1998; 22:144962.47 Riopel
MA, Ronnett BM, Kurman RJ. Evaluation of diagnostic criteria
and behavior of ovarian intestinal-type mucinous tumors:
atypicalproliferative (borderline) tumors and intraepithelial,
microinvasive,invasive, and metastatic carcinomas. Am J Surg Pathol
1999; 23:61735.
48 Lee KR, Scully RE. Mucinous tumors of the ovary: a
clinicopathologicstudy of 196 borderline tumors (of intestinal
type) and carcinomas,including an evaluation of 11 cases with
pseudomyxoma peritonei.Am J Surg Pathol2000; 24:144764.
49 Nomura K, Aizawa S. Noninvasive, microinvasive, and
invasivemucinous carcinomas of the ovary: a clinicopathologic
analysis of40 cases. Cancer2000; 89:154146.
50 McKenney JK, Balzer BL, Longacre TA. Lymph node involvementin
ovarian serous tumors of low malignant potential
(borderlinetumors): pathology, prognosis, and proposed
classification.Am J Surg Pathol2006; 30:61424.
51 Kim KR, Lee HI, Lee SK, Ro JY, Robboy SJ. Is stromal
microinvasionin primary mucinous ovarian tumors with mucin
granuloma trueinvasion? Am J Surg Pathol 2007; 31:54654.
52 Koskas M, Uzan C, Gouy S, et al. Prognostic factors of a
largeretrospective series of mucinous borderline tumors of the
ovary(excluding peritoneal pseudomyxoma). Ann Surg
Oncol2011;18:4048.
53 Khunamornpong S, Settakorn J, Sukpan K, Suprasert
P,Siriaunkgul S. Mucinous tumor of low malignant
potential(borderline or atypical proliferative tumor) of the ovary:
a study of171 cases with the assessment of intraepithelial
carcinoma andmicroinvasion. Int J Gynecol Pathol2011; 30:21830.
54 Ronnett BM, Kajdacsy-Balla A, Gilks CB, et al. Mucinous
borderlineovarian tumors: points of general agreement and
persistentcontroversies regarding nomenclature, diagnostic
criteria, andbehavior. Hum Pathol2004; 35:94960.
55 Acs G. Serous and mucinous borderline (low malignant
potential)tumors of the ovary. Am J Clin Pathol2005;
123(suppl):S1357.
56 Hart WR. Mucinous tumors of the ovary: a review. Int J
Gynecol Pathol
2005; 24:425.57 Caduff RF, Svoboda-Newman SM, Ferguson AW,
Johnston CM,
Frank TS. Comparison of mutations of Ki-RAS and
p53immunoreactivity in borderline and malignant epithelial
ovariantumors. Am J Surg Pathol1999; 23:32328.
58 Kurman R, Shih IM. Pathogenesis of ovarian cancer: lessons
frommorphology and molecular biology and their clinical
implications.Int J Gynecol Pathol2008: 27:15160.
59 Rodrguez IM, Prat J. Mucinous tumors of the ovary:a
clinicopathologic analysis of 75 borderline tumors (of
intestinaltype) and carcinomas. Am J Surg Pathol2002; 26:13952.
60 Mackay HJ, Brady MF, Oza AM, et al, on behalf of the
GynecologicCancer InterGroup. Prognostic relevance of uncommon
ovarianhistology in women with stage III/IV epithelial ovarian
cancer.Int J Gynecol Cancer2010; 20:94552.
61 Bamias A, Psaltopoulou T, Sotiropoulou M, et al. Mucinous
butnot clear cell histology is associated with inferior survival
inpatients with advanced stage ovarian carcinoma treated with
platinum-paclitaxel chemotherapy. Cancer2010; 116:146268.62 Van
Calster B, Timmerman D, Bourne T, et al. Discrimination
between benign and malignant adnexal masses by
specialistultrasound examination versus serum CA-125.J Natl Cancer
Inst2007;99:170614.
63 Fauvet R, Boccara J, Dufournet C, Poncelet C, Dara
E.Laparoscopic management of borderline ovarian tumors: results of
aFrench multicenter study. Ann Oncol 2005; 16:40310.
64 Thomassin-Naggara I, Toussaint I, Perrot N, et al.
Characterization ofcomplex adnexal masses: value of adding
perfusion- and diffusion-weighted MR imaging to conventional MR
imaging. Radiology2011;258:793803.
65 Uzan C, Kane A, Rey A, Gouy S, Duvillard P, Morice P.
Outcomesafter conservative treatment of advanced-stage serous
borderlinetumors of the ovary. Ann Oncol2010; 21:5560.
66 Nomura K, Aizawa S, Hano H. Ovarian mucinous borderline
tumorsof intestinal type without intraepithelial carcinoma: are
they stilltumors of low malignant potential? Pathol Int2004;
54:42024.
67 Poncelet C, Fauvet R, Boccara J, Darai E. Recurrence after
cystectomyfor borderline ovarian tumors: results of a French
multicenter study.
Ann Surg Oncol2006; 13:56571.68 Morice P, Camatte C,
Larregain-Fournier D, Thoury A, Duvillard P,
Castaigne D. Port-site implantation after laparoscopic treatment
ofborderline ovarian tumors. Obstet Gynecol2004; 104:116770.
69 Lin PS, Gershenson DM, Bevers MW, Lucas KR, Burke TW, Silva
EG.The current status of surgical staging of ovarian serous
borderlinetumors. Cancer1999; 85:90511.
70 Fauvet R, Boccara J, Dufournet C, David-Montefiore E,
Poncelet C,Dara E. Restaging surgery for women with borderline
ovariantumors: results of a French multicenter study.
Cancer2004;100:114551.
71 Camatte S, Morice P, Rey A, et al. Impact of surgical staging
inpatients with macroscopic stage I ovarian borderline
tumours:analysis of a continuous series of 101 cases. Eur J
Cancer2004;40:184249.
72 Snider DD, Stuart GC, Nation JG, Robertson DI. Evaluation
ofsurgical staging in stage I low malignant potential ovarian
tumors.Gynecol Oncol1991; 40:12932.
73 Winter WE III, Kucera PR, Rodgers W, McBroom JW, Olsen
C,Maxwell GL. Surgical staging in patients with ovarian tumors of
lowmalignant potential. Obstet Gynecol2002; 100:67176.
74 Ramirez PT, Slomovitz BM, McQuinn L, et al. Role of
appendectomyat the time of primary surgery in patients with
early-stage ovariancancer. Gynecol Oncol2006; 103:88890.
75 Lesieur B, Kane A, Duvillard P, et al. Prognostic value of
lymph nodeinvolvement in ovarian serous borderline tumors. Am J
Obstet Gynecol2011; 204:438.e17.
76 McKenney JK, Balzer BL, Longacre TA. Patterns of stromal
invasionin ovarian serous tumors of low malignant potential
(borderlinetumors): a reevaluation of the concept of stromal
microinvasion.Am J Surg Pathol2006; 30:120921.
77 Fadare O, Orejudos MP, Jain R, et al. A comparative analysis
oflymphatic vessel density in ovarian serous tumors of low
malignantpotential (borderline tumors) with and without lymph
nodeinvolvement. Int J Gynecol Pathol2008; 27:48390.
78 Kanat-Pektas M, Ozat M, Gungor T, Sahin I, Yalcin H, Ozdal
B.Complete lymph node dissection: is it essential for the
treatmentof borderline epithelial ovarian tumors? Arch Gynecol
Obstet2011;283:87984.
79 Djordjevic B, Malpica A. Lymph node involvement in ovarian
seroustumors of low malignant potential: a clinicopathologic study
of36 cases. Am J Surg Pathol2010; 34:19.
80 Barakat RR, Benjamin I, Lewis JL Jr, Saigo PE, Curtin
JP,Hoskins WJ. Platinum-based chemotherapy for advanced-stageserous
ovarian carcinoma of low malignant potential. Gynecol Oncol1995;
59:39093.
81 Trop C, Kaern J, Vergote IB, Kristensen G, Abeler V. Are
borderlinetumors of the ovary overtreated both surgically and
systemically?A review of four prospective randomized trials
including 253 patientswith borderline tumors. Gynecol Oncol 1993;
51:23643.
82 Sutton GP, Bundy BN, Omura GA, Yordan EL, Beecham
JB,Bonfiglio T. Stage III ovarian tumors of low malignant
potentialtreated with cisplatin combination therapy (a Gynecologic
Oncology
Group study). Gynecol Oncol1991; 41:23033.83 Faluyi O, Mackean
M, Gourley C, Bryant A, Dickinson HO.
Interventions for the treatment of borderline ovarian
tumours.Cochrane Database Syst Rev2010; 9:CD007696.
84 Santillan A, Kim YW, Zahurak ML, et al. Differences
ofchemoresistance assay between invasive
micropapillary/low-gradeserous ovarian carcinoma and high-grade
serous ovarian carcinoma.Int J Gynecol Cancer2007; 17:60106.
85 Zanetta G, Rota S, Lissoni A, Meni A, Brancatelli G, Buda
A.Ultrasound, physical examination, and CA 125 measurement for
thedetection of recurrence after conservative surgery for early
borderlineovarian tumors. Gynecol Oncol2001; 81:6366.
86 Uzan C, Kane A, Rey A, et al. How to follow up
advanced-stageborderline tumours? Mode of diagnosis of recurrence
in a large seriesstage IIIII serous borderline tumours of the
ovary. Ann Oncol2011;22:63135.