Embed Size (px)
Citation preview
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 1 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWER
243 Proposal Submission Ms Gonzales is now Ms Fuentes. This is the same individual
306 N/A 31
187 WellCare N/A
15 Appendix B
292 Appendix C N/A 5
287 Appendix EE N/A 2
QUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
Coventry Health Care of Louisiana,
Inc.
4/18/2011 CCN-P
Proposers' Conference
Presentation
RFP
21.11.3
Slide 22;
p. 248
Slide 22 of the 4/18/2011 CCN-P Proposers' Conference Presentation indicates proposals should be submitted to Mary Fuentes, but page 248 of the RFP indicates Mary Gonzalez. Who is the correct person to send proposals to?
AmeriHealth Mercy of Louisiana
4/19/11 Conference
Highlights of ACG Risk Adjustment Model
Please advise as to whether the tentative decision to require 2 or more instances of a diagnosis to classify certain chronic conditions stands and clarify which conditions are impacted.
A study may be performed to evaluate the impact of the 2 or more diagnosis requirement on Louisiana's Medicaid population in the third quarter of this year using the data collected to support the cost weight development. See document in Procurement Library titled Chronic Conditions (Q 306)
4/19/2011 Rate
Conference Presentation
CCN-P (Prepaid Model) Rate Setting
Slide Page Number 12
"Best judgment" was used to arrive at the 14.69% overall managed care factor. Can Mercer share how "best" translates into this factor's position in the range of sound managed care factors? (i.e. 25th percentile?, median? etc.)
The positioning of rates within the range of actuarial soundness was decided by DHH in consultation with Mercer.
Coventry Health Care of Louisiana,
Inc.
# 12 on form
23.49 Termination for Convenience
1
271
Conflict between these 2 -- Section 23.49 says state can terminate for convenience; Appendix B says either party can terminate for convenience. Which is correct?
Appendix B, # 12 will be amended to indicate that DHH only can terminate for convenience.
§ 23.49 is correct.
AmeriHealth Mercy of Louisiana
HIPAA Business Associate Agreement
Section H.3. of Appendix C references Section F.3. of Appendix C; however, there is no Section F.3. Please clarify this reference.
Appendix C will be amended to correct the F.3 reference to F.2
AmeriHealth Mercy of Louisiana
Coordination of CCN Fraud and Abuse Complaints and
Referrals
Please clarify the timeframe for referral of suspected fraud or abuse to the Program Integrity Section. The 3 day timeframe referenced in Appendix EE appears to conflict with the timeframes for fraud and abuse referrals referenced in Sections 15.5 and 23.19.1 of the RFP.
3 business days as specified in Appendix EE is the correct timeframe for referral to Program Integrity. Section 15.5.1 refers to Federal Requirements and the 23.19.1 timeframe will be amended to "as soon as practical after discovering suspected incidents, but no more than 3 business days."

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 2 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
153 WellCare Appendix EE N/A 2
580 Appendix G N/A 20
1 Appendix G N/A 2
Coordination of CCN Fraud and Abuse Complaints and
Referrals
Please clarify the required reporting for fraud and abuse. Under "Fraud and Abuse Referrals," the CCN is responsible for reporting suspected fraud and abuse to the Program Integrity Section. However, the 3rd bullet references that the Medicaid Coordinated Care Section will send a copy to Program Integrity of any F&A reports received from the CCNs. Is this the F&A Activity Report referenced on page 218 of the RFP? How does the F&A Activity Report relate to the reporting described on page 186 of the RFP? And how does this report/these reports relate to the report referenced on the top of the 2nd page of Appendix EE (complaints data to Program Integrity monthly)?
No, the report on page 218 is a quarterly report. The third bullet under Fraud and Abuse Referrals in Appendix EE stating "The Medicaid Coordinated Care Section will send a copy to Program Integrity of any fraud and abuse reports received from the CCNs within three (3) business days" is for referrals made by the CCN to MCCS within three (3) business days.
The F&A Activity report is a quarterly report encompassing all activity in the timeframe. The format of this report is To Be Determined.
The report referred to in "The CCN will be required to capture data on complaints they receive and shall send reports to Program Integrity monthly" is requesting a monthly status update on each complaint.
United Healthcare of Louisiana
Administration & Profit Load Mercer Cert. & Rate Development
Can Mercer or DHH provide additional information regarding the assumptions for comparable programs used to determine the administrative portions of the rates.
No specific comparable information is available. However, Mercer considered the percentages used to be comparable to other states.
Coventry Health Care of Louisiana,
Inc.Rate Methodology
Overview
The Rate Development document mentions Inpatient & Outpatient cost reconciliations that are applied to the base data. Can you provide additional detail (beyond the overall impact shown in the Rate Development Overview) to help us understand the impact of these settlements? What providers will receive these settlements? What is the average amount these providers have received? Does this amount vary by provider, by Inpatient and Outpatient services, and has it varied over time for each provider?
These settlement amounts vary by hospital and from year to year. Average interim settlement for cost reports ending in 2009 was a recoupment of $110,461. Average interim settlement for cost reports ending in 2010 was a recoupment of $44,817.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 3 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
2 Appendix G N/A 2 Refer to answer to Question # 1
3 Appendix G N/A 2 yes- it varies by provider and varies from year to year.
5 Appendix G N/A 4 Yes
603 Appendix G N/A N/A 4
4 Appendix G N/A 4
433 Appendix G N/A 6 Yes
432 Appendix G N/A 6
604 Appendix G N/A N/A 7
Coventry Health Care of Louisiana,
Inc.Rate Methodology
OverviewAlso regarding Inpatient & Outpatient cost reconciliations applied to the base data, what is the average amount affected providers have received?
Coventry Health Care of Louisiana,
Inc.Rate Methodology
Overview
Also regarding Inpatient & Outpatient cost reconciliations applied to the base data, does the settlement amount vary by provider, by Inpatient and Outpatient services, and has it varied over time for each provider?
Coventry Health Care of Louisiana,
Inc.Retroactive Eligibility
(AA.3.4)
Mercer's databook mentions individuals other than newborns will not be enrolled in a health plan until up to 30 days following Medicaid eligibility. Is the enrollment process the same for members eligible due to pregnancy as it is for all other Medicaid-eligible members?
Children's Hospital Health Plan
Can Mercer share support for the IBNR assumptions and hospital cost settlements?
See Procurement Library document titled Incurred But Not Reported (IBNR) ( Q603)
Coventry Health Care of Louisiana,
Inc.
Incurred-but not-Reported Claims
Adjustments
Considering the data used by Mercer is net of TPL and subrogation, what would cause the IBNR completion factor for SFY09 to be negative (-0.07%)?
There could be a number of factors responsible. For example, late recoupments of overpayment, as well as late receipt of TPL and subrogation.
Coventry Health Care of Louisiana,
Inc.
FQHC and RHC Reimbursement
(AA.3.9)
CCN-Ps are required to pay FQHCs and RHCs at the current Prospective Payment System (PPS) rate. Can you provide CCNs with the historical PPS rates for FQHCs and RHCs between the beginning of the base data period (July 2008) through the current PPS rates?
Coventry Health Care of Louisiana,
Inc.Third-Party Liability
(AA.3.6)Is DHH currently using a vendor for identifying Third Party Liability and subrogation opportunities? If so, is DHH willing to share who the vendor is?
Currently DHH has a contractor to identify Third Party Liability. DHH performs subrogation in-house based on claim review and referrals from providers, insurance carriers and attorneys. The contractor is Health Management Systems (HMS).
Children's Hospital Health Plan
The overall annual trend rate applied was 3.67%. Could you share the data that was used to come to that amount?
Mercer divided statewide dollars after trending to phase 1 by statewide dollars before trending and then annualized the factor. The dollars are based off of SFY10 member months.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 4 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
6 Appendix G N/A Trend Development 7
7 Appendix G N/A 8
605 Appendix G N/A N/A 17 See document in Procurement Library
606 Appendix G N/A N/A 20
607 Appendix G N/A N/A 21
Coventry Health Care of Louisiana,
Inc.
When Mercer reviews Louisiana FFS claims data for trend development, how long of a time period is reviewed? Is it just the SFY09 and SFY10 data period included in the databook?
Mercer considered claims incurred from July 2007 through June 2010 for trend development. The data book only shows information for SFY09 and SFY10. As noted in Mercer’s certification letter and in the technical presentation, many other sources of trend information were considered in addition to Louisiana’s historical experience.
Coventry Health Care of Louisiana,
Inc.Trend Development
(Table)
The rate development narrative shows all categories of service with the exception of Outpatient Hospital and Emergency Room except unit cost trend of 0%. Understanding that unit cost reimbursement changes for other categories of service are handled explicitly through the "Fee Schedule Change" factor, do you expect there to be no other factors beyond fee schedule changes impacting unit cost? For instance, do you expect no increase in cost per service for new technologies or provider billing practice changes?
As discussed in the actuarial presentation, fee schedules are not expected to be increased during the projection period. The exception is an increase to 100% of Medicare for certain primary care codes effective 1/1/13 as required in the Affordable Care Act. Managed care organizations are expected to manage provider billing practice changes to ensure they do not inflate costs inappropriately. New technologies were considered in setting the utilization component of trend.
Children's Hospital Health Plan
Can you share the Mercer preventable hospital admissions study?
Children's Hospital Health Plan
By keeping all outlier claims in the baseline the rates have accounted for their expected costs, but reinsurance companies require margin and that has not been accounted for.
The decision to reinsure or not is up to the individual CCN after considering all of the related issues, including any margin. As stated in the rate letter, profit and margin load of 1.8% was included in the rates.
Children's Hospital Health Plan
The document references that Mercer created a range of actuarially sound rates by rate cell? Can the ranges be shared with the bidders?
The actuarially sound rate ranges have been developed, and the Capitation Rates are within the actuarially sound ranges. DHH has elected not to disclose at the placement in the rate range.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 5 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
438 Appendix G N/A Risk Adjustment 21
437 Appendix G N/A 21
8 Appendix G N/A 24
608 Appendix G N/A N/A N/A
609 Appendix G N/A N/A N/A
Coventry Health Care of Louisiana,
Inc.
To what extent will members' Mental Health and Pharmacy FFS data be used in calculating risk scores for risk adjustment of a CCN's rates?
Pharmacy data will not be used in the disease classification process. Mental health and physical health providers and related diagnoses will be used in the disease classification process. The costs associated with pharmacy (CCN-P version only) and specialized mental health will be excluded from the cost weight development.
Coventry Health Care of Louisiana,
Inc.Rate Development
OverviewWill DHH make available to CCNs the member-level risk score detail, so that CCNs can understand the basis for their risk scores?
The ACG model agreement with Medicaid agencies precludes the sharing of member-level results. Please see the response to #487, which describes the reporting that will be provided.
Coventry Health Care of Louisiana,
Inc.Attachment A - CCN-P
Rate Summary
Comparing the CY2012 rates gross of GME to the previous rate development from the mid-2010 shows an overall decrease of ~6% (adjusted to the SFY10 population mix) even though the current rates are for a later time period than were the previous rates. What drivers lead you to expect that the costs for this population have decreased since the rates were previously in mid-2010?
As indicated in the actuarial presentation, no analysis has been attempted of the impact of the various differences between the previous set of draft rates and the final ones, primarily due to the rebasing of the base data. A few of the potential differences include: use of claims from SFY 2010, a roughly 2% provider rate cut, a reconsideration of trends based on the more recent base data, and a reassessment of the likelihood of fee schedule increases in the next few years.
Children's Hospital Health Plan
Will the 2013 rates utilize any managed care data or will it mimic the approach used for 2012? When will managed care experience be incorporated in the process?
This has yet to be determined. It depends, for example, on success in obtaining encounter data from CCNs.
Children's Hospital Health Plan
Individually the admin, profit, and managed care savings assumptions may be reasonable, but collectively they are conflicting. Large managed care savings can not be achieved without admin expenses on the high side. Would DHH consider a higher admin rate in year 1 to support maximum effort to impact costs sooner?
The rates do incorporate high admin expenses for low PMPMs and low admin expenses for high PMPMs. Mercer considers the admin rates to be adequate.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 6 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
610 Appendix G N/A N/A N/A
611 Appendix G N/A N/A N/A Will Medicaid only plans be subject to premium tax? No
305 Appendix G N/A 29
578 Appendix G N/A 16
288 Appendix G N/A 2
189 WellCare Appendix G N/A 2
Children's Hospital Health Plan
There can be significant variation in the incidence of premature babies across the CCNs. The risk adjustment methodology currently does not account for members under age 1. Would DHH consider either risk adjusting those members or doing some sort of carve out for low birth weight babies?
Due to the limited (non-existent) information regarding newborn risk variation in the initial years of the CCN programs, the newborn rates will not be risk adjusted and there will not be any further delineation to the rate structure to account for low birth weight babies. These policies may be revisited once some historical experience exists on the newborn risk variation.
Children's Hospital Health Plan
AmeriHealth Mercy of Louisiana
Attachment B - Rate Development Overview
Our understanding is that hospital cost settlements to date have been reflected in the rate setting process. Is it DHH's intent to adjust the rates at a future time to reflect additional cost settlements? What are expected future settlements for the time periods used in rate setting?
No further adjustments to the capitation rates are planned. See response to question 430 for details as to which settlements have been included and why DHH does not believe additional settlements will have a material impact.
United Healthcare of Louisiana
Data Smoothing & Managed Care
Assumptions - Mercer Cert. & Rate
Development
Did Mercer adjust the Managed Care Savings (MCS) factors for GSA's 2 and 3 since the MCOs will have less than 12 months to achieve the same savings levels of GSA 1?
The same managed care factors were used to generate savings for all three GSAs. The absolute dollar savings will vary by GSA based on the duration of the program due to staggered program start dates. Impact of savings by elapsed time is hard to quantify.
AmeriHealth Mercy of Louisiana
Rate Methodology - Overview
The rating document indicates that an actuarially sound range was developed for each cell and region, and that the published rates fall within that range. Is it possible for the ranges to be published to gain a better understanding of the width of the rate range?
The actuarially sound rate ranges have been developed, and the Capitation Rates are within the actuarially sound ranges. DHHS prefers that the placement in the rate range not be disclosed.
Attachment A CCN-P Rate Summary
Please confirm whether "unpaid claim reserves" includes reserves for all incurred dates not just limited to the current MLR Reporting Year. For example, the reserve total will also include provision for liabilities for prior MLR Reporting Years if such liabilities remain, even after closing the reporting for that MLR Reporting Year.
The unpaid claim reserves includes consideration for all liabilities incurred but not paid or reported within the dates of service outlined in the Data book.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 7 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
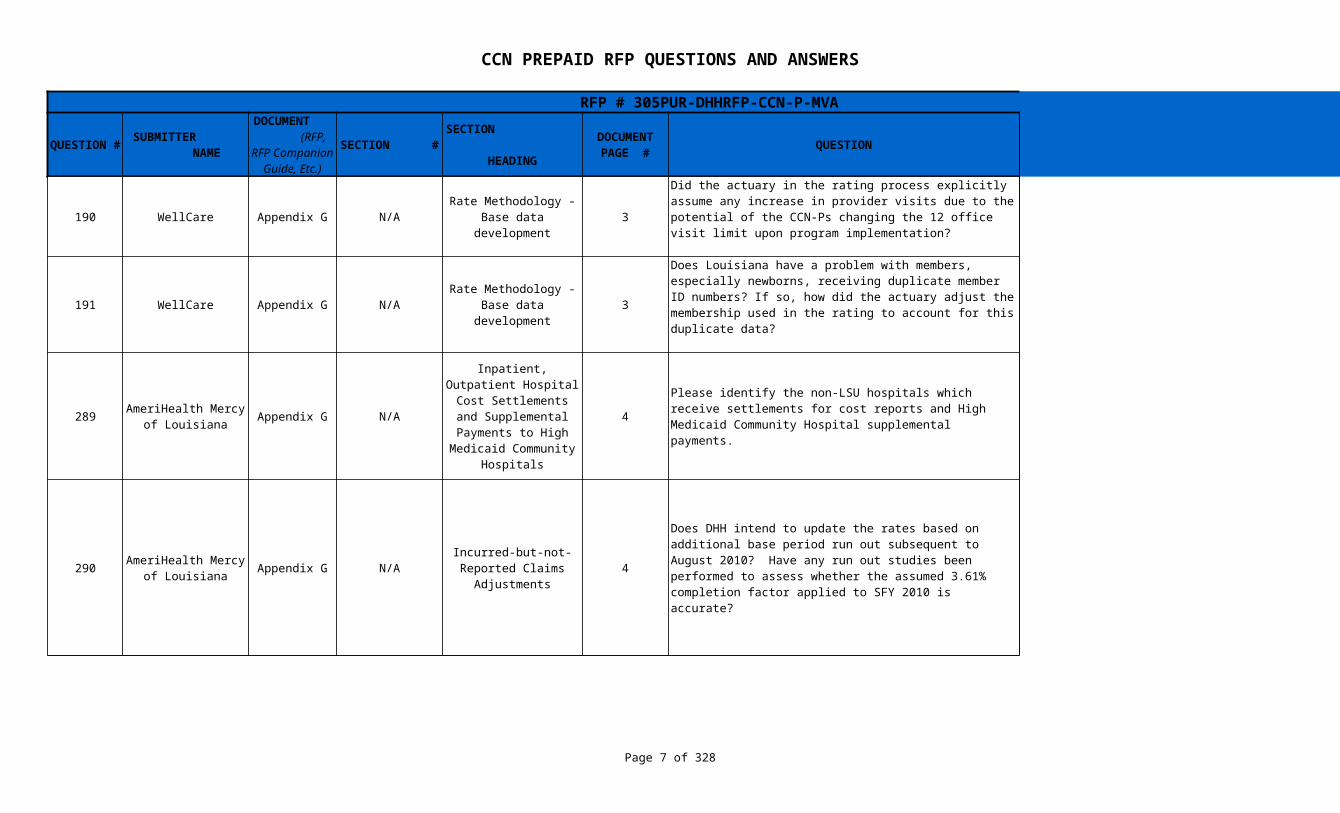
190 WellCare Appendix G N/A 3
191 WellCare Appendix G N/A 3 No, the incidence of duplicate IDs was immaterial.
289 Appendix G N/A 4
290 Appendix G N/A 4
Rate Methodology - Base data development
Did the actuary in the rating process explicitly assume any increase in provider visits due to the potential of the CCN-Ps changing the 12 office visit limit upon program implementation?
CCN-Ps change the 12 visit limit we would expect this to be because they expect to generate savings elsewhere.
Rate Methodology - Base data development
Does Louisiana have a problem with members, especially newborns, receiving duplicate member ID numbers? If so, how did the actuary adjust the membership used in the rating to account for this duplicate data?
AmeriHealth Mercy of Louisiana
Inpatient, Outpatient Hospital Cost
Settlements and Supplemental
Payments to High Medicaid Community
Hospitals
Please identify the non-LSU hospitals which receive settlements for cost reports and High Medicaid Community Hospital supplemental payments.
See document in Procurement Library titled Hospitals Receiving Cost Settlements (Q-289)
AmeriHealth Mercy of Louisiana
Incurred-but-not-Reported Claims
Adjustments
Does DHH intend to update the rates based on additional base period run out subsequent to August 2010? Have any run out studies been performed to assess whether the assumed 3.61% completion factor applied to SFY 2010 is accurate?
The IBNR estimates included in the rates are the best estimate of incurred claims for the data used in rate setting. Sufficient consideration has been included by Mercer for outstanding claims liability that would be representative of the total cost of the program in any given year. The magnitude of the factor used in SFY 2010 is deemed appropriate based on Mercer's review of the claims runout considered in the IBNR development. No additional adjustments would be applied prior to the implementation of the program due to IBNR reconsideration.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 8 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
430 Appendix G N/A 4
431 Appendix G N/A 4
Coventry Health Care of Louisiana,
Inc.
Inpatient, Outpatient Hospital Cost
Settlements, and Supplemental
Payments to High Medicaid Community
Hospitals –
The Rate Development document mentions Inpatient and Outpatient cost settlements based on cost reports, and the adjustment Mercer applies to the base data to capture their impact varies significantly between the 2 base data years (3.6% for SFY09 and 1.3% for SFY10). Can DHH provide an explanation of the process and timing by which CCNs will cost settle with providers?
Mercer's rate development, specifically the adjustment you reference, reflects all cost settlements paid through the beginning of SFY11. DHH advises that, for most hospitals, 2010 fiscal year preliminary settlements have been included but final settlements have not. DHH also advises that final settlements are not expected to materially change the aggregate payment. There could be a number of reasons for the difference between the two years, one of them being that DHH paid out $50 million in cost settlements more in SFY09 than SFY10 to LSU hospitals for inpatient services. The process and timing of settlements between CCNs and hospitals will depend on each CCN's contract with each hospital. DHH simply requires that the amount paid to the hospital, including any settlement, not be less than the equivalent FFS amount, also including any settlement.
Coventry Health Care of Louisiana,
Inc.
Inpatient, Outpatient Hospital Cost
Settlements, and Supplemental
Payments to High Medicaid Community
Hospitals –
The Rate Development document mentions Inpatient and Outpatient cost settlements based on cost reports. Are these settlement amounts based strictly on Medicaid utilization for the providers, or on some other basis?
Yes, where the Medicaid FFS methodology for a hospital provider includes a cost settlement provision, the settlements are based on Medicaid utilization.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 9 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
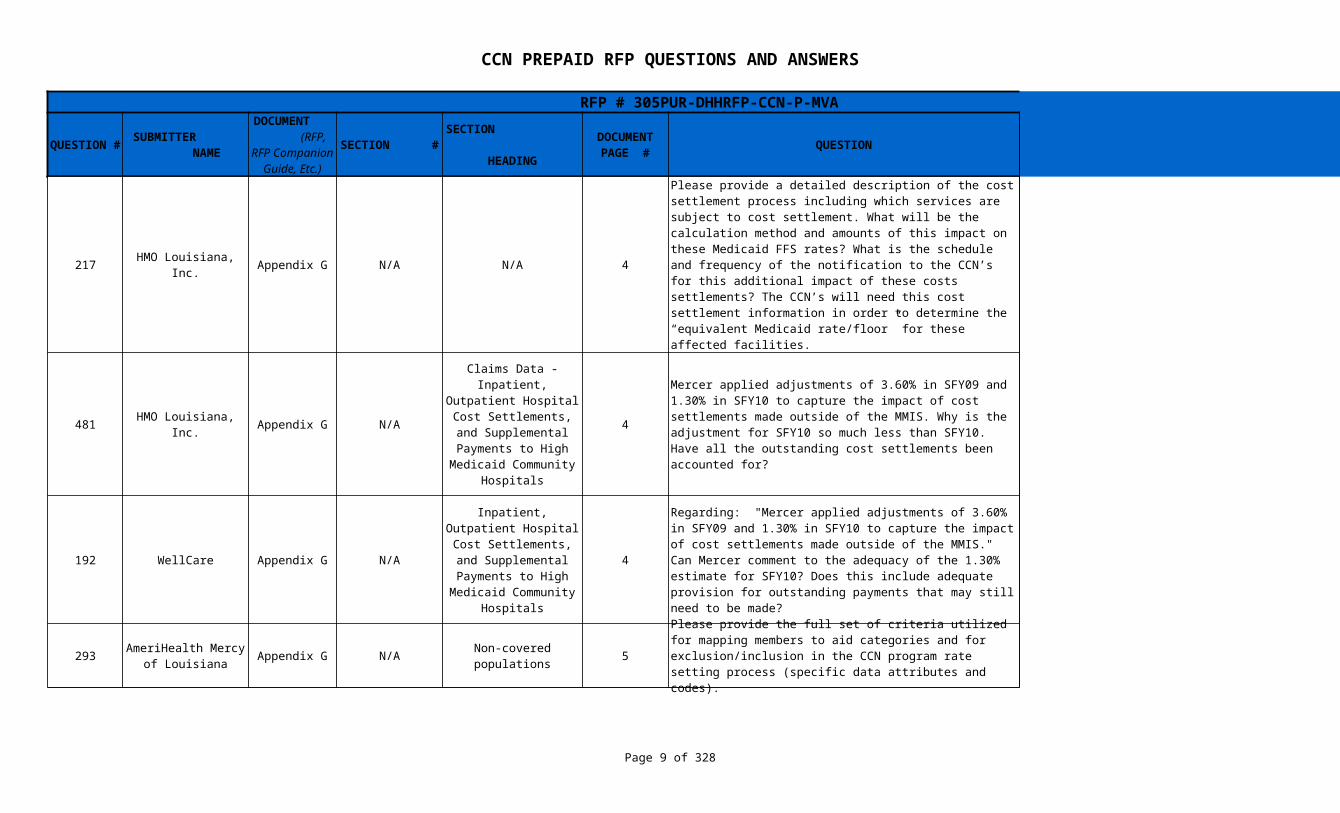
217 HMO Louisiana, Inc. Appendix G N/A N/A 4
481 HMO Louisiana, Inc. Appendix G N/A 4 See responses to #387 and #430.
192 WellCare Appendix G N/A 4
293 Appendix G N/A 5
Please provide a detailed description of the cost settlement process including which services are subject to cost settlement. What will be the calculation method and amounts of this impact on these Medicaid FFS rates? What is the schedule and frequency of the notification to the CCN’s for this additional impact of these costs settlements? The CCN’s will need this cost settlement information in order to determine the “equivalent Medicaid rate/floor” for these affected facilities.
Small rural hospitals: all outpatient services except labs are cost settled at 110% of costs. State owned hospitals: All outpatient and inpatient services (except labs) are cost settled at 100% of costs. Children's specialty hospitals: all outpatient services (except labs) are cost settled at 86.15% of costs. Inpatient services are cost settled at 88.82% of costs. All other in-state hospitals: Non-fee schedule outpatient services are cost settled at 69.71% of costs. Hospitals file cost reports annually throughout the year.
Claims Data - Inpatient, Outpatient Hospital
Cost Settlements, and Supplemental
Payments to HighMedicaid Community
Hospitals
Mercer applied adjustments of 3.60% in SFY09 and 1.30% in SFY10 to capture the impact of cost settlements made outside of the MMIS. Why is the adjustment for SFY10 so much less than SFY10. Have all the outstanding cost settlements been accounted for?
Inpatient, Outpatient Hospital Cost
Settlements, and Supplemental
Payments to High Medicaid Community
Hospitals
Regarding: "Mercer applied adjustments of 3.60% in SFY09 and 1.30% in SFY10 to capture the impact of cost settlements made outside of the MMIS." Can Mercer comment to the adequacy of the 1.30% estimate for SFY10? Does this include adequate provision for outstanding payments that may still need to be made?
In Mercer's opinion, the adjustments are appropriate. See responses to #387, #430 and #481.
AmeriHealth Mercy of Louisiana
Non-covered populations
Please provide the full set of criteria utilized for mapping members to aid categories and for exclusion/inclusion in the CCN program rate setting process (specific data attributes and codes).
Refer to Procurement Library document titled Category of Assistance (COA) Crosswalk (Q 293)
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 10 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
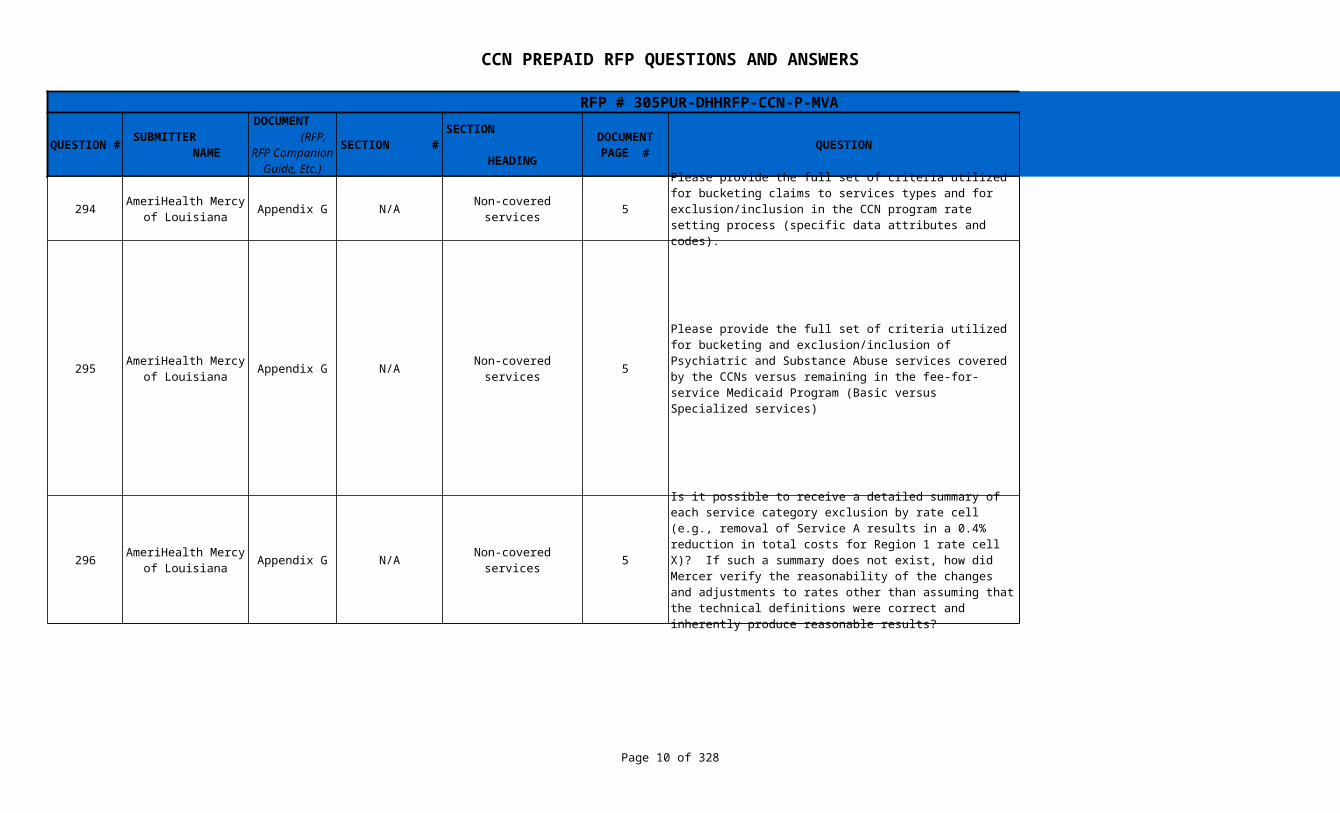
294 Appendix G N/A Non-covered services 5
295 Appendix G N/A Non-covered services 5
296 Appendix G N/A Non-covered services 5
AmeriHealth Mercy of Louisiana
Please provide the full set of criteria utilized for bucketing claims to services types and for exclusion/inclusion in the CCN program rate setting process (specific data attributes and codes).
Refer to Procurement Library document titled Category of Service (COS) Crosswalk (Q294)
AmeriHealth Mercy of Louisiana
Please provide the full set of criteria utilized for bucketing and exclusion/inclusion of Psychiatric and Substance Abuse services covered by the CCNs versus remaining in the fee-for-service Medicaid Program (Basic versus Specialized services)
Mercer identified and excluded Specialized behavioral health services through the following codes (except for FQHC/RHC facilities which are still responsible for those services):CLC_Claim_Cat_Serv = 02, 10, 11, 42, 50, 74, or 79 orCLP_Serv_Prov_Type = 69, 96, 18, 31, 64, 68, 74, or 77orCLP_Serv_Prov_Spec1 = 26, 27, 62, 78, 95, 96, 4D, 5H, 5M, 6A, 6B, 6C, 6D, 6E, 6F, or 9BorCLH_Treat_Place = 51, 52, 53, 55, 56, or 57.
Mercer then identified basic behavioral services through the following primary diagnosis codes:290.xx-319.xx
AmeriHealth Mercy of Louisiana
Is it possible to receive a detailed summary of each service category exclusion by rate cell (e.g., removal of Service A results in a 0.4% reduction in total costs for Region 1 rate cell X)? If such a summary does not exist, how did Mercer verify the reasonability of the changes and adjustments to rates other than assuming that the technical definitions were correct and inherently produce reasonable results?
This is not possible because data for services and populations other than those to be included in CCNs have not been captured. Mercer has no reason to believe that DHH's fiscal agent has not accurately assigned service codes.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 11 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
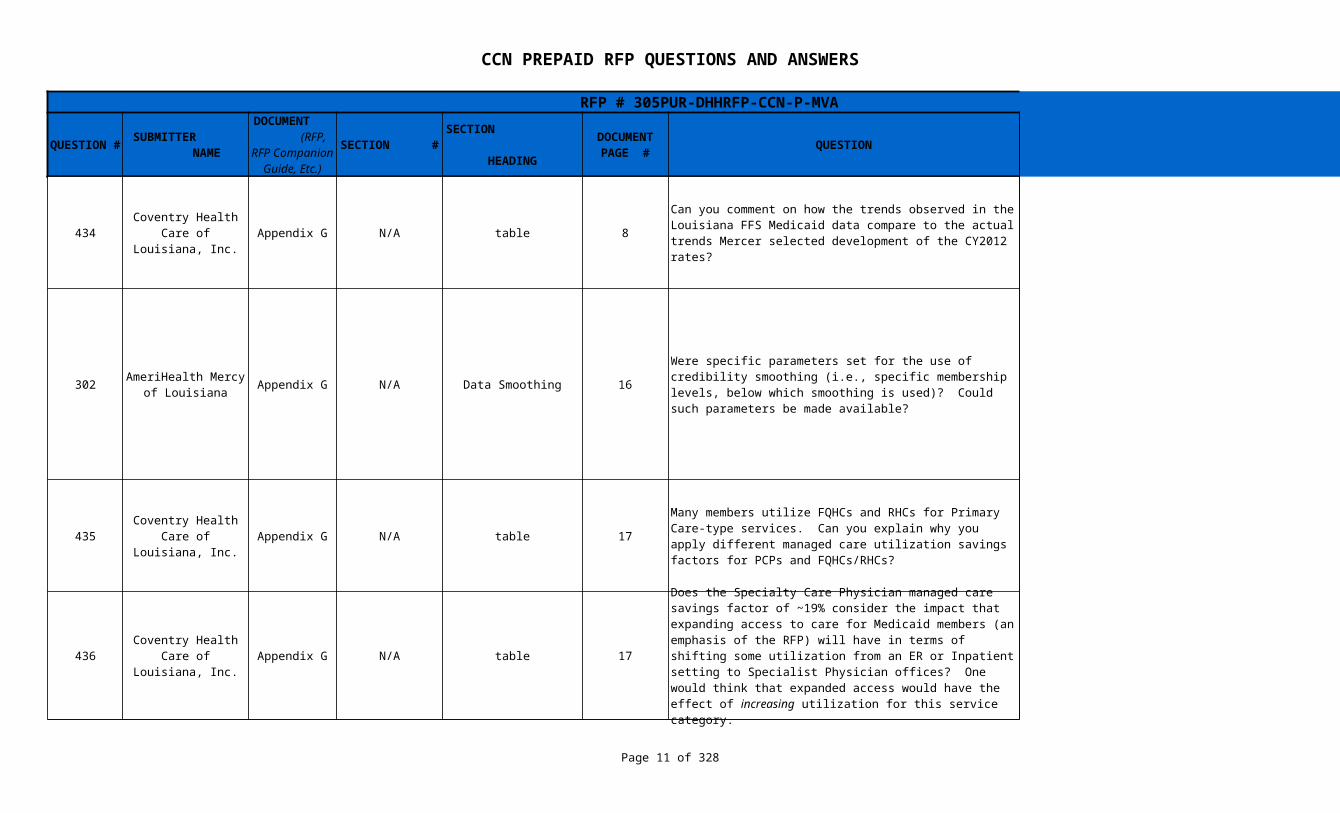
434 Appendix G N/A table 8
302 Appendix G N/A Data Smoothing 16
435 Appendix G N/A table 17
436 Appendix G N/A table 17
Coventry Health Care of Louisiana,
Inc.
Can you comment on how the trends observed in the Louisiana FFS Medicaid data compare to the actual trends Mercer selected development of the CY2012 rates?
Mercer considered FFS claims incurred from July 2007 through June 2010 for trend development. The data book only shows information for SFY09 and SFY10. As noted in Mercer’s certification letter and in the technical presentation, many other sources of trend information were considered in addition to Louisiana’s historical experience.
AmeriHealth Mercy of Louisiana
Were specific parameters set for the use of credibility smoothing (i.e., specific membership levels, below which smoothing is used)? Could such parameters be made available?
100% weighting of statewide PMPMs were applied for SSI children, C&F adults not including 19-44 Females, Foster Care Children, and Breast and Cervical Cancer rate cells due to low membership in those categories at the regional level. The impact of smoothing can be seen on a rate cell by rate cell basis in the exhibits to the certification letter. No adjustment was made for regional differences. Member months for those categories were distinctively lower than the rest. Although there was not a specific threshold Mercer set for data smoothing, the member months for these categories were below 30,000.
Coventry Health Care of Louisiana,
Inc.
Many members utilize FQHCs and RHCs for Primary Care-type services. Can you explain why you apply different managed care utilization savings factors for PCPs and FQHCs/RHCs?
The utilization of primary-care type services in FQHCs/RHCs is generally less than in a traditional PCP arrangement. Managed care assumptions within those two service categories are set to incentivize the use of primary care services and it is anticipated there would be more of an uptick in the PCP category. In addition, FQHC/RHC data is a mix of PCP/SCP.
Coventry Health Care of Louisiana,
Inc.
Does the Specialty Care Physician managed care savings factor of ~19% consider the impact that expanding access to care for Medicaid members (an emphasis of the RFP) will have in terms of shifting some utilization from an ER or Inpatient setting to Specialist Physician offices? One would think that expanded access would have the effect of increasing utilization for this service category.
While the managed care savings factors did not explicitly consider impact of expansion, this factor was considered and built in other pricing assumptions. For example, reduction of inpatient days should reduce SCP services.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 12 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
193 WellCare Appendix G N/A 20
195 WellCare Appendix G N/A 24 See response to #545.
196 WellCare Appendix G N/A 24
197 WellCare Appendix G N/A 24 This has not been analyzed.
194 WellCare Appendix G N/A 24 NICU costs are isolated in the newborn capitation rate cells.
Commercial Reinsurance
Will the "detailed data" (to be provided by the state via secure disk) provide a basis to assess high dollar claimants experience? For example, will claims include a unique member identifier so that claims can be accumulated to assess aggregate annual membership spend? This is important to be able to assess reinsurance strategy. In the absence of this information, will DHH be able to provide some experience regarding the incidence and severity of high dollar claimants?
A revised data set including a dummy member ID is being prepared. This will enable CCNs to aggregate an individual's claims to understand high claiming patterns. However you will not know whether or not you will enroll them.
Attachment A CCN-P Rate Summary
Is there a reason that some of the cost settlement adjustments shown in the rate development are greater than 1.00 and some are less than 1.00?
Attachment A CCN-P Rate Summary
Given the relatively high rate for the 0-2 month rate cell, why wasn't a different NICU kick payment established?
Various rate cell structures were considered before finalizing.
Attachment A CCN-P Rate Summary
What factors drive the higher New Orleans maternity delivery payment? Are these driven by higher complexity in the case mix?
Attachment A CCN-P Rate Summary
Can you confirm whether any costs for NICU cases are in the maternity cells, or are they isolated in the newborn capitation rate cells?
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 13 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
476 HMO Louisiana, Inc. Appendix G N/A 25
477 HMO Louisiana, Inc. Appendix G N/A 25
478 HMO Louisiana, Inc. Appendix G N/A 25
Claims Data - Inpatient, Outpatient Hospital
Cost Settlements, and Supplemental
Payments to HighMedicaid Community
Hospitals
Please provide a detailed description of the cost settlement process. Specifically, what services are subject to cost settlement, and how the amounts will be quantified for the rate setting process.
Under DHH's current process for cost settlements, hospitals are paid a per diem rate based on the fee schedule. For hospitals subject to cost settlements, DHH pays a percentage of cost to the hospitals based on the hospitals' cost reports. If DHH already paid more than this new amount, then DHH will recoup money from the hospitals. If DHH had paid less than this new amount, then DHH will need to make up the difference to the hospitals. These cost settlement amounts were provided by DHH and were netted out by fiscal year, region, and outpatient versus inpatient services by Mercer. Any changes in percentage of costs from the base data period to the effective period are reflected in the fee schedule changes adjustments. See the State Plan for further details on the cost settlement process.
Claims Data - Inpatient, Outpatient Hospital
Cost Settlements, and Supplemental
Payments to HighMedicaid Community
Hospitals
What is the justification in the regional variances in the cost settlement adjustment factors? For example, the SFY09 cost settlement factor for SSI (0-2 months, Male and Female) for New Orleans is 1.1296, whereas the factor for Mandeville is 1.0135.
Each region's specific adjustment was based on the cost settlements of the hospitals within the region. More of the New Orleans hospitals qualify for cost settlement.
Claims Data - Inpatient, Outpatient Hospital
Cost Settlements, and Supplemental
Payments to HighMedicaid Community
Hospitals
What is the justification in the rating category variances in the cost settlement adjustment factors? For example, the SFY09 cost settlement factor for New Orleans for SSI (3-11 months, Male and Female) is 1.1174, whereas the factor for Family and Children (3-11 months, Male and Female) is 1.0475.
The cost settlement adjustments are the same across rate cells at the inpatient and outpatient service level. However, when the total dollars by category of service are summed up in aggregate by rate cell, the impact of the cost settlement adjustment will differ. Typically there is more hospitalization and thus more settlement for SSI.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 14 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
479 HMO Louisiana, Inc. Appendix G N/A 26 See response to #430.
480 HMO Louisiana, Inc. Appendix G N/A 27 See response to #430.
421 Appendix G N/A N/A 30
469 HMO Louisiana, Inc. Appendix G N/A 34
470 HMO Louisiana, Inc. Appendix G N/A 34
Claims Data - Inpatient, Outpatient Hospital
Cost Settlements, and Supplemental
Payments to HighMedicaid Community
Hospitals
What cost settlements are still outstanding for SFY09 and SFY10?
Claims Data - Inpatient, Outpatient Hospital
Cost Settlements, and Supplemental
Payments to HighMedicaid Community
Hospitals
How have any outstanding cost settlements for FY09 and FY10 been incorporated into the rate development?
AmeriHealth Mercy of Louisiana
The risk adjustment methodology document states that risk adjustment will begin with the fourth month of operation in a given region. We recommend that risk adjustment should begin with the first month. If significant adverse selection occurs, 3 months of non risk adjusted revenue could represent a significant financial disadvantage for the affected plan. If administrative timing is a concern, this revenue could be adjusted retroactively.
The decision to delay the risk adjustment process allows the CCN-Ps to anticipate its revenue for the initial quarter of the program. Furthermore, it allows DHH to wait until after the enrollment stabilizes (after the initial two months) to evaluate the health risk attraction patterns.
Programmatic Changes/Rate Issues
Were there any changes in scope of covered services from SFY09 to SFY10 for services included in the CCN-P program?
No changes in scope of services occurred from SFY09 to SFY10.
Programmatic Changes/Rate Issues
Are there any future planned changes to the scope of covered services that have occurred or will occur post SFY10 for services included in the CCN-P program?
No such plans exist at this time within CCN core benefits and services.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 15 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
471 HMO Louisiana, Inc. Appendix G N/A 34 See response to #386.
472 HMO Louisiana, Inc. Appendix G N/A 34 See response to #386.
473 HMO Louisiana, Inc. Appendix G N/A 34 See response to #386.
474 HMO Louisiana, Inc. Appendix G N/A 34 Yes, that is the intent.
475 HMO Louisiana, Inc. Appendix G N/A 34
390 Appendix G N/A 2/16 No decision has been made regarding future rate setting.
386 Appendix G N/A 10 - 12
Programmatic Changes/Rate Issues
Please provide an itemization of each of the fee schedule changes with the date it was implemented. Also, please indicate which fee schedule adjustments are applicable to the SFY09 and SFY10 data.
Programmatic Changes/Rate Issues
What data was used in the calculation of the adjustments for fee schedule changes?
Programmatic Changes/Rate Issues
How was the data used in the calculation of the adjustments for fee schedule changes analyzed to arrive at the adjustment factors used in the rate setting process?
Programmatic Changes/Rate Issues
Are the adjustment factors for fee schedule changes intended to adjust the SFY09 and SFY10 to be on a CY12 basis based on fee schedule changes that happened during and after each of the SFYs?
Programmatic Changes/Rate Issues
Are there any future planned fee schedule changes that would impact the CY2012 claim costs?
Mercer is not aware of any additional adjustments at this time.
AmeriHealth Mercy of Louisiana
Rate Methodology - Overview / Data
Smoothing
The published rates are based on two years of base data (SFY 2009 and SFY 2010). In the development these base periods are weighted 40% and 60%, respectively. Is it DHH's intent to continue using two base period years in future rate developments, and if so, will the 40% and 60% weights continue to be used?
AmeriHealth Mercy of Louisiana
Programmatic Changes / Rate Issues
The process documentation memo does not contain the information necessary to validate the reimbursement adjustments made to the base data. The document explains the most recent reimbursement change by category of care (inpatient, physician ,etc.), but does not include a full listing of all reimbursement changes that have occurred since the beginning of SFY 2009. A comprehensive list including all changes would allow for validation of the adjustment factors calculated by Mercer.
All other reimbursement changes through 1/1/2011 should be posted on DHH's fee schedule website (http://www.lamedicaid.com/provweb1/fee_schedules/feeschedulesindex.htm). We did not want to make the certification document any longer or more complex than necessary or to risk misleading a reader regarding any details in an attempt to be concise.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 16 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
387 Appendix G N/A 10-12
422 Appendix G N/A N/A 30-43
395 Appendix G N/A 6 & 7
AmeriHealth Mercy of Louisiana
Programmatic Changes/Rate Issues
Per this reference "The per diem rates for state hospitals have increased significantly since the base data period, however this primarily affects the relative weights of the per diems versus cost settlements and has little impact on the total payment". Do the per diem rates as currently posted on the State website (effective date of 8/1/2010, revised 8/28/2010) include cost settlement amounts (cost report and/or High Medicaid supplemental payments) and are they reflective of the changes noted in regards to State hospital rates? If not, when we may anticipate that updated per diem rates will be posted for all facilities? Likewise, please provide current outpatient cost-to-charge ratios for all facilities.
The per diem rates for state hospitals as of 8/28/2010 do not include cost settlement amounts or the 2% rate cut on 1/1/2011. Refer to Procurement Library document titled DHH Interim Outpatient Rates by Hospital (Q 387) for current outpatient cost-to-charge rates.
AmeriHealth Mercy of Louisiana
The risk adjustment methodology document states that members new to Medicaid, that are not included in the risk score assignment process, will be assumed to have the region average score of the given population. We recommend that for a plan that has significant adverse selection and credible membership size, that these new members be assigned the average score of the plan for the given population. It is reasonable to assume that the acuity attraction patterns (influenced by relative networks and programs) would apply to new members as well. This is a practice used in many other states.
Since the CCN-P program is new, it is possible that those unscored members may have different attraction patterns than the scored members. This assumption will likely be revisited over time and may change once more history exists within the new program.
AmeriHealth Mercy of Louisiana
Rate Category Groupings
Please advise as to which rate cell contains well baby admits and days: the under age 1 rate cell or the maternity kick payment cell ? Please provide a separate count of these admits and days.
The 0-2 months rate cells contain Well Baby admits and days. For SFY09, Well Baby days are 43,907 and admits are 13,171. For SFY10, days are 41,969 and admits are 12,162. Note these numbers are raw and uncompleted.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 17 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
396 Appendix G N/A 6 & 7
404 Appendix G N/A N/A
429 Appendix G N/A N/A N/A The unit of measurement is Trips.
229 HMO Louisiana, Inc. Appendix G N/A N/A N/A See response to #386.
230 HMO Louisiana, Inc. Appendix G N/A N/A N/A See response to #386.
231 HMO Louisiana, Inc. Appendix G N/A N/A N/A
232 HMO Louisiana, Inc. Appendix G N/A N/A N/A See response to #548.
AmeriHealth Mercy of Louisiana
Rate Category Groupings
Please provide a detailed listing with detailed codes of all services included in the maternity kick payment rate.
See Procurement Library document titled Maternity Codes (Q396)
AmeriHealth Mercy of Louisiana
Rate Methodology - Overview
What is the overall level of targeted managed care savings in the current set of rates (managed care savings less MCO admin plus marginal FFS admin as compared to managed care)? Will a similar target remain going forward?
Very approximately, Managed care is expected to reduce claims by 15% with much of the savings being offset by CCN administration, yielding a net savings of 3-4%.
Coventry Health Care of Louisiana,
Inc.
In the summarized databook, what unit and unit per 1,000 measure is used for Emergency Transportation and Non-Emergency transportation? Is it miles, trips, or some other unit?
Fee schedule adjustments - What data was used as the basis for the adjustments for fee schedule changes?
Fee schedule adjustments - How was that data analyzed to arrive at the adjustment factors used in the rate setting process?
Fee schedule adjustments - What is the justification of the variance in the fee schedule adjustments across the different rating categories? For example, the Inpatient Hospital adjustment for SFY09 for SSI is -6.01% whereas the adjustment for Family and Children is -9.63%.
The fee schedule adjustments are the same across rate cells at the category of service level. However, when the total dollars by category of service are summed up in aggregate by rate cell, the impact of the fee schedule adjustment will differ. Fee schedule adjustments are different by year, category of aid, and category of service.
Managed Care Adjustments - What information and/or data was used to arrive at the managed care utilization and unit cost assumptions?
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 18 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
233 HMO Louisiana, Inc. Appendix G N/A N/A N/A
234 HMO Louisiana, Inc. Appendix G N/A N/A N/A
235 HMO Louisiana, Inc. Appendix G N/A N/A N/A
236 HMO Louisiana, Inc. Appendix G N/A N/A N/A
237 HMO Louisiana, Inc. Appendix G N/A N/A N/A
238 HMO Louisiana, Inc. Appendix G N/A N/A N/A See response to #477.
Managed Care Adjustments - What is the justification of the large negative managed care utilization assumptions for Inpatient Hospital, Outpatient Hospital, Specialty Physician Care, Lab/Radiology, DME, Clinic, and Emergency Room services.
These categories typically afford the largest opportunities for savings when a managed care program is implemented for the first time in a FFS care setting as shown by other managed care programs. The value of managed care is reflected when care giving is provided in appropriate settings and the managed care percentages reflect these changes.
Managed Care Adjustments - What is the basis and rationale behind the difference in managed care utilization adjustment for Inpatient Hospital services between the Family and Children rating category and the other rating categories? The managed care utilization assumption for Family and Children is -33.70%, whereas for the other rating categories it is -23.67%.
The Managed Care assumptions for Inpatient Hospital services varied between the Family and Children rating category and all others to reflect service utilization differences. It is anticipated additional savings could be generated through efficient MCO management of care for the Family and Children rating category, which had unusually high service utilization from the base data used for rate setting.
IP and OP Hospital Cost Settlements - Please provide an itemization of all adjustments which are included in the cost settlement factors.
See Document in Procurement Library titled In-patient (IP) and Out Patient (OP) Cost Settlement Adjustments (Q235)
IP and OP Hospital Cost Settlements - What data was used as the basis for the IP and OP Hospital Cost Settlement adjustment factors used in the rate setting process?
Adjustment factors were based on the State's actual aggregate settlement payments. Also see response to #476.
IP and OP Hospital Cost Settlements - What was the process by which that data was analyzed to arrive at the cost settlement adjustment factors used?
Historical payments were compared to per diem amounts. Also see response to #476.
IP and OP Hospital Cost Settlements - What is the justification in the regional variances in the cost settlement adjustment factors? For example, the SFY09 cost settlement factor for SSI (0-2 months, Male and Female) for New Orleans is 1.1296, whereas the factor for Mandeville is 1.0135.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 19 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
239 HMO Louisiana, Inc. Appendix G N/A N/A N/A See response to #478.
228 HMO Louisiana, Inc. Appendix G N/A N/A N/A
579 Appendix G N/A 21
717 Appendix G N/A Trend - Attachment B 29 - 36
726 Aetna Appendix G N/A 16
IP and OP Hospital Cost Settlements - What is the justification in the rating category variances in the cost settlement adjustment factors? For example, the SFY09 cost settlement factor for New Orleans for SSI (3-11 months, Male and Female) is 1.1174, whereas the factor for Family and Children (3-11 months, Male and Female) is 1.0475.
Fee schedule adjustments - Please provide an itemization of each of the fee schedule changes with the date it was implemented. Also, please indicate which fee schedule adjustments are applicable to the SFY09 and SFY10 data.
Refer to Administrative Rules included in the Louisiana Register
United Healthcare of Louisiana
Risk Adjustment - Mercer Cert. & Rate
DevelopmentHow will the risk scores be developed, by plans overall or by GSA?
The risk scores will be developed for each GSA. So, if a CCN-P operates in two GSAs, they will be provided with two sets of risk scores.
Aetna Better Health, Inc.
How was trend for FY09 to FY10 determined? What adjustments were applied to differentiate this trend from the trend applied to the weighted FY10 trend?
Mercer considered claims incurred from July 2007 to June 2010 by category of service and category of aid for utilization and cost categories. SFY09 and SFY10 data was trended to the effective period using appropriate trend at service and aid categories.
Managed Care Assumptions
In the Rate Conference meeting April 19th, 2011, it was mentioned that regional PMPM costs were trended differently to reflect the various implementation phases. While the cost differential is represented in the trend, please comment why this is not also reflected in the managed care savings assumptions. For example, if 20% managed care savings are achievable over twelve months, approximately 13% would be achievable over eight months on a proportionate basis. The treatment of the managed care savings assumption is not consistent with the treatment of trended PMPM costs.
The impact of trend is directly related to the length of the trending period. The impact of managed care assumptions would require complex assumptions about timing of impact. This is unlikely to be linear.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 20 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
721 Appendix G N/A Data Smoothing 16
724 Appendix G N/A 16
725 Appendix G N/A 20 An outliers file is included in the data extract.
716 Appendix G N/A Trend 8-10
719 Appendix G N/A Programmatic Changes 10 - 11
720 Appendix G N/A Programmatic Changes 10 - 11
Aetna Better Health, Inc.
Please provide more detail on how smoothing was performed by rate cell. How have regional unit cost differences been taken into account in the development?
100% weighting of statewide PMPMs were applied for SSI children, C&F adults not including 19-44 Females, Foster Care Children, and Breast and Cervical Cancer rate cells due to low membership in those categories at the regional level. The impact of smoothing can be seen on a rate cell by rate cell basis in the exhibits to the certification letter. No adjustment was made for regional differences.
Aetna Better Health, Inc.
Managed Care Assumptions
We noticed that while the overall managed care savings assumption is 14.7%, it is significantly higher for newborns (20-26%). Please provide information supporting this higher managed care savings assumption for these rate cells.
Managed care rates as well as savings opportunities are highest for the newborns rate cell. Good prenatal care and access to PCP services should help generate larger savings for this rate cell. There appears to be significant opportunities to reduce newborn length of stay, particularly if low birth weights are addressed.
Aetna Better Health, Inc.
Commercial Reinsurance
Please provide detail on the outlier claims that were built into the rates. For example PMPM by rate cell as well as total claims per member.
Aetna Better Health, Inc.
Please explain how the unit cost trend of 0% was calculated. It does not appear to be reasonable that there would be no unit cost increases for physicians, FQHC's, nurses, labs, home health care, transportation, DME, and inpatient services from 2008 - 2012. Was the unit cost trend developed based on the medical cost index for the state of Louisiana or was it based on the trend in Medicaid fee-for-service payments?
Please note that most Medicaid fee schedules have been cut and are expected to remain frozen during this period.
Aetna Better Health, Inc.
Can you break down the total programmatic changes by each programmatic change and by rate cell?
Refer to Procurement Library document titled Fee Schedule Adjustments (Q 719)
Aetna Better Health, Inc.
How has Mercer accounted for increased utilization by providers to offset the fee schedule decreases in the programmatic changes?
Appropriate provisions have been made within the trend factors and managed care assumptions to allow for physician practice changes. However, the MCO is responsible for monitoring appropriate provider utilization within the capitation payments on an ongoing basis.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 21 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
573 WellPoint Appendix G N/A -
722 Appendix G N/A AA.3.0 p. 6, AA.3.0
392 N/A N/A See response to #610.
612 Appendix H N/A N/A 1
In the Louisiana rates, there is a separate rate category for “Breast and Cervical Cancer, All Ages”.
Are these regular TANF members who get identified with these conditions? Or are they a separate population all together?
This is the optional Breast and Cervical Cancer Program created by Public Law `106-354 for uninsured women under the age of 65 and not otherwise eligible for Medicaid who are screened by a CDC certified screening program. The income limit for the CDC program is 250% FPL.
Aetna Better Health, Inc.
Please describe the rationale for removing this fee from the rate development? How much was paid to providers on a total dollar and PMPM basis? How have Community Care access payments been incorporated in the rate development?
For prepaid plans, CMS rules require that the PCCM fee not be used in determining capitation rates. The CCN-P administrative load was determined considering the case management and primary care services applicable to the program.
AmeriHealth Mercy of Louisiana
Appendix G; Louisiana
Medicaid CCN Program Actuarial
Briefing Dated 4/19/12
34-36 (Actuarial Briefing)
It is our understanding that DHH does not intend to risk adjust the 0-2 month and 3-12 month rate cells. It is very possible that different network strategies among health plans may result in disparate levels of risk within these rate cells. Has DHH performed sensitivity/scenario analysis around the impact of network strategy on the relative risk of the <12 month rate cells among plans? Other states use relatively straightforward risk adjustment techniques such as low birth weight kicker payments.
Children's Hospital Health Plan
States that if 50% of more of the total capitation payment is received for members with less than 12 months of experience, then the experience of those members will be excluded from that MLR report. Does DHH expect the MLR report to apply in 2012?
It is possible some CCNs will have more than 50% of their capitation payments for members with 12 months of experience in MLR Reporting Year 2012. Additionally, experience may be excluded; CCNs have the option to not defer reporting until the next MLR Reporting Year.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 22 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
9 Appendix H N/A 1
439 Appendix H N/A 1 Yes
440 Appendix H N/A 1
441 Appendix H N/A 1
Coventry Health Care of Louisiana,
Inc.Reporting
Requirements - C.
Because CCNs can exclude members with fewer than 12 months of experience from their MLR reporting for purposes determining MLR requirements (if 50% or more of the CCNs capitation payment is attributable to these members), does that mean CCNs can forgo reporting their MLR in 2012 as by definition all members will have fewer than 12 months of experience, and instead report both their 2012 and 2013 aggregate experience in their CY2013 MLR reporting?
A CCN operating in GSA A only beginning 1/12 will have 12 months experience for 100% of is members. Others may have more than 50% of their capitation payment attributable to members who have been in the plan for 12 months. CCNs in which 50% or more of the annual capitation payment is attributable to members with less than 12 months of experience have the option of reporting both their 2012 and 2013 aggregate experience in their CY 2013 MLR reporting.
Coventry Health Care of Louisiana,
Inc.Medical Loss Ratio
(MLR) RequirementsAre the additional health benefits described in Section S.2 of the CCN-P Proposal Evaluation considered "Paid Claims" for purposes of MLR reporting?
Coventry Health Care of Louisiana,
Inc.
Reporting Requirements
B. Timing and Form of Report
Appendix H states that the denominator of a CCN's MLR includes all capitation payments received from DHH. How is a CCN to treat capitation payments received in one reporting year for the previous reporting year? For instance, delivery kick payments often have a lag of one or more months, so kick payments for births occurring in December of one reporting year are likely to continue trickling in through January and February of the next reporting year.
Capitation payments--defined as "all monies paid by DHH to the CCN for providing core benefits and services as defined in the terms of the contract" are to be counted in the MLR Reporting year in which they are actually received.
Coventry Health Care of Louisiana,
Inc.
Reporting Requirements
D. Capitation Payments
How are retroactive capitation payment adjustments (either positive or negative) for an MLR reporting year received after reporting has been done to be accounted for? Will the CCN be able to reflect those retroactive amounts in the following reporting year?
Yes, these are reflected for the MLR Reporting Year in which they actually occur.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 23 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
576 Appendix H N/A 1
442 Appendix H N/A 2
443 Appendix H N/A 3
444 Appendix H N/A C. Exclusions 5 Yes
United Healthcare of Louisiana
Medical Loss Ratio (MLR) Refund
Since 100% of the capitation payments in CY 2012 will be for new members, and an MCO has the option to exclude the experience of new members if they constitute greater than 50% of the total capitation payment, Is it expected that an MCO would not an MLR Refund calculation to DHH for CY 2012 by August 1, 2013?
It is possible for 50% or more of capitation payments received by a plan in 2012 to be for members with 12 months experience, assuming a January 2012 go live date. DHH's expectation is that some CCNs may not submit a MLR Report for 2012 because of the degree of new experience and will combine 2012 experience with the 2013 report.
Coventry Health Care of Louisiana,
Inc.
Reimbursement for Clinical Services
Provided to Enrollees
On occasion, CCNs must establish a premium deficiency reserve (PDR) when expected premiums for a future period of time are insufficient to cover future medical costs and administrative expenses. How are CCNs to account for PDRs for purposes of reporting their MLR?
Premium Deficiency Reserve are not an allowable cost in calculating the MLR ratio for Louisiana Medicaid
Coventry Health Care of Louisiana,
Inc.
Activities that Improve Health Care Quality
B. Activity Requirements
Appendix H includes a list of requirements an activity must be designed to do in order to be considered as a quality-improvement activity ("Activities that Improve Health Care Quality", B.1. a.-j.). The list of requirements includes 10 items an activity must be designed to do in order to be considered improving quality. Must every activity meet every one of the 10 requirements? Many requirements do not seem relevant for each individual activity.
An activity need not meet all 10 requirements. It must meet at least one of the requirements
Coventry Health Care of Louisiana,
Inc.
Appendix H states that CCNs can not include activities "designed primary to control or contain costs" as quality improvement activities. If activities are intended to improve the quality of care and meet such requirements, but at the same time reduce medical costs as well, can CCNs include such activities in the MLR calculation?
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 24 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
567 WellPoint Appendix H N/A -
613 Appendix H N/A N/A N/A No
614 Appendix H N/A N/A N/A No
10 Appendix H N/A
784 Appendix H N/A N/A
We surmise that Appendix H, defining medical loss ratio, may have been developed prior to HHS enacting a federal regulation in November 2010 which defined with great specificity and consistency the calculation of medical loss ratio. The new federal regulation mandates all US health insurance companies comply with the NAIC MLR federal definition beginning 1/1/11. The federal regulation was approved unanimously by all 50 state insurance commissioners. Will the state consider conforming in the future to the NAIC MLR definition rather than requiring a definition that varies from the consistent definition required for all other external reporting purposes?
DHH's MLR definition and policy and Appendix H were developed after enactment of the federal regulation. The federal regulation is not applicable to the Medicaid product. DHH will not consider further liberalization of the MLR definition for Louisiana Medicaid managed care that is contained in the RFP and Appendix H.
Children's Hospital Health Plan
The federal MLR rules take into consideration credibility based on the number of covered lives. Will DHH consider that?
Children's Hospital Health Plan
Because of the cyclical nature of profit and loss in Managed Medicaid, other states allow for loss carry forwards to offset profits in current years when calculating profit sharing. Will DHH consider incorporating that approach with the MLR calculation?
Coventry Health Care of Louisiana,
Inc.
NAIC recommends a credibility adjustment based on membership in the calculation of MLR for compliance with minimum MLR thresholds. Is there a reason DHH doesn't consider adopting a credibility adjustment for smaller CCNs whose financial experience is likely to fluctuate?
Size of the CCN is not a factor in DHH's MLR expectation for CCNs. The DHH policy is an adaptation for Louisiana Medicaid managed care and not an exact replica of the MLR policy for commercial insurance.
Amerigroup Corporation
Medical Loss Ratio (MLR) Requirements
What are the rules for including prescription drug rebates? Are both paid and accrued rebates included?
Prescription drugs dispensed at pharmacies are excluded from core benefits and services under the Contract.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 25 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
789 Appendix H N/A N/A
790 Appendix H N/A N/A
792 Appendix H N/A N/A
791 Appendix H N/A N/A
Amerigroup Corporation
Medical Loss Ratio (MLR) Requirements
In settling the 85% MLR cap, can the plan include all incentive payments to providers?
See Appendix H, Page 2 which states Adjustments that may (emphasis ours) be included in incurred claims:a. The amount of incentive and bonus payments made to providers
Amerigroup Corporation
Medical Loss Ratio (MLR) Requirements
Please clarify the premium tax provisions applied to premium paid to each health plan: a. Will premium tax be added to the published premium capitation? b. If yes, the premium tax component of premium revenue should be excluded from the denominator for purposes of calculating the MLR for each health plan? c. How are retroactive premium adjustments processed in the following year handled in determining the premium amount in the MLR report? d. Are there any special provisions health plans should be aware of related to premium taxes, reporting, and performance measurement?
a. Premium tax will not be added to the published premium capitation b. N/A c. Premiums--including any adjustments are shown for the MLR Reporting Year in which the payment are adjustment actually occurs. D. Not that we know of at this time
Amerigroup Corporation
Medical Loss Ratio (MLR) Requirements
Can you confirm that overpayment recoveries are reported on a date of service basis? If so, how will a health plan and the state account for recoveries after the reporting period run-out?
That is correct. They would be reported for the next MLR Reporting Year.
Amerigroup Corporation
Medical Loss Ratio (MLR) Requirements
Please clarify the run-out period for claims payments/IBNR on the MLR report: a. Is it 3 months after the reporting year or March 31? b. Are payments made more than 3 months after the reporting period not included on any MLR report? c. Confirm that IBNR as of March 31 for prior year service dates can be included in the MLR report? d. Will there be any consideration of possibly extending the run-out period for calculating any rebate owed?
Refer to the explanation on Page 2 of Appendix H. DHH did not define a "run out period" however Unpaid Claim Reserves are defined as reserves and liabilities established to account for claims that were incurred during the MLR reporting year but had not been paid within 3 months of the end of the MLR reporting year. Payments made more than 3 months after the reporting period should be accounted for in Unpaid Claim Reserves (see Page 2 of Appendix H) c. That is correct d. No

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 26 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
154 WellCare N/A N/A
621 Appendix I N/A N/A
615 Appendix I N/A 183 It is not a Medicaid covered service for ages 21 to 65
104 Appendix I N/A
419 Appendix II N/A N/A
491 HMO Louisiana, Inc. Appendix J N/A 1
Appendix H and Appendix
KKMedical Loss Ratio
(MLR) Requirements
Please confirm that the State intends that additional health benefits/value-added services, as specified in S.2 of Appendix KK, be treated as "medical" expenses for purposes of the MLR, either as "clinical services" or "activities that improve health care quality." Please describe/identify any value-added services that would not be included as "medical."
DHH's intent is that additional health benefits/value added services be classifiable as medical expenses for purposes of MLR, either as clinical services or activities that improve health care quality.
Children's Hospital Health Plan
Louisiana State Plan Services
This one-page Attachment I lists various benefit categories and indicates their applicability to CCN-P requirement to manage. The benefit line "Behavioral/Mental Health (Non-EPSDT)" indicates for CCN-P that we're responsible for BASIC LEVEL ONLY. Would DHH please clarify what this means? Specifically, which BH/MH services are the CCN-P's responsible to manage?
See Glossary for definition of Basic Behavioral Health and Specialized Behavioral Health; also Section § 6.3.4 of the RFP as well as the Medicaid State Plan and policy manual located in the procurement library.
Children's Hospital Health Plan
Louisiana State Plan Services
Inpatient Psychiatric Services for Children under 21 and adults over age 65, what about all ages in between?
Coventry Health Care of Louisiana,
Inc.Louisiana State Plan
Services1 (183
showing on document)
Is there a listing available of what organs are covered for transplants?
Transplant Rule has been added to CCN-P Procurement Library under Benefits and Services.
AmeriHealth Mercy of Louisiana
CCN Model Attestation Letter for Reports
Please clarify for what type of reports the CCN is supposed to submit the attestation set for in Appendix II versus the Quarterly Certification Statement in the CCN-P Financial Reporting Companion Guide.
The attestation is applicable for all reports submitted to DHH.
Louisiana CCN Administrative Performance
Measurement Set
What percent of Call Center calls answered by a live person incurs a penalty if not answered within 30 seconds?
90% or greater calls must be answered within 30 seconds. This can be by a live operator or the IVR automated system. However, wait time on the phone line to talk to a live person cannot exceed three minutes. This performance standard will be modified to include the option of an automated IVR system answering the line within 30 minutes. This language has been modified. See Addendum #4.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 27 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
450 Appendix J N/A All
445 Appendix J N/A N/A See Question # 365
622 Appendix J N/A N/A Yes
155 WellCare Appendix JJ N/A N/A
530 WellPoint Appendix KK F.5 28
517 WellPoint Appendix KK 53
Coventry Health Care of Louisiana,
Inc.
Louisiana CCN Administrative Performance
Measurement Set
Will reporting on performance measures be by contract or GSA?
All performance measures shall be reported as an entity . An entity is corporate level and may cover multiple GSAs. Entities with common corporate structure will be reviewed and evaluated statewide, not by GSA.
Coventry Health Care of Louisiana,
Inc.
Louisiana CCN Administrative Performance
Measurement Set
Can DHH provide an explanation of how they intend to establish CCN benchmarks for the Incentive Based, Level I, and Level II performance measures? Will CCN risk scores be taken into account in setting these benchmarks, and if so, how will risk scores be incorporated?
Children's Hospital Health Plan
Louisiana CCN Administrative Performance
Measurement Set
In the conference on April 19 we discussed the NCQA certification of plans' HEDIS data. Please confirm, do plans need to obtain NCQA certification of their self-reported HEDIS measurements?
Demonstration and Assessment of System
Readiness
When will DHH provide to the CCN a test plan that will outline the activities thatneed to be performed by the CCN prior to the Go-Live Date of the Contract?
Refer to Appendix H of Systems Companion Guide
Does Medicaid have a fee schedule for telemedicine and what is the prior approval process for telemedicine from the State?
There is no fee schedule for telemedicine and there is no PA process. Providers bill their claims with the GT modifier to denote that it is a telemedicine claim
R.3
The second paragraph refers to “(a)”.
Is this referring to the first paragraph? Can the State provide any further clarification on what the State is seeking in response to this second paragraph?
Language has been amended to change language from "(a)" to " paragraph above". With the aforementioned correction, we believe the paragraph is self-explanatory.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 28 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
304 Appendix KK 28
314 Appendix KK EPSDT System 37
AmeriHealth Mercy of Louisiana F.3
Coordinating Carved-Out Services
What services are provided under "Targeted Case Management"?
access to needed medical, social, educational, and other services. TCM includes the following assistance: Comprehensive assessment and periodic reassessment of individual needs, to determine the need for any medical, educational, social, or other services. These assessment activities include taking client history, identifying the individual’s needs and completing related documentation; and gathering information from other sources such as family members, medical providers, social workers, and educators (if necessary), to form a complete assessment of the eligible individual; • Development and periodic revision of a specific care plan that is based on the information collected through the assessment that is based on the information collected through the assessment that specifies the goals and actions to address the medical, social, educational, and other services needed by the individual; includes activities such as ensuring the active participation of the eligible individual, and working with the individual (or the individual’s authorized health care decision maker) and others to develop those goals; and identifies a course of action to respond to the assess needs of the eligible individual; • Monitoring and follow-up activities and contacts that are necessary to ensure the care plan is implemented and adequately addresses the eligible individual’s needs, and which may be with the individual, family members, service providers, or other entities or individuals and conducted as frequently as necessary, and including at least one annual monitoring, to determine whether the following conditions are met: services are being furnished in accordance with the individual’s care plan; services in the care plan are adequate; and changes in the needs or status of the individual are reflected in the care plan. Monitoring and follow-up activities include making necessary adjustments in the care plan and service arrangements with providers.
AmeriHealth Mercy of Louisiana I.1
Does the state have a system for tracking immunizations provided by clinics or during special health promotions? Are they required to also use the Louisiana Immunization Network for Kids (LINKS) ?
Yes the LINKS system. Vaccines for Children (VFC) users are currently mandated to use the LINKS system. It is also a requirement for CommunityCARE 2.0 provider participation.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 29 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
462 Appendix KK B.10 10
464 Appendix KK F.8 Service Coordination 34
465 Appendix KK G.4 Provider Network 36 Should the reference to G.3 in this question be to G.1? Yes
466 Appendix KK G.1 Provider Network 40 Should this question be labeled G.15 instead of G.1? Yes
467 Appendix KK M.2 55 For bullet point 1 - is the number 30,000 or 50,000?
446 Appendix KK S.2 64
468 Appendix KK R.12 Information Systems 67
451 Appendix KK S.2 73
463 Appendix KK C.2 and C.4 25 & 27
Coventry Health Care of Louisiana,
Inc.Qualifications and
ExperienceIs there a specific reason the last 4 digits of the social security # are needed? Can these be sent directly to DHH so has not to be included in the RFP response?
For validation of identity purposes. DHH will provide a secure way for CCNs to provide this information in the event previous DHH employees are employed by the CCN.
Coventry Health Care of Louisiana,
Inc.
If there is no moral and religious objection to providing services, is there a need to describe plans to provide services (e.g. birth control)?
F. 8 is only applicable if the CCN is claiming moral or religious objections
Coventry Health Care of Louisiana,
Inc.
Coventry Health Care of Louisiana,
Inc.
Coventry Health Care of Louisiana,
Inc.Emergency
Management Plan Thirty thousand; Amended to read " You have thirty thousand (30,000)
Coventry Health Care of Louisiana,
Inc.Added Value to
Louisiana
For the additional health benefits described in Sect S.2 of the Proposal Submission document, can the additional benefits offered be contingent on the member first undertaking certain actions (such as a PCP visit) that encourage improved health outcomes?
Yes, but the assumption on the impact of the condition(s) that must be met on utilization must be included in the actuarial certification of the value of the benefit.
Coventry Health Care of Louisiana,
Inc.
Is DHH looking for an organizational chart to answer this question? If not, what is the DHH preferred answer format for this question.
DHH is not requesting an organizational chart to meet this requirement. There is no preferred response format.
Coventry Health Care of Louisiana,
Inc. Added Value to
LouisianaWill home health visits to pregnant members be considered an additional benefit to members?
Home health is a mandatory service and therefore would not be considered an additional benefit unless it is in excess of the 50 visit annual limit for enrollees age 21 and over or more than 1 visit daily .
Coventry Health Care of Louisiana,
Inc.Planned Approach to
Project What is the difference between C.2 and C.4? The questions appear to be one in the same.
C.2 is the narrative; C-4 refers to the Microsoft Project or comparable product
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 30 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
264 Appendix KK R.10, bullet 3 Information Systems pg. 236
265 Appendix KK R.1, Bullet 3 Information Systems
266 Appendix KK R.1, Bullet 3 Information Systems What format will the authorizations be in?
12 Appendix KK N/A 15
529 WellPoint Appendix KK F.3 27
285 Appendix KK B 9,12
161 WellCare Appendix KK B.10 10 May we include resumes/job descriptions as an attachment? Yes
Coventry Health Care of Louisiana,
Inc.
What is the expectation of the state? What kind of ad-hoc reports? What kind of access do they expect to have to the systems?
As stated in Section 16.10.2, CCNs shall allow DHH personnel, agents of the Louisiana Attorney General's Office or individuals authorized by DHH or the Attorney General's office direct access to its data for the purpose of data mining and review. Access may be remote or on-site. The ad hoc report could be to extract any data contained in the system.
Coventry Health Care of Louisiana,
Inc.
Please confirm that we will receive two one time files one on claims and one on auths for our “initial” set of enrollees for each region. we would receive daily enrollment incremental files with a weekly full file.
That is correct. In addition Medicaid claims data for carved out services will be refreshed weekly on an ongoing basis. The daily and weekly enrollment files will be the responsibility of the Enrollment Broker.
Coventry Health Care of Louisiana,
Inc.That information will be added to the Systems Companion Guide
Coventry Health Care of Louisiana,
Inc.
Part II. Technical Approach -
Qualifications and Experience
Can the CCN limit its response to those affiliates that conduct Medicaid business. If we have to include information for our affiliates, which are commercial health plans, the response to this question will require a considerable amount of research across all commercial affiliate companies which would be quite onerous to gather.
No. DHH considers contract termination due to breach of contract to be relevant whether it was for Medicaid business or non-Medicaid business.
Who are the high-volume providers for dental, specialized behavioral health, personal care services and targeted case management?
Refer to the Medicaid Provider Listing in the Procurement Library which can be sorted by provider type and includes number of unduplicated recipients.
Louisiana Healthcare Connections
Qualifications and Experience
Question B.8 asks for an org chart showing structure and lines of responsibility. This chart is to be marked Chart A. Question B.9 and Question B.12 also ask for Org Charts, however the instructions only state that B.12 should be marked Chart B. Should B.9 be marked Chart B. and B.12 be marked Chart C.?
The Organizational Chart requested in Question B9 is that of the proposed Louisiana operation. It should be clearly labeled as such.
Qualifications and Experience
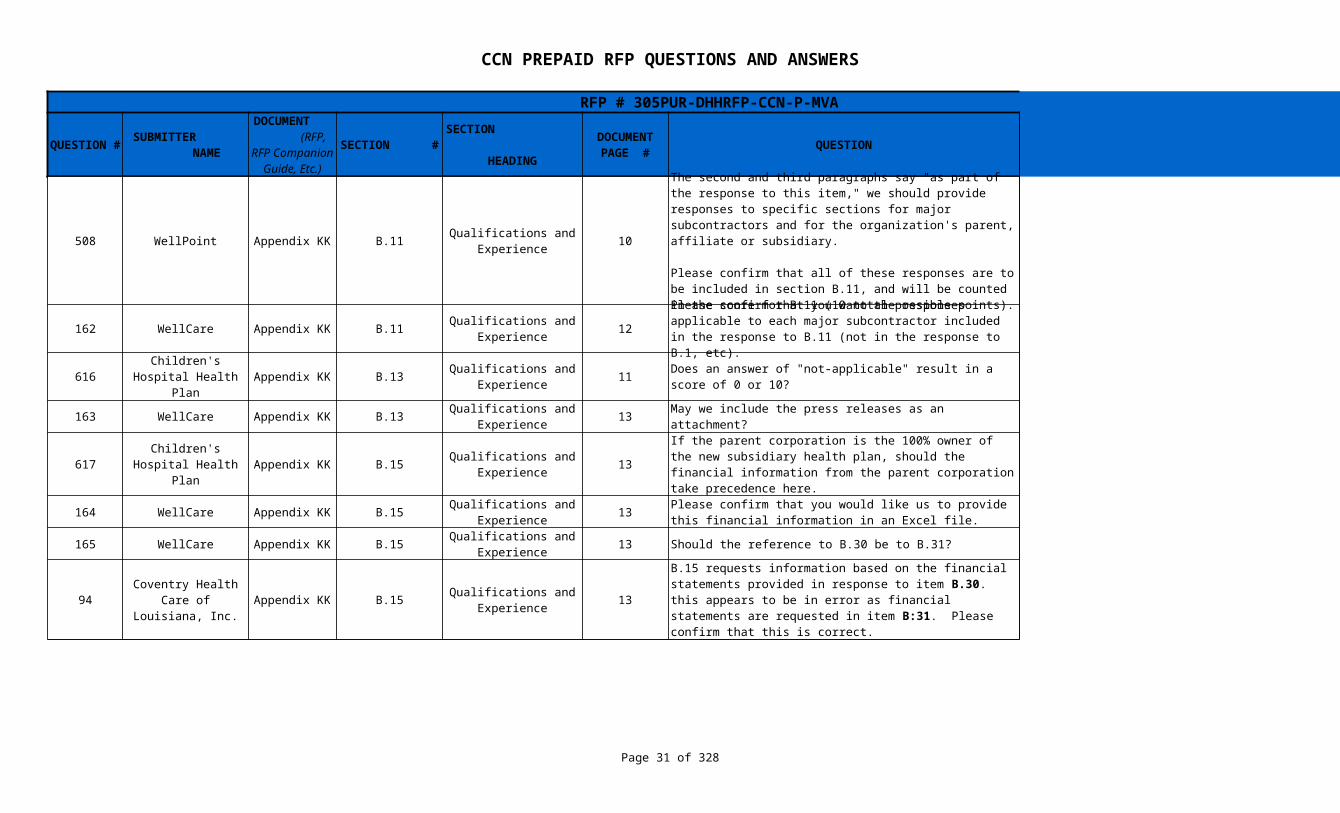
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 31 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
508 WellPoint Appendix KK B.11 10
162 WellCare Appendix KK B.11 12 Confirmed
616 Appendix KK B.13 11
163 WellCare Appendix KK B.13 13 May we include the press releases as an attachment? Yes
617 Appendix KK B.15 13 Yes
164 WellCare Appendix KK B.15 13 Confirmed
165 WellCare Appendix KK B.15 13 Should the reference to B.30 be to B.31? Yes
94 Appendix KK B.15 13 B:31 is correct
Qualifications and Experience
The second and third paragraphs say "as part of the response to this item," we should provide responses to specific sections for major subcontractors and for the organization's parent, affiliate or subsidiary.
Please confirm that all of these responses are to be included in section B.11, and will be counted in the score for B.11 (10 total possible points).
The CCN should include the requested information in the response to B.11
Qualifications and Experience
Please confirm that you want the responses applicable to each major subcontractor included in the response to B.11 (not in the response to B.1, etc).
Children's Hospital Health Plan
Qualifications and Experience
Does an answer of "not-applicable" result in a score of 0 or 10?
Neither--the content of such press releases can reflect both positively and negatively on Qualifications and Experience
Qualifications and Experience
Children's Hospital Health Plan
Qualifications and Experience
If the parent corporation is the 100% owner of the new subsidiary health plan, should the financial information from the parent corporation take precedence here.
Qualifications and Experience
Please confirm that you would like us to provide this financial information in an Excel file.
Qualifications and Experience
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.15 requests information based on the financial statements provided in response to item B.30. this appears to be in error as financial statements are requested in item B:31. Please confirm that this is correct.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 32 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
513 WellPoint Appendix KK 11, 12, 41
166 WellCare Appendix KK B.16 14 Confirmed
618 Appendix KK B.16 and B.24 12 & 14
11 Appendix KK B.17 and B.18 14-15
95 Appendix KK B.19 15
167 WellCare Appendix KK B.23 16 May we include the NCQA report card as an attachment? Yes
168 WellCare Appendix KK B.24 16 May we include the EQRO report as an attachment? Yes
B.15,B.16, and
J.7Qualifications and
ExperienceThese sections specify "Excel format." Should this be provided as appendices to the proposal?
The information should be provided in chronological order within the proposal . If creating certain portions of the proposal in Excel is problematic, comparable tables can be created in Word. The intent is that the information be in table format rather than narrative style.
Qualifications and Experience
Please confirm that you would like us to provide this experience information in an Excel file.
Children's Hospital Health Plan
Qualifications and Experience
Louisiana does not currently have Medicaid managed care; therefore, these categories of scoring would seem to greatly disadvantage Louisiana Provider-Sponsored Health plans as it would be impossible for them to provide what is being requested. How is that accommodated for in the scoring?
Information can be provided for prime subcontractors/third party administrators with managed care experience if applicable. Experience is a factor in proposal evaluation.
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
Can the CCN limit its response to those affiliates that conduct Medicaid business. If we have to include information for our affiliates, which are commercial health plans, the response to this question will require a considerable amount of research and would require us having to account for and list every occurrence of an employer group terminating/non-renewing coverage, etc. Should our response also include if an affiliate of the CCN exited a state Medicaid program?
The response should also include if an affiliate of the CCN exited a state Medicaid program. The CCN can limit its response to those affiliates that conduct Medicaid, Medicare, and CHIP business.
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.19 requests financial ratings from three different agencies. Is it acceptable to provide the ratings for the parent entity since they are guaranteeing the performance of the Prosper under this RFP?
Yes. If the entity proposing has financial ratings ("as applicable"), those should be submitted as well.
Qualifications and Experience
Qualifications and Experience

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 33 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
512 WellPoint Appendix KK B.27 16
169 WellCare Appendix KK B.27 19
170 WellCare Appendix KK B.29 22 May we provide a copy of the COA as an attachment? Yes
171 WellCare Appendix KK B.30 22 Yes
172 WellCare Appendix KK B.31 24 Yes
Qualifications and Experience
Should the first sentence read "…for your organization for relevant contracts, with at least one reference from a contract with a state Medicaid agency or other large similar government or large private industry contract."
Section B.11 also says each major subcontractor should respond to B.27. Could this requirement be restricted to the proposing organization only? This is a huge effort and there could be 20 or more reference letters to be solicited. In addition, it would seem that a reference for a major subcontractor A would have to send the letter to A first (in order to show the reference that A approves of this request), and then A would forward the letter to the proposing organization for submission in the proposal.
The first sentence has been amended to read, " Submit client references (minimum of three, maximum of five) for your organization from for major subcontractors; with at least one reference from for a major subcontractor who you have had with a state Medicaid agency or other large similar government or large private industry contract. " References are requested for major subcontractors (as defined in the Glossary) as well as for the prime subcontractor. All letters of reference are to be sealed and submitted with the proposal.
Qualifications and Experience
Please clarify the requirement to submit client references "for your organization from major subcontractors." Do you mean for our organization and major subcontractors? Similarly, regarding "with at least one reference from a subcontractor who have had with a state Medicaid agency..." do you mean that at least one reference for us and any major subcontractor should be from a State Medicaid agency...?
Currently Reads: Submit client references (minimum of three, maximum of five) for your organization from major subcontractors; with at least one reference from a major subcontractor who have had with a state Medicaid agency or other large similar government or large private industry contract. The RFP is being amended to read : Submit client references (minimum of three, maximum of five) for your organization for major contracts; with at least one reference for a major contract you have had with a state Medicaid agency or other large similar government or large private industry contract.
Qualifications and Experience
Qualifications and Experience
May we provide the requested documentation as an attachment?
Qualifications and Experience
May we provide the requested financial documentation as an attachment?
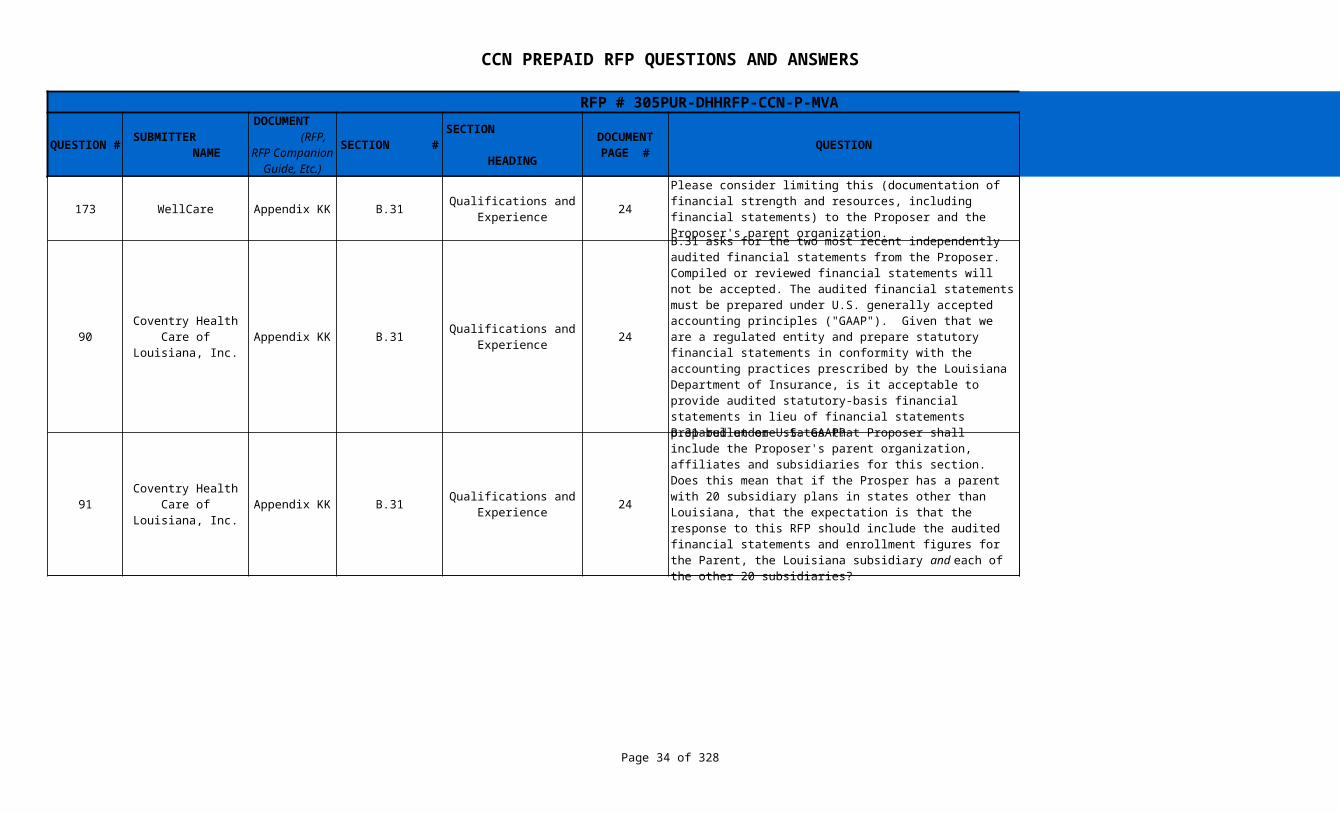
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 34 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
173 WellCare Appendix KK B.31 24
90 Appendix KK B.31 24 Yes
91 Appendix KK B.31 24
Qualifications and Experience
Please consider limiting this (documentation of financial strength and resources, including financial statements) to the Proposer and the Proposer's parent organization.
B. 31 is being amended to require the financial statements for the Proposer and the Proposer's parent organization only.
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.31 asks for the two most recent independently audited financial statements from the Proposer. Compiled or reviewed financial statements will not be accepted. The audited financial statements must be prepared under U.S. generally accepted accounting principles ("GAAP"). Given that we are a regulated entity and prepare statutory financial statements in conformity with the accounting practices prescribed by the Louisiana Department of Insurance, is it acceptable to provide audited statutory-basis financial statements in lieu of financial statements prepared under U.S. GAAP?
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.31 bullet one states that Proposer shall include the Proposer's parent organization, affiliates and subsidiaries for this section. Does this mean that if the Prosper has a parent with 20 subsidiary plans in states other than Louisiana, that the expectation is that the response to this RFP should include the audited financial statements and enrollment figures for the Parent, the Louisiana subsidiary and each of the other 20 subsidiaries?
The language will be amended to include proposer and proposer's parent organization only.
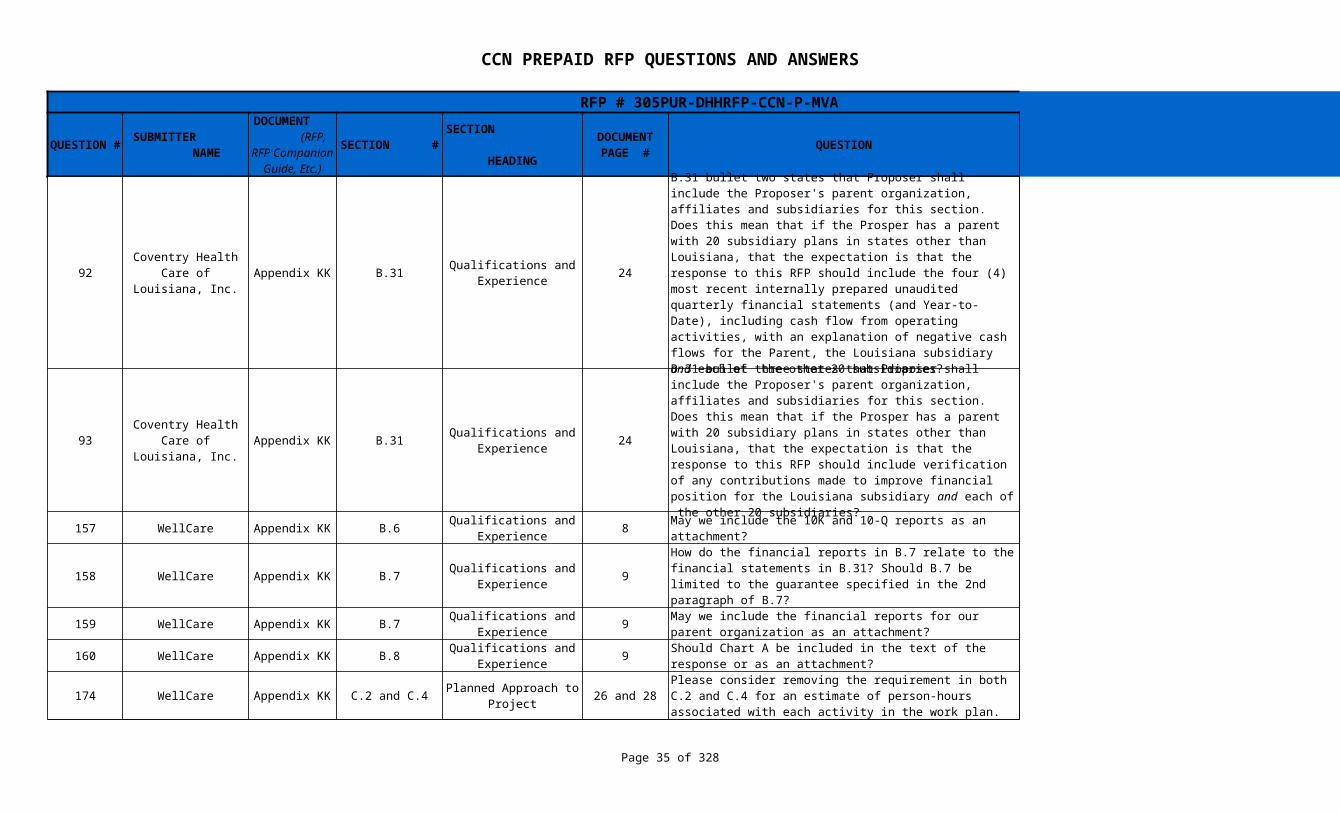
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 35 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
92 Appendix KK B.31 24
93 Appendix KK B.31 24
157 WellCare Appendix KK B.6 8 May we include the 10K and 10-Q reports as an attachment? Yes
158 WellCare Appendix KK B.7 9
159 WellCare Appendix KK B.7 9 Yes
160 WellCare Appendix KK B.8 9 DHH prefers that it be submitted as an attachment
174 WellCare Appendix KK C.2 and C.4 26 and 28 No revision will be made.
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.31 bullet two states that Proposer shall include the Proposer's parent organization, affiliates and subsidiaries for this section. Does this mean that if the Prosper has a parent with 20 subsidiary plans in states other than Louisiana, that the expectation is that the response to this RFP should include the four (4) most recent internally prepared unaudited quarterly financial statements (and Year-to-Date), including cash flow from operating activities, with an explanation of negative cash flows for the Parent, the Louisiana subsidiary and each of the other 20 subsidiaries?
The language will be amended to include proposer and proposer's parent organization only.
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.31 bullet three states that Proposer shall include the Proposer's parent organization, affiliates and subsidiaries for this section. Does this mean that if the Prosper has a parent with 20 subsidiary plans in states other than Louisiana, that the expectation is that the response to this RFP should include verification of any contributions made to improve financial position for the Louisiana subsidiary and each of the other 20 subsidiaries?
The language will be amended to include proposer and proposer's parent organization only.
Qualifications and Experience
Qualifications and Experience
How do the financial reports in B.7 relate to the financial statements in B.31? Should B.7 be limited to the guarantee specified in the 2nd paragraph of B.7?
There is some overlap between the first half of B.7 and B.31. B.7 can be limited to the guarantee specified in the 2nd paragraph with the financial reports responsive to B.31
Qualifications and Experience
May we include the financial reports for our parent organization as an attachment?
Qualifications and Experience
Should Chart A be included in the text of the response or as an attachment?
Planned Approach to Project
Please consider removing the requirement in both C.2 and C.4 for an estimate of person-hours associated with each activity in the work plan.
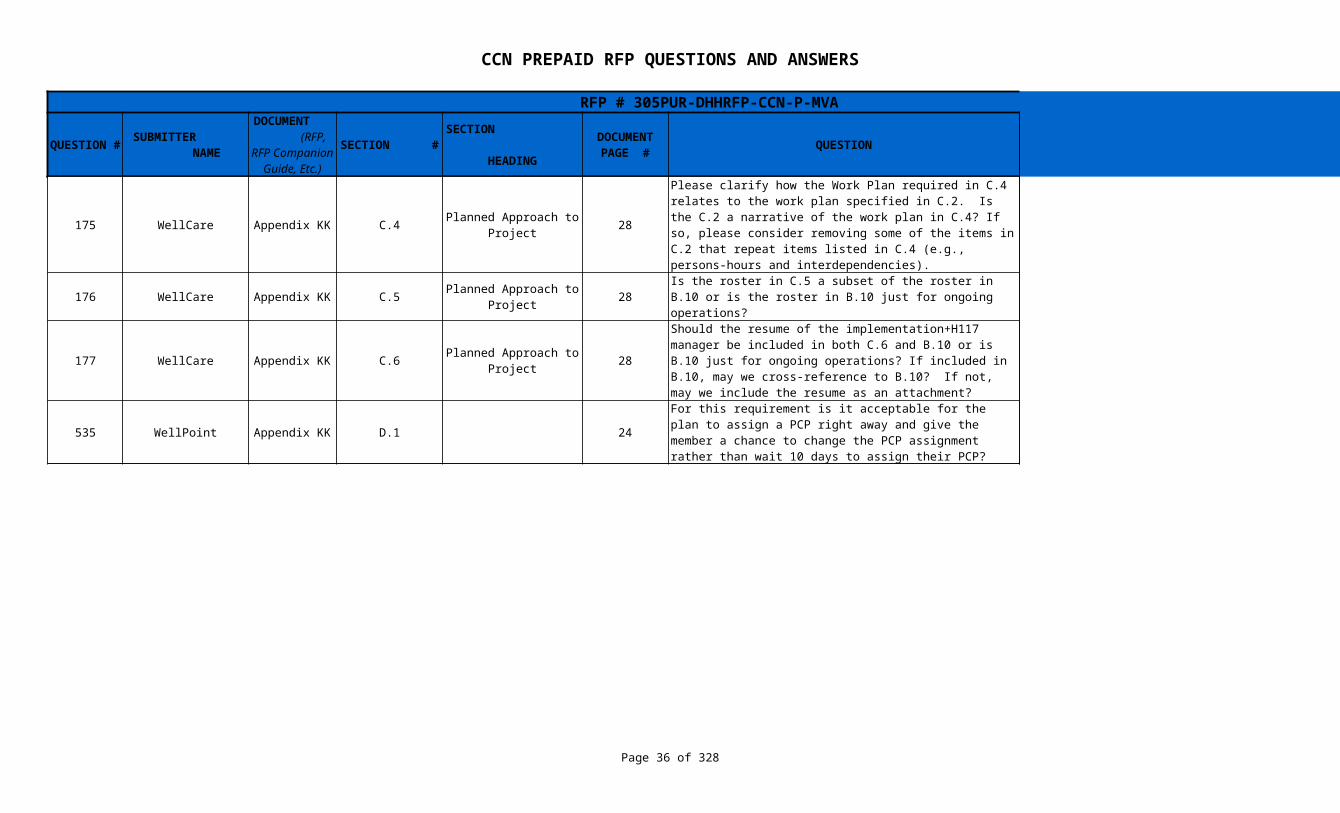
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 36 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
175 WellCare Appendix KK C.4 28
176 WellCare Appendix KK C.5 28
177 WellCare Appendix KK C.6 28
535 WellPoint Appendix KK D.1 24 Yes
Planned Approach to Project
Please clarify how the Work Plan required in C.4 relates to the work plan specified in C.2. Is the C.2 a narrative of the work plan in C.4? If so, please consider removing some of the items in C.2 that repeat items listed in C.4 (e.g., persons-hours and interdependencies).
C.4 refers to the document (s) created in Microsoft Project or similar software while C.2 refers to the written narrative
Planned Approach to Project
Is the roster in C.5 a subset of the roster in B.10 or is the roster in B.10 just for ongoing operations?
The C.5 Roster is specific to the implementation team. B.10 refers to the ongoing Contract operations effective the "go live" date.
Planned Approach to Project
Should the resume of the implementation+H117 manager be included in both C.6 and B.10 or is B.10 just for ongoing operations? If included in B.10, may we cross-reference to B.10? If not, may we include the resume as an attachment?
The resume can be included as an attachment and can be cross referenced.
For this requirement is it acceptable for the plan to assign a PCP right away and give the member a chance to change the PCP assignment rather than wait 10 days to assign their PCP?
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 37 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
527 WellPoint Appendix KK F.1 26
523 WellPoint Appendix KK F.1 26 Care management type data is not available for members
524 WellPoint Appendix KK F.1 26
525 WellPoint Appendix KK F.1 26
526 WellPoint Appendix KK F.1 26
528 WellPoint Appendix KK F.2 27 Will we get access to LEERS from the State? Network hospitals can get access to LEERS
531 WellPoint Appendix KK F.6 28 Yes
What communication will the State have with members and providers regarding this transition?
The state has already engaged in extensive outreach and education with the provider community, through open forums and conference calls as well as the production of a CCN Resource Guide for Providers, available on the Making Medicaid Better Web site. As the time for member choice draws closer, the state will launch an extensive outreach and education campaign to reach Medicaid recipients and educate them on the enrollment process. This will include discussion of timelines, and a readiness kit that will guide them in making appropriate and well-informed health decisions for their families. The state will employ an outreach and education contractor and an Enrollment Broker that will assist with this process. The state anticipates a media campaign, direct mail outreach and community events to help bolster the active selection of a CCN by Medicaid recipients.
Can the State provide us care management type data for the members?
What is the State's expectation for this requirement when we don't have the member history?
The CCN is responsible for identifying any special health needs of members assigned to the CCN and must have a process for doing so.
For files on claims and pharmacy how often will we receive the data? Will we get data on an ongoing basis from other plans as members change plans?
Weekly; DHH will provide data from the FFS Medicaid program for benefits not included in the CCN core benefits and services. CCNs are responsible for coordination of care for members changing plans, which may include exchange of data.
Does the State have risk assessments that you can share with us?
No Medicaid does not conduct Risk Assessment in the current program
Will the State provide permission to use cell phones and email addresses to contact members by the plan?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 38 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
220 HMO Louisiana, Inc. Appendix KK F.1 Service Coordination 26
420 Appendix KK G.1 Provider Network 30
619 Appendix KK G.1 Provider Network 30
Will you be able to provide an authorization file, claims file, pharmacy file in advance so we can test our processes?
Yes, upon award of Contract files for system testing will be made available.
AmeriHealth Mercy of Louisiana
Please confirm that it is sufficient to list specialty providers and other providers, by provider type, along with the corresponding count of providers that have executed a contract or Letter of Intent.
Appendix KK is being amended to add the following information needed for each provider for whom the proposer has a Letter of Intent or executed contract: The CCN must complete a spreadsheet with 1. Practitioner Last Name, First Name and Title - For types of service such as primary care providers and specialist, list the practitioner’s name and practitioner title such as MD, NP (Nurse Practitioner), PA (Physician Assistant), etc. 2. Practice Name/Provider Name - - Indicate the name of the provider. For practitioners indicate the professional association/group name, if applicable. 3. Business Location Address - Indicate the business location address where services are provided including but not limited to, 1st line of address, 2nd line of address, City, State, Postal Code 4. Provider Type and Specialty Code - Indicate the practitioner’s specialty using Medicaid Provider Type and Specialty Codes. 5. New Patient - Indicate whether or not the provider is accepting new patients. 6. Age Restriction - Indicate any age restrictions for the provider’s practice. For instance, if a physician only sees patients up to age 19, indicate < 19; if a physician only sees patients age 13 or above, indicate > 13. 7. If PCP - the number of potential linkages. 8. If LOI or contract executed. 9. GEO coding for this location
Children's Hospital Health Plan
The section discusses providing a listing of the proposed network using the "List of Required" providers. Is this referring to 7.7.3.3 or is referring to all potential network providers?
Appendix E - Listing of Required and Optional Providers is being added to the appendices section.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 39 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
218 HMO Louisiana, Inc. Appendix KK G.1 Provider Network 30 Define allowable out of network providers.
227 HMO Louisiana, Inc. Appendix KK G.1 Provider Network 30
494 HMO Louisiana, Inc. Appendix KK G.1 Provider Network 30
209 HMO Louisiana, Inc. Appendix KK G.1 Provider Network 30
777 Appendix KK G.1 Provider Network 35 That is correct
178 WellCare Appendix KK G.1 Provider Network 35 Yes
Appendix E is being added to the RFP as an addendum . An out-of-network provider is one with which the CCN does not have a contract.
App KK-G.1 it states in the last paragraph, last sentence, “you should provide individual maps as well as overlay maps to demonstrate distance relationships between provider types”. We understand the individual maps requirement but what exactly do you want to see when you state overlay maps to demonstrate distance relationships between provider types? We usually show the average distance a member has to travel to their providers and if there are any members that fall outside of the access standards provided.
DHH will geo-code Medicaid recipients. CCN maps of major type of providers, such as but not limited to PCP, FQHC/RHCs, and hospitals will be used by DHH to determine travel distance for recipients for each parish within a GSA.
G.1 states that we must provide along with the provider listing the number of potential linkages to PCP. Can we use what is published on the DHH website today since we were not able to add this question to the LOI? For the provider listing, do you want to see all fields that were asked through the LOI or what was obtained through the LOI that is in appendix FF?
No, PCPs may not be willing to accept new patients or have restrictions such as age/sex.
Yes, the information in Appendix FF is requested along with GeoAccess coding and maps as specified in Appendix KK.
Can we get a listing of all members currently enrolled their zip codes for each member under the policy to be able to run our access standards? The hard drive that was received with the DHH data didn't have member zip codes.
Potential Enrollees by zip code can be found in the Procurement Library under the heading Medicaid Enrollment and then selecting Potential CCN Enrollment--2011 Data
Amerigroup Corporation
Please confirm that the reference to item "G.1" on this page is a typographical error and that the reference is actually "G.15".
May we include the listing and GeoAccess maps as appendices?
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 40 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
521 WellPoint Appendix KK G.1 Provider Network 30 No, not all PCPs are willing to accept the maximum capacity.
180 WellCare Appendix KK G.13 Provider Network 38 Yes
211 HMO Louisiana, Inc. Appendix KK G.4 Provider Network 31
522 WellPoint Appendix KK G.4 Provider Network 31
179 WellCare Appendix KK G.4 Provider Network 36 Please confirm that the reference to G.3 should be G.1.
532 WellPoint Appendix KK I.1 EPSDT 37 Yes
534 WellPoint Appendix KK J.4 Quality Management 39
181 WellCare Appendix KK J.5 Quality Management 46 Yes, these are synonymous
514 WellPoint Appendix KK J.7 Quality Management 41 Yes
182 WellCare Appendix KK J.7 Quality Management 47 Yes
219 HMO Louisiana, Inc. Appendix KK Quality Management 39
We assume that we can use the State listed capacity for the number of linkages per PCP as we were not able to make changes to the LOIs to ask this question. Is this a valid assumption?
May we include the sample quality profile reports as an appendix?
G.4 of Appendix KK states that DHH will provide a listing of the significant traditional providers on the Making Medicaid Better website. When will that be made available?
The total dollars paid per provider as well as unduplicated Medicaid enrollees in SFY 11 are included in the Louisiana Medicaid Provider Listing in the Procurement Library. This information is in Excel and sortable by fields.
We were unable to find the STP file on the DHH website. Can the State please make the listing available for the plans?
The provider listing showing SFY 10 total payments has been added to the procurement library
This has been amended to correct the reference from G.3 to G.1
Do we need to submit vision, hearing and dental separately for EPSDT tracking?
For this question does the State want 10 years worth of improvement projects or a sampling of specific studies?
Any projects or studies referenced in the response to J.4 should be completed in 2001 or later
Please confirm that in the intro "QAIP" is the same as "QAPI." Also, when used in the bullets, is "QAIP" the same as quality improvement activities?
Please confirm that HEDIS results can also be included for a TPA who will provide quality and UM services.
Please confirm that you want us to provide the HEDIS measures in an Excel file.
Please clarify the types of focus studies and quality improvement projects. For example, claims, health, customer service? Is the requirement to have ALL such information dating from 2001 to the present, or to include information not dated prior to 2001?
Projects shall include those in which the outcomes resulting in cost savings realized, process efficiencies, and improvements to member health status. Such descriptions should address such activities since 2001 and how issues and root causes were identified, and what was changed.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 41 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
183 WellCare Appendix KK K.1 Member Materials 49
533 WellPoint Appendix KK K.5 Member Materials 44 Section K is relative to Member materials
156 WellCare Appendix KK 4
89 Appendix KK L.1 Customer Service 52
184 WellCare Appendix KK L.2 Customer Service 51 May we provide the hotline reports as an attachment? Yes
297 Appendix KK N/A 11
778 Appendix KK P.1 51
Please confirm that we should provide more than one example of member education materials and that we can include these as attachments.
Proposers may provide more than one example of member education materials and can include these as attachments
Does this requirement/question apply to member and provider portals?
Part II: Technical Proposal & Evaluation
Guide
How will items with points (not a range) be scored? Will the evaluator rate the response on a scale (e.g., 0-5) or simply assign points based on the total possible points?
Scoring will be via Consensus Scoring with the assignment of points based on the total possible points.
Coventry Health Care of Louisiana,
Inc
Please provide clarification to the second half (where it begins with(3)) of the second bullet under question L.1 in Appendix KK. The bullet states "Process for routing calls to appropriate persons, including escalation;(3) the type of information that is available to customer service staff and how this is provided (e.g., hard copy at the person's desk or on-line search capacity). Should the (3) be a separate bullet under this question or is it referring to the type of information provided to customer service as it relates to call routing?
The information following "(3)" is not a separate bullet. It refers to the type of information and formats for that information that is provided to customer service staff relative to call routing and escalation
AmeriHealth Mercy of Louisiana
PART II: Technical Approach
Item B.15 (5) refers to "debt-to-worth ratio". Does the state mean "debt-to-net worth"? If so, please state what balance sheet items other than external accounts payable and long-term debt are required in the numerator?
Yes. DHH is not specifying the balance sheet items for the calculation.
Amerigroup Corporation
Section P. Third Party Liability
The fourth bullet appears incomplete, ending with "how you would adapt your". Please provide the missing text to clarify what would need to be adapted.
The words " current operations to meet contract requirements." were inadvertently omitted. Has been added via addendum.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 42 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
247 Appendix KK Part II, B.16 p. 14 Total premiums received
286 Appendix KK Q.3 Claims Management 51
185 WellCare Appendix KK R.1 Information Systems 58 May we provide the work plan as an attachment? Yes
516 WellPoint Appendix KK Information Systems 52
96 Appendix KK Information Systems 66
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
For the "annual contract payments" regarding the ten largest (as measured by number of enrollees) managed care contracts for populations other than Medicaid/CHIP and/or other low-income individuals within the last five (5) years, are you requesting the amount paid out for the contract or the premium payment received?
Louisiana Healthcare Connections
Please clarify this question: Q.3 Describe your methodology for ensuring that the claims processing, including adherence to all service authorization procedures, are met.
Addendum to read Describe your methodology for ensuring that the requirements for claims processing, including adherence to all service authorization procedures are met.
R.1third bullet
The question asks for the bidder’s process for accepting “one-time” data feeds (such as the initial set of CCN enrollees).
Can the State make record layouts or general descriptions of these “one-time” data feeds available? Is the enrollment feed in a standard HIPAA format for electronic transactions?
The exact record layout and field for the Enrollment File are still in development. DHH intends to use standard HIPAA compliant formats for electronic transactions
Coventry Health Care of Louisiana,
Inc.R.10
third bullet
Can data be provided in a format DHH can use to query from or is access to the CCN-Ps actual system required? If access to the CCN-Ps system is required, how many DHH staff will need access? Is there a specific format/type of report which DHH will want to be to create?
The question asks for the capabilities of the Proposer including " the ability in a secure, inquiry-only environment for authorized DHH staff to create and/or generate reports out of your systems on an ad-hoc basis." The response should include whether the Proposer's system has this capability and any parameters such as number of DHH staff and format/type of reports that DHH could create.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 43 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
394 Appendix KK R.5 and R.6 Information Systems 55-56
788 Appendix KK S.1 59-63
AmeriHealth Mercy of Louisiana
In Appendix KK item R.5 and R.6, the instructions indicated to “address all of the requirements in Section 17.” That is clear. However, for those Appendix KK queries/requirements where specific RFP sections are referenced in only parentheses, such as “Section E: Chronic Care/Disease Management (Section § 6 of RFP)”, is the bidder to assume that they should address all of the requirements in Section 6?
The reference is to the Section in which the item is addressed. It is not a request to address everything in that Section within the response.
Amerigroup Corporation
Added Value to Louisiana Providers and
CCN Members
The guidance states that “For increased provider payments to be considered in the evaluation, they must represent an increase in the minimum payment rates for all providers associated with the CCN’s operating policies and not negotiated rates for a subset of the providers”. Please confirm whether an incentive program that is offered to all PCP’s but that requires a certain amount of membership threshold to be met will meet the requirement of “all providers”, even though not all providers will be eligible for the program if the membership threshold is not met. Also, the guidance states “If you are awarded a contract, the response to this section will become part of your contract with DHH and DHH will confirm your compliance. The incentives and enhanced payments, for providers and expanded benefits to members proposed herein cannot be revised downward during the initial thirty-six (36) month term of the contract, as such programs were considered in the evaluation of the Proposal. Increases in payments or benefits during the term of the contract may be implemented.” Please confirm that the estimates of the amounts to be paid under incentive programs as required to be documented in Appendix OO are meant to be estimates only (since by nature incentive programs depend on whether providers actually achieve the incentive objectives / measures)and are not meant to be contractually-binding amounts to be paid. Also, please clarify which year Appendix OO is meant to apply to? All years under the contract, or just the 1st year?
Yes, an incentive program that is offered to all PCPs but that requires a specific enrollment threshold meets the RFP requirement. The intent is to evaluate an incentive program that any provider can meet based upon a consistent application of criteria rather than negotiated incentives based upon more subjective and variable considerations. Note that the PMPM amounts reported should reflect the value for the plan's entire enrollment for the eligibility group/age being reported; do not base the PMPM value on only the subset of providers anticipated to participate in the incentive program. Appendix OO applies to year one of the contract, but as indicated, the incentives are expected to apply throughout the contract period. The amounts reported are estimates, and not contractually-binding amounts per se. DHH does consider the incentive programs as part of the RFP response, but acknowledges that the value of such incentives may vary from the estimates. Actuarial documentation must be provided supporting the determination of the incentive valuation. The intent of the multiple year requirement is to prevent the termination of incentives following the awards of the contracts.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 44 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
515 WellPoint Appendix KK 59, 65 In each GSA
226 HMO Louisiana, Inc. Appendix KK S.2 64
278 Appendix KK C 26-28
714 Appendix KK G Provider Network 36
689 Appendix KK G Provider Network 39 Yes (our Page reference is 34 of Appendix KK)
S.1 and S.2
Added Value to Louisiana Providers and
CCN Members
RFP 2.1.1.6 requires a CCN-P to "have a network capacity to enroll a minimum of 75,000 Medicaid members into the network in each DHH designated GSA for which a proposal is being submitted."
Is the "projected utilization for 75,000 members" and "assuming enrollment of 75,000 members" per GSA, or total statewide?
Added Value to Louisiana Providers and
CCN MembersSince a member has 10 days before choosing a PCP, are we prohibited from sending ID Cards prior to the 10 days?
This question is not pertinent to this section of the RFP appendices. Language outlining this information can be found in section 12.11.2 and 12.13 of the RFP. The CCN must send a Member ID card with the member welcome packet. The welcome packet must be sent within 10 business days from the date of the receipt of the file from DHH or the enrollment broker identifying a new enrollee. Because the Member ID card must contain the PCP name, if there is no PCP named at the time of enrollment, the CCN will have to send the card without the PCP and resend a new card when a PCP is selected.
Louisiana Healthcare Connections
Planned Approach to Project
Please clarify the differences between question C.2 and C.4. They both seem to reference submission of the work plan. Is question C.2 requesting a description of the work plan vs. the actual work plan document?
C-4 refers to the chart created in Microsoft Project. C-2 includes the in-depth narrative.
Aetna Better Health, Inc.
This section states DHH will make the STP listing available on www.MakingMedicaidBetter.com. Can this list be posted as soon as possible to assist Network in ensuring all STPs are included in the target provider population?
Payment by provider as well as unduplicated recipients are included on the Medicaid Provider file in the Procurement Library. We believe there is adequate information to identify the STPs by using the sort feature in this Excel workbook.
Aetna Better Health, Inc.
Please confirm that the second question on page 39 (which currently reads "G1") is actually "G15".

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 45 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
620 Appendix KK Technical Approach 22
13 17
14 B.4 7
398 N/A Appendices
399 Appendix MM N/A Appendix
Children's Hospital Health Plan
How will the scoring of multi-bulleted Yes / No questions within each category be scored? Are they weighted equally? Also, some categories with KK seem to have yes/no all/nothing type answers. Does this mean all or no points?
Each requirement will be scored in its entirety. There is no additional breakdown for mutli-bulleted items. DHH will need further clarification to respond to the statement and third question.
Coventry Health Care of Louisiana,
Inc.Appendix KK Appendix KK
Part II. Technical Approach -
Qualifications and Experience
Can the CCN limit its response to those affiliates that conduct Medicaid business. If we have to include information for our affiliates, which are commercial health plans, the response to this question will require a considerable amount of research across all commercial affiliate companies which would be quite onerous to gather.
DHH considers state and federal regulatory action within the last five years to be relevant whether it was for Medicaid business or non-Medicaid business.
Coventry Health Care of Louisiana,
Inc.Appendix KK
Part II. Technical Approach -
Qualifications and Experience
Can the CCN limit its response to those affiliates that conduct Medicaid business?
DHH considers pending or recent litigation to be relevant whether it is for Medicaid business or non-Medicaid business
AmeriHealth Mercy of Louisiana
Appendix LAppendix MAppendix N
Acknowledgment and Consent Forms -
Sterilization, Hysterectomy and
Abortion
Please confirm that DHH does not expect the CCN to obtain member signature on these forms. Since the provider of the services is responsible for obtaining informed consent, it seems more appropriate for the CCN to require its providers to obtain the necessary signatures.
That is correct. The CCN does have responsibility for assuring that their contract providers are complying with requirements
AmeriHealth Mercy of Louisiana
Attestation of Provider Network Submissions
Please confirm that Appendix MM is to be completed after award of a contract as part of the Readiness Review. Additionally, the second part of the 1st bullet is unclear - does this mean that amendments to a bidder's existing provider contracts that are necessary to bring such existing contracts into compliance with the CCN-P Program requirements need to be approved by DHH prior to their execution?
Appendix MM will be revised
Yes, the CCN must amend their existing contracts to be in compliance with the CCN’s contract with DHH and those amended contracts must be approved by DHH. The CCN may submit a “master” version for approval in lieu of each individual subcontract.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 46 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
729 Appendix MM N/A 1Aetna Better Health, Inc.
Attestation of Provider Network Submission
If the CCN has exceptions to it's provider model contract as a result of negotiations with a provider, what is the process that DHH wants to use for approval of these exceptions? Would DHH consider adding the following language to the contract:The CCN shall submit all contract changes that materially impact the terms and conditions ofthe contract to DHH for approval. Requests to modify previously approved provider modelcontracts must be submitted to and approved by DHH prior to execution of any modelcontract modifications. The CCN shall electronically submit a redline version of therequested contract modifications or copy of the modifications made in an attachment (e.g.special provision exhibit/attachment) that have been incorporated into and with the modelcontract.(This language is referenced from the Application Policy and Procedures Guide.)
An addendum will be made for section 7.12.7 to incorporate subcontract changes.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 47 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
447 Appendix P N/A 2
414 N/A N/A N/A
630 N/A N/A N/A
Coventry Health Care of Louisiana,
Inc.
Section h. Termination of Agreement and
Destruction of Records
The Data Use Agreement for a Limited Data Set stipulates that the Data User must destroy the information at the earlier of its submission of its proposal to DHH, or the date of the deadline for submission of the proposal. Actuaries are bound by certain Standards of Practice in the execution of their work, and may at times be called upon to demonstrate that their work product followed these Standards. Destroying the Limited Data Set would make it challenging for actuaries to demonstrate their compliance with Standards of Practice if the analyses relied on data that they no longer had access to. Will DHH allow CCNs to keep the Limited Data Set to allow actuaries to satisfy any inquiries around compliance with Actuarial Standards of Practice?
No. The requirement to destroy supersedes. In the event that actuaries must produce the Limited Data Set, it can be obtained from DHH by signing another Data Use Agreement. DHH will retain the Limited Data Set exactly as given to the CCN proposers.
AmeriHealth Mercy of Louisiana
Appendix P /Limited Data
Set
The Louisiana Medicaid Limited Data Set is consistent with file layout and documentation provided the Data Use Agreement. However, per previous communications, we were under the impression that member, provider, claim and claim line identifiers would be provided in this dataset (masked). As these represent key elements needed for evaluation of the proposal, particularly in the areas of understanding the population for medical management and provider network strategies, please clarify as to whether this information will be made available to the prospective CCNs.
DHH is working to add this information to the Limited Data Set.
Children's Hospital Health Plan
Baseline Quality Data
Can DHH provide this baseline Quality data at the Region Level (regions 1 thru 9)? The Statewide data is very useful as a guide, but the region-specific data would allow plans to see where they need to get to.
Regional and GSA level baseline data for the Incentive Based measures has been placed in the Procurement Library under Quality.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 48 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
17 7 of 15
16 N/A 10 of 15
188 WellCare N/A
393
Coventry Health Care of Louisiana,
Inc.
CCN State Fair Hearing
Companion Guide
CCN Review and Conference
CCN Review and Conference Section of the Guide: In other markets where we have Medicaid MCOs, the member requests a state fair hearing directly from the state agency; not the health plan. Certainly, the health plan will assist member with requesting such, but the concept in this companion guide that the member can request the state fair hearing to the CCN, and then the CCN has to reconsider its decision that has already gone through an appeal process that meets federal requirements seems to add an unnecessary layer that is not required by federal law, or consistent with what we've seen elsewhere.
Members may contact the CCN rather than the DAL to request the State Fair Hearing . The CCN has the option to informally reconsider the decision and resolve to the appellant's satisfaction without an actual hearing. Policies and procedures relative to State Fair Hearings are driven by Blanchard vs. Forrest.
Coventry Health Care of Louisiana,
Inc.
CCN State Fair Hearing
Companion Guide+D241
Claimant/Appellant Opt to Make Request
to the DAL
Companion guide states, "If the claimant/appellant prefers to mail the State Fair Hearing request directly to the DAL, the CCN shall provide the address….." We suspect that in many cases, the member, having already been informed of his right to go to the DAL, will do so directly, without going back to the CCN after exhausting appeal rights. Why does this process, as outlined, assume that there will be so much interaction between the member and CCN after the CCN has concluded its internal appeal process?
The inclusion of written procedures is based on the fact that Medicaid recipients mail State Fair Hearing requests to local eligibility and state Medicaid Offices (who mailed the Notice of Decision) rather than the Division of Administrative Law (DAL) even though they are provided with the DAL mailing address. DHH does not have prior Medicaid managed care experience to assume where enrollees will direct the request for a State Fair Hearing when notified by the CCN that their internal appeals process has been exhausted.
CCN-P Proposers'
Conference - 4/19/2011
Rate Conference
Presentation
Risk Adjustment - Both Models
Slide Page Number 36
Slide indicates "CCN's that have less than 50 members in the consolidated group will be assigned the average population risk score." Question is whether the calculated risk score for these members will be incorporated into determining the average?
All scored recipients will be included in the calculation of the average population risk score.
AmeriHealth Mercy of Louisiana
CCN-P Request for Proposals & Appendix G
5.6.2 (RFP); Appendix page
10
Determination of CCN Rates (RFP) / Trend
Development (Appendix)
35 (RFP); 10 (Appendix)
Please explain the rationale behind the 0% trend assumption for the maternity kicker payment.
Most fee schedules are frozen and utilization per case is not expected to increase.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 49 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
569 WellPoint Claims Data -
570 WellPoint Claims Data -
571 WellPoint Claims Data -
539 WellPoint Data Book -
540 WellPoint Data Book -
Is there patient Unique Identifier information in Claim, outlier, delivery file we can use to identify disease prevalence and clinical condition distribution?
Since CCN contractors will be required to sign a BAA with DHH, Molina will distribute unique recipient identifier information using the Louisiana Medicaid Recipient ID number.
For outpatient and Professional claims, are data at line level? Which means one claim can have multiple records in the claim file? And if so, how can we group the records into one visit. By looking into some sample records, we did not find many visits under “outpatient”.
Yes. Mercer defined a claim by using the first 11 digits of the clc_claim _icn + elig_id + clc_service_from_date + clp_bill_prov_id. Some of these fields may not be in the claims extract. It may not be possible to group by visits.
As we analyze the claims data, we will have more questions. Is it possible for us to get a contact person in case we need to get better understanding of the data?
Questions must be submitted in writing through the process outlined in the RFP.
The base data for FY2010 used in attachment B of the rate book (around $173-174 PMPM) is lower than what is shown in the data book (around ($178 PMPM excluding Rx), on average for the entire State. Can Mercer review this and explain why there is a difference (what adjustments were made to the databook that are not already explained)? If this was not intentional, can Mercer correct this?
The base data for SFY10 in Attachment B is before applying completion factors whereas the data book is already completed. If you apply the completion factors to the base data, the numbers should match.
The data book shows the exact same "units" for IP hospital for Region 1 and 2 for the 0-2 month rate cell for FY09. This would appear to be an error due to the preciseness of the figure (2285.03709717658). Can the State confirm what the right figures are and whether there are other errors in the data book?
These figures are correct. After adding in outlier claims, both regions experienced 2,280 days of inpatient stay for the 0-2 month SSI rate cell. Since the completion factor is the same across regions, the completed number is also identical.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 50 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
541 WellPoint Data Book -
542 WellPoint Data Book - The adjustment for duplicate members was immaterial.
543 WellPoint Data Book - Yes, the FQHC/RHCs are paid on a PPS basis in FFS Medicaid.
544 WellPoint Data Book -
545 WellPoint Data Book -
The data used in the rate development already excludes certain services/populations that will not be covered. Can an overall approximation be developed showing what % of total cost was excluded to demonstrate the reasonableness of those exclusions?
Data for Services and populations other than those to be covered by the CCNs have not been captured and the corresponding percentage of current costs have therefore never been calculated.
Mercer adjusted the eligibility data to exclude duplicate member ID's. Can this adjustment be quantified so the plans can understand the magnitude of this issue?
For FQHC/RHC costs, what is the basis for the data included in the rates? Is it the actual payments that were made at that time based on the PPS rate in effect during those months?
The rate setting includes an adjustment for hospital costs settlement of 3.6% for 2009 and 1.3% for 2010. Yet, in the rate meeting, it was not clear that either year's calculation was complete. How were these estimated for rate setting and when will final cost settlements be calculated? Why is 2010 assumed to be so much lower than 2009? Can the bidders receive cost settlement information by hospital to assist with contracting and analysis, separately for inpatient and outpatient?
See responses to #387, #430 and #481. No further adjustments are planned.
Some of the adjustments for costs settlements are negative (e.g., P. 29, region 1 BCC adjustment = 0.8969, Region 1 Family and Children 45+ Female adjustment = 0.9965). Can Mercer explain why there are negative cost settlement adjustments?
Cost settlement adjustments can be negative or positive. Negative amounts reflects recoupments from the hospitals due to the interim payment being higher the cost settled amount, which is a percentage of hospital costs. Positive amounts reflects payments from DHH to the hospitals due to the interim payment being lower than the cost settled amount.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 51 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
546 WellPoint Data Book -
547 WellPoint Data Book -
548 WellPoint Data Book -
How was the data/eligibility adjusted for members who were enrolled in Medicaid, lost eligibility, and then re-enrolled? Was the first 30 days of experience/eligibility after re-enrollment also excluded? Is there different timing assumed than for truly new members?
Yes, the first 30 days of eligibility and claims after re-enrollment were excluded. Re-enrolled members are treated the same as new members.
The unit cost trends in general appear very low, given the following: --Historically, the hospitals have received cost settlements, suggesting that 0% trend is not likely going forward. --The FQHC/RHC reimbursement has been tied to the PPS rate. Given that, is it reasonable to expect 0% unit cost trend going forward? --There is no separate assumption for scope creep or mix of services increasing --Trends from 2009 to 2010 appear to be roughly 6%, about 2-2.5% higher than the assumed trend of 3.67%, after adjusting for the fee schedule reductions that have occurred during that time and excluding the estimated hospital cost settlement impact.
Given all of these issues, can Mercer and/or the State consider including higher, more reasonable trends?
Mercer and DHH are currently reconsidering trend and provider rate issues relevant to the rate period.
The magnitude of the managed care savings appears very high for the first year of this contract. Can the State consider using more reasonable assumptions given this is a new program? Please also note that since pharmacy is carved out, but that is typically an area that contributes to significant savings by moving to managed care, it will be harder to achieve the overall savings of almost 15%.
The savings factor describes the extent of change the system that DHH and its partner CCNs must be able to deliver if the initiative is to be cost effective.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 52 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
549 WellPoint Data Book - See response to #578.
550 WellPoint Data Book -
551 WellPoint Data Book -
552 WellPoint Data Book -
553 WellPoint Data Book -
Phase 2 and Phase 3 will only be effective for 10 and 8 months respectively (not a full 12 months). To be accurate, the managed care savings should be reduced to reflect this difference. We have seen this type of adjustment for reduced savings for less than 12 months in other states and believe this would be reasonable.
The unit cost increases for the categories that have big utilization savings (due to higher intensity of remaining services) appears very low given the magnitude of the utilization reductions (e.g., IP hospital for family assumes more than a 33% reduction but only a 2% increase in intensity). What is the source of these assumptions? Can they be adjusted upward to more accurately reflect the expected intensity of remaining services? On a related note, should the outlier claims adjustment increase following the reduction to claims assumed here?
As discussed in the actuarial presentation, fee schedules are not expected to be increased during the projection period. See response to Question # 7 for the one known exception. Managed care organizations are expected to manage provider billing practice changes to ensure they do not inflate costs inappropriately.
Should the managed care savings assumptions be reduced in Phase 3 since those counties are more rural than the other regions? This would appear to be a reasonable assumption.
The same managed care factors were used to generate savings for all three phases. The absolute dollar savings will vary by phase based on the duration of the program due to staggered program start dates. Actual data from first year experience will be studied to set future rates.
How wide is the range from the midpoint to the upper and lower bound of the rate ranges?
This varies by rate cell and has not been specifically calculated.
Given the apparent aggressiveness of the trend assumed, the managed care savings, and the reliance on significant assumptions and estimate for the first year in the program, can the State consider using the midpoint of the actuarial range rather than 25% above the low end of the range?
Rates represent the degree of change to the system that DHH and its partner CCNs must achieve to meet the state's financial objectives.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 53 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
723 Data Book
718 See response to #539.
186 WellCare 1.03 General Instructions 3
Aetna Better Health, Inc.
How are costs for infusion drugs reflected in the data book? Are there certain infusion drugs excluded?
Excluded pharmacy defined within the RFP is “prescription drugs dispensed through pharmacies”; therefore, those types of drugs covered in a physician program would be covered through the CCN.
Aetna Better Health, Inc.
Databook vs. Actuarial
Certification Databook &
Attachment B
Databook - PMPM costs, Attachment B - pages 29- 36
Our initial review indicates an unexpected difference between the FY09 & FY10 PMPM costs in the databook the FY09 & FY10 PMPM costs in the rate development (Attachment B) of the actuarial certification? For example, New Orleans, Family & children, ages 6-13, the databook (less pharmacy) has FY09 = $40.99 and FY10 = $43.09. Attachment B (page 29) has these values as $41.12 and $42.12 respectively. It appears that FY09 values are overstated by 0.3% and FY10 values are understated by approximately 2.2% in the rate development compared to the databook. This would understate the true blended rate by 1.2%. If adjustments were made to the databook PMPM values, please detail these by rate cell.
Financial Reporting
Guide
The Supplemental Financial Reporting Guide for Prepaid Coordinated Care Networks (CCN-P) states that financial reporting should only address covered services for recipients eligible for the CCN-P Program. Certain health plans may intend to write the CCN-P line of business in the same licensed HMO as other lines of business (e.g., commercial, Medicare). While separating revenue or expenses can readily be done by line of business, separating assets and liabilities that way is difficult. Does DHH have any suggestions to alleviate this issue? Please confirm that it is not the intention of DHH that Proposer's isolate the CCN-P line of business in its own HMO.
DHH expects the Proposer to isolate the CCN-P line of business and report on it separately from other lines of business.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 54 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
623 N/A N/A 22
624 N/A N/A N/A
625 N/A N/A N/A
536 WellPoint General N/A -
555 WellPoint General N/A - See response to Question # 111.
556 WellPoint General N/A -
537 WellPoint General N/A -
Children's Hospital Health Plan
Financial Reporting
Guide
The instructions clarify that multiple month inpatient stays should be recorded in the admission month. Should transfers be recorded based on the admit month of the first admission or the 2nd?
Transfers should be recorded based on the admit month of the second admission.
Children's Hospital Health Plan
Financial Reporting
Guide
The quarterly profitability statements and utilization report provide a lot of detail but only for the current quarter. Since those reports are created without any paid claims run out, there is a significant amount of IBNP estimate in the numbers which minimizes its value. Has DHH considered showing these reports on a YTD basis or having prior quarters continually restated to include current data?
The quarterly profitability statements and utilization are designed to incorporate IBNR adjustments. To the extent that prior IBNR estimates require adjustment, this should be reported in the current quarter. Continuous restatement of prior quarters is deemed to be too cumbersome. Analysis of quarterly trending will be performed by DHH once financial statements are submitted and aberrations or inconsistencies from prior quarters will require explanations to the extent they are not addressed in footnote disclosures.
Children's Hospital Health Plan
Financial Reporting
Guide
The logic used to group claims into all of the required types of service is not always straightforward. Will DHH provide the codes used to do so?
At this time, DHH does not plan to develop hierarchical coding definitions for financial reporting service categories. It is incumbent upon the CCN-P to configure their systems using general industry coding logic to report upon each service category.
What functions and/or roles need to have the desktop configuration prescribed in the RFP in the system's requirements?
Call Center Operations, Claims EDI Operations, Authorized Services Operations, Member Services Operations.
Pharmacy services are carved out. Does the state provide pharmacy data to the CCN? Need to know file format, frequency, etc.
Dental services are carved out but dental data is needed for EPSDT/Form 416 reporting. What dental data will the state provide? Need to know file format, frequency, etc.
DHH will provide all claims data for carved out services, refreshed weekly , from which the dental data can be extracted. The file format for Medicaid claims data will be added to the Systems Companion Guide.
Does the State want to develop regulations that require plans to share medical records and facility reviews so providers aren't reviewed by numerous plans?
It is the CCNs responsibility to develop procedures and protocols for the review process.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 55 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
557 WellPoint General N/A -
563 WellPoint General N/A - Does HEDIS need to be reported by region?
Generally, what data is provided by the state to the CCN (for services that are carved out) to support the QAPI program? Need to know file format, frequency, etc.
SFY 09 and 10 claims data is available for entities once a flash drive, Letter of Intent, and a signed Data Use Agreement has been provided. Claims data for carved out services will be available to CCNs and refreshed weekly. The file format has not been finalized
All performance measures shall be reported at the CCN-model and entity level . An entity is corporate level and may cover multiple GSAs. Entities with common corporate structure will be reviewed and evaluated statewide, not by GSA.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 56 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
250 General N/A
252 General N/A Currently we do not have a single source provider for glasses
Coventry Health Care of Louisiana,
Inc.
current CPT codes in the Louisiana Medicaid FFS Fee Schedule currently reported for reimbursement consideration.
http://www.lamedicaid.com/provweb1/fee_schedules/FEESCHED.pdf
• 92002 EYE EXAM; INTERMEDIATE; NEW PT 47.09• 92002 EYE EXAM; INTERMEDIATE; NEW PT 56.50 • 92004 EYE EXAM; COMPREHENSIVE; NEW PT 89.15• 92004 EYE EXAM; COMPREHENSIVE; NEW PT 106.97 • 92012 EYE EXAM; INTERMEDIATE; ESTABL PT 49.59• 92012 EYE EXAM; INTERMEDIATE; ESTABL PT 59.51 • 92014 EYE EXAM; COMPREHENSIVE; ESTABL PT 72.62• 92014 EYE EXAM; COMPREHENSIVE; ESTABL PT 87.15
As evidenced by the CPT code definitions included in the current Louisiana Medicaid FFS fee schedule “routine eye examination” is not in the description. Additionally, enrollees of Louisiana Medicaid have unlimited access to medically necessary and appropriate medical services which are often billed using the same 92XXX series codes. Delineation is needed between routine and medical codes to insure proper access, utilization and payment. Therefore, can the CCN’s vision care partner/vendor utilize the following Health Care Procedural Coding System “HCPCS” codes; S0620 (new patient) and S0621 established patient) as the routine eye examination, as these codes are specifically defined as "routine eye examination including spectacle refraction".
With the introduction of the HCPCS codes into the Louisiana Medicaid program we will be able to not only use our current provider rates, but also more accurately report routine eye encounters vs. eye medical encounters.
These are the correct fees. The following codes are the ones for children 0-15: 92002 EYE EXAM; INTERMEDIATE; NEW PT 56.50 92004 EYE EXAM; COMPREHENSIVE; NEW PT 106.97 92012 EYE EXAM; INTERMEDIATE; ESTABL PT 59.51 92014 EYE EXAM; COMPREHENSIVE; ESTABL PT 87.15 The following codes are for recipients 16 years old and older:92002 EYE EXAM; INTERMEDIATE; NEW PT 47.09 92004 EYE EXAM; COMPREHENSIVE; NEW PT 89.15 92012 EYE EXAM; INTERMEDIATE; ESTABL PT 49.59 92014 EYE EXAM; COMPREHENSIVE; ESTABL PT 72.62
Coventry Health Care of Louisiana,
Inc.
In order to control quality and costs; can the CCN’s vision care partner/vendor mandate the use of a single source optical surfacing laboratory for the fabrication of eligible eyeglasses?
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 57 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
253 General N/A We currently do not pay a dispensing fee
249 General N/A Yes; yes as an expanded benefit.
251 General N/A Yes
Coventry Health Care of Louisiana,
Inc.
Is the CCN’s vision care partner/vendor required to pay a dispensing fee to contracted providers for delivery and fitting of covered eyewear?
Coventry Health Care of Louisiana,
Inc.
Are the CCN’s vision care partner/vendor required to mirror the current Louisiana Medicaid FFS Fee Schedule for the codes contained? Can payment be made for codes not on the current Louisiana Medicaid FFS Fee Schedule?
Coventry Health Care of Louisiana,
Inc.
It is our understanding at this point, that the “mandated” routine eye care benefit for members under the age of 21 will be as follows (based upon the Louisiana Medicaid FFS Vision (Eye Wear) Provider Manual which was released on April 21, 2011 - http://www.lamedicaid.com/provweb1/Providermanuals/manuals/Eye-Wear/Eye-Wear.pdf):· One Routine Eye Examination Per Year ($0 Co-pay)· Up to three (3) pair of Regular Eyeglasses Per Year without review (prior-authorization) when Member meets certain minimum refractive requirements ($0 Co-pay)
Can the CCN’s vision care partner/vendor mandate prior-authorization of 2nd and 3rd pair of eyeglasses within the calendar year?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 58 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
684 General N/A
683 General N/A Yes, weekly
685 General N/A
686 General N/A
413 General N/A N/A N/A
415 General N/A N/A N/A
403 General N/A N/A N/A
Aetna Better Health, Inc.
Does DHH envision a role for the CCN collaborating with DHH's PBM to improve pharmacy savings and quality of care? If yes, please describe.
DHH's Pharmacy Benefits Management Section (managed in-house) is available and willing to collaborate with CCNs to improve pharmacy savings and quality of care. The prospective CCN may include suggestions/requests as part of the proposal or subsequent to Contract award.
Aetna Better Health, Inc.
Will we receive a paid claims data file for pharmacy, dental, and behavioral health carve-outs? If yes, what is the frequency that the state will provide these data?
Aetna Better Health, Inc.
We have received inquiries from providers regarding where the providers submits their claims for providing services to newly eligible members from the date of eligibility to the date they are enrolled with the health plan. Our assumption is in these instances the provider would bill the state as fee for service. Please advise where providers can get questions similar to this one answered.
Such questions can be submitted to CoordinatedCareNetworks@ la.gov. Until someone is enrolled in a CCN which will be prospectively on the first day of a month except for newborns, they will receive services through the Medicaid FFS program and submit bills to the Medicaid fiscal intermediary.
Aetna Better Health, Inc.
Are the CCNs to offer their standard provider subcontract to the Office of Public Health or is DHH going to provide a document for the CCNs to utilize? If the CCNs are to utilize their own document, are CCNs permitted to engage OPH in contract/LOI discussions at this time?
DHH is not providing a document for the CCNs to utilize in subcontracting with OPH. Prospective CCNs are permitted to engage OPH in contract/LOI discussions at this time.
AmeriHealth Mercy of Louisiana
Please advise as to what the average increase in outpatient charge/ cost levels has been since FY 07/08?
Recent history of the average CCR's: 10/08: .2798, 2/09: .2618, 7/09: .2592, 10/09: .2411, 3/10: .2270, 6/10: .2262, 10/10: .2156, 5/11: .2132
AmeriHealth Mercy of Louisiana
Will DHH provide historical paid inpatient and outpatient dollars and days/visits summarized by facility and member parish? This would provide a mechanism for the prospective CCNs to determine high volume facilities for each parish and region.
MRO-46 report provides inpatient utilization by parish. MWM-19 report provides total expenditures by parish.
AmeriHealth Mercy of Louisiana
Please provide the average % of Cesarean versus Vaginal Deliveries by Region and Parish.
This information has been placed in the Procurement Library under Quality

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 59 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
410 General N/A N/A N/A
411 General N/A N/A N/A
412 General N/A N/A N/A
418 General N/A N/A N/A
416 General N/A N/A N/A DHH does not reimburse hospitals on the basis of DRGs
417 General N/A N/A N/A
497 HMO Louisiana, Inc. Appendix KK B.17 12
407 N/A N/A N/A An updated Hospital manual will be online soon.
408 N/A N/A N/A
405 N/A N/A
AmeriHealth Mercy of Louisiana
Please provide a detailed listing of covered services (with appropriate code sets where available)
These are included in the Medicaid services chart, manuals and fee schedules at www.LaMedicaid.com
AmeriHealth Mercy of Louisiana
Please provide detailed listings of benefit limitations (with appropriate code sets where available)
These are included in the Medicaid services chart, manuals and fee schedules at www.LaMedicaid.com
AmeriHealth Mercy of Louisiana
Please clarify whether referrals have been required historically for any non-PCP provided service outside of the CommunityCare Program.
Historically referrals have been required for some non-PCP provided service outside of the CommunityCare Program. If the recipient is linked to a PCP and the service is not an “exempt” service, then a referral from the PCP is required.
AmeriHealth Mercy of Louisiana
Will DHH provide the # of admits in addition to the # of days shown for each rate cell in the data book.
Since claims are paid on a per diem basis, it will be difficult to provide admit data.
AmeriHealth Mercy of Louisiana
Will DHH provide historical paid inpatient dollars and days summarized by DRG of major diagnostic category?
AmeriHealth Mercy of Louisiana
Will DHH provide historical paid physician dollars and visits, summarized by member parish and provider ID? This would be helpful in determining major providers for each parish or region.
CCN can ascertain from the Provider Listing by sorting on unduplicated enrollees and payments.
Qualifications and Experience
Could you please define the types considered in this requirement. Fox example, insurance contracts with our customers vs. vendor/government contracts.
DHH is most interested in contracts for the kinds of services that DHH is seeking to procure and the reason for termination of those contracts.
AmeriHealth Mercy of Louisiana
lamedicaid website
Will DHH be providing updated Hospital Provider Handbooks/training documentation?
AmeriHealth Mercy of Louisiana
lamedicaid website
Will DHH be providing updated Professional Handbooks/training documentation?
An updated Professional Services manual will be online soon.
AmeriHealth Mercy of Louisiana
Louisiana Register Vol 29, No. 12
December 20, 2003
Hospital Program Out -of-State Hospitals Inpatient Services Reimbursement
Reduction
This document was provided by the State in follow-up to a conference call held on 9/24/2010 with prospective CCNs. Please provide current "Medicaid per diem rates of the state wherein the services are provided" for border or other states paid historically in Medicaid Program. Also, please provide a current rate listing for outpatient reimbursement to these hospitals.
Outpatient fee -for- service codes are paid from the TOS 30 fee schedule that is online. Codes that are paid at a % of billed charges are paid at 31.04% of billed charges. The inpatient per diems have not changed since the last document was provided.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 60 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
86 N/A N/A N/A N/A
84 N/A N/A N/A N/A
88 N/A N/A N/A N/A
85 N/A N/A N/A N/A
87 N/A N/A N/A N/A
782 N/A N/A N/A N/A
Barbara Coopersmith @
Pediatric Medical Clinic
Can you furnish us with a list of the companies that are applying as CCNs?
DHH has posted on the MakingMedicaidBetter.com website the name of those entities that have submitted a non-binding Letter of Intent to propose. As DHH receives additional letters, we will be posting them in the procurement library of the appropriate CCN model type.
Bill Barton @ McKesson Health
SolutionsAre the attendees lists from the proposers' conferences on Monday, April 18 and Tuesday, April 19, posted on the Web?
Yes. All details from the proposers' conferences can be found at www.MakingMedicaidBetter.com
Iris Malone@Lourdes Regional Medical
Center
Will School based Health Centers be able to continue their "waived" status for providing care to school kids without going through their PCP for approval? Also will Nurse Practitioners be able to get reimbursed for services at these school based health centers even if they are not considered the student's PCP?
School-based health centers will be required to follow the procedures and protocols of the CCN.
Reimbursement for nurse practitioners will be depend on the terms and conditions specified in the contract that is signed with the CCN.
Marty Bennett @ Riverside Family
Medicine
We are an RHC in lower Livingston Parish. Our service area includes Regions 2 & 9. If there are 2-3 CCN's, per model, assigned to each GSA is there consideration or guidance from DHH as to how we should pursue contracting? Could this mean we could potentially have to contract w. 12 (3 each model and 6 each GSA) CCN's?
DHH has posted in the Procurement Libraries on the MakingMedicaidBetter.com website the names of those entities that have submitted a Letter of Intent to propose for CCN-P and CCN-S, along with contact information for each. The exact number of contract
Todd Johnson @ Bayer HealthCare
Diabetes Care
What effect will the CCN Implementation have on those Diabetes Meters and Strips that are currently covered by LA Medicaid today? Will each CCN have its own preferred formulary with respect to glucose meters and strips?
DME and supplies are a covered service in the CCN-P. Each CCN may have their own formulary,
Amerigroup Corporation
How will the CCN initiative interface with the Coordinated Systems of Care initiative being implemented by the Department of Children and Family Services?
The CSoC State Management Organization will coordinate specialized behavioral health services. The CCN will interface with the SMO in making referrals for specialized behavioral health.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 61 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
406 N/A N/A N/A
282 14 N/A N/A
400 N/A N/A N/A When will this be available for review?
215 HMO Louisiana, Inc. RFP 1.9 Schedule of Events 9
500 Adams and Reese RFP 1.9 Schedule of Events 10 That is correct
279 RFP 1.9 Schedule of Events 10 3/1/12 is correct
280 RFP 1.9 Schedule of Events 10 The Readiness Review is scheduled for 2011 rather than 12
246 RFP 1.9 Schedule of Events p. 10 Correct
245 RFP 1.9 Schedule of Events p. 9 Correct
AmeriHealth Mercy of Louisiana
Outpatient Hospital Fee
Schedules posted to
lamedicaid website
Please clarify how the prospective CCNs may identify Sole Community, Small Rural, State versus other facilities for appropriate understanding of application of the specific fee schedules.
A breakdown of hospitals by sole community, small rural and state has been posted in the CCN Procurement Library, located under Traditional Medicaid Providers.
Louisiana Healthcare Connections
Quality Companion
GuideWhen does DHH plan to make the Quality Companion Guide available?
The EQRO will develop the Quality Companion Guide. The Quality Companion Guide should be available on 1/1/12.
AmeriHealth Mercy of Louisiana
Quality Companion
GuideThe EQRO will develop the Quality Companion Guide. The Quality Companion Guide should be available on 1/1/12.
Readiness review will occur September 1 to October 15. Will these reviews be conducted all at once or will different areas of operation be reviewed separately? In either event, what order of review is to be expected?
The first step in Readiness Reviews will be a be a desk review of submissions that are due within 30 days of the date the CCN signs the contract. The on-site Readiness Review will be at the CCN's Louisiana location and may also include a systems review at an out-of-state location if applicable. Additional information relative to the order of review will be provided after announcement of Contract Award.
Please confirm the correct "Go Live" Date for GSA "B" is March 1, 2012.
Louisiana Healthcare Connections
The Go-Live for GSA B is listed as 3/1/2011, please confirm that this date should be 3/1/2012?
Louisiana Healthcare Connections
The Readiness Review date for GSA C is listed as September-December 2012, but the Go-Live is scheduled for 5/1/2012 - please clarify this timeline.
Coventry Health Care of Louisiana,
Inc.The go-live date for GSA 'B' says "March 1, 2011". This should be "March 1, 2012", correct?
Coventry Health Care of Louisiana,
Inc.The deadline for member enrollment says "December 23, 20011". It should be "December 23, 2011".

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 62 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
299 RFP 2.4 15
631 RFP 2.6 Bond Requirements 17 And addendum will be issued to correct the numbering
581 RFP 2.6 Bond Requirements 17-18
632 RFP 3.0 Eligibility 19 et seq
272 RFP 4.1 29
AmeriHealth Mercy of Louisiana
Moral and Religious Objections
Please confirm that a CCN may elect not to cover family planning services because of moral or religious objections. Also, if the CCN elects not to cover family planning services because of moral or religious objections, what is the mechanism for members to access such benefits? If the CCN elects not to provide family planning services, will this negatively affect the bidder's score?
CCNS may elect not to cover family planning services because of moral or religious objections. CCNS may assure that members receive services and provide coordination and reimbursement. Alternatively, the CCN's capitation payment will be reduced and the services will be reimbursed FFS. CCNs that elect not to provider family planning services must complete Item F-8 of Appendix KK . Depending on the response, the score may or may not be negatively affected.
Children's Hospital Health Plan
The sub-paragraph number is incorrectly established i.e. 2.6.1 sub 2.5.11, 2.5.12 etc…
Louisiana Hospital Association
In the event of a default by the CCN, what priority order will debts of the CCN to providers be paid?
The bond is not intended to pay debts to providers. The purpose of the bond is to assure that DHH administrative costs and the additional unbudgeted costs for purchasing health care for enrollees elsewhere in the event of CCN contract early termination is accounted for.
Children's Hospital Health Plan
Can you explain the SPAN OF COVERAGE concept used by Louisiana Medicaid? For example: (1) If some is already an inpatient on the day they become Medicaid or CHIP eligible who is responsible for paying the hospital bill? (2) If someone is in the hospital on the day they age termed from Medicaid/CHIP, how is the bill paid? NOTE: The situation of a member moving from CCN A to CCN B while an inpatient is already addressed in 6.32.3.
The RFP language has been amended to state that the relinquishing CCN is responsible for the member’s hospitalization until the member is discharged. The receiving CCN is responsible for all other care.
Louisiana Healthcare Connections
4.1.6.13 Member Services Manager
Is this the correct description for a Member Services Manager? The description is more provider focused.
This has been amended to read as follows: Member Services Manager to coordinate communications between the CCN and its members There shall be sufficient Member Services staff to enable members to receive prompt resolution of their problems or inquiries and appropriate education about participation in the CCN program.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 63 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
498 HMO Louisiana, Inc. RFP 4.2 In-State Positions 31
495 HMO Louisiana, Inc. RFP 5.0 CCN Reimbursement 33 No.
583 RFP 5.12 Third Party Liability 37 DHH Legal is reviewing this request.
The list of key positions and the requirement for them to be located in the State of Louisiana differs. Please clarify which positions shall be in Louisiana and which positions should be in Louisiana?
Section 4.2 of the RFP states the positions that should be located in Louisiana. Requirements for some positions are that the individual have a Louisiana license.
As implemented through CMS Medicaid managed care regulations, the actuarial soundness provision requires state pay premiums to its participating Medicaid health plans that are actuarially sound: neither too high or too low. Will the state’s budgetary status (especially economic downturns) play any role in overriding “actuarially sound” principles? If so, what is methodology (weighted factor) used in forecasting?
Louisiana Hospital Association
If the CCN's total collections exceed the total amount of the CCN's financial liability for the member, what will be the CCN's responsibility with respect to those dollars? In situations where a third party is liable and Medicaid has submitted payment, LA RS 46:446.6 gives health care provider the right to recover the difference between the health insurer's original obligation for services provided to the insured and the amount the health care provider received from Medicaid, provided that the amount of the original obligation exceeds the amount paid by Medicaid. The LHA recommends that DHH incorporate the aforementioned statute and DHH's current process into the RFP to provide clarity as to how the TPL process works in Louisiana.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 64 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
308 RFP 5.2 33
482 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35 What cost settlements are made outside of the MMIS?
483 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35 What version of the ACGs will be used?
484 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35
AmeriHealth Mercy of Louisiana
Maternity Kick Payments
Please advise as to the average lag time between a delivery event and receipt of the kick payment. Also, please advise as to whether there are circumstances under which CCNs may input delivery information into the Louisiana Electronic Event Registration System, independent of the hospitals submission, to ensure timely receipt of kick payments.
DHH will receive a monthly file from LEERS, so that the kick payments coincide with capitation payments. The CCNs are not to update LEERS, as this is responsibility of the Hospitals.
Inpatient hospital services – state hospitals, children’s hospital, & transplant services in all hospitals; Outpatient hospital non fee schedule services – all hospitals, note rural hospitals paid 110%; Outpatient hospital all fee schedule except lab – rural hospitals (110% of cost); Outpatient hospitals outpatient surgery & rehab – children’s hospital; Rural health clinics licensed as a hospital department to a small rural hospital – 110% of cost; Note – state hospitals paid costs on all fee schedule services except lab through UPL
ACG Case-Mix System Medicaid Software version 9.0, which only uses diagnoses for risk scoring purposes.
Will the ACGs risk adjustment model be used to develop concurrent or prospective risk scores?
ACG developers recommend using ACG mutually exclusive cells and concurrent model for risk adjustment of prepaid payment due to: * simplicity* less prone to manipulation * stability * ease of making local calibrations based on PMPM average.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 65 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
485 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35
486 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35
487 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35
488 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35
489 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35 Will pharmacy data be used in the risk adjustment process?
490 HMO Louisiana, Inc. RFP 5.7 Risk Adjustment 35
Please provide additional detail on how age and gender will be considered and not double counted in the risk adjustment process.
The inherent risk within the demographic (age/sex) based rates will be evaluated. This will be accomplished by calculating the average PMPM for each CCN-P based on its own member demographics and then comparing this value to the overall (all CCNs) PMPM. The ACG-based relative risk score will then be divided by the inherent rate risk value. An example of this calculation was provided in the Tuesday, April 19th presentation (slide #38-40) to the potential CCNs which can be accessed through the Making Medicaid Better website.
Please provide additional detail on how members who have enough months of enrollment to be scored, but who have no claim experience will be included in the risk adjustment process.
Members without any historical claims experience, but with six or more months of Medicaid eligibility will receive the combined average cost (on a relative basis) for the following ACG categories: Non-users and No diagnoses or only unclassified diagnoses.
Please explain how the CCNs will be able to evaluate the risk adjustment methodology used to adjust the capitation rates? What information will be made available to the CCNs so that they can evaluate the process?
Each CCN-P will receive its distribution of its members by ACG category. For comparison purposes, the distribution of members by ACG category will also be provided for All CCNs combined. A separate report with these values will be provided for each risk-adjustment consolidated group and GSA.
What process will be used to calibrate the ACGs to this Medicaid population?
Two years of historical Louisiana Medicaid data will be used to develop the relative cost attributable to each ACG.
No, only diagnoses will be used to classify members into ACG categories.
How will prior claim costs be incorporated into the risk adjustment process?
Prior claim costs corresponding to covered benefits will be incorporated in the development of cost weights. However, prior costs will not be a determinant in the ACG classification. Only diagnoses will be used to classify members into ACG categories.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 66 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
783 RFP 5.9 Medical Loss Ratio 36 No
110 RFP 5.9 Medical Loss Ratio 36
582 RFP 5.9 Medical Loss Ratio 36
329 RFP 6.17 55
701 RFP 6.2 43
734 Advocacy Center RFP 6.20 56
Amerigroup Corporation
With the inclusion of a requirement of “at risk” plans to return premium if a plan reports an annual MLR below 85%, will the state also implement a maximum MLR exposure where by plans will be provided additional premium in the event care costs run above breakeven levels for the plan?
Coventry Health Care of Louisiana,
Inc.Return of Funds - MLR below 85% will need to be reimbursed. How should reimbursements be sent?
Via check or bank draft made payable to the Louisiana Department of Health & Hospitals no later than August 1st following the MLR Reporting year.
Louisiana Hospital Association
The language in the MLR calculation appendix (H) varies somewhat from the federal language. Can DHH clarify the variance?
DHH's language is an adaptation of the federal requirements specifically for Louisiana Medicaid health plans.
AmeriHealth Mercy of Louisiana
DME, Prosthetics, Orthotics, and Certain
Supplies (DMEPOS)Please clarify whether CCNs are required to cover DMEPOS for members over the age of 21.
Yes, DMEPOS is a covered service for Louisiana Medicaid enrollees age 21 and older and is included in CCN core benefits and services.
Aetna Better Health, Inc.
Eye Care and Vision Services
Do all enrolled and eligible members have eye care and vision service benefits? If all members have eye care and vision service benefits, what are the specific benefits and/or excluded services for those members eligible for EPSDT and those not eligible for EPSDT? What is the states fee for service schedule for eye care and vision services including eye wear (glasses and contact lenses)?
Vision services are only covered for recipients under age 21 (EPSDT eligible individuals).. Our fee schedule is posted online
Medical Transportation Services
What sanctions apply if a CCN fails to schedule or actually provide non-emergency medical transportation for plan members as required?
Failure to provide a CCN covered service thatis not otherwise associated with a performance standard and such failure results in actual harm to a member or places a member at risk of imminent harm.Seventy-five hundred dollars ($7,500.00) percalendar day for each incident of noncomplianceper CCN per GSA.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 67 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
409 RFP 6.2 N/A
741 Advocacy Center RFP 6.31 62
633 RFP 6.31 Continuity of DME… 62
AmeriHealth Mercy of Louisiana
Excluded Services/ Prohibited Services
Please provide detailed listings of excluded services (with appropriate code sets where available)
We rarely list specific codes/services that we do not cover. If the service is not listed in our policy/fee schedule, then it is not covered.
Continuity for DME< Prosthetics, Orthotics, and Certain Supplies
The RFP provides that "In the event a Medicaid member entering the CCN is receiving Medicaid covered durable medical equipment, prosthetics, orthotics, and certain supplies services the day before CCN enrollment, whether such services were provided by another CCN or Medicaid fee-for-service, the CCN shall be responsible for the costs of continuation of these services, without any form of prior approval and without regard to whether such services are being provided by contract or non-contract providers. The CCN shall provide continuation of such services for up to thirty (30) calendar days or until the member may be reasonably transferred (within timeframe specified in this RFP) without disruption, whichever is less." If the member cannot "be reasonably transferred" within the 30 days (and indeed the time frames DHH is allowing for prior approvals would not generally generate a decision within 30 days of enrollment), why must the services that DHH previously determined to be "medically necessary" be terminated?
This provision does not require services to be terminated, it provides a timeframe in which the CCN must transition care from either FFS provider or another CCN.
Children's Hospital Health Plan
Does a mechanism exist whereby the CCN will know that a new member is already receiving DME, prosthetics, orthotics, other certain supplies, or other services where continuity of services is the CCN's responsibility?
In conjunction with the transition of enrollees who have been receiving services through FFS Medicaid, DHH will provide historic claims data for analysis. In addition, DHH will --to the extent possible--identify members with ongoing authorizations for NEMT (to dialysis, for example) and certain supplies.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 68 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
634 RFP 6.36 66
397 RFP 6.39 Care Transition 68, 69 Section 6.39 is being deleted.
585 RFP 6.8 49
586 RFP 7.1 70 Refer to definition of "Documented Attempt" in Glossary
Children's Hospital Health Plan
Chronic Care Management Program
(CCMP)
When will we receive Claims data to support requirements regarding number of patients in specific disease states (Hypertension as precursor to CAD or stroke, Sickle Cell Anemia, COPD, Low Back Pain, Chronic Pain)
SFY 09 and 10 claims data is available for entities once a flash drive, Letter of Intent, and a signed Data Use Agreement has been provided. The data set is being modified to include a pseudo-identifier to identify the number of payments in specific disease states.
AmeriHealth Mercy of Louisiana
This seems to be redundant with Sections 6.32.1 -6.32.5 (p. 63) -- Should Section 6.39 be deleted?
Louisiana Hospital Association
Emergency Medical Services and Post
Stabilization Services
In section 6.8, it states that the CCN shall reimburse the professional component of these services at a rate equal to or greater than the Medicaid fee for service rate when a CCN provider authorizes these services. This appears to be inconsistent with previous material indicating the requirement of authorization of emergency services is prohibited. Can DHH clarify?Also, what about the technical component or global reimbursement?
Section 6.8 refers to Emergency ancillary services which include, but are not limited to, radiology, pathology, emergency medicine and anesthesiology.
Louisiana Hospital Association
General Provider Network Requirements
In section 7.1.6, it states that if a current Medicaid provider requests participation in a CCN, the CCN shall make a good faith effort to execute a contract. In the event an agreement cannot be reached and the provider does not participate in the CCN, the CCN has met this requirement. Can DHH provide some clarity as to what will be considered "good faith" or "bona fide"? To what degree will a good faith effort by a CCN be measured? Will providers have the ability to challenge/appeal the out-of-network rate of 90% of the Medicaid rate for lack of "good faith"?Also, over what period of time do the documented attempts have to occur before that timeframe resets? Is it 3 per year? 3 per CCN contract term with the State? 3 total?
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 69 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
212 HMO Louisiana, Inc. RFP 7.12 91
506 RFP 8.1 95
635 RFP 8.8 104
Subcontract Requirements
Dawn Cantrell raised this question in the CCN Workgroup. The RFP allows us to enter into agreements with subcontractors, but we need clarity about DHH’s ability to work directly with our subcontractor. Will DHH work directly with our subcontractors, or will all information, files, payments, etc. come directly to the CCN?
DHH will not work directly with the subcontractor unless so requested by the CCN and approved by DHH.
Kyle Viator - LSU Health System
Utilization Management General
Requirements
Could additional detail be provided in this section relative to the CCN's responsibility for identifying alternative placements for patients who may no longer be in need of placement in an acute care setting? We would recommend specifically including language that would prohibit CCNs from denying hospital inpatient days due to inability to locate a lower level of care for a patient as this is a care management responsibility of the CCN. Again, as the state's safety net hospital network we have a much higher Medicaid patient mix than other hospitals across the state. Historically, at discharge we have experienced a significant challenge in access to alternative providers at more appropriate levels of care for Medicaid patients.
The RFP has been amended to add Section § 8.3.
Children's Hospital Health Plan
PCP Utilization & Quality Profile
Reporting Requirements
Does DHH have a specific format that must be used by the CCN to provide the annual report to DHH?
The CCN should submit sample templates or proposed formats for the annual report.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 70 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
589 RFP 9 105
348 RFP 9.1 105
577 RFP 9.11 105
Louisiana Hospital Association
Minimum Reimbursement to In-
Network Providers
Can DHH further clarify how transplant and hemophilia services are to be reimbursed, both in-network and out-of-network?
Transplant services are reimbursed in the interim at the hospital's prospective per diem rate. Actual costs of the transplant services (by type) are calculated on the hospital's filed cost report. Final payment is cost subject to each hospital's transplant per diem limitation (separate limit for each approved type of transplant). Hospitals meeting the criteria (major teaching hospital affiliated with a comprehensive hemophilia care center) are reimbursed for their costs of blood products per patient that are in excess of $50,000.
AmeriHealth Mercy of Louisiana
Minimum Reimbursement to In-
Network Providers
Per the RFP, the CCNs "rate of reimbursement shall be no less than the published Medicaid fee-for-service rate in effect on date of service"... and "for providers who receive cost based reimbursement for Medicaid services, the published Medicaid fee-for-service rate shall be the rate that would be received in the fee-for-service Medicaid program". Please confirm that payments made to cost based providers by the CCNS based on the prospective published rates will not need to be subsequently adjusted for cost settlement results. If CCNs must cost settle for any services please provide documentation clarifying the process and associated timeframes.
Since reimbursement must be not less than it would have been without CCNs, the CCN will need to adjust for cost settlement results. Documentation requested will be available following award of contracts.
United Healthcare of Louisiana
Minimum Reimbursement to In-
Network Providers
The fee schedule link on the LA Medicaid website does not include chiropractic codes (98940-98943). However, chiropractic is a covered benefit. Where would the reimbursement rates for these codes be located?
Providers have to contact Molina Provider Relations to obtain reimbursement for these codes. Chiropractors are only reimbursed for 2 procedure codes and not all of the procedure codes on the Professional Services Fee Schedule, therefore, they are not included on it. Current reimbursement is as follows: 98740-17.64 (recipients 16+) and 21.17 (0-15) 98941-24.47 (recipients 16+) and 29.37 (0-15)

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 71 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
590 RFP 9.3 106
132 WellCare RFP 9.3 106 No
216 HMO Louisiana, Inc. RFP 9.9 111
18 RFP 11 118 Please advise who is the contracted enrollment broker.
Louisiana Hospital Association
Reimbursement to Out-of-Network Requirements
Will DHH require the CCN to report the number, dollar amount, and type of claim by provider when the service is provided out of network? If so, how often? How will DHH make this reporting publicly available and accessible?
The reporting requirement for out-of-network services is still under development.
Reimbursement to Out-of-Network
Providers
Are there any payment reciprocity rules with Medicaid providers in border states (out of network)? Specifically if a provider in a border state excepts Medicaid in their respective state -- do they have to accept payment for Medicaid in LA if they see a LA Medicaid member? If so, what rates will apply (i.e. Medicaid reimbursement in their respective state or LA Medicaid reimbursement)?
Supplemental Provider Payments
Section 9.9 indicates that the CCN is not responsible for reimbursement of GME. Section 9.1.1 requires that the CCN rate of reimbursement shall be no less than the published Medicaid fee for service rate in effect on the date of service. Please provide the process, formulas, etc, that will be used for DHH to determine compliance with this requirement, given that published per diems for hospitals include compensation for GME and are not distinctly documented. If this is not the case, then can DHH clarify how it currently pays hospitals for GME at the specific hospital level.
The hospital per diem rates currently posted in the Procurement Library exclude GME.
Coventry Health Care of Louisiana,
Inc.Eligibility, Enrollment
and DisenrollmentThe contracted enrollment broker for the CCN Program will be selected through a competitive procurement process.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 72 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
776 RFP 11.13 130
558 WellPoint RFP 11.14 Daily Updates 124
636 RFP 11.14 Daily Updates 130
141 WellCare RFP 11.14 Daily Updates 130 When will the 834 companion guide be made available?
108 RFP 11.5 120 Will the county code, parish or name be on the 834 file?
637 RFP 12.1 132
595 RFP 12.10 143
Amerigroup Corporation
Enrollment and Disenrollment Update
This item states that the DHH Enrollment Broker will be provided updated enrollment and disenrollment information to the CCN-P on a regular basis. Will this information be limited to name, address, telephone number and preferred PCP or will additional information be included in the file? Will the CCN-P be given or have access to any other information about new members, e.g., historical fee for service claims data or encounter claims information if an enrollee was previously in another CCN-P?
Additional information will be included in the file, including but not limited to preferred language, whether member is new or was previously Medicaid FFS, previous CCN if any, TPL, Special Needs indicator. CCNs will have access to historic fee for service claims data and information on utilization from the relinquishing CCN if applicable.
The RFP requires the CCN to develop a PCP automatic assignment methodology in "collaboration" with DHH and requires DHH approval prior to implementation. Could DHH clarify what criteria they look for in the approval process?
The PCP automatic assignment methodology would include factors comparable to DHH's automatic assignment methodology to a CCN.
Children's Hospital Health Plan
Are the members in the Daily 834 file only pregnant women and newborns or are other categories of members also enrolled on a daily basis?
The 834 Enrollment File will include all newly assigned members.
Proposers shall utilize the Implementation Guide from CMS, and the EB shall assist DHH in creating a systems companion guide.
Coventry Health Care of Louisiana,
Inc.Members Relocating to
Another GSAYes DHH will provide a parish code/description file on the makingmedicaidbetter.com website.
Children's Hospital Health Plan
Marketing and Member Education
What Marketing efforts are afforded to allow CCN Providers with existing non-enrolled Medicaid members to retain these members during the enrollment process?
Section 12.7 provides guidance on provider marketing. All marketing and member materials used by providers must comply with the guidance detailed in section 12 and must be approved by DHH prior to distribution or use.
Louisiana Hospital Association
CCN Website Guidelines
The provider manual does not appear to be specifically listed as a requirement for the CCN website. Will DHH be mandating that the CCN make available the most current version of the provider manual prominently on its website?
See § 10.3.2.1
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 73 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
283 RFP 12.11 146
284 RFP 12.16 154
359 RFP 12.17 156
Louisiana Healthcare Connections
12.11.2.3 Welcome Calls
It appears we have 21 days for make welcome calls to new members for the initial wave and 14 days for ongoing membership. It further states we are required to make 3 attempts. Q - Is the expectation that all three attempts will be completed in the date range above or the 1st attempt?
It is the expectation that all three attempts will be made within that date range.
Louisiana Healthcare Connections
12.16.2 Call Center Performance Standards
12.16.2.1 states that 90% of calls need to be answered in 30 secondsPage 231 - Under the penalties section it states 95% of calls answered with in 30 seconds Q - Which % is correct?
90% is correct. The monetary penalties language has been modified to reflect that change. See Addendum #4.
AmeriHealth Mercy of Louisiana
Notice to Members of Terminated Providers
Is prior review & approval by DHH necessary for the form of written member notices of terminated providers? May the CCN adopt a template member notice?
Yes. The CCN may create a template for provider termination notice to be approved by DHH. The CCN will not have to provide the termination notice of a specific provider to DHH prior to distribution for the purpose of member material approval.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 74 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
754 Advocacy Center RFP 13.0 159
361 RFP 13 159
19 RFP 13 159 - 169
Member Grievance and Appeal Procedures
In response to Advocacy Center comments to § 3731(B)(1) of the Notice of Intent, as submitted to the Legislature, the Department wrote that "The Department is including in the RFP/contract requirements language that any appeal of an "action" will go directly to the state Fair hearing process. Concurrently, the CCN will do an informal review and be given the opportunity to reverse their initial decision which would result in dismissal of the state fair hearing by the Division of Administrative Law. The informal reconsideration is comparable to the current agency Conference for eligibility-related appeals. ¶ The role of CCNs in the appeal process is being limited to informal reconsiderations of appeals that will be regarded as state fair hearings." But this provision of the RFP is instead inconsistent with the Department's response submitted to the legislature, by stating "The member must exhaust the CCN's internal grievance/appeal procedures prior to accessing the State Fair Hearing process." What action is the Department taking that is consistent with Mr. Gregory's official response to comments, dated April 8, 2011?
Subsequent to Mr. Gregory's letter, in finalizing the grievance and appeals requirements a change was made. The CCN's internal review process is accelerated and must be completed within 30 days, or sooner if criteria for an expedited appeal is met.
AmeriHealth Mercy of Louisiana
Member Grievance and Appeals Procedures
Incorrect RFP section references are contained throughout Section 13. Please revise to reflect the correct RFP section references.
Refer to question #49 and addendum 3 for revisions to Section 13.
Coventry Health Care of Louisiana,
Inc.Member Grievance and
Appeals ProceduresPlease advise what the requirement is for day timeframes that do not specifically state business or calendar days.
Refer to 23.51 2 Time is of the Essence in Terms in Conditions which states that "any reference to “days” shall be deemed calendar days unless otherwise specifically stated."
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 75 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
757 Advocacy Center RFP 13.11 169 The correct reference should be "13.4.2, 18.0 and 18.8"
781 RFP 13.6 163 Yes, the Department will contract for Ombudsman services.
496 HMO Louisiana, Inc. RFP 14.3 Performance Measures 172 See Question # 365
101 RFP 14.4 178
198 HMO Louisiana, Inc. RFP 14.8 179
596 RFP 14.8 179
572 WellPoint RFP 15.6 187
262 RFP 16.5 Systems Refresh Plan pg 195 Does the state want to see our release process/plan? Yes
Recordkeeping and Reporting
Requirements
What are the intended references in the following sentence (§13.9 does not seem to be the right reference, and a second one seems to be missing): "Reports of grievances and resolutions shall be submitted to DHH as specified in §13.9 and of this RFP."
Amerigroup Corporation Notice of Action
Will there be an ombudsman program established to provide guidance and advice as Medicaid managed care beneficiaries navigate fair hearings, in-plan procedures, and dispute resolution?
When will the benchmarks for the five ($) Incentive Based performance measures be announced, and what is the methodology or standard used in determining these benchmarks?
Coventry Health Care of Louisiana,
Inc.Member Satisfaction
SurveysWill the first CAHPS survey be due at the first HEDIS submission?
The language is being amended to state that the CAHPS surveys will be due with all other Performance Measures
Health Plan Accreditation
How long does CCN have to become URAC accredited from the time of implementation of CCN? Is the URAC Health Plan module the only expected module to be achieved?
The CCN must become either URAC or NCQA accredited on the earliest possible date the CCN can apply for recognition.
Louisiana Hospital Association
Health Plan Accreditation
When will the plans be required to secure NCQA or URAC accreditation? The RFP does not directly speak to timing in this section.
The expectation is that CCNs will apply for accreditation at the earliest possible date which will differ depending on whether they are considered a new health plan.
We suggest the requirement for medical record auditing be coordinated across the CCNs. If a provider is commonly contracted across 6 CCNs, then the burden would be lower on the provider who wouldn't be asked 6 times, and the burden would be lower on the auditing team.
It is the CCNs responsibility to develop procedures and protocols for the review process.
Coventry Health Care of Louisiana,
Inc.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 76 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
787 RFP 16.9 Provider Enrollment 196Amerigroup Corporation
Please consider changing for following language from this section: “The CCN shall utilize these codes within their provider enrollment system. The objective is to coordinate the provider enrollment records of the CCN with the same provider type, specialty and sub-specialty codes as those used by DHH and the Enrollment Broker.” TO: “In order to coordinate provider enrollment records, the CCN shall utilize the published list of Louisiana Medicaid provider types, specialty, and sub-specialty codes in all provider data communications with DHH and the Enrollment Broker .”
Based on the suggestion, the language has been adopted by DHH. See Addendum.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 77 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
20 RFP 16.9 Provider Enrollment 196Coventry Health
Care of Louisiana, Inc.
The clause at the end of 16.9 leading up to the subsections 16.9.1-16.9.4 does not read right when read with the subsections - may be missing a verb? Please clarify; depending on response we may have additional questions.
utilize these codes within their provider enrollment system. The objective is to coordinate the provider enrollment records of the CCN with the same provider type, specialty and sub-specialty codes as those used by DHH and the Enrollment Broker.
16.9.1. The CCN shall provide the following:
a).Provider name, address, licensing information, Tax ID, National Provider Identifier (NPI), taxonomy and payment information;
b) All relevant provider ownership information as prescribed by DHH, federal or state laws; and
c) Performance of all federal or state mandated exclusion background checks on all providers (owners and managers). The providers shall perform the same for all their employees at least annually.
16.9.2.. The CCN Provider enrollment systems shall include, at minimum, the following functionality:
a) Audit trail and history of changes made to the provider file;
b) Automated interfaces with all licensing and medical boards;
c) Automated alerts when provider licenses are nearing expiration;
d) Retention of NPI requirements;
e) System generated letters to providers when their licenses are nearing expiration;
f) Linkages of individual providers to groups;
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 78 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
758 Advocacy Center RFP 20.5 235
244 RFP 21.4 Code of Ethics p. 246 Correct
380 RFP 22.5 Post-Turnover Services 255 Six (6) years
201 HMO Louisiana, Inc. RFP 23 Terms and Conditions 256
382 RFP 23.18 Force Majeure 262
493 HMO Louisiana, Inc. RFP 23.22 HIPAA Compliance 263
Excessive reversals on appeal
The RFP provides a single fine of $25,000 per year for plans with more than 10% of decisions reversed by state fair hearing decisions. It is easy to see that a plan with a 40% reversal rate could save far more than the $25,000. This is especially so, since for each request pursued to state appeal, many other recipients treated similarly may fail to appeal to that level. If a CCN is reversed on more than 10% of appeals, what if any sanctions, in addition to the $25,000 penalty, could it be subject to?
An addendum will be issued to revise the language to reflect DHH's original intent.
Coventry Health Care of Louisiana,
Inc.There is an error in the second sentence where it says "...they only entity…". It should be "...the only entity…".
AmeriHealth Mercy of Louisiana
The record retention timeframe is different than what is referenced in other sections - 5 years vs. 6 years. Please clarify the applicable timeframe.
Is a Louisianan licensed health insurer, as opposed to an health maintenance organization, qualified to be a CNN-P
This question should be directed to the Louisiana Department of Insurance.
AmeriHealth Mercy of Louisiana
The provision references Section 14.38 of the RFP; however, there is no such section. Please clarify the reference. The correct reference is §23.14
Who will distribute the NPP of Privacy Practice? If we will do it, are we sending a Notice they drafted or we drafted?
Each CCN is responsible for distribution of the HIPAA Privacy Notice to their members as part of the Welcome Packet. DHH will provide a template within 30 days of the date the Contracts are approved.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 79 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
240 RFP 23.25 265 Yes
381 RFP 23.3 Assessment of Fees 258
385 RFP 23.41 Rate Adjustments 269
Coventry Health Care of Louisiana,
Inc.Homeland Security
Considerations
The RFP states that the CCN shall perform the services to be provided under this Contract entirely within the boundaries of the United States. Bidder is contemplating subcontractor certain credentialing functions to a third party that will further subcontract one component of the credentialing process primary source verification to a company located outside of the United States. Primary source verification is limited to verifying the accuracy and truthfulness of information provided in the provider's application such as: licensure, educational background, work history, certifications and registrations such as DEA number, malpractice claims history, hospital privileges, board certifications, office locations. The Bidder still retains responsibility for approving the credentialing file and making the final decision regarding providers seeking credentialing. Would the use of the subcontractor's subcontractor that is located outside of the United States for this one component of the credentialing process violate section 23.25 of the RFP?
AmeriHealth Mercy of Louisiana
Is there a mechanism to handle disputes of amounts determined by DHH to be owed under Section 23.3?
Yes, Section 23.30 states "The CCN may request in writing an interpretation of the issues relating to the Contract from the Medicaid CCN Program Director. In the event the CCN disputes the interpretation by the Medicaid CCN Program Director, the CCN shall submit a written reconsideration request to the Medicaid Director.
AmeriHealth Mercy of Louisiana
Please confirm that the "provisions of the RFP for contract termination" that would apply would be the Termination for Convenience provision set forth in Section 23.49 of the RFP. Please confirm.
Nothing in this section shall limit DHH's right to terminate the Contract or to pursue any other legal or equitable remedies.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 80 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
119 WellCare RFP
774 RFP 4 and 12
291 RFP 1.6.1 Proposer Comments 5 Appendix B,
2.3.1 General CCN Requirements 14
This section requests the financial statements of persons with a controlling interest or with an ownership interest of 5% or more. This information would seem to be relevant in the case of a partnership, S corporation, sole proprietorship or similar entity; however may impact privacy of such individuals in the case of C corporations, particularly those that are, or are owned by, publicly-traded corporations. Publicly traded corporations may not be able to obtain the financial statements of persons or entities that own 5% or more of their stock since such owners are generally passive investors with no connection to the company apart from having purchased its stock in the open market. Could DHH clarify this requirement in the case of CNNs that are, or are owned by, publicly traded corporations?
2.3.1 will be amended in the RFP to read "As required in 42 CFR 455.104 (a), the CCN-P (hereafter called CCN in this RFP) shall provide DHH with full and complete information on the identity of each person or corporation with an ownership interest of five percent or greater (5%+) in the CCN, or any subcontractor in which the CCN has 5% or more ownership interest. The CCN shall also provide such required information including, but not limited to financial statements, for each person or entity with ownership or controlling interest of 5% or more in the CCN and any of its subcontractors, including all entities owned or controlled by a parent organization. This information shall be provided to DHH on the approved Disclosure Form and whenever changes in ownership occur."
Amerigroup Corporation
1.2.6 and 2.1.2
Purpose of RFP and Requirements for CCN-
P Entity
This item states that there could be as many as 3 CCN-Ps awarded contracts in each GSA. Item 2.1.2 states that a bidding entity may propose as both a CCN-P and as a CCN-S in the same GSA. If as many as 3 CCN-Ps can be awarded contracts to serve a single GSA and CCN-Ss can also bid to serve the same GSA, can you please clarify how many total entities could be awarded contracts in a single GSA?
A maximum of six entities; theoretically, as few as three entities
AmeriHealth Mercy of Louisiana
Proposers are cautioned to carefully review the RFP, including the "pro forma contract" -- Please clarify which document(s), and/or sections thereof, comprise the "pro forma contract."
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 81 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
507 RFP 10.1.1.3 153 An addendum will be issued to revise the language.
594 RFP 10.4.2 Provider Handbook 114 The means and timing is at the discretion of the CCN
351 RFP 10.4.3 Provider Handbook 114 30 days from the date the contract with DHH is signed
638 RFP 10.5.2 115 Yes
21 RFP 10.6.2.10 116 What is the required format for reporting complaints?
Kyle Viator - LSU Health System
Voluntary Selection of a CCN
Can adjustments be made to the requirement that special permission would have to be granted by DHH in order for family members to be assigned to different CCNs? There is concern that families might find it a considerable hardship to go through this process which will not be well known. As the state's public safety net provider we have historically provided access to services, including primary care which will be the main basis of network linkage, to an underserved population who has had considerable difficulty getting access to private providers through Medicaid. As such, we are concerned that children who have greater access to the private provider networks due to the enhanced reimbursement rate for their services may end up getting linked to a network that would not include the safety net providers and thus create difficulty in accessing timely and quality primary care for their parents.
Louisiana Hospital Association
This section states that the CCN shall disseminate bulletins as needed to incorporate any changes to the provider handbook, but does not cover means or timing. Can DHH clarify?
AmeriHealth Mercy of Louisiana
Please clarify whether the provider handbook must be presented to DHH for approval 30 days "prior to" the date the CCN Contract is signed, or 30 days "from" the date the CCN Contract is signed. [The original language is "no later than 30 days prior from the date..."
Children's Hospital Health Plan
Provider Education and Training
Can the Provider Training Manual and the Provider Handbook (10.4.3) be one in the same document?
Coventry Health Care of Louisiana,
Inc.Provider Complaint
SystemDHH intends to provide the format for this report no later than 60 days after Contracts are signed.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 82 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
22 RFP
23 RFP 10.6.3.1 117 Please define the meaning of a pre-processed claim.
Coventry Health Care of Louisiana,
Inc.
10.6.2.11
17.5.2
Provider Complaint System
Claims Dispute Management
116
209
Please clarify that the internal claims dispute procedure referenced in 17.5.2 is the process that must be exhausted prior to the provider seeking arbitration pursuant to Section 10.6.2.11. Why does 17.5.2 require the CCN to send these disputes to an independent reviewer, whereas 10.6.1 and 10.6.2 and their subparts specify the CCN's investigation and resolution responsibilities. Please explain how all of this is supposed to function. Typically, we do not send provider claims disputes for external review in other Medicaid markets.
to complaints concerning the CCN's policies, procedures or any aspect of the CCN's administrative functions.
Section 10.6.2.11 will be revised to read: "The provider complaint process shall not include provider payment issues. The provider shall adhere to the claims dispute process specified in Section 17.5.2 for denied or underpaid claims or group of claims bundled."
Section 17.5.2.1 will be revised to read: "The CCN shall develop an internal claims dispute process for those claims or group of claims that have been denied or underpaid. The process must be submitted to DHH for approval within thirty (30) days of the date the Contract is signed by the CCN.
Section 17.5.2.2 will be revised to read: "The Claims Dispute process shall allow providers the option to request binding arbitration for claims that have denied or underpaid claims or a group of claims bundled, by a private arbitrator who is certified by a nationally recognized association that provides training and certification in alternative dispute resolution. If the CCN and the provider are unable to agree on an association, the rules of the American Arbitration Association shall apply. The arbitrator shall have experience and expertise in the health care field and shall be selected according to the rules of his or her certifying association. Arbitration conducted pursuant to this section shall be binding on all parties. The arbitrator shall conduct a hearing and issue a final ruling within ninety (90) days of being selected, unless the CCN and the provider mutually agree to extend this deadline. All costs of arbitration, not including attorney’s fees, shall be shared equally by the parties."
The Claims Dispute process specified in 17.5.2 is concerning services that have been provided and a claim has been filled. The CCN provider must exhaust the internal claims dispute procedures approved by DHH prior to seeking arbitration pursuant to revised Section 17.5.2.2.
Coventry Health Care of Louisiana,
Inc.Provider Complaint
SystemSection 10.6.3.1 shall be revised to replace the work "pre-processed" with "processed". The RFP is being amended to removed the word "pre-processed"

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 83 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
24 RFP 117
352 RFP 10.6.3.3 117
25 RFP 11.1.1 Enrollment Counseling 118
26 RFP 11.1.1 Enrollment Counseling 118 When is the annual open enrollment period?
509 WellPoint RFP 118, 143 Yes
Coventry Health Care of Louisiana,
Inc.10.6.3.2 and
10.6.3.3Provider Complaint
System
Confirm that this direction to the provider to file all appeals for the denial, reduction or suspension of medically necessary services through the state fair hearing process would be done as the provider acting on the member's behalf, after the member has exhausted the CCN's internal appeals process, and with the member's consent.
Correct, the provider acting only on the written consent of the member, may file an appeal and must exhaust the CCN's appeal process before requesting a state fair hearing.
AmeriHealth Mercy of Louisiana
Provider Complaint System
The provision allows a provider to request an administrative hearing with the Division of Administrative Law. Would this request be made as part of the state fair hearing process? Please clarify.
The state fair hearing process is operated by the Division of Administrative Law.
Coventry Health Care of Louisiana,
Inc.
Please confirm the date when enrollment counseling/open enrollment will begin and does the CCN support the enrollment broker during this time?
See the Schedule of Events in Section 1.9 of the RFP for the date choice packets will be mailed to potential enrollees for each GSA. The CCN is responsible to provide the materials outlined in the Section 12 of the RFP. All dates in the Schedule of Events are subject to change. The earliest date for enrollment counseling/open enrollment for Area A residents is 11/16/11. The CCN must provide their provider directory and a brochure for inclusion in the member choice packets
Coventry Health Care of Louisiana,
Inc.
There will not be a single open enrollment period . . The annual open enrollment period will be tied to initial enrollment in a CCN and the Medicaid eligibility annual renewal date.
11.1.2.3 and 12.10.6.4
Will DHH/Enrollment Broker provide a member enrollment website that lists/compares the expanded services/benefits provided by each plan?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 84 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
27 RFP 11.1.2.4 Enrollment Counseling 119
28 RFP 11.1.3 Enrollment Counseling 119
771 RFP 11.10.3 Change in Status 123
29 RFP 11.10.3 Change in Status 123
Coventry Health Care of Louisiana,
Inc.How will the CCN be informed of members with special needs, via 834 or other means?
If the Medicaid recipient self declares they have special health care needs the Enrollment Broker will provide an indicator via the 834. DHH will provide up to two years of historical claims data, if available, for each enrollee to the CCN at the time of enrollment which can be used to identify members with special health needs. Additionally, the CCN is responsible during the welcome call within 14 business days of assignment to inquire whether the member has any special health care needs.
Coventry Health Care of Louisiana,
Inc.
What is the enrollment brokers process for CCN and PCP selection? And will the enrollment broker do auto-assignment? If so, what is the timeframe?
The enrollment broker will provide multiple methods for enrollees to select a CCN and indicate their PCP preference, if any. Potential enrollees may call the Enrollment Broker hotline, submit choices via the Internet, or receive personal assistance from the Enrollment Broker or other DHH designated. agent. Refer to § 11.3 relative to auto-assignment. Refer to §11.2.2 and §11.3.1 for timeframes.
Amerigroup Corporation
This section states the CCN shall agree to report in writing to DHH's Medicaid customer Services Unit any changes in contact information or living arrangements for families or individual members within 5 business days of identification. Does the definition of "in writing" include electronic notification, such as e-mailed spreadsheets?
Yes DHH will provide an e-mail address for the Medicaid Customer Service Unit. Also, see response to Comment # 29
Coventry Health Care of Louisiana,
Inc.
Is there a required format in which changes in contact information or living arrangements for families should be sent, and to whom at the DHH should this information be sent to?
As stated in §1.10.3 the information shall be reporting in writing to the Medicaid Customer Service Unit. DHH is developing a web based reporting form for this purpose.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 85 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
772 RFP 11.10.4.1 Newborn Enrollment 123
639 RFP 11.10.4.2 Newborn Enrollment 123
640 RFP Newborn Enrollment 123
761 RFP
30 RFP 11.10.5.2 123
Amerigroup Corporation
This section states the CCN shall contact members who are expectant mothers 60 calendar days prior to the expected date of delivery to encourage the mother to choose a CCN and a PCP for her newborn. Can you clarify if there is a required\preferred form of contact?
DHH is not stipulating a required/preferred form of contact. The contact may be telephonic, electronic mail, or postal mail.
Children's Hospital Health Plan
(1) If the CCN possesses sufficient information to complete the REQUEST FOR NEWBORN process, can the CNN perform this function directly in cases where the hospital has not done so in a timely manner? (2) How long after DHH received this request will it take for the newborn to be assigned an ID#?
The hospital must complete the Request for Newborn ID. An ID # is assigned and returned via fax to the hospital and physician(s) indicated on the form within three (3) working days.
Children's Hospital Health Plan
11.10.4.2 and 11.10.4.3
We are unclear as to when the Request for Newborn Manual system is used vs. the LEERS system.
These are two separate processes. The Request for Newborn ID is completed by the Hospital to obtain a Medicaid ID number for the newborn when a Medicaid enrollee gives birth. LEERS is (Louisiana Electronic Event Registration System) s operated by the Office of Public Health/Vital Records and the LEERS Birth Module automates the process for registering births in the state.
Amerigroup Corporation
11.10.4.2 and 11.10.4.3 Newborn Enrollment 123
These sections refer to “hospital sub-contractors” reporting births using the Request for Newborn Manual system and to “hospital providers” registering births through LEERS. We would appreciate clarification on whether “hospital sub-contractors” and “hospital providers” refer to the same entity and whether or not the Request for Newborn Manual System and LEERs are the same or different systems. If different, can you please provide additional details about how these two systems differ.
"Hospital sub-contractors" refers to CCN in-network hospitals. The reference to hospital providers is to the CCN's in- network hospitals as well. Therefore these terms are used interchangeably. Refer to response to Comment # 640
Coventry Health Care of Louisiana,
Inc.Assignment to Primary
Care ProvidersWhat is the timeframe for the member to select a CCN or PCP with the enrollment broker?
.See § 11.2.2 and §11.3.1 for timeframes for members to select a CCN and indicate PCP preference to the CCN.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 86 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
31 RFP 11.10.5.4 123
762 RFP 11.10.5.4
32 RFP 11.10.5.5 124 Yes
Coventry Health Care of Louisiana,
Inc.Assignment To Primary
Care Providers
Will any other identifiable provider information be sent along with the providers name on the member file from the enrollment broker such as the providers NPI, State ID number etc.?
The member file layout will be specified in the Systems Companion Guide.
Amerigroup Corporation
Assignment of Primary Care Providers 123
This section indicates that we will receive the PCP name on the Member File so that the CCN can use this information to assign the member’s selected PCP upon processing the Member File. Using names for programmatic matching always yields problematic results. We know that using Unique IDs, when available, are a much better choice for programmatic matching and would suggest this approach if possible. Given that the provider NPI is a required data element for the Provider Enrollment file, which the CCNs will be sending to the Enrollment Broker, we would like to request that the NPI be provided by the Enrollment Broker as the PCP identifier on the Member File.
The NPI will be included on the 834 file transfer.
Coventry Health Care of Louisiana,
Inc.Assignment of Primary
Care ProvidersIs the ID card acceptable as notification to the member of their selected PCP?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 87 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
785 RFP 11.10.5.6-9 124 See Addendums to Section 11.10.5.6=9
33 RFP 11.10.5.9 124 Yes- See Addendums to Section 11..10.5.6-9
764 RFP 11.11.11
Amerigroup Corporation
Assignment of Primary Care Providers
Current language indicates that a member who did not inform the Enrollment Broker of their PCP selection will be contacted within 10 business days as part of the welcome process and assisted with selecting a PCP. And, if after ten (10) days a member has not selected a PCP, that member is to be auto assigned a PCP. In order to ensure that Members have an assigned PCP as soon as possible, we propose the following language change which allows for immediate assignment of the PCP and member change of PCP as desired: - 11.10.5.6 <no change> - 11.10.5.7 Auto-assign a PCP to each member who has not selected a PCP no later than ten (10) business days after receiving the Member File from the Enrollment Broker - 11.10.5.7b Contact each member during the welcome process (see welcome call requirements in section 12.11.2.3) and shall review PCP assignment and assist the member in the process of changing their PCP as needed. - 11.10.5.8 <no change> - 11.10.5.9 <remove>
Coventry Health Care of Louisiana,
Inc.Assignment of Primary
Care Providers
If the member has not selected a pap, is it acceptable to auto-assign the member a PCP on the first day of enrollment so that the member will have a PCP available to them when they receive their card with the opportunity to change the selected PCP.
Amerigroup Corporation PCP Auto-Assignments 125
Indicates that the CCN is required to provide notification of PCP terminations by close of business the next business day. Please advise the means by which this information is to be communicated. (There is a provider directory which the CCNs are required to send to the EB; however the frequency of this file does not seem to support the timeliness of this communication requirement, as the requirement is no less than weekly.)
Via electronic communication. The exact process and format of information will be established by the Enrollment Broker.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 88 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
34 RFP 11.11.2 PCP Auto-Assignments 124
763 RFP 11.11.2
35 RFP 11.11.3 PCP Auto-Assignments 124 The Proposer is the prospective CCN
137 WellCare RFP 11.11.3 PCP Auto-Assignment 124
36 RFP 11.11.7 PCP Auto-Assignments 125
353 RFP 11.11.8 PCP Auto-Assignments 125 See response to Comment # 37.
37 RFP 11.11.8 PCP Auto-Assignments 125 Please define 'with cause" as referenced in this section.
Coventry Health Care of Louisiana,
Inc.Please confirm if this section is referring to the State or the CCN?
Section § 11.11 contains requirements for the CCN. The Enrollment Broker will make CCN Auto-Assignments but not PCP Auto-Assignments.
Amerigroup Corporation PCP Auto-Assignments 124
As designated in this section, there is great value to the member if the CCN utilizes immediate family relationships when assigning PCPs to members who have not previously made a PCP selection. In order to connect members to their immediate family members, some type of family link will need to be provided. We would recommend that this family link information be included as part of the member data on the Member File from the Enrollment Broker to ensure the appropriate involvement of the members family.
A Case Number is among the fields that will be included in the Enrollment File. The Case Number can be used to identify additional family members.
Coventry Health Care of Louisiana,
Inc.Please confirm who the "proposer" is as referenced in this section.
Is the Proposer limited to using age, sex, and geographic proximity in the auto-assignment process or can we consider other factors, e.g., language (if it's provided)?
Preferred language can be a factor in the PCP auto-assignment
Coventry Health Care of Louisiana,
Inc.Please define the intent of the member being locked in to the selected PCP.
The CCN has the option to lock in the member to the selected PCP after 90 days and change the PCP during the subsequent nine months only if cause is demonstrated.
AmeriHealth Mercy of Louisiana
What constitutes "with cause" under this section and does the CCN determine if such cause exists?
Coventry Health Care of Louisiana,
Inc.
The CCN's reasons for cause to disenroll from a PCP (if the CCN has a lock in period for PCP) should be similar to DHH's reasons for cause for disenrollment from a CCN.
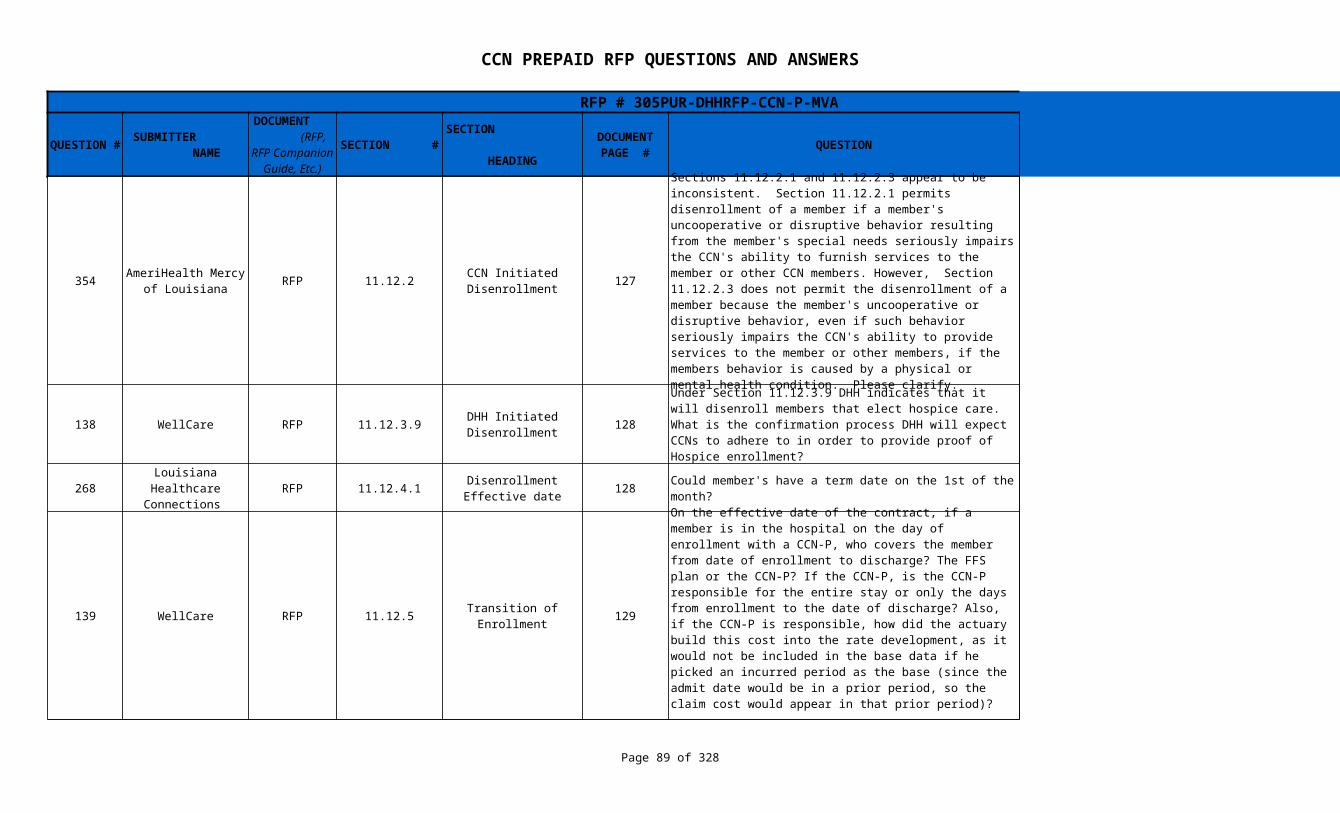
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 89 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
354 RFP 11.12.2 127
138 WellCare RFP 11.12.3.9 128
268 RFP 11.12.4.1 128 Could member's have a term date on the 1st of the month?
139 WellCare RFP 11.12.5 129
AmeriHealth Mercy of Louisiana
CCN Initiated Disenrollment
Sections 11.12.2.1 and 11.12.2.3 appear to be inconsistent. Section 11.12.2.1 permits disenrollment of a member if a member's uncooperative or disruptive behavior resulting from the member's special needs seriously impairs the CCN's ability to furnish services to the member or other CCN members. However, Section 11.12.2.3 does not permit the disenrollment of a member because the member's uncooperative or disruptive behavior, even if such behavior seriously impairs the CCN's ability to provide services to the member or other members, if the members behavior is caused by a physical or mental health condition. Please clarify.
Section 11.12.2.3 is being amended as follows: The member’s behavior is disruptive, unruly, abusive or uncooperative to the extent that enrollment in the CCN seriously impairs the organization’s ability to furnish services to either the member or other members. and the member’s behavior is not caused by a physical or mental health condition.
DHH Initiated Disenrollment
Under Section 11.12.3.9 DHH indicates that it will disenroll members that elect hospice care. What is the confirmation process DHH will expect CCNs to adhere to in order to provide proof of Hospice enrollment?
DHH's hospice unit receives notice of admission of Medicaid enrollees to hospice and authorizes hospice payment. DHH does not expect CCNs to provide proof of hospice enrollment and DHH is the source of such proof.
Louisiana Healthcare Connections
Disenrollment Effective date
Yes Termination is always effective the first day of a month. If CCN eligible on the first day of the month they are eligible for the entire month
Transition of Enrollment
On the effective date of the contract, if a member is in the hospital on the day of enrollment with a CCN-P, who covers the member from date of enrollment to discharge? The FFS plan or the CCN-P? If the CCN-P, is the CCN-P responsible for the entire stay or only the days from enrollment to the date of discharge? Also, if the CCN-P is responsible, how did the actuary build this cost into the rate development, as it would not be included in the base data if he picked an incurred period as the base (since the admit date would be in a prior period, so the claim cost would appear in that prior period)?
Fee-for-service through the date of discharge only for inpatient hospital costs.
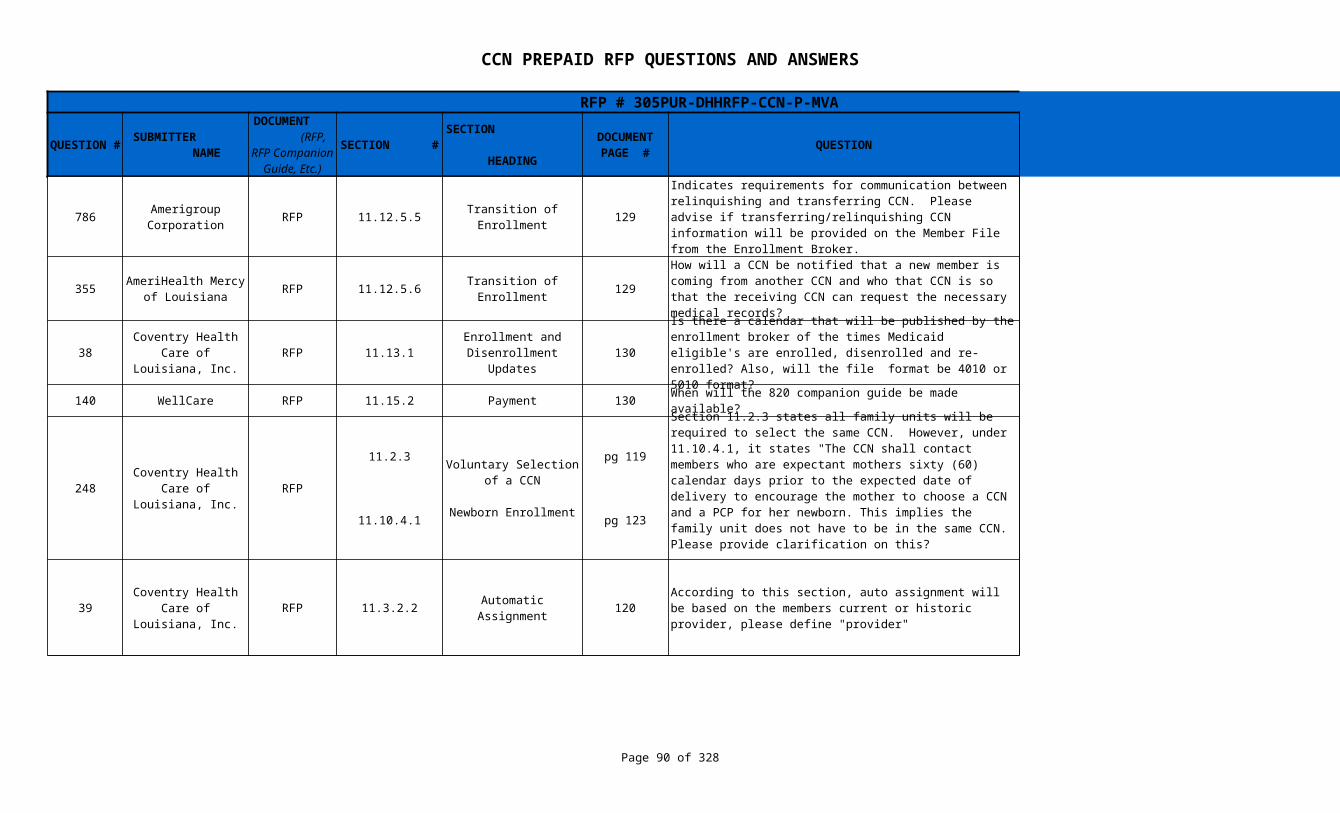
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 90 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
786 RFP 11.12.5.5 129 Yes
355 RFP 11.12.5.6 129 A special field will be added to the 834 file.
38 RFP 11.13.1 130
140 WellCare RFP 11.15.2 Payment 130 When will the 820 companion guide be made available? Proposers shall utilize the Implementation Guide from CMS.
248 RFP
39 RFP 11.3.2.2 Automatic Assignment 120
Amerigroup Corporation
Transition of Enrollment
Indicates requirements for communication between relinquishing and transferring CCN. Please advise if transferring/relinquishing CCN information will be provided on the Member File from the Enrollment Broker.
AmeriHealth Mercy of Louisiana
Transition of Enrollment
How will a CCN be notified that a new member is coming from another CCN and who that CCN is so that the receiving CCN can request the necessary medical records?
Coventry Health Care of Louisiana,
Inc.Enrollment and
Disenrollment Updates
Is there a calendar that will be published by the enrollment broker of the times Medicaid eligible's are enrolled, disenrolled and re-enrolled? Also, will the file format be 4010 or 5010 format?
All Medicaid enrollment and disenrollment--except for newborns--will be effective at 12:01 AM on the first day of a month. The File format will be 5010 beginning January 1, 2012.
Coventry Health Care of Louisiana,
Inc.
11.2.3
11.10.4.1
Voluntary Selection of a CCN
Newborn Enrollment
pg 119
pg 123
Section 11.2.3 states all family units will be required to select the same CCN. However, under 11.10.4.1, it states "The CCN shall contact members who are expectant mothers sixty (60) calendar days prior to the expected date of delivery to encourage the mother to choose a CCN and a PCP for her newborn. This implies the family unit does not have to be in the same CCN. Please provide clarification on this?
That is correct. The RFP is being amended to clarify that all family members are not required to be in the same CCN.
Coventry Health Care of Louisiana,
Inc.
According to this section, auto assignment will be based on the members current or historic provider, please define "provider"
For auto assignment purposes we will be looking at the CommunityCARE 2.0 PCP if applicable. If the enrollee is not transitioning from CommunityCARE we will look at the physician (PCP or specialty), FQHC, RHC, or clinic that billed for the most visits in the prior 12 months.
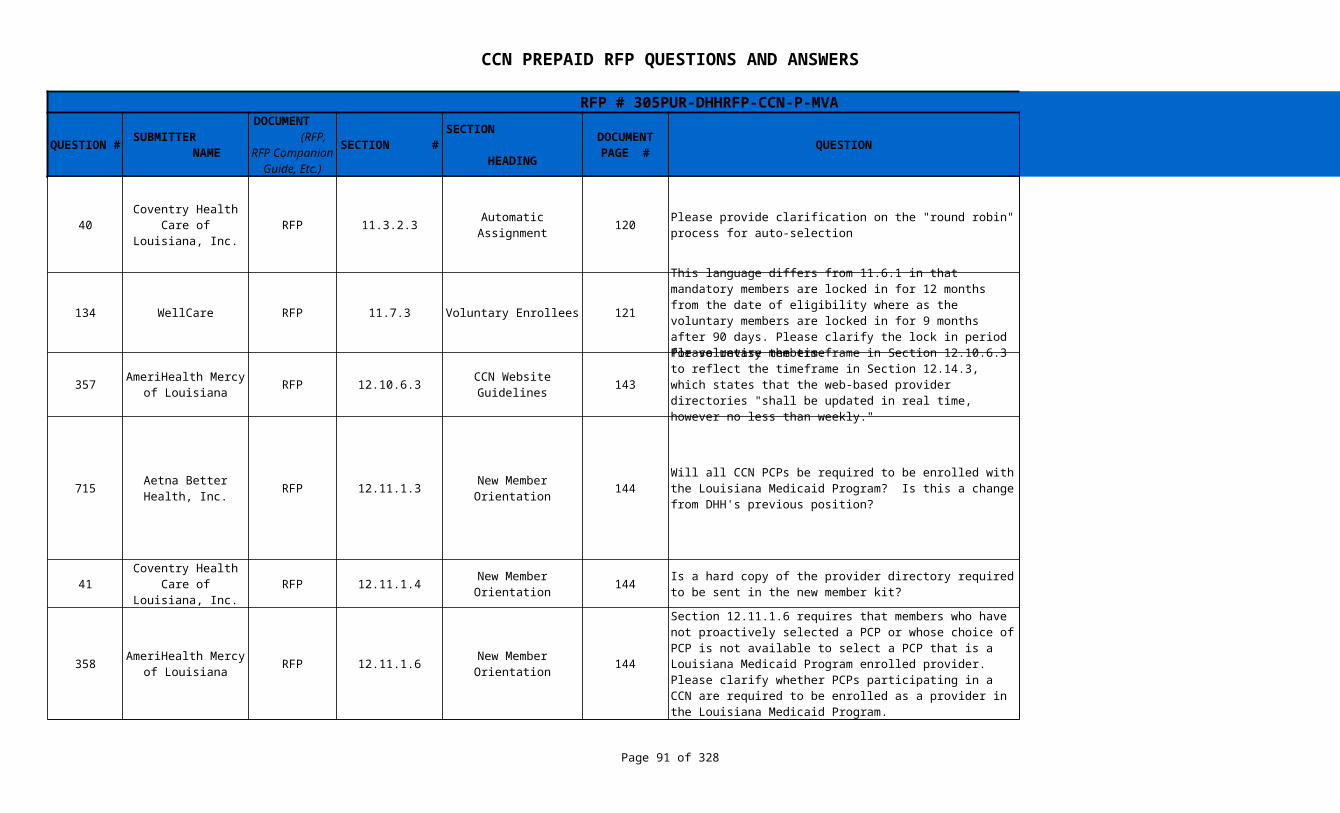
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 91 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
40 RFP 11.3.2.3 Automatic Assignment 120
134 WellCare RFP 11.7.3 Voluntary Enrollees 121
357 RFP 12.10.6.3 143 Change made. See Addendum #4.
715 RFP 12.11.1.3 144
41 RFP 12.11.1.4 144
358 RFP 12.11.1.6 144
Coventry Health Care of Louisiana,
Inc.Please provide clarification on the "round robin" process for auto-selection
"Round robin" is an arrangement of choosing all elements (CCNs) in a group equally in some rational order, usually from the top to the bottom of a list (of CCNs with whom the provider is enrolled as a network provider) and then starting again at the top of the list, and so on.
This language differs from 11.6.1 in that mandatory members are locked in for 12 months from the date of eligibility where as the voluntary members are locked in for 9 months after 90 days. Please clarify the lock in period for voluntary members.
This is two different ways of saying 12 months (12 months from initial date) or 90 days (3 months) plus 9 months which also equals 12 months
AmeriHealth Mercy of Louisiana
CCN Website Guidelines
Please revise the timeframe in Section 12.10.6.3 to reflect the timeframe in Section 12.14.3, which states that the web-based provider directories "shall be updated in real time, however no less than weekly."
Aetna Better Health, Inc.
New Member Orientation
Will all CCN PCPs be required to be enrolled with the Louisiana Medicaid Program? Is this a change from DHH's previous position?
The section relating to CCN providers and their Medicaid provider enrollment is actually found in Section 12.11.1.6. Providers participating in the CCN Prepaid program will not be required to enroll as Medicaid providers. If the provider is participating in the CCN Shared Savings model, then they must be enrolled as a Medicaid Provider. Language in 12.11.1.6 has been modified to reflect this change. See Addendum #4.
Coventry Health Care of Louisiana,
Inc.New Member
OrientationIs a hard copy of the provider directory required to be sent in the new member kit?
Yes. At this time, CMS requires hard copies of provider directors with at a minimum, the names of PCPs, specialty physicians and hospitals.
AmeriHealth Mercy of Louisiana
New Member Orientation
Section 12.11.1.6 requires that members who have not proactively selected a PCP or whose choice of PCP is not available to select a PCP that is a Louisiana Medicaid Program enrolled provider. Please clarify whether PCPs participating in a CCN are required to be enrolled as a provider in the Louisiana Medicaid Program.
Providers participating in the CCN Prepaid program will not be required to enroll as Medicaid providers. If the provider is participating in the CCN Shared Savings model, then they must be enrolled as a Medicaid Provider.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 92 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
773 RFP 12.11.2.1 145
779 RFP 12.11.2.3 146
641 RFP 12.11.2.3 Welcome Calls 146 There is no prescribed format for this report.
42 RFP 12.12.2.22 149
Amerigroup Corporation
Communication with New Enrollees
Please confirm the CCN can send the Member ID card separately and earlier than the welcome pack so that members can be aware of PCP contact information as soon as possible.
The CCN may issue the CCN Member ID card separately from the member kit, but the CCN must demonstrate good reason for the separation of the enrollment packet pieces. In addition, the member ID card, if distributed separately, would still have to meet the timing deadline established for the member kit - 21 days for CCN implementation and 10 days post-implementation. As part of the card mailing, the CCN must explain the purpose of the card, how to use the card, and how to use it in tandem with the DHH-issued card. This language has been modified. See Addendum #4.
Amerigroup Corporation
Communication with New Enrollees
Since the CCN may receive files on a daily basis, the CCN could receive a member on the 2nd of the month that would be eligible the first of the following month (almost 30 days later). We do not believe that it would be appropriate to start welcoming the member to the plan, or be in their best interests when they still have almost a month before they are effective. Please reconfirm DHH’s previous answer to this question received on 9/10/2010 that the 14 day welcome call requirement to be from the date of "eligibility" as opposed to "receipt of file date".
Children's Hospital Health Plan
The last bullet in this section indicates a monthly report of members that could not be contacted. Is there a format for this report?
Coventry Health Care of Louisiana,
Inc.CCN Member
HandbookPlease advise if a Fax number is required to be published for member services. A fax number is not normally provided to members unless for expedited or urgent issues.
Yes. A Fax number is required to be published for member services.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 93 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
752 Advocacy Center RFP 12.12.2.26 149
753 Advocacy Center RFP 12.12.2.26 149
43 RFP 12.13.1 150
699 RFP 12.13.1.2 150/151
CCN Member plan booklet
The RFP provides that the Member plan booklet should explain the duty to report any private health insurance coverage the member has. Must the booklet also explain the CCN's obligation to pay any coinsurance, copayments, and deductibles the member would otherwise be responsible for under their private insurance policy, and the fact that these individuals can seek care through the network of their private insurer and are not limited to providers enrolled with the CCN-P? (See §5.2.12.4)
DHH will provide a standard template for the member booklet for use by all CCNs. DHH will consider the incorporation of this language as well.
CCN Member plan booklet
The RFP provides that the Member plan booklet should explain the duty to report any private health insurance coverage the member has. Should the booklet also explain the coordination of benefits and treatment of costs that are not covered by the private insurance, other than coinsurance, copayments, and deductibles (such as charges exceeding the private plan's limits)?
DHH will provide a standard template for the member booklet for use by all CCNs. DHH will consider the incorporation of this language as well.
Coventry Health Care of Louisiana,
Inc.Member Identification
(ID) CardsPlease advise if It is required to have the PCP's address printed on the ID card or if the PCP's name and phone number is acceptable.
No. The address is not required. This language has been modified. See Addendum #4.
Aetna Better Health, Inc.
Due to limited space on the ID card, traditionally other state Medicaid agencies have not required including the PCP's address as standard practice. Would the state consider removing this requirement?
This requirement has been modified. The address is not required. This language has been modified. See Addendum #4.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 94 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
44 RFP 12.13.2 151
642 RFP 12.13.2 151
728 RFP 151/152 This is a CMS requirement.
208 HMO Louisiana, Inc. RFP 12.14.1.4 152
Coventry Health Care of Louisiana,
Inc.Member Identification
(ID) CardsIs it acceptable to send the member ID card separate from the member kit?
The CCN may issue the CCN Member ID card separately from the member kit, but the CCN must demonstrate good reason for the separation of the enrollment packet pieces. In addition, the member ID card, if distributed separately, would still have to meet the timing deadline established for the member kit - 21 days for CCN implementation and 10 days post-implementation. As part of the card mailing, the CCN must explain the purpose of the card, how to use the card, and how to use it in tandem with the DHH-issued card. See Addendum #4.
Children's Hospital Health Plan
Member Identification Cards
This paragraph requires that the ID Card and the Welcome Packet be issued together. Most plans will use fulfillment vendors for these functions. The issuance of the ID Card is usually handled by a separate vendor than the Welcome Packet. In addition, the ID Card should be sent first class whereas the Welcome Packet is more cost-effectively issued in pre-sort mail. Can this requirement be changed to permit consecutive issuance versus concurrent issuance?
The CCN may issue the CCN Member ID card separately from the member kit, but the CCN must demonstrate good reason for the separation of the enrollment packet pieces. In addition, the member ID card, if distributed separately, would still have to meet the timing deadline established for the member kit - 21 days for CCN implementation and 10 days post-implementation. As part of the card mailing, the CCN must explain the purpose of the card, how to use the card, and how to use it in tandem with the DHH-issued card. This language has been modified. See Addendum #4.
Aetna Better Health, Inc.
12.14.1 and 12.14.3
Provider Directory for Members
We recommend DHH consider not requiring the CCN to produce and distribute hard copy provider directories. Instead we recommend the DHH consider allowing the CCN to provide to members, potential members and the enrollment broker electronic versions of the provider directory.
Provider Directory for Members
In regards to abbreviated hard copy provider directory for enrollment brokers, how is DHH defining abbreviated (for example would mileage radius be a component for abbreviation). Also, what are the required fields/data elements?
Abbreviated provider types must include at a minimum PCPs, specialists and hospitals.
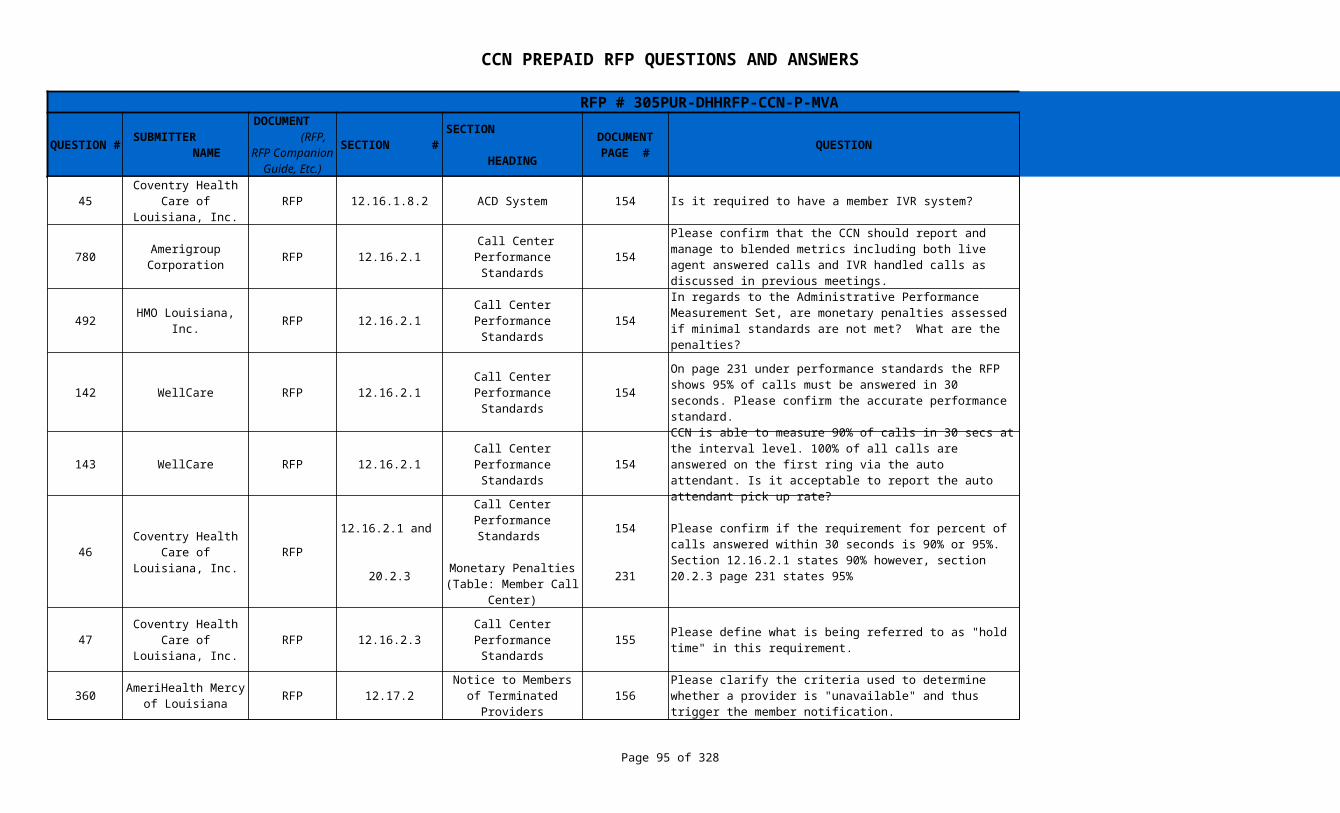
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 95 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
45 RFP 12.16.1.8.2 ACD System 154 Is it required to have a member IVR system? Refer to § 12.15.3
780 RFP 12.16.2.1 154
492 HMO Louisiana, Inc. RFP 12.16.2.1 154
142 WellCare RFP 12.16.2.1 154
143 WellCare RFP 12.16.2.1 154
46 RFP
47 RFP 12.16.2.3 155
360 RFP 12.17.2 156
Coventry Health Care of Louisiana,
Inc.
Amerigroup Corporation
Call Center Performance Standards
Please confirm that the CCN should report and manage to blended metrics including both live agent answered calls and IVR handled calls as discussed in previous meetings.
Bothy types of calls should be reported and segregated, not blended.
Call Center Performance Standards
In regards to the Administrative Performance Measurement Set, are monetary penalties assessed if minimal standards are not met? What are the penalties?
Yes. There are monetary penalties tied to the call center performance standards. A table of monetary penalties can be found in Section 20.2.3. The member call center specifics can be found on page #231.
Call Center Performance Standards
On page 231 under performance standards the RFP shows 95% of calls must be answered in 30 seconds. Please confirm the accurate performance standard.
The accurate performance standard is 90%. The reference on page #231 has been modified to reflect the standard. . The language in 12.16.2.1 has been modified as well to clarify the use of the automatic system. See Addendum #4.
Call Center Performance Standards
CCN is able to measure 90% of calls in 30 secs at the interval level. 100% of all calls are answered on the first ring via the auto attendant. Is it acceptable to report the auto attendant pick up rate?
No. The auto attendant pick up rate does not give an accurate picture of the call centers accessibility and is not an acceptable reporting measure for the pick up rate.
Coventry Health Care of Louisiana,
Inc.
12.16.2.1 and
20.2.3
Call Center Performance Standards
Monetary Penalties (Table: Member Call
Center)
154
231
Please confirm if the requirement for percent of calls answered within 30 seconds is 90% or 95%. Section 12.16.2.1 states 90% however, section 20.2.3 page 231 states 95%
Section 12.16.2.1 is being amended to read -"Answer ninety-five (95) percent of calls within thirty (30) seconds or an automatic call pickup system:" Section 20.2.3 will remain the same.
Coventry Health Care of Louisiana,
Inc.Call Center
Performance StandardsPlease define what is being referred to as "hold time" in this requirement.
Hold time is defined as the time from when the CCN's customer service representative (CSR) puts the ACD call on Hold to the time the CSR becomes active on the call again or the caller abandons the call.
AmeriHealth Mercy of Louisiana
Notice to Members of Terminated Providers
Please clarify the criteria used to determine whether a provider is "unavailable" and thus trigger the member notification.
Refer to 12.17.3 for guidance on what constitutes a provider becoming "unavailable".
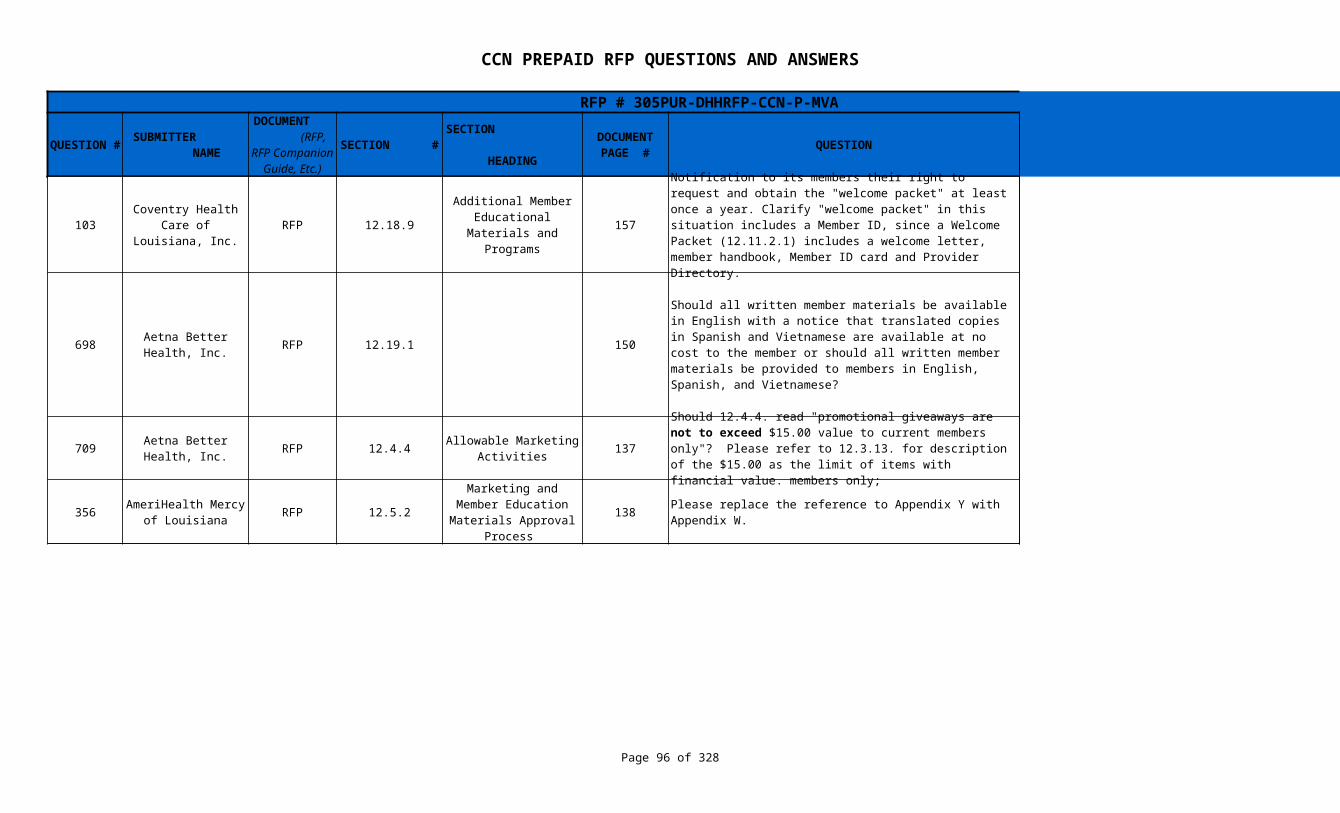
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 96 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
103 RFP 12.18.9 157
698 RFP 12.19.1 150
709 RFP 12.4.4 137
356 RFP 12.5.2 138 Change made. See Addendum #4.
Coventry Health Care of Louisiana,
Inc.
Additional Member Educational Materials
and Programs
Notification to its members their right to request and obtain the "welcome packet" at least once a year. Clarify "welcome packet" in this situation includes a Member ID, since a Welcome Packet (12.11.2.1) includes a welcome letter, member handbook, Member ID card and Provider Directory.
Section 12.18.9 does refer to the welcome packet noted in 12.11.2.1. The CCN shall provide, upon request, all items listed in 12.11.2.1 except for the member ID card. The language in section 12.18.9 will be modified to clarify this request. See addendum #4.
Aetna Better Health, Inc.
Should all written member materials be available in English with a notice that translated copies in Spanish and Vietnamese are available at no cost to the member or should all written member materials be provided to members in English, Spanish, and Vietnamese?
Written member materials should be available in English with a notice, written in that language, that translated copies in Spanish and Vietnamese are available. However, translation is not limited to Spanish and Vietnamese. These are the primary language that has been needed during Medicaid outreach. The CCN must also provide interpretation for other languages upon request in keeping with 12.19.2.
Aetna Better Health, Inc.
Allowable Marketing Activities
Should 12.4.4. read "promotional giveaways are not to exceed $15.00 value to current members only"? Please refer to 12.3.13. for description of the $15.00 as the limit of items with financial value. members only;
This is accurate. The CCN is limited to items under the $15 value mark for non-members. The CCN has more flexibility when it comes to promotions or giveaways with current members. That can exceed the $15 mark.
AmeriHealth Mercy of Louisiana
Marketing and Member Education Materials Approval
Process
Please replace the reference to Appendix Y with Appendix W.
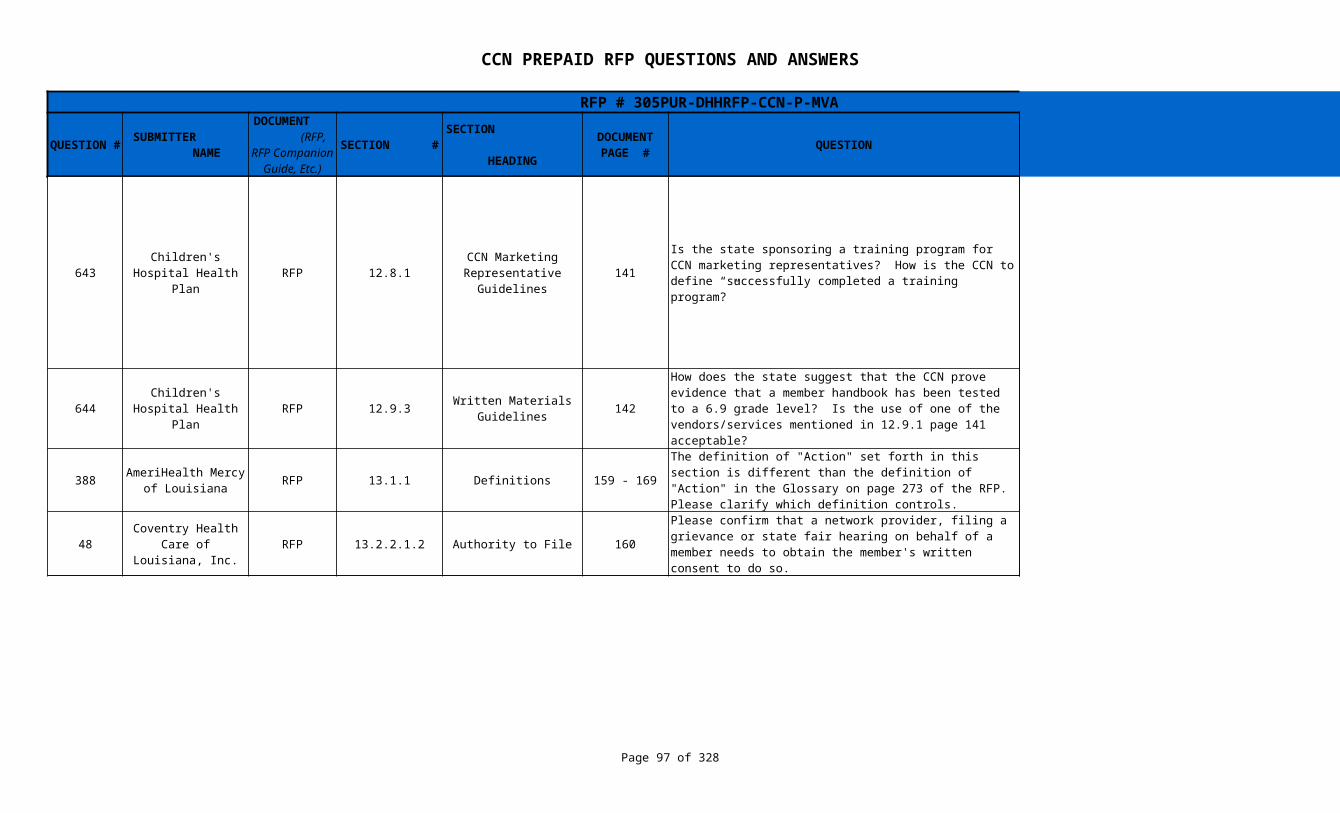
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 97 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
643 RFP 12.8.1 141
644 RFP 12.9.3 142
388 RFP 13.1.1 Definitions 159 - 169
48 RFP 13.2.2.1.2 Authority to File 160
Children's Hospital Health Plan
CCN Marketing Representative
Guidelines
Is the state sponsoring a training program for CCN marketing representatives? How is the CCN to define “successfully completed a training program?”
No. The state will not sponsor training for the CCN marketing representatives. The CCN is responsible for creating a training curriculum (Section 12.2.3.8) as part of the requirements of the CCN Marketing and Member Education Plan (Section 12.2). Once the training is approved by DHH, the CCN must ensure all marketing representatives complete the training. The state will provide basic Medicaid eligibility information for use in the training, but the CCN must create the curriculum and incorporate CCN basics including marketing education for its representatives (including prohibited and allowable activities).
Children's Hospital Health Plan
Written Materials Guidelines
How does the state suggest that the CCN prove evidence that a member handbook has been tested to a 6.9 grade level? Is the use of one of the vendors/services mentioned in 12.9.1 page 141 acceptable?
The CCN must only provide the evidence if requested by DHH. The CCN should use one of the methods listed in 12.9.1 to determine the grade level.
AmeriHealth Mercy of Louisiana
The definition of "Action" set forth in this section is different than the definition of "Action" in the Glossary on page 273 of the RFP. Please clarify which definition controls.
The definition of Action in section 13.1.1 is correct. The definition in the Glossary will be amended.
Coventry Health Care of Louisiana,
Inc.
Please confirm that a network provider, filing a grievance or state fair hearing on behalf of a member needs to obtain the member's written consent to do so.
Correct. The provider, filing a grievance or state fair hearing on behalf of a member must obtain the member's written consent.
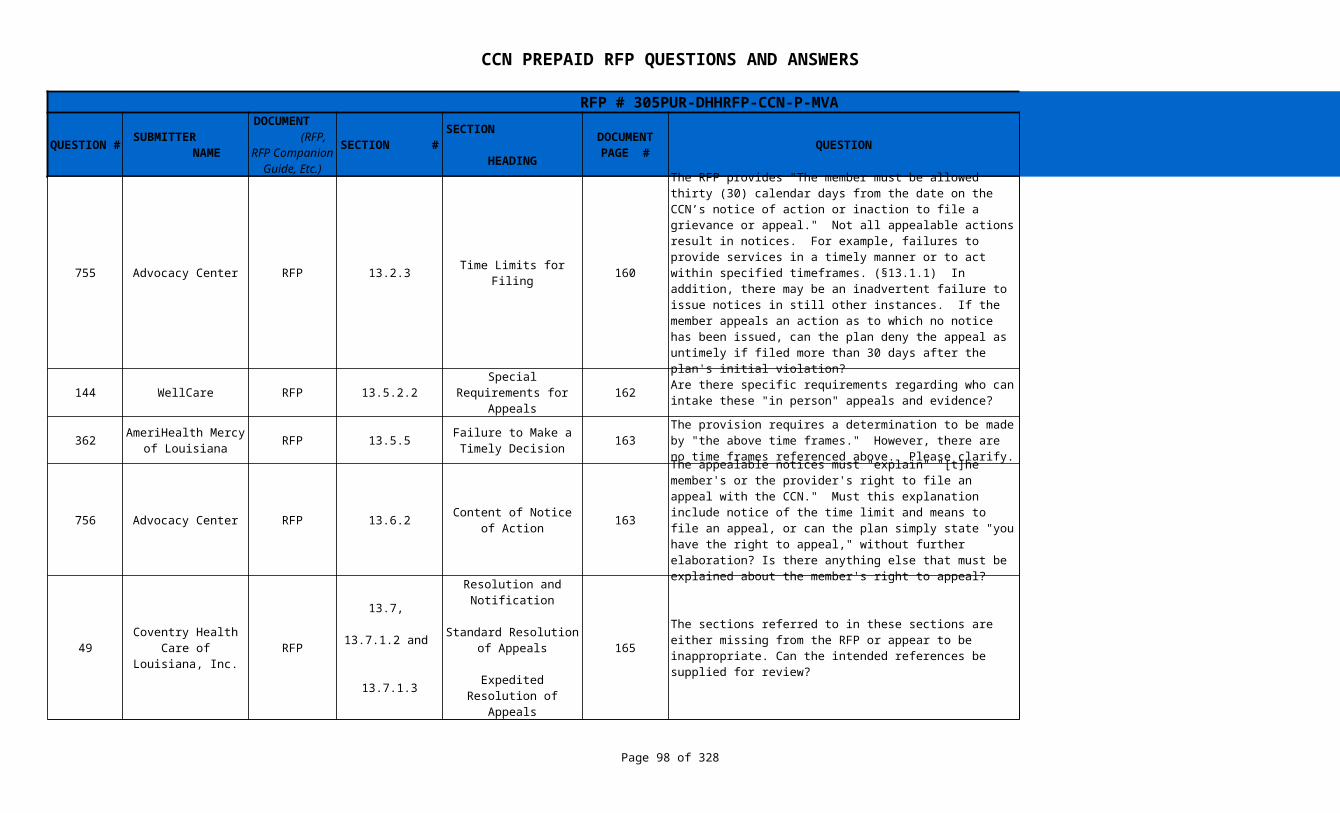
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 98 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
755 Advocacy Center RFP 13.2.3 Time Limits for Filing 160
144 WellCare RFP 13.5.2.2 162 No
362 RFP 13.5.5 163
756 Advocacy Center RFP 13.6.2 163
49 RFP 165
The RFP provides "The member must be allowed thirty (30) calendar days from the date on the CCN’s notice of action or inaction to file a grievance or appeal." Not all appealable actions result in notices. For example, failures to provide services in a timely manner or to act within specified timeframes. (§13.1.1) In addition, there may be an inadvertent failure to issue notices in still other instances. If the member appeals an action as to which no notice has been issued, can the plan deny the appeal as untimely if filed more than 30 days after the plan's initial violation?
This is referring to the 30 days from the "inaction" (examples which you have cited) and not from the "notice of inaction." We would not expect a notice to accompany the inaction/failure to act.
Special Requirements for Appeals
Are there specific requirements regarding who can intake these "in person" appeals and evidence?
AmeriHealth Mercy of Louisiana
Failure to Make a Timely Decision
The provision requires a determination to be made by "the above time frames." However, there are no time frames referenced above. Please clarify.
Refer to addendum 3. The language will be amended to “if a determination is not made in accordance with the timeframes specified in section 13.7 of this RFP…”
Content of Notice of Action
The appealable notices must "explain" "[t]he member's or the provider's right to file an appeal with the CCN." Must this explanation include notice of the time limit and means to file an appeal, or can the plan simply state "you have the right to appeal," without further elaboration? Is there anything else that must be explained about the member's right to appeal?
The explanation must include (but is not limited to) timeframes for filing the appeal, who can file, to whom the appeal request should be directed, that they can be represented by a person of their choosing and the number to call for assistance in filing an appeal.
Coventry Health Care of Louisiana,
Inc.
13.7,
13.7.1.2 and
13.7.1.3
Resolution and Notification
Standard Resolution of Appeals
Expedited Resolution of Appeals
The sections referred to in these sections are either missing from the RFP or appear to be inappropriate. Can the intended references be supplied for review?
The references will be revised as follows:
Section 13.7 shall reference "13.7.1"; and
Section 13.7.1.2 shall reference "13.7.2"
Section 13.7.1.3 shall reference "13.7.2".
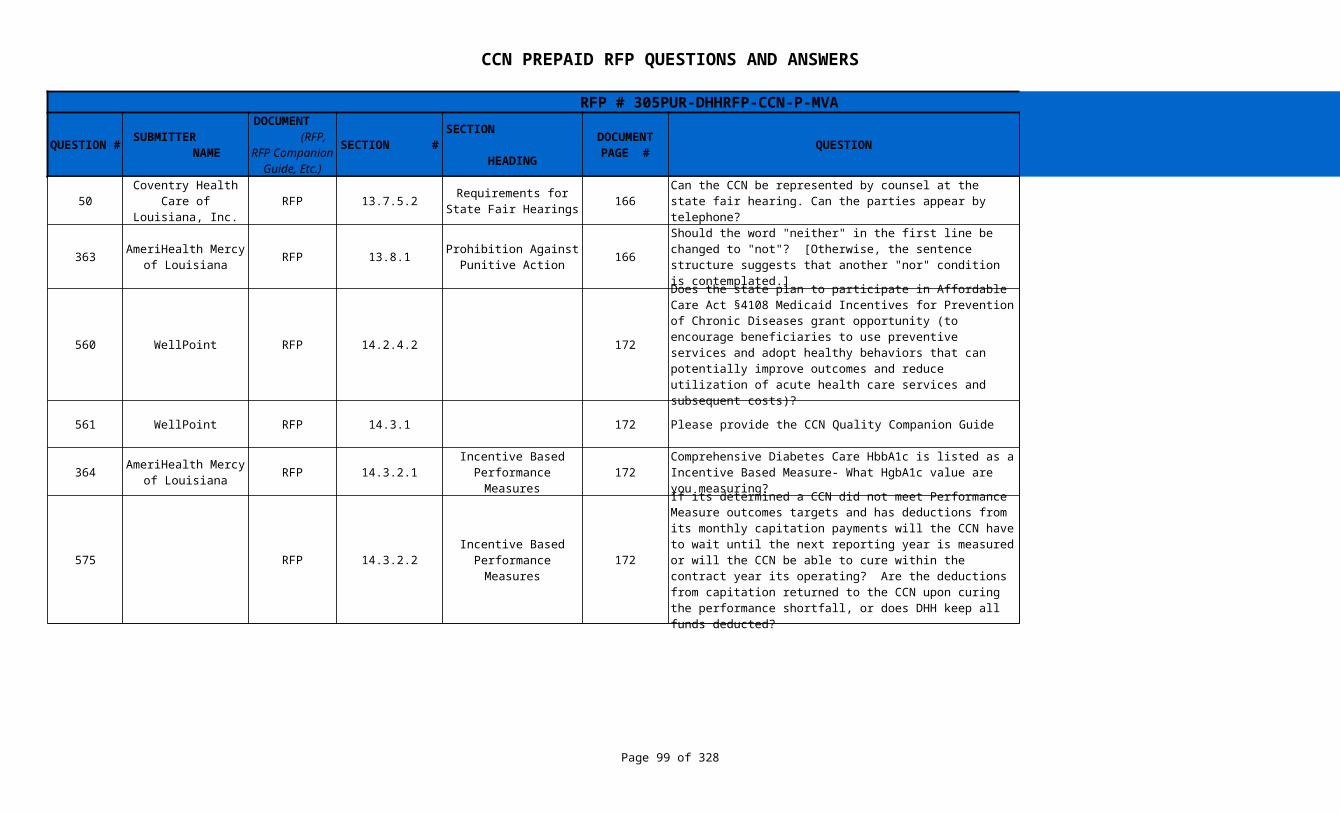
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 99 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
50 RFP 13.7.5.2 166
363 RFP 13.8.1 166 Yes
560 WellPoint RFP 14.2.4.2 172 There is no plan to do so at this time.
561 WellPoint RFP 14.3.1 172 Please provide the CCN Quality Companion Guide
364 RFP 14.3.2.1 172 Refer to the most current HEDIS specifications.
575 RFP 14.3.2.2 172
Coventry Health Care of Louisiana,
Inc.Requirements for State
Fair HearingsCan the CCN be represented by counsel at the state fair hearing. Can the parties appear by telephone?
Yes the CCN can be represented by counsel. The parties may appear by telephone.
AmeriHealth Mercy of Louisiana
Prohibition Against Punitive Action
Should the word "neither" in the first line be changed to "not"? [Otherwise, the sentence structure suggests that another "nor" condition is contemplated.]
Does the state plan to participate in Affordable Care Act §4108 Medicaid Incentives for Prevention of Chronic Diseases grant opportunity (to encourage beneficiaries to use preventive services and adopt healthy behaviors that can potentially improve outcomes and reduce utilization of acute health care services and subsequent costs)?
The EQRO will develop the Quality Companion Guide. The Quality Companion Guide should be available on 1/1/12.
AmeriHealth Mercy of Louisiana
Incentive Based Performance Measures
Comprehensive Diabetes Care HbbA1c is listed as a Incentive Based Measure- What HgbA1c value are you measuring?
Incentive Based Performance Measures
If its determined a CCN did not meet Performance Measure outcomes targets and has deductions from its monthly capitation payments will the CCN have to wait until the next reporting year is measured or will the CCN be able to cure within the contract year its operating? Are the deductions from capitation returned to the CCN upon curing the performance shortfall, or does DHH keep all funds deducted?
The reduction in the capitation payment will be for 12 months as HEDIS measures are calculated on calendar years following 6 months of claims runout. DHH will keep all funds deducted and these will not be returned to the CCN upon curing the performance shortfall.
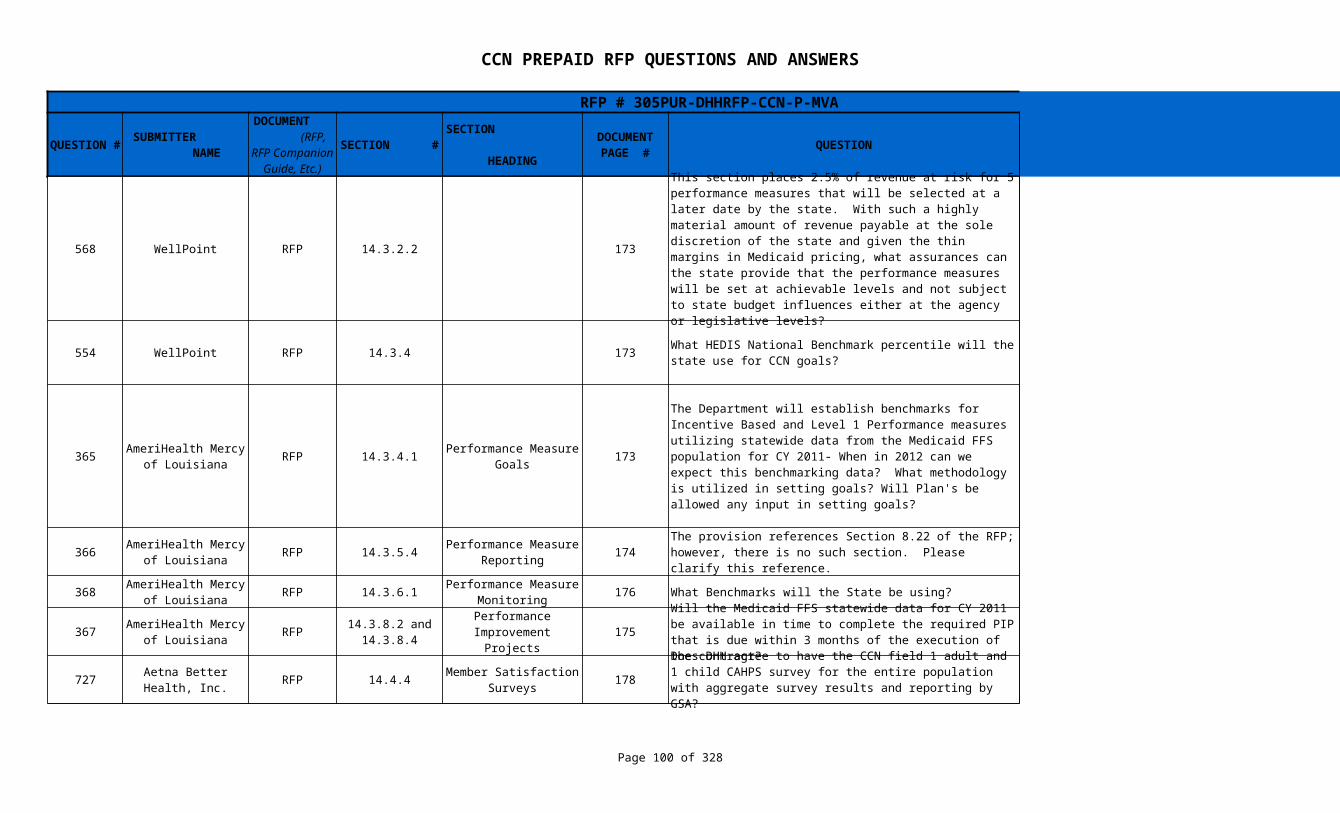
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 100 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
568 WellPoint RFP 14.3.2.2 173 See Question # 365
554 WellPoint RFP 14.3.4 173
365 RFP 14.3.4.1 173
366 RFP 14.3.5.4 174 The correct Reference is 8.7.
368 RFP 14.3.6.1 176 What Benchmarks will the State be using? See Question # 365
367 RFP 175
727 RFP 14.4.4 178 CAHPS survey results shall be reported for each CCN GSA.
This section places 2.5% of revenue at risk for 5 performance measures that will be selected at a later date by the state. With such a highly material amount of revenue payable at the sole discretion of the state and given the thin margins in Medicaid pricing, what assurances can the state provide that the performance measures will be set at achievable levels and not subject to state budget influences either at the agency or legislative levels?
What HEDIS National Benchmark percentile will the state use for CCN goals?
DHH is not establishing HEDIS National Benchmark percentile goals. The goal will be relative improvement from the baseline in FFS in HEDIS measurement year 2011
AmeriHealth Mercy of Louisiana
Performance Measure Goals
The Department will establish benchmarks for Incentive Based and Level 1 Performance measures utilizing statewide data from the Medicaid FFS population for CY 2011- When in 2012 can we expect this benchmarking data? What methodology is utilized in setting goals? Will Plan's be allowed any input in setting goals?
DHH is reviewing this issue. It is our intent to provide the benchmarking methodology by the go live date. Also, language revised to state that " The Department will establish benchmarks for Incentive Based and Level I Performance measures utilizing statewide data of the Medicaid Fee for Service Population CommunityCARE population for CY 2011 with the expectation that performance improves by a certain percentage.
AmeriHealth Mercy of Louisiana
Performance Measure Reporting
The provision references Section 8.22 of the RFP; however, there is no such section. Please clarify this reference.
AmeriHealth Mercy of Louisiana
Performance Measure Monitoring
AmeriHealth Mercy of Louisiana
14.3.8.2 and 14.3.8.4
Performance Improvement Projects
Will the Medicaid FFS statewide data for CY 2011 be available in time to complete the required PIP that is due within 3 months of the execution of the contract?
2009 and 2010 Medicaid FFS statewide data will be available. Medicaid FFS statewide data for 2011 will be available in July 2012.
Aetna Better Health, Inc.
Member Satisfaction Surveys
Does DHH agree to have the CCN field 1 adult and 1 child CAHPS survey for the entire population with aggregate survey results and reporting by GSA?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 101 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
99 RFP 14.4.4 178 CAHPS survey results shall be reported for each CCN GSA.
100 RFP 14.4.8 178
562 WellPoint RFP 14.4.8 178
369 RFP 14.4.8. 178
645 RFP 14.8.1 179
370 RFP 14.9.1 180
Coventry Health Care of Louisiana,
Inc.Member Satisfaction
SurveysWill the state reconsider reporting CAHPS surveys by GSA for plans awarded contracts for all 3 GSAs and allow 3 CAHPS instead of 9 CAHPS surveys?
Coventry Health Care of Louisiana,
Inc.Member Satisfaction
Surveys
Member satisfaction reports are due 120 days after the end of the plan year. This requirement conflicts with NCQA requirements. CAHPS surveys are due with HEDIS in June of each year.
Language will be amended to state that CAHPS surveys are due with Level I and Level II reporting measures
Member Satisfaction Surveys
For Member Satisfaction Surveys, please confirm that “plan year” is a calendar year. Also need the size of each region. The CAHPS survey closes mid-May and NCQA allows regional reporting only if the different regions are large enough. A contract requirement to submit a CAHPS report to DHH by region by May 1st could be problematic. In addition, what guidance from the state can we use to ensure our methodology for determining a statistically valid sample aligns with the state’s expectations?
Language will be amended to state that CAHPS surveys are due with Level I and Level II reporting measures. The most current HEDIS specifications shall be followed.
AmeriHealth Mercy of Louisiana
Member Satisfaction Surveys
Will the State align the due dates for reporting member satisfaction survey results with the timeframes established by NCQA for CAHPS, which would be beyond the 120 days after the end of the year?
Language will be amended to state that CAHPS surveys are due with Level I and Level II reporting measures
Children's Hospital Health Plan
Health Plan Accreditation
(1) How long after implementation will the CCN be given to obtain NCQA or URAC accreditation? (2) If the CCN uses a Third Party Administrator, can this requirement be met by the TPA being NCQA or URAC accredited?
The expectation is that CCNs will apply for accreditation at the earliest possible date. According to the URAC websites the minimum wait time from receipt of application to accreditation can be six months or more
AmeriHealth Mercy of Louisiana
Credentialing and Recredentialing of
Providers and Clinical Staff
Would DHH be willing to allow providers to use either the Louisiana Standardized Credentialing Application form or The Council for Affordable Quality Healthcare, Inc. (CAQH) application form?
The Louisiana Standardized Credentialing Application form shall be used.
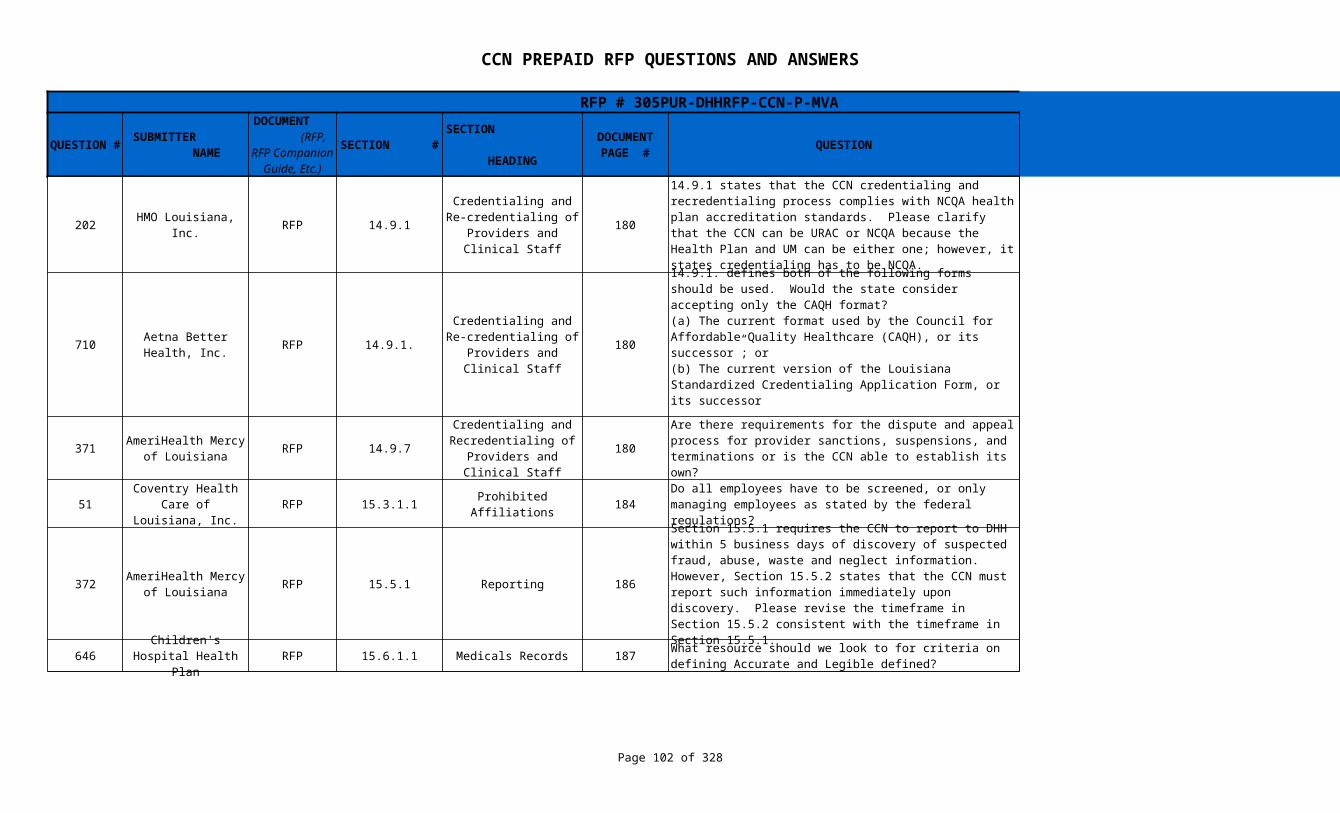
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 102 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
202 HMO Louisiana, Inc. RFP 14.9.1 180
710 RFP 14.9.1. 180
371 RFP 14.9.7 180 CCN shall establish their own procedures.
51 RFP 15.3.1.1 Prohibited Affiliations 184
372 RFP 15.5.1 Reporting 186
646 RFP 15.6.1.1 Medicals Records 187 A business dictionary.
Credentialing and Re-credentialing of
Providers and Clinical Staff
14.9.1 states that the CCN credentialing and recredentialing process complies with NCQA health plan accreditation standards. Please clarify that the CCN can be URAC or NCQA because the Health Plan and UM can be either one; however, it states credentialing has to be NCQA.
The credentialing and recredentialing standards may be either NCQA or URAC.
Aetna Better Health, Inc.
Credentialing and Re-credentialing of
Providers and Clinical Staff
14.9.1. defines both of the following forms should be used. Would the state consider accepting only the CAQH format?(a) The current format used by the Council for Affordable Quality Healthcare (CAQH), or its successor”; or(b) The current version of the Louisiana Standardized Credentialing Application Form, or its successor
The Louisiana Standardized Credentialing Application form shall be used.
AmeriHealth Mercy of Louisiana
Credentialing and Recredentialing of
Providers and Clinical Staff
Are there requirements for the dispute and appeal process for provider sanctions, suspensions, and terminations or is the CCN able to establish its own?
Coventry Health Care of Louisiana,
Inc.Do all employees have to be screened, or only managing employees as stated by the federal regulations?
Only those required as required to comply with federal regulations.
AmeriHealth Mercy of Louisiana
Section 15.5.1 requires the CCN to report to DHH within 5 business days of discovery of suspected fraud, abuse, waste and neglect information. However, Section 15.5.2 states that the CCN must report such information immediately upon discovery. Please revise the timeframe in Section 15.5.2 consistent with the timeframe in Section 15.5.1.
15.5.1 is referring to the Federal requirement for any employee of the CCN who discovers fraud, abuse, waste and neglect information.
15.5.2 is concerning the quarterly reporting provided by the CCNs compliance officer.
Children's Hospital Health Plan
What resource should we look to for criteria on defining Accurate and Legible defined?
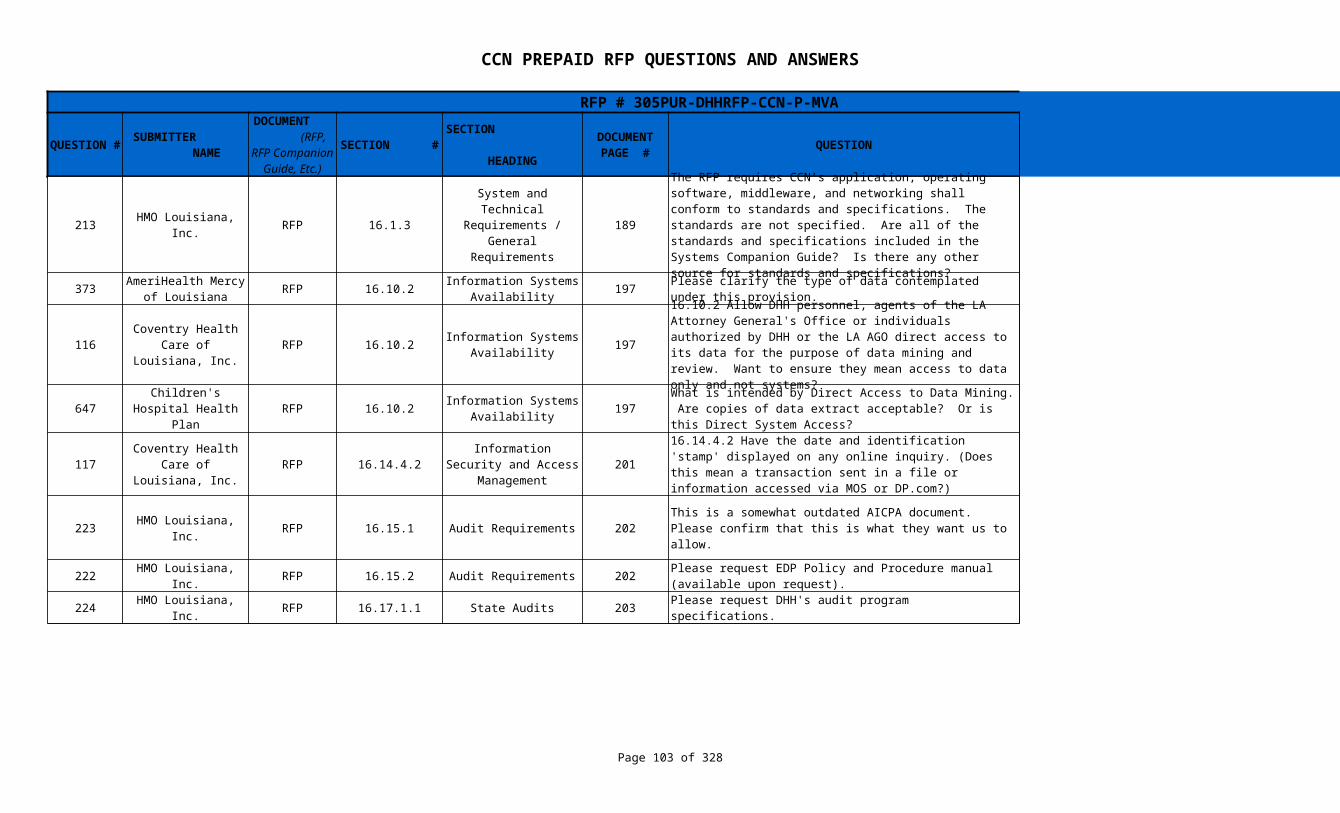
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 103 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
213 HMO Louisiana, Inc. RFP 16.1.3 189
373 RFP 16.10.2 197 When DHH personnel, agents of the Louisiana Attorney General’s Office or individuals authorized by DHH or the Louisiana Attorney General’s Office perform reviews, there are no limitations on what they can review.
116 RFP 16.10.2 197
647 RFP 16.10.2 197 See response to questions # 116 and # 373.
117 RFP 16.14.4.2 201
223 HMO Louisiana, Inc. RFP 16.15.1 Audit Requirements 202
222 HMO Louisiana, Inc. RFP 16.15.2 Audit Requirements 202
224 HMO Louisiana, Inc. RFP 16.17.1.1 State Audits 203 Please request DHH's audit program specifications.
System and Technical Requirements /
General Requirements
The RFP requires CCN’s application, operating software, middleware, and networking shall conform to standards and specifications. The standards are not specified. Are all of the standards and specifications included in the Systems Companion Guide? Is there any other source for standards and specifications?
See § 16.3.11
AmeriHealth Mercy of Louisiana
Information Systems Availability
Please clarify the type of data contemplated under this provision.
Coventry Health Care of Louisiana,
Inc.Information Systems
Availability
16.10.2 Allow DHH personnel, agents of the LA Attorney General's Office or individuals authorized by DHH or the LA AGO direct access to its data for the purpose of data mining and review. Want to ensure they mean access to data only and not systems?
DHH requires remote access to data and systems. DHH also reserves the right to visit on-site as necessary.
Children's Hospital Health Plan
Information Systems Availability
What is intended by Direct Access to Data Mining. Are copies of data extract acceptable? Or is this Direct System Access?
Coventry Health Care of Louisiana,
Inc.
Information Security and Access
Management
16.14.4.2 Have the date and identification 'stamp' displayed on any online inquiry. (Does this mean a transaction sent in a file or information accessed via MOS or DP.com?)
The contractor's application systems must record appropriate audit log information for online inquiry and update transactions. Provide further clarification of MOS and DP.com.
This is a somewhat outdated AICPA document. Please confirm that this is what they want us to allow.
DHH is aware of the upcoming changes to AICPA anticipated in June 2011. It is our intent that CCNs provide audits based on the industry standards at the time of the audit.
Please request EDP Policy and Procedure manual (available upon request).
This is a manual that the CCN shall create and make available to DHH at DHH's request.
The language has been revised to remove the reference to DHH's audit program specifications.
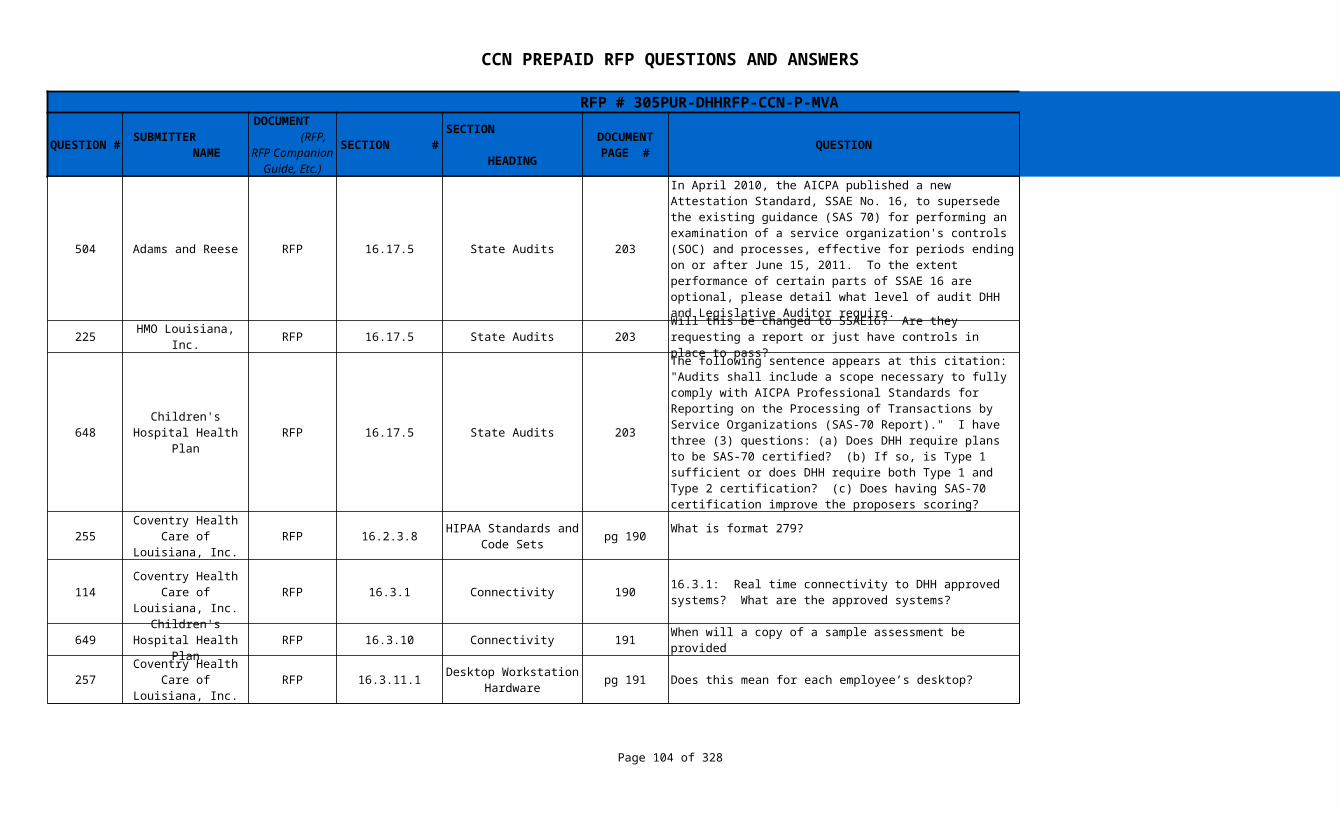
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 104 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
504 Adams and Reese RFP 16.17.5 State Audits 203
225 HMO Louisiana, Inc. RFP 16.17.5 State Audits 203 See Response to Questions # 223 and # 648.
648 RFP 16.17.5 State Audits 203
255 RFP 16.2.3.8 pg 190 Amended to delete 279
114 RFP 16.3.1 Connectivity 190
649 RFP 16.3.10 Connectivity 191 When will a copy of a sample assessment be provided
257 RFP 16.3.11.1 pg 191 Does this mean for each employee’s desktop? Yes
In April 2010, the AICPA published a new Attestation Standard, SSAE No. 16, to supersede the existing guidance (SAS 70) for performing an examination of a service organization's controls (SOC) and processes, effective for periods ending on or after June 15, 2011. To the extent performance of certain parts of SSAE 16 are optional, please detail what level of audit DHH and Legislative Auditor require.
Type II engagement to include:1. Independent service auditor's report (i.e. opinion) 2. Service organization's description of controls. 3. Information provided by the independent service auditor; includes a description of the service auditor's tests of operating effectiveness and the results of those tests 4. Other information provided by the service organization (e.g. glossary of terms).
Will this be changed to SSAE16? Are they requesting a report or just have controls in place to pass?
Children's Hospital Health Plan
The following sentence appears at this citation: "Audits shall include a scope necessary to fully comply with AICPA Professional Standards for Reporting on the Processing of Transactions by Service Organizations (SAS-70 Report)." I have three (3) questions: (a) Does DHH require plans to be SAS-70 certified? (b) If so, is Type 1 sufficient or does DHH require both Type 1 and Type 2 certification? (c) Does having SAS-70 certification improve the proposers scoring?
(a) See response to question 223 above.(b) DHH requires Type II certification.(c) DHH will review and score the CCN's entire response to all requirements as outlined in Appendix KK.
Coventry Health Care of Louisiana,
Inc.HIPAA Standards and
Code SetsWhat is format 279?
Coventry Health Care of Louisiana,
Inc.16.3.1: Real time connectivity to DHH approved systems? What are the approved systems?
The Fiscal Intermediary is noted for the purpose of downloading files, submitting encounters, etc., and the Enrollment Broker for enrollment/disenrollment files and reports.
Children's Hospital Health Plan
DHH will attempt to have the assessment on the Making Medicaid Better website by June 15, 2011.
Coventry Health Care of Louisiana,
Inc.Desktop Workstation
Hardware

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 105 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
256 RFP 16.3.2 Connectivity pg 190 What are the document management standards of DHH?
650 RFP 16.3.4 Connectivity 190
651 RFP 16.3.5 Connectivity 190
652 RFP 16.3.8 Connectivity 191
Coventry Health Care of Louisiana,
Inc.
(1) retain paper documents for a minimum of 3 years, (which may be in imaged form)(2) establish appropriate document indexing, archival and retrieval capabilities, whether paper- or image-based.(3) provide DHH personnel with ability to request and obtain copies of document(s), whether paper- or image-based.
Children's Hospital Health Plan
Please elaborate on intent timing and implementation of the PHR and / or E.H.R.
PHRs are in a later phase of HIE, and will likely not be integrated until 2013.
Children's Hospital Health Plan
Please elaborate on intent timing and implementation of the proposed state wide HIE
By the end of 2011 statewide capabilities will be in place for Phase I of the HIE. Phase I includes the HIE elements required for Meaningful Use Stage I as well as an Emergency Department visit registry that will enable emergency departments to identify if a patient that presents has reason.
Children's Hospital Health Plan
What is the probability of a change in FI and would this change involve Content or Processes
DHH’s current MMIS contract expired December 31, 2010. DHH exercised its right to extend all or part of a five (5) year extension to its current FI. DHH shall require the CCN to comply with transitional requirements as necessary should DHH contract with a new FI during the Contract at no cost to DHH or its FI. This may involve both content and/or processes.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 106 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
258 RFP 16.4.2.3 pg 193 Which user manuals? Who is the audience?
214 HMO Louisiana, Inc. RFP 16.4.2.4 193
259 RFP 16.4.2.5 pg 193 Who is the audience? Is this for members and providers? See response to Question # 258
260 RFP 16.4.2.7 pg 193 Is this in reference to our testing guides?
Coventry Health Care of Louisiana,
Inc.
Information Systems Documentation Requirements
It is DHH's expectation that the contractor will compile -- for individual application systems that are used within the scope of their contract -- appropriate Systems Documentation manuals that effectively outline, identify, describe and document the information technologies, designs, programs, networking, server architecture, production control processes, and other aspects of information systems. The audience is principally any users of the application system, the IT organization working for the contractor, etc., but DHH should be considered an audience, too.
Information Systems Documentation Requirements
The CCN shall ensure that system changes impacting DHH are prior approved in writing. What are the guidelines to determine if DHH approval is required?
See § 16.4.3
Coventry Health Care of Louisiana,
Inc.
Information Systems Documentation Requirements
Coventry Health Care of Louisiana,
Inc.
Information Systems Documentation Requirements
Yes - A Systems Quality Assurance Plan should include at a minimum:(1) Description of the system, application, components that are targeted for change.(2) Detailed test plan.(3) User acceptance test plan and documentation.(4) post-implementation monitoring plan.(5) updated systems documentation.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 107 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
261 RFP 16.4.3.7 System Changes Pg 195 What kind of testing and what kind of access is needed?
263 RFP 16.6.1 pg 195 Is this referencing any letters or correspondence?
115 RFP 16.8.1 196
269 RFP 16.8.2 196
Coventry Health Care of Louisiana,
Inc.
The FI contract is very stringent on the management of systems changes. If a CCN organization plans a System change/modification to an application that interfaces with DHH or the FI, then they should follow, at a minimum, these test guidelines:(1) Prior to modification, submit to DHH a project plan addressing the tasks and time frames necessary for the systems change/modification.(2) Prior to modification, submit to DHH a test plan addressing all components that will be modified.(3) Obtain DHH approval of the test plan.(4) Obtain DHH approval of the time frame(s) outlined in the project plan.(5) Review with DHH in a formal user-acceptance test setting, the test results.
Submission of this process may be via e-mail and/or telepresence.
Coventry Health Care of Louisiana,
Inc.Other Electronic Data
ExchangeYes, letters and other correspondence should be included in the patient master record and provider master record, respectively.
Coventry Health Care of Louisiana,
Inc.
Eligibility and Enrollment Data
Exchange
16.8.1 Receive, process and update enrollment files sent daily by the enrollment broker. Are update files sent daily? Full file, updates only? Or included in the daily enrollment file?
Update enrollment files will be sent daily by the Enrollment Broker. The full file will be sent weekly following C.O.B. on Friday. There will also be a monthly file produced on the third to last working day of the month.
Louisiana Healthcare Connections
Eligibility and Enrollment Data
Exchange
Please confirm if daily is M-F or S-S? Does this include holidays? Is the expectation to process file within 24 hours with include weekends or business days? Does this time to process the file also apply to any monthly full audit files or just the daily files?
Daily is M-F. It does not include state-designated holidays . The 24 hours references working days. The time requirement applies to the daily files.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 108 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
711 RFP 16.9. Provider Enrollment 196
52 RFP 17.1.15 Claims Management 205
118 RFP 17.3.1 Explanation of Benefits 207
597 RFP 17.3.1 Explanation of Benefits 207
712 RFP 17.5. 206
Aetna Better Health, Inc.
This section references DHH posting a list at the onset of the contract of specialty and subspecialty codes that the CCN must utilize within their provider enrollment system. When will DHH provide the list of provider codes? We recommend providing this list as soon as possible to avoid errors in coding providers during the build of the provider subsystem in our computer system.
Refer to Systems Companion Guide, Section G
Coventry Health Care of Louisiana,
Inc.Please define "gross adjustments" as referred to in this section.
If the contractor needs to make pricing-based adjustments on a retrospective basis to a large group of provider claims in their system, this would be considered "gross adjustments".
Coventry Health Care of Louisiana,
Inc.
17.3 CCN shall within 45 days of payment of claims, provide individual notices to a sample group of the members who received services Must include:service furnishedprovider furnishing the servicedate on which the service was furnishedamount of the payment made for the serviceWhat is the "sample group" size?
Sample size shall be not less than 1% of members for whom a claim was paid in the previous 45 days.
Louisiana Hospital Association
Can DHH explain the intent of this section? It refers to a sample group of members.
Medicaid regulations ( Section 433.1116 (e) require that Medicaid claims systems, as a condition of FFP, must provide individual notices, within 45 days of payment of claims, to all or a sample group of persons who receive services under the Plan.
Aetna Better Health, Inc.
Claims Processing Methodology Requirements
In our review, we were unable to locate language related to the Correct Coding Initiative (CCI) and CCI approaches. We recommend the state include a subsection within 17.5 that requires the CCN to include nationally recognized methodologies to correctly pay claims including but not limited to:• CCI for Professional and Outpatient services;• Multiple Surgical Reductions;• Global Day E & M Bundling.
17.1.10 The CCN must comply with requirements of Section 6507 of the Patient Protection and Affordable Care Act of 2010, regarding “Mandatory State Use of National Correct Coding Initiatives,” including all applicable rules, regulations, and methodologies implemented as a result of this initiative.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 109 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
713 RFP 17.5. 206
374 RFP 17.5.2 209
564 WellPoint RFP 17.5.2 209
53 RFP 17.5.2.2 209 Is this requirement the same as section 10.6.2.11 page 116? Yes
565 WellPoint RFP 17.5.3 209
598 RFP 17.5.4 Data Reporting 210
Aetna Better Health, Inc.
Claims Processing Methodology Requirements
Under what circumstances would a CCN not be permitted to require it's participating providers to follow industry standard coding methodologies?
The only exception is for atypical providers, who are not required to obtain an NPI from NPPES. DHH recognizes the following provider types as atypical:Non-emergency medical transportation.
AmeriHealth Mercy of Louisiana
Claims Dispute Management
Are there internal requirements for the internal claims dispute procedure or is the CCN able to establish its own procedures?
The CCN shall develop their own internal claims dispute procedures and adhere to requirements as stated in Section 17.5.2.
Is it the expectation for the CCN to submit all claim disputes to the independent reviewer in the event our internal review establishes that we should find in favor of the provider? Can the CCN be the first level of contact or is it expected that all appeals go directly to the independent reviewers?
Claim disputes must be sent to the independent reviewer if they cannot be resolved at the CCN level. The CCN can be the first level of contact.
Coventry Health Care of Louisiana,
Inc.Claims Dispute Management
Could state provide report format for Claims Payment Accuracy Report?
A copy of the report will be added to the Systems Companion Guide.
Louisiana Hospital Association
While there are provisions for data reporting around time/accuracy, as well as possible sanctions for CCNs not meeting those targets, what happens if a CCN provides inaccurate or incomplete information that is ultimately used by a provider for participation in such programs such as Medicare DSH or 340B and the incorrect data adversely affects that provider's ability to participate in those programs, thus costing the provider money? Does DHH plan to implement requirements for the CCN to make the provider whole?
DHH currently provides hospitals direct access to the Medicaid Fiscal Intermediary (Molina) to validate patient Medicaid eligibility information used for Medicare DSH. Molina bills hospitals for this service. There are no plans to change this process.
Neither the CCN’s nor DHH are responsible for the accuracy of hospital’s Medicare DSH calculations. Hospitals could, however, address reporting requirements needed for purposes of Medicare DSH during their negotiations with CCN’s.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 110 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
148 WellCare RFP 17.5.4.12 Encounter Data 212
538 WellPoint RFP 212, 220
107 RFP 17.5.4.13 212
146 WellCare RFP 17.5.4.8 Encounter Data 211
How is the 95% encounter submission rate calculated? How is the denominator determined for this SLA? Our assumption of the numerator is the number of encounters accepted without any errors by the fiscal agent.
The submission rate is different from the acceptance rate. The submission rate refers to the percentage of paid claims that were submitted to the Medicaid Fiscal Intermediary as encounter within the contractual timeframe. The acceptance rate is the number of encounters accepted without errors. The Medicaid Fiscal Intermediary will use an internal audit of the CCN showing claims received and encounters submitted to calculate the submission rate. The denominator will come from the CCN, the number of claims received in the submission month.
17.5.4.12 and 18.8
Para. 17.5.4.12 asks for encounter data at least monthly, while the report submission chart in 18.8 references a weekly frequency. Please clarify. We think the monthly submission is typical.
CCNs are required to at least submit monthly, however, the Fiscal Intermediary can accept submissions as frequently as weekly.
Coventry Health Care of Louisiana,
Inc.
Adherence to Key Claims Management
Standards
Is there a limit to the size of encounter files? Is there any need to split encounter files by line of business, region, type of encounter (ie maternity), etc.?
25 MG is the file size limit. There is no need to split by business, region, etc.
Duplicate Rejections: Will the State provide the CMOs with a list of encounters that were rejected for duplicate error codes. We will be interested in understanding the details of the original encounter and the duplicate encounter. This will help us understand the root cause for the duplicate issue. (Example: there could be difference in procedure modifiers)
The Medicaid Fiscal Intermediary will provide a report with the TCN that denied for duplicate but will not provide the original TCN the encounter duplicated against.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 111 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
147 WellCare RFP 17.5.4.8 Encounter Data 211
599 RFP 17.5.4.9 Denial Reporting 211 DHH has taken the comment under advisement.
501 Adams and Reese RFP 2.1.1.2 12
Provider Registry: Will the State share the validation logic used for verifying if the provider in the encounter matches the provider in the Provider Registry. The following will help us implement validations similar to the fiscal agent: Fields used for validation, sequence of the fields used for validation, validation rules for each field
The principal validation logic checks for values in all required fields, as noted in the Systems Companion Guide (SCG) . Any required fields that are not populated will cause a record to be rejected. With respect to specific validation edits, we are expecting a valid provider NPI (as issued by NPPES) and taxonomy(ies). If the provider is already enrolled with Louisiana Medicaid, then we expect a valid Louisiana Medicaid Provider ID. Also, we expect to find valid provider type and provider specialty values, and if sub-specialty values are entered, they should be valid values based on the value table from the SCG.
Louisiana Hospital Association
During the Systems/Technical meeting on 4/19, the health plans expressed concern around getting credit in their scoring for services that may have been rendered but were denied for an administrative reason. However, administrative denial reporting is not required by the health plans in this section. In the interest of transparency and an indicator of proper behavior by a health plan, it is imperative that this type of reporting be required and added to the list on page 211.
Scope of Work, Requirements for CCN-
P Entity
What types of "managed care organizations", i.e. HMO, PPO, etc. would DHH qualify as a proposer, assuming the organization is licensed by LDOI under La. R.S. 22:1016.
This question should be directed to the Louisiana Department of Insurance.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 112 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
54 RFP 12
502 Adams and Reese RFP 2.1.1.3 12
653 RFP 2.1.1.5 12
503 Adams and Reese RFP 2.1.1.6. 12
55 RFP 2.23.12.1 259 There is no 42 CFR Part 376. Please provide correct citation. The correct citation is 2 CFR, Part 376.
Coventry Health Care of Louisiana,
Inc.2.1.1.2 & B.29 Requirements for CCN-
P EntityIf the CCN is currently a licensed HMO in the state of Louisiana, and holds a COA as such, is that sufficient, or is there a separate licensure/certification that is necessary.
Yes the CCN may utilize its current license or COA, however the CCN is required to report all expenditures (See Financial Reporting Guide) for this contract separate and apart from its commercial product. The CCN is also responsible to get any and all approvals from the Louisiana Department of Insurance necessary for the inclusion of the Medicaid contract under the current DOI license. Please contact the Louisiana Department of Insurance to determine the license or COA that is needed to comply with RS 22:1016 which governs Medicaid prepaid entities.
Scope of Work, Requirements for CCN-
P Entity
La. R.S. 12:24 does not cover nonprofit corporations. Please confirm a nonprofit corporation would not qualify as a proposer in response to the CCN-P or CCN-S RFPs.
This question should be directed to the Louisiana Department of Insurance.
Children's Hospital Health Plan
Requirements for CCN-P Entity
For new plans, is the NCQA New Plans certification sufficient to meet this requirement? How long after contract award will the CCN-P have to obtain the certification?
1) NCQA New Heath Plan Accreditation is sufficient to meet the requirement for plans that are less than three years old.
2) The CCN must become either URAC or NCQA accredited on the earliest possible date the CCN can apply for recognition.
Scope of Work, Requirements for CCN-
P Entity
What methodology will DHH use to determine whether network capacity is sufficient for enrollment of 75,000 Medicaid members in a GSA? What data must proposers submit to ensure accurate conclusion by DHH?
The CCN is required to submit a listing of providers with provider type, name, address for which they have LOIs and/or subcontracts.
Coventry Health Care of Louisiana,
Inc.Debarment
/Suspension/Exclusion

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 113 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
298 RFP 2.3.1 14
654 RFP 2.3.2 14
731 Advocacy Center RFP 2.4.1.1 15 Yes, This will be corrected via addendum to the RFP
56 RFP 2.5.1.1 15 This is a acceptable.
270 RFP 2.5.1.1 15 No
57 RFP 2.5.1.3 15
AmeriHealth Mercy of Louisiana
General CCN Requirements
The second part of the ownership disclosure requirement is unclear -- The first part calls for disclosure of: (1) ownership of the CCN; and of (2) any subcontractors owned by the CCN, which is clear. Is the second part asking for disclosure of information for any subcontractor or only related parties? Would all ownership disclosure requirements be met by filing of the CMS 1513 Form, as required in Section 18.2 of the RFP (p. 213)? If not, what is the "approved Disclosure Form" referenced in Section 2.3.1?
The second part is asking for disclosure of information for each person or entity with ownership or controlling interest of 5% or more in the CCN and any of its subcontractors, including all entities owned or controlled by a parent organization.
CMS Form 1513 may be used for reporting these persons or entities.
Children's Hospital Health Plan
General CCN Requirements
We have reviewed the list of Louisiana State Holidays. There are numerous days that our organization does not specifically recognize as a holiday, e.g. Veteran's Day. We do, however, recognize as a holiday the Day after Thanksgiving. Are we permitted to substitute holidays for purposes of closing the customer call center or other similar administrative departments?
No, the CCN customer call center and all administrative departments shall be operational on all DHH regularly scheduled business days. However, the Governor of Louisiana normally proclaims the day after Thanksgiving a state holiday.
Moral and Religious Objections
The RFP states that if a plan will not provide counseling or a referral service because of a moral or religious objection, it must notify "DHH with its proposal whenever it adopts the policy during the term of the Contract." Is there a typographical error in the sentence; is the provision intended to require notice to "DHH with its proposal or, if later, whenever it adopts the policy during the term of the Contract" ?
Coventry Health Care of Louisiana,
Inc.General Insurance
InformationCertificates of Insurance have facsimile signatures of the authorized representative of the insurer which is standard practice. Confirm this is acceptable.
Louisiana Healthcare Connections
General Insurance Information
Can the insurance be issued in the name of the parent company of the CCN as long as the CCN is covered by the policy?
Coventry Health Care of Louisiana,
Inc.General Insurance
InformationWe do not release copies of these policies; they are proprietary. Confirm that is acceptable.
The RFP requires the contractor to provide copies of insurance policies to DHH, if DHH so requests; that will not be changed.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 114 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
271 RFP 2.5.1.3 15
300 RFP 2.5.1.4 15 No.
301 RFP 2.5.4 Reinsurance 16
58 RFP 2.5.5.2 17
59 RFP 2.5.6 17 What are examples of special hazards?
Louisiana Healthcare Connections
General Insurance Information
Section 2.5.1.1. says the insurance needs to be submitted and approved; however, 2.5.1.3. states it should be submitted on request, does DHH want proof of insurance submitted for approval?
2.5.1.1 says work shall not commence until all insurance is acquired and the certificate shall be provided. 2.5.1.3 makes reference to the entire policy which DHH may review.
AmeriHealth Mercy of Louisiana
General Insurance Information
Could the CCN meet the intent of this requirement by making an affirmative covenant to provide 30 days' advance notice to DHH of, and obtain DHH's consent for, the cancellation, expiration or amendment of the CCN's insurance policies? The requirement for policies of insurance to be written so as to include the notice requirement to DHH would be cumbersome and difficult to administer where the CCN is insured as part of a corporate-wide insurance program.
AmeriHealth Mercy of Louisiana
Section 2.5.4.1 requires the CCN to file contracts of reinsurance or a summary of the plan of self-insurance. However, Section 2.5.4.3 requires the CCN to "maintain reinsurance agreements throughout the Contract period." Please clarify whether a CCN must obtain reinsurance or whether it is permitted to self-insure. Also, the words "shall be filed with the reinsurance agreements" in Section 2.5.4.2 should be deleted as the sentence does not appear to make sense if this language is included.
Section § 2.5.4.1 provides a choice of either reinsurance or self-insurance. Section § 2.5.4.3 states that reinsurance, if applicable, must be maintained during the life of the contract.
Coventry Health Care of Louisiana,
Inc.Errors and Omissions
InsuranceCCN's E&O policy is written by a risk retention group and therefore not rated by A.M Best. Please confirm how we should address this.
The RFP requires the contractor to provide copies of insurance policies to DHH, if DHH so requests; that will not be changed.
Coventry Health Care of Louisiana,
Inc.Insurance Covering
Special Hazards
There may not be any special hazards associated with the CCN-P contract, but generally special hazards are hazards faced by the contractors’ employees or sub-contractors which may subject them to serious health or safety issues. Office of Risk Management's insurance guidance include as examples pollution and chemicals.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 115 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
60 RFP 2.5.7 17
206 HMO Louisiana, Inc. RFP 2.5.8 17 Address the need for subcontractors to have reinsurance. DHH is holding the CCN responsible
61 RFP 2.6.1 17
62 RFP 2.6.1 17 DHH does not have a form
574 RFP 2.6.1 Bond Requirements 17 No
602 Walgreens RFP 20.11.1 Proposal Format 327
150 WellCare RFP 20.13.1.11 240
700 RFP 20.2.3 Operations Readiness 228
Coventry Health Care of Louisiana,
Inc.
Licensed and Non-Licensed Motor
VehiclesWhat if auto policy does not cover use of any non-licensed motor vehicle? How is this relevant for this RFP?
The relevancy of the RFP is that DHH wants to assure that non-licensed motor vehicles are covered by insurance when in use.
Subcontractor's Insurance
Coventry Health Care of Louisiana,
Inc.Performance Bond or
SubstitutePlease confirm that CCN can secure a 1-year performance bond that can be renewed every 12-months, consistent with direction we received during previous application process.
A one-year performance bond that shall be renewed every 12 months is acceptable.
Coventry Health Care of Louisiana,
Inc.Performance Bond or
SubstituteCan CCN use its own, or its surety's bond form, or does DHH have a form the CCN is to use? If the latter, please provide.
United Healthcare of Louisiana
Would DHH consider a parental guarantee of ten (10) million dollars ($10,000,000) in lieu of a performance bond?
Related to submittal requirements, can maps and other exhibits that don't fit well on 8.5x11 paper, can we use larger foldouts or other means?
Neither the CCN’s nor DHH are responsible for the accuracy of hospital’s Medicare DSH calculations. Hospitals could, however, address reporting requirements needed for purposes of Medicare DSH during their negotiations with CCN’s.
Misconduct for Which Intermediate Sanctions
May Be Imposed
Is there a limitation on this clause that the care can only be determined to meet the standard for sanction if that care is not consistent with the standard of care in that region of the state. For example, if someone sues a network provider for malpractice and court comes back and finds no malpractice b/c the care is consistent with the community standard of care, under this provision, would DHH still apply the sanction?
No, there is no such limitation. The factors of goods or services that are 1) insufficient for the member's needs, 2) harmful to the member, or 3) of grossly inferior quality are not tied to community standards. As stated in § 20.13.1.11, this determination is at the sole discretion of DHH.
Aetna Better Health, Inc.
Please clarify the date the CCNs network is required to be certified without monetary penalty. Is it 95 days from operational start date or Oct 7th?
The CCN must provide Network Adequacy Documentation no later than the date specified in the Schedule of Events.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 116 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
149 WellCare RFP 20.2.3 Penalties 229 Yes
376 RFP 20.22.1 243
377 RFP 20.23.2 243 Correct, a addendum will be issued to correct the reference.
378 RFP 20.24.3 244 Correct, a addendum will be issued to correct the reference.
600 Walgreens RFP 20.9.3 Proposal Prohibitions 324 Yes
601 Walgreens RFP 20.9.3 Proposal Prohibitions 324 No, not for the same CCN-model
151 WellCare RFP 21.11.2 Proposal Submission 248
Can the State provide additional insight into when this penalty will be applied? Does this mean if an encounter identified during Medical record review is missing in our encounter submissions we will be eligible for a penalty? “Ten thousand dollars ($10,000.00) per occurrence of medical record review by DHH or its designee where the CCN or its providers denotes provision of services which were not submitted in the encounter data regardless of whether or not the provider was paid for the service that was documented.”
AmeriHealth Mercy of Louisiana
Termination for CCN Insolvency, Bankruptcy,
Instability of FundsPlease clarify the criteria used to determine whether the CCN has become financially unstable.
Determinations of financial solvency or lack thereof will be made by the Louisiana Department of Insurance
AmeriHealth Mercy of Louisiana
Termination for Ownership Violations
The provision references Sections 20.21.1.1-20.21.1.3 of the RFP; however, there are no such sections. Please clarify this reference.
AmeriHealth Mercy of Louisiana
Special Rules for Temporary
Management
The provision references Sections 20.21.1.1-20.21.1.3 of the RFP; however, there are no such sections. Please clarify this reference.
Can an entity serve as primary for CCN-P and subcontract for CCN-S (or vice versa?)
Can an entity bid under a Joint Venture also bid as a subcontractor?
Is it acceptable if the electronic copy of the proposal is provided in PDF? If so, the RFP requires that a couple of items (e.g., information in response to B.16) be in Excel format. If you still want them in Excel, can we provide these files in addition to the PDF? If we cannot provide the proposal in PDF, please consider allowing the attachments to be provided in PDF.
Yes; Yes, the electronic version may include data in multiple formats (pdf, Excel, Word, Visio, etc).

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 117 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
152 WellCare RFP 21.11.2 Proposal Submission 248
688 RFP 21.11.2. Proposal Submission 248
379 RFP 21.12.6 249 One copy of the redacted version is needed.
687 RFP 21.17. Proposal Format 250 No
511 WellPoint RFP 251
Does the Proposer have discretion regarding the number of files and naming conventions for the electronic files or does DHH have specific requirements for this?
DHH does not have specific requirements for naming conventions or number of electronic files.
Aetna Better Health, Inc.
In regards to the electronic copy of the proposal, which format is preferred by the State (i.e., MS Word or is a PDF file acceptable)?
DHH does not have a preference. The "Find" feature is sometimes more successful in Word.
AmeriHealth Mercy of Louisiana
Proprietary and/or Confidential Information
If a Proposer submits a redacted version of its proposal (redacting its confidential information), must ten (10) copies of the redacted version be provided? [Note that Section 21.11.2 of the RFP (p. 248) requires the submission of one (1) original + ten (10) copies of the Proposal.]
Aetna Better Health, Inc.
Is there a minimum/maximum size for graphics (e.g., flowcharts, tables, etc.)?
21.17.5 and 21.17.6
Is it correct that our responses to Sections A, B, C, D, E, and F should each be in a separate binder? And that our responses to Sections G through S can be combined and do not have to be separately bound?
Section 21.7.6 is being amended to indicate that Sections B-S (rather than B-F) be in a separate binder from Section 21.17.6 Currently Reads The response to the Technical Requirements Sections (Sections B-F) should be in separate binder (s) and clearly labeled with contents. The Proposer should duplicate the CCN-P Proposal Submission and Evaluation Requirements, Section B-F . . . 21.17.6 Should Read The response to the Technical Requirements Sections (Sections B-S) should be in separate binder (s) and clearly labeled with contents. The Proposer should duplicate the CCN-P Proposal Submission and Evaluation Requirements, Section B-S . . .
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 118 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
383 RFP 23.19.1 Fraudulent Activity 263
566 WellPoint RFP 23.2.3 257 Has DDH identified any Limited English Proficiency groups?
384 RFP 23.40.5 Prohibited Payments 269
207 HMO Louisiana, Inc. RFP 23.45.1 270 The correct reference is La R.S. 46:56.
389 RFP 3.1.3 / 9.4 19/106
63 RFP 3.4.1.1 20
64 RFP 3.4.1.1. 20
303 RFP 23
AmeriHealth Mercy of Louisiana
This provision requires that suspected fraud or abuse be reported to DHH "as soon as practical after discovering suspected incidents." This timeframe is different than the timeframes referenced in Section 15.5 of the RFP and in Appendix EE. Please clarify the timeframe for such reports.
3 business days as specified in Appendix EE is the correct timeframe for referral to Program Integrity. Section 15.5.1 refers to Federal Requirements and the 23.19.1 timeframe will be amended to "as soon as practical after discovering suspected incidents, but no more than 3 business days."
The Procurement Library contains a file with preferred language as indicated on the Eligibility File at the parish level.
AmeriHealth Mercy of Louisiana
What "organization" is this requirement intended to apply to - the home health provider or the CCN? Also, are there specific requirements for the surety bond?.
The organization referred to is the CCN.
Safeguarding Information
The reference listed is La R.S. 45:56, however this does not exist. Would they please supply the corrected reference?
AmeriHealth Mercy of Louisiana
Eligibility Determinations / Effective Date of Payment for New
Members
When an individual is determined to be eligible for Medicaid, what retroactivity, if any, is applied? Per section 9.4 a member is effective on the beginning of the following month, are they any situations where retroactive eligibility is applied?
Retroactive eligibility will be provided through Medicaid fee-for-service with the exception of newborns.
Coventry Health Care of Louisiana,
Inc.Mandatory CCN
PopulationsHow are member populations identified on the on the file and how should they be reported back to the DHH?
Member populations are identified on the file by their aid category and case type.
Coventry Health Care of Louisiana,
Inc.Mandatory CCN
Populations
Please advise what the reporting structure is for membership populations. Are FITAP and LIFC members allowed to be rolled up for reporting or should they be reported separately?
The aid groupings for capitation purposes are 1) Children under age 19, 2) Parents, 3) A/B/D, and 4)Breast and Cervical Cancer and 5) Foster Children. Adults in both FITAP and LIFC are included in the Parents grouping.
AmeriHealth Mercy of Louisiana
3.6.1 through 3.6.11
Excluded CCN Populations
How is this reflected in the capitation rate payment process? Was the development of the capitation rates consistent with this payment approach?
The populations outlined on Page 23 of the RFP are excluded from the CCN program and therefore their FFS claims and eligibility data are not included in the base data used for rate development.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 119 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
65 RFP 3.6.3 23
66 RFP 4.1.6 Key Staff Positions 26
391 RFP 4.1.6 Key Staff Positions 25 - 30
499 HMO Louisiana, Inc. RFP 4.1.6.13 29
203 HMO Louisiana, Inc. RFP 4.1.6.2 26 Yes
67 RFP 4.1.6.5 27
Coventry Health Care of Louisiana,
Inc.Excluded CCN Populations
Please advise if members have Medicare part D but not yet have Medicare part A & B, are they still eligible for Medicaid?
Medicare beneficiaries cannot enroll in Medicare Part D if they are not enrolled in Medicare Part A or B.
Coventry Health Care of Louisiana,
Inc.
Previously, when we were going through the application process, we sent Social Security Numbers directly to Ruth Kennedy under separate cover so that they could be protected and kept confidential. Will this be allowed going forward?
DHH will establish a process to assure confidentiality after Contracts are signed.
AmeriHealth Mercy of Louisiana
Please clarify whether all of the individual positions listed in 4.1.6.1 through 4.1.6.17 are the "key staff" positions that are subject to limitations and special reporting requirements in Sections 4.1.1, 4.1.3, 4.1.4, 4.1.5 and 4.1.6.
Yes, 4.1.6.1 through 4.1.6.17 are the key staff positions referred to in 4.1.1, 4.1.3, 4.1.4, 4.1.5, and 4.1.6.
Member Services Manager
The Provider Services Manager description is under Member Service Manager. Is this intended to apply to member or provider?
The Member Services Manager description has been amended
Medical Director / CMO
The Medical Director shall be actively involved in all major clinical and quality management components of the CCN, including credentialing and referral management, medical policies and procedures, etc. Can the CCN Medical Director oversee staff that already handles these duties?
Coventry Health Care of Louisiana,
Inc.Grievance System
Management
Business Continuity Planning & Emergency Coord. position reference Services for members who may need to be evacuated to other areas of the state or out of state. Is it the responsibility of BCP&E Coordinator to coordinate the movement of homebound members with large equipment? or manage and oversee the emergency plan with VP,GM and Dir.Health Service? We do have a corporate team who can handle this position. Joanne Storbeck.
Correct reference is 4.1.6.6. The parish Office of Emergency Management is responsible for the transfer of citizens and necessary medical equipment to safety. The purpose of the BCP&E position is to manage and oversee the CCN's emergency management plan (EMP). Refer to § 23.14.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 120 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
120 WellCare RFP 30
121 WellCare RFP 4.5.1 and 4.5.2 32
313 RFP 5.11.1 Return of Funds 36
655 RFP 5.12.1 37
315 RFP 5.12.2.2 Third Party Liability 37
4.1.7.1 and 4.1.7.2
Key Staff Positions - Additional Required
Staff
Will the DHH reconsider having a "Louisiana" licensed nurse, physician or physician's assistant as long as they are licensed? Can the staff member who is a Louisiana licensed registered nurse, physician or physician's assistant also be the person who is providing the direction? Or, is this at least two people?
This staff shall include a Louisiana licensed registered nurse, physician or physician's assistant. The staff will work under the direction of a Louisiana-licensed registered nurse, physician or physician's assistant. It is at least two people.
Annual Reporting to DHH
Please confirm that an organization and functional organization chart are not required as part of the RFP submission? If they are, would DHH prefer to see interim employees or would they prefer to see all open positions that we would recruit for as part of the readiness process?
Refer to Appendix KK, B.8, B.9 and B.12. DHH prefers to see all open positions that would be recruited rather than interim employees who will not be actually be assigned to the Louisiana account.
AmeriHealth Mercy of Louisiana
Is there a mechanism to handle disputes of amounts determined by DHH to be owed under Sections 5.11.1 and 5.11.2?
Yes, Section 23.30 states "The CCN may request in writing an interpretation of the issues relating to the Contract from the Medicaid CCN Program Director. In the event the CCN disputes the interpretation by the Medicaid CCN Program Director, the CCN shall submit a written reconsideration request to the Medicaid Director.
Children's Hospital Health Plan
General TPL Information
Does DHH collect TPL/COB information from clients upon enrollment? If so, will DHH share that information with the CCN's?
Yes. TPL information will be included in the 834 Enrollment File sent to the CCN.
AmeriHealth Mercy of Louisiana
Is it the States expectation the CCN go after the primary insurer or could the CCN recoup the overpayment from the provider with the appropriate denial code requesting the provider to submit the claim to the private insurer.
The 5.12.2.2 requirement is the CCN will bill the private insurance to recoup payment from the primary insurer.
No, the CCN may not recoup the overpayment from the provider and request the provider to submit the claim to the private insurer.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 121 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
656 RFP 5.12.2.2 Cost Avoidance 37
775 RFP 5.12.3.4 39
68 RFP 5.12.3.4 39
254 RFP 5.12.3.4 pg. 39
69 RFP 5.12.3.4 39
316 RFP 5.12.3.5 39 An addendum will be made to correct the sentence
Children's Hospital Health Plan
This verbiage indicates that the "CCN shall bill the private insurance within 60 days from discovery of coverage". It is DHH's intention that all COB be handled on a pay-and-chase basis? Can the CCN deny claims for COB if the CCN has information that another payer exists?
The CCN shall adjudicate claims for medical treatment associated with labor, delivery and EPSDT in accordance with federal and state law.
Amerigroup Corporation
Third Party Liability Post-Payment
Recoveries
There is a requirement that the CCN-P regularly provide newly identified third party coverage information to the DHH vendor but there is no mention of DHH or its vendor providing known or newly identified third party coverage information to the CCN-P at the time of enrollment or periodically thereafter. Will such information be provided and if so on what frequency?
The data will transmitted electronically from the FI to the CCN daily.
Coventry Health Care of Louisiana,
Inc.Post Payment
RecoveriesPlease advise who the DHH contracted vendor is that Third party liability information should be provided and is there a required format?
The CCN should provide post payment recoveries to the Fiscal Intermediary (Molina) via encounter data.
Coventry Health Care of Louisiana,
Inc.Post-payment
RecoveriesWhat is the format for this information i.e. electronic, fax, report?
The CCN should provide post payment recoveries to the Fiscal Intermediary (Molina) via encounter data.
Coventry Health Care of Louisiana,
Inc.Post Payment
Recoveries
requests the CCN must report the existence of Third Party Liability, to the DHH contracted vendor on a monthly basis by the 15th working day of the month from the date of discovery. Section 5.12.5.4 indicates the CCN shall report members with third party coverage to DHH on a monthly basis by the 15th working day of the month. Can you please clarify if these requirements are referencing the same reporting requirement/report or if they are the difference reports and if so can it be clarified the requirements of each.
No, these are two (2) separate requirements. Section 5.12.3.4 speaks to reporting of Third Party Liability as defined in the Glossary. Section 5.12.5.4 speaks to reporting health insurance coverage on a member.
AmeriHealth Mercy of Louisiana
Post-Payment Recoveries
Please revise the last part of the sentence to state, "...and may seek reimbursement when claims in the aggregate are or less than $500."
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 122 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
70 RFP 5.12.3.7 39
71 RFP 5.12.4 39
Coventry Health Care of Louisiana,
Inc.Post Payment
Recoveries
indicates that prior to accepting a Third Party Liability settlement on claims equal to or greater than $25,000, the CCN shall obtain approval from the DHH. Does the $25,000 threshold apply the paid value of the claims comprising a lien that was paid by the CCN regardless if the available funds from which we can pursue a recovery are less than the $25,000 paid? What is the process to submit this approval to the DHH and is there a turn around time that the state strives to achieve on such responses?
Acceptance of DHHs approval must be obtained when the total amount of all claims is equal to or greater than $25,000.00 regardless of the amount of available funds from recovery can be pursued. Approval is not needed when processing claims pursuant to a health insurance policy. The process requires that the CCN contact the Eligibility Special Services Section for requesting approval for settlement authority. The turnaround time will be within ten business days from receipt of a completed request for approval.
Coventry Health Care of Louisiana,
Inc.Distribution of TPL
Recoveries
Distribution of TPL Recoveries reads that the CCN may retain up to 100% of its TPL collections if all of the following conditions exist:
Section 5.12.4.1 The total collections received do not exceed the total amount of the CCN financial liability for the member. Can you please clarify the intent of this requirement and provide an example of what is being referenced as the total amount of the CCN financial liability for the member.
Section 5.12.4.2 There are no payments made by DHH related to fee for service reinsurance administrative costs. How is it being determined if the DHH had rendered payments for the aforementioned items and will the DHH provide a listing of TPL cases being pursued from the liable third party for which the member may be continuing to treat and accumulate expenses that were incurred by the CCN?
Section 5.12.4.1 - The intent of this requirement is to protect the member's interest in settlement funds. An example would be, if a CCN has paid $10,000.00 in claims for the member and there is a settlement of $50,000.00. The CCN would only be able to collect up to $10,000.00 from the settlement. Section 5.12.4.2 - The intent of this requirement is to protect DHH's interest so that DHH is first reimbursed from settlement funds, any fee-for-service, reinsurance or administrative costs which may have paid by DHH for the member. It is not the intent of DHH to provide a listing of TPL cases at this time.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 123 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
657 RFP 5.12.5.1 39
72 RFP 5.12.6.1 40
307 RFP 5.2.2 33 The CCNs will not have access to LEERS .
Children's Hospital Health Plan
TPL Reporting Requirements
How is COB information collected by the CCN submitted to DHH? Is there a specific file layout for this data transmission? Will DHH be providing a Joint Interface Plan detailing the report file layouts expected of the CCN for this deliverable as well as other reports cited in the RFP?
Molina will develop a web application that will permit a CCN-P organization to enter and submit TPL information for an enrolled recipient. The information will be collected and stored by Molina, and then forwarded on a weekly basis to the DHH TPL contractor, HMS. HMS will use the information to update the MMIS mainframe TPL Resource File, after which, Molina will establish a process to sense the update and issue a status back to the submitting CCN-P organization via the web application. Once complete, these format requirements will be added to the Systems Companion Guide.
Coventry Health Care of Louisiana,
Inc.
DHH Right to Conduct Identification and
Pursuit of TPL
When the CCN fails to collect payment from the Third Party Liability within 365 days from the date of service DHH may invoke its right to pursue recovery. For cases of third party liability such as medical malpractice, contested workers compensation, or other instances where litigation is involved, the lifecycle of a recovery can extend beyond 365 days from the date of service. Is the 365 day requirement only pertaining to recovery of other insurance such as recovery of funds from Medicare or another commercial carrier?
No. The 365 day limit applies to all Third Party Liability claims.
AmeriHealth Mercy of Louisiana
Maternity Kick Payments
Will the CCNs have access to Louisiana Electronic Event Registration System (LEERS) maternity data for their members?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 124 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
309 RFP 5.4.2 and 5.4.3 Payment Adjustments 34
310 RFP 5.6.4 35 No
311 RFP 5.6.6 35
312 RFP 5.7.1 Risk Adjustment 35
273 RFP 6.1.5 42 The correct Reference is 2.4.
AmeriHealth Mercy of Louisiana
Section 5.4.2 indicates that in cases where a member switched from a CCN eligible aid category to a CCN excluded aid category that previous capitation payments will be recouped from the CCN. Section 5.4.3 indicates that in cases of retroactive Medicare enrollment that a CCN should recoup payments from a provider and instruct the provider to resubmit the claims to Medicare and secondarily to the Medicaid FFS program. What is the correct procedure for handling payments in cases where the member is determined to have retroactive eligibility in another non-CCN program? Is this process consistent with the capitation rate development?
The CCN shall instruct the provider to resubmit the claim(s) through Medicaid MMIS directly and DHH will pay the claim subject to the twelve (12) month limitation described above, after recoupment of the PMPM has been made. In order for the provider to be reimbursed by DHH they must be enrolled with Medicaid.
Yes, this is consistent with the capitation rate development.
AmeriHealth Mercy of Louisiana
Determination of CCN Rates
This section indicates that future rates may be set based on encounter and/or financial data as the CCN program matures and FFS data is no longer available. Are there specific parameters for the level of FFS data that is necessary to continue setting rates using the current methodology?
AmeriHealth Mercy of Louisiana
Determination of CCN Rates
What is the anticipated schedule for revisions to the capitation rates?
The rates will be adjusted as deemed necessary by the Department.
AmeriHealth Mercy of Louisiana
Please provide detailed methodology regarding the adjustments that will be made to the ACG risk assignment process to account for the fact that CCNs will not be at risk for pharmacy services. Will two sets of risk weights be calculated, and how will normalization between these weights be applied?
Two sets of cost weights will be developed. One set for each CCN program (CCN-P) and (CCN-S) to reflect the differences between the benefits covered/evaluated under each program. Since the pre-paid rates and the benchmarks were developed based on the entire population, each CCN-P/CCN-S will be compared to the risk for All CCNs. The results will vary depending upon which program is being evaluated and in turn which set of cost weights were used.
Louisiana Healthcare Connections
Core Benefits and Services
Family planning makes reference to section 6.1.13.; however, this section does not exist in the RFP. Should this be 2.4?
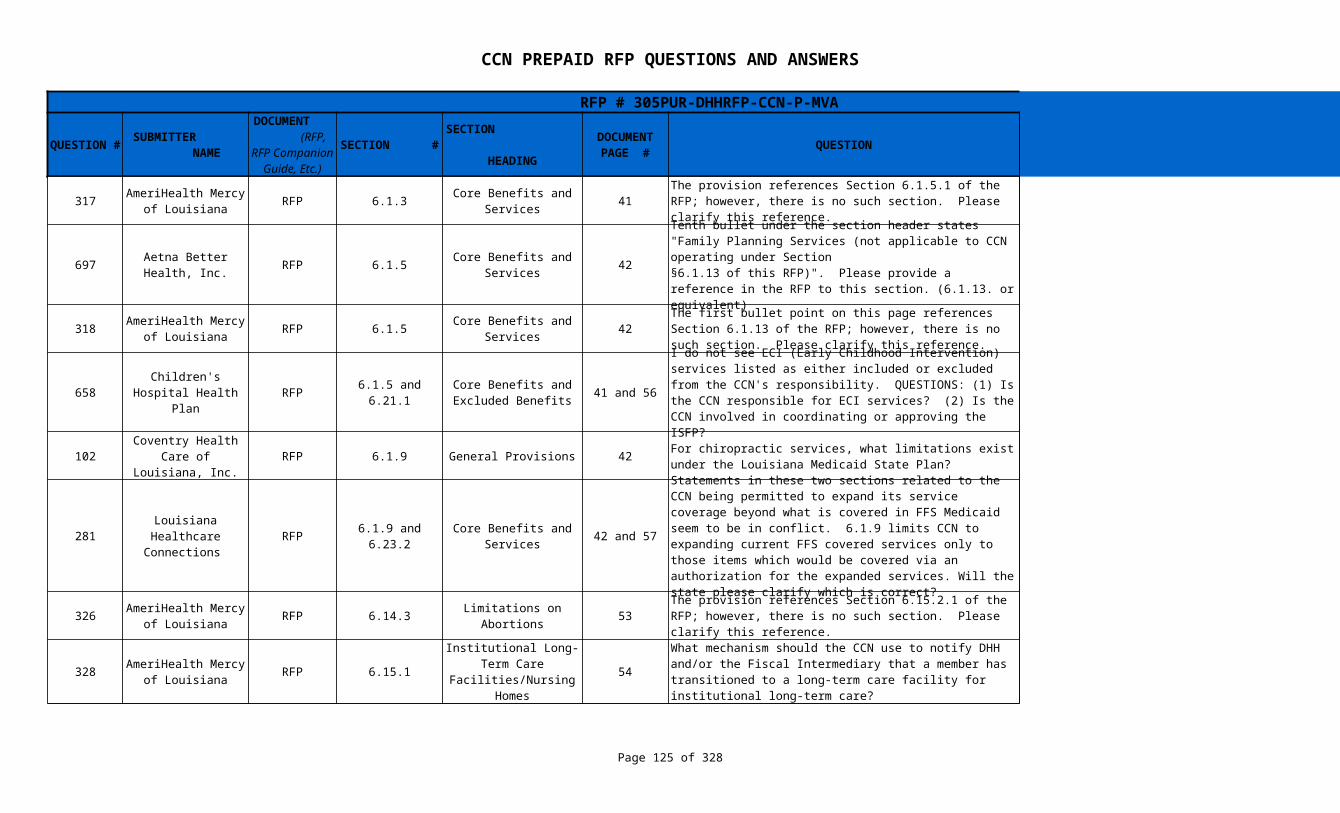
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 125 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
317 RFP 6.1.3 41 The correct Reference is 6.1.5.
697 RFP 6.1.5 42 The correct Reference is 2.4.
318 RFP 6.1.5 42 The correct Reference is 2.4.
658 RFP 6.1.5 and 6.21.1 41 and 56
102 RFP 6.1.9 General Provisions 42
281 RFP 6.1.9 and 6.23.2 42 and 57
326 RFP 6.14.3 53 The correct reference is §6.14.2.
328 RFP 6.15.1 54
AmeriHealth Mercy of Louisiana
Core Benefits and Services
The provision references Section 6.1.5.1 of the RFP; however, there is no such section. Please clarify this reference.
Aetna Better Health, Inc.
Core Benefits and Services
Tenth bullet under the section header states "Family Planning Services (not applicable to CCN operating under Section§6.1.13 of this RFP)". Please provide a reference in the RFP to this section. (6.1.13. or equivalent)
AmeriHealth Mercy of Louisiana
Core Benefits and Services
The first bullet point on this page references Section 6.1.13 of the RFP; however, there is no such section. Please clarify this reference.
Children's Hospital Health Plan
Core Benefits and Excluded Benefits
I do not see ECI (Early Childhood Intervention) services listed as either included or excluded from the CCN's responsibility. QUESTIONS: (1) Is the CCN responsible for ECI services? (2) Is the CCN involved in coordinating or approving the ISFP?
Refer to section 6.21.1.1 The CCN is not responsible for ECI services, nor is the CCN involved in coordinating or approving the ISFP.
Coventry Health Care of Louisiana,
Inc.For chiropractic services, what limitations exist under the Louisiana Medicaid State Plan?
Refer to the Medicaid Service Chart under Benefits and Services in the CCN-P Procurement Library.
Louisiana Healthcare Connections
Core Benefits and Services
Statements in these two sections related to the CCN being permitted to expand its service coverage beyond what is covered in FFS Medicaid seem to be in conflict. 6.1.9 limits CCN to expanding current FFS covered services only to those items which would be covered via an authorization for the expanded services. Will the state please clarify which is correct?
Refer to the Medicaid Service Chart under Benefits and Services in the CCN-P Procurement Library. http://new.dhh.louisiana.gov/assets/docs/Making_Medicaid_Better/Resources/Medicaid_Services_Chart.pdf
AmeriHealth Mercy of Louisiana
Limitations on Abortions
The provision references Section 6.15.2.1 of the RFP; however, there is no such section. Please clarify this reference.
AmeriHealth Mercy of Louisiana
Institutional Long-Term Care Facilities/Nursing
Homes
What mechanism should the CCN use to notify DHH and/or the Fiscal Intermediary that a member has transitioned to a long-term care facility for institutional long-term care?
DHH is electronically notified of all nursing facility admissions by the facilities themselves.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 126 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
327 RFP 6.15.1 54
125 WellCare RFP 6.15.2 54
423 APS Healthcare RFP 6.16 and 6.16.2 55
702 RFP 6.16.2 55 Is the initial phase in period from 1/1/2012 until 5/1/2012?
73 RFP 6.16.3 55
330 RFP 6.16.3.3 55
AmeriHealth Mercy of Louisiana
Institutional Long-Term Care Facilities/Nursing
Homes
What are the system edits that affect the disenrollment date of a CCN member who transitions to nursing home level of care?
The last date that a member can be disenrolled with an effective date of the first day of the following month is the third to last working day of the month. On the second to last and last working days of the month, the disenrollment would be effective for the 1st day of the second month
Institutional Long-Term Care Facilities/Nursing
Homes
The preceding paragraph says they will be disenrolled at the "earliest effective date allowed by system edits" what does this mean?
DHH (Medicaid eligibility) is notified by the nursing facility when an individual is admitted. The case will immediately be changed to a LTC Case Type on the eligibility system. System edits do not allow a change effective the first day of the following month if the change is entered on the second-to-last or last working day of the month. For such cases, the effective date will be the first day of the second month.
Medical Services for Special Populations,
This section outlines the responsibilities of the CCN in identifying members with special health care needs. Will the Department make available claims data to the CCN from the MMIS for members to help in identification of individuals with special healthcare needs?
Yes, the Department will make available two years of historic claims data from the MMIS for members assigned to them
Aetna Better Health, Inc.
Medical Services for Special Populations
180 days (or 6 months) begins on the “go live date” for that member. For some it will be 1/12 through 6/12 (assuming no delays in implementation). For GSA C, it would be 5/12 through 11/12.
Coventry Health Care of Louisiana,
Inc.Medical Services for Special Populations
How will the enrollment broker notify the CCN of members with special needs?
If the Medicaid recipient self declares they have special health care needs to the Enrollment Broker the Enrollment Broker will provide an indicator via the X 12 834 file.
AmeriHealth Mercy of Louisiana
Medical Services for Special Populations
What special health care needs are captured by the Enrollment Broker and transmitted through the eligibility file?
Those special health needs that are self-declared by the enrollee to the Enrollment Broker.
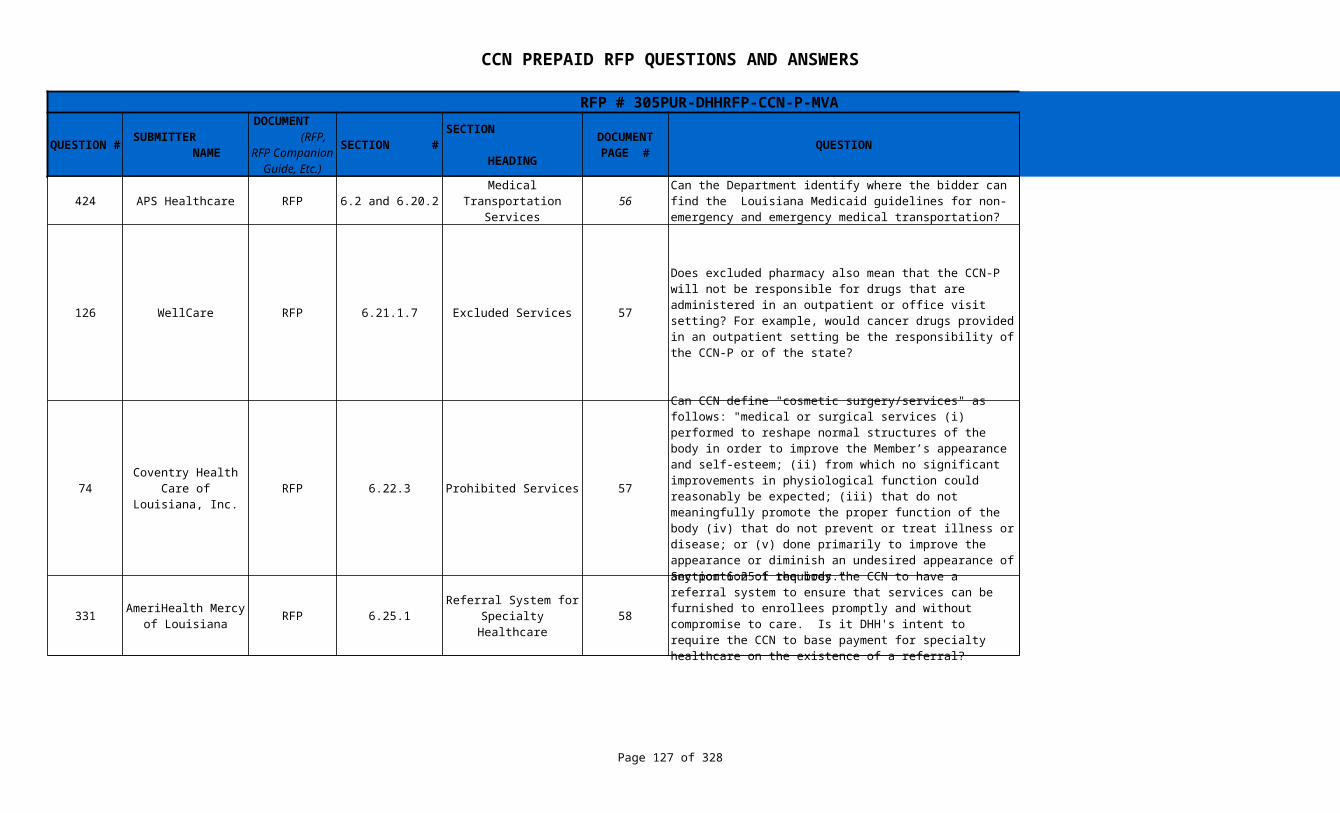
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 127 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
424 APS Healthcare RFP 6.2 and 6.20.2 56
126 WellCare RFP 6.21.1.7 Excluded Services 57
74 RFP 6.22.3 Prohibited Services 57 DHH shall utilize the definition as defined for Fee For Service.
331 RFP 6.25.1 58 DHH has no such requirement
Medical Transportation Services
Can the Department identify where the bidder can find the Louisiana Medicaid guidelines for non-emergency and emergency medical transportation?
The url to the Transportation Provider Manual is http://www.lamedicaid.com/provweb1/Providermanuals/manuals/MED_TRANS/MED_TRANS.pdf
Does excluded pharmacy also mean that the CCN-P will not be responsible for drugs that are administered in an outpatient or office visit setting? For example, would cancer drugs provided in an outpatient setting be the responsibility of the CCN-P or of the state?
Excluded pharmacy defined within the RFP is "prescription drugs dispensed through pharmacies"; therefore, those types of drugs covered in the physician program would be covered through the CCN.If it is a J code that is payable, then the Professional Services Program would currently pay for the drug. Otherwise, the provider could write a prescription for the drug, have the recipient take it to the pharmacy to fill it and return to the doctor's office to have it injected
Coventry Health Care of Louisiana,
Inc.
Can CCN define "cosmetic surgery/services" as follows: "medical or surgical services (i) performed to reshape normal structures of the body in order to improve the Member’s appearance and self-esteem; (ii) from which no significant improvements in physiological function could reasonably be expected; (iii) that do not meaningfully promote the proper function of the body (iv) that do not prevent or treat illness or disease; or (v) done primarily to improve the appearance or diminish an undesired appearance of any portion of the body."
AmeriHealth Mercy of Louisiana
Referral System for Specialty Healthcare
Section 6.25.1 requires the CCN to have a referral system to ensure that services can be furnished to enrollees promptly and without compromise to care. Is it DHH's intent to require the CCN to base payment for specialty healthcare on the existence of a referral?
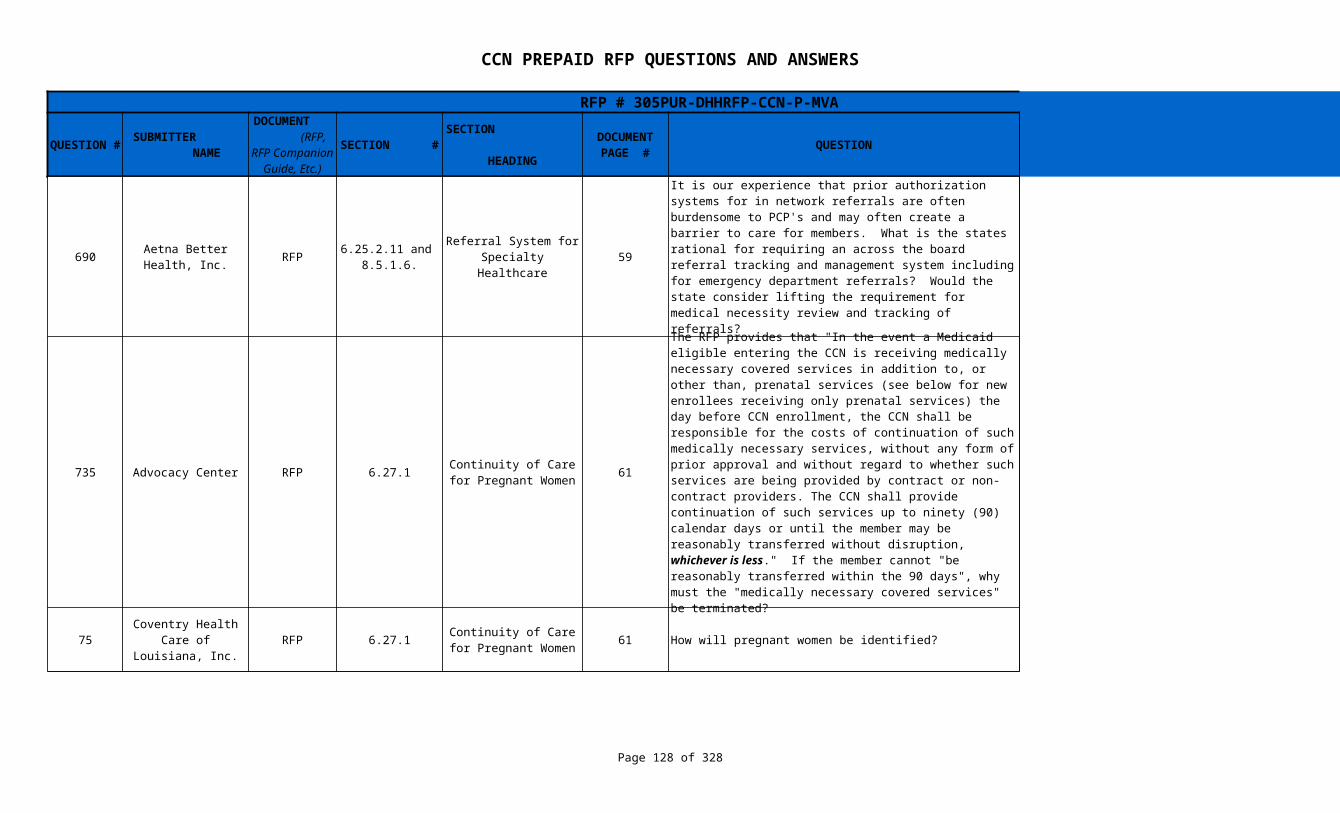
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 128 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
690 RFP 59
735 Advocacy Center RFP 6.27.1 61
75 RFP 6.27.1 61 How will pregnant women be identified?
Aetna Better Health, Inc.
6.25.2.11 and 8.5.1.6.
Referral System for Specialty Healthcare
It is our experience that prior authorization systems for in network referrals are often burdensome to PCP's and may often create a barrier to care for members. What is the states rational for requiring an across the board referral tracking and management system including for emergency department referrals? Would the state consider lifting the requirement for medical necessity review and tracking of referrals?
DHH is not requiring the tracking of referrals. If the CCN does require referrals as a condition of payment, DHH strongly encourages the use of electronic referrals as an alternative to paper. The sentence that reads " In the event a referral is made via the telephone, the CCN shall ensure that referral data, including the final decision, is maintained in a data file that can be accessed electronically by the CCN, the provider and DHH."
Continuity of Care for Pregnant Women
The RFP provides that "In the event a Medicaid eligible entering the CCN is receiving medically necessary covered services in addition to, or other than, prenatal services (see below for new enrollees receiving only prenatal services) the day before CCN enrollment, the CCN shall be responsible for the costs of continuation of such medically necessary services, without any form of prior approval and without regard to whether such services are being provided by contract or non-contract providers. The CCN shall provide continuation of such services up to ninety (90) calendar days or until the member may be reasonably transferred without disruption, whichever is less." If the member cannot "be reasonably transferred within the 90 days", why must the "medically necessary covered services" be terminated?
This provision does not require services to be terminated, it provides a timeframe in which the CCN must transition care from either FFS provider or another CCN.
Coventry Health Care of Louisiana,
Inc.Continuity of Care for
Pregnant Women
Women whose basis of eligibility is pregnancy will be identified by their Type Case (13, 53, 104, and 127) which will be included on the Enrollment File provided to the CCN by the Enrollment Broker

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 129 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
736 Advocacy Center RFP 6.29.1 61
738 Advocacy Center RFP 6.29.1 61
739 Advocacy Center RFP 6.29.1 61
Continuity of Care for Individuals with Special
Health Needs
The RFP provides that "During the initial implementation of the CCN Program in the event a Medicaid/CHIP eligible entering the CCN is receiving medically necessary covered services, the day before CCN enrollment, the CCN shall provide continuation/coordination of such services up to ninety (90) calendar days or until the member may be reasonably transferred without disruption, whichever is less." If the member cannot "be reasonably transferred within the 90 days" (for example because of providers who are absorbing hundreds of new clients in addition to their prior patient loads--indeed the RFP allows 180 days for identification of special health care needs at the initial roll-outs, §6.16.2), why must the "medically necessary covered services" be terminated?
This provision does not require services to be terminated, it provides a timeframe in which the CCN must transition care from either FFS provider or another CCN.
Continuity of Care for Individuals with Special
Health Needs
Given plans are to be provided with recipient's claims data, if a plan fails to assess and provide prior authorizations for a recipient's ongoing medically necessary services within the 90 day period, what action will DHH take against the CCN?
If decision is not made timely, the CCN must provide the core benefits and services being requested.If a determination is not made by the above time frames, the member’s request will be deemed to have been approved as of the date upon which a final determination should have been made.
Continuity of Care for Individuals with Special
Health Needs
If a plan fails to assess and provide prior authorizations for a recipient's ongoing medically necessary services within the 90 day period, what options will be immediately available to the recipient who has lost access to medically necessary services like ostomy, respiratory, tracheotomy, etc., supplies or rehabilitative services?
If decision is not made timely, the CCN must provide the core benefits and services being requested.If a determination is not made by the above time frames, the member’s request will be deemed to have been approved as of the date upon which a final determination should have been made.
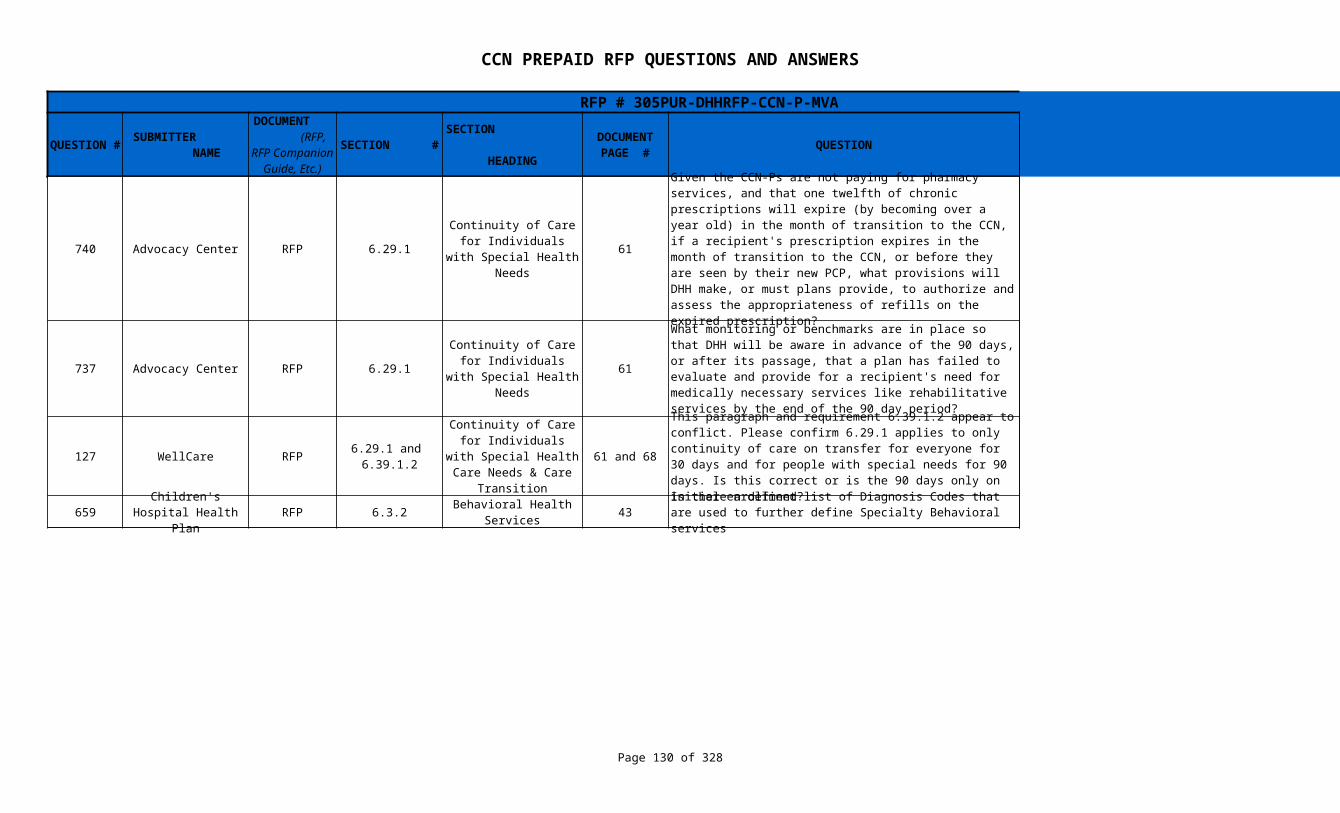
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 130 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
740 Advocacy Center RFP 6.29.1 61
737 Advocacy Center RFP 6.29.1 61 See Question # 365
127 WellCare RFP 61 and 68 The 90 days is for initial enrollment only.
659 RFP 6.3.2 43 See Question #518
Continuity of Care for Individuals with Special
Health Needs
Given the CCN-Ps are not paying for pharmacy services, and that one twelfth of chronic prescriptions will expire (by becoming over a year old) in the month of transition to the CCN, if a recipient's prescription expires in the month of transition to the CCN, or before they are seen by their new PCP, what provisions will DHH make, or must plans provide, to authorize and assess the appropriateness of refills on the expired prescription?
See Question # 33 and 785. Any prescriptions in which the authorization has expired, the pharmacist would contact the patient’s physician for needed refills.
Continuity of Care for Individuals with Special
Health Needs
What monitoring or benchmarks are in place so that DHH will be aware in advance of the 90 days, or after its passage, that a plan has failed to evaluate and provide for a recipient's need for medically necessary services like rehabilitative services by the end of the 90 day period?
6.29.1 and 6.39.1.2
Continuity of Care for Individuals with Special
Health Care Needs & Care Transition
This paragraph and requirement 6.39.1.2 appear to conflict. Please confirm 6.29.1 applies to only continuity of care on transfer for everyone for 30 days and for people with special needs for 90 days. Is this correct or is the 90 days only on initial enrollment?
Children's Hospital Health Plan
Behavioral Health Services
Is there a defined list of Diagnosis Codes that are used to further define Specialty Behavioral services
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 131 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
518 WellPoint RFP 43 - 446.3.2.2 and 6.3.4.2
Section 6.3.2.2 indicates services provided by a psychiatrist, psychologist, and/or mental health rehabilitation providers are specialized mental health services, which are not the responsibility of the CNN. However, section 6.3.4.2 states, “Those behavioral health services for individuals whose need for such services is secondary to a primary medical condition in any episode of care [are the responsibility of the CCN]”
Can the state confirm that if a psychiatrist, psychologist, and/or mental health rehabilitation provider renders a service, but the diagnosis is secondary to a medical diagnosis, that the CCN is responsible?
Codes 96150-96155 are all regarded as specialized behavioral health. Medicaid managed care enrollees in MCOs and PCCMs will be enrolled in the SMO to receive specialized behavioral health services. The following services for Medicaid MCO beneficiaries are excluded from the SMO and included in the CCN prepaid rates. All other mental health and substance abuse services and beneficiaries are included in SMO. • Acute detoxification (Revenue codes of 116, 126, 136, 146, 156 as well as 202 and 204 with DT diagnoses to accommodate for Delirium Tremens (DT)),• Mental health services provided in a medical (physical health) Medicaid MCO Member's PCP or medical office (i.e., MD, DO, or RHC other than services provided by a psychiatrist)• Mental health services provided in a Federally Qualified Health Center and • Emergency room services except services provided to members with primary codes of 290 through 319.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 132 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
319 RFP 6.3.3 43
320 RFP 6.3.3 43
AmeriHealth Mercy of Louisiana
Basic Behavioral Health Services
How will the CCN be made aware of the criteria for screening protocols and determining whether an individual meets criteria for specialized behavioral health?
It is DHH's intent that behavioral health training and expertise will not be required. If a CCN provider or case manager believes that an individual needs care by a psychiatrist, rehabilitative outpatient care, residential, addiction disorder care, or inpatient psychiatric or other behavioral health care beyond the purview of the primary care provider (or beyond the scope of behavioral health services offered by FQHC treating the individual), the CCN provider may refer the individual to the Statewide Management Organization (SMO) for screening. The SMO will be responsible for screening all referred individuals and referring the adult/child to medically necessary specialized behavioral health services. The SMO will be utilizing a brief CANS screen for all children as well as utilizing national American Society of Addiction Medicine (ASAM) criteria for substance abuse services. Existing criteria for adult clinic and rehabilitation services will be utilized.
AmeriHealth Mercy of Louisiana
Basic Behavioral Health Services
Does application of the criteria for screening protocols (for determining whether an individual meets criteria for specialized behavioral health) require behavioral health training and expertise? Must the reviewer have specialized qualifications in order to accurately apply the criteria?
The CCN provider or case manager may refer any individual to the SMO if the provider believes that an individual needs care by a psychiatrist, rehabilitative outpatient care, residential, addiction disorder care, or inpatient psychiatric or other behavioral health care beyond the purview of the primary care provider (or beyond the scope of behavioral health services offered by FQHC treating the individual). Family members, consumers, advocates, schools, etc can refer an individual to the SMO.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 133 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
519 WellPoint RFP 6.3.3 and 6.3.4.1 43 - 44 See Question # 320
321 RFP 6.3.4 44
Basic Behavioral Health Services
Section 6.3.3 states, “Criteria for screening protocols and determining whether an individual meets the criteria for specialized behavioral health services shall be determined by DHH and are based on factors relating to age, diagnosis, disability (acuity) and duration of the mental health illness/condition.” Additionally, section 6.3.4.1 states, “The CCN shall utilize the screening tools and protocols approved by DHH.”
Are there existing criteria , tools, and/or protocols that DHH can provide?
AmeriHealth Mercy of Louisiana
Basic Behavioral Health Services
Section 6.3.4 does not provide an all-inclusive list of items that are to be covered by the CCN as "basic behavioral health services." Please clarify whether such a list exists and if so, can DHH share that list with bidders?
Basic Behavioral Health services to be included for CCN's are as follows: CPT 99201-99215. Medicaid managed care enrollees in MCOs and PCCMs will be enrolled in the SMO to receive specialized behavioral health services. The following services for Medicaid MCO beneficiaries are excluded from the SMO and included in the CCN prepaid rates. All other mental health and substance abuse services and beneficiaries are included in SMO. • Acute detoxification (Revenue codes of 116, 126, 136, 146, 156 as well as 202 and 204 with DT diagnoses to accommodate for Delirium Tremens (DT))• Mental health services provided in a medical (physical health) Medicaid MCO Member's PCP or medical office (i.e., MD, DO, or RHC other than services provided by a psychiatrist)• Mental health services provided in a Federally Qualified Health Center and • Emergency room services except services provided to members with primary codes of 290 through 319.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 134 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
694 RFP 6.3.4.2 44 See Question # 518
695 RFP 6.3.4.2 44
520 WellPoint RFP 6.3.4.2 44 See Question # 122
660 RFP 6.3.4.2 44 See Question # 122
274 RFP 6.30.5 62
742 Advocacy Center RFP 6.30.3 62 No, that is not prohibited.
Aetna Better Health, Inc.
Basic Behavioral Health Services
Would the CCN cover Health and Behavior Assessment and Intervention CPT Codes 96150-96155? These are services provided in a PCP practice by a BH clinician without requiring a BH diagnosis?
Aetna Better Health, Inc.
Basic Behavioral Health Services
The RFP states that the CCN will cover "Inpatient hospital services based on medical necessity, including:Acute Medical Detoxification". This implies outpatient detox remains with the MBHO. Please define and describe the obligations of the MBHO and CCN to coordinate care for members.
Outpatient detox is the responsibility of the Children's System of Care/SMO. CCNs have the responsibility for inpatient detox to stabilize and care for the patient until the receiving facility accepts the patient.
Basic Behavioral Health Services
Section 6.3.4.2 states basic behavioral health services include “Outpatient non-psychiatric hospital services.”
Please provide further details and/or examples of what these services entail.
Children's Hospital Health Plan
Basic Behavioral Health Services
Need a better understanding of Behavioral Health Services. Please define "outpatient non-psychiatric services"
Louisiana Healthcare Connections
Continuity for Behavioral Health Care
This provision indicates that the CCN should document in the member's medical record; however, medical records are maintained by each treating provider. Please confirm that your intent is that CCNs document in the member's record within the CCN's systems.
That is correct--within the member's administrative record maintained by the CCN.
Continuity for Behavioral Health Care
The RFP requires referral for emergency behavioral services to the “nearest emergency medical provider.” If the plan can also offer a referral to a more qualified provider, is that prohibited?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 135 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
696 RFP 6.30.3 62
703 RFP 6.30.3 62
76 RFP 6.32.1 Care Transition 63
704 RFP 6.32.3 Care Transition 63
Aetna Better Health, Inc.
Continuity for Behavioral Health Care
In instances where the member is presented to the CCN provider or MBHO provider and admitted to the emergency department, how would the CCN be aware of the emergency department referral to do the required follow-up? Is this follow-up requirement limited to the instance where the CCN and not the network provider or the MBHO makes the referral?
The CCN is responsible in all cases where the CCN enrollee presents at the emergency room services except services provided to members with primary codes of 290 through 319. Federal requirements that should be included in the CCN contract with emergency rooms should outline requirements for emergency rooms to contact the CCN when necessary for post-stabilization authorization. These requirements are based on the situations described, and are not limited to instances in which the CCN makes the referral. Furthermore, the CCN will likely be billed by the hospital providing the emergency service, providing the CCN with additional information for evaluating possible referrals.
Aetna Better Health, Inc.
Continuity for Behavioral Health Care
Please clarify the responsibility of the CCN to pay for all services, including psychiatric evaluative services, as part of emergency services.
Payment for emergency health services including those services that are coded as behavioral health are the responsibility of the CCN
Coventry Health Care of Louisiana,
Inc.How will members who are transferred from another CCN or the FFS program be identified?
An indicator will be included in the 834 Enrollment File transmitted to the CCN by the Enrollment Broker
Aetna Better Health, Inc.
This section states if a member is transferred between CCNs but is hospitalized at the time the transfer shall be effective for the date of enrollment into the receiving CCN; this would result in the hospital needing to split the bill for the hospital stay. In similar instances in other state Medicaid contracts, the relinquishing CCN remains responsible for the member's hospitalization until the member is discharged. Then the receiving CCN is responsible for all other care. We recommend that the DHH consider revising this section for administrative simplicity for the member, the hospital and the CCNs.
The RFP language has been amended to state that the relinquishing CCN is responsible for the member’s hospitalization until the member is discharged. The receiving CCN is responsible for all other care.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 136 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
332 RFP 6.32.4 Care Transition 63
661 RFP 6.32.4 Care Transition 63 Yes
733 Advocacy Center RFP 6.5.1 EPSDT Well Child Visits 45
AmeriHealth Mercy of Louisiana
Is there a state mandated rate that providers can charge the CCN for copying of medical records?
Louisiana Statute includes the following allowable charges for record copying: If the original treatment records are generated, maintained, or stored in paper form, copies shall be provided upon payment of a reasonable copying charge, not to exceed:
• one dollar per page for the first twenty-five pages,
• fifty cents per page for twenty-six to three hundred fifty pages,
• and twenty-five cents per page thereafter,
• a handling charge not to exceed twenty-five dollars,
• and actual postage.
Children's Hospital Health Plan
This paragraph requires the receiving CCN to obtain a full set of medical records from the previous CCN when a member moves from one plan to another. Will the inbound 834 eligibility file identify transfer-in members and the plan from which they came?
The RFP states that EPSDT services are "comprehensive and preventative." In deciding whether to provide EPSDT services can plans limit services to those they determine cost-effective at reducing future medical costs?
No; the EPSDT statute and federal Medicaid regulations require that states cover all services within the scope of the federal Medicaid program, including services outside the Medicaid State Plan, if necessary to correct or ameliorate a known medical condition ( 42 U.S.C. § 1396d(r)(5) and the CMS Medicaid State Manual).

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 137 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
732 Advocacy Center RFP 6.5.1 & 6.5.2 EPSDT Well Child Visits 45 By the most recent statute and state plan provisions.
559 WellPoint RFP 6.5.4 46 What periodicity schedule (edition/year) is used for EPSDT?
730 RFP 6.5.6 EPSDT Well Child Visits 46
322 RFP 6.5.6.1 EPSDT Well Child Visits 46
324 RFP 6.6.4 Immunizations 47
584 RFP 6.7.1.2 47
The RFP states that EPSDT emphasizes preventative services and that plans should comply with the federal EPSDT regulations, statute, and CMS guidance. The federal regulations are inconsistent with the statute and the state plan, in that they make EPSDT provision of services not in the state plan "discretionary." 42 C.F.R. §441.57. Are plans governed by the federal regulations promulgated in 1984, or by the more recent statute and state plan provisions?
The Louisiana EPSDT periodicity schedule can be found in the Procurement Library. See http://www.la-kidmed.com/Forms/EducationalMaterials.aspx
Aetna Better Health, Inc.
Please confirm if the 75% age group in the periodicity table is the aggregate for all measures.
The 75% is of eligible members under the age of twenty- one (21) that have received at least one (1) EPSDT well child visits for FFY 2012. ( Line 10 of CMS 416)
AmeriHealth Mercy of Louisiana
What methodology will be utilized to measure well visits from health plan encounters? Are there any continuous eligibility requirements used when reporting this information?
Refer to CMS 416 instructions located in the Procurement library.
AmeriHealth Mercy of Louisiana
Will the CCNs be able to receive historical data on their members from the Louisiana Immunization Network for Kids (LINKS)?
An enrolled provider can log on to LINKS and retrieve their members immunization record regardless of who administered the immunization.
Louisiana Hospital Association
Emergency Medical Services and Post
Stabilization Services
Can DHH elaborate on 6.7.1.2 and the requirement for CCN's to advise all CCN members of the provisions governing in and out-of-service-area use of emergency services as defined in the glossary? How are CCN's going to be required to carry this out and how will it be measured?
In reviewing the Member Handbook, DHH will determine whether the CCN's policy on in and out-of-service area use of emergency services is addressed.
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 138 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
323 RFP 6.7.1.3 47
325 RFP 6.7.2.1.2.2 48 Language amended to remove the 6.7.2.1.4.1 reference.
205 HMO Louisiana, Inc. RFP 7.1.14 71 Only those requirements applicable to providers..
662 RFP 7.1.15.10 73
334 RFP 7.1.15.10 73 Yes
204 HMO Louisiana, Inc. RFP 7.1.15.10 73
AmeriHealth Mercy of Louisiana
Emergency Medical Services
Please clarify whether it is permissible to deny payment to the provider for emergency services if the CCN or PCP is not notified after the 10-day period specified in this section. It is not clear whether the limitation is with respect to the time period, or the non-notification.
The CCN must allow 10 days for the notification. If the notification of emergency services is not provided to the CCN within 10 days, they can deny payment
AmeriHealth Mercy of Louisiana
Post Stabilization Services
The provision references Section 6.7.2.1.4.1 of the RFP; however, there is no such section. Please clarify this reference.
General Provider Network Requirements
The CNN’s network providers shall comply with all requirements set forth in this RFP.” Does these mean that only those requirements placed on a provider versus all requirements placed on the CCN?
Children's Hospital Health Plan
General Provider Network Requirements
What is the state’s preferred method of validating provider demographic data? Also, does this stipulation apply to contract and non contracted providers?
DHH does not have a preferred method for validation. The stipulation is applicable only to contract providers. The intent is to minimize obsolete information in Provider Directories.
AmeriHealth Mercy of Louisiana
General Provider Network Requirements
Will DHH accept CCNs making best efforts to validate provider demographic data on a quarterly basis?
General Provider Network Requirements
The CCN shall at least quarterly validate provider demographic data to ensure that current, accurate, and clean data is on file for all contracted providers. Failure to do so may result in monetary penalties up to $5,000 per day against the CCN. With what frequency of on-site visits and accuracy of data does DHH expect this item to be accomplished?
The expectation is that provider data (provider name, address, telephone number, NPI, whether accepting new patients languages spoken, contract #, contract begin date, contract end date ) be current. For items that are subject to change, the CCN is ultimately responsible for accuracy of the information. DHH has no requirement for on-site visits.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 139 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
333 RFP 7.1.15.2 72
77 RFP
663 RFP 70
664 RFP 70 and 71
AmeriHealth Mercy of Louisiana
General Provider Network Requirements
Section 7.1.15.2 requires providers to be "eligible" to enroll as Louisiana Medicaid providers. Please clarify the criteria for determining eligibility for enrollment and whether DHH is responsible for determining eligibility.
Please see the Provider Eligibility page of lamedicaid.com at the following link: http://www.lamedicaid.com/provweb1/Provider_Enrollment/ProviderEnrollmentIndex.htm To be eligible to enroll, a provider cannot be on any federal or state exclusion list.
Coventry Health Care of Louisiana,
Inc.
7.1.15.3 and
15.4
General Provider Network Requirements
Excluded Providers
72
186
Please confirm that the new CMS screening regulations that were issued in February 2011 now require the state Medicaid agencies to conduct screening of providers in EPLS and LEIE, not the managed care organizations.
In their response to comments received regarding the proposed Rule, CMS states the following: Section 455.436 does not mandate that States require their providers to check the LEIE and EPLS on a monthly basis to determine whether the providers’ employees and contractors have been excluded. We do however, recommend that States consider making this a requirement for all providers and contractors, including managed care contractors in their Medicaid programs and CHIP [emphasis ours]
Children's Hospital Health Plan
7.1.6, 7.1.7 and 7.1.8
General Provider Network Requirements
The use of the phrase any willing provider seems to conflict with limitation of network. Please clarify
We do not see the phrase “any willing provider” in Sections § 7.1.6, §7.1.7 or §7.1.8.
Children's Hospital Health Plan
7.1.6 through 7.1.11
General Provider Network Requirements
The language in these sections is confusing. Some paragraphs seems to contradict other paragraphs. Paragraph 7.1.6 (page 70) implies an "any willing provider" requirement. Paragraph 7.1.8 (page 71) softens the concept of "any willing provider". Paragraph 7.1.11 (page 71) provides the ability to deny participation. Would DHH make a definitive statement to the effect that this RFP does not represent an "any willing provider" contract, provided that the plan has sufficient providers to meet network adequacy and to manage timely access to all Covered Services for members?
§7.1.6 is not intended and does not include an “any willing provider” requirement. As stated, CCNs are encouraged to make a good faith effort to negotiate a contract with current Medicaid providers who request to be a network member. This RFP does not represent an “any willing provider” contract. Evaluation of proposals includes inclusion of Significant Traditional Providers (STPs).
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 140 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
665 RFP 7.11.1 90
666 RFP 7.11.5 91 Define PC PCP Collaborative activities
343 RFP 7.12.12 93 Yes
105 RFP DHH in still working on the Louisiana Medicaid policy.
667 RFP 7.12.6 92
342 RFP 7.12.7 92
Children's Hospital Health Plan
Patient-Centered Medical Home (PCMH)
Define “go live date”, e.g. go live date of the agreement with the state or from the PCMH program
This refers to the date services become the responsibility of the CCN in the GSA
Children's Hospital Health Plan
Patient-Centered Medical Home (PCMH)
The CCN should join and participate in Patient-Centered Primary Care Collaborative Centers. Information on the PC PCC can be found at http://www.pcpcc.net
AmeriHealth Mercy of Louisiana
Subcontract Requirements
This section requires all subcontracts to contain the terms and conditions listed in section 23 of the RFP, yet some of these terms and conditions are unique to the DHH-CCN relationship. May the CCN develop a standard subcontractor addendum, for DHH approval, that incorporates all relevant portions of section 23 of the RFP as they would apply to the CCN-subcontractor relationship?
Coventry Health Care of Louisiana,
Inc.
7.12.5.7 and 9.5.13
Glossary - Subcontractor requirements
Claims Processing Requirements
Provider Preventable Conditions
92108
293
Will DHH further specifically define OPPCs (other provider preventable conditions) as required by the proposed ruling for Section 2702 of the Patient Protection and Affordable Care Act of 2010 which prohibits Federal payments to States for any amounts expended for providing medical assistance for health care-acquired conditions. It would authorize States to identify "other provider-preventable conditions" for which Medicaid payment would be prohibited.
Children's Hospital Health Plan
Subcontract Requirements
By when do major subcontracts need to be submitted to DHH for approval if plan is in GSA A?
The CCN must initially provide subcontractor information as specified in B.11 of Appendix KK with submission of proposal. The final subcontract must be submitted 30 after the contract has been signed by the DHH.
AmeriHealth Mercy of Louisiana
Subcontract Requirements
Please clarify -- there is a reference in this section to both "this RFP" and to "this Contract." Does DHH intend for the RFP to function as the CCN Contract? Also, please confirm that the reference to section 7.6 is correct.
The Contract includes the RFP and in the order of precedence, the RFP is first.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 141 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
587 RFP 7.2.2.3 Mainstreaming 73
668 RFP 7.3.2 74
242 RFP 7.3.2.2.1 74 We are doing an addendum to say 10 miles or 30 minutes
221 HMO Louisiana, Inc. RFP 7.3.2.2.1 74
669 RFP 7.5.1 Timely Access 75 See Glossary for definition of immediate
Louisiana Hospital Association
In this section, 'preference to private pay or Medicaid fee-for-service patients' is listed as an example of discriminatory practices. This seems to be a broad stroke that would seem to qualify a provider's business decision to limit or not accept Medicaid or Medicaid managed care patients as a discriminatory act. Could DHH clarify?
Federal Medicaid regulations strictly prohibit Medicaid managed care providers showing preference to private pay or Medicaid fee for service patients. See 42 CRF, Part 438.206 ( c ) (1) (ii) which states, that each MCO must "ensure that the network providers offer hours of operation that are no less than the hours of operation offered to commercial enrollees or comparable to Medicaid fee-for-service, if the provide serves only Medicaid enrollees"
Children's Hospital Health Plan
Travel Time and Distance
(1) At what point in time will we be required to Proof Time and Distance? (2) When will street level address data be provided
These requirements are due with the GSA Network Adequacy Documentation Deadline within the Schedule of Events.
Coventry Health Care of Louisiana,
Inc.Time and Distance to
Hospitals
I noticed on pg. 74 of the RFP, the "Time and Distance to Hospitals," 7.3.2.2.1, only specifies thirty (30) minutes for urban hospitals. Since no other time and distance criteria are stated in "minutes" only, should we ask the State for clarification? (Previously, the CCN-P document from last Fall had the parameter as 30 miles.)
Travel Time and Distance / Time and Distance to Hospitals
The RFP states that hospitals in an urban area has to be 30 minutes from the member's residence. Is this correct or should it read 30 miles? If it is 30 minutes, then can we convert it to 1 mile per minute?
Thirty minutes is correct, assuming normal urban travel time as determined by mapping software as per 7.3.2.
Children's Hospital Health Plan
What guidelines are utilized to define the term "immediately"? Do the rule and regulations of EMTALA govern here?
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 142 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
588 RFP 7.5.10 Timely Access 76
768 RFP 7.5.4 75
670 RFP 7.6.2 77 The CCN can require that their network PCPs notify them .
705 RFP 7.6.2 77 Internal Medicine should be included in Section 7.6.2
335 RFP 7.6.7 78 Yes
Louisiana Hospital Association
7.5.10 states that the CCN shall monitor provider regularly to determine compliance with this section through such methods as mystery shopping and staged scenarios in an effort to reduce the unnecessary use of alternative methods of access to care such as emergency room visits and take corrective action if there is a failure to comply. Could DHH clarify the intent and limitations of this section?
DHH believes it is self-explanatory. The intent is that the CCN monitor contract providers to assure timely access standards are being adhered to.
Amerigroup Corporation
Timely Access, Maternity Care
The timeframe for initial maternity appointments for newly enrolled members is calculated from the postmark date. However, since mail can take 2-3 days to reach a new member and since welcome calls where the CCN would discover a member is pregnant may not occur until 4 business days after the mailing (per 12.11.2.1), we would like further clarification of the requirement for a new member to have an initial maternity appointment within 3 days of postmark
This timeframe is only be applicable for newly enrolled members whose basis of eligibility is pregnancy as indicated by the Type Case on the 834 Enrollment File and therefore known to the CCN upon receipt of the Enrollment File of if the member has self -identified to the Enrollment Broker that they are pregnant and the information is included in the 834 Enrollment File.
Children's Hospital Health Plan
Assurance of Adequate PCP Access and
CapacityHow will the Plan no if the cumulative Medicaid Linkages have approached or exceeded 2,500 for all CCNs?
Aetna Better Health, Inc.
Assurance of Adequate PCP Access and
CapacityIt appears Internal Medicine is missing from the first bullet under 7.6.2. Please confirm if this should be included.
AmeriHealth Mercy of Louisiana
Assurance of Adequate PCP Access and
Capacity
Will DHH agree notification to the Enrollment Broker would occur within 7 days of the CCN becoming aware of a provider who will not accept new patients?
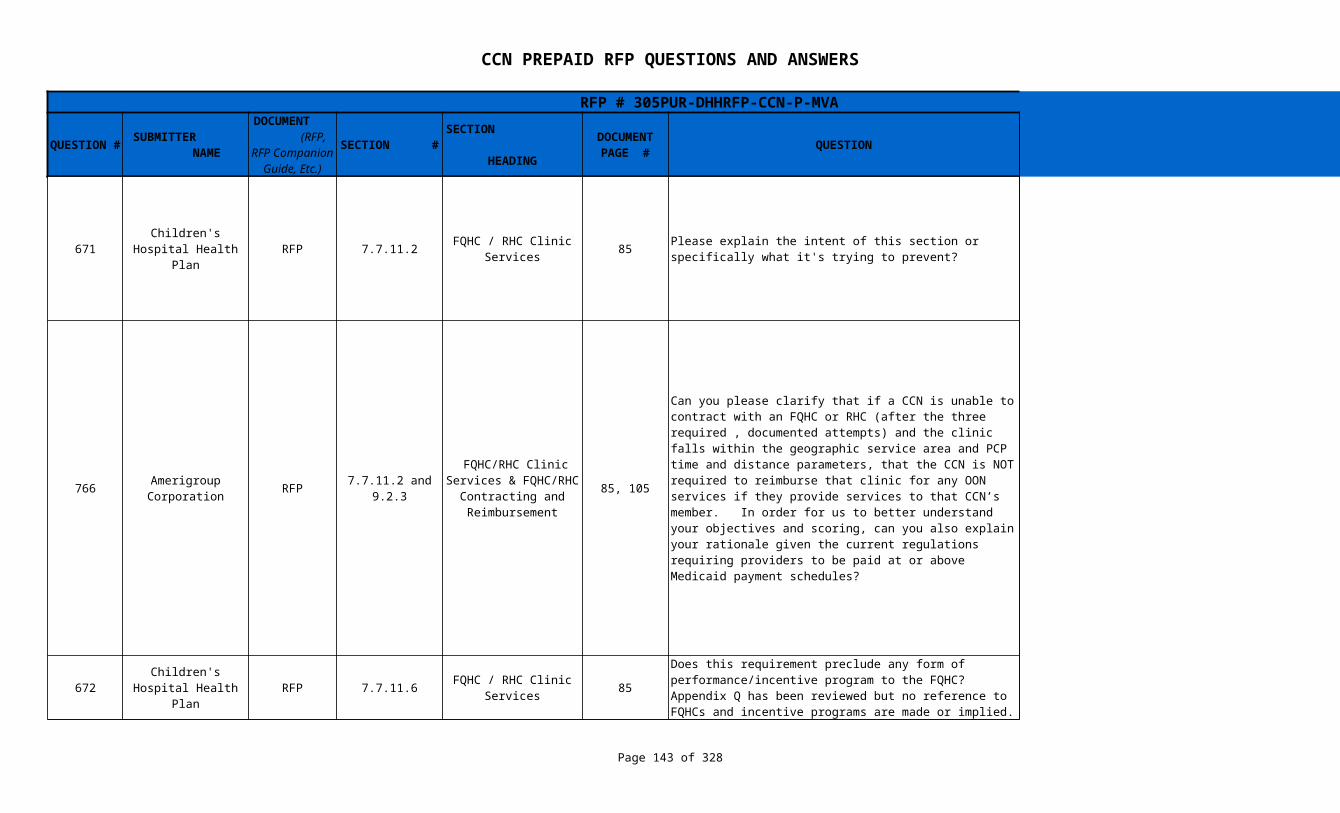
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 143 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
671 RFP 7.7.11.2 85
766 RFP 85, 105
672 RFP 7.7.11.6 85 No.
Children's Hospital Health Plan
FQHC / RHC Clinic Services
Please explain the intent of this section or specifically what it's trying to prevent?
The rationale is to comply with federal Medicaid regulations that state Medicaid managed care enrollees must have access to FQHC services. If an FQHC within time and distance standards to a member’s residence is a network provider in any CCN, then the Medicaid enrollee has access to FQHC services by enrolling in that CCN, and other CCNs are not required to pay for the FQHC services out of network.
Amerigroup Corporation
7.7.11.2 and 9.2.3
FQHC/RHC Clinic Services & FQHC/RHC
Contracting and Reimbursement
Can you please clarify that if a CCN is unable to contract with an FQHC or RHC (after the three required , documented attempts) and the clinic falls within the geographic service area and PCP time and distance parameters, that the CCN is NOT required to reimburse that clinic for any OON services if they provide services to that CCN’s member. In order for us to better understand your objectives and scoring, can you also explain your rationale given the current regulations requiring providers to be paid at or above Medicaid payment schedules?
The rationale is to comply with federal Medicaid regulations that require that Medicaid managed care enrollees have access to FQHC services. If a CCN has attempted to contract with an FQHC or RHC as required per the RFP, the CCN shall notify DHH that efforts to have the FQHC participate as a network provider have been unsuccessful and the reason(s) that the FQHC refuses to contract. DHH will review and make a determination, based on the the adequacy of the plan's network in the geographic service area and based on the availability of in-network FQHC services through another CCN participating in the same service area, as to whether or not the CCN must reimburse that clinic for any out-of-network services provided to that CCN's member. If the CCN made the required efforts to contract with the FQHC, has an adequate provider network in the absence of that FQHC's participation, and in-network FQHC services are available through another CCN, then the CCN will not be required to pay for the FQHC services out of network.
Children's Hospital Health Plan
FQHC / RHC Clinic Services
Does this requirement preclude any form of performance/incentive program to the FQHC? Appendix Q has been reviewed but no reference to FQHCs and incentive programs are made or implied.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 144 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
673 RFP 7.7.12 School-based Clinics 85
708 RFP 7.7.14 86
674 RFP 7.7.14 86
340 RFP 86 Refer to Section 7.7.14.2
770 RFP 7.7.14.2 86
339 RFP 7.7.14.2 86
129 WellCare RFP 7.7.2.2 PCP Responsibilities 78 The language will be amended to reference 6.33.
Children's Hospital Health Plan
This paragraph requires the CCN to offer a contract to all SBHC's. In our experience, these clinics cannot meet the requirements of a PCP, but may be able to provide other care coordination services. Are CCN's allowed to require SBHC's to notify the member's PCP of all services provided? Are CCN's required to pay SBHC's without regard to prior authorization requirements?
CCNs are allowed to require contract SBHCs to notify the member's PCP of all services provided. CCNs are not required to pay SBHCs without regard to prior authorization requirements.
Aetna Better Health, Inc.
Significant Traditional Providers
This section references: PCPs (as defined in Section 7.4.1.2) Please provide a reference in the RFP to this section. (7.4.1.2. or equivalent)
The language will be amended to reference Sections 7.6.1 and 7.6.2 and the Primary Care Provider (PCP) definition in the Glossary section of the RFP.
Children's Hospital Health Plan
Significant Traditional Providers
Please explain the overall intent of this section. Please explain why only two years under contract
The overall intent is to provider an opportunity for current Medicaid providers to participate in the CCN program. We believe that after two years, there will be sufficient performance on which to base the decision to continue to offer a contract.
AmeriHealth Mercy of Louisiana
7.7.14 and Glossary
Significant Traditional Providers
Please identify the specific STPs comprising each provider type/class that the CCNs shall make good faith efforts to include in their network for the first 2 years of operation.
Amerigroup Corporation
Significant Traditional Providers
There is a reference to a Section 7.4.1.2; however, no such section exists in the RFP.
The language will be amended to reference Sections 7.6.1 and 7.6.2 and the Primary Care Provider (PCP) definition in the Glossary section of the RFP.
AmeriHealth Mercy of Louisiana
Significant Traditional Providers
The provision references Section 7.4.1.2 of the RFP; however, there is no such section. Please clarify this reference.
The language will be amended to reference Sections 7.6.1 and 7.6.2 and the Primary Care Provider (PCP) definition in the Glossary section of the RFP.
The 4th bullet references the PCP to "coordinate case management services" including "screening and assessment, development of plan of care…and other responsibilities defined in 6.32." Should the reference be to 6.33 (Case Management) instead of 6.32 (Care Transition)?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 145 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
765 RFP 7.7.3.3 80
130 WellCare RFP 7.7.3.3 80
706 RFP 7.7.3.3 81 The bullet will be removed from the RFP.
707 RFP 7.7.3.3 80-81
336 RFP 7.7.5.3 Access to Hospitals 82
743 Advocacy Center RFP 7.7.5.3 Access to Hospitals 83
Amerigroup Corporation
Access to Specialty Providers
The sections indicate covered services include “Chiropractic” as a covered service. In discussions with some state chiropractors, they have indicated that LA Medicaid previously reimbursed for these services but no longer do unless there is proof of medical necessity. Can you please confirm that this is a covered benefit and is reimbursable under current LA Medicaid?
Chiropractic services is covered under LA Medicaid for children under age 21 only. Please see question #577.
Access Standards and Guidelines
This section includes geriatric medicine within the subsection of required internal medicine providers and requires specialists to be within 60 minutes of 75% of members and 90 minutes of all members. Does the provider need to be board certified in geriatric medicine?
DHH desires and encourages the use of Board Certified / Board Eligible providers within the network whenever possible. However, individuals with specialized training within a particular field of medicine and who have privileges to provide that level of care may substitute for Board Certified providers if needed. Documentation of the specialized training and privileges to practice must be made available to DHH upon request.
Aetna Better Health, Inc.
Access to Specialty Providers
Please clarify the providers that would fall under the area of Medical Services as described in the third bullet from the bottom of this list.
Aetna Better Health, Inc.
Access to Specialty Providers
Please clarify the type of providers are as the Intensive Critical Care - Adolescent Medicine, Physical Medicine and Rehab, Psychiatry, Radiology and Respiratory/Pulmonary Specialty?
The RFP will be amended to make Adolescent Medicine, Physical Medicine and Rehab, Psychiatry, Radiology and Respiratory/Pulmonary Specialty closed bullets.
AmeriHealth Mercy of Louisiana
Section 7.7.5.3 indicates that the CCN may contract with out-of-state hospitals in the trade area. What does DHH consider the "trade area" to be?
Trade area is defined as counties in bordering states adjacent to Louisiana.
The RFP provides that "The CCN may contract with out-of-state hospitals in the trade area." Is this meant to imply that the CCN may not in addition contract with providers outside of the trade area (e.g. M.D. Anderson Hospital in Houston when appropriate for cancer care)?
No, it is not meant to preclude contracting with out of state hospitals outside the trade area.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 146 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
744 Advocacy Center RFP 7.7.5.3 Access to Hospitals 83
745 Advocacy Center RFP 7.7.5.3 Access to Hospitals 83
675 RFP 7.7.5.3 Access to Hospitals 83 What does in the “trade” area mean?
337 RFP 7.7.7 83
769 RFP 7.7.8.2 Prenatal Care Services 84 The language will be amended to reference Section 7.5.4.
338 RFP 7.7.8.2 Prenatal Care Services 84 The language will be amended to reference Section 7.5.4.
The RFP provides that "The CCN may contract with out-of-state hospitals in the trade area." Is this meant to imply that the CCN may not in addition contract with providers outside of the trade area, regardless of the fact that it believes another hospital could provide superior care or that such care would be cost effective for the recipient, and the CCN will cover all associated costs (such as transportation)?
No, it is not meant to preclude contracting with providers outside the trade area.
If the department's intent is to prevent contracting with out of state hospitals in the circumstances described in the previous two questions, will the Department cover the plans' costs if there is litigation on the issue, given the recent appellate court ruling that Louisiana's Medicaid program cannot discriminate against out of state hospitals?
It is not DHH"s intent to prevent contracting with out of state hospitals. The reference to out of state hospitals in the trade area is that they can be contracted with to meet the network adequacy requirement.
Children's Hospital Health Plan
The trade area refers to community standards for where health care is received by the general public residing in an area, including hospitals that are out of state.
AmeriHealth Mercy of Louisiana
Direct Access to Women's Health Care
Please confirm that the CCN is not required to provide family planning services if it objects to the provision of such services on the basis of moral or religious grounds. If the CCN elects not to provide, reimburse for, or provide coverage for family planning services because of an objection on moral or religious grounds, what is the mechanism for members to access such benefits?
Please see Section 2.4 and 12.12.2.10
Amerigroup Corporation
There is a reference to a Section 7.3.4.4; Please confirm the correct reference should be 7.5.4
AmeriHealth Mercy of Louisiana
The provision references Section 7.3.4.4 of the RFP; however, there is no such section. Please clarify this reference.
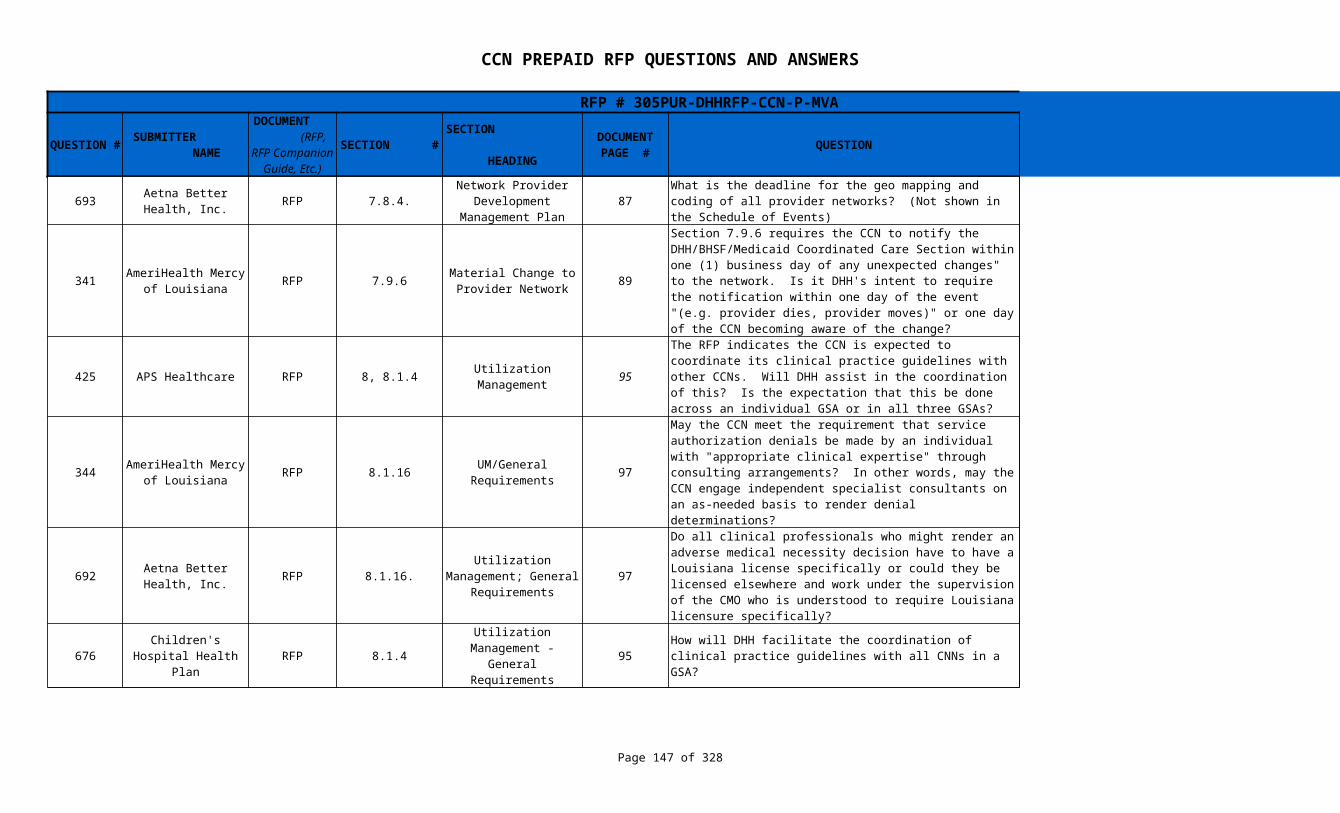
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 147 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
693 RFP 7.8.4. 87
341 RFP 7.9.6 89
425 APS Healthcare RFP 8, 8.1.4 95
344 RFP 8.1.16 97
692 RFP 8.1.16. 97
676 RFP 8.1.4 95 Through the EQRO , the Quality Committee and/or LHCQF.
Aetna Better Health, Inc.
Network Provider Development
Management PlanWhat is the deadline for the geo mapping and coding of all provider networks? (Not shown in the Schedule of Events)
Geo mapping is due with the GSA Network Adequacy Documentation Deadline within the Schedule of Events.
AmeriHealth Mercy of Louisiana
Material Change to Provider Network
Section 7.9.6 requires the CCN to notify the DHH/BHSF/Medicaid Coordinated Care Section within one (1) business day of any unexpected changes" to the network. Is it DHH's intent to require the notification within one day of the event "(e.g. provider dies, provider moves)" or one day of the CCN becoming aware of the change?
The CCN is required to notify DHH within one day after becoming aware of the change.
Utilization Management
The RFP indicates the CCN is expected to coordinate its clinical practice guidelines with other CCNs. Will DHH assist in the coordination of this? Is the expectation that this be done across an individual GSA or in all three GSAs?
The Quality Committee , LHCQF and/or the EQRO will assist the CCN in coordinating clinical practice guidelines with other CCNs. It is expected to be done across all GSAs.
AmeriHealth Mercy of Louisiana
UM/General Requirements
May the CCN meet the requirement that service authorization denials be made by an individual with "appropriate clinical expertise" through consulting arrangements? In other words, may the CCN engage independent specialist consultants on an as-needed basis to render denial determinations?
The CCN must provide written follow-up to the provider for all approved service authorizations. Documented confirmation is required for extended stay or additional services within two (2) business days. Members who are an inpatient in a facility must be notified within one (1) business day of an approval extension by the CCN, facility or provider.
Aetna Better Health, Inc.
Utilization Management; General
Requirements
Do all clinical professionals who might render an adverse medical necessity decision have to have a Louisiana license specifically or could they be licensed elsewhere and work under the supervision of the CMO who is understood to require Louisiana licensure specifically?
All clinical professionals who might render an adverse medical necessity decision may have a license outside of Louisiana if they are working under the supervision of the CMO that has a Louisiana License.
Children's Hospital Health Plan
Utilization Management - General
RequirementsHow will DHH facilitate the coordination of clinical practice guidelines with all CNNs in a GSA?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 148 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
691 RFP 8.1.4. 95
746 Advocacy Center RFP 8.1.7.4 96
210 HMO Louisiana, Inc. RFP 99
345 RFP 8.5.1.3 Post Authorization 101
Aetna Better Health, Inc.
Utilization Management; General
Requirements
Would the state consider another entity (eg., LaHQF) to help coordinate the development of uniform clinical practice guidelines between CCNs? Would the state consider transitioning to this type of approach as a part of the first renewal? How would the state propose we build in the single source of practice guidelines into our rates?
The Quality Committee , LHCQF and/or the EQRO will assist the CCN in coordinating clinical practice guidelines with other CCNs. DHH encourages cooperation among CCNs to adopt uniform best practice guidelines. Each CCN has flexibility in rate determination. Building in the single source of practice guidelines into rates is left up to each entity.
Utilization Management
The proposer must identify their medical personnel if utilization management decisions will be based on their experience rather than strictly on third party criteria or guidelines. The Notice of Intent requires that those deciding grievances and appeals "were not involved in any previous level of review or decision-making; and... have the appropriate clinical expertise, as determined by the department, in treating the member's condition or disease" (§3727.A.3.). Where do the plans identify the existence of these other, independent personnel, so that the department can determine their appropriateness?
Section 8.1.1 requires the CCN submit their UM polices and procedures to DHH for Written approval within thirty (30) days from the date the Contract is signed, annually thereafter, and prior to any revisions.
8.2.2.9 through 8.2.3
Utilization Management
Committee
Medical records site review. When is the CCN expected to start these site reviews? Can only the providers new to Medicaid have a site review within the first year and all current providers be placed on a 2 year cycle? Could one CCN do the site reviews per GSA since the providers would have to be reviewed by each CCN that they are contracted with?
The CCN shall review each site at least one (1) time during each two (2) year period. It is the CCNs responsibility to develop procedures and protocols for the review process. Reciprocal agreements with other CCNs may be pursued; however, the CCN is fully responsible for the accuracy of the medical records for their network providers.
AmeriHealth Mercy of Louisiana
Please clarify if the extension of the 72 hour timeframe is in reference to the expedited service authorization timeframe in Section 8.5.1.2.1.
The 72 hour timeframe is in reference to the expedited service authorization.
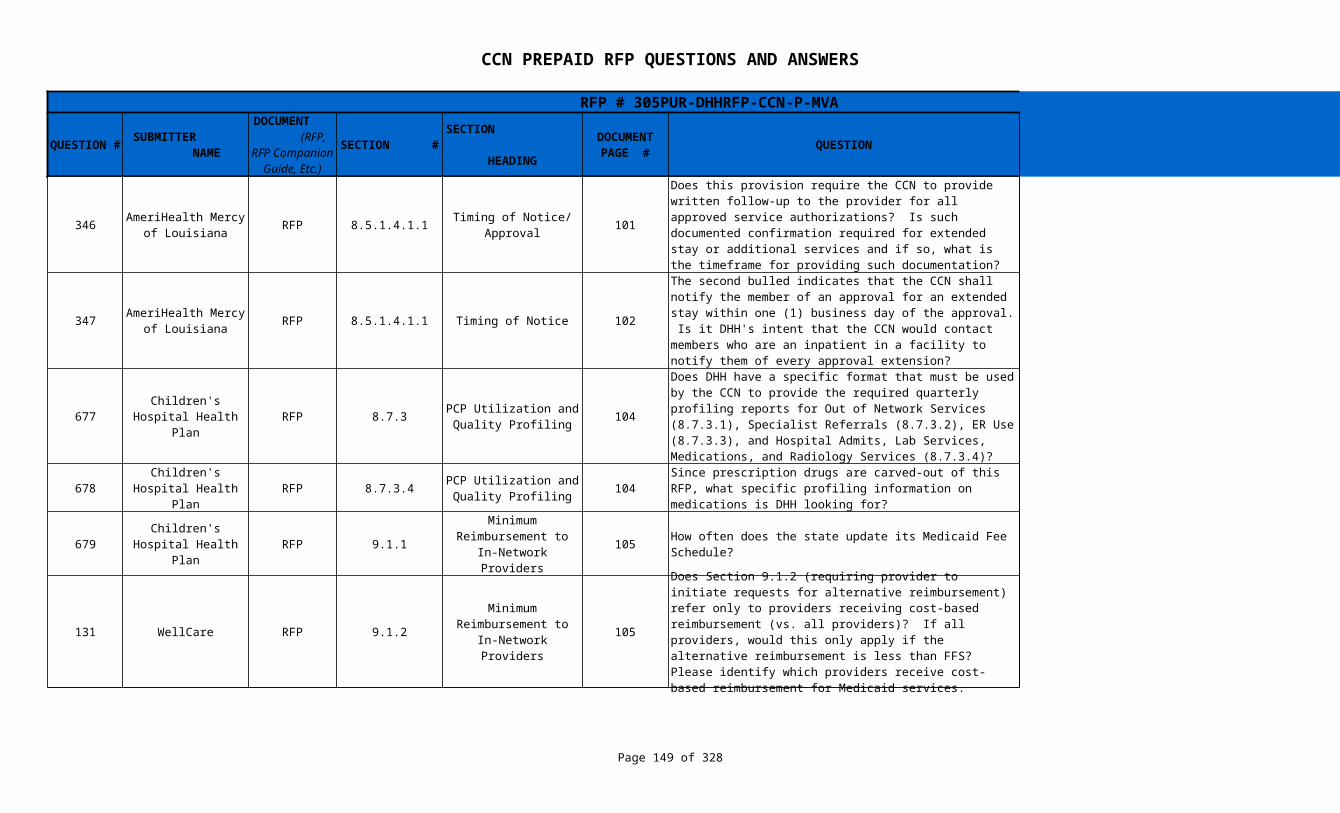
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 149 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
346 RFP 8.5.1.4.1.1 101
347 RFP 8.5.1.4.1.1 Timing of Notice 102 Yes
677 RFP 8.7.3 104
678 RFP 8.7.3.4 104
679 RFP 9.1.1 105 How often does the state update its Medicaid Fee Schedule?
131 WellCare RFP 9.1.2 105
AmeriHealth Mercy of Louisiana
Timing of Notice/ Approval
Does this provision require the CCN to provide written follow-up to the provider for all approved service authorizations? Is such documented confirmation required for extended stay or additional services and if so, what is the timeframe for providing such documentation?
The CCN must provide written follow-up to the provider for all approved service authorizations. Documented confirmation is required for extended stay or additional services within two (2) business days.
AmeriHealth Mercy of Louisiana
The second bulled indicates that the CCN shall notify the member of an approval for an extended stay within one (1) business day of the approval. Is it DHH's intent that the CCN would contact members who are an inpatient in a facility to notify them of every approval extension?
Children's Hospital Health Plan
PCP Utilization and Quality Profiling
Does DHH have a specific format that must be used by the CCN to provide the required quarterly profiling reports for Out of Network Services (8.7.3.1), Specialist Referrals (8.7.3.2), ER Use (8.7.3.3), and Hospital Admits, Lab Services, Medications, and Radiology Services (8.7.3.4)?
Not at this time. Proposers are encouraged to submit samples of existing reports with their proposals for consideration by DHH.
Children's Hospital Health Plan
PCP Utilization and Quality Profiling
Since prescription drugs are carved-out of this RFP, what specific profiling information on medications is DHH looking for?
DHH is looking for the over and under utilization of medication. This data may be obtained from the weekly pharmacy data updates.
Children's Hospital Health Plan
Minimum Reimbursement to In-
Network Providers
When fees change. Rates may be increased or reduced by either DHH or through legislative statute. Some fees are based on Medicare rates and adjusted accordingly
Minimum Reimbursement to In-
Network Providers
Does Section 9.1.2 (requiring provider to initiate requests for alternative reimbursement) refer only to providers receiving cost-based reimbursement (vs. all providers)? If all providers, would this only apply if the alternative reimbursement is less than FFS? Please identify which providers receive cost-based reimbursement for Medicaid services.
It is applicable to all providers and is applicable to any differences in reimbursement methodologies and reimbursement rates that are less than would be payable under Medicaid fee for service.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 150 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
349 RFP 9.2.7 106 Section 9.2.7 is referencing Section 9.2.6
747 Advocacy Center RFP 9.3.1 106
748 Advocacy Center RFP 9.3.1 106
350 RFP 9.3.1 106 No
78 RFP 9.3.1 106
AmeriHealth Mercy of Louisiana
FQHC/RHC Contracting & Reimbursement
What "rights" is DHH referring to, under the requirement to "inform members of these rights"?
Reimbursement to Out-of-Network
providers
The RFP specifies rates to be paid to out of network providers. 42 C.F.R. § 431.52 specifies conditions under which the state Medicaid program must pay for out of state care. Is the CCN-P responsible for covering the cost out of state care that meets the conditions of 42 C.F.R. § 431.52?
Yes, the CCN-P is responsible for covering the cost of health care under §431.52 (b) (1) through (2). The CCN will make the determination required in §431.52(b)(3). §431.52(b)(4) is only applicable if the provider is within the CCN's provider network or as approved by the CCN if out-of-network provider.
Reimbursement to Out-of-Network
providers
The RFP specifies rates to be paid to out of network providers. For what non-emergency situations is the CCN-P required to cover the cost of care received out of plan, and outside of a GSA served by the plan, if the care was received within the state of Louisiana?
Core benefits and services for which the CCN does not have an in-network provider within the GSA
AmeriHealth Mercy of Louisiana
Reimbursement to Out-of-Network
Providers
Reimbursement for OON Providers - On page 280, DHH states this starts after the contract Award which is very close to the Readiness Review and Go Live dates for Phase A. Would DHH account for any attempts made prior to the Contract Award?
Coventry Health Care of Louisiana,
Inc.
Reimbursement to Out-of-Network
Providers
How will this be enforced against out-of-network providers if they refuse to accept 90% of Medicaid FFS rate and the out-of-network provider brings suit against the member or CCN for payment of billed charges, or amount greater than 90% of Medicaid FFS.
An out of network provider has the right to refuse to provide non-emergency services. If the CCN must refer or make otherwise make arrangements for a member to receive services through an out-of-network provider because a qualified provider is not available within the network, the CCN must ensure that the member is not "balanced-billed" or does not otherwise incur out-of-pocket costs since the member would not incur a cost had the service been provided by an in-network provider. In this case, the member cannot be charged for any difference between the out-of-network payment and the FFS amount.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 151 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
79 RFP 9.3.1 106
275 RFP 9.5.2 107
276 RFP 9.5.7 107 Refer to definition of Clean Claim in Glossary
Coventry Health Care of Louisiana,
Inc.
Reimbursement to Out-of-Network
Providers
This section states CCN is not required to pay more than 90% of the Medicaid FFS rate to an out of network provider if we have made three documented attempts to contract. Are out of network providers required to hold the member harmless for the balance due?
If the CCN must refer or make otherwise make arrangements for a member to receive services through an out-of-network provider because a qualified provider is not available within the network, the CCN must ensure that the member is not "balanced-billed" or does not otherwise incur out-of-pocket costs since the member would not incur a cost had the service been provided by an in-network provider. In this case, the member cannot be charged for any difference between the out-of-network payment and the FFS amount.
Louisiana Healthcare Connections
Claims Processing Requirements
Please confirm that the payment cycle may be moved to a different day if/when the regular payment day falls on a DHH/CCN holiday?
Payment will be made via EFT on the Tuesday nearest the 15 day of the month. If Tuesday is a holiday, the payment will be made the next working day . See Appendix # V for Monthly Payment Schedule through June, 2014.
Louisiana Healthcare Connections
Claims Processing Requirements
9.5.7. requires the CCN to suspend the claim if it is unclean and request the information needed to adjudicate the claim. It goes on to say that once the information is received the CCN must process the claim within 15 days of the receipt of the claim. Should this be within 15 days of receiving the information to make the claim clean? What if the CCN doesn't receive the information from the provider until after 15 days of receipt?
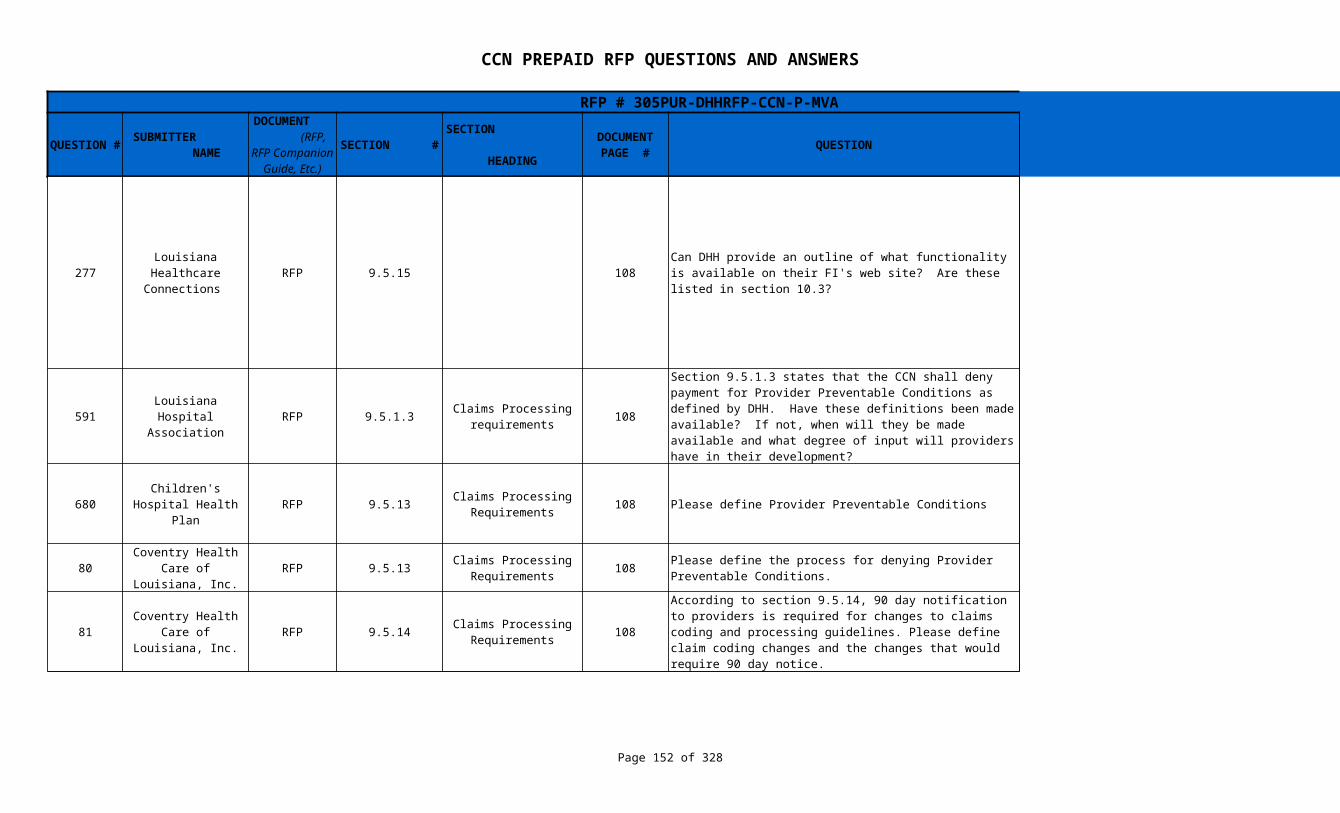
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 152 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
277 RFP 9.5.15 108
591 RFP 9.5.1.3 108
680 RFP 9.5.13 108 Please define Provider Preventable Conditions
80 RFP 9.5.13 108
81 RFP 9.5.14 108
Louisiana Healthcare Connections
Can DHH provide an outline of what functionality is available on their FI's web site? Are these listed in section 10.3?
FIs web functionality includes CCN Providers being able to use the assigned Medicaid provider ID to register on the LMMIS provider website, these providers will be able to access protected provider applications such as MEVs, an 820 file download, a web application which allows initial and weekly claims history file download, a web application that permits CCNs to upload their provider registry and download registry update, a web application which allows CCNs to single-entry of TPL information, encounter remittance file downloads, etc. These are not the same as Section 10.3.
Louisiana Hospital Association
Claims Processing requirements
Section 9.5.1.3 states that the CCN shall deny payment for Provider Preventable Conditions as defined by DHH. Have these definitions been made available? If not, when will they be made available and what degree of input will providers have in their development?
DHH has not yet established policy for Louisiana Medicaid relative to Provider Preventable Conditions as defined in in the February 2011 Federal Register. DHH will utilize the Administrative Rulemaking process which provides an opportunity for provider input.
Children's Hospital Health Plan
Claims Processing Requirements
Refer to the proposed rule published in the Federal Register/Vol. 76, No. 33 /Thursday, February 17, 2011, page 9288 http://edocket.access.gpo.gov/2011/pdf/2011-3548.pdf
Coventry Health Care of Louisiana,
Inc.Claims Processing
RequirementsPlease define the process for denying Provider Preventable Conditions.
DHH is currently in the process of developing PPC policy for its fee-for-service Medicaid program
Coventry Health Care of Louisiana,
Inc.Claims Processing
Requirements
According to section 9.5.14, 90 day notification to providers is required for changes to claims coding and processing guidelines. Please define claim coding changes and the changes that would require 90 day notice.
Examples are:(1) changes to claims payment processing schedules;(2) changes to procedure formulary(ies);(3) changes to provider claims submission guidelines;(4) changes to other claims payment methodologies.
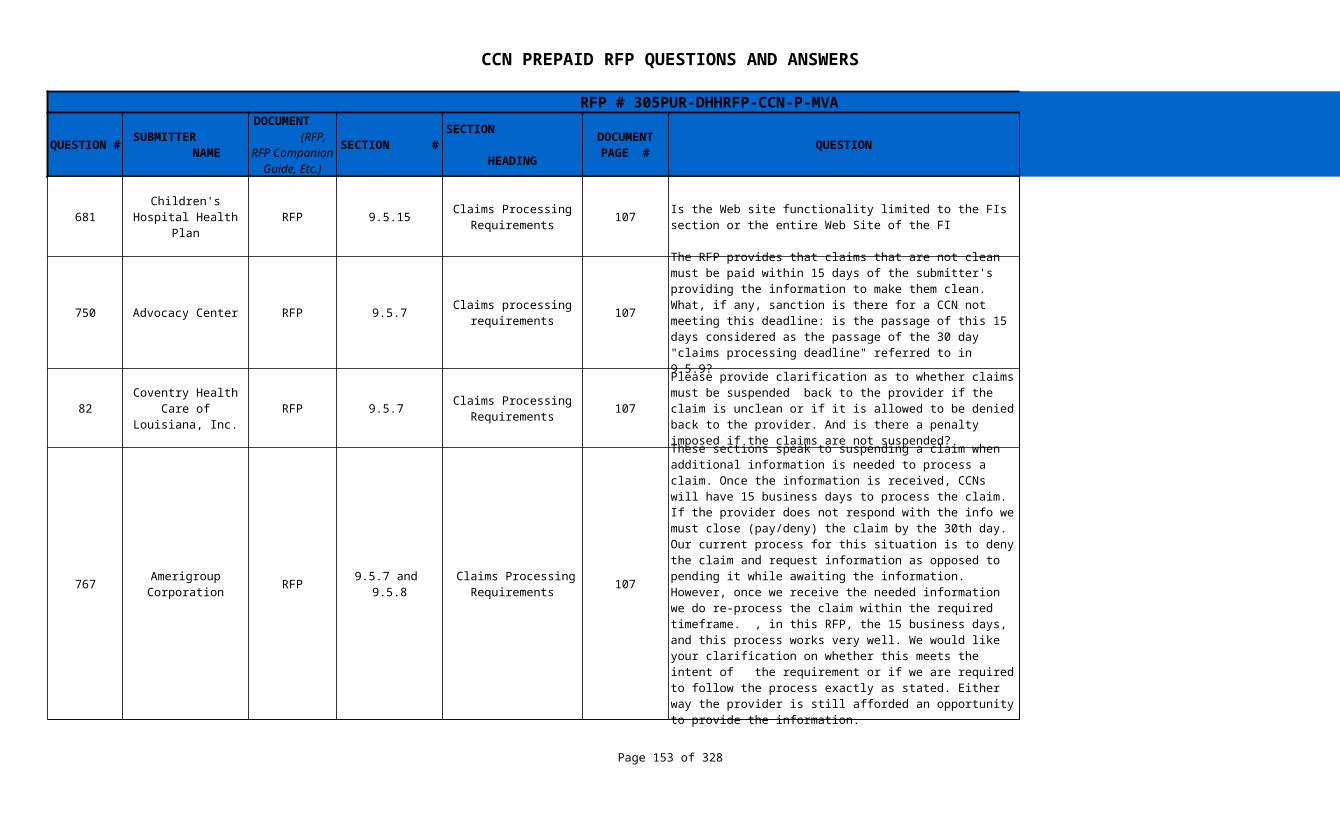
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 153 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
681 RFP 9.5.15 107
750 Advocacy Center RFP 9.5.7 107 Language in Sections 9.5.7 is being amended
82 RFP 9.5.7 107 See response to Question # 750
767 RFP 107 See response to Questions # 749 and # 750
Children's Hospital Health Plan
Claims Processing Requirements
Is the Web site functionality limited to the FIs section or the entire Web Site of the FI
FI web services that should be replicated/enhanced on the CCNs web site are:(1) Provider access to member enrollment with the CCN, including identification of PCP.(2) claims status inquiry.
Claims processing requirements
The RFP provides that claims that are not clean must be paid within 15 days of the submitter's providing the information to make them clean. What, if any, sanction is there for a CCN not meeting this deadline: is the passage of this 15 days considered as the passage of the 30 day "claims processing deadline" referred to in 9.5.9?
Coventry Health Care of Louisiana,
Inc.Claims Processing
Requirements
Please provide clarification as to whether claims must be suspended back to the provider if the claim is unclean or if it is allowed to be denied back to the provider. And is there a penalty imposed if the claims are not suspended?
Amerigroup Corporation
9.5.7 and 9.5.8
Claims Processing Requirements
These sections speak to suspending a claim when additional information is needed to process a claim. Once the information is received, CCNs will have 15 business days to process the claim. If the provider does not respond with the info we must close (pay/deny) the claim by the 30th day. Our current process for this situation is to deny the claim and request information as opposed to pending it while awaiting the information. However, once we receive the needed information we do re-process the claim within the required timeframe. , in this RFP, the 15 business days, and this process works very well. We would like your clarification on whether this meets the intent of the requirement or if we are required to follow the process exactly as stated. Either way the provider is still afforded an opportunity to provide the information.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 154 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
749 Advocacy Center RFP 9.5.8 107 Language in Sections 9.5.8 is being amended
83 RFP 9.5.8 107 See response to Question # 749
751 Advocacy Center RFP 9.5.9
592 RFP 9.7.1.5 109
593 RFP 9.7.1.6. 109
682 RFP 9.8.2.1 111
510 WellPoint RFP N/A - Is there any significant out-of-state utilization?
Claims Processing Requirements
The end of the requirement expressed in this provision seems to be missing some words. What is the correct text?
Coventry Health Care of Louisiana,
Inc.Claims Processing
RequirementsDo suspended/denied claims not closed within 30 days need to be reported to DHH?
Claims Processing Requirements
108; see also p. 230
The RFP requires that interest be paid on claims not "adjudicated" (which is defined as denied or paid) by the 30 day "claims processing deadline". Does the interest run on all clean claims not adjudicated within 30 days of submission of a clean claim?
Yes, there will be interest applied to all clean claims not adjudicated within 30 days of receipt.
Louisiana Hospital Association
Payment for Emergency Services
and Post-Stabilization Services
Section 9.7.1.3 states that the CCN may require, as a condition of payment, notification by the provider of emergency services while Section 9.7.1.2 states that the CCN may not refuse to cover emergency services based on lack of notification. Can DHH clarify this discrepancy?
The language in the referenced sections has been amended. The CCN may enter into contracts with providers or facilities that require, as a condition of payment for emergency services, notification to the PCP or other designated contact within 10 business days of the emergency room visit. The policy for non-payment must be addressed in their Provider Manual
Louisiana Hospital Association
Payment for Emergency Services
and Post-Stabilization Services
This section states that a CCN is financially responsible and shall deny not emergency medical transportation because the condition was subsequently determined to be non-emergent. While appropriate language, why were all providers of emergency services not included in this section? Exclusion of any providers of emergency services would appear to violate the spirit of the prudent layperson standard.
The RFP language has been amended to state "the CCN shall be financially responsible for emergency medical services, including transportation, and shall not retroactively deny a claim for emergency services, including transportation, to an emergency provider because the condition, which appeared to be an Emergency Medical Condition under the prudent layperson standard, was subsequently determined to be non-emergency in nature."
Children's Hospital Health Plan
Physician Incentive Plans
This section suggests that capitation is a form of provider incentive payment. Is that interpretation accurate?
This reference is to provider sub-capitation which may or may not be an incentive arrangement
Out of state utilization can be evaluated using the Medicaid Provider Listing and sorting providers by Region and identifying Out of State Providers (both in and out of trade area)

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 155 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
760 Advocacy Center RFP N/A 296
759 Advocacy Center RFP N/A
401 RFP N/A N/A N/A
Glossary - Significant Traditional Providers
The RFP defines "Significant Traditional Providers" with whom plans are expected to contract as "Those Medicaid enrolled providers that provided the top eighty percent (80%) of Medicaid services for the CCN-eligible population in the base year of 2010." Lists of these providers do not seem to be posted on the Department's website. When will these listings be available for plans' inspection?
The total dollars paid in SFY 11 has been added to the Provider Listing in the Procurement Library
Glossary - Durable Medical Equipment,
Prosthetics, Orthotics and certain Supplies
280; see also pages 55-56
The RFP specifies that plans are to cover "Durable Medical Equipment, Prosthetics, Orthotics and certain Supplies" and specifies only that "POS is inclusive of prosthetics, orthotics and certain supplies. Certain supplies are those medical supplies that are of an expendable nature, such as catheters and diapers." The term "medical supplies" is very ambiguous, ranging from items FDA approved, items with solely medical applications, items primarily used in medical applications, and items useful primarily for other purposes (such as the equipment in some augmentative communication devices). Is there a listing available for plans (for instance HCPC or other listings) showing the breadth and limitations on the supplies the Louisiana Medicaid program has covered and expects plans to cover?
Refer to the DME manual located online at www.lamedicaid.com as a reference; however for under 21 we must considered all request to establish medical necessity for the supply/equipment. The fee schedule that is located on the Medicaid website is another listing that may be viewed for items that are considered covered.
AmeriHealth Mercy of Louisiana
Is the bidder required to respond only to the queries/requirements enumerated in Appendix KK – CCN-P Proposal Submission and Evaluation Requirements? Given the above definitions of “must,, “is required,” “shall” and “will,” is the bidder required to respond to all statements appearing throughout Sections 2.0 to 20.0 of the RFP that contain these terms even if these requirements are not specified or referenced in Appendix KK – CCN-P Proposal Submission and Evaluation Requirements?
The bidder is not required to respond to all statements appearing throughout Section 2.0 to 20.0 that contain the terms "must", "is required" "shall" and "will" unless it is addressed in a specific question in Appendix KK.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 156 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
199 HMO Louisiana, Inc. RFP N/A N/A N/A
200 HMO Louisiana, Inc. RFP N/A N/A N/A NPI numbers
428 RFP 1.9 Schedule of Events 9 When will the first daily and monthly 834 files be sent?
135 WellCare RFP 11.8 Open Enrollment 121
449 RFP 21.21 253
133 WellCare RFP 10.1.3 Provider Relations 112 Yes
136 WellCare RFP 11.11.1.1 PCP Auto-Assignment 124
Who's the current Mental Health Vendor and PBM for Medicaid?Will they provide us with claims data thru the State and how often?
Louisiana Medicaid does not have a mental health vendor or PBM. DHH will provide claims data weekly for Medicaid services that continue to be provided through the FFS program
Will Providers use current Medicaid provider numbers, receive new provider numbers from DHH or the CCN, or use NPI numbers?
Coventry Health Care of Louisiana,
Inc.
The intent is to mail the initial choice letters 11/15/11 (assuming 1/1/12 "go live" date). The initial file would be sent 11/18 and then daily thereafter. The monthly file will be created on the third to last working day of the month.
Will the state migrate to an annual open enrollment period after program implementation for all 3 regions for a common open enrollment for all beneficiaries, or continue to hold rolling open enrollment by beneficiary specific eligibility period?
DHH intends to continue holding rolling open enrollment for CCN members and will not migrate to a single 60 day annual open enrollment period.
Coventry Health Care of Louisiana,
Inc.Notice of Contract
AwardsWill there be one contract for multiple GSA award or will a CCN receive one contract per GSA?
Each entity will enter into a single CCN-P Contract for all GSAs in which they are awarded a CCN-P contract.
Does "emergent provider issues" (to be handled 24/7) refer primarily to prior authorization requests and verifying enrollment of members with an emergent or urgent medical condition? If not, what else is contemplated?
This section says that the CCN will assign a PCP when the member doesn't make a selection after a "voluntary" selection of a CCN. It is expected that the CCN will also assign a PCP when a member who has been auto-assigned to the CCN does not select a PCP. Will the enrollment broker assign a PCP when the member is auto-assigned to a CCN and transmit that assignment to the selected CCN?
All PCP assignment will be by the CCN. If an individual indicates a PCP preference, that information will be transmitted by the Enrollment Broker to the CCN.
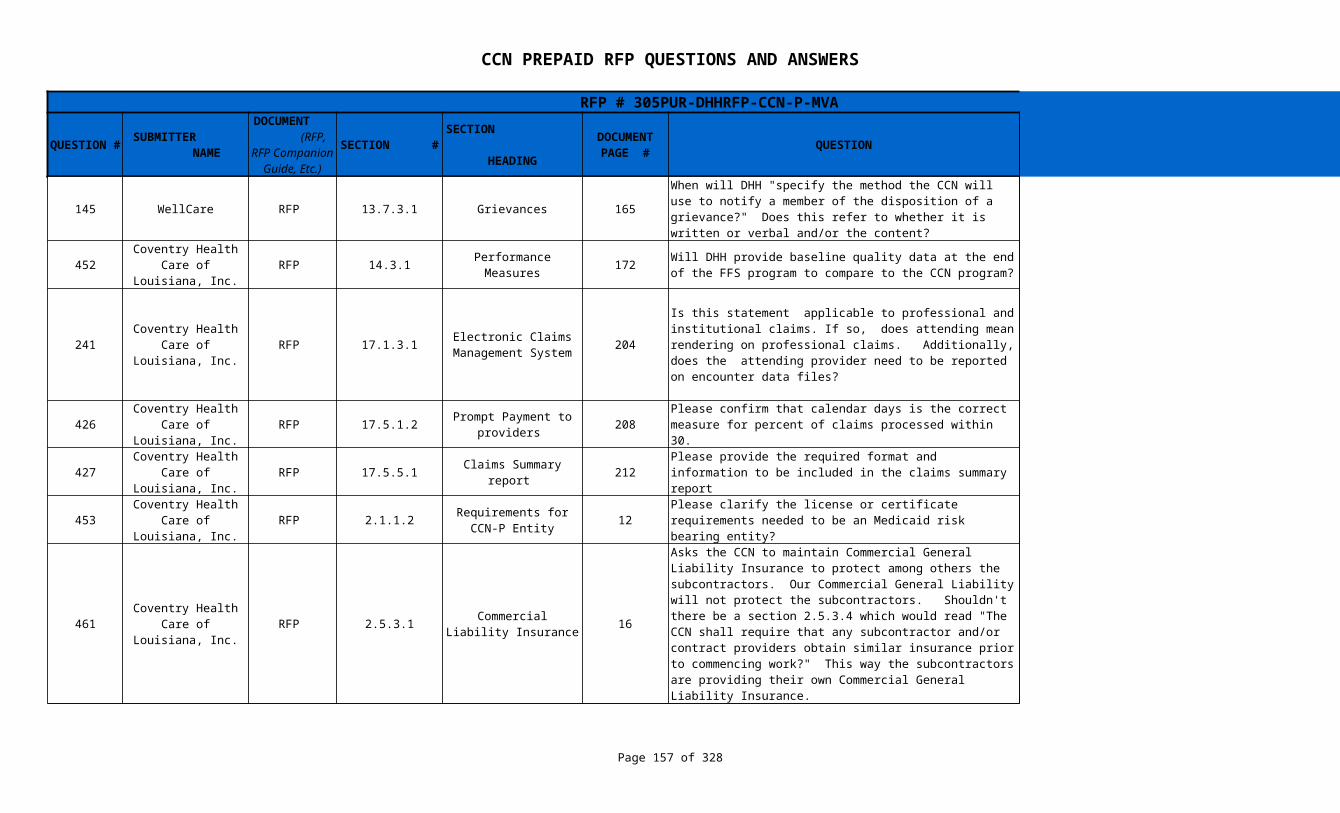
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 157 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
145 WellCare RFP 13.7.3.1 Grievances 165
452 RFP 14.3.1 Performance Measures 172
241 RFP 17.1.3.1 204
426 RFP 17.5.1.2 208 Correct
427 RFP 17.5.5.1 212 This will be provided once the Contracts have been awarded
453 RFP 2.1.1.2 12
461 RFP 2.5.3.1 16
When will DHH "specify the method the CCN will use to notify a member of the disposition of a grievance?" Does this refer to whether it is written or verbal and/or the content?
The CCN shall notify a member of the disposition of a grievance in writing.
Coventry Health Care of Louisiana,
Inc.Will DHH provide baseline quality data at the end of the FFS program to compare to the CCN program?
2009, 2010, and 2011 HEDIS Year quality data will be provided.
Coventry Health Care of Louisiana,
Inc.Electronic Claims
Management System
Is this statement applicable to professional and institutional claims. If so, does attending mean rendering on professional claims. Additionally, does the attending provider need to be reported on encounter data files?
The rendering or servicing provider must be submitted on encounter claims with the applicable NPI, taxonomy and zip+4. If the provider is not currently providing services on a FFS basis the CCN must submit the required provider registry information as described in the Systems Companion Guide.
Coventry Health Care of Louisiana,
Inc.Prompt Payment to
providers Please confirm that calendar days is the correct measure for percent of claims processed within 30.
Coventry Health Care of Louisiana,
Inc.Claims Summary report Please provide the required format and information to be
included in the claims summary report
Coventry Health Care of Louisiana,
Inc.Requirements for CCN-
P EntityPlease clarify the license or certificate requirements needed to be an Medicaid risk bearing entity?
This question should be directed to the Louisiana Department of Insurance.
Coventry Health Care of Louisiana,
Inc.Commercial Liability
Insurance
Asks the CCN to maintain Commercial General Liability Insurance to protect among others the subcontractors. Our Commercial General Liability will not protect the subcontractors. Shouldn't there be a section 2.5.3.4 which would read "The CCN shall require that any subcontractor and/or contract providers obtain similar insurance prior to commencing work?" This way the subcontractors are providing their own Commercial General Liability Insurance.
The Department will require the CCN to acquire and maintain the requested coverage.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 158 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
375 RFP 20.13.1.9 240
448 RFP 30 & 100 DHH does not believe it is a conflict
122 WellCare RFP 6.3.4.2 44
123 WellCare RFP 6.3.4.2 44
AmeriHealth Mercy of Louisiana
Misconduct for Which Intermediate Sanctions
May be Imposed
Please revise the provision as follows, "The CCN has failed to furnish any information reasonably requested by DHH regarding payments for provider goods or services provided pursuant to the Contract."
The language will remain as written since DHH does not intend to make unreasonable requests for information to the CCN.
Coventry Health Care of Louisiana,
Inc.4.1.7.1 and
8.5.1.1.1
Prior Authorization Staff
Standard Service Authorization
Is there a conflict between requiring prior auth staff to authorize healthcare 24/7 and making 80% of standard service authorization determinations within 2 business days? Should this be understood as requiring staff 24/7 but needing to make only 80% of all determinations within two business days?
Basic Behavioral Health Services
Please clarify what types of behavioral health services are included in "outpatient non-psychiatric hospital services" and the type of provider that would provide these services. Is this intended to refer to non-BH medical services?
a. Physical and medication stabilization and referral to either PCP or appropriate specialty BH services, as indicated. (Ex.#1- Patient not properly taking prescribed psychotropic meds may report to ER. Ex.#2 – Alcohol/drug OD reporting to ER. Ex.#3-Distraught patient with physical and/or emotional symptoms reporting to ER where “R/O clinical depression” is the diagnosis.)- ER Physician and /or social worker.b. Psychological or social work consultation for health and behavior assessment to identify psychological, behavioral, emotional, cognitive and social factors related to the prevention, treatment or management of physical health problems. CPT codes 96150-96155. (Ex.#1 Eval prior to stomach surgery to treat morbid obesity. Ex.#2 Counseling patient after heart surgery re: necessary lifestyle changes.) May or may not result in referral to specialty BH treatment.
Basic Behavioral Health Services
Please clarify the CCNs responsibility with respect to members "whose need for such services is secondary to a primary medical condition in any given episode of care."
See response to Question # 122. Such services would be physical health focused, rather than mental health focused.

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 159 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
124 WellCare RFP 6.3.4.2 44
128 WellCare RFP Care Transition Section 6.39 and Section 11.12.5 is being deleted.
Basic Behavioral Health Services
Please confirm CCN responsibility for any inpatient behavioral health services is restricted to detox only.
The CCN -P is responsible for all inpatient services where the enrollee does not have a primary diagnosis of behavioral health except as noted below for acute detoxification.
All costs for inpatient hospital admissions for Medicaid enrollees with a primary diagnosis of behavioral health are included in the behavioral health program except that the following services for Medicaid managed care enrollees in MCOs (e.g., CCN-P) will be excluded from the behavioral health program and included in the MCO prepaid rates: • Acute detoxification (Revenue codes of 116, 126, 136, 146, 156 as well as 202 and 204 with DT diagnoses to accommodate for Delirium Tremens (DT)), • Mental health services provided in a medical (physical health) Medicaid MCO Member's PCP or medical office (i.e., MD, DO, or RHC other than services provided by a psychiatrist), • Mental health services provided in a Federally Qualified Health Center, and • Emergency room services except services provided to members with primary codes of 290 through 319.
6.32, 6.39, and 11.12.5
63, 68, and 129
It appears that these sections repeat some, but not all, of the same care transition requirements. Please clarify whether/which requirements apply to transition between providers within a CCN's network and to transition from a CCN to another CCN or FFS.
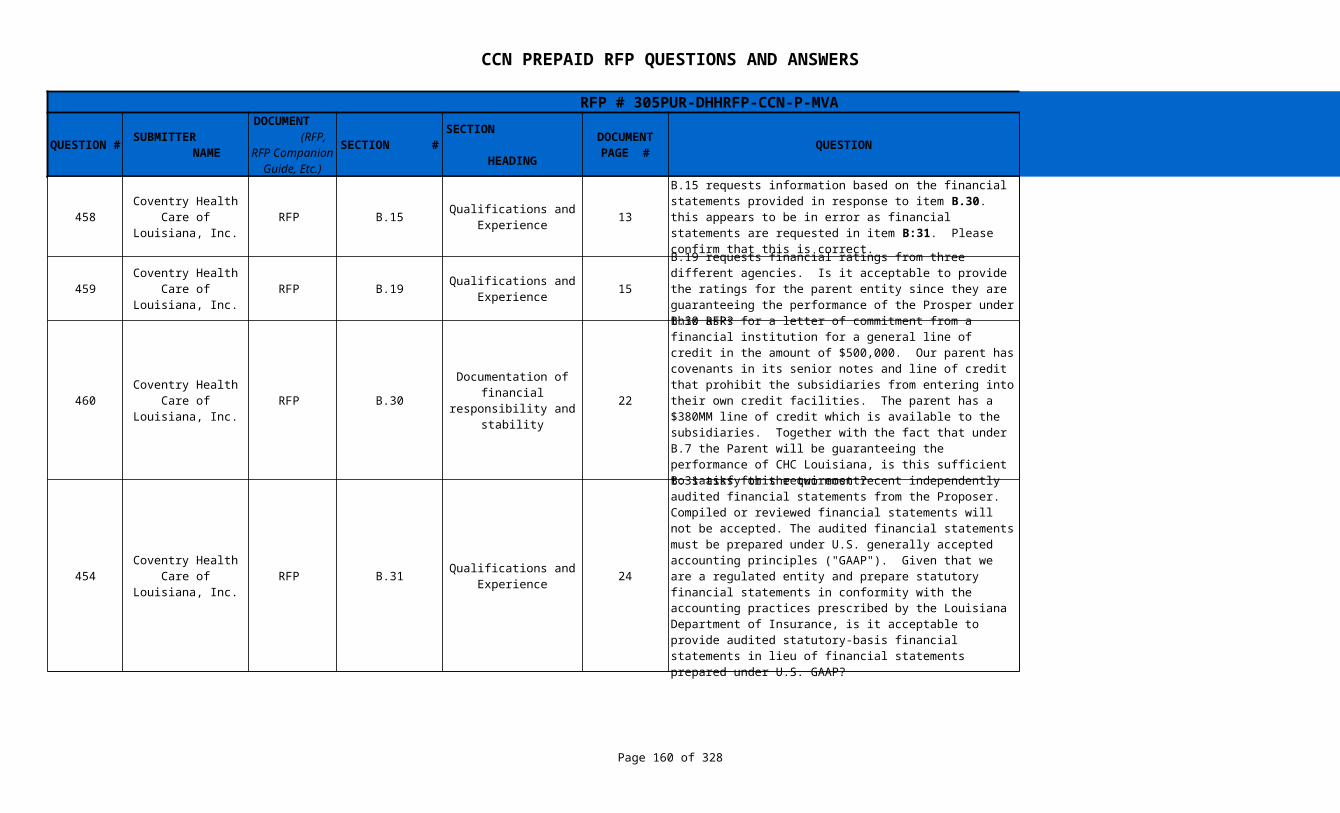
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 160 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
458 RFP B.15 13 The correct reference is B.31
459 RFP B.19 15
460 RFP B.30 22 Yes
454 RFP B.31 24 Yes
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.15 requests information based on the financial statements provided in response to item B.30. this appears to be in error as financial statements are requested in item B:31. Please confirm that this is correct.
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.19 requests financial ratings from three different agencies. Is it acceptable to provide the ratings for the parent entity since they are guaranteeing the performance of the Prosper under this RFP?
If the proposing entity has no entity, it may provide ratings for the parent entity.
Coventry Health Care of Louisiana,
Inc.
Documentation of financial responsibility
and stability
B.30 asks for a letter of commitment from a financial institution for a general line of credit in the amount of $500,000. Our parent has covenants in its senior notes and line of credit that prohibit the subsidiaries from entering into their own credit facilities. The parent has a $380MM line of credit which is available to the subsidiaries. Together with the fact that under B.7 the Parent will be guaranteeing the performance of CHC Louisiana, is this sufficient to satisfy this requirement?
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.31 asks for the two most recent independently audited financial statements from the Proposer. Compiled or reviewed financial statements will not be accepted. The audited financial statements must be prepared under U.S. generally accepted accounting principles ("GAAP"). Given that we are a regulated entity and prepare statutory financial statements in conformity with the accounting practices prescribed by the Louisiana Department of Insurance, is it acceptable to provide audited statutory-basis financial statements in lieu of financial statements prepared under U.S. GAAP?
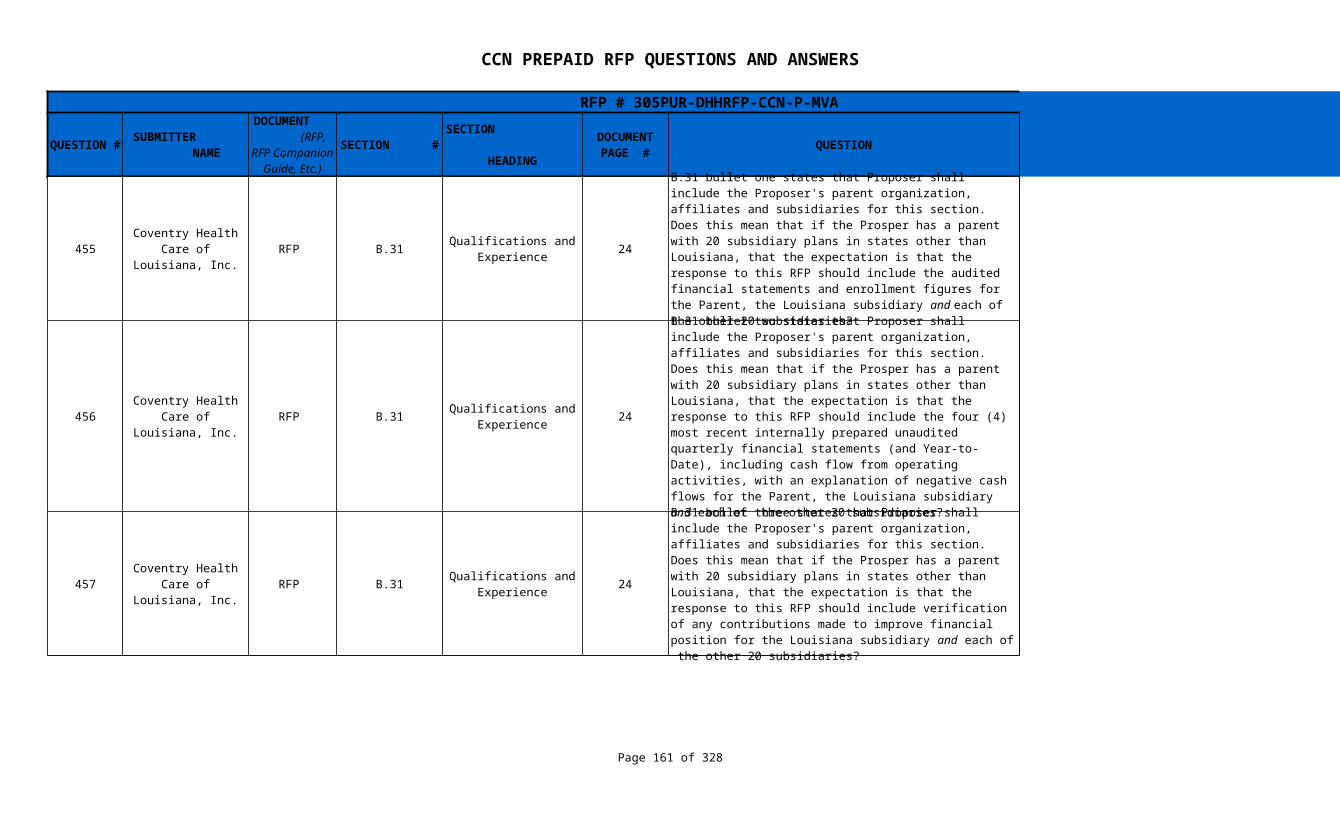
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 161 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
455 RFP B.31 24 This is being amended to exclude subsidiaries and affiliates.
456 RFP B.31 24 This is being amended to exclude subsidiaries and affiliates.
457 RFP B.31 24 This is being amended to exclude subsidiaries and affiliates.
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.31 bullet one states that Proposer shall include the Proposer's parent organization, affiliates and subsidiaries for this section. Does this mean that if the Prosper has a parent with 20 subsidiary plans in states other than Louisiana, that the expectation is that the response to this RFP should include the audited financial statements and enrollment figures for the Parent, the Louisiana subsidiary and each of the other 20 subsidiaries?
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.31 bullet two states that Proposer shall include the Proposer's parent organization, affiliates and subsidiaries for this section. Does this mean that if the Prosper has a parent with 20 subsidiary plans in states other than Louisiana, that the expectation is that the response to this RFP should include the four (4) most recent internally prepared unaudited quarterly financial statements (and Year-to-Date), including cash flow from operating activities, with an explanation of negative cash flows for the Parent, the Louisiana subsidiary and each of the other 20 subsidiaries?
Coventry Health Care of Louisiana,
Inc.Qualifications and
Experience
B.31 bullet three states that Proposer shall include the Proposer's parent organization, affiliates and subsidiaries for this section. Does this mean that if the Prosper has a parent with 20 subsidiary plans in states other than Louisiana, that the expectation is that the response to this RFP should include verification of any contributions made to improve financial position for the Louisiana subsidiary and each of the other 20 subsidiaries?
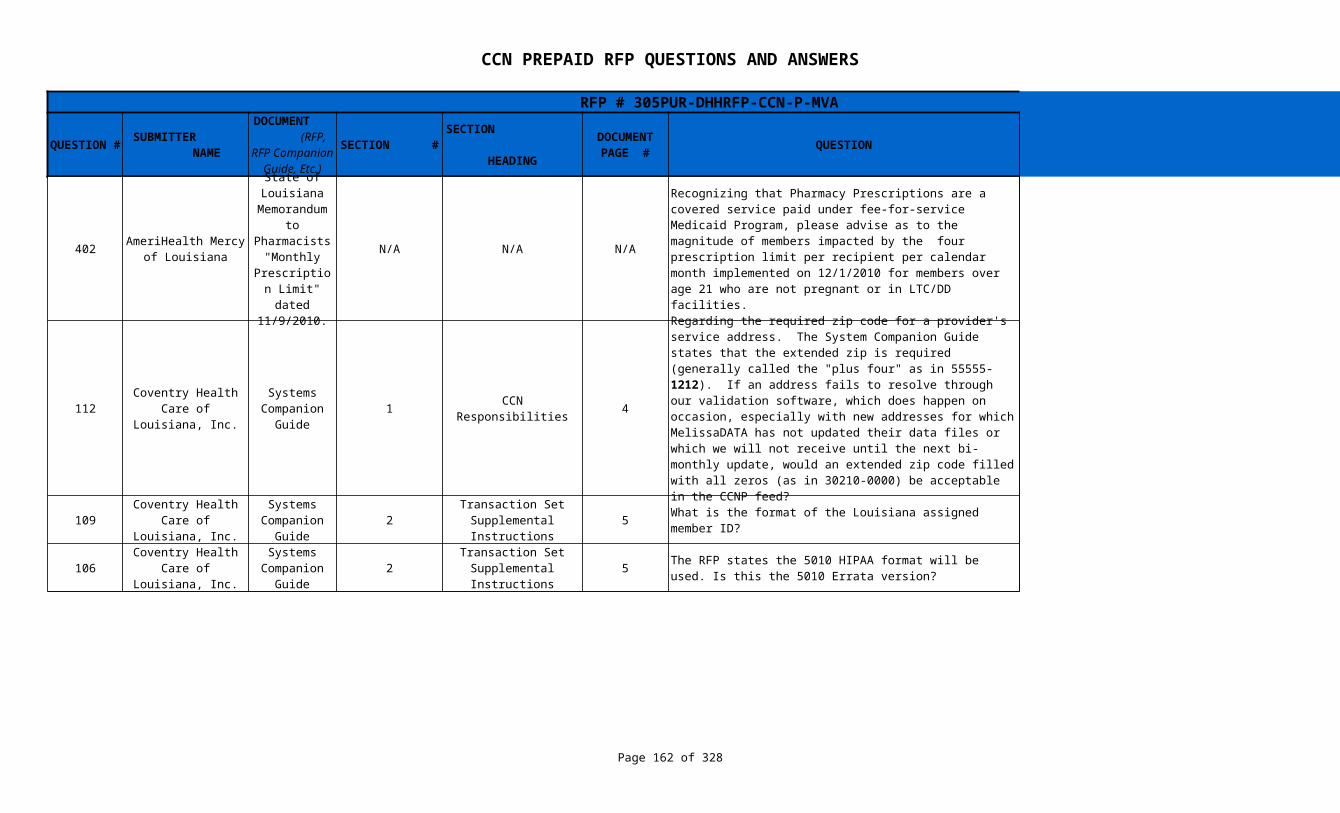
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 162 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
402 N/A N/A N/A
112 1 CCN Responsibilities 4
109 2 5 What is the format of the Louisiana assigned member ID?
106 2 5 Yes
AmeriHealth Mercy of Louisiana
State of Louisiana
Memorandum to
Pharmacists "Monthly
Prescription Limit" dated 11/9/2010.
Recognizing that Pharmacy Prescriptions are a covered service paid under fee-for-service Medicaid Program, please advise as to the magnitude of members impacted by the four prescription limit per recipient per calendar month implemented on 12/1/2010 for members over age 21 who are not pregnant or in LTC/DD facilities.
35,432 members impacted by the four prescription limit per recipient per calendar month implemented on 12/1/2010
Coventry Health Care of Louisiana,
Inc.
Systems Companion
Guide
Regarding the required zip code for a provider's service address. The System Companion Guide states that the extended zip is required (generally called the "plus four" as in 55555-1212). If an address fails to resolve through our validation software, which does happen on occasion, especially with new addresses for which MelissaDATA has not updated their data files or which we will not receive until the next bi-monthly update, would an extended zip code filled with all zeros (as in 30210-0000) be acceptable in the CCNP feed?
The encounter will likely deny if the correct zip+4 is in the provider enrollment file/provider registry. Since the contractor has the control of the information submitted on the provider registry, they should take appropriate actions to ensure the zip codes correspond. DHH will accept zero values in the extended zip part via the provider registry and via encounter transactions.
Coventry Health Care of Louisiana,
Inc.
Systems Companion
Guide
Transaction Set Supplemental Instructions
It is a 13-digit number that has no discernable pattern or sequence.
Coventry Health Care of Louisiana,
Inc.
Systems Companion
Guide
Transaction Set Supplemental Instructions
The RFP states the 5010 HIPAA format will be used. Is this the 5010 Errata version?

CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 163 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
626 2 7
627 3 15
Children's Hospital Health Plan
Systems Companion
Guide
Transaction Set Supplemental Instructions
Paragraph 1 of the "Category II CPT Codes" section is confusing. The paragraph reads as follows and prompts several questions: "Category II CPT Codes. DHH requires the use of applicable Category II CPT Codes or HCPCS Level II G Codes for performance measurement. These codes will facilitate data collection about the quality of care rendered by coding certain services and test results that support nationally established performance measures. In conjunction with the Category II CPT Codes, the PQRI quality-data codes (QDCs) follow current rules for reporting other CPT and HCPCS codes." My questions are: (a) The HCPCS Level II G-codes are not performance measurement codes; they are merely extensions of procedure codes not classified already in CPT4 coding. What do G-codes have to do with PQRI-QDC's? (b) The PQRI-QDC codes are part of the CPT4 code data sets, but not related - as far as I can tell - to the G-codes. Are Louisiana Medicaid providers submitting the PQRI QDC codes at the present in the fee-for-service world?
The Systems Companion Guide will be amended to remove HCPCS Level II G Codes and PQRI quality-data codes (QDCs).
Children's Hospital Health Plan
Systems Companion
GuideRepairable Denial Edit
Codes and Descriptions
Are "repairable error" actually accepted into the DHH warehouse? If so, are they repaired through submission of Frequency "7" transaction? Are VOIDS (frequency "8" transactions) allowed to be submitted?
Denied encounters will not be accepted into the data warehouse. The Medicaid Fiscal Intermediary will produce reports that identify which encounters denied and will provide edit codes. If the encounter is repairable, the CCN must make repairs and resubmit the encounters. Please refer to the Systems Companion Guide for instructions and a list of repairable edit codes.
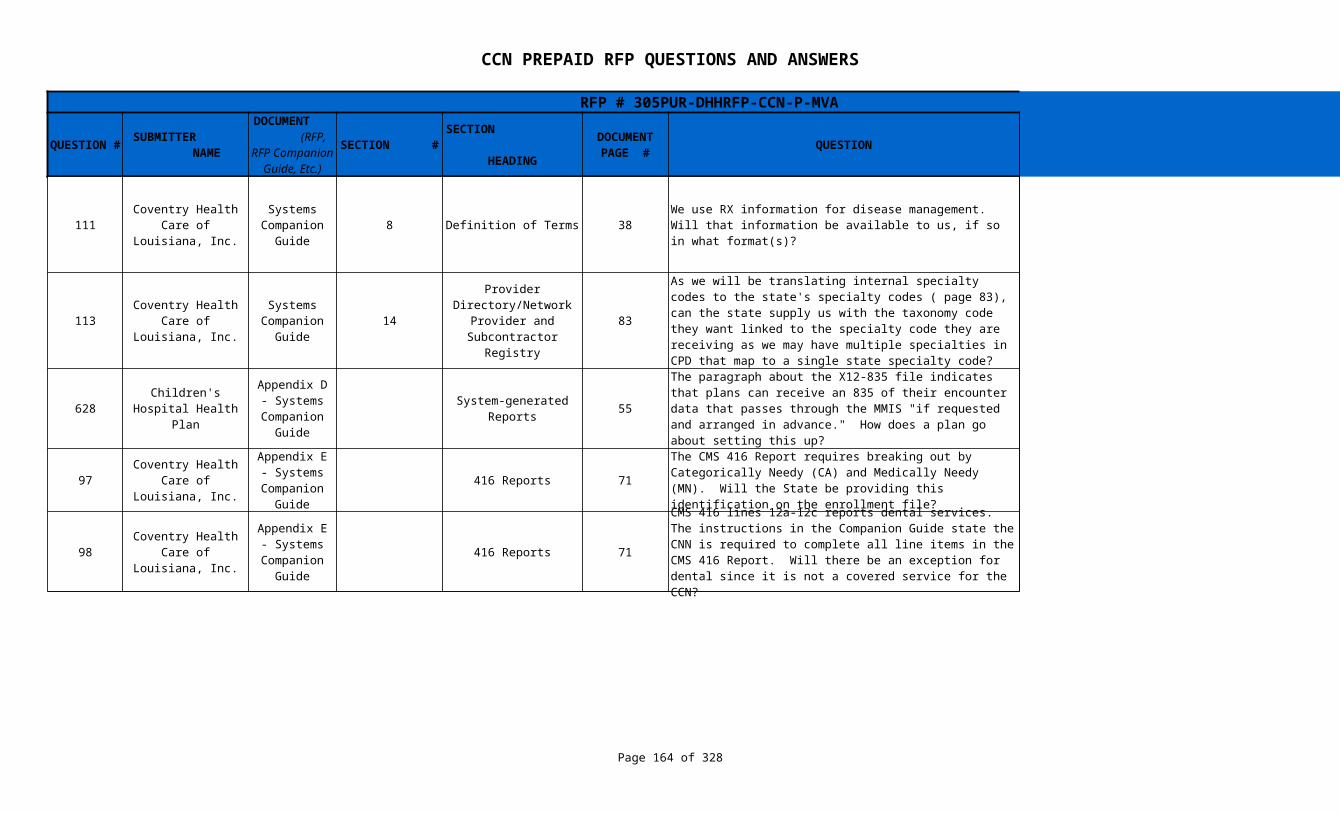
CCN PREPAID RFP QUESTIONS AND ANSWERS
Page 164 of 164
RFP # 305PUR-DHHRFP-CCN-P-MVA
SECTION # QUESTION ANSWERQUESTION #
SUBMITTER NAME
DOCUMENT (RFP, RFP Companion Guide, Etc.)
SECTION HEADING
DOCUMENT PAGE #
111 8 Definition of Terms 38
113 14 83
628 55
97 416 Reports 71
98 416 Reports 71 No, see response to Question # 532
Coventry Health Care of Louisiana,
Inc.
Systems Companion
GuideWe use RX information for disease management. Will that information be available to us, if so in what format(s)?
Yes, Rx information is available on the one-time 2-year claims history file and the weekly claims file that will be provided by the Fiscal Intermediary after successful completion of the readiness review. We will update the Systems Companion Guide to include this format.
Coventry Health Care of Louisiana,
Inc.
Systems Companion
Guide
Provider Directory/Network
Provider and Subcontractor Registry
As we will be translating internal specialty codes to the state's specialty codes ( page 83), can the state supply us with the taxonomy code they want linked to the specialty code they are receiving as we may have multiple specialties in CPD that map to a single state specialty code?
A provider type to specialty cross-walk is provided in the Systems Companion Guide. The taxonomy code reported to you by your providers should determine the state specialty code. DHH will not provide a crosswalk of NPPES taxonomy values with the State's provider specialty codes.
Children's Hospital Health Plan
Appendix D - Systems
Companion Guide
System-generated Reports
The paragraph about the X12-835 file indicates that plans can receive an 835 of their encounter data that passes through the MMIS "if requested and arranged in advance." How does a plan go about setting this up?
A CCN must make a request in writing to DHH in advance of encounter testing in order to obtain 835s.
Coventry Health Care of Louisiana,
Inc.
Appendix E - Systems
Companion Guide
The CMS 416 Report requires breaking out by Categorically Needy (CA) and Medically Needy (MN). Will the State be providing this identification on the enrollment file?
The Enrollment File will contain the Case Type and CCNs will be provided with the crosswalk for Case Type to Categorically Needy and Medically Needy
Coventry Health Care of Louisiana,
Inc.
Appendix E - Systems
Companion Guide
CMS 416 lines 12a-12c reports dental services. The instructions in the Companion Guide state the CNN is required to complete all line items in the CMS 416 Report. Will there be an exception for dental since it is not a covered service for the CCN?





























