Embed Size (px)
Citation preview

edicine 12 (2011) 41–46
Cardiovascular Revascularization MImaging
Would coronary collaterals to the infarct-related artery serve as a marker ofviability in patients with prior myocardial infarction? A study with
trimetazidine-99mTc-sestamibi imaging☆
Amr Adel, Abdel-Hamid Mohamed, Wail Nammas⁎
Faculty of Medicine, Cardiology Department, Ain Shams University, Cairo, Egypt
Received 4 September 2009; received in revised form 9 November 2009; accepted 13 November 2009
Abstract Background: Visualization of collateral circulation to the infarct-related artery on coronary
☆ Financial disclo⁎ Corresponding
Ain Shams UniversityP.O. 11381, Egypt. Te
E-mail address: w
1553-8389/09/$ – seedoi:10.1016/j.carrev.2
angiography was suggested to predict viability in the infarct zone as demonstrated by dobutaminestress echocardiography.Methods and materials: We enrolled 30 consecutive patients referred from our catheterization labswith prior Q-wave myocardial infarction at least 6 months before study enrollment. Patients wereclassified according to the presence of collaterals to the infarct-related artery into two groups:collateral group with Rentrop Grade 1–3 collaterals, and noncollateral group with Rentrop Grade 0collaterals. Patients underwent resting 99mTc-sestamibi imaging study with the administration oftrimetazidine, using the standard technique, within 4 days of coronary angiography. Viability in aspecific territory was defined when at least 50% of its individual segments were classified as viable.Results: The visualization of collaterals by coronary angiography was able to predict viability in theterritory supplied by the infarct-related artery with a sensitivity of 88.2%; specificity of 53.8%;positive and negative predictive values of 71.4% and 77.8%, respectively; and a diagnostic accuracyof 73.3%. The presence of viability increased progressively, in a statistically significant manner,from Rentrop Grade 0 to Grade 1 and Grade 2 [2 (22.2%), 5 (50%), 10 (91%), respectively, P=.04].Conclusions: Visualization of coronary collaterals to the infarct-related artery by coronaryangiography may predict with a high sensitivity but a low specificity the presence of viability in theterritory supplied by that artery.© 2011 Elsevier Inc. All rights reserved.
Keywords: Nuclear cardiology; Coronary collaterals; Myocardial viability
1. Introduction
With the vast progress in the field of coronaryrevascularization over the past two decades, predicting thepresence of viable myocardium has acquired great clinical
sure: No author has a conflict of interest to declare.author. Faculty of Medicine, Cardiology Department,Hospitals, Ain Shams University, Abbassia, Cairol.: +20 12 4063718; fax: +20 2 [email protected] (W. Nammas).
front matter © 2011 Elsevier Inc. All rights reserved.009.11.004
importance, especially in patients assigned for interventionaltreatment [1]. Myocardial viability represents impairment incontractility that is potentially reversible if blood supply isadequately restored [2]. Assumingly, improving blood flowto viable dysfunctional zones results in subsequent improve-ment of regional and global left ventricular function, heartfailure symptoms, functional capacity, and long-termsurvival [3]. This paradigm was supported by the results ofseveral studies where only patients with severe leftventricular dysfunction who had viable myocardium im-proved after revascularization [4].

42 A. Adel et al. / Cardiovascular Revascularization Medicine 12 (2011) 41–46
The visualization of collateral circulation to the infarct-related artery on coronary angiography was suggested topredict the presence of viability in the infarct zone asdemonstrated by dobutamine stress echocardiography [5,6].In a retrospective study design, we sought to explore theability of coronary collaterals to the infarct-related arteryseen by coronary angiography to predict viability in theinfarct territory as shown by 99mTc-sestamibi single photonemission computed tomography (SPECT).
2. Patients and methods
2.1. Patient selection
The study included 30 consecutive patients referred to ourcatheterization labs with prior myocardial infarction, duringthe period from May 2004 to August 2005. Patients wereconsidered eligible for inclusion if they had evidence of priorQ-wave myocardial infarction at least 6 months before studyenrollment. Prior myocardial infarction was defined based on12-lead electrocardiogram showing abnormal Q waves (≥1mm in width) in at least two contiguous leads and previouslaboratory evidence of elevated cardiac biomarkers at thetime of the index infarction: CK-MB and/or troponin morethan twice the upper limit of normal laboratory reference.The indication for coronary angiography was postinfarctionangina in all patients. We excluded patients with prior non-Q-wave myocardial infarction; those with postinfarctionsevere hemodynamic instability; those with significantvalvular or congenital heart disease, or any myocardialdisease apart from ischemia; those who underwent priorpercutaneous coronary angioplasty or surgical coronarybypass; those with atrial fibrillation or bundle branchblock; those with marked obesity (body mass index N30);and those with limited life expectancy due to coexistentdisease (e.g., malignancy). Patients were receiving conven-tional medical therapy according to standard clinicalpractice. Before inclusion, an informed written consentwas obtained from each patient and the study protocol wasreviewed and approved by our local institutional humanresearch committee as it conforms to the ethical guidelines ofthe 1975 Declaration of Helsinki, as revised in 2002.
2.2. Definitions
The presence of hypertension was defined as systolicblood pressure ≥140 mmHg and/or diastolic blood pressure≥90 mmHg, previously recorded by repeated noninvasiveoffice measurements, which lead to lifestyle modification orantihypertensive drug therapy. The presence of diabetesmellitus was defined as fasting plasma glucose ≥126 mg/dl,and/or 2 h post glucose load ≥200 mg/dl, or specificantidiabetic drug therapy. Dyslipidemia was defined as LDLcholesterol N100 mg/dl, and/or serum triglycerides N150 mg/dl, and/or HDL cholesterol b40 mg/dl and b50 mg/dl in
women. Heart failure was defined clinically according to thestandard criteria as validated by the Framingham Heart Study[7]. Diagnosis required the simultaneous presence of at leasttwo major criteria or one major criterion in conjunction withtwo minor criteria. Major criteria included paroxysmalnocturnal dyspnea, neck vein distension, rales, radiographiccardiomegaly, acute pulmonary edema, S3 gallop, increasedcentral venous pressure (N16 cmH2O at right atrium),hepatojugular reflux, and weight loss N4.5 kg in 5 days inresponse to treatment. Minor criteria included bilateral ankleedema, nocturnal cough, dyspnea on ordinary exertion,hepatomegaly, pleural effusion, decrease in vital capacity byone third from maximum recorded, and tachycardia (heartrate N120 beats/min).
2.3. Coronary angiography
All patients underwent selective left and right coronaryarteriography using the standard technique, and theangiographic data were retrospectively analyzed by a singleexpert independent interventionalist, blinded to the clinicalfindings. No intracoronary pharmacologic agents weregiven. Each major epicardial vessel was assessed in atleast two perpendicular planes, and the infarct-related artery(predicted from the site of myocardial infarction seen inelectrocardiogram) was identified by either total occlusionor evidence of plaque ulceration. Collateral circulation tothe infarct-related artery was evaluated according to theclassification system described by Rentrop et al. [8] (Grade0=no visible coronary collaterals. Grade 1=collateralcirculation fills only the side branches of the recipientcoronary artery. Grade 2=collateral circulation partially fillsthe epicardial segments of the recipient coronary artery.Grade 3=collateral circulation completely fills the epicardialsegments of the recipient coronary artery). Patients wereclassified into two groups: collateral group with RentropGrade 1–3 collaterals and noncollateral group with RentropGrade 0 collaterals. Retrospective data were extracted byreviewing the angiographic data registered in the databaseof our catheterization laboratory.
2.4. 99mTc-Sestamibi SPECT imaging protocol
Patients underwent resting 99mTc-sestamibi imagingstudy with the administration of trimetazidine, using thestandard imaging technique, within 4 days of coronaryangiography, provided that no ischemic events wererecorded during the time from coronary angiography to99mTc-sestamibi imaging. Trimetazidine [trimetazidine dihy-drochloride (Vastarel), Servier, France] was administered bythe oral route the day before the study (60 mg in threedivided equal doses 8 h apart) and 1 h before performing thestudy (60 mg single dose). Injection of 25–30 mCi ofradioactive tracer was performed 45–60 min before SPECTimage acquisition. Images were acquired using a rotatingsingle-head gamma camera (GE Starcam 4000i, UK)

Table 1Baseline characteristic of the whole study cohort and the two individual study groups
Whole cohort (N=30) Collateral group (n=21) Control group (n=9) P
Age (years) 52.2±8.6 51.1±8.5 53.7±8.9 .968Male gender 27 (90) 18 (85.7) 9 (100) .232Smoking 11 (36.7) 7 (33.3) 4 (44.4) .563Diabetes 13 (43.3) 12 (57.1) 1 (11.1) .060Hypertension 16 (53.3) 12 (57.1) 4 (44.4) .523Dyslipidemia 13 (43.3) 12 (57.1) 1 (11.1) .060Systolic BP (mmHg) 138±18 134±18 144±18 .648Diastolic BP (mmHg) 84±14 81±15 87±12 .391Heart rate (bpm) 76±9 75±9 78±9 .725Prior angina 11 (36.7) 8 (38.1) 3 (33.3) .804Heart failure 5 (16.7) 1 (4.8) 4 (44.4) .008Ejection fraction (%) 37±7 40±7 33±6 .003
Continuous variables are presented as mean±S.D., while categorical variables are presented as numbers (percentage).BP indicates blood pressure; bpm, beats per minute.
Table 2The distribution of viability detected by 99mTc-sestamibi imaging betweenthe two individual study groups
Without viability (n=13) With viability (n=17)
6 (46.2) 15 (88.2) Collateral group (n=21)7 (53.8) 2 (11.8) Control group (n=9)
Data are expressed as numbers (percent).
43A. Adel et al. / Cardiovascular Revascularization Medicine 12 (2011) 41–46
equipped with low-energy all-purpose collimators. Energywindows of 20% were respectively centered on the 140-keVpeaks of 99mTc-sestamibi. Thirty-two images were obtainedover 180° extending from the 45° right anterior oblique tothe 45° left posterior oblique projections. All studies weresubjected to quality- control checks and corrections whennecessary for camera nonuniformity, center-of-rotation off-sets, patient motion, and “upward creep” [9].
2.5. 99mTc-Sestamibi SPECT image analysis
Two experienced nuclear cardiologists blinded to theclinical and angiographic data analyzed the SPECT images.The vascular assignment of myocardial segments to theconventional anatomic distribution of major coronaryarteries was performed according to the 17-segment scoringsystem [10]. Segmental 99mTc-sestamibi uptake was scoredby use of the four-point scoring system. Patterns of viabilitywere based on the segmental radiotracer uptake [10].Segments were then individually classified into viable ornonviable. The presence of viability in a specific coronaryarterial territory was defined when at least 50% of itsindividual segments were classified as viable [11,12].
2.6. Statistical analysis
All continuous variables were presented as mean±S.D., ifthey were normally distributed. Differences in the normallydistributed variables were assessed using the t test.Categorical variables were described with absolute andrelative (percentage) frequencies. For testing the hypothesisof no difference between groups, a Fisher's Exact Test or χ2
test was used for categorical variables, as appropriate. Thesensitivity, specificity, positive and negative predictivevalues, and diagnostic accuracy were calculated accordingto the standard definitions. The distribution of myocardialviability among the different Rentrop grades of coronarycollateral development, and the correlation between heartfailure and viability were compared using the Pearson χ2
test. All tests were two sided and a probability value ofPb.05 was considered statistically significant. Analyseswere performed with the SPSS version 12.0 statisticalpackage (SPSS, Inc., Chicago, IL, USA).
3. Results
3.1. Baseline demographic and clinical characteristics
A total of 30 patients were enrolled in the current study,which comprised 21 patients with collaterals (collateralgroup) and nine patients without (noncollateral group).Table 1 shows the baseline clinical characteristics of thewhole series, as well as the two individual groups. The meanage of the whole study cohort was 52.2±8.6 years, 27 (90%)being males. The two individual groups were statisticallyhomogenous regarding age, sex, resting heart rate, systolicand diastolic blood pressure, coronary risk factors, pasthistory of angina. However, heart failure was found morefrequently in the noncollateral group as compared to thecollateral group (P=.008), and left ventricular ejectionfraction was significantly higher in the collateral group(P=.003).
3.2. Myocardial viability in patients with collaterals
Table 2 shows the distribution of viability detected by99mTc-sestamibi imaging between the two individual groups.The visualization of collaterals by coronary angiography wasable to predict the presence of viability in the territory

Table 3The distribution of viability detected by 99mTc-sestamibi imaging among patient subgroups with different Rentrop grades
P value Rentrop Grade 2 (n=11) Rentrop Grade 1 (n=10) Rentrop Grade 0 (n=9)
.04 10 (91) 5 (50) 2 (22.2) With viability (n=17)
Data are expressed as numbers (percent).
44 A. Adel et al. / Cardiovascular Revascularization Medicine 12 (2011) 41–46
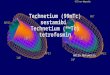
supplied by the infarct-related artery with a sensitivity of88.2%; specificity of 53.8%; positive and negative predictivevalues of 71.4% and 77.8%, respectively; and a diagnosticaccuracy of 73.3%. Table 3 shows the distribution ofviability among the different Rentrop grades of coronarycollaterals. The presence of viability increased progressively,in a statistically significant manner, from Rentrop Grade 0 toGrade 1 and Grade 2 [2 (22.2%), 5 (50%), 10 (91%),respectively, P=.04] (Fig. 1).
4. Discussion
The issue of detecting myocardial viability beforecoronary revascularization has long been a matter of debate.It is always recommended to search for viable myocardiumbefore revascularization of an occluded coronary artery;however, there is no practical yet sensitive method ofassessing myocardial viability in the catheterization labora-tory [5]. Our findings suggest that the visualization ofcollaterals to the infarct-related artery at coronary angiogra-phy may predict the presence of viability in the territorysupplied by this artery with a high sensitivity but a lowspecificity, and the higher the Rentrop grade of collaterals,the more the likelihood of the presence of viability.
4.1. Significance of coronary collateral circulation
Several studies emphasized the functional importance ofcoronary collateral circulation [13–19]. The presence ofcollaterals can limit infarct size, prevent infarct expansion,improve perfusion, and preserve myocardial viability in theinfarct-related artery territory, and thus would improve
Fig. 1. Distribution of viability detected by 99mTc-sestamibi imaging amongpatient subgroups with different Rentrop grades.
recovery of impaired left ventricular function after revascu-larization, although it does not protect against stress-inducedischemia [5,6,13–17,20]. It seems also that the presence ofmyocardial ischemia is a prerequisite for the development ofcoronary collaterals, and, therefore, coronary collaterals maywell indicate ischemic myocardium that could potentially besalvaged by reperfusion [5].
4.2. Prediction of viability based on collaterals
In agreement with our results, several prior reportsaddressed the issue that the presence of collaterals couldpredict the presence of viability in the supplied region[21–23]. A recent study stated that good collateralsdemonstrated by coronary angiography have a high sensitiv-ity and positive predictive value for the prediction of viabilityas shown by dobutamine stress echocardiography andconcluded that one can decide for percutaneous or evensurgical revascularization depending solely on the assess-ment of coronary collateral circulation [5]. Furthermore, Tatliet al. [6], in their study of myocardial viability using colorkinesis dobutamine stress echocardiography, concluded thatearly revascularization could be carried out in patients withgood coronary collateral circulation even without doing anyfurther test of viability. Most of these studies, however,identified viability based on a positive dobutamine stressechocardiography (only one used 99mTc-sestamibi imaging).Lee et al. [24] instead measured pressure-derived fractionalcollateral flow (collateral flow index) in the setting of acutemyocardial infarction and found that pressure-derivedfractional collateral flow was the most powerful predictorof myocardial contractile recovery following revasculariza-tion. They concluded also that there is a linear and significantcorrelation between good collaterals and pressure-derivedfractional collateral flow.
Yet, these observations should be taken with cautionbefore recommending to adopt collateral grade as a criterionfor revascularization of coronary occlusions. Previously, onestudy reported that recovery of impaired contractility afterrevascularization of a chronically occluded artery is notdirectly related to the quality of collateral circulation, sincecollateral development does not essentially require thepresence of viable myocardium [25]. Moreover, anotherstudy observed no difference between patients with andwithout evidence of myocardial viability, concerning thepresence of visible collaterals by coronary angiography [26].
Furthermore, the mean sensitivity and specificity of99mTc-sestamibi imaging to detect myocardial viability havebeen reported as 81% and 66%, respectively, with positive

45A. Adel et al. / Cardiovascular Revascularization Medicine 12 (2011) 41–46
and negative predictive values of 71% and 77%, respectively[27]. It is helpful to acknowledge this limitation of 99mTc-sestamibi imaging while trying to estimate the predictivepower and accuracy of another diagnostic test based on thefindings of 99mTc-sestamibi imaging.
4.3. Employment of trimetazidine in 99mTc-sestamibi imaging
In the current study, we employed a protocol of resting99mTc-sestamibi imaging after oral administration of trime-tazidine. A substantial body of evidence indicates that99mTc-sestamibi may be a good marker for viability [28–30].Both trimetazidine and 99mTc-sestamibi share the sameintracellular target, which is the mitochondrion. As meta-bolic reserve does exist in the hibernating state, trimetazidinemight exploit this reserve by increasing mitochondrialmetabolism. One study demonstrated that trimetazidinewas associated with an increase in 99mTc-sestamibi uptakein infarcted but viable myocardial areas and stated that thisincrease was probably related to an improvement inmitochondrial oxidative metabolism that is essential for99mTc-sestamibi retention [31]. The authors concluded thatcoupling trimetazidine administration to 99mTc-sestamibiperfusion scintigraphy may represent a better means ofdetecting viable myocardium [31].
4.4. Clinical implications
On-screen grading of collaterals is a simple, rapid, readilyachievable, inexpensive means to predict myocardialviability with a relatively high sensitivity. Thus, it canserve—at least—as a good screening test for myocardialviability, i.e., absence of collaterals may exclude viabilitywith a fairly good accuracy. Accordingly, it would be morecost-effective that only patients with evidence of visiblecollaterals by coronary angiography be triaged for furtherviability testing by a more reliable “acknowledged” test. Inthe modern era of escalating health care costs, physicianswill do both the patients and the government a great favor bynot referring patients with low likelihood of viability forfurther costly testing.
4.5. Limitations of the study
Our findings are based on a single-center study with arelatively small sample size of the cohort, a fact that makes itdifficult to generalize our results to all patients with priormyocardial infarction undergoing risk stratification forpredicting the presence of viability. Multicenter studiesusing the same protocol and examining a larger number ofpatients are needed. Another limitation is that we did notmeasure pressure-derived fractional collateral flow in ourpatients; however, a linear significant correlation existsbetween the grade collaterals and pressure-derived fractionalcollateral flow [21]. Visualized well-formed collateralswould reflect a higher fractional collateral flow and thence
a higher likelihood of viability. Additionally, quantitativefunctional measurement of relative or absolute collateralflow obtained during a brief vascular occlusion (recruitablecollateral supply to the area of interest) was not employed.This later currently serves as the reference for assessing thehuman coronary collateral circulation. Moreover, theangiographic grading of collateral vessels is sensitive tovariations in the technique applied and is subject to intra- andinterobserver variability.
4.6. Conclusion
Our data suggest that visualization of coronary collateralsto the infarct-related artery at coronary angiography maypredict, with a high sensitivity but a low specificity, thepresence of viability in the territory supplied by that artery.
Acknowledgments
We deeply appreciate the faithful efforts and sincerecollaboration of all members of staff of the catheterizationlaboratory in Ain Shams University Hospital, who haverigorously participated in the production of this work.
References
[1] Dilsizian V, Bonow RO. Current diagnostic techniques of assessingmyocardial viability in patients with hibernating and stunnedmyocardium. Circulation 1993;87(1):1–20.
[2] Hoffmann R. Stress echocardiography before and after interventionaltherapy. In: Marwick TH, editor. Cardiac stress testing and imaging, Aclinician's guide. New York: Churchill Livingston, 1996. p. 355–67.
[3] Beller GA. Comparison of 201Tl scintigraphy and low-dose dobuta-mine echocardiography for the noninvasive assessment of myocardialviability. Circulation 1996;94(11):2712–9.
[4] Jiménez Borreguero LJ, Ruiz-Salmerón R. Assessment of myocardialviability in patients before revascularization. Rev Esp Cardiol 2003;56(7):721–33.
[5] Kumbasar D, Akyürek O, Dincer I, Atmaca Y, Kiliçkap M, Erol C,Oral D. Good collaterals predict viable myocardium. Angiology 2007;58(5):550–5.
[6] Tatli E, Surucu H, Oztekin E, Ulucay A, Ozcelik F, Ozer O, Aktoz M.Effect of coronary collateral vessels in left ventricular segmentalmotions and myocardial viability using color kinesis dobutamine stressechocardiography. Saudi Med J 2006;27(10):1468–72.
[7] McKee PA, Castelli WP, McNamara PM, Kannel WB. The naturalhistory of congestive heart failure: the Framingham Study. N Engl JMed 1971;285(26):1441–6.
[8] Rentrop KP, Cohen M, Blanke H, Phillips RA. Changes in collateralchannel filling immediately after controlled coronary artery occlusionby an angioplasty balloon in human subjects. J Am Coll Cardiol 1985;5(3):587–92.
[9] Baron J, Chouraqui P. Myocardial single-photon emission computedtomographic quality assurance. J Nucl Cardiol 1996;3(2):157–66.
[10] Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, LaskeyWK, Pennell DJ, Rumberger JA, Ryan T, Verani MS, American HeartAssociation Writing Group on Myocardial Segmentation and Regis-tration for Cardiac Imaging. Standardized myocardial segmentationand nomenclature for tomographic imaging of the heart: a statement forhealthcare professionals from the Cardiac Imaging Committee of theCouncil on Clinical Cardiology of the American Heart Association.Circulation 2002;105(4):539–42.

46 A. Adel et al. / Cardiovascular Revascularization Medicine 12 (2011) 41–46
[11] Bonow RO, Dilsizian V, Cuocolo A, Bacharach SL. Identification ofviable myocardium in patients with chronic coronary artery disease andleft ventricular dysfunction. Comparison of thallium scintigraphy withreinjection and PET imaging with 18F-fluorodeoxyglucose. Circulation1991;83(1):26–37.
[12] Bonow RO, Dilsizian V. Thallium 201 for assessment of myocardialviability. Semin Nucl Med 1991;21(3):230–41.
[13] Cohen M, Rentrop KP. Limitation of myocardial ischemia bycollateral circulation during sudden controlled coronary arteryocclusion in human subjects: a prospective study. Circulation 1986;74(3):469–76.
[14] Newman PE. The coronary collateral circulation: determinants andfunctional significance in ischemic heart disease. Am Heart J 1981;102(3):431–45.
[15] Goldberg HL, Goldstein J, Borer JS, Moses JW, Collins MB.Functional importance of coronary collateral vessels. Am J Cardiol1984;53(6):694–9.
[16] Gregg DE, Patterson RE. Functional importance of the coronarycollaterals. N Engl J Med 1980;303(24):1404–6.
[17] Hecht HS, Aroesty JM, Morkin E, LaRala PJ, Paulin S. Role of thecoronary collateral circulation in the preservation of left ventricularfunction. Radiology 1975;114(2):305–13.
[18] Popma J, Bittl J. Coronary angiography and intravascular ultrasono-graphy. In: Braunwald E, editor. Heart Disease: A Textbook of Cardio-vascular Medicine. Philadelphia: WB Saunders, 2001. p. 387–421.
[19] Hansen JF. Coronary collateral circulation: clinical significance andinfluence on survival in patients with coronary artery occlusion. AmHeart J 1989;117(2):290–5.
[20] Chammas E, Hussein A, Ballane G, Helou A, Yatim A, Tarcha W,Ghanem G. Myocardial perfusion in patients with a totally occludedleft anterior descending coronary artery reinjected by a normal rightcoronary artery: the role of collateral circulation. Angiology 2008;59(4):464–8.
[21] Leclercq F, Messner-Pellenc P, Moragues C, Moragues C, Rivalland F,Carabasse D, Davy JM, Grolleau-Raoux R. Myocardial viabilityassessed by dobutamine echocardiography in acute myocardialinfarction after successful primary coronary angioplasty. Am J Cardiol1997;80(1):6–10.
[22] Poli A, Previtali M, Lanzarini L, Fetiveau R, Diotallevi P, Ferrario M,Mussini A, Specchia G, Montemartini C. Comparison of dobutaminestress echocardiography with dipyridamole stress echocardiography
for detection of viable myocardium after myocardial infarction treatedwith thrombolysis. Heart 1996;75(3):240–6.
[23] Ragosta M, Powers ER, Samady H, Gimple LW, Sarembock IJ, BellerGA. Relationship between extent of residual myocardial viability andcoronary flow reserve in patients with recent myocardial infarction.Am Heart J 2001;141(3):456–62.
[24] Lee CW, Park SW, Cho GY, Hong MK, Kim JJ, Kang DH, Song JK,Lee HJ, Park SJ. Pressure-derived fractional collateral blood flow: aprimary determinant of left ventricular recovery after reperfused acutemyocardial infarction. J Am Coll Cardiol 2000;35(4):949–55.
[25] Werner GS, Surber R, Kuethe F, Emig U, Schwarz G, Bahrmann P,Figulla HR. Collaterals and the recovery of left ventricular functionafter recanalization of a chronic total coronary occlusion. Am Heart J2005;149(1):129–37.
[26] Main ML, Grayburn PA, Landau C, Afridi I. Relation of contractilereserve during low-dose dobutamine echocardiography and angio-graphic extent and severity of coronary artery disease in the presence ofleft ventricular dysfunction. Am J Cardiol 1997;79(10):1309–13.
[27] Bax JJ, Poldermans D, Elhendy A, Boersma E, Rahimtoola SH.Sensitivity, specificity, and predictive accuracies of various noninva-sive techniques for detecting hibernating myocardium. Curr ProblCardiol 2001;26(2):147–86.
[28] Kauffman GJ, Boyne TS, Watson DD, Smith WH, Beller GA.Comparison of rest thallium-201 imaging and rest technetium-99msestamibi imaging for assessment of myocardial viability in patientswith coronary artery disease and severe left ventricular dysfunction.J Am Coll Cardiol 1996;27(7):1592–7.
[29] Dilsizian V, Arrighi JA, Diodati JG, Quyyumi AA, Alavi K, BacharachSL, Marin-Neto JA, Katsiyiannis PT, Bonow RO. Myocardial viabilityin patients with chronic coronary artery disease. Comparison of 99mTc-sestamibi with thallium reinjection and [18F]fluorodeoxyglucose.Circulation 1994;89(2):578–87.
[30] Udelson JE, Coleman PS, Metherall J, Pandian NG, Gomez AR,Griffith JL, Shea NL, Oates E, Konstam MA. Predicting recovery ofsevere regional ventricular dysfunction. Comparison of restingscintigraphy with 201Tl and 99mTc-sestamibi. Circulation 1994;89(6):2552–61.
[31] Ciavolella M, Greco C, Tavolaro R, Tanzilli G, Scopinaro F, CampaPP. Acute oral trimetazidine administration increases resting techne-tium 99m sestamibi uptake in hibernating myocardium. J Nucl Cardiol1998;5(2):128–33.