Embed Size (px)
Citation preview

Lyd S£Sg&) - /C/).l)_met of
The World Bank
FOR OMCLAL USE ONLY
MICROFfTCHIR CuPY Repo Wnl. 11255-IND
Peport So. tI255;_lN Tye (3 TTitle, THIR-D comMUNITY HE~ALTH AND NUT
Author, SUSAN STC(TITExt. 1g2537 Room.A10115 Dept. * ,3Pf{
STAFF APPRAISAL REPORT
INDONESIA
THIRD COMMUNITY HEALTH AND NUTRITION PROJECT
December 4, 1992
Asia Country Department 111Population and Human Resources D'vision
i doement hai a resrice dtributon n may be used by reciet_ onAy in the performace of
their official duties. Its coatemt may not otherwise be disclosed without World Bman auftlrmadiea.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

CURRENCY EQUIVALENTS(as of November, 1992)
Currency Unit = Indonesian Rupiah (Rp)
US$1.00 = Rp 2,020Rp 1 million = US$495
FISCAL YEAR
April 1 - March 31
ABBREVIATIONS AND ACRONYMS
BAPPENAS = National Economic Development Planning AgencyBAPPEDA = Provincial Economic Development Planning AgencyBKKBN = National Family Planning Coordinating BoardBPGD = Provincial or District Nutrition Improvement BoardCBR = Crude Birth RateCHIPPS = Comprehensive Health Services - Province SpecificDEPKES = Ministry of Health (Departemen Kesehatan)DIK = Annual Routine BudgetDIP = Annual Development Budget (Daftar Isian Proyek)DUP - Annual Development Projects (preliminary)GOI = Government of IndonesiaIBI = Indonesian Midwives AssociationIDD = Iodine Deficiency DisorderIEC = Information Education and CommunicationU = JrianJayaINPRES = Instrucksi PresidenKfW = Kreditanstalt fur Wiederaufbau (German Bank for Reconstruction and
Development)LAM - Local Area MonitoringLITBANGKES = Center for Research and DevelopmentLCB = Local Competitive BiddingMCH = Maternal and Child HealthMOH = Ministry of Home AffairsMPC = Media Production CenterNGO = Non-Governmental OrganizationNTT = Nusa Tenggara TimurOED = Operations Evaluation DepartmentPCR = Project Completion ReportPEM = Protein Energy MalnutritionPKK F Family Welfare MovementPO = Operational GuidelinesPOSYANDU = Health and Family Planning Village GatheringPPAR = Project Performance Audit ReportPUSKESMAS = Health CenterREPELITA V = Fifth National Five-year Development PlanSUSENAS = National Economic SurveyTBA = Traditional Birth AttendantTFR = Total Fertility RateUNDP = United Nations Development ProgrammeUNFPA = United Nations Fund for Population ActivitiesUPGK = Family Nutrition Improvement ProgrammeUSAID = U.S. Agency for International DevelopmentWHO = World Health OrganizationWi - West Java

FOR OMCIAL USE ONLY
DEFINMONS
Cont ive Prevaenc Propton of madried women of reproductive age (1S-44)estmatd to be using contapto
Cld Mort RAte Annual daft of chdren 1-5 yas per 1,000 chdren in thesame age group.
Crude Birth Rat Number of live births per year per 1000.
Crde Dleah Rate Number of deaths per yea per 1000.
Total Ferdliy Rate The averae nmber of live chdren dt would be born perw f she were to Ive to the end of her childbearing years
and bear children acording to a given set of age-pecificfertDly rates. The Total Fertity Rate ofte seves as anetimate of the average number of children per family.
Tnfnt Mortlty Rate Anal number of deaths of infants under one year per 1000ite births during the same year.
Low Birth Weig A le-bom inft with a birth weight of less ta 2,500 grams(5 1/2 Ibs) is said to have low birth weight
Maten Death The death of a woman while pregnant or withn 42 days ofdeliery or teation of pregnancy, irespective of thedmuato or the site of the pregcy or its management but notfrom accdenta or hnidentl causes.
Materal Motlty Ratio Number of maten deaths In a given period divided by thenumber of live birbs durig the same perid. The maternalmortity rate, formally ratio, is usuay eapressed per 100,000brh*s.
Neonatal Motality Rate Number of neonata deaths (death of a live born chld within 28days of birh) per 1000 live births per year.
Post-neonatal Mortality Number of post-neonatal deaths (death Ratebetwe 28 days and one year after birth) per 1000 live birtsper year.
Perinah Refrs to the period beween the 28th week of pregnan ndthe end of the fist week after birth
Perinatal Mor yRate Pednatal deaths include late fetal deaths (fetal deaths of 28 ormore weeb of gestation) and deaths of Infants less than oneweek old. The peinatal mortaity rate is the ratio of perindeaths in a given pae to live births during the same period.
This document has a restricted distribution and may be used by recipients only in the performanceof their official duties. Its contents may not otherwise be disclosed without World Bank authorizati

Sdobe _nonl TW_
bids. midwifeBO Read of Dhtrk Govemntdua vmwaDim Kescoatan Dati I PvciWl Hea OfFicDinas KeedwAaa Dati B District Ralt OfficeDokabbs DistDict Healt OfficerDuln (Jayl Traditional Bihth Attendsatgugps bown sroup of Isladskader group of volntes
disrictKocamaten ~~~~subdistrict
POSYSO"negrae heaMily planing communthy giuerlngPa heat cenr
,asbmmn P606813to Subbeat t
1-I
THIRD COMUNY HLT AND TRON PROJECT
LOAN AND PROWr SumgAr
U ew. Rpulc of ndonesia
Amount: US$93.5 miion equivalent
Taa Rpayable In 20 yam hludW S yeas of gia, at ke stndard varableInteres rate.
Duserde.a: Iho goal of the projec Is to elevate nfit, ddld ad mateal heat b,,Xn the efetvenes a£cmmnt healt q h ad nutrito nevniin five provic (West Java, C al Java, al t Nun TWgaraa andblan-Jaya).- Tis-would be acNpIshed by: a) buldig pinl andkaIuaten caacity to-pn Implement and evalut Safe od, ChildSurvival and Nutiton and (b) by srgteIng the capacity ofthe centra Mistry of Healt, prmariy the Dirctrae Gnal for
n I n y Heft* to svpport provhn e -. Mmhowicv l ServiceL Ed _ Yaln cd f coon n o hn
Safe Moterod Child Survival, Nuito and Beat Educato Seckbup ineach provnc wi Im newly deipe apraches to eachintvewntin wMch wi be 6iluated by kaipat and prvnca staff proto uioa t_o addWod WAate _d eac pwvhwc. A SU
for Commuiy Healt, te Centr fr Heat Edon and dte Cene forHealth Daa tD build their caacits fr polcy provo oftemnical to loca leels, ond uwnlbordng of .taining,
i an D midereiewf project progrAes wmll refineintv plan ad adu rourc alcion within th globa esimaeof project osts finaized at apprais. By the ad of the prjec, it iB expcd
measurdan In ifant and man motat, and In nuhiona staus.Moreo, k Is adpatd that eaowh provie wll ha o cap y to sece
flg anld po ot b dbnion each of te areas, and dth prvie nd ka1opma hal nth tewill dow cm In their planing ad evalution s . Atthe cter, it is ttd d the Commuy Healh Directr w havesigniican amdditona si n plannin and evalutio of safe montherhood,Eld sucavin wld e onpro , he 1b Haf lab_ winha"o hMpoV C)apa tD _em ham andieCtouterft ftHaAesdoca w"M be stentend

-
1ae:m lhe direct safed d, cid survival nd nuton nterveions wilbenefit appoxity 1.5 mMin fmiies, denti on de bads of needs, Inth five provines. Servic in each of hee as wi be improved inqualiy, and dir reach wM be expnded dhough more efficient ta-Sedtg ofresoues on key demographic eves. Won's heath stus wi beimprve, and fmae hea pwiders, pclay tUradonalh abirthand vilage midwives wi become mr prodctve. Prvincial and kabuaten
sk In health plaming and management will be improved, whie fthersuemlh_t of DIP and reatd procedures wi be pursued.
1ke: TI maor sk of the project is dut provines, which have not hadrespoibiity or authority for to development of detad interventionsrategies, will develo pl of lothan desrae qlty, in tms of bothsW_ub and process, in the first years of th project To address this risk,te project prvi for ethenin the cpacty of the cent le tosupport the development of mpved plans, nd the dvlopmet of an
atkbuae and pwv levds
(US$ mfllin)
Prvna Sevce Deivery and Capcity1. Service Deivery 30.5 20.0 50.52. Caacity Building 21.8 14.9 36.7
Subtooa M3
Cer Support and Capacit Building1. Picy Development, Plning and
Project Coordinion 6.3 2.6 8.92. TechnIc Services for Provinces 14.7 8.5 23.23. ner-provic programs and research 3.5 1.3 4.84. Capacity buding 2.9 7.3 10.2
Subto~ 19.7 LL
Tou B 2.21 li1x
Physical Contingees 2.3 2.8 5.1Price C:oieies 17.5 7.2 24.7
fg lcuive of tarn and dut ested at US$6.0 mllio equent.

-ill-
- (IJS$ miUS ion)
MRD 45.4 48.1 93.5&adh *tatr fur(W) 2.0 16.5 18 5
Government of Indonla 52.1 - 52.1
Total P 9bai" 14
EsdmatodpiabIKMm@_ (US$ mMIn)
BkFY i 1 19 9 9USS mfikm
Annual 6.0 9.0 16.0 19.0 17.0 15.0 11.5Cumdative 6.0 15.0 31.0 50.0 67.0 82.0 93.5
So fAd Not 2pplicable
M IBRD No. 24137.

-lv-
INDONESU
ITHORD COMMUNrrY BEALTH AND NUT ITION PROJECT
BANC DATA La
Total Area 1990 1,919,440 insTotl Populaton 1990 178.2Populaion Growth Raft 1985-90 1.7% per annumCrude Birth Rate 1990 2611000Crude Death Rate 1990 9/1,000Total Ferity Rafe 1990 3.1Lif Epecncy at Birth 1992 62 yea
Female 1990 64 yeamale 1990 60 years
Ifant Moraty Rate 1990 73/1,000Maternal Mortality Ratio 1990 450W100,000Urbn Population as Prt
of Tota Poulat 1990 31%Adult LItay Iate
Tota 1986 92%Females 1986 75%
Age SMuture 19900-14 35.8%15-64 60.364+ 3.9%
Popu<lon per Physca L984 9.410Bis atteaded by haft staff 1985 43%Babies with low birt weqt 1985 14%Daily calore spply (per cpta) 1989 2,750
1965 1,791Contraep P _vace 1990 50%Per Capit Gros Natlal Product 1992 $610
/A Bank estimates.

.v *
ENDONEI
THIRD COMMNITY --EALT AND NTRITION PIOJECT
STAFF APPRAISAL REPORT
CONUMTPage No.
1 IEALTH AND NURMION SECOR EUM AND tIATEGY ... 1
A. Healtha dNdNWrltoStatS u .......... ................. 1B. Communiy Halt and NWuriton Plisnd Programs ......... 3C. Suppo Sysem for Cmmunty Health dNWutrnPogram. s .. 6D. Key Sectotais ue ............... 8
2 LESONS PROM PASr t1ssI CE AND BANK sTR EBG ... 11
A. .Bk* ..................................... * * * 11B. PolH Dialogue adul Projec ..... ............. . 11C. hnpllcatlm onsr Bank Strategy aind Role . ... .. .. .. .. .. . .. .. 1s
3 THMPROJBECT ..................................... 17
A. ProjectObjects ................................. 17B. ProjectlDescdpton ............. .. 17C>. Proect 0rabto san M _gm .................................. 29D. Proje Plaing, Evaluton ain S .......... 31
This report is based on the findings of an appraisal minio which visited Imloea In June/Juy199. The miusio was led by Ms. Susa Stou and Include Mr. Samuel Llebeoumn PrincipalP 4oin M. Fs& Saada Popubim Sp,a1h, Mr. Harry Go, Sad - or InAdio, Dr. E.ba Opertin Offce, 16. Cad B, Operatos Asdt; mmPet Hywood. Pubic Hath nd NurkitionS list, Dr. Moys FreymanS Pubi efath andMC Speil and Mr. Tany ScottHe Educai SpcaisL Ms ChrOisine H CboWal Dr. CwasPiwr bJani appaised the prect on behaf of KM. Ms. Dadn YudhaMs. Julia Nanucci akd Ms. Dphn GaFprovWidedefice d diM sufpttrout houte production of tdhs eport Te work was managed by Me. Shwn Nwl. Pee reviewemwere Dr. JoeLus bdlaa MNMR); Mr. Rihwd Hea (ASTPH; Mr. Nat Colett(*P) and Me. Virin Rhd (ASM. Ms. Maiae Hog, Dire (EA3DR) adMr. C. Gipin, Chif (A3) hav enorsed the proct..

-vi-
PNo.
4 PROJEC'rCOC S, RNANCING, PROCUREMENTAND D9IS.......4EN.I. . . ...... 34
A. Costs ...... . ... .. ... 34B. Fiancig ...................................... 37C. Procurenmet .................................... 39D. DIbsen ........... ..... . ............... 40E. Accounts, Audits AM Reports. . ........................ 42
5 IENEI1IsANDlRI S ....... ........................ 44
6 AGREEMENTS REACHED AND REOIMENDATON ....... .. 46
A\NNBEMS
1. Selected Heath Srvice Incam by Proince and Kbqatena. Tabls 1-6b. Maps
2. Summary of Provinci Service r)elvey C;o: Inki Plas3. Summary of Expditures by Comonent and Area (1) and by Central Unt (JR)4. Format for IKabt and Prvinial Sevice Divery PlaS. Hlth and Nuiion Eucation Stray6. An A aesot of Dedson Maig at the Kabupat and Pusemas Leves:
Pr minary TORs7. Community Health and Nutition Reseach Laboratories to Suppor Provincial Programs8. Projet Montig ad Evlustlon Genea Ibdicatos9. Proe Cost Estimate
11. IIp-n hSehdMe12. EstmatedO c_ Assiste Sched oe13. Summary of Felowships14A SqyvW= MnPh15. SelectedD W in ProjecPFles
Chart : Nifi*suo SHaft w; n StucxteChart 2: PiniHw ROM pnSzAknE d StructuChart 3: Proje Mnagemst Stuce
MR. IBID 24137 - Sqtembe, 1992. Indoe Projeed Coveage by Pmvi adKaiga*n)

1REALTH AND NUTRITION SECTOR ISSUES
AND STRATEGY
A. EALT Am NuTmON STAU
1.1 Inlonesia has made impressive progress in commnty health ad uition sincethe 1960s. Survey data from the 1980s show better ntritional status, with significant InceasIn aveg caloric intake, and reducdons in the prevaence of moderte and sever manutrionamong young children. Income and nutritional gains, along with feiity decln probblyaccount for much of the imp ve decline in the infant morialit rate (IM) from an estmated124 dets per tousand births in the late 1960s to 105 in th late 1970s and was estimated at73 in the 1990 census. Conibutory factors to these trends inclade a disciplined, commnity-boe family planning progrm, improved access to immiz n and other prenive andcurtve health sevices diough the establishmet of nearly 6,000 hea ces and linbedsubcontet and village-level posyandu, and a vigorous, hnovative program of nutritionedcatlonad monoring.
1.2 Despke thee gis, Indonesia coniues to face seious mmuny health andn_utitn chalenges. Ihe results of a recent Demographic and Health Survey as wll a the 1990Cenu reveal a disturbing stall in the previous rate of decline In tnfimt mortality as wel asslower tO irn covera of basic provendve progams, padclay imi ofinfants an prant women, previously anticipated. Most obvious pes, areproblemsrlating to the very bhg levels of maternal mortality and morbidity which, in the contest of theIceasing proporton of all ianmt deas that occur in the pernal period, uggests a need tomrove the quality and fveness of care during the birh process Itself. Morer, pockets
of low nutrilona status are evide aross the couty, and micro t defici,parculaly of iodine and Vitamin A, buttess unaceptably high levels of inbnt and childmortaity-especially among the poor, and in the Easte islands.
1.3 Health Status. Income and ntional ains along with fiity deline probablyaccount for muh of e impressive fal in the Infat mortality rae. Anohr corbuta y factrhas been hIcrsed coverage of ztion against childhood dise. Access to
o.1 .1 and other preventive and curative health seces e d with the tduing the 1980s of a network of nearly 6,000 health centers, each staffed by vaiou medicalandparamedical personel, and each servig several subeters and about 40 posyau. Surveyfidings suggest that this system is gaining ce and delivering a growing volume ofservies. Mie 1987 Nadonra Socoeconomic Survey (SUSENAS) entid an icrasedtndency for lower and midde expenditre groups, ru and urdb, to vist healt cente forIrea _t In 1987, 30 percent of the rua poor (lower four deciles) in Java and 26 percet inthe Out Islands visited health cens for care when m in 1987 ompred with only 17 pecentand 11 percen respectively in 1978.

-2 -
1.4 Although damn sang nft ad children fel haply over th lst ten yes,materD morbidt and motat icasshow ls ap ross. Morver, ecen studies
sgst t firther rectdons In botkhI and matenal motality wi require; mocoo_ncentrat atteno on problem ao ed with manl hlth ad nutritional status piorto and durig pe , wel as Improved avaialt of sui able seices andmedical cao at birth. her ar no a tsc mews of the naional leves of materamortlity because of the lack of vit regsttion a society where over 75 pert of aldelivries tak place In t hom and reaod deaf are 110t_ Hwer, various sconductd since t late 1970s report rates 1/ vying bawen 1.5 ad 7.2 matern dots per1,000 live birts. GOT edmates the national maternal mortlity rat to be 450 dths per100,000 live birhs.
1.S Nutrtona Stu. Survy data fro dto 198h show significant increases Inavea caoric inte, and redcton In the pmra e of modrate atd severe manu_ionamong youg chldrn hes advnwces atrbutable to grwth in food producton and ruralemployment, and beer monoing of shQorgs andtmprvd management and distbutio offood sWlies. Anoter fator, was hoe UPOK program which used monthly vilgmeetig (now cagled posyadu) to promots nuritin educat Nevertheless, malutton, abiologlly obstcle to improved matn and nt heth status, continu inmy pockets of 1avaa and s uneptby high througout the Eae ilands.Improvements in n8utitn stU wll requie hImved D practes acrs t entrepopulain, but espcay among pregnant wome and youg dren, a wel as contiuede-or to ho efoot proa_ and dbtbodw systms. Impoving _mknWsatus amnnifant and young girs miught contute to redu In th1 ddr of poor outcomes for both
mohers and babies In the long ru
1.6 Fetltyaand myPlann. has madeagrebasrdeswardsreduingfertty. Since 1970, frtil rtes havb fallen by 40 perent from a of£ famiyplaning and use of moder a i, ecomic d p n d Imrved womeseducatin Mm remakale decline h rtiy, which hua reaed repacement levels in pasof la, directly contrite to redue rids of matoen mrt through reduced nmber ofprenes and i likely contribtinS to betr Ia halt us toughrdon In thenumbers of risky birt, tat is th to wome who arm too young or too od, and those tht arespaced too closely tgether. Nwevrthless, fertty sae8 remain h in mimy of the outerIsads, and y _ in poor are, In n those in urban slm, in co res and thelanles do not have ready access tO family plni services. Futeogress in fmilyplanning will require efortsm to mainai and and boh th qult and quantity of familyplang dand m t and child hbt sevices in tose .
1.7 IJn_. There are sveal I r Hk linkages among thse aspecs ofmmunityhealth and nutritional status. Maernal hea is closedy l d wh child hl. Neonmorty acou for about 40 per ce of al hi deats in Idonesa and eghy pern of
Il Ca tnal reer. to maenl noiaty =too typiay rfe tdo mteal nxuft m&die is do nmb of mtnld deat per 1,000 Da bhs Formay, d. m_trnl mrtaity btis di nmbr of aerad deas per 100,000 wm of zpwdmti sgo. The ditincto isimportlat, - de matera nwxty io ud _¢mu obsteti Mks, and wM decin only ifpata and obtt ce is iroved. Mm matemal uuxt zat on to ad= ba onfondsobsrc dab_ nd di. dab atiut* to hi*gh ft.

'Il [Id

or$a at' ora .I1 b

-5-
particular to allocadag the resources necessary for ensuring ta the health system in EastenIndoesia strengthened and that hea sevices rach the poor whaever they are found. Teneed to rapidly mprove the quaity and effectveness of heat services through more efficientmanageme at central, provinial and kult levels has als emered as a firdamental policyobtjecdve. Bodk DepKs and Eap cite the work Initiated though the Third Healh Projectand to be extended throug this project, as a base for examination of whether decenrizedapproaches to community health and mtrion promote Wpovement In program fctdveness.
1.14 The Sife Motherhood trAt. The growing recogn of perin andmatermal health risks as major health problems, in conjuncton with the need to imprve theacceblity and utilization of moe effdcve family planing methods, has led GOI to developa Naiondal Se Moerhood StrateV. The Safe Mothehood Strategy recommends that thefolowng major actvities become th focus of Governet action: () inasing awarens andthe c t of leadersi to Safe Mothehod go0a, (I) bprwving the malablity and useof information about maternal mortality and morbidity, OIl strengtening maternal health care,inluding mtiion and family planning services at vile, subdistrict and distict leves,(Qv) IWmpoving for trainal birth atte , midwives and other halh profssionals,(v) strengthening the management and spevision of MCH services, patic y at the districtand province levels, (vi) improving iformon, education and comni_cation acties directedtoward Saf Mothood goals, and (vii) Impoving the status of wom The strategy includedalso the develop of specfic plans for Saf Mothehood for each prvic. These plans havebeen conidered in the developmt of this project.
1.15 Nuotn PoUcy and Prams. While nutrition i sedom a major direct caeof death, the inracton between nurion, infection and other evens (incuding the fcts ofmicronutrIet defidencies on child survival and of low hemoglobin leves on survival of womenfollowing hemorrhag during partrition) ieas th Imvements In nutritiona status are animportant fctor in the decline of infa and cid mortaity. Purther impven can beexpected to cont to furher dedines In the immdiate fut Indonesi's commitment to
rter IMEprovemen in the food and nuton siuton of the popation is shown in Repelita VIn which food and nuftrion policies fou on four objectves: i) consolidation of food self-sfflciency through incased food production; (i) reducin d _ependec on rice and improvwingnutritiona status for the poplatin trwough iceased dlvh cn of food cnmpton;
improving nutrond sts of hints, childr and preant women; and (iv) improvingnutritional stats of the population trough measures to reduce the prevalenc of nuriondiseases such u protein and energy defidencies, vitamin A defcieny, nutitoa anemia andgoiter. Natonal and povinal effts to p of tis policy wM illnvolve inersectracoop on, pacullybetwnheth and a e. As withoher iterveonsto impvehealth, this policy i justified on the basis of reduction in the burden of illnem and prturedeath, Its contributio to human capital formion and, hIdirecdy, to redung poverty byotrbuting to the factors brnging about lower feti ates. lhose food and mntion policies
are a compont of pov&ty alleviation, a prhiary go of Relita V. Iheir mp _n willoccur in the contex of an increasing emphas ca
1.16 Th governme has established a prom for impwvement of family ntiion,The Family Nutrition ovement Progm (UPOK). The UPK i an inter-sectoral bodyinvolving Depkes, BKKBN, D alt of Religious Affars and the D mad of Agilur.U lK provides mmut -based growth moniing, mntriion first aid acdvities and nurtoacoun g for mothers. These services are pwvied thwough the itgrted heat post

-6-
(posyandu) with suppo frm the Naonal Family Welfare (PKK. Ihe program haswimessed mjo Improvemns in reahing its trgt, as Idiad by Iacrmn covage ofchildrn under 5 from 40 pecent In 1984/85 to 80 pecet In 1987. Hower, the success ofthe progm has not bee unifom acros all reion in hie countries, stg t need for aeaspecific plansas wdl as alerativ qViservice to d eivey eseiay iathe less populatedareas of te county.
C. SUwor Swuu FM CO NWTY REALl AnD NurnMN PROGRAMS
1.17 Plnng and Budgetig for Community Heath and Nutiidon. Recent sectorwork (Indonesia Te in Health Planing and Budgeting, Report No. 7291-IND) and the UNHealth Project O. 3042-IND) illuminate to effectier community health and mntrionprograms (see par.. 2.9 - 2.14) in nt curret fiwcl pr . Sourc of fince anehigly fwith difft and dy in f cd p ,capia and recurret budgets, as wel aspecal purpos flds Iwuding the NW S for healthand Iw p i fimy ad. Mm centnd dwdo_M budgot (APN), which includesforeign a , is managed amost entiry at the center, Is the muaor budget for desonsabout health e . This stru lmits thecope and hIcentive for active decisonmaingl at the local levd and saps acot y
1.18 Moreover, the lenghyprocess ofppa , rviwing and finalizing nnualPBNbudgets (th DIs) is tseilf highly fragmented-tirte maJor project head ar used to budgetfor community health and utrion activitie-and oly ilves provhi (not district level)decisio makers In a briefcn of broa torm set at th ctra level. Typically,pwvncil and disttlevelo s lear of the final outomes of the budget proes wel aftethe beging of the year, when it is dhifu to adjusL C l lvel progam uns are assignedresponsbiity for prepari sticty specffled op io gidnes which direct localinviemepl"- Gudldines hmseves can only be revised through a lengthy processaininvolving the central unts whose staff lack the 1m ad resources to visit local settigs withsufcient freqency and/or depth to allow pproiJudaem about alrnaive apoestD PVW-Mn J--- Al tothe, pocesm foa plning ommunty halt adnuition progrms inhibitlocal kntativ Hmitabiltyofloca halt staffto design or implemetspecific resonses to local conditIons and severdy lmit th hire of local gove n andoffkics in seice covea or quty.
1.19 Bealth bf adlon Systn. bIfidiemt p ing and budeti procedrm adthe absence of Inentives for improved pIn th sector are reinfrced by profoundgaps In e quantty, quait and tisss of inomaion about health ad nutrdti outcomes.The Ministry of Health relies primariy on h and inequent collect of servicestis for rqport on the hInal operaton of tho inistry and occasiona ad hoc surveof hedth stat. Infomaion an key heat outcomes, -nluding bih and death rates ecollected every ten years though the natona cmuus ad at five year intervals tbmugh a mid-census survey. Th use of these data for tehing ad mbontg kec_am and vlage levelieei therefore prese svera problmen, nclud iacrate of thepopulation in ned of services, patculay for ant a d healb h care, and unreliabe andinccurae esmation of program cveage.
1.20 Moreover, curent sysm for collection and diribut of service staiscs aeows and tims _onmmng, and do amt addimedo masfu_ ruk_ of pd an d

lg,,aLilllli, SlW'l IulEo

-8-
side, ining the two suc of ew in field settings requires skills in marketing and hateducaton that are fiquetly missig In provincial and kabupaten health offices.
1.2S Although PKM is well-desigped on paper, it lacks clear short and long termobjectvea whi, combnd wh undear job descripton ncoges a 'penalic' approachto staffanaent and a dilution of highly constrained techical sil wihworloads. Working relatdonhips between PK1M and its 'dient' progrm units, a wel aprovia PKM offices, are als largely informal and confused, witb esuig tesonconning responsibility for the content of educational materials and technical aspects of
d Most of the technical assistance made available to PKCM has been tared tospcific campaign, rater tha to the development of PKM's capacity to manage heath adeducato and an agenda detedmied at local, provincial and national levels. Pa tend to reflectthe avallabflity of funds and related objectives of paricular national and especay nnatonaldonr agencies rahr than prov l and local analyses of health and nutrition condon. P!KMalso lack a clear staff delopment plan for improving its imted skil mix, despie stog
among curmt staff, at provinca as well as central leves, on the need foraddifional skls. Skills In 'contracting out" responsibility for audiene rearch and mediaproduction/distributlon need to be strenghened.
1.26 M ealthDanpower. Ihe Ministry of Health and the Bank are iniating sector workto analyze constain and opporties in the health manpower subsector. Although deftve
scoud await the results of this exercise, four aspect of the bsector arerelevamt to the gols ad excted outcomes of this project. First, the absence of a centralcapacity to anyze nd aculate health manpower plams has led to sevea problems, idingconsderble confusion and overlap concening instiutioal responsibility for halt manpowerpoicy, i Inve--mt in the quality of training programs, and central/provinca tensionsconceing reponibity for staff deployment. Second, the appropriate primary conce wthhe sk, nube and disttion of service delivery staff in the last 10 years has resulted in
muIainming for rs and andys with skills appropriate for managingpublic or private health services. Despite 10 years of investm in the dwelopme of Schoolsof Public Heal, Nutrition Aademies and other higher level isuions, the quality drelevwm of public health ad nutrition research remains wealk Third, as discussed exensivelywith Dq%es in the conteD of the Fifth Popation Project the rent decision to train and deployvillage midwives da dW Desa), has revealed a mber of critical bsues concernnctCaion and Hlem procedures for health providers, dVployment pctic, and the quaitof pe- and insrvice traing.
1.27 The radonhp of public sector health provider workers to taitonalnd privatesector providers also requires darification and resolution in the near futore. Last, extensiveanalyses of the poywdu mov and performance suggest that the principles of wlwawLrm
that lead to reliance on vlage women (dr) for posyandu promotion and maagement areunrealistic. More ralc reward and nentive structs wl be necessary to encourag thislevel of work and reduce the high drop out rates that now prevail.
D. KEY SECrORAL ISSUES
1.28 What Inte-vatkos would make a difference the health ad nutition stat.of Indo_l E the dshrt term? Although Indonesia has been so far successl in developingbasic health services and nutrition services, includig the delivery of family plannig, much

-9 -
rmains to be done. lhe stability in the it morality rates from 1965 to the 1990 censusreport higlUie need to build on and accelera he advances of die early 1980s. In th netem, the greatest Impact on health status wil contnue to rest from Improvemens In nt andmatal heath. To farte reduce infant and maternal mortalit, heth seg needs todvlop an appoach whi ) impo uing among both consumes and provides,of the factors influening maternal ad Inn health, and most importanty, how t recognize,prevent nd if neceary manage the risk surrunding th birth event; and (2) make moreefective use of available health facles and staff in the mangeme of obstetc and pediatricemeencies. Imrving nutritional stats thrugh steps such as nutroeduccad ncasingthe ditbuton and osumpton of mncron-tients, and impoed food producdon and usepatter, are o necessary and wold conbte to Ip v n I health stats. Many of thestp to achiwe the gols, such as improved transport and mmu linbkges betweenhealth centers and ditict hospials, strengthened clinical skills at all lvels, and better use ofepideological da in mig health coices will alo be necessay for the management of thehealth r at Indonesa wil face as is popubtion ages in the coming decades.
1.29 ow cam obstacle to more efective peforoae of _k and posyaund(rlocal serice deivey anels") be overcome? Most important, however, Capacities toimpoe the perfomance of healft centers and posyandu wil need to be strengthened as a basefor improving the quality and coverage of basic services directd at community health andnutrn Norms for the loca magmn of puskesmas and for te introductin andmangent of posyand are well established. Supporting admnitraiv procedu, such asthe use of microplanning for health center work programs, Inmroved mateias for posyandueducational acies and others have been Idenfied and implemented, at Ieast in selectvesetti_ . Thes norms, and may of the suggested adjustmet, were developed in the firstntanc on the basis of eady expeience with both sysms in JavaAli. These guideines may
not be effective in settinp which differ socially, economically and geographically fromJava/iall. Manaers at the ditict and helth cener level need to be able to adapt the posyauoncept to each local wvkomet, according to faors ihat may inuen its success. Although
opeonal norms are wel deveoped in some setings, steps to adopt dtese procedures topartcula local conditions, to complement noma operadtg procedure with creative use ofunique local resources, and to ensure that all staff are routinely involved in making workprocedures more effectve withn particular settings wil require a much more intensive efort tomonitor and evaluate pu and posyandu performance agast crta which are direcdyeflective of desired changes in health and nutriton stus. Improving provinal and kabupaten
level skills in program evaluaton and analysis of the d of program effectivenswould contute to this goa.
1.30 Eow can plnning and budgeing procedur be Improved? Making servicedelivery channels more effctive, especially in remote and poor areas, will in tur requireImprving currmnt planning and budgeig procedu. Three steps need to be taken to imprvethe planning and budget procedur which govern comnmnity beal and nutito First,syms to masure spcf health outcomes and deco making pattrs need to shift fiom onefcused on the amm the availabiliy of ipu toward a sharper focus on achievigspecific oumes or aspects of program ffectiveaess. Second, steps need to be taken tocomolidate the curret n_ of budget soues and to make highly centiHzed, rigidbudgeig procedures for heath more flexble and resposie to loca condtios.Lat, one ems embodying thes prnples are designed, efforts to promote and apply these

IHIjjIqll[511 Ii
V1" Ii i*h3 aiii11111 liii§ l {{§st#-}tS}|~~~~~~.
ii:|2WW

2LESSONS FROM PAST EXPERENCE
AND BANK STRATEGY
A BACKG
2.1 To date, the Bank has ficed five projec in ndonesisk in haft and nutritionto US$156 million and five population projects for a total of US$211.8 mMion a
su_marized In Table 2.1. Ihe first the projec in the health and nuttion sct and the fstfour poluin projects are complete. he Bank has lo coadutd a varety of inomal andfora sa analyses including, In 1989, a study of planing and budgeg Issues In theheah sector and a prpective study of the allenge and opporti faing the famiyplahing prom in the 1990s. OED sponsored a doeaed cas study of the bisbtory ofpoplation lendingI Indoneda and most recenty, the RBk completed a major study of heatfinacing and an infomal nte on AIDS for dscussion with podicymakers In indonesa
B POucy DIaam AND PAo W
2.2 PolIy Dialogue. Ihe Bans dlogue withGOI an health issues has steadilygrown in scope and depth. At the begining of the 1980s, the Bans focus was ot improvinghalt services and malaria control in one provine rather ta on a sector point ofview. IheFit Nutrition Project (Li. 1373-IND) helped target poicy dicusson on the problem ofservice deliy In dise setig and on the need to Improve tIn ing and reerch in noutrition.Secow work on health planning and budgeting in the lt 1980s d Bak/DEPKESdbicusio an topics such as health financing and methods for poving the use of human,fiancial and infomation resources. From lts earlier focus an problems of provifor operational and maineance costs at all lvels of the sector, hhi has led t todas specificfocus on the role of health isrn in ensuin the prvision of high qualty services ataffordable prices in public and private settings. An eady Invesmt project in halth mwpower(Ln. 2542-IND), was orietd prmarily to te constuction nd equipment of sdectd t
mtdio.sThe intent was to help GOI meet part of is pressing needs for pamedic trningpenig the devdopmet of a more comprehensive aproach to mapower deopmn isesin tbe sector. This project seed t hiHghtthe auy co hresoce plning in te sector. Drawing ans th is 1 p a tbotstudy of health mapower iss as a stop tward the deveopment of moe sophiscated poiciesin ths crucial subsector.
2.3 Today's heat policy agenda long-ru concerns with how Indonesiaprepaes to adjust its heat system to the heath needs of an ag populaton as well asContinuing efforts to extend and improve the efctiveness of pimay heat servi. Inaddition, evidec sugges hat HIV i on nd actio AIDS cases could also s rapidly,

- 12-
Table 2.1: BAN OPATImS, SwcroR WORK AD EvALuANs o F lftocrPErF UNM IN POPQATION, MALTE AM NRamoN
Project Apprval Loan/Credt Amunt StusDaft Numbar (USS million)
Hilt and Nutrton
First Nutrition 03/O1M La. 1373 13.0 ClosedProvincl Health 02108183 La. 2235 27.0 ClosedSecond Heath (Manpower
Developmt) 04/14/85 La. 2542 39.0 OngoingSecond Community Health
and Nutition 11126/85 La. 2636 33.4 ClosedThid Health Project 04f2S/89 La. 3042 OngoIng
Subtotal15
Population I 03/28m Cr. 300 13.2 ClosedPopulation It 06/3~0m La. 1472 24.S ClosedPopuation m 06/10/80 LI. 1869 35.0 ClosedPopuation TV 03107/85 La. 2529 351 ClosedFift Populatio 02108191 LaL. 3298 104.0 Ongoing(Family Planning and SafeMotheho) Projed
Subtotal ail
Roma Sectw Reportsma
Indonesi - Issues In Hal Plnning and Budgetng; Report No. 7291-IND, February 28,1989.Indeia - Famiy PlWang Pesectin the 199Js, A World Bank Cout Study.Waigton, DC: World Bank. April, 1990.Indonesia - Hath Inunce Ises In the 199fs; Report No. 999-ND, Ja y 9, 1992.
PiaLo r PERFRMANC Au=rr RoTs (PPARs)Report No. 3748 P aion I (Credi 0300). May, 1985Report No. 6276 Puaon H (Loan. 1472). June, 1986
PROMECr COMMLETON REpor PC)Report No. 5757 First Nutio Project (Lm 1373). June, 1985Report No. na. Secod Population Project (Loan 1472). September, 1985Report No. 7564 Third PopWuaio PFroject (Loan 1869). December, 1988Report No. na. Provin Heath Project (Loan 2235). June, 1990

- 13 -
placing now burden on the health systm In dealng with the shift toward a greaterpoportonate burde fom adul and dronic disses, the curt heath system wI need touero ai adjusmnts anas sh as the scope of prventive health measures; thenmbe ad mix of persa ; the oriontatn of medical educaton; the distrbto, scale andsohitiato of faii, refera stm, asd capit equimen finig
and the publicrvate divson of rlea. Onoing discusion of a recen sectorrport on Health Insurance and te preprton of a Health IV project provide a context forrevwing these Issue.
2.4 In the nea term, policy dialogue focuses on issues which need to be addresed toprove the prmary health care system. A first concern is t ensure th health problems are
deied at the loal level, and receive priorkt ttion at the field level. bis can be done bys g that those most aware of local condio and requiements, i.e. k n and
pu kesmhealth nmage and workers, have a large role In settiDg prioties and designinghelth niative. Responilble staff also need the managerial and budgetay aority to developand implement loc plan. Finally, this approch wil need to draw on regularly updated dataan Icidene, outme and sevice utilition. Ihe capaciy to generte and use such informationwill have to be enhanced. Secondly, more and better sdlled human resources wil be requiredIf the focus on locally derioed ries is to work. Although many facities and personnelae now in place, there remain critical staff vacnies, sk ddeficiencies, and shortages of drugsand trnor hese misspig componen und program effeciveness, especialy in poorerar wh more severe public heath problems. Personnel policies coverig coditions ofservice, houg options, prwtion possibilities and critea, career developmen, rightsren transfer within and betwoee regios, and the use of contacta arrangements may need
hater adjusment and refining as well and are therflbre an important topic for near term policydicusion. A fnl major dimension of policy discussion concerns the need to sort healthcenter level nwove nwth technical frsc 1iom units located at the distict, provinceand even the cne. A reoientation of the role of Jabed units needs as nmch
n as does the crn effrt to improve capacity and sk at the provincw anddistict leels.
2.5 Prdct Ex,iee. ImpIntan of the past population and health projects hasbeen reasonably smooth following some niiaW delays in project cution In most of theplio. Several los have bee learned from these projects. The Prvicua Health Project,te Fist Nution Prject, and the first fDur populaun projects were heavy oriented toward'bricks and mort with the Irgest prportion of aU llpe for buildigp follwed closelyby for epment, ture and vehiles. The popuation projects In particular
sistd the BKKBN in establishing dirict and provic level magement capacity and in theprovo of the materials, qpipmet and veicles needed to suport Its active fmily plningpromotion efrts. TIe Fhrst Nutition project, one of the first in the Bank's nutitin pordblio,pmvidd aly epeie in the development of tnques for mntrition education and provideda base for the deveopment of natonal nutrition policy. While usefl to basicRi-E-Rd-0 1-01 -m-buildfag aW _mnagenM nimprovet" needs, tee projects tended to focus Bank andbonower aention, to the completion of dbbwmt and proam plans rher thm to the
_Dt~o afidd ladE reSts.
2.6 I Scoand Nuriton and Community Health Project (NCH - U, ln 2636-D)and the Iid Health PoJect (L 30424ND) are e most Immediate predecessors to ti project.Ibe Second (Hoalth Mpower) Project 2542-IND) also provides valuale negatve les

-14-
for the projec I ncipal o fom NCR-II did crflly designed hteveows, forknow tO promote bzr Ireafm of darhea dieso, can work but must be dd tD
reflect local geograic, economic and cidmologlcal conditions. Replicaon of successfldrs i more a mater of rbg managem and desa pinciples, rar tha of
wholsae adopdon of 'model' p,ro m or interventIons. For example, NCH-I proved that itwa fble and ffcdve to more rapidly expnd th network of posyandu employed by theDeps to provi sices, but did litle to show how posyandu could be made more efectivegive certa specific _. While lossons oncerning the efectivens of poyandu,ncluing in pa rproblem relat to rapid urnover and high drop outaes among vilage
levd volut kader wer we documented though the project, the project was less successflin creang a _o in which alt tve solutions to these problem od beexmined. Ihe project also had pacly well-documented eperin the dvelopment oftraining and prmoinl campais and reated materials through a series of activities bsd withthe Ctr for Healt EduI Thes activities conutd direcy to consumer knowledgeof the rtonal for and srvices offed through the posyandu system. Rowever, the actvteswero carried out largly on an ad hoc bais, and lasting hmpact on the Center for HealthEducations capacy to dei, manage and evauate other halth and nutrition educational
has bee les than desred. Th Second (Health Manpower) Health Project hassffered from unfortate dlas In impi as well as poor fit with develomen in thwsctr and is typical of eary construction oriened projects. pmrving the fnco andperformance of selected schools and fce built in the project will be a god of tis project.
2.7 On a more psiside, th experiences of NCR-U, patily when compedwith the ThW Health Project (Li 3042-D), heped the Bank and DepKes tO reone theed to find was tD 'locai' genal policy diecdons and program gidance in order to get
more resuts. This project shows hiatnventions can be focused and made more eff ctive byenhancig the uthrity and resonsbility ofprvncandkhealth officals. However,inceasg the 'locatop ' of t nonplanning den on skimprovementsat the local level, and ad In the central role, which enable staff to suppor, not directlocal ntevato. Th projea has a hd Impont success In tablishing t fibility ofpie adjtment for local halt seve and with tie deveopment of tools to promotehWestated bedth plaval pg at t Xe pudmmu, kbupaten and provincia levels. TR's inovatonsin this area, in particlr the desig of the Basic Health Services Project, a fomat for
the _mag m of all com_mity health programs at the health center level, formthe sttng point for the curt poject's poicy efts relatig to Imeprved planning.
2.8 Recnt analys Of bhea and population projects draw atenion to sralImportant asec of project speviio. Bank procedures and reporting m In the fistsoneatim of projcs woe pedved to be hiexible and poorly matched to DepKs' orBKBN's need to adjt the use of avaie resoures according to lessons learned In the ealystag of proga deveopdmn. Anhr cricsm of ealy suevison effot emphsize tediuty of providing su t rke poliy or techical cage whot local daily contactwith patcpatig offias and the Bank's rative lack of emphas on detailed aspects of project
_ A concluson ftom this is that suervision hwould stike anapprort Wbaance betwe asdhc to prgm gols and objectivs dermined at appraisana die needto a4jW pocFto whih eqaimw during I np -- -- - - Scoon, recut
dranv tion to lack of adequate Idicat as t what targes projecto_Lwstd mept; ip Io abndc of surh ojets, pebenrce for bscome rafie subjrctin.Leas, past ptbdado ad lho projecW ha" beena cdtcized fDr 10UfCf flelE visi during

supvisn, and the absece of a tecal presence _ the Bank In Jakata I see tohae ds coordintio with other dns In key aqsecs of program I
2.9 Ohw doom. Conmunty halth nd urionmp rogms ha reved tecncaland financial support from al th m ajor donors. Sevra acivities financed by USAID, theWHO and UNICEF durig the 1980s are epecily rela to ths projec The experencesof the USAMD financed Copr s Health Progrm-Prvisc Speic (CHIPS) prjectawls provides lessons of use to tho cumre projec In partlar, the evuaton of ta eflbrtpoints out that the sustainability of efl to deole health planing and budgeing to theprovincial and W lvel rquie systematic and intnive eft to adjust tems ofreference and roles at the centr lvel. Mreovert, building imped manail skills at aUleVes is also Wey to succef effos to bIn_ove the spcificiy and quality of loca communityhealdth plas. The CHIPPS proje also shows ta chanig tho channeing of funds tokabupte and proviuce levd prmote grat local involveme in program quality. InaddWion, USAUD is prvMidg support to an et to crese tho caacity of NGOs to provvitechnical support and additonal sevices to complement goverment efo which woud be ofuse to the project USADD also ficed a program of support to the five Schools of PublicHealth durig the 1980s whih prwvide a base for his project's e t to Impro the qualityand rdevace of commuity healt and nuition traing and resach activies. WHO has alae and varied program in the halt sector, Including support for health planning at the centlevel as welU as major teccal and finamial suppo, in collabion with UNDP, toward thedvopment of the natia Safe Motherood program. WHO has also recenty sponsored workto assist cifying tho staegc direcoas for done S hools of Pulic Health of directrelevance to this project. UNICEP has a long trdiion of iay ntraining Itaditnbirth a_ and has been a pmay spnsor of community ntdri and nutdtim edaonoffrs In Indoneia. Moreowr, its toehical and financial support for the expanded program onimmi911dw played a major role in _o 8s rdative sccss in hse programs. Morereendy, UNICEF has begun to work on te modification of local and m)anning and budgetig techniques and is wodring to imprv apoache to trang traditional
tjhCh a _lnu.
C. JM WoS i BAN SmAUGY Am RoLz
2.10 Raionle for bank hJol it. Involveme In the heat sector i central tothe Bak's human resoce and poverty alleviaton staeges. Further invs In commuityheat nd nutrition wvill f te the replicatin of lessom leaned cnernin the ecveneasof ptilar nutm ton and heh a itervent. They wWuld also hel to improe theproduciit of cuet staff and filides, nd pculayin th Eas region, hp to supplythe adtona mapowe, fit n redlatd transport ad communication y tat aroneeded. lve in he process of acheing more effective local hath intvenin wouldprovde a veil for diaoge, with MOB and Bapns on the alocaton of deveopmen adrcurrent for community health and nution programs.
2.11 PtIjeet State ad C _ite. lhe proect is a direct fow-p to the SondNurion and Commuity Halt (NCR II) and Health Mapower prjec, which each asistedin egt g the desgnl and impnt of service ddivery trgi and the on-gingTd. Halt Project which initiated a provinceased appch. As such, the project wil sistin the prepraion of stategies and intervntion prgrams which go beyond tadiiona unifomappoaces and tu ebl the provinces to address dinctive bigh piorty local community

-16-
health and non problems. Halth and nutritio educatio actvii In CNN M wil bedesigned to etod posiive lessons lerd in NCH I. Staff dvlopmnt efft at theprinci level wil streonthe Iv tga , utilizig schools and ciites supported underHeath Mpower. Projdct financing wil be desiWd to apply lessons learned in the ThidHealth prject, which has succsiully with the devolution of responsibiity forpreparan of health budgets in Nusa Tenggara Barut (NTB) and Kalmn Timu, tocommity hedlth and imon program bugets In parideipang provinces. Ihe project alsobuids on lessns leamed In projects supported by ote donors, giding partdialady the'Comprehensive Hath Improvement Program - Province SpeciflW, (CHIPPS) a mjor effrtto ean about on and Improved health planing financed by USAID and othsm.
2.12 ITe project abo complements the recendy initiated Fifth (Famiy Plannn and SafeMotbedo) Population Project. It will build on the prparion of provci Sa Motoodprogrm and wtil strengt refeal stmuctures and suWort sysm to enable midwives tainedunder Populato V to accomplish their service delivery amctions. Morwver, CHN IM dshresa progrm_ic app roh tothe development of specific annual m entaon plans with tbeFifth popultion project Anothe common intere in both projecsl concersm the role hatImproved local Inomation on famfly heat status mIgh play in Imroving accoubiy forhealth and family planning program performance and the development of better indicators ofprogr quality and readL

- 17 -
3TIlE PROJECT
A. Noi= O,ncVs
3.1 The goal of the project is to elevate inat, dcild and maternal heath stats byimproving the pecificity and efectivees of Safe Motherhood, Chld Suvival and Nuitionprogms, iluding health and nfitoneducation, the provinces of rlan Jaya, Ma , NusTeggra Thur (NM ), West Java and Central Java. To achieve these objectives, the projectwil assist these provinces in the preparation and imp -mn of strategies and hteventionprogms to address high prority local ommuity heldth and nutrition problems. Lessonsleaned in the initl phases of the project wil inform subsequent steps to expand coverage.These objectives would be accomplished by (a) building provini capacito pln, implemnand evualu progms in each of these areas, and (b) by strengthening the capacity of the centrMnstry of Healdt, priarily the Direcorate Gneral of Community Health, to sutpovinal efonts. Plnng and budgeting procedures would be modified, building on lessleared in the Tid Health Project, to ensure suficient flexiblity n the maagemt ofresources at cenral, provinl, and kabupam levels to adieve greater speccity ande tveness in health programs.
3.2 Targeting those most in need, ddined by economic, epological nd nutinalcrteria, is a key feature of this project. Ther , provincial proposas have been designed topase specific kabupaten, based on inicos of need, through the six years of the projectperiod, as maized in Table 3.1. TisD approach allows for the devedopmnt and analysis ofnew appraches to service delivery and pU interventions on a smaler scaein loca settigs, prior to exeion to the provinci level. Adjus in planns andbudgetig procedures, and to the reative priority of and apa to pgram aluation win
ilae this approach. Targeting criteria and methds will be Improved troug the coure ofthe project.
B. PAoeCr DESCRIUDIN
3.3 The project consists of two major compone nadd g provinci and centallevel capacy to develop and suppotprov al and kabupaten comm y health and nutrtpXroms. The Pincal Sere Delwey and pacity Dee apxent componet comists ofinterentins in Safe Miotood, Child Survival and Nutrition in West Java, Central Java, knaya, malulm and Nusa Teggara Timur (NT). By fcusing anon on the Eae Islands
this sectio wod contribute to mor equiabk distrbion of sectra resources, nd help toclose the gV in the availability of health facilides and staff betw th Eaen Isblands andJavalBali. In West and Centra Java, the prect would hdp tD ehan the quai andeJc1es of the infrstrcwtr and staff that are already in place, and, if succefu, would

- 18-
have reut measble on a naiona scale. Codatig the prject in more developed,rdeatdyively _ and dsly popuaeidava at h sme tme as In the poor, cualyhetroge s and sprdy p d Eas als afford th Misty of Heth anopportuny to demonstrate its capaUciy to mo perfbman in a range of setting.
3.4 Achieving more decive co_mmuy hel and nutrition program rests wIll_cmi the adaptation of cuent modls of service ddivey, ig especally th
pOsyadu d pkms level opeatig pocedr In each of the prvinc. here isad ab denc 69 pfand p _uat } level halt Irs are every able to
defin ad Implemen more effctve progm in loc setigs. However, thee is lit qudestionthat they would also benefit firom addion sklrls in health planing ad manaent, as wellas more fiequn and new forms of eci support frm the cent level. Moroer,establishing th flexibility ta would promo loca adaptations wl lo require adjh_u inaspet of th central ad prviniawa as wel a esblishmentofew c aat the centrl lvel. Accogy, a Cnral Sapoei ad Cqdy Buldig component wi helpthe Diecrate Gena for Communty Healt, the Center for Halt Education (PKM and theCete for Heat formation (t ta) to build thei cacies in policy develomnt andprogram planning, the proviion of technic support to loca levels, and the conduCt ofntrprovinlcal prgam and rearch. Steps to Improve the qulity and rdeeva of education
for healh and nutrition staff would be tok, and three lotd surveine shes would beestablished.
Poln SeDelgivey an Capadty BUding (JS$108.3 mMion idng tng e)
3.5 Each of the five prov in the project has prpad a specific program toprov service deivery and reltod ttutiona pacities, in g staff developma his
componen of the project is thus made up of ea of the fl provinc pogrms. Ane 2provides a detild description of servie ddiy and cqpaiy buidn ex to be nin the first 18 months in each of the five pvmces. All of the povin proects wM followa "leam by doing approach to the dervepmet of the itevento packges. Moreo, eachprovnce will, during the first 18 mts of prject Impi enge In detailedprepartions aof particular bvens nd inate staff development and £t actvienesay for Imroved perman during s years. Ih flloing sctdons providea brief overview of each of the five provii projects, fusig fst on sev delivery andsecond an capacity buigf oft . Ana I pwvkles ba d gwuinformainon on each of teprovine. Amnex M provides an overview of the distbutn of project costs acro servicdde y hiventon caegorie and by province. Tbl 3.1 bdow pres a summary of thephaig of project kab tn by yea.
3.6 MTm provincial compon also lude a hea* ad ntion edwatoni which wM enable pvinces to adapt media matals to loca needs and
conditis. This will be copishd by prvdn provin level Centers for HealfhEducaton (PIM) inis with a media packag prqoed by the contal PW In Jakata Thmedia pakg wi include par y executed media maeals which focus on safe nd ,child suviv and nutrition. Provi wi need to adapt materal and produce them locally,fDoowing pret4et and resions da e inoD account locSa acndkii and hiternons.Qualiative and pacptry research dies to gathr formative data for prga planing andmaeias devopment and mea trcking studies to monior progam aeecution commonactves acoss te prvinces.

-19 -
Irian Jaya
3.7 SvIce Dd y (US$20.1 mlion cluding ge ies). l view of its size,isolation, rdative povety, and sparse poputi, the ajor hmmdiat dbcha for Imrvingcommunity healt and nutriion In ua Jaya to expand the nework of health faidiies adstaff to mpwve the accessibilty of sevIces. he devdopment of afordable transport andcommuncation methods to superv tho prvion of village based servics and to maneemergency refeals are also ncea. It wi also be hImtat to carefy desi, withintensive participation from concned loca grups, culuray approprate methods forImpoving birthig, child care aduron behaviors. The dominant fat of the hlan Jayaservice delivery component Iude the construction of ne health centers and _len andconstuction of six nusngiwifey chool and a mu-stram acad fer toe developmentof indigenous heath mapower. Inovative medhods of extending outrh of basic serices toovercome geogra phic Isdfon I ing the povin of ga fi ng (US304,000) forsporti NGOs in the provision of svies woud also be developed.
3.8 As regards s m h , _ s has been placed on n of shcentes at the rate of about 35 units In each kbpam, Icluding provision of ddivery rooms,traiing and sueviso of newly recrued br th _, widi special nn D ciurdifferences between differet part of the prvince, and malaria contol. Complnng theseactes, effos to Improve dd nal (US$12.4 mllion) cive c wrl s such as twohealth centers h-paen faclitis per d n and housing for staff. In addiion outrachservice will be exended thwough Inreased foot patrols and use and o f tho costeff nectivene of the flying doctor modd of exdig servies t remote aa. The prvincealso proposes to conduct a deted e ln of the rdative costs and effectves of malariatreatmet as compared to prevonti pogrm por to pvci-ie imp o ofmalaria education. Effors to bywma*ou w (US$0.7 milion) in laya wil focuson nuition ducation and inter-sectoral oinilon. hese wil be based on the rests of aprvince wide nuitional statu and dietary survey. IDD control actvits wM be tagt toareas of the provincesow to hae the hiahest prevaenc dan Jaya plans to contruct andoutft a media center duing the first y of 1h project as part of its he" aaconprogm(US$1.0 million). his woud conto sgfl y to efficence and Impoed nand produn of media pakages produ at the centr as few f t ar avalao locallyfor producton. Prvncal healt education staff will reive tehal d t goverseas on audialW ad media produto to compleme t invest_n n adbuildings. A Health an N RonReshFund, to be m ged by th provn planning umitwould be used tD eiu the applicatio of epetse in ethography, ahpoloy and othersocio-utural senc to the developme of specific service dlvery and promotonalactvites.
3.9 Capacty buid (UJS$1.1 milLn dg Ies) klan Jaya wouldfocus on three major effrts: (1) iuprvem t of capaty for loc p adpi anayss(US$2.2 million) throug t prvision of a long-tem advisor In epideigy and healtplanning and a relaed taining prgru, the of local monitg and eautonoffices at the kabupat levd, and dto h of the Heth and Nution Resarch Fund,(2) step to trghe cowdola St NM he mangemnt of aBureau and the development of a gmrnts ind of about Rp 100 mIblion per yea to enorgloca NGOs wh now provide services to about 25 pecet of the pouaton, to improve orexpand the reach of their services In hard tD reach es, and (3) a ma*or St4ffDeWop

-20-
(US$12.1 mMion) progrm basal on the deveopmet of a multi-stream academy to providet gtan oportunities for lly rcuid l1aoraty anaysis (190) asIstatphamait (185;195 nutrition asstt and 290 anrn in curricula to be deveoped incollsboaion with the Cnter for th Prsoe ang n Jakarta About US$0.8 millionwould be used to stengh Pojea OrgwaiUo ad Maragew. Other activities nudefelowshps for local and ovesea training, and oational resarch to addess policy andmanagerial issu. Major objectivs of the acton research program wil be to bring medicaanthropological expe to the qgtion of how bes t promote improved safe bith andnutitonal practces among indigenous peoples. in addito, a major efort to update curnt dataon ntritional stats and to map odine diciency would be undetaken
3.10 ServiDivery(US3.3millionincluding congeies)Muku alsofacesjorgeographic obtals to the development of cnmmuniy heath ad nutrto servces, in additionto shortages of facilities, staff and epmnt. Constraints in the recruitment and _of fclny skilled adminstrtive staff are also appt, and costs of aport aresu.ity highr dta in oiher setigs. Srvice delivery actvies in Maluk. thoerefreemphasize the impemet of basic services ntough more carefil analysis of the geogrhic
adulr conditiu among the isands, collection of baseline data and organzaton of sevicedelivey around groups of idands (gs besr) and improved access through proviion oftnsort The major iems of e x p_e for upgmading services woud Ilude rdiablitationof health ctes, the provion of equipmnt and obyn beds for health ceters with beds, therehabbliatst of subcwfts and the pwovion of addiion m c equipment for sub ceters inremote areas where refeal to the health cetr ad hospitl level is rarely eible. Th s*moihe*ood (US$0.9 million) progm would strgte h exsng delivry system fthroutraining traditionalbirth n , Impoving midUwife deploymet nd equiing nd Iovingtrport and referal syom. Some op nl research directed tward the cost-effectivenssof atrnative MCH pwaches and etbnograpblc studies to refte health edu atati be cred out In the first three yeas. Impvemt of basic aW suiwal aces (UJS$0.6)will involve coUection of basn ifrmation, and training heth cene staff in suadardtreatmn regm . These altnates will be Integrad in the imp l schdue foryears 3-6 of the project. The curaret mix of basic naIon s s (US$0.9 million) would bemainaine duiqg the first 18 months of the projec while dy eseblWbng beterbaseline estimates of need trough provicwide surveys of the incidence and prevaenco ofPEM and IDD. Ihe survey will allow me focused targeting of programs in the latter yeas.
Caton tnresearch will be directed at issues in IDD, the role of agriculture in nutitioainterventio and surveiane. In hAe ed&caon (US$0.9 million) Mal wll esblishcpacit adapt draft media pakages prodced at th cntra level to tho specifi cnfound in Malu. The contet of the campags to be dovdoped would be drmined in close
coodw the Vacffcation of tho safe _ohwhood and child survivA itventionStseg to be designed in the first 18 monts of the pojct.
3.11 Capaty ilding (USS 13.2 millin inue of co ce). Because of thenazed nate of the Ii designs of the provi Safe Mtod, Child survival and
Nutina Imprm progras, and grwing recogniton of the need for gater Vsecficityin the progam plan, Milum would trea the buget Itms for all pu and posyandusevies as subject to during tho poject. The conduc of a seies of dealedpanning cises, including prepaion of maps to assi In Identificaton of sites for the

-21 -
devlopmet of heath centers with beds, tcha assisutce In th devlopment of trauimaterials and the develpment of more efficientd dbe conducted by tho project maagemet group duing the first 18 months of the prom. Tecosts for the impleme of service deivery actvities, nluding for additionalfaciities and equipmet ae to be as a Prject Daevopmea Fund to be nmaagedthroug Project Organion ad Managemnt (US$6.7 milion). SAfDewelpw (US$4.8million) is another dominant fatur of the capacy budlg s pon for Maluku. At thecore of this eoflrt Is a plan to build three nursing s hools In TW, Masobi, and Ambon. ITetaning progms wil emphasize th adaptaton of core curicula with conent developed forspecfic arvs of this diverse povie. Surveys of iodine deficiency and on ethography (Policyand Prom Development US$1.7 million) would be icroated Into emergi servicedeivey pla. In addition, qualiiv fidd sdies will allow the province to adjust its heathplans to loca needs. As in hian Jaya and NIT, Maluku wil seek tecal assistance inplanning Interventions at the gugus besar level fm a long term itational consultant inepideioloyand heat plang.
Nma Taigpaa 1mu (NIM)
3.12 Sewlce Delvery (US$19.3 million ncusive of contin ). Service deiveryinterventions in the N1T project (US$19.3 milion), will focus on improving service accessibilityby improving transport and building on the role of loca heth care provides. This will bebased on an evauation of the role of NGOs In healt sevie devry, planned during the secondyear of the project S* modrh*ood (US$9.5 million) actities aim at bprving the qualityof service though pron of equipment, fmrher taning at all levels, and provision oftransport. Manals and form or rng ali levels of service povs and ficaton andrevisions of supervision and case _ pracdces would also be imple d. Theseactvitis ar partiary aimed at strengthening the referra system for obstetric emergency casesamng health centers with beds. Tho chid svW swtvy (US$4.8) miion) mphasi
training of health center staff in the area of e gdemiology and disease surveillance, caemanagement and cmunit patcon. Resources are also locaed to innsify outreachefforts for the remote are., oncurly with impog th cold dain for vaccines.
Ma Ii of outreach acvs wM follow a study of posyandu permace In the secondye of the project. To bnpdw nwrlosals (US$3.2 millW location pecificnteventd for PEM will be based on a study of food cmption pate in the first yearof the project. Empis wil also be based on use of Loca Area Monitg (LAW formanagemt of nuition intervento. A basdine on lDD ms wi be used to target lodinecapsue distibution. Nutritonal program designs for interventons in three subdisticts in eachof he distrs will be based on this wor The mntrition progam wil also include theoperational research and extenosion of modd organizatona intervento. Hlh and itolkmecon (US$1.8 million) would nc on s the ddivey of heat mges
to remote areas and hard-to-each audiences. is wMi be accoplished through increased useof audio-visu£aqupme and prvsion of wireess s to remote ar for public educationthgh sm group setting. A mae_ _r would be appointed to assit in thedevelopment of ths progrm A related effort wil involve taining leader in health educationmethods to enhance i ona outeach dbft at the ommunity level.
3.13 Caat Bulding (US$6.3 million) stheo e use of moniorng ad evauatona a tool for defining intven and bpoving program effecie. This wOuld includethe tbmen of a Monior and Evuation Officet at the kbupa le, on a conact

- 22 -
Tabb 3.1: HDOONESIA TD Co_my AND NmnUwN PRoJcrProjet Raft by Diatrkt is
*M ISE Iq 1OM1O
mRw E g §_
l I m m U|
la Kabupam thot an oAt iaolmh in dW paujea sin VAt bX ind dadInthi ta!
-23 -
basis. he M&E offcer, to be recruited from Sl leve gduates of tue Schools of Pubic Healtwould recive specialized triig In the povisin of advic and wpport to the Dokabu trothe use of both qualiave and quanttative resh tecnique, hxncug fiquen emeof conumer and sevice reach. Eah of the ohr four provices partidpadtg in theproject proposes to adapt NTrs secntionzt digown v o the basicproblems which mrg from the lack of adequate data on feiity and mortity at tho vileand kbWt lovd, the N1Tr componet also Includes an bnovative proposa tD use churchrecords to improve local taget of sces and stff tme. NlT emph ontissues and monit is also relocted in a strong resarch component Furthe, NIT wouldesbish a computrzed data bank to moqt Ileto of project funded interveions.Lst, N7T proposes a major INvesm In staff devlopment, cuding Inservic tning Inepidemiology for disrict level staf Iuin nue, and the development a mti-sreamacademy for basic traiig of allied helth povids indg lab i, andothr In a multi-stam academy to be rnvated In Kupang. Now n gmidwfe schoolswill be built in Tual and Masoli.
Cal Java
3.14 Sew Delivery US9A millio). he sviedelivery c onent ofh CentalJava projec emphasizes the mpwovement of exstig sevies with some activities dircted toidentiyiqg and test altnative approaches In the eary years of the project. Work to improve'* mothrhood (US$6.1) services will focus on the quality of serices delivered thoughTBA's, through in ith a range of taining and hdmal ientive progam.Health enters wih beds would be suect of a taget needs tsm hat would serve toguide Improved p ae of this tpe of faciliy throughout te provice. Te provicewould also e with the use of ambulance servies to eNdce the nmbers of mat ycam which are referd to lat* to be effcdtvely mangd. Ths wHI be accompanied by anoxminaflon of m gdal issues red to the halt center, its role in the real system andthe cost effectiveness of mobile health unisn the ealy yar of the project Changes indicatedby this a on will then be inpe _id more widy In the latr part of the project. CdIdswvi (US$0.4 mllioan) progrm would focau an _ g and Inmpovin the reach of thePosyandu program. Por ample, he prwject woud examine methods for ass posyandupuformnceeas wel as for rowarg vlaes whos posynd are most successl. The projectwill alo develop and evalae use of specially desgned chmneys to Impro house venlaonas a prevetve nmau for aute respiratory lness. Effors to b_1w iualoil swOMS$0.8 million) would Icude stroh thr ou cr ovidsdocted cwvhlW or District Nuaition Iaprovenwo Board at the kabupate level capacity torespond to reques for fnds from Inc aecie otherkth the Mistry of Health In addiion,the project would also support a pilot project on the effect of prie sbsuidis an weaning foods,and on tho we of nutritin education on the a IOg temaltenaO to rdinc on din cqalod plhad (USS2.1million) in Cntral Java would Icude a speial study on modia eftctiveness desidd todeemine t best media chann for deirng messages to a vadety of targt groups. Anng P 0 - I Study wM also be conducted amnng Moseim laders to Idntify inovative ways touse thi inlueia group to deiver health educatin s . The additio of several mobilecmnIcdation units would also hance nurl outrach efi-ts.
3.15 Capacty Bdg (S6.3 mllim including ) efIrs tin Cenrl Javawoud ficu on imprvn the skills of curt sevice ddWery staff thmugh bot imprved

- 24 -
as oi city and deldberate staff development. Central Java wouldlemt a lar SffDewlope (US4.7 million). A total of 479 felowships are planned
during th CNN m project for in-coy training ht staff years of ovea fellowshp Inpublic health, managemet and apldemlokoy and 24 short cur wold al be inluded.Approxately half of k uy feUllowshps aeto train nrtion asistat within he province.Posons (formai) wi be avalb for thesm asistns tD be employed upon gradu_a Tofuter enhc the qualwt of services the Poky and Progrm Dewlopomm componen (UJS$1.lmillion) would pwvide failities to support mproved management of health informadon andupgrade provkici offices. The Project Orgwaron and Managment Comonent (US$0.5mlion) includes provon for the developmet of birth and death sample regist and foractive irch an Iron consmption among pregant women. In addition, capacity builn wilinclude the design, based on an analysis of current patterns of decision-making, of a progrmto tran health centr leader in Wprvd m_aemet tchniques, and the estblimeNt of acommunity health and nutitio laboatoy in the provic to facilitate Imprvements in programeffectvens (s Annex VD).
West Java
3.16 Srvice Delivery (US$11.7 million including cotingencies). In the S*Mtherhood (US$4.3 mill) component a Project Development Fund would exam theeffctivens of dedicaed umatemity huts and other opions available to the pusksmas dotorfor Improving sfe mothehood. In addition, provisons for eqipme and train of th heathpoviders are planmed to Improve the quaty of care and the raefeal system. Additionaltransport Is provkied for toe distics in whih access is limited. Plans also include caufl
of equipmet and drug supplies, and the adaptatin of manuals to improve theseysm deloped in the hid Heath Prect to local needs. Ihe hild swnW (UJS$3.3
mili) program indludes development of Innovative aproaches to improve the coverage of thervices. In paricua, this ivolve identifying snd assi aroaches for managing diarhe
cas such as relying on the kader for diarea case identification and distribution of ORS. ThePrposa l alsoIdifie an intograted trahn package at the different levels of the health carsystem. Effots to hww io.d agus (US$2.4 million) would develop new programsfocusing on the posdu and possle co ep t strategies. In order to improve itr-seca c for nutiton progas, ways of animatig BPGD will be explored inseveral p An Ifrmation nework sudy will be carried out in West Java to dminethe range of nework avalbe for heal and maWon educaio (US$1.7 mlion). Emphasiswill be placed on non-formal and noraditional foma networks, f on the flow ofino t betee and withi commuies so that these can be utilized more efecthdvy.Hspitl dca efforts will be strengthened trugh training and mpoved mat sdvopmenL
3.17 Capacy lbuilding (UJS$3.6 million) efforts in West Java would concena onfirst, compledon of a care _l of cmt decsion making patterns at the puskemslevel adogous to that beig conductd in Centa Java (Annx 6), and second the deveopntof a management trann for heat center leaders and staff. As regards Poliy ad PrognmDeelopun (US$1.0 mllion) West Java plans to develop a segW for the provisionof seriesin urban are., and to systmatlly introduceqpm and drug managent procedurtested in the Third Health project in all project kaIpten. The Staff Dewlpmen (US$2.3million) plan includes a program to trn additid nutition ass in aU kabpaten, thepreparaIon ad intio n of a prgm of integrad heath management services,

-25 -
_mqpmt bfor health center and subeaer staff as wei as 14 overseas S2 level feliowships,10 overseas short courses,ad 24 S2 levd and 44 SI level In-country felowships in pt ofpublic healh managemet
Cetal Support and Capadty UulIdng (US$55.8 milion inlusie ofcotges)
3.18 I he go of th mponent is to that cena leve u ad agndcies of theMnisry of Health ae able to pwvide support to prwoinca d kabupaen lve effor tovroe service deivery quality and ectiveess. This would Involve changing the role andapacities of relevant prgm units witbin the Directorate Geneal of Community Health as well
as s athe capacities of the Cenr for Health Education and the Center for HealthData, with each of the affected uni expected to play a stronger leadersip role as regards PoUcyDeweopme, Plualg and Coodbalo. Specifically, each unit would ceate on theprovidng of policy support to provica proposa through spnoring techical assistance intihe prparation of provincial proposas and would conduct policy developmet work in areas,such as quality assurance, or the use of radio wco ca , which would be too costy todevelop at th provica level. In addiion, each unit would provide additonal or new Te*dcaSecs to provin and kbupaten as a way to assist in buiding captes at O levels inal apects of program planning and implemetiaon. Despite the need for the locaization ofservie ddeery shtegies, sveral tedcnical aud outsading clinical issues within each of themajor program areas would be most effectively addressed through central levl leadership.Deveopm technicl guiines for th development of pr vice and service trainingprograms fo instance, or reserh to moor n tiom-vide tends in key nuiona and heatwould teefoe be supporte by bntqpvlndal Program and Research to be conducted by eachceral unit. Last C4pacy BUd effs, including higbly selecive addiona staff positions,
1ntemadmd and local technical asstance and a sy c staff develoment program woudasist each unit to adjutD their new rols.
Directoate Geoed of Cmnity Heath (US$21.3 milion cudgo gences)
3.19 Dredtorat for Healeh Center Domdon ( JS$7.1 million includigM). he cruci management and te un in the ddivery of health sevices is
the health center. Ihe Dectora for Health Center Prmoton, wh is resoible fornational policy coning the role, equpment, and perfrmne of heat centers, has anImportant role to play In the evolion of health sevies tD fit the chaging siun. In ItsPolicy Deveopment PMing and Project Coordion (US$0.1 million) project his cenal unitwill s r annual policy workshp and the deveopment of more effctve managemente est heng management at the district level, devdopment of a commuty ursigstraegy and impoving the role of the health ceer wh beds as a refr unit for modts andchildren. The Dirtote wDI also sponsor two iportt studies during the course of theproject. Fist, an opeonal study on the role of radio cmcation as part of te refrasystem in the five proect provinces wil compliment the development of additional radiop 11 I a_ cadon capacity in each of the five provines. A second study of equal importac isone on the possible role of a second-in-command at the heat center to avoid the problemscaused by the high turv of halt center doctors. Ihe Director wil also me thedevelopment of two major sporting sies for the project the dveopmet of QualtyAsace procedbu diroeed at hmpoving the qualiqt of Safe Motherood actvies, and amajor expanon of a rado u O nenw* to promote improvem nts the rdefrsystem for the mamet of obstetic aid peditric emeagnce on a selected basis. Both of

-26-
thes acivies are nooated as learnig _ , which cold be expnd on a largerscale by GOIurces or ih futprojects. C caD newlopmet acivities i s unkit includeshort-tnm overse taining in survoellae techiqe and S2 levd training in mursing.
3.20 D irctoae for NUubd (JS$4.0 million including cotgencies). Nutritionalsttus has hImont efc health both directly and Idirey toh intcion withinfcto dise. I portac of nuton program lies In their abiity to improvenutiol stas, thus wovig healt through ability t resist the iitial ifecton andlor itgonsequences. Activities of the central nutrtion com Ivlve those aimed at national level
planng, the provison of tecical to the pronces, orgizaton and monitoring oftaing, ierov itvention programs and opeaional and applied reseach. Tosrgte It re In Polky Dewlopme and Piwnubg (JS$0.6 million) the Directorate willconctrate on the sea for long-term solutions to nuftiion problemn. Examples includeassessmen of the uti of an approach based on -nd the way In which nuritionproblems vary with dffeencs in ecology and subsequet formuaton of Interventions specificto the parac ulha and identfication of the barriers to more widespread use andffectivenss of odized salt. Linked with these acdvWes will be cost-eectiveness studies of
curnty used short-term itervenon such as Iodine capsudes and massive doses of vitamin A.Provision is also made for an anm natonal policy workshop. 'Te Directorate would also playa contnuing role in the provisio of Tedhcal SevwsbD to the provinces, particularly in relionto inon s5rve ys. Ihe progrm development actvii carried out for ntional level planingwi also contribute to the pool of sk and iormatn available to the provinces from thecental uni Policy work on salt iodization and the analyis of the link between nutrtionalproblems, food and agricultua production paterns and the use of ecological zones to planspcific nutrtion Interventions would also be conducted. hmepnwldaprograms to be funded
der this coponet iude upgrading the odine batories, of nution problemsOf low _ -c groups and a study of zinc status. The activities would conute to thepool of ills ad inf on needed for the center to fulfill its role in providing advice andteical asstane to th prvine.
3.21 Dretoate for Famiy Healh (US$2.2 milion). The D iectora of FamflyHalt has the boad objective of providing tehicd and policy wpport to the provines anddistrits to promote and sren n safe and cild urvival in ves. As part ofthe ovall acdvity, the directo wl posor several iter-sectort meetings at the natonallevel to promote of safe mothehood among other goveent depatms.Anual meetinp of proinc MC pronel wM also be hed to enable dicsion of thicalIsa in the areas of safe modthhod and ild suvival and to promote saring of positiveeperiee davloped with each of the proines. Specfic tecal atance to theprovine wil concentrw on cost-offictiveness, of imanam of supplies formidwives, and use of medi audit to assi in problem Ietficatin at the healti ceer,kabpaten, and pwvinia leves. Fnally, the diision wM conduct operto research on safemothalumd. and dild survval focusing especiay on modeds for assessing chnges in relevanthealth outcomes and stengthen its own staff capacity through a training program.
3.22 1 _Agtdnhl s_uane (UJS$4.3 million). A secom major efort to improveth Ue of outme and efectvens ifmation for dedsion making in health and ntionwod be tho etabl of two logiadina suvellace sites In NTr and Cntral Jav andoe site in West Java. As dSetd in Annex 7, these sites, to be maaged tough theDiectot Genal of Community alh with provided by GadJa Mada University

lit"* £81 fll j~ij~jjiJ~f~j4 fI tm I
iii III IP, III? I iiui)b~~~~~~~~~~~~~~~~~~~~~~4II I lit iPjfuhiIi JI'IJ~~~~~~~~~~~~~e

- 28 -
recried tchaic asl sto work with the Cer and thu Naimal Stg Committe tofurter develop the specifications, concerig content and link to dedsio making, for themoten of the infmation stm(s) to be deloped and to filta kabupaten and p emaslevel deinitions of ned In the deveopment of informaton system plans. nh Cener would alsodesW and Implement, In thei first 18 mot of the project, a progrm to emine the feasibityof employing sample t rghtion tecques at the healh center ad kabupate level tD measurehealth outcomes. Mm design anid Impleenaio of ths system would be developed incoordinato with the fidings of the asement of kabupaten and puskma level decisionmaking (se Awn 6) to be implemented In West and Central Java. A program to reform theealth Center Reporti Form (S2PT?), includin the desig of a manual form for the system
would also be conducted in the first 18 monts of the ptojec Following the completon of thespolicy developmn steps, the Cene would focus its atti on the povion of TeducSerlcand Capcly Bulding topw . Thi prgrm would conentate on the prvisonof hardwae "stems to s8Ut, f essayr, the operations of the health information sstemDin egodatos, dte Genme provded assuraces t it wod cause the Cew firHlth hbmadkn wWn MOH to caoy out ard fiandh to the Ban* afbabl stuy on
emloying swqk reAtion tchnqu at te Kabqiat and health cener lwis to measrhe otcome, revew and reWse as wessay the Heath Gent Rportng Foms (S2PP%, anddesgn and test a mwwalbfnM ofthe new rporting system pror to th procrme of omptewequpens reqir frtenew healthbynadonsystm An fiprovn Progras andReearch subcmoent would prwvide suot r t bostticans as well a systemdevelopmet pesonneil to manage the systems at entra, provia and bb_ lovels.
Cental Manpower Support (US=15.2 miio ding es)
3.25 The objectve of this oponent is to srgthen the quaity and relevance of theresearch and ting acvities being conducted in hig education wnshi areinvolved with the paricipati prvinces. In addition, the component would sppo thedeveIlment of thrOe major mw polcy sdes to complement ongoing sectoral and policyinitiatives beig uda by DEPKES. Suport for the Shools of PuNc Health would beprovided to the Unive of Indonesia, Hauddin Universit, Ailangga University and theUniversity of Dipneoo. ITe project will support activities which promote a dloser woingrelatihip betwee the schools of public halth and the project provinces. Tese acivitieincude funds for universty staff to spnd an itenship working at vaous levs of the helhsystem, technical to the provces, and joint prove/Schodl of Public Healthseminars and workshps to be hdd in the provins. TrUg felloships are to be proviedto kbbupa and provicial staff for the futher str o f staff sills. In addition,parcula support wil be prvided for the deveopm of of public heat ntrionat te University of Indonesia and un Univemit.
3.26 Support wl also be prided t tbhis component for further s hemnuri research and aining at the siue Penanx Bogor (IPB). Th would ivve fundsfor food and ntionpolicy sudies, technical and taining. Further stenhg ofthe Akad GOil wi be suprtd though this project with Vecial ate to uriculumdevelopment ad pgrdng of staff skills at the Akdemis most closy oncemrnd with theproject provinces.
3.27 Other ac es in this component relt to strenghening inservice and prerviceh trainig and pesonl procedures and pacties witin Depk. Ihe Cer For Hel

.29g.
Persod Trintg will receve spport for a range of facilis and actvWi includng sededconsuio sand novaton of budings, curriculm, development, ad training of trainers.Curriculum developmen and slected other acties of te Comer for eaM MWVr7*nin wi as recei support Finaiy, varios acdvities located within the Bwea ofPersme wil be s rted. Thee inlude vauatns of th pfomance of the contradoctor poicy, the vage midwife, and carr devopment whn the e system of lcdonadclassificatn, as weDl as best practice" studies for the disct and heatth center levels.
C. PnwzT ORGAMZIN M A
3.28 Status of Projec Peparation. Master euipme lists, location and proof ofacquisition of the sites for project in the provces, draft LCB doument for thepwrcurement of civil works and goods and ICB documents for the pocurm of goods werepropd prior to negotatons and reviewed at neotation. Terms of rfter for all
tecnc assice nd major studis inuded in the ptoject were reviewed by theppraisal mio Th amo of inrnatio t cal assistc to be prcured under te
loan-about 9 perceat of the loan amou-is confned to specides and experien requrementsnot available from local con0utat.
Proect
3.29 Te Director General of Community Health widn the Mistry of Health (MOH)would be Project Director and wil have the oveal responsibility for the project Te ProjectDiector will be responsible for decisions invoving he ovral direction of the project and policyissues. A seond echdon official has bee assiged as ProJect M2ager and would beresole for managing the lmpl of the project. He wil be acountable for alltechnical and Ie aspect of the project. Decidsions about the project wil be made bythe Project Manager, with he knowledge and approval of the Project Director as neceary.Both a -1-e and tedncaopolcions would be made by the Project Manager whowold likely nvolve other echdon H officials as necessary. An mtecoral Adviory Board,composed of echeon I officials from DepKa, Baeas, Office of A iative Reform,Istitute of Natona A and Minsy of Fiance and Ministry of Home Affairs(MOH) (Office of Regional De ropment, and Ofice of Geeral Adminison and LAutwomy) originally established through the Ihid Realth Project, would f te in oralconsultation and rdi and assit proct npldan monitorig. The A*oyBead woud conne tD serv he Tir Heath Project as well as other BanDepkescolleaboa projecs in the health sector. A Project Steei*g CmmWee, cmposed of edcelonII officials from within the MOB would advis the Project Mamger in opeatl mats. Teinvolvemnt of oher MOB staff In the Project would be conducted according to the nomastuctre and fonctionalcangm within the X Miity. The Project Steing Commitewould be chared by te Poject Me ndwould ude re from the DhictorateGenal of mm b Disease Control and Environmnt Health, Setat General,Dhrecue Gneral of )4 A Services, Diectora Genral of Food and Drug, and theNatial Istte of Health ses h and DTdo nhe Project Diector would appointTask Fre to accomph scific purposes, such as advis on research, a necesay to achieveproje objectivres.
3.30 A Project Sertat cnisting of six fll-tdme powfeols In fine, planningand mluadw od procurement, and two upport staff bas been be established by the project to

- 30-
facilitate project implementation. The staff of the Project Secretaiat will report to the ProjectManager. The SecreWiat wll be headed by a Adl-time Executiv Secretary. Tbe Secretariatwill coordinat project acivities betwee the central and provincial levels including procurementof goods and services for the centrl level, placement of staff for training overseas,administraion of project financial accounts and managing the Special Account, and monitoringand evaluation of the project. A Management Advisory group, of international specialistsrecruited as necessary would serve as project advisors, including a project implementadonspecialist for the KfW compone. During negotitons, the Government provided assurancesthat a Management Advisory Groqp, with qualfed stqff in adequate nmbers would beestablished by July 31, 1993. An organizational chart and Terms of Reference for these unitswere submitted prior to negotiations for the project.
3.31 lhe Head of the Provinci Health Office would be the Provincial Project Director(PPD) who wold have principal responsibility for all project related activities in the province.A Provincial Planning Officer would be appointed in each project province; an echelon m levelofficial from the Provincial Planning Division would be appointed to manage the provincial levelproject activities and would be responsible for both technical and administrative matters. Thiswould not be a full-time assignment but would be performed by the Provincial Planning Divisionofficer in addition to normal structu duties. Ihe Provincial Project Managers would besupported by fill-time staff, the composition of which would vary depending on the province,but would include a minimum of two technical staff, one with a strong background in technicalissues, and a second with abilities related to monitoring and planning. Beyond this staff, theproject would rely on existng structural and fimctional staff of the Division of Planning, whichwould be responsible for the adminisaon and coordination of the project in the province,districts and subdistricts. Responsibilities for the implementation of the provincal componentwould be assiged to the following office divisions of the Provincial Health Office: HealthCenter Development, Nutrition, Community Participation; and Units of the Provincial HealthBureau: Mother and Child Health, Health Education, Disease Control and Health InformationSystem.
3.32 The District Health Officer (Dlokabu), assisted by a Monitoring and EvaluationOfficer, will be responsible as Pimbagpro for managing the kabupaten level project activities.Durlng negodations, the Governent provded assurances that by Aprg 15 of the fiscal year Inw*kh project actvies commence in a kabqaten, commencing April 15, 1994, It wouldstrengn the planndng, monorng and evaluaton capacity of such kabupaten, indcudtg, tfrequied, ppoinng a qWaled monoring and evaluation officer to the kobaten Healthffice. At the subdistrict level, the puskesmas-in-charge would be responsible for project plans,
implemention and evaluwtion.
3.33 Implementation Schedule. The project would be implemented over a period ofsix years, starting April 1, 1993 and ending March 31, 1999, coinciding with Indonesia's fisclyears. A project implementation schedule is presented in Annex 13. This schedule, as well asthe detailed cost tables, will provide the general framework for preparing annual implementationplans by the Director General of Community Health and each of the participating provinces,which will be reviewed by the Bank semi-annally, coincident with the GOI planning processand fiscal year. The Project completon is expected to be on March 31, 1999 and the loanclosing date would be September 30, 1999.
-31 -
D. PRO=cr PLAW, EVAWAON AND S v STRDIY
3.34 Annal Plu!. The paradon and eiw of annual plans for each of the majorintervention areas (Safe Moterhood, Child Survival, mpwoved Nutitioal Stau and Health andNutrition Education) by each of the pticipating povinces wil be mhe major veicdle forsupervision and evduation of the project. Each prvince would oqanize these plans into asingle CmmunIy Health and *altWon Progran to be Implemented in the subuent projectyear. Plans for the fist 18 mon of the project were reviewed at appraisal, inuding theidentificaon of item of ex _i which would be available as Prom DelopmentActivities. In each project year, the dotau from participating kabupaten would prepare specicplans in each hiterventonarea for submisionto he Povincial planningunlit, at least 30 workingdays prior to the fia preparation of the prvia DUP. Ihe pwvinci planning would,in tun, prepare a summay Annual Pvhcal Prject Plan which would include summarystatemnts of each kabupat plan and an overall of th project. Anex 4 providesan initial suggesion for the content and structure of the draft prvincia plans. These planswould be fowaded to B _p and MOP for rview pror to an annual Project ReviewMetng, to be attended by al pardcpating pvinces and central program uni pdor tofinaization of te annmal DIP and the allocation of INPES. This wbch woWdcombine proposed DIP, IPS and Bank _ , would alo be available for Bakreview and come and would form the basis for tho prepaon of Annual w qpPlan by the central Project Secretia he format and timing of this annual procewould itself be subject tO review and modificatin durig the project.
3.35 aon oftu an Reech. A codinati body for rem ch andstudies would be established to nor the quality and completton of project related researchinitives and to ensme ther mely approval. Specifically, the Center for Resrch andDevelopmen (Litangkes) and the D ireate Genal of Co_mmuity Halh woud form aRearch Review Team whose membesip would iude a of he ccommnity and e e of th cental program units. This tem would review andforwad for Bank approval all reseach proposals above US$50,000. Durig neotdaiow, teGovernment provided assuc ta It would prepare and jbnls to the Ban* by Agw 31,1993 for Its pprowl procedr and dnsmble for establishig annua research programpri es uder the Project, and there, carly out su*ch rearchpogrm In acodac W&the 4 Frovedprocedus and tbm tbk.
3.36 IndInosPeoples. eopuladonoflraya, MauuandNIincludeedhicminori and tdbal groups whos itert the project dsoul respect and prott ITh proessof prqmig kaupa and prvcepifc comuqt heath and nutrition progra,including the use of qaiative and participatory rsach to dentify halt problems, woudafford opportunities for assurig ta the views of these groups ar consid duig project
The pwvision of resores for the conduct of qualiaive reearch to kabpatlevel Monitoring and Evaluao offices would faciltate the applicaton of participatory planningprinciples to the desig of specific healh and nutition i In addition the Heft dNutrtio Research Fund to be implemented in ran JIya would be employed to assure hincorporation of cultual and pepective on halth nd nutrional behavioamown indigeus peoples into Annual Prvincia Pfoposs. Dri negtaIs, deGwrwet prov4uanw tw ea pject provic and _Vasen woud preae andflauWh to the Ban*fifr Its review and conet by Sember 15 hi each year, cmenci inSember 15,1993, audetldpwspr l e enatis ofprojt actiies. Assuranc

-32-
wfre also proided that sch pans wd ldWe th reoadto, agreed by th Borrwand the Ba* qfIwahrpooga and ethgahi sui cwie owt In the pujec prohneihabitd by ndgenous people, ard meaures, satctoy to he Bank to ensure dtatgo wnw taages and non-gemad orgaosengaged In e deey of muyhealh and ntrin serias to Wdgenospeopl take Inofoi cnsderadon te prfrecs oftese benicies Assraswerealso provde at prf e would be e(ed throughthe Gowrnm I's edstg conslaion mecims.
Monitorn sand Evalaton
3.37 Montrig and evaluation of project activities would be key to mut efeWtveimpleentain of tO project. luee major types of monitoig and evaluation would beconducted.
3.38 First, the project would monor and amnually review progre toward theIsitutonl deveomn objecives for each of the provinces, the central program unitS and theSchools incuded in the Cent Manpower Support compont. Me broad focus of thisa_essment would be on the project's conution to achieving a shift ftom input-based tooutme and output based planning and evaluation for service devery progms in theparticipating prvine and program units. At th central level, ihe revew woild focus on thequali of the plans for the use of Program Developmn Acdv, or innovaive acves, forservice delivery including a review of the basibilit of the approach to asing efetveneproposed by the prvn. This review would be praed by the centra program unis. At theprvica level, a quaitative review of the availabii ty and utility of techicalassistance prwided by the Dieorat eneral of Communy Health would be preaed by theproject pwvinces. ese uatins would be summa in narrative form by the centraP3rojec Secart for disuon during the Anmal Project Review Meetin between the Bank,cenral nistry of Healt, Bappen and the participating pvins. Ihe objective of thisexaercise would be to attempt to acpate any woorpWd obstesto e impII of pvince specific plns, and to id possible solutions to theseproblems. The review woud be held in councton with Boank supervision ission. A centalfocus for this review in the fifst and second years ofproject impI at would be on Dhecontent, fomat, and qu4alit of the sevice delivery plans prepaed by each prvince. A secondarea would be to assess fte developmt of kabupate and level analyses of progrme ivens, udgthe Ocollecton and use of data on local needs for targeting and evaluationpurposes.
3.39 Annal Progres Reeorts would be prepared for each of the five provices andthe central program units, and submitted by ihe Project Secradatt the Bank for revowi prito a regulady schduled Amual Review mission about the mid-Point of each project year. Eachpln would be monitored regulary accorig to the dates agreed for each of the actions and alsoreviewed amnmually. Mning woud const of mesremnt of progress of p w aat ofqupment, transport and matls (icuding t materials) and provica distruon,
utilizaton and . The amnmal plans woud Inclde, for Bk review, a list of thebiddig packages proposed for pmsM in the s year. DurIng negotatons theGornwwnt proded asrancs t each of the Provina Planng Unts In te ProjectProvis woudd by Setmb.er 15 o eadh yea, commcing on Setmber 15, 1994, pre_proge. - -nprogress reports h would be revewed by the Project Searit and
fed to te Rank J It review and cat.

-33 -
3.40 v tmanCeE ion. An evaluationoftheproject's directImpacton matenor infn m i not feasible because multiple facr beyond the scope of the projectIlluence health and ntiutionalss. However, a principa objecve of the projeat would betoD improve tho avaibilty of key oupu and ome ndicators of health stt and service_ibity and utlization indicatmorsi amual review in each of the five provinces. Rae
than rdey on ad hoc suveys for this purpose, the projec woud include a program to strength capaciy of SUSENAS to collect anual data on Int mortliy and Its major co
erinat, nonatal, and inf mortality) and (Idrec) etmates of matnal mraity at theprovindallvel. Duing negoiats, dhe Govemwprvedarnesm da twoud,flaxashto the B1nk by July 31, 1993, a pln, saftLwv y to the BJank for the montorbag andeladon of the Project, ncluding. (a) die medlogyofor the apcin of the Boow'sMata Economic and Socal Suwiy MUS J) In the ewuadon of ProJc, andlb) prcedue for enswrng the eRcw monitoring and eluon of the real n of thebenf oftheProjea in regardto Indigenouspeoe in theprojectprvWnces. The same swould provide kabupat level service utilizaton rates to auist in project monitoring. Becauseof the liHnkges with the measrement of conmption and inome indicators in the SUSENASdata set, two special studies of project processes and reach would be conducted at least 6 motspri to die scheduled mid-tem review and 6 months prior to the project closing to assist in theanaly of project impact. Ad hoc surveys desgned by eah of the provinces, such as effortsto map nutitonal deficiencies, evaluate costs of alterative alarm and transport systems, and
vluaos of meic audits of mateal deaths would also contr to monorizg of proectAnnxm 8 provides a listing of Mlustrative perfdrmance indicators to be used in th
evalaton of project performance.
3.41 Mid-trm Review. Given the developmental natume of the project, a mid-taneaduaton wold be essential toDp the sbseque years of tie project. T review wouldalso provide an opportunity to expand successf element of the project, or to cancd thosedeemined to be less ective thmn originaly desgned. Dng negodons. the Govwntpovidd asawce ta It wuld 0) by Semxber 15, 199, prware and jlAh to dhe DankAbr I pprowl a planfor rrying out a mid-Werm project revew, fdl) by June 15, 1996, ca7yow, in c t the Bak, a mid-ten Projectarevew pu n to such qWrovd pa,and 111) hreore, prpdy take aU such s reod as a res of such mid-tenreWiew and w*kh are requiW to acieve the ojecives of the Proect.
SUPqVISIo Stt
3.42 To facilitate close interacon with Provincal Planing Units, the Project SecreaiatIn Depkes, p and with the diatg Steerilg Committee, as wel as with othrdoors, de Bk would conduct semi-annual review of project hnpi through asuevison mission around October of eah year at an esmated cost of 18 SWs ad a smalersei-annud suevison mission in April of each year at an avrage cost of 9 SWs, for a totlof 27 SW8 for fidld supervision anually In the fit three years of the project. In field thesemission, the Bank would draw on a panel of Senior Policy Advisons who winl be saected toensure connuity and strxmg working rtonhips with the log-tm contamnsbased in Indonesia. Th Advisors woud include Indonesan and inteaonal ts. To
_ei" p lwvSsexchange of experience, the larger Annual Supervion would be hostedby one of the five provinces in each year of project impl ti The other povinces andconned central uni would be invited to present project durg this meedng. Agnda and the topical focus for each Annud Review woud be aged between the Bank and Ihe

-34-
Proj Sral-dat al ammcssd at ut 3 mohS pror to eac meeting. Addtonasuperv y vis and support would be provided on as as need bads houg the life of theprojec. Annx 14 provides a npla for he Project

-35-
4PROJECT COSTS, FINANCING, PROCUREMENT
AND DINBUS IS
A. COPS
4.1 Im tot cost of the projct s edmated at US$164.1 millon equivalent (ip 326.9billion), Icudicng g s. To esimad costs by projc ompnt are summaridbelow in Table 4.1 ad by category of aepend e In Tabe 4.2. Dale project cost by year,purpose and componentsar gv In A 9.
4.2 Basln Cots. BaseW costs amed at Nvbe l9 pr. Ciwork co are based on avea squa mter t costs in th provinces frgOvernment buid . Th cost of land Is not Ided Inine aben cost. FuPiu costs arebised an list of andad localbl avaiae wt , and wh s werot avable, on10 pert of rd ed ivl work. Medical, offic equipment, boats ad v*ls costs are basedon current prices for simila imported or locally availble lthz. Jutructoncl materias costsa daived fom prices curently bden paid for silar im under on-ging halt projects.Costs for ntumadonal nd It-country c_uito are basod on guidein foraqppropriately qualiie expeit. Cosw for reearch and study awards are based on recentexperienc from compar-able techWnical of odhe health projects. Unit cost for in-conry fellowshipsrn fm US$600 p proram fr hort-m d US$20,000 per prognanfor log-tem flowships, and ovea feowsbips are _O at US$10,000 pe prgm forsot-term ad US$60,000 per progm fr lon-tm felwhps. Short-tm n-coutrytraing cost vary widey depndn on th type of trainIng bn given ad its locaton, andavag between US$9"40 per traInIng day. Ie ann fo projec costs ha beeaged bete fte Bnk ad the central and prvni Dps. Dmg cot wae bas onupspdce whodula. Recummt cow am baW on standad govaumallowan for salary,honwraIa trvel pe dem, O&I ad b
4.3 Cntq ^Ien Alswai. Physical (US$5.1 mi represt3.8 paerut and pHoo co _ JUS$24.7 mImo) 18.4 percent of the t basline 008c .Physical of 10 peret hae been alwed fo c"i wrk, fbr eqipment,boats and viddes, S pacm fw 1brftedond mmater, and 0 percent for all ote caWore.Price co Snt es hae boeen cacul at a procd incese of 6 pecen per yea for localcos and at 3.7 pecet pe yea for bip cos for all categories.
4.4 Frwp Exdia Comb. FPip Ukag Cos are eosmated at US$64.6miion (esnting about 39 percent of tot proct coos) ad ar bsd on a dd analysisof _Tenditum under dsmi proet in In10n8ia. The foW esang percentae areesdmas follows: (a) c works, l "Irnlture hnluctond mateas -30 percent;

Table 4.1: Flow Cm SumMAY sy ComFoKmqf
s TolfcPo Bo
16 § TolUl Loeid FO' Todl EBuo Cosl8
Sdo aw ;=22,763.4 19,143.3 41,906.7 11.4 9.6 21.0 46 16Cbgd onwivg 22,763.S 11,109.9 33,873.4 11.4 5.6 17.0 33 1314 notOndWAS 10,894.1 1,998.4 1289S 5.S 1.0 6.S 16 5Hie od 4,316.7 7,531.2 11,847.9 2.2 3.8 6.0 6 4BubtotaSl uvicoDdiuy 6D.7.7 3792.M M520 Il 2u Sp M s
7,399.4 3,817.0 11,216.4 3.7 1.9 S.6 34 45,689.2 10,706.8 16,395.0 2.9 5.3 8.2 65 6
30,320.8 15,327 45,623.S IS.2 7.7 22.9 34 17Subeomlo Caty Bod 43d4g9.4 29.825.5 732L4 M9 7 2!
1LCmtal_t8 91C!1. P_8
12,614.S S,1SI.7 17,766.2 6.3 2.6 8.9 29 72. TedlmEdsfqoe81iDtpce8 29,184.0 16,880.0 46,064.0 14.7 8.S 23.2 37 173. J v il pro 6,985.3 2,502.4 9,487.7 3.S 1.3 4.8 27 34. C b g S,830.9 14,S74.6 20,406.S 2.9 7.3 10.2 71 8TOW Cmd" hm . M 39108.7 9.723 2u m !M a I"now B CNN 1S8.761.8 108,717.0 L 267,47L1 ZL HA INA
PhY-d 1 4,530.9 5,666.6 10,197.S 2.3 2.8 S.1 56 4PMoo Osli_ 34,981.S 14,248.0 49,229.S 17.5 7.2 24.7 29 18Tdd ftj 198,= 12431.63272 I2WL 9 w 31 MA 1L I

TAbl.4.: SummA or Pa,oJr Com w CATRm or
s Ttal:LaW TOWla w FO Po TOWd81 costs
L wasmm CostsA. Cii Wt od8Now 8mldine 26,403.2 9,901.2 36,304.4 13.3 4.9 18.2 27 146517.0 2 . 8,960.9 3.3 1.2 4.5 27 3
D. IF -Vub81,509.7 566.1 2,075.8 0.8 0.2 1.0 20 1god mie" sqvhn12,628.0 35,2.0 475,880. 6. 17.6 24.0 182,349.2 10,571.6 12,920.8 1.2 5.3 6.S SS _IodVdiles" 16.486.9 46389.7 6866 1. . 1E a24 IF W-1 62,9761 C. hm& fia ms S,433.1- 1-,7.0 7,'175.1 -t12 D. T Aodst_
F coneawa 1,369.1 12,3 13,691.4 0.7 6.2 6.9 90 52,402.4 .6 3,003.0 1.2 0.3 1.5 20 1Subtial Tol A ~~~~~~~3.771.S 1 16.644 19 6S 84 1 L1 F18,3840 .0 0 2U,21.0 Z U 117F. Tnio-JgOvaser_ 2,041.8 18,375.9 20,417.7 1.0 9.2 10.2 90 814,M.8 2,599.0 17,326.8 7.4 1.3 8.7 15 628,888.0 4,850.0 33,738.0 14.4 2.5 16.9 15 1210,100.0 1,314.0 11,414.0 5.0 0.7 5.7 12 4S. pTg-so NOSS.7LS7.6 2.1L9 B2.8965 i 4L S au
8282.0 740.0 9,022.0 4.1 0.4 4.5 9 3141UL33 104. 6 245.143.9 29 W auL1
A.D. w 3,086.6 3,086.6 6,173.2 1.6 1.5 3.1 SO 2B. Sdalie 662.4 - 664 0.3 - 0.3 -C..Sqm
6,001.8 666.9 6,668.7 3.0 0.4 3.4 10 2Opo aintlace 7,359.8 817.8 8,177.6 3.7 0.4 4.1 10 3593.9 59.4 653.3 0.3 0.3 9SW O_aIf 2oaf L39SS 1S41 I.496 1Q 08E
Pnost CW_;34,981.5 14,248.0 49,2295 17.5 7.2 24.7 29 18l d 98 72 12 324s6.1 22 OA AU1 2 J2

-38-
(b) equimentM boats dirsicle. anmon miu d overea felowshIps -90 percent(c) n-country - 20 pecn; (d) resah and sdis, d-couY feowsIps, in-c0oW ra ft8h_l& wmt dqN6 od cojft mngemm coo - 15 pcit; (e) dru -50 percent;(t) ftvel Anvancs, doubakm, O&M ap_aidte ad consumable mterials - 10 percen;
4.5 Tu and DWul. Ind1c ae ad due areestimed at Rp 12.0 bllion(US$6.0 mMlon) based on doe r 10 Opect value added 'tax n localy purdcasedcn stLqnruction kmatrils goods, and Instrcdional matderil.
IL FANG .
4.6 Mh tot prject cos of US$164.1 mMilo equivale would be finamced by aproposedlo of US$93.5 millionequvalent, coveig62 pertoftotal ptojectoos eudgtaxes and reserved pm tof veic (Mle 4.3). Ihe t fub r Wderufl(KW) would cofin 66 pfercen of eequim e sud igtaeofUS$18.5mMilLo equivalet (DM 30 Million), coer 12 p at of to projct o excuding taxesand reserve ( 5 pece of breo and 2 pert of loed eal). Mm
TWWbe 4.3: JwNaCM PLAN(US$ milin
.. DD~~IRD/KfW
M9 KfW . Iilomda Totl %
*wil V/Mb 10.8 - 16.4 27.2 40- - 1.2 1.2 0
mE= : boat ws & 6.9 18.5 2.8 28.2 90V*icl - - 6.5 6.5 0Instruc mInal e 2.4 1.0 3.4 70
couguitm _ 7.7 - - 7.7 100InwourAry conmatoo 1.8 - - 1.8 100Research & sles 13.4 - - 13.4 100Overseas fowps 11.6 - - 11.6 100Workshop and
-mtuny flowuhlps 10.5 - - 10.5 100Inhcountry training 19.9 - 8.5 28.4 70
Pxject _ a 5.4 - - 5.4 100lnc_l rocx Cosa 13- 1.7 13.7 0
UngUalaNd i3.1 - 2.0 5.1 61
IDml 2Lu IJ .i Az
La 1d mag l cost for nwbstve a e (S$3.5 millo), and projectmanagemetCosts (US$1.9 milo).

-39 -
(25 pecn of1feig nd 2 percent of loc). Thewid mIts annual budget tmaining casmq of $52.1 min euWalt (32 pect of tot projcCos Ihndig am). m propose Bank kmn w not become effecve u ite KW gratagreement bomes dective.
4.7 Recrrt Cessad N. A nme ta of heproJet wlllgo tOrecurrent costs a conentIony undetood. As dshow In Annx 9, abo US$11.2 mi_loor 8 pct of the to bas project coss ae for recurt cost. whi wold be fnocd bytho Ge_umc Ihi owS&iem ch btt d operaioa awsuevisoy tmv¢the prvion of a small number of addiion staff for health education at the prvncial levdin sdecd provinces, and increased pplis of drqs for Sdao Mothood and Child Swvivalpogams. in view of recent positive trends in opeaonal and _ budes,c Itemsdo no prese any m aj of iby.
4.8 Howevr, eredf are sinfcanmtdiecly refected In tho prptnal d i of b anc rotfl4. Ibo abof the project is to big about significant, meas urble In the u galty andeffectvens of community heat and nutritn prorm. To this endo project seek toeNle local heath aII, p dy at th s ms d kbupat levs to adaptth resources ma be hrugh crl and provincial budgs to these neeo. TMe key
m t ht would be used t atcut proosed s io to loca heat polms is thePaoSm Davom Avies ix wch resure (eqitet .t wonkbop, tmead othr x ) have boeen ll _oced acs revant categories of proje 0ost. Eachkabupae and prvin wod be epetd fo pr e dd Pln spcifying how th ItmIdcuded h activitie are to bemployd4 as wel to spocify the euion criteia (see
Ana8) ad mesrmn mehostob e ued. omoubo die exp _du. Uhs a of esoPlans would, In tur, prvIde isgtO as to which typs of rcure expen (e.g.,aleati uses of tainn, trasport or sup to Imprv dh fctv of PoM 0rposyndu) shuld be over theonr rwn.
4.9 Sal n d pedural stps wodd be tn to ensure hat postivresus which mer om the Prgm Dvlopm Acite ar sustained over dt long rn.First, plm for the use of hes fuids, I pecicationsof th epectd outcoomes of theproject, would be preare by khptanad provincia oM*cIl prio to being submitted toCen eel ofis fir reviw. Officials of th Prvnca Planin Boram (Dape) adMinsties of Fiac woud be Ivolved in th reiw of the projdct prposs. Second, eadhpropoa woud inchdo a a of which put of dh rutne buts (DIK mih beaffi by the findiqp ad a statement of th criteria aght which dh project is to be Judged.TIId, die conUd unit(s) with. _ah" oil Muff ulti for the propos (e.g., Dhect of
Famiy Helh for Safe l wd _) wo a t am pwvicia te inegtatb& wit rlvat offics in th M strY of Finc at Pvd a ad Oeal levls,an agread schedule andlor acion, plan for how fidins wou4 be cpated in ftmeVe0SI of etherdthe DP or DI, or both. Tlhee m wud, in tn, bo_oe monid byhe C6tal Pojet Secreariat and by Bank p i . This approac, paulaldydo ue of the PMV= Dadop_m Acides, woud tims be ouM in Idfying which
_Wmdkwu (kvaamw or r rn t) shud become natedi ele et Of comm ty healthand utritin prgram byond this project. Morov, tbis a ch wod ilia andpromoW tho active Puddpio Of an Ivds of th Misy of Hea ina earch fo
I I I I te8t. Each mcOC8 fn wowd also crut to ln ru sustainability

-40-
in that it would help the Ministry of Health to demonstrate, tirough on-the-ground results, itsown credibility as a source of public service.
C. PRocuREMENr
4.10 The procurement responsibilites for the project would be carried ot by each ofthe five Provincial Project Maager offices and the Central Project Manager office. lbeproceat gemes are outlioed in Table 4.4.
4.11 Procurement methods for civil works, goods and technical assistance are describedbdow:
(a) Ciil works tot Aing about US$29.4 million equivalent. Becuse of thegeogrhical dispersion of project sites and because of the small contrt size, allcontacts for civil work would be awarded on the basis of local competitive bidding(LCB) procedures acceptable to the Bank, in which foreign firms would be allowedto participate. lhe Govenwmentprovidedproof of land acquisitionfor oia sltesfornew construalon prior to negodations. Contracts for civil works costing less thanUS$100,000 up to an aggregate amount of US$500,000 million equivalent, wouldbe awarded on the basis of three price quotations from qualified contractors.Contacts for civil works in remote villages, costing less than US$50,000equivalent, up to an aggregate amount of US$500,000 may be awarded throughdirect c an.
(b) Equipment, boats and medical suppUes totalling about US$30.5 milionequivalent, including contingencies, of which US$18.5 million equivalent wouldbe parallel coffanced by the KfW (Financial Cooperation of the Federal Republicof Germany), using the Bank Procurement Guidelines of May 1992 for the-procurement of KfW financed goods. Equipment, boats and medical supplieswould be grouped to the extent practicable to form bid packages costngUS$200,000 or more. These packages would be awarded under IntemationalCompetitive Bidding (ICB) procedures in accordance with Bank guidelines.Contract packages financed by the Bank and valued less than US$200,000, up toan aegate limit of US$4.4 million including taxes, would be awarded throughLocal Competitive Bidding (LCB) procedures acceptable to the Bank. Contractpackages valued less than US$50,000 or equipment of a specialized nature forwhich LCB is not pratical, up to an aggregate limit of US$3.1 million includingtaes may be purchased dtugh international or local shopping on the basis of aminimum of three competitive price quotations.
(c) Vehicle costs would total about US$7.0 million equivalent. The Government ofIndonesia bans the import of vehicles, therefore vehicle procurement is consideredreserve procurement and Bank financing would not be used to purchase vehicles.However, at negotiations, assurances were obtained fiom the Govruneat ofIndonesathat the veicles neededfor the project would be procured by 00a widera schedule and timetable agreed with the Bank.
(d) Instruclional materiahls totalling about US$3.6 million equivalent. MostInstuctional materals would be printed manuals, guidelines, books, teaching

-41 -
Tabeb 4.4:
Procuement Total cotxaUXe iudW
ICB LCB Others La N.B.P. c es
CQvl Works 27.4 2.0 29.4(10.8) (1.0) (11.8)
PurnIur 1.3 1.3
Equ*pent, boats ndmedical supplies 3.0 4.4 3.1 20.01k 30.5
(3.0) (3.5) (2.0) (8.5)Vehicles k 7.0 7.0
hntrctonal matewis 2.2 1.4 3.6(1.9) (1.0) (2.9)
Consultant servc 9.5 9.5(9.5) (9.5)
Research and stdies 13.4 13.4(13.4) (13.4)
Fellowshjps 22.1 22.1(22.1) (22.1)
Worshops and in-country talnin 28.2 28.2(19-9) (19.9)
Project mangmt IA 5.4 5.4(5.4) (5.4)
bncrmet recurrat costs 13.7 13.7
(3.0) (16.2) (74.3) (93.5)
Not.: Figues in parentheses ar he respective anwts finaned by the Bak N.B.F.: NotBank-Fhnced.
La cludes n ationl and loca shopping, selecton of Ios i faowing Banlkin.
US$18.5 million is cofinanced by KfW using Bak gudin.lrwm pro_m finxced by GOL
Id Project incudes x directly redated to the m a t of theproject such as tve consle mateas, honoria etc., but ecudes salaries.

-42 -
materials, ad sandad med fom procured and prne lay. Printgseve woud be prced through LCB procedures frm prvae printg
by each Pvincial Projec Manager and by the Ctral ProjectManager. Aleady prind materials such as sndard meic foms, book andtacig mdters, up to an limit of US$I mmiion, could be procuredthrough local hopping an the basis of a minimum of thre com ve pricequotatiom or aftr negotation, directly from publish and locA distibutors, orbookjbber.
(e) Cmuadt svie for tech adsi and special studies totaling aboutUS$9.5 milo equivaent and rearch and sudies toting about US$13.4miion euvalent. lhese conacts would be rewarded in accordan with theBank ifor Use of Consultants.
(M Ovs and in_untry fellwhip totall about US$22.1 miion equivaleatPla_mm of candh id n freign insiuto would be made on the basis ofreevc and qualy of the prgms .ofred, cos, ad prior eperiene,accrding to goveanmnt eb procedures accetle to the Bank.
4.12 ProaremlmA Review. folowing bis an ouine regarding prorement review:
(a) By lo effecves, the Bank wil cary out a prior review of (i) standardbig dds for civil wodr and goods contrcs to be awaded under LCBad IC procedur, (i) letters of hnvita fo consultant sevices, to ascertaintheir cnomiy with the Bank guidelines. The ap ved c would beused as maswr dowent for al t bidding.
(b) Except for those in pama (c) below, aU conrcb valued at or over US$200,000wold be sbject to prior rvi by the Bank, whereas cotrct underUS$200,000 In valu woud be sbject to radom post-reviw;
(c) AR contact for and ihe mam of oveseas feUowships,research and studies and co tans would be subject to prior review by the Bank;aSn
(d) laountry fllowsip, i ty trning ad worksops wold be subject torndom post-eview by the Bnk.
l i expected that prior riew woud cover about 43 percent of the contcs to be fumded fromtheloan.
D.
4.13 The propoed lo of US$93.5 million equalt woud be dissed ov a prioof about7 yea (Ann 10). aren epected to be coleted by the mb 30,1999, the LAW Closing Date. Ihe _ s e has b b with somead bs to reSect the estas of the Spcal Account, on the _ement profile fa
projeft in etimated for FY93 a based on te proposed initiadeposit in the project Specia Accoun D _ would be made as folows:

-43 -
(a) Clvii word (onNRES fnded) 90% of toal pdurescii works, for provinciac-1* buildin
(B) Equipment (excp vedces), 100% of f_reignboats and mecal supplies 100% of local (ex-factory)
_ ,~~ ad 65% of loca
(c) bIstuctio materials 70% of tot pd
(d) Cosltat svices, resarch nd 100% Of totalastdies and felowships
(e) Wokshops ad lcuntry qting 70% of total ex_
(f) Projec mnagme 100% Of total
fbr equipment financed by KfW f dlow fW dKis pidU d Iawoac with the a iKbetwe GOI nd KtW. EquIpmst, boat and med sulesex_hxlbm would first be disbrsed aginst the K*W finds unti such fnds are coWletely
4.14 D from th loan for al conUa exceedin US20,000 per conact,and far tecni a nmudig resarch and sdies) and ovee felowshps would be=de, asit hall_ AU odur di--soon would be mado Wat s_w of_qmdkuw forts whi relevant would be reaid by reonsWle agncies and madeavaib for riew as requested by visitig Bank misaim. To fa c Itate a&)dc AccoW woud b esalished at Bank ndona to be used by DepKs under thedirecton of te Director Geal of t Budget, Misy of ina, folwig esbdprocer. Ih Special Acou would be used agaist ellble _pr all cstegories.Upon Lan Effecivee and confimaon of the o Spe Aco, Bank on roept of an picatdon from the Diector Gera of the Budget, Mistry ofFinne,would make an initdepost of up to US$6.0 miion, wbich i bse on ge need for feds tocover ho exe on averag four mont. Appcon for repl tof SpalAccount would be submitted to the Bank quartery or when th balace is O pe t of theinta deposit, or more fhquety if necessay, in amnts of not less t US$200,000 perapplication Applicatiofor dirct payment and speci t would be a minium ofUS$100,000 per appHcain.
E ACCWaS, AmS AND Rwomu
4.15 DepK would establish project acus for all project ependiu at both theprovi and cea levds, to b in accord e with sound dg p .Account for the _ of Expet e MOM) and Specl Accou woud beo nsywately. Ech Provic Project Mnage would snd financial for Ual projecteqmdkuw for each fisl year to th Prjec Se aaL mhe Proct Sectarit wouldclhsoffdate fi" provid fhcial _eme with t al la&d I" cinadd statement and

-44 -
prepar a conoled fianca reprt Mm finanWial nad consodte port WOudbo edby t auditors acceptable to the Bank inclug a saat audit opinion nSOE .qwam
4.16 Certified copies of the consodated fiial rpot an the project for each fisclyear, togdher with the adibors ent, would be funhr ed to the Bank as soon as avb1e,but not late than ne MOha afte the end of each govenm t fisca year. Mhe PojSecretariat will main separe project account in a form satfacry to the Bank for annualaudits. Thes account, iluding the Special Accou and SOEs wil be udited amually byindepent aiors acceptable to the Bnk and wil inlude opinions on alleincluding se made against SOEs. In the case of SOEs, the audit repot showd conain aseprate opini by said aiors as to webther the em of expendite submitted duringsuch fiscl year, togetr with the procedures and intenal contrs involved in their preartion,can be reied upon to sxpport the rdead wirwal. IMe Setari wM submit tho auditedaccounts to the Bank no later ham nin mos after the close of each fisca year to which hyrela commencing calendar year I992. DepKes wodd also mnior progms in prectimplemoand report to the Bank each m on this progress. Witin six months aft
the completion of DepKs would submit a project completion report to the Bank

I4tiIt1~ L I
Mn 11111.~~ItWISI 1 2

-46-
approaches to esig the alali of doc4rs and mwives In hard-to-r and remoteareks, and procedur fo Ing servie tranin wiin prvInces wm be improv.Last central, provincial, kaxpae ad health center capacitie to assess and monitor chanin prwm dfecdvmm ad trends ii health and n iona outcomes wil h been
through ceaig the availability and u of nformation syms for thmanagementof Depkes peonnel and flnan sytm as wl as pariodic, valid of yey outcome s through upgrdg of health compot of the Nationd Socal andE wmmic Sure 3USENAS).
5.4 Project Rik. The mor isk for the project Is a dsice provincia anidbbqWm he& _ m t- -r 1 have not yet had sufficient expeein de preparation andhnpl n of speciffc Saf Motherood, Child Survival and Nutrin Irv tios, thequalt of these pl wil be dipo , epecially in the ealy yea of the project Toaddres ts risk, th pect des caUs far a range of capaity-building and staff devdopmetInervewntionsattheprvinci, kabupaten} adhe enterleves. Inaddidon, SchoolsofPublicHeat and rearch and tainin,g In nutrion, the Aa Gizi and IPEB, wi adapttheir rearch and training programs to meet provicial nee. An y recruied and
inted Panel of Speciaw also povide tchnical advisory nd, If ncsay, spVeiadco nuldtation s0vic to support prvincial eforts ad sur crow progrm and cross provincesharing of success expeiece. Th estabHi hent of an integrated methodfor Wgefg nd ovuft inevnin at healh czentr, b dWf anid pwvi loves wddalso hep proanet hp;ivements In intervention qualty and ffeetvene during the course ofthe project. A secod major skis 1bat theorizia, flsca and magal adj_to be developed btough tie project would nt be replicable in oer provinces, or would not beficiay sustainable. To mimize tis isk, the prject caUs for the development of supoiv
q e_* -9 *_ changes amog the key cmmunity halt and mntitiooffices at the cen lvIad has a planned satgy to positive project findings into fte routn and caphibudget. lhe involvem woud esu thoe needs and perspectives of other provinces arconidred as the proje dvelp. The projec costs are wiin the range of fina ing c d for the soctor in oach of hese proVi accordg to cu trends.Mover, revie of the costs and effetvea of specific itvenio andIor sevice
e particularly high costmtem transport,c and stafftraining are to be monitd and ealuated durig the course of the project.
5.5 _be me mown neve V c ne_ of- halt and nroan pgrams.

-47 -
6AGREEMENTS REACHED AND RECOMMENDATIONS
6.1 Prior to negotations the Goverment furnished the lowing to theBan:
(a) An oIl dwart and detaied terms of rernoe r the central PojectSeret wihin the Drorate Genrl of Commnity Heath, nludingspcfcion of ts prposed ratinsip with other centra units of DepKes,including Pus Data, PKM and LItangkes (para 3.29);
(b) Detaied Terms of Refirence dewcrbig the roles and 1mctons of the PovWiilPlaning Unis and the Dokabu in the pmat and Impl_ne of theprojet (paras. 3.31);
(c) Daft LQ docD n for the pc of civl wors and goods and ICBdocumnt for the p.mnent of goods (par 4.12 (a));
6.2 At ne the Govenmnt gmae that:
(a) the Govenment dsll manta, widn Depkes, until compledon of the Poject,the Project Sering Commte, aired by the Projet Maaer, and nhcludireprntatives of Bappens and of the following offices of Depqe: thDirectore Genea of C i Di Control and ' -E
the Secretarat Geal, the Dectrat Gwenal of Mec Seavices, theDiorat General of Food and Drugs, and the National litute of HeathRearch and Dvdpmen (param 3.29);
(b) the Goverment shall mainn wihin Dopkes, until completion of the Project, thoProject Secretariat with qualfied staff in adequate numbers, _Iudin an ExecutiveSecretary, a Plaming, oariog and Evaluaon Offier, a Fmance Officer, anda t Officer (bara. 3.29);
(c) Depkes sh mtain untl completon of the Project (i) a Project Director, whoshall be th Dire or G al of Commnity Hlh of Dqe s, and sha berespoie for ovea Projet Im pI and (I) a Projct Mang, whoshil be repnsble fo te dayto-day imp ., of the Project, gtechicl and eo aspects (para 3.31);
(d) by July 31, 1993, ebis and thereaft mabin with Depes, until compleonof the Project, a Mangem Advisoy Group with ed staff in ad te

-48 -
mubers, Including a Community Health Advisor and a Project ImplemeSpeciaWist, acceptable to the Bank (para. 3.30);
(e) omnxmencing April 15, 1994, by April 15 of the Fisca Year in which Projectactives commence in a Kabupaten, strengthen the planning, monitoring andevaluation capacity of such Kabupaten, including, if required, aupointng aqualified monitoring and evaluation officer to the Kabupaten Health Office (para.3.32);
-(f) commencing on September 15, 1993, and by September 15 of each subsequentyear, it would cause each project province and kabupaten to prepare and furnito the Bank, annual detailed plans for implementation of project activities. Suchplans shall include:
(I) if relevant, innovative activies for improvement of the quaity andeffectiveness of community health and nuition prgrams, includingevaluadon criteria for such innovative activities (para. 3.34);
(ii) the recommendations, agreed by the Borrower and the Bank, of theanthropological and ethnographic studies carried out in the pject provincesinhabited by Indigenous People (para. 3.36); and
(ii) measures, satisfatory to the Bank, to ensure that govement and non-governmental organizations engaged in the delivery of community health andnutrition services to Indigenous People take into full consideration theprefernces of Indigenous People beneficiaries of the Project, which wouldbe identified through the Government's existing consultation mechanisms asset forth in Decree No. 9 of 1982 relating to guidance for planning,evaluation and monitoring of development programs at the local level(para. 3.36);
(g) by July 31, 1993, frnish to the Bank a plan, satisfactory to the Bank, for themonitoring and evaluation of the project, induding:
() the methodology for the application of National Economic and Social Survey(SUSENAS) In the evaluation of the Project (para. 3.40);
(i3) the procedures for ensuring the effective monitoring and evaluation of therealization of the benefits of the project in regard to indigenous people inproject provinces (para. 3.40);
(h) by August 31, 1993, it would prepare and furnish to the Bank for its approval,procedures and timetables for establishing annual research program priorities underthe Project, and, thereafter, carry out such reseach programs in accordance withthe approved procedures and timetables (para. 3.35);
(I) commencing on September 15, 1994, and by September 15 of each subsequentyear, it would cause the provincial planning units of the Project Provinces toprepare and furnish to the Bank for its review and comment, annal

-49 -
huplenentA Projec report, Such repor to be prepaed inconsultato with the Project Seaiat para. 3.39).
0) ber proeedi with the pplos-of quipme for the for Healncormation, co o tbe cau the Center for Health Infmaon to carry outand fIis to the Bank a faubity study on the use sampeat tex and halt cetr levds to me hel outcmes; to reviewand revs as neessay the Het Center Repotn Fams (S2PTP); and t ddesiad test a manual form of the w reporng system (par. 3.42);
(k) that he Goverm t would: (i) byS _ 15, 1994, prep and rnish to thBank fr its approval a plan for carrying out a mid-tem Prodt review; (i) byJun 15, 1994, carry out, In consultationwiththeBank, a mid-temProject reviewpwrsu to his pa; and i) promply take al such acions a at of the mid-m review and which are quired to aciv the objectves oft project (pa 3.41);
(k) underta to acqu the boao amd vhicles rquied for Project Imple inaccordane with a scbedule and tmetable agreed with the Bak [pa. 4.11(c)I.
6.3 The foRowing will be a condition of effctivees:
(a) ta condiko precede to hed effvenes of KfW Gant otettoe rdated to the cdveness of the Loan Agreement, hav been Alfilied.
6.4 Suject to t above condions ad a , t pwjoc woud co _ asitabe bads for a Bank loan of US93.5 mion equiat to the Republic of Indonsa for atm of 20 year, inuding a grce period of five years, at the Bans staad varia eteest

Tabh 1: Sdmtu l nfrimoru he us PrOtvegs Inthe Thltd Comnauny Beant and Nutridma Pf9sJe
_puion 3,26,644 1,641,414 1,U9,274 28,521,692 35,378,483AmJMO 47,350 414,O 77,871 34,S02 44,330PuDion. DuIt 69 4 24 827 796% < SYM 41% 41% 43% 39% 32%% >)i0You 4% 1% 3% 3% 3.5% IIshommli 77& 7 66k 51 71.6Cabdbka no 31 - 29.8 Ciud.deat am 111 ' 7.2 6.1k 9.2T7d h1 dfy tab -
ULat5abr5_1= _ tol fd0 5.8X 54X t3d 24* i5 CSd9 %]M o 76% 55X ff%fX % P g -wmm wkbin 772 v_ookudo4 41X 34% 20% 47X 70%is int wiDtI Mo 6% 76% 32% es% 96%*BMW nded byam" % -7d 26% - - 31%B _ea c.I 151 110 92 i30 m2B
8ub_aml ei-.17 534 432 1,264 1,143Rfslhe witlhbedin 33 37 22 123 87Npual: Raft tam 214 107,269 20,101 390M 48997lbptaio &ub4fth _ 6j322 27,811 4.21 226 31A04
pudo phym 19,931 9,88 11,779 12,210 160Pbpok*w Nwn 1822 1,434 9m6 5,650 3,864P1puad: iUwih 10.183 12.f0 6,824. 10,293 24,365Popu n : bad 1,S44 1,1 929 I2 2,708
E aMLM 6,154039 325,8 176,248 1,4049 7,6199t -aumut) 21,341,405 4,019,931 1,W7,791 11,000,091 19,38,184ROWARS 3,345,164 16,001,031
lrr"l ~~~~~~~30,84,69 4,345,766 1,892,92 12,406,081 43006,11llwJMt sdahat.for NTTrs*1nto 51987JmomIUDR f rr ^1w nwI=hs=a o4I dTlhe CDR ed CD r N1Te ret9a to 1985.Ib CDRt r CelJava o 1985.The ttoat hr s tO a 1980 4uro..- ,wad e ', mhr Catgal Jat a the r 1to wv. modOe, and mid.
OQ

-S1i- ANNEX IPage 2 of 19
I OR'aa Etii ;5fi!
: ; i Z t t t
I _i'l^Zd I
] iSt:t'X~~~lEgtg: k {~~l 2 3 ̂ _ ^I
I~~*.~I1J a

Tbe 3: Sdcted 5 by Dist Levd for NTj 1990
"Ol .. q -g i s s~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~,.
lbs t) 522,944 71 12,755 I" 8D 24M i6,152umor Taplb 8det (1) 348,067 88 24,86 4,144 12,431 23,24 969
TUt T_eog Uli (2) 1N3,052 61 13,S88 1,359 9591 18,117 543aft ) 216,060 8a 24,007 1,715 1,M 3,86 9,00Alr (1) 144,w so 24,10S 1,315 674 13,14 6,0.P rlOmit( 26,79 86 i8s9"3 1.6m 13967 14,764 5,424gm& (1) 246,867 143 24,687 2,397 7,0S3 22,442 4,488lain(l) 218,841 107 18,237 1,216 6,632 21,684 6,M39Ngadk ) 196,100 65 22,011 1,152 6,831 19,810 6,191ma.oami) 499,458 70 27,748 2,538 20,811 29,380 6,572Sbs umob (7b 3) 152,646 22 15,295 968 8,997 15,295 5,274Sunubs a W ( 291,921 72 32,436 2,754 16,218 29,192 6,487
Tawl 3,8,644 6 19,931 1,822 10,183 21,647 6,322
(1) = Phme. 1O2) - Pm 2() - Phus3.
ii

TamLe 4k Sd x&bdi todrs by Didrict Levd for West java, iM
Kod 3.r 12) 271,341 9,591 3,015 379 3,769 24.667 15,329Kod 5 bouxd 3) 11938 9,8n 3,242 697 2t789 17134 23,612KGd DEaodz 2.056,915 25,400 2,905 885 8,904 44,716 S,A891Kod Chebo (1) 254,477 7,863 3.915 912 2,925 15M95 22,268Chujiar (1) 1R,62067 508 32,590 7,013 6"463 47,488 30,219Dbaondg 301,332 1,096 21,778 8,146 31,081 50,815 35,179Gbuup3 1,748.616 572 26,494 4,857 43,71U 40,665 22,418lhibmnadaY 1,814.912 714 20,624 3,A9 25,562 44,266 15,124Cmnis 1,478,476 578 25,491 4,361 28,990 35,202 23,846Kni^eap 892,228 958 22,306 5,187 10,025 44,611 33,045Ckrdb (1) 1,649,428 1,766 39,272 6,320 29,990 53.207 45,817M~ah&^pengka 1,092I023 962 25,801 3,712 21,958 44.871 29,486Sbuawdaig 831,809 857 18063 - 28,663 33,27 18,083Iodauuuyu 1,446,931 864 38,077 6,318 41,341 53,590 30,144Subdbs 1,206,664 610 34,476 6,817 38j2S 50,278 19,462pugwakait ) 50,039 544 20,109 4,896 29,634 43,311 15,217
aunwang (3) 1.491,556 1,034 22,62 5,737 22,947 53,270 40,312Dbaoud (3) 2.104/.92 1,496 24,470 7,038 28,09 70.146 63,769TupoSang (1) 2,764,988 2,257 21,772 7,473 1S,691 74,729 95,344Scang (2) 1,470,938 862 24,112 3,305 42,024 49,928 35,874
Tota 337483 798 16.045 3.773 24. 31.004(1) - Pbu 1(2) = Phwa 2(3) = Pbase3.
th0

Table5 Sdseted Judmimgs by DbkftrltArvd of lyan JAm 1990
-~~~~~~~~~~~~~~~~~~~~ .
UiVn(1) 20S,722 2 WM 1.6 17.W 11g5 24
pW M3M39 6 278 2.6M 32.M 255 G.5
J O(1) 25 5 4.W 1,m 10.715 9.5 35.79t
Fs" ) mow 5 14.3 2,4 241 IMB 4*61
H*lc own 2 9," on 5,Nt limp I"IWAN s Ale It7 GAN. n.lm _ 19M S 9.46 I,l71 6.66 11*8 2.928
auI~d 1200994 4 l,123 t,1t1 6.24 S12 1.638
Ya (mpm0 91l 246 ,1M 21 10.7I 19'
Dkk Numb, (2) 90843 25 6M 450 9,O" 9,34 2.753
Tuu 1.641.414 4 9.8 717 13,131 1KM 5.07
(1) - Phan 10 m PhauS2

Table 6: Sdected Indlcatw by DWrk L4eVI r4r CO"ra JaVa. 19W
go. Mbsgung 123,213 6.485 3,423 n8 8,801 24643 205KD. Pe_aop 242,874 12,783 10,12 5,16 20,40 40,479 17,go. Tegal 22l,713 6,381 i - - 32,816 16,8MO.. s_a.ag 1,250,971 3,159 1,385 - 7,968 44,678 52,124K.. 8 g 98.071 5,162 3,772 67 3,269 19,614 14,010K.. Suua 504j76 10,727 3,908 640 1,601 45,834 22,917Dmuus (2) 1,348,2 960 27,27 11,97 17,748 39,671 64.Pab_Om ) 732,278 a8u 33,2S - - 33,614 15,919Ca_p( 1487,30 n 30,98 C S , 111 18362 64,6 25,2
_NOMWM( 771,774 681 20,310 9,70 t18824 23X7 22,51Magiu1 (1) 1,015,872 883 31,746 7,1t 19,161 3907 26MBThu W p3) 616.75B de 29,0 - 369 21, 2WoSbo (1) 6551 63 20,16 44 m7 39,150 17PWO* w ) 70,788 639 25,28 9.34 63,708 31,4 18,i2
dixm CZ) 1120,92 824 20,795 11,439 17,S15 36,161 19,666Jd1o_p G9,80 7WS 13,217 5,736 7,617 33,324 1490pmho 1,114,28 1,006 21,427 7,792 14,661 4A,5M 32,771T1g (2) *1239,35t 1,328 42,736 16,307 21,36 53,8 23,167op (3) 1521,35 86 7,118 12.7 21,741 46,116 3239hMU8 _g 7810 729 S,48 4,412 10,395 32,992 148X
Ku.1 (2) 799,117 752 17,372 5,223 18,4 36,324 loDamk 822,826 865 2833 10,285 17,517 41,141 22,239owobo.p 1,148.330 5,458 30,219 8,0t7 26,096 4A67 21,667
Pi t() 1,064,115 673 18,347 2,313 24,184 39,412 3S,471jam (1) 827,657 778 27,589 . 22,990 45,981 25,P81 tR_me (2) 513L690 476 16 S.645 214 33.01 12 842

-56 - IPage 7 of 19
I In[E, I
- t -
- --t - -; ,-
' !!!s1III

Central & West Java, IndonesiaPopulation Density by Kabupaten, 1990
1DKI Jakarta
El 50
750so- 1000 * ~200 - 500. * ~500 - 750.a*, ~750 - i 000 _.t
* 1000 - 2000 .
)2000 HI I and m are project phases

;apaUdan/W Eastern IndonesiaO0 ( so Population Density by Kabupaten, 1990
100 - 200 40
* 750- 1000* 1000 - 2000 Maluku I* )200-so00
NTT
10 lop~~~~~~~~~~~~~
N I, II~~~~~~~~~~~1 and MI ame project pae

Central & West Java, IndonesiaPopulation Per Health Center by Kabupaten, 1990
OKI Jakarta
10 (10000X 10000O- 15000
15000 - 20000 !1* 20000 - 25000
* 25000 - 30000* 30000 - 35000* 35000 - 40000
.* ' ) 40000 | 1, 11 and m are project phases40000 asesi

Populatlon/HC Eastern Indonesia[ < I10000 Population Per Health Center by Kabupaten, 1990
10000 - 1500015000 - 20000 04020000 - 25000 26
* 25000 - 30000 o* 30000 - 35000
35000 - 40000 | Maluku Irian Jaya* ~> 40000
NWr
mur 1!
." |1, I and Im are projec ph

Central & West Java, IndonesiaHealth Centers Per Area by Kabupaten, 1990
West
HCsI1,000 Km2
* ~( 5* ~5-10
I 1,f10-15* ~15-20
* 20 -2525 - 3030 - 35
.Q1 ) 35 I, II and m are project phases

_ HC,A Eastern Indonesia( 5 Health Centers Per Area by Kabupaten, 1990
* 5-10* 10-15* 15 - 20* 20-25
25 - 30 i
30 - 35 Maluku Irian Jaya)35
NTr _ is.
_ur 1 and I a r
.N |I II and III are project phases|

Central & West Java, IndonesiaHealth Centers Per Area Per Population by Kabupaten, 1990
alaxiwh '' }"@ ' |~Cntra
.~~~~~~~~~~~~~~~~l IMOOD Km /100.00 POP.
l 1 0.25 - 0.50 11t* 0.50 - 1.00.'.i * 1.00 - t.50
.4* 1.50 - 3.00o3.00 - 15.00 .
15.00 - 100.00^ 2 ) 100.00 . [1, II and m are project phases

HC/1000 Km 0000 Pp. Eastern Indonesia* ( 0.25 Health Centers Per Area Per Population by Kabupaten, 19900.25 - 0.50* 0.50 - 1.00
* 1.00 - 1.50* ~1.5Q - .3.00 *
3.00 - 15.0015.00 -100.00 MaIuk u
Irian JayaLI ) 100.00
NIT
II U and H are projec pha

* Central & West Java, IndonesiaPopulation Per Physician by Kabupaten, 1990
1DKI Jakarla
Population/Physician
1] (~~10000
10000 - 1500
* 1O000 - 20000
20000 - 25000 . o
.* ) 25000 I, _H and m are project phases

Populaflon/Physician Eastern hIdonesiaJ < 10000 Population Per Physician by Kabupaten, 1990
10000 - 15000
15000 - 20000
* 20000 - 25000
U. |> 25000 |,
.,T , ,i-N'rr ' _l ._ Sm~~~~~~~ur
I, II and Im are project pha

Central & West Java, IndonesiaPopulation Per Midwife by Kabupaten, 1990
West
q~~~~~~~~~~~~~~~~~~~~
Population/Midwife | (5000
5000 - 75007,500 - 10000
10000 - 15000
15000 - 2000020000 - 2500025000 - 30000
* ~~) 30000n H0 D0001 I U and X11 are project phaeseIs

Populdtlon/Midwife Eastern IndonesiaO < 5000 Population Per Midwife by Kabupaten, 1990
X 000 - 7500.v7500 - 10000 .41
* w 100- isooo 1,1* 15000 - 20000
* 20000 - 25000
*25000 - 30000 IrianuJaya: >30000Ml
40~~~~~~~~~~~~~~~~
co
4_ adtrercpmurhs
|I, E and m are proje A

IN ONRTKIRD COMMUNiTY HELTHI AND NUTRITION PROJECT
Or OF PROVINCAL SERVKIE D,uvuv Coh9oNnwIDInL PLAMTable 1: MaW: SAn MoT oDSvic
-.Ihuuheofudild.ml zequlad data. .u to -oles -eris Iounsdon hw do S p-oje' p--wbuse. -Co t a- -oto - - o" b --s h'I'1h1i .RkWmaultouyhioet, *a mm be VW of*.SWr/lIUSN dffi t or hdqsmedozm.
2. HaNiag ad .ow&uia.mmdng:T gt b wlawu oieia fd.dfaeimcaswi h Condust aosdhe1hs.ssdawswib pacIkpAtla kern mtasa. Ca_i"immodsa boaM now,io rntdoea w a d_ o_e ne. Mm agidbe ce. eslua _a.b. hoao_ w*dsps;*. W*adsape MO). an iIdoAfb"v=AmUVRMMR ad
3. Thiq: hi ma, dociaq, an MW. To om m n .1m i iliea o k ps nin ean lto us t$hhtromm.
4. WS. dnWomwb a ed ovi l DX NA= udImasgutddiwkWdlouto he aneda, givo ead.ovlpqu CoaluetWS ad peoid. tO I DI_ tessuhA" .a atedIMai I Liua od. goab nd dogl. go WS h Iehd.k a mkm D sid Osm a
S. Dnp. h as uuda a Me _ nd s1. g hi dadio. afn n ! db fd a tba. clmqmh. tbam" hi hsmde usada "mm pregmi war Mii hawmheintsatuas of and med"a pfob. km alua; mnda.o. D _abetai;
6. Ope.ado_ aueeh an oo.etuivamuof ei Ca do smcb ad po oel aid _ be_ hM MI dpos n dsley. am hd.dv am atua l7. JeAst munsu(n"Oid-wem end On. The aid-mnm and fi.1 .walndosdr w be a Mow4sp to do baselEs data Clist Jf.nd am hma Idlemn hi meAhuba mdoo7hstif. Lb mbade wi beta 6 a os anesi ladl , dilt will ewba D-tofmmt bhaMst (dial a IuAlAhd
be d.vepe txaw duuio hi So pya dt 1t1p_acime Mudoftand wab"Man..S. Tesblmal auateam. .s4 MM apslala to adin din gtohos In hiahWaovmd prjoot. Napem TOSs and asa heal oritAt.L
_ _ _ _ _ g SS _ . .-- A _ z ~~~~~~~ R

Table 2: MAWIKU Cmw SURVIVAL
rtxf d R|gis _ o | _ _-_- -r- -- i --- -------------- - 3-ba. AB .todhind 0 s ad Paaomuilt lsoo tbasuilaata haoasItdsoe m eWsdm1fta ai.m..al f buoy
I I amus~~~~~~~~~_ dilL_S. .eatbaofadsdia luq*u data. bWW Paoddout 0adI el mg am aMdf ansvs ARI oda doelledaapeat as . a *Coadahba mvayto uBis bedhas lsamIa .
. Pl Aaad msedn Tol _cUdi da . l# Ctsnab.W 3dlissia a a_ _ ciii bairn.S e _ 1 Imapo.uguwamssllau I 01.avb. aW a vb _ _ _ lkd4
3. uaS dsBe azih iauli. h~iatbiassa owJUtabags llS autazii raus wella Conut i swle_to as ahqrgas
a. AR adf heasosad ofaasdb. Katsi wlag Iw
Oaswadoda tkv so* .Laasdhi_ b"L
4. All d. wA N d vidsuvaL Pane iU oaq uf tAI L d_qa. - Tm * of 8S. Opulma u Admaband I se*.Unotdse pas peag and ebdar alewava Cooie doe nmub t sad povMs cels sad bseas
a. Bklahasm hr paosyud massobadom svailaMe wduwd1v blld aMylvauovlua lb iwoepealhtsmhsic Ex I'Mt akeadve fat ddaflvs dail m,tvsaid usIths palsy htr dbd sausval pseise drAuatbe dow&W dodga Go yaa ad obodd psvlie by ra abE AN *am.wg.mb *¢ __ anyvl dhpsasaidS n _ _ ia_ust; _ I Ior _l b r_n2 mi3 Qfp*t.b. Cahrdolag5u_ddaL
6.Iss meos tmdll d fi_ . A Iub EWw a oW ad t a hr be a asvwau b to dii bonlgo diftt d dam an wmbo ad l__i d ihWnlaod
^b. We spehrphiidu_ aid pom ye., lb o, d _sbais wM be aid 1-_qvC! subs. dir wr salasad .- AI
?~~~~~~~~~~~emtoaa. lb vbmlam E e ussu e sels Xlalstam da-dt wE eod _oisaum.givathhna.L b dewleped bahit*aafsgas d I In psajas do pnt baybm 2!lam
0

-71-~~~~~NN! Page 3 of 20
:11 tj i 01
~~I 'i i'i I l iii111
huh lill til i i !I J 1lt|ji{l I I jtI
|~ Ii ' |s jtsi| I |3iii l |l

Table 4: MAUiKU HEALTH EW>C&IT
1. Wod*op&- P do~ta pmWIuIm ddug aid mdhWakspm Iv BB Cuing WIamd gmddehqu m lqb-ias
iLWI
b.~~~~~~~~~~~~~~ ,.! I .NI I -.. Iw i| 1I -f
2. Reao"h & do"as PaWl bainelosdmmsa ewabo - -gataa of aeduesdoilma in -can"udIV aa and palds fiorme to It BB ad*l a. 113 ce. cmeuiabasel.. nway gtai n h. ttdm C ehsmdwsdmlpaaa.AIM, II amaib. Qumihathe Sadles 06 PGB) qeuh gaalsdkvs auea to help hesbd meamgsm canh d eo lm maeed w beC. R ani holA,a health edusden; dm. as weE as man wlaudn of hospital bamed Iweti educatIon
d. 33 camfpomest Inpu Ins-nmm dm4y.
S. Media psek ea In O*ncfimTA&wish le evise deSvas pIng 00oGiceion, heNBteam wI Itwe medi nminng Ow S"eah o f h impvc deUvmya. Sesmee deflvuaqpmaumdol u-wide a packag Iv eack ofdew phased louauew Im. ocosponats that an adopted to hea imeds.b. momambood packg2. dibd wewysl pw_e ege4. N_Ull o peekmgee. NmBe_Xp mpes 1n..
4. Rp4mc;W Igolitw UePeOv md tdo difticu A dot fu tech to adopt toe media asemess hard... and disidhet Sheoupmaha3t-t NB u S. loca needs.b. NowWInMI kepm-
S. mining and stffng Give. she amw saraeg w dewehpmneaofheuld& education saege., trmainn of Conuct and owahated the thsI pig. leauk anda.Taimo..mamd of NC affcmiR 33 eas pwi I acnh w kn0ao hag ffc Ala.,addltloo. deploy adimodasit almeshed.;b h omak peopmam amgAumant wil bo addd a. she hea"t doff.
b. AdMnbBdof ; ooa "
UWkdwdupa isbeftsedusafion As patod tefd capacity builin In headt oduoaldow Selcti ad pawidha healt h admoatwmMlips7. Ivowahcs l4mi whtonwUb osttdda h eahntd, ad fiiCenduct she ntcin Sold the and mindS. sud aid
a. BB5 udtrahn Wd (uid.tui* sahmAstlEn w alivlvoollcie of inlcin ooapuaiu o damein She hmesaga pow uie btso mesh am baNt odmandon dezaegics.6. PuAd evadLuain mesvalat pr4ejctpeabmn..
iN X; X~~~~~~~~~~~~~~~~~~

Tabb 5: JUAN JAYM SAn MoTuooD
1. mc_ u.bs ... . . hTO td. o(#=b l --AP. a.d Vs a-d. -d - a en a.-hd . pwundil kmhdiW_ aeV.
1. Tahiha..M dyaas~ quaity of mnis dslvw of sbstalnetl. ddfvesy am. ad Cooduct and ewatdow lb. waNlq O do dIuis puida. Ammwl Carn; tmluae0of Umh.b. TlA (headu& mw)S. YEW issrha e in makis eomtzo
3.3plibaudequlmesa BMW adequat_ e t an provided f ow lTBk/ and MWa be MCE P ba__mm and dasbs. tso vlm T3A' MW'sa. Malas cb qupmw l aeab i a" to bus Paktab. MW d"guvy Ihi well. as 6ce roded he do m nlah au 'progam.
d. W4_. ad b t asah.
4. Diuma asnaausal 1dusb aEil auaesgpgsj n Pmmmsnsat and dliiidosaotdins.a.Makal p_ ; b s pb. bnUabnte
a. h S edh mya IakubmCand humn uye,Vlah hula to Isses am qalty fmibnhdslvuud ed lucrass dwAm frequesfof ueiviwlslo andbudns mix mhdbi syom p_u;i l. padsmasefb dIdifaa asioe d pdha. IIm Ni., ad hi Kb. MW eod , Ulme do NM kvh and pomam dubovaug MCD a u dmd bep Appoit MMD coosdztm() and dlm Olslrjb dsasdehwdJs
Inyme lbs nkag a be.. db aa whedhl Ie2iras aba and zepost arn d*abh iky to hng crnovan pedgnmam..
a.2sraihof atio"C AM Mgna C .11 be p Iing emegency ebded eano. The zesovatlos of NC wMl equi CmAdosht Urn esnamsand nmalmebswnaof Ur easaeoldeiws, uema abe.& u*it to puoid MCD aevime beltw sd to be ibi to bIusdlsauuagaoy bsilamLselladloa, ubes It is an poemito in,sbe dbon cane to boapdLu.
d. Thayems mony beahmi. Poi.bd elasotb mss ae oe asbeed hon jamsue8 . RR"a as Urn aprpdao dlbumassaa of am, boub andbidis to NC at hospita.ds suem i b einrga Camyae a d &r*i am"ut hi inalgAc .ansgmmBtofargmy sIeI ls case
6. Rasauh nMbAft-ieals ady. To uedesitnd dos kwh atoasmla pebi and lo vadallion sasso dkmCnutUn ny n nopssissmaai a abi
7. MiRed oatol opeullas-sobooledusatla.n An expedmneunsa propeasto engpao. Om. efflsdveaesaf tealting monasa ooatuo Devesop dbs oyodnmasd modcl hind &a Stwo yeam ad tat shoob. Thi wi Bl tate eauad bebs. Itls lrntbohmid as put of PM" seldi of an osahuliot l d cir i b of _o, lbwdoo_ boso p oducadu SMM -
0

TAbl 6: MAN JAYAU CLD StVWAL
1. IAm w I sUalCM eb4.iC Ailhis Towenre bob alma.o e uC a.d mb WE be baLk. D do ohe mgg aths *Wi admWoe _a ulb mfs. CesrnoalmfN laahat M Aburigfthmfl aita& UswmeusckalC.15 iablee le t _ha.bendae bRhnvmotHCwth be Sds ad bi a4 l ebeMu _ee sels
b. Be aoemhu,sh do- nmo m sItd amsabmdms sushea.m NC sad flak lavalvemegisk*. sinim rncwith e vWhg emmgs7cy that caasttb.sbees obuqItb.
Co nw; s_t RDC ad mb
o.UI.MCniieno
2. Tnbd To a _quadir. aNe ad pr_o ebeSIhe am sil requred he de Cm"dais maute as mobh dthenalg.a. VW -bf In iolaed an%u Pg*GLb. Pul heamweft"muw0. NC sat # et In IhI_ q
a. s e;mm ws anablul _ o e ilr, --iny do th a hak l vascatha and equ the RC wit dob. Mol ed q to e _m e. PM kw
s.*p_dr,_ Ilb _ _ ht SI _Xt
e. Nmqmeeuy mugeq set
4. Jayvh,pcrAdinpsrhznMM: MueilimAlm to O3 Sakkd h Is hP etoo 'pcsyadub iak aardoe ddllee hbv CO*Addua Vad evdlntte.*l.' ConMdkOCt h mUsIa.r8-a. DoW w lvpep. Ikaduri beau Imorduaa. Effe t f yra,. parfonnuaae Incldetainsn ucbs,a ad ad auxmin the ..vt1 elbot canpathraneceb. spasMucm aysmlm caautkmluo' lsuo. aoummanypsaluptick Nwmd mwinolalas
S. Iseadtaycsluad actl*m Tbaa r'asuta me sMnJjaaddoht tallsadpeumlo Cooa doa h sailvItes ad amine thei ecod-s&al Inauaa. Onlt es IN=ea patedu provide Urn sedd are wil betempnyca* ovsmcaaby Isesasg the eudoc pvldk health came to thosnu =m esb. FI!ng deern Unapula patb ad haing doe qfing docr go to eo aes lhi ud decline
padg y ton amser dodm s plIced ha h sm positons au thC: Wblt lb r wllm be evatd atIo ea of phef b oe p*
to ene It halbl " Sg term foeb.
to

Tb 7: IAM JAYA fm
Is mdii. drnswlyem G&Wl mdhn aMm. Thiwilmi 896dat Orndeaol, o&wmohs a aMA tos baum dot oaIbboemUm.
2 , . II. , , l . a ..u. .- , ... d m . s...... . . . . . . . . . C...MA..w. .e-0ov d.k ummm and gmahadS.HB H3ugmoi*l I.31mmi,uep.no r.atg ovmm Odahepndieu. I. C="daWSUr.wImd pinvIbgMdhawafoHBprnisy
wadAim oft HE smgu bbe diuI md, SWe do dismallytoU de_vubp.uetppwduiem a rndo bkumgOm. wm be oamduuui
4. Ugpauss he miii. mido.d h, EC. Iposb qupmh avdu eni inalssmde %s mdii This doob oo. qupumt sod marhwua b eam ieUn Fos.OMaM bald. wOe 0040h.q4I to Ihatmi mu M&l dro mu,. popudos
- - __bm
S.Nkblnmgeonudwsspo &mfnlags go. uwmasuumiigm Lvii pembepui be aned ft dub.A. eoledug DmA.. Ur psokp duaft ton Ott p4eel yew, teo3.11I__Su, dWii *medve. mu an to pomdb. vow -leaof domS dimli Ab OMa ad P.M geAMm. he iosa d l InMS WMlWi _U8 kSU W ge*bdd d. i. deu_
apeo.smhi tra mvi dlvey4.8gb ~~~~~~~~ _-~~~~~HC. ello*_*t8aa_"b_L P_X__S hoFisXopns_~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
__ ~~~~~~~~~~~~~~~~~~~0

Table. : &SAN JAYA- HEALT EiUWAnON
_~ ~ ~ ~ ~ ~ ~ ~~~Fcmg I Iubii _u an _u.ld pln __e _R Codu di. .:. an -- _ _ _ ea
2. Ream" & nild.: Novde, baslnesnue edmd anhe kneaof awmmarzs of head6 ednoathmi. linsn Coomtntdie macsu and p iovieby to do. HEB Wuaega. NIbaidime muvey gecual. and dais mamid to MCEB asaoes and tetihh. in puaslolma. Also, pllg.
db..
S. Medi m&apmb hk eoqno%% w l wh do. mcmii dsIvy euy paugnfhss ,fi do. HB bam wil Poi.M" i nofik am rahodenve e~ea. Se_mI. iilmy Oam prode*package coldipland asnealinu. cmaym dus ane skeie toda. oomumky aAd doeb. Sob mo.iobod pubesk pevia0. 0idM auwviv pickup;d. be limd pockage;
0. NW adoud. n and pudnualoe;L FM memoycii samples
4. Media esase qnlp.ums.Ptm*d Soe provnead tos diAidts vld doi.b tolsA adopedi mail packageso Pomchasod admbaanW do.anput
3. 0 ll wape: onuilmoteluds cn lt a COeauc di* Oces.ORC). ~~~~~~~~~~~wIl be dovliped
6. e"iuffi ad- 'aIus~ GivendienedA ww d59 at .vpme.teleadi educatonamsauges II mungot Pry"d aNW evhab t e dietemg pI a. Rankul soda. AdSloal m94 haft prvesa ei aseilels ht nuia ths cng et Mdltboed a deploy adCd otaff 11in 3Lb. SnIuh of e -_ _;on I3d
7.MIodiIpIa beNa eucaton. As put oldi e pacity bulidha in bealk admasths Selecio ad proviinghealfth ndmio wdmip.S. fubnIdaada.~.(Laid BE yaclalt to auist dee provnc In kqmogdo pwi=L Ptqm~mu~Ta ad mack 33qaolaLi
9. 3vsoairn Mh4r vbto i ecsleeulgteSnigad n lconouct doe kckig aNd the Saul evam andy anda. BB bakn Amdy (M4m1den, vashade wil Ivnvov caollcion of ll ondois conayaaht IDi. In die baslnen provMide bys t the nw heaftth edna itoegbLeb. rlod arabmion. to graba"" prjoec petwmfonuc.
bed_~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~l
0

Table 9: NT SA MOWDOD
1. Blqulp.ut and bsine maak To mnhe caayof JC tD e wih m eOYNs e,to pmvido and du e Ib ea. llC _ ol ,p_naIeaua,h eqlamaede hi nuaau f te cod chi; to ut. tha eatInh s 1mt blood tmlon eoup*., w uaMZ ao ie ve wmndedipupztto iman and _ a
chat..i I aql.ufr poqandnb. TBA kt, W Mt.;ILOUY M m agans auulact adOSOYN bedd. CT_: Mana%aidd G&W
2. lThngw Conduc mad valuat dho btrann.a. ClWInca mopaavlhimutvanu fi An amaih dt.p to Ivnyso feqlty otoat psovidd and to inysui ha limnknwiling A midwve amd ThA'; In&&b ishmi ayamaI
b. T1htoeRRlm sunlesAt To doms.ptheat ofhe th w. in deeofa hig tk pn lee andAMNC hi mms dom and M s; In deaig wi*h diet eam ycme
a. Ta&ftl can b. abde and at As pest is, u gndln de pacity . halth cetma to pzvlda widw mope omiadig and isiacaa hteRC ahtl bealthmve
4. TinIng ht amw TEA..ic TEAs. hd mai v of utul b peas cm In do vilge nw
TEA.will- he -nad oI"mps Urn.qualty cthmevhespe ldadby thea
_dbrgiDgal~~~hetCd _ , It
3. ?umotf4WD m To m o_t p en UII btw m suan lseb of hbet cam seus Pmhase alb 4WD
4.Mdllmotpqe eihoCB:. As paot ovepipao poV e upavlu of tbid mde, b eg Amigptaff end m stohwe tnda p _gsumapoweralm Is ti tm aeaea glveahap ueaUneda
SMOup endonues mpisms TO ams aeuaempplas of medclippll amavailblead kentblets s Piczand dieiut ha mppia".IL has tijet.; pea of haImi u pIgmb. Othew meftdica pl m h NC.
6. opeadoI com inrm__oo t vlIemvlkatwym fptogng tmuil. hr -".te m Paov.an am eam Ae ofdh Bfpaiof*hm_ _se ama. aqieclail doing dhia smy an what. hI beconmeombls thee pQoa shue .d anh dthi c iveneml
ammRs wil he evaluated and thewir 0 v wil he somldeady eat of i-fnmv ecca otheai ua>ce.
phesl,otdtops*at.
%O II

Tab. 10: NITT cCD SURVIVAL- -
1. Umambal dims. eeuuL* Uhaid deemms am wmi com tme of k la1sad m.mtak snow .111. Is Imsa anmgmd duiumb ftbooIl oeus.L. 34 NIT. Thi pwSamw dill- I om* i 1 _utto ddi pl_Um Abq, ca_mdw m- Is l 4 _b. 41~a 1 dis s sdmds OmdmldaumeqMlinpaa em"e l_ * i a tieMll g9pmSmi insawba s4ad de mw- ss is -1a e m t 1epo
. nkmda. !Ssu a i~.u Iti Flown ad., m Ntowak Qmuulm a geum"jPw s IAe N m a IIPA ciubs owhe MOO"
L Cab admm; asahum msmiwvth .suA pddly k _ibw mahimpup _alpmuS osa d.
a. Teahiq DC doff amU dd b vmAmsIl bgdmo i fipemw vii. Immsded ri. d iam
b._ DPmA m sms and
4. Dmps sad inWed app es dmahs, AUl, To em. it me" api%s seeded* ft dfiosIt uanu avdib. pum id idadbmsidaimpsd -mou-nd msdh.
S. q_ZW_wo coe f PDsm _tohbrg Bn 0ow vt mlof_htoS. postlaul aumto nys.oosagut asvdlhm ftomn m t rni i il su.er oxpealhufwdoa. qubly I Examine of me ~if rassm sad isit of"s ,meses i is. u_etmspueCi as hum ses 151 lssew fissi s buima seas tenves w oat m.a. opeashmi soft Ow now. smug . ofiotemadrml bnin gms.h do mome otiks envies to is somut -. Lb. Gomm lipse
Pive_ .~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~C

Table 11: NT.r: NUrnMON- Mrn~~~~~~~~~~OW~~~~~em Rtea
1. ofau Id : To M4 MDD prav n IT. h lAiM MtP hat s mg ppgb o MDD C0oudr mme sa" p s sd dstrbue lowsS. £umy and gawksa of MDI)pbs.Fioh r.mpigaeaulnapoce adl, fIda Thisdrem lesrbe "Inkd ov"eul haaw aMaahDb. lo" .#apssI m m d apadusw be 6aiWgaed. bld sess wl ben pa pel p f** ovesst pvanr_.disbd iha AMy to tagt IDD.
2.1 iuohaflg aa*l cawed ith walahdg wedab abot =Wmiia I in an cesad nd etalatraI . bovidempuoa"anda. *Pumowy hfsitg ti ~ to cane ouudam bib a, Aid spsebe fo childdmau o am ae" ds effectvsaun _eiqg mautrin te ofb. Talf m*VimlM LN; _ ifed Aom mhaatu wM be dtlwad. Ti wi be d asa dt reahg *m a d and in 6* so a w h edC. MistnWg VuW; an at til um alend edusad can be a dIIwe. cbil_dr.d. TupnsI at M
S. Ad Poch" fa ADmuIed
3. huussls.I gihvid Aneesih sp a kV amm plari of mAteldornlpubupoIsiB to M Prod retid *strata Iuimmu .ooriwAiaaa. Davepdmmombas fw' I aMhli aa antDam so c et, aepecilal agehadi am. l?Wi WiMbemeooI akhie.alme aseewa a4r a fint I do area.b. ysusi aMs ehsmIs SW
4. ?oa delapa_eaipasa lb T pio na dia l aawasdohe b te dier cii E ms t a dtd ad o a toTh pusyI Ia, in &t ir_lmI barns, ha t _be l vey efeatiwe In NIT. Th eaaWt as a dv a lfore dhg chage In healtawoaree in dkis packag will* e plaapssbh msdhfsIUas of la posyaada with. deles sraeg l.a ire do t I"ofso roIs.eamepiasmt omae y aihs meded to a da imi mahvig levL This erA dasdtwl be tWd by ls etd opsIof dke prefect ed then n a bisams2 sdS.
S. buvSIgANe and audgout bmoublo To taget &*n mai problms ad chas po gr dor. In dass mmae ancoring CoadiutdUrn ma1adgsadlkmlas rgaasvieis ofpaugrmaelllths-mededto provie ewmnIths addhustina eadVbIti
, ... ... , .......... , .. S- ,- , ., ,.iaNa
0

Tabb 12: NTh- HzLTl EWmIcAION
I. Vadabnp Fooo~~Pauakts o wpewh3lt dmse" and uiN.dlozhup he HL couaske6m. Vs sad pwlds hWAit ean B naqasmia.4~ I. . .. ... . ..
b._
2. Rasaih & sdisM bl.ledaaluae* es fsaau fhat uaanaaah Coalmadkeimihan uvd wat wHgta. RAP mawp gwo=4 an &s rbtd to NCR utiou sail mad*ha in pat. Al.. Plmht.b. Mdtoftatmadhles; 1 eW qumlw ve to help hodo _wisss madw bl mods wl be*. Quaflhwa *Am ( F. _1a.
3.:mdpasm bo .iqlune a smilevasypqaauilssa, 6w onwill PNovdMm mapstt each of mw sAn. dulloa. Sol he dullvmypuudqpsad. a bpaeagswhasI twpla inmwvamoLe uusaymuiadm2 an efieadiv to dw iinmuaily adothb.Sa dmda4dpg y.e. a,ud mavl _uod. Ubhd_e peahapa
£g Nlwsaseaaybvd.
4. 3qup%ma RuN w al. a w d usless doo with w ko$olsto adapt 6w mdi aus bedaa and mabsal do M*upemmL5. MPC 0q~~~~~1 to edl sda.
a.,C Be esasw _n _d Nahls dat 6w now. ans;
b. AM Wt madld equlps.g
S. Us ftmffi -a l tamIg Given 6w nam mansg h d.wIopaeu of hea*t educationsomogs,aa brabha of PmWol.ad wbaltuath. mtzanhgagaa Rcav adWa. Aiblomi d4f bealth peoulds is comesbla 6w inkIg this ebasg offoaW&a M*Anal MM deploy adMditles fffkw ND.b. Tsif t dMOM - WMAm bekagdu.aNd.fa omk
6.Pllowdlps In hbalt abubadem As Peat of do eapasiq bullin In health eocdatu Selatlas sd pzovidthod hse a .Jncs las Alow ps.7. Bnaladow ED _rlmdw (ill x_; w bo ad ug X ta g duy. Cosudo t Wd and pan bi.y to hath
edo" _ Wdse_ ' ' I"' - - ' - -- -- I --i -'d - - , - L . I0

Tabl 13: CmiRAL JAVA. SAF MOmlnooD
a. V eqa m su m ThiswibeanlltiedbyprvideleseededticldchanbVaccneca a ell; h vacn A. C et beoeqipped dl ca reed hib. MW k, TIIA nt; ftvg Pate df t wM que egquig lCs h boayo. HO and posymudequpau; seebsam eabAt enieggecy equlpoaus Electdct is eael fr boibd. LabolomquIt d ebatemiss vc atbfim y a wyl s fe ame g e e eam poedure, electti_meUry eoqupam fe UC_o Seneic. elm _se ud.
e. matio _ a I
2. Idtmdndludals TEA a, Tol etwtin tTBAs us P s.d sus d .
S. Vddisc Inyrovbgt m s eosulalitiovlngite l )y!- his wi bsdowat huh.and di bdb_ .a. Iosa_ it cmakyMus; aNll leheof dw tsa MU. will ada be ud to sUit eqor ease binb. Mobile so Iuprowa faadd ot _a_olb - to it RC. lbi wM be mstod In it packe it NC pa_ps_ge iye d1valopuetin elaon s it mW ad c1 os_ fbcs easof s pecede. Maoydafw NC dp; d. 4WDea p pr nce
4. dsd:i d
aSiA modnedand ptogai -ocrs iwbeaae&od i ot cvnesflf.a s Al pe itayplan i itiiiphase f itprojec4devlemmaa; nuhaodpraheadi etItsetoneta hud Obeadryled sees it shul be abmtted behi do prjoje ladado.. An
peuise This willlde, i_us i elazh to it viae _mwive ad TbAs ad evl auetls ofi r lleasand b odkoicesdk linkages it _ eyl _m Al. itb slv Iand tpes o d ddanindas vlabo I pvice diou be prvie by it sawedwl t pi-ls le sad bof skIl a sud t pls of it *pwject. wi1laddmsedin its pacaps. belcolsoraad in plsne _tpla 2 and 3 -of it
PWW
bJbat c_pg develomu ams rlat to doe h castes a a min uit In it real sys 1 and it A pelnay - it it At phase of o prjectbalne in di ias needed to _uss mviees a it cs, -nd it outreach ones to doAd be _obad beh tke proect itlne. Anit vlage ms&el so t f pas dead mese at elderbveL Heat cene evalt of it difhea abasmv and it celsamugean ad id qpe of pesosuad seang needed aso lmo h i dwI avaib so it proic damn be prvd by it adbe addemd in 6i paage. Moves an evautn of it role of subulan (r otfdi £bddtprojecL Rcoaaedati1mwlllhMUs in inpuvlngeilacslvmaeuofitb _eil n i. hadvantasa hea be cded inid pl an it pbae2 ad 3 of grididwAnageof acquirng hese biead ds _ enad spertle coat pojectwibeaddas bs ea rotitht c_ paka.
S. Dre_g1 s it _is Jebhoodayesatloam. haute adequate mapply of hug. it matches. Puw_luass ad dibtabt hus.

-82- ~~~~A.NNhPage 14 of 20
s1 ,II I-* .1i 1lIf ii I iiIjl ii
i xI 11t IIIi!
l iii § 11,111l Xji1 ii,X t ii' }1 It
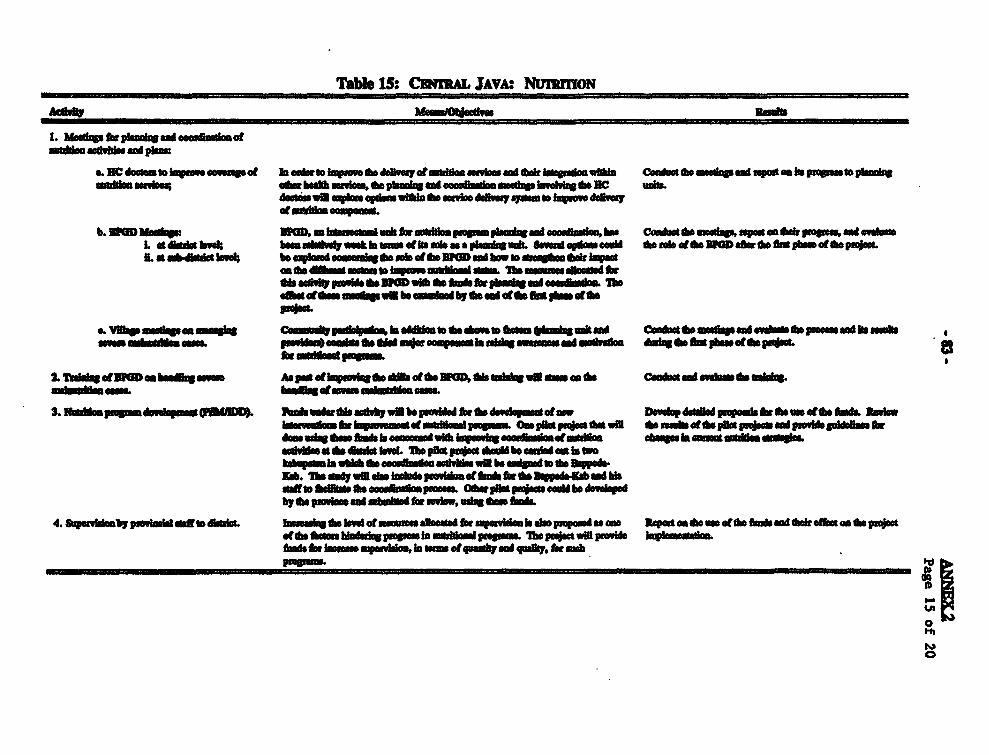
Tbe 1S: CIRAL JAVA. NuTRoN
1. Megb3s mAhtizpa" oni
a. DC doma kV IS ofs..ua. h a*,to law ii ov .o A57.tsddo m NWk &* gmi bgao ddhh Clo~ d a. imis ad upon aos hepop=sto ph.siswsIIba - mint bhaab m II no to pimiqt and " Ce mmssdqshwoMz do Be mitoduas in spoisero qanswIU r wak dsvsq Ijw - iso weddw
.tmwhmiim wupsm
b. IMNDMsulq. hD, - bsaua.t..almuh Sm stWMl hlU. pug. la.ia ad ce_, baa 1 cua.*mboo Co_&w awuabm pmaask X _ _ atdi _ vL a dut wk; bbm * Sm-m_S'qdowi a dis .ta. IPOD da s oa t *tdepm.L.at wbdlu bo*l b. eqimad .ssh - U.. ddWmis.a d hew odaqaodwk loVwe
amssdIdgmu soMuts ymn uusblossddL a. TheUsMIMasafloed S_d__tfpo*W_tA&whotwbw#N"_SX,Lg
_._adeukhasL- .ithuvss wiO m s I win gad a.d_X_ E Ceft d*fMp .motd idda
S. IkbmpsofamdlmmaIUD AsudaeetlIa loh owIbe gaMm_d.sopd a wlsdo DewI "d gpuu ft is. X*_
3.1 ~ ~ ~ ~ ~~~~~~~~~~~~11 o II A I I a -atom DovdopddS* iwdufidko1WL aM_K__ at mud mp"dZ OmgtXto 1 14_t11pltPSS
desuay .s.Oti isuammuiviaisyay.a aiumafsidioa .bwsaayuk'sw dmat dmU*eIs nA do itia hveSM hpl*p*m4 isaube ambi as in to
kabyaiaa thsa .eaeooduua snu. win be .sludwasew boda-Nab. lbr*vdwbb wbaaff mdBma b e a. eeu pmo.. Oiser pWagujesa be sAms,lopabyo a. ps -alm "baftbifo,reiw,m vft&mssebLa
4. ftwiosby p1soultlal t _sL hamasreUnsaveS a , saailsesd It ubels isetum d aa s pon odooned A and a.k deNt an dor guJotdks*,hwsaae nyasaisiss am at qudaakd qoalky, M MaIm ngmkoba
0

-84-~~~~MI! Page-16 of 20
jI iiitl t1
I i' gFt |4 |{{|t tX !F§ z I8 ii}X3lt1

Table 17: Wwr JAVA SAW MOmzmwooDAcOf ILwa Palim nmbd
1. Rgin d.hpua hd. w b Tks rs..I wbo nud oodwelhp" emS seam bea.L eI I bes L Dweya Alaadbd pha LwE aedvheS tbe labdidso'mba m.m "Ovihu. abmdve. wIN in . dm.a .el. .M of _ ra gbes.tha _ ...e ad . .adak_q*Sd X~~~~ISGlbpmMw&wTBA*d._tt Sottit_-w olTmsuahy hate' d way. .(.OuI4UiII- darn sbg aidwidflhbe pIDA.. i_r do aid otdIu.. 2 adpS.adinedn dataPpesbi..
a. nw NCda. a iwwae MdoIeemtuI-Irn Ia it.. pard add60a. mi doh egmt ud (la 1.m-~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
e. DeAdaethafI4.N
4. MeiNud.pwLomw abO
a. Mciift
b. 8_ b ot_|rI >_ *D _e h_d-* MO_. f
f. W rUd- ,thd. MWbd ap_pwM adus ;.e
S. Vdhern.s.qde To btbeo. 7anusa Lw heag :l_lt h ,.k. Sboat _d iaIw.esb
LPMIL~~~~~~~~~~~~Id l o b~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~l
5 To tali a I bun P os_alEtdi_*o_

Tle 18: W;r JAVA CHL SMVIVAL
1. Ws to hmmlU dbEd umyd woMkh Voi 1w at s - JmwinwaOmuimd ggag.. aad uwdUaopujetmad coh Ws, binmtat.toasWadhggPOW ma upw. an ha uc amdd o"ME. adduas I alzmmu . ddad" 61Kd aovala I p.u a wadhggm buciAmm In do dhEd =PWol a
I *adm em l nmmusmMOg To Iuaon 1 sou "t mmaban hm o.*ch_vemuet C_t*"wmiAq mE pd=omw=Wllp sash cuash1buum ed& a duu,*aW%I eshatmlagpmdobd ubash Abdm sMd uluM sOm g m Iwdww lao 4 dh diaodG ( mI All111..) w be ooo*Nud.
S. 2T ai AW% and d__m T a os COOl&o "db rrt sMd.ah _c_t%wsmug het w6 mads dbEd baMs p6mbm. lbs anmab wM bo hpgau
4.Pg A1 Mmh_dMwv 96 Ws _b wdk d
*. ~ deinu~ ~w la ahi od b 4 emm etuaibEiy.b. hidc
4. ~duw mmt ha. hiebam*d. bE. willIdo Mr hid.aus s hau. adiuuhmdd.spiaga Do-- ii e ln a N ila w sy ,
quads lu_a_b manV dadE hi lasywc p*u
a. Tiunhfthi Upimicd miadg dao bhui wIa and pmespanI'A a bowm coM awba he opo*um.b.Sp%wiMhiuii idas" voch achpmud.
- ~ ~ ~ _ 0t -mbq and,
U-
6. SwcagoauI'm la hI" IL m mdIa*.uu latp mhsabus*b o Cctlao -II S a awp i astla As
aswMinw 0eido mernmapdimaeddhusghuama*d.
7. ARJ dauga To asm osd.9aa so"A at&la miold.. P c aud dhiAth las All ding.
L. Mouodns and evabomus 111 bncds l& cogs hin Udo paumuI to psovids mo zaaabma Conusia doudeiwlng ad pavue nd. p maneduslo pojCte
0

Table 19:0 Wugr JAVA: Numrnow
I. Usyada dovaspewf &a&a beauds,di wil be uned to sdd.. Ba coofo*EgvomosatahI Cndsd. '.4t embtd mmdlya in nukhiiedietbeaowlup.v'OnqaaapauI .m I IUnslWbP will alehulden ddy oG and osyaaI lwb(po tv.UT1a odand dem
2.3 MD 134 PM ngSm 4wethpmsn Bnds. bassnuste ds,ahpn dabsaula aunaghl todM D aid Put In do DwaIp M ahui - a hrban. 1, eeemsaznd wluuledo
__ n*<^o .bem i - bS_XXamdmdstdk
du$negs Is do fle 2 yeau .10w #=isi and hInaorpmg Baa mobi kWs in I.peiiiIiUis a nd 3.
S. KMgrnew bwe 0w muoboahggmtudhm To.eost0w,sYqaps das a Ceadu tag _gXadtodo ee_dbskm 1a. Tid_es ottl a lelli aId, -ppaamiad Aslb detlohly biL usn aiOilotdy ob. Iddagf&aabpeumi (F 0*4).*. Iylwainarnotdma mzveq.
4.1W ingmutudeThsohamol To rpema P31 sei 0wdl a dw TonD hans, sa" o1 eIab CDoapad eudaB 1, Ina.T ThIi3IUGD aonl asivib 0w do 8DlGeooeld, t, and kndm planned.b. Tzabti IFbYmv. Thing .tTo .wb. l hae1ase*
S. W D _ __isslusraatamlpagr bso hba nil tmpairnalI b loseussm c no_es Cloosot and walmdad he *#.planing&, Smbahmtuuahmoasswl0w). asa*Lwhlh Thsk uirbsom bown way offli'min n affesin mRl.eossm palsieIn dver of muabmi paoheL bhs.Tha roam WEa be mad to *so& idon0 roli|_ipb^L~~~~ovm _*II*b_XgeboL all IsaiDi.nsdang prowlin ar auish tadae_ .1 1Pw ml_bi,,*_l__brd'BOaD~flum
6.l,'w o 13o 4 aIN he_nsabab . bsl ot ompooanasl mdnyW Male cas A sewassa,_ miAioAmasamad nudtr0w 4mvu ftotaV Rs m e wmil b ao hr b
7.-1W gif& Tesyshooabed: Toallocu.0wooca tW ony. Bamads e alMbe P,d. rd rpetal n man hr Xlfe PMa d
and ebom lnuiayiedlu. .t10w ducdaomddnL eI
0 A~~~~~~~~~~~~~~~~~~~~

Tale 20k WM JAVA HELIW EIoNCAN
-b o -. pvm -n Realbwd
ILI W JIIRL
WS.
2. RIlasmau& adhaM P?oulde hemlie dbwnnus vibe te -,- atwm at Coaa*doe br saihad pzv iomlse to do BE iadegh planin.a. KA mevey( &M doWi..) bulb .acasouloshaa In gPaul aid &M. aided tob. QuaDuy. dum (120PM MCM mavioew and medkia inpeadsbI Alao. spedaa. Mandlasm woakt dndy (24 qubnaalv maceach to help tamn be maiagm aneddb&M*a hea =Ad wil be dew as vell a ad* an lubmadlos
zwo4 _ d Z_ l_m_bkd
S. med packagea: c 4 Ib go do dulft7p og PAVU0, mNedia Um g be c .Ofd bIMND deliVwy *M%WBM gk usa Svieo dvay _ ;msacam be HEa will WM ,l da paa l eawc of elbiwo be c _mmmlt and be lmidcin.b. Bo mmbadanopaag; bke p_and bfe_wdom As well m _ b
d. NU_dh pach;a
4. Eqapamat pssvhw packg and &due POW&e dito vincm ado dbe db VAdomb b clto hubs..nd nulamIs e esft"eiPbpasage adeptbe medi macage Io local made
S. Tnwahe. Glues be meateg be dsmhpmatohaal Push.beealalg ad men be hvofbuwle. sAnuag pwAimsbeiua. Dhasut an R34 edmaulMaas tiiig cthulb Pescie and er ae e do aag.b. llo maf anbi odutle; a b a c l.0. NC m.e
6 bww p bl b deaA pat et apauei blbdml Saconu anid I ua buedtuehk'dpe
7. TechnIAl adaMeffA. Aoldbd pein In fmauadzsprnlm and dbia Taft SW mlocal cinssnlu-land hi adapdvg meda pacbkaso local _m
S. B _a old4aom ebe td u btbaoking Conubt be UNing dy ad prd to bulb dcoad= W*Se.La. :MU4 HE tacidgu ady ddy. A fd1 evalaion wil bad an data colecI Conded fism hul _ol-db. FIm eaats eStat to produce , Ifmalosa In cvered to
beo beeSfln andy QW)
0

TEIRD CONMRMUN HEALTH AND NUtnUtMON PROJECF
SUMARYOF IR Y1 ByQmoW wr AND ARI(US$ Om)
L I'mvhdu Cempmms
8h&Madmiad 8,54.8 4.3 12*47 6.1 1,89. 0.9 18,994.2 9.5 11,92.2 6.0 53,521.5 26.8 42% 25% 16%CDi Om il ml 6,53A. 33 81.4 OR4 1,180.3 0.6 9,530.4 4.8 24,664A 12A 42,M3.1 21.5 34% 20% 12%NaysalqNaII Iam- 4,814.8 2.4 1,520.8 0.8 1,761.1 0.9 6,444.6 3.2 1,415.1 0.7 15,9A6 8.0 13% 7% SSIHulialwadou 3,318.1 1.7 4,214.4 2.1 1,694.8 0.9 3,54.1 1L8 1,94.8 1.0 14,78.2 7IS 12S 7% 5%
8i,a"u 23,88. 11.7 18.7593 9.4 6.4258 3.3 38,518.8 19.3 39,943.7 20.1 126,95.2 63.8 10% so% 39%s
IL ImlUdimi Dsmad.u #ad C.mkv hiub
F&yb t gmIDwvshpms 1,906 1.0 2,186.4 1.1 3,441.8 1.7 1,461.6 0.7 4,406.7 2.2 13,405.0 6.7 25% 6% 4%
*Mmmmuao 735.7 0.3 956.7 0.5 13,W25. 6.7 3,52.4 1.8 1,583.4 0.8 20,09A 10.1 23% 9% 6%staff D.whsm 4.707.9 2.3 9,381.9 4.7 9,5973 4.8 7,514.8 3.8 24,123.2 12.1 55,325 27.7 62% 26% 17%
&*SoIu 7,350.1 3.6 12,525.0 6.2 26,22. -13.2 12.498.8 63 30,113.3 15.1 $88.7W.? 44.5 100% 41% 27%
7.2. 3063.2 15.3 31,284.3 15A 2,&778.3 16.5 51,017. 25.6 70,057.0 35.2 21.5,7749 1083 - 100% 66%

EL Caira Suypoi Swukm mi Ova*I UuWidg
~-Nmu II_D bd,P&Hd Nod Low Dmse oam O aw~~~~~B 0$ P WS VUs$ Rp Us$ 14 U BP U B_$
Nejieg srma 5,17. 2.6 4,60.5 2.3
FbsgswapWA 18. 0.1 1183 0.1 1,1742 0.A 20.5 0.1 0. 0.1 9,819.2 49
TOAh I Wt 0 6. 4.8 266.1 0.1 6.7 0.1 $,90 43 34A 1.7 2,W4 LIP I
Oqiuai & 25.7 0.1 60S 0.0 101. 0.1 1ton 10
_bqawIumaI 9132 0X la" 0.1 1".9 0.1 1423 0.1 54.023
Opndeum 3,515 1 1 1^.8 0.5 103 0 418.9 0.2 311 0.1
_Sdodood 761A 0.4 12.8 1.1 4,1.1 1,152.5 0.6 7,113.2 3X5 39 4.1
Tod 14,065.3 7.1 4,37.5 2.2 1,018.0 4.0 2,1703 1.1 8,90.0 4.3 5,175 2. 11,1834 5.6 27," 13.8
w

U Coam Supt Si. and 8Cauadt
3~dP~*U3m~ .inNwlMna 4oNsihm"am* bud d..*.. J,..
1~~~u$ mokm=N i U9 UMs hag ha
~~~~.Eiuma ,.*~~~~~~~~~~~~~~~~~~~~~~~~~M 4.9 9% S-a
howb"n
4 tl2 ,seulm 15. ies i
_ m
QRPWRAM& 219"~~~~~~~~~~~~~~ US 5% IsIW 251.0 Is
_pmgdomd& UW Si
A_
s,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~t. MIQ 12tS I°
T_ 6^ A*IA 29 $04 u 2I7 IA 4X 3 4. A L S 18

INDONESIATEIRD COMMUNITY HEALTH AND NUTRTON PROJECT
FORMAT FOR KABuPATEN AND PROVINCaAL SERvicE DEivERY PLAN
BRecd ,ama -n MI.. San* I I Inud. In oVIalndaor Lel SiWn Bvaatiou Plan?
BY B.eulmaffmVENTIMS lnwator(s)l Dat Memaurent po I. fisu) _ __Scie (fan)
SouteS) akod(s).DL Pv.
DPt Paw. Diat. Pro.I_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Y es N o v Y N oL SAFE MOThRHOOP
A. Health PtublemFor eample:1. MO} ba ldm
B. Detemants (a/Caa Factos)a)For exampl:
1. 2.etc -
C. I nrieao sratsFor exmb:
1. Ime aaswanss of matraheafth pniblema et comsaknny andamon healt wadher
.2. Improve bkwedge amonhe works about bigh dsk'Pre a andreferral syaem3. Imov manageme ofobtti mrency cae, that
4. Improve elysmS. Wmpom Tr cove6. hvonuterml
7.1# Sal u ldlsategs
.V See Acx 8 fif a ILe of sqUestd ioDm

D. k. ..For -nriI . Thh _mwer nTmandMW. on unasnsetoftiabi Pr*8rafs7
2. Upgramu .dhi .Firmaw3. Jnaz.mmpplyofirntab ets4. boom A of
S. li mlibeof poraadw etmO6.etc __ _ _ _ l
I. CHILD SURVIVAL
A. Haddh PtebmFor wounple:
1. Hnisetodmeta&y*.-.
2. DetermIns d.
For exuapl:
%0I. Low" tww2. Neonat tetmas3. Did.l d _ses4.etc , _
C. Irgeeeton o S otregeForwexmple:
1. bi2. Iprove ubsok sabotmOeds an to
a. bv" 4usdmmof
4.el
D. InputsFor example:
1. Pwd equopwt fo old chain2. Train Kaderondnbedacam te3. P= ose about diatealdsae and dhir dage4. etc..

L NUU_ _ _
A. RO_hM h.au
2. MDS. Nsoddel An.m_
B.Dstaniam,a
C. S _ _0 Of ." _0 .W .pa-
S. I*akozthd aoalodWl
2. Jftisgzu wau Idomaa, Po wars., about
Outdtkiona Vaon of isad kmr
4.3g. _______ - -p
4. h S sFor .imuph
1. lm soostolodls
2. b kpsvo eduoslwlaawsanaboe atltoumof viinsaoffood
S. To abls wsomessad - dlg*Gm4. IairovhEsusto,alg
D. iqintVoW eamaipi:
1. lasasa ssonzo.to hO2. Provide .adle opn.ssS. Taisi hseft worbis an
4. ProId koe ables

DONESATHIttD COMMUNiTY HEALTH AND NUTRITION IPROJECT
JO3MT FOR KA5UA1BK AND PRONIAL SWnCI DELIVU PLN
m - -sP
D@mvinI113N8 faisarga)J/ Data 0 hm fim) ftw* tm *am)
D~ is. DKL hoI _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Yv N ol Ye N
L . RW8U..dMdW_____ ____ID__ _D_s ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~~~Y N
, .1.ur$
1._ .snhs.2g.. $W. ______
LSOZ --MR- -
C. NO" mWl.ikUgI
a_..OMFor mnw.:
1. su__S 41. Iaft..wumasIta
C. q badbwmbmg
3. h ammet.idmu2. Ja.s.ineAw.
obld .,gaboums t ba*U4.JWvium slat s.d
S. hoTaweeaof
4. Jvmvweradmgm
7. .__ _ _ _
= _ u~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~'

-96- ANNE 5Page 2 of 3
l i I IdII II t iI

£ C Sv L6
XHNNV--

- 98 -
ANE6Page I of 2
TmRD COMMUAITY HEALTH ANM NUTRiTION PROJECT
AN AW O DCIMN MAKN AT 1II KAUWAUNAN PU8K9MIM
P Inary TOlh
1. Th key decsion maes in the heat servic deir system are the dokabu,pussms docwt and ot staff in charge of tho Each hsu potentIaly avaible alarge number of alteatve was of meeting the hel eds Inh areas of respnibility. For
,he O health cear doctor ca assg his staff to work whhin the healt center or Invaio outeach acdvie. Moover, in suwb outreach acvies he can vay the intesity andmix of af Ivdlvem and he can have his staff enga In a wido number of Inwaction Inth commnity. hese, might Inude vist In support of th posyandu as wel a vaious odtcontac with difiert members ofthe community. Siilay, the dokabu has some diK_qcontrol ov resourc, staff, tets and goals assined to health ceners In his aea.
2. For Weslavaastady needeotat exms h actualor poteal pro mcoptdons and scpe of *cotrl avabo to the hath center doctor and dokabu. Tis studywould ha a nmber of componeand objectives:
* to determine ah rag of options c io y resorted tD by these offiials;
* to Idfy runcoddnvePntona opti thd t bh been employd, apey effcvely,by soMe d m;
* to exmine which could be employed. Teu might hIlde nrmaef tot in support of posyndu, 'sweep' coverag a wide rag of dircted use of
staff in su t of particuar objee, inceasn th intensity of staffinvolvemt and use of finacal and othr reward, use of part timetmUpoay or Contract workers, adjusti hour workd by staf, and so f80d
* to review program and optons t aro employed In ote Indonenprovnces as weill a in odthr cotries (eg. tain and hn non-tenured villagebasod heath and nutitm workrs, selected use of lty fes and rbaes).
* to emine th posle role of NGOs in dliery ofserie and support of staE
* to esmut reowms earned can be retaid in the halt cntr.
3. Tew study, which shold begin at lo= #ctlwn, should be cared out by ateam up of _ dod gand local woring in cooperation with th West Java
hath d _atmeat The study would rey princpay on qualitative methods, paiculy I-depthinI wh cuar and fmr dobus, hath cenr doctors and other rdevat observe.

_ 99 - AMMA
Page 2 of 2
4. The sudy wo be epcted to dboat to 1 sane, of opto av_lab todeciso make in p_ur S ther servic deiy dobjedv. In his rrd, tho study shouldd%iy prgm mptios whicb e cume enly sot big utiid but which are dato 1pfiotn in CHN3. Mh sudy wm alo considr was of gaoug ow well decim makes atkabupate_sand kecamat levl hav deemind nd used qaropria opto. For imace, theslau* could recmnmmd padoWn bwofim gd di d tt d idght be applied as well asindicats tht mI be used a a way of evlaWg the pau an of deision mdes.

to 0
N ~~~~~~~~~~~~~~~~~~~~C 1I11 '1iji III'~~~~~~~~~~~~~~~E

- 101 - Ab2X1Page 2 of 7
Mh moniorn system would collet two tpes of data, namy sae al nd periodccrossectoal data. Th uequeal data would record the mar healt nd demographic eventsin the monitrd househols. It would also allow ra for these evens to be calculd by_h4 fthe number of people over m who are at risk of the evet The sequea even
histoies can be coleced by vib which range firquec from wee to yes. For majorIIlc and heat evet collection cycles of about 90 days provide an adequa banc
between Infomation accuray and efficic of the surellac sysm However, some eventsmay require much more intsive data collection. For eample to y monitor acuteinfectio disease eves In dhdre, twice weeky or weeky surveillance is often requird.
Finally an Impotn aspect of this sequni data collecton is that it needs to be acdvely linkedover time by use of specificaly designed Individ Idnifiers.
lhe or3,,wecional data is collected by spec modules at various times but can belied to the lontuodi data. Typically this data iacords household such associoeco i status, eployment, educational religion, attitudes to health servces,heat practices, healt service utiliz as well as housdehld riskio. Thisinfrmion is needed for the analysis of health program effii and as modifying factors inedological stdies and hImpact _ of heth interveDtions.
Route suwlac reprs of the data collected In the monit systm providevauable desriptive nformadon about dcanges in morality and frtility rates, the incidence andprelce of diaes, disabil and health service contact in the study popltio Thecommunity heallh abory needs to rporthese findins rply er the completion of eachdata collDe cycle. This can only be adieved by designing an efficet data prssng andaysis systm. Ihe most difu step in this process is the desgnp and mo ofcomp progm that can efiety count the timee nron m needed for calculatingthese re.
In countries with devdoped vit record and halt iomato sms reospectvelike of the demophic and health data is used to reonsu the popul cohorts.Alernaely the demohic and health data can be used to gatr iormation prspectivelyto eval a publc health interve Tm roaches ar not yet feble in Indonesiawhere vital record systems are incomplete and where many heat events occur outsde theformalhesh care syst8L 7hu8 a vital chuwxwisdc of a community halt reearch laboratoyis that i ita longitnal rerch either directed at idfying risk fictors f1r heatevet or s _ of halth ierntn.
Poteil Drawbacks to a Community Heat Reseb laboatory
There a number of risks and technical limitato to be conidered when plannnto invest in a community health rch laboratry. The ris rdate to the cost and thefasibility of hg demographic srveilne over a sustaned period of time. The
tehical mi se o the xtnal valdity of research finins fom the study area dthe poteta distng effet of a prolonged presen of the research team in the community.Each of te ikses ae exlored In more del below.
CoAt. It is exsve to Implement and maintai a long-em demoaphc and haltsurveillmc field area. he cost is influenced by the itensity of the survelance field area. Teco is Inlenced by the inten of the surveillnce method, the existng infrcr for the

- 102 -Page 3 of 7
fidd am e d d troure alloon to h project keo gme hpl thecmmuy halt resarvh l or . Iho o st D to be blaw e inst the lr amof vuble uaon that can be produced fAm a lug-tWm ha realaboroy. It is alo w re com t em ciet tad long-er communty haftlaboaW tahr dna swmof£bo_ kdd est, andodindfr P. m - adimplemented by a varit of s
FsuIbeMIty. It is a comple pooss to deo, imple ad mainin a longitdinafild r areav It rqs cared fild to maintainte qualtyW oyfth datacollected,ffctive man_gement of linkges be to dat prosig and field stzff and awelldesiedW infomaonmanenmt adg data m lssssm Rowe, advaceswith miclo cm q ttecthnlogy make the ImPi ofh dia mmagmnat and analysisolf d _w BWscdcommky had& iedd resead mmr via
Exteal Valdity of Ro1rc _ Rel. A commoly risd queston is wheher tresut of hea studies In a small population cn provi bdet i usd *r largesce publc halth prm. Th mw to dhs qusi dqmIs on what srt of studyreultsare underOW6918
Disoriw ffet s ofPtiimqud Cuztcwith heCsmmnieiy. Another concernwitha long-term community health resarh laboaitoy is doe possibliffty that tho ruUiedsearchactviy might iuec Se halth of de communiy. Thoug thi isa concer k should benotd ta ther ae my community health reseac labortoie have montoed te samepopulation fo 20 yes or mo and sti cote to produ valubl rnao about heflthIneventos. Morev , with 8 syse desned to take only a sampl of howakd firom eachcommunity and with only thr to fOu visits pe year it vuley thAt die activityilsW Mofe kehoaft ffthunod.
*Nojec Components
* Descriptinof Ptopoed FM Ps. The projec wl estas two ld amr forlongitu l fty h rc b on a of b oitm a distict Oneof teare wM be locatd In Java ad th ohe in eantem Idons Creia fr sdecdingthe sites will Ilde: whehr or not k is a proity dtict f1r te Commnity Heal andNutrti UI whethe or not the ha bee prvu resear& ad population monoring in the ar ke sc feasibility of d In the aand finaly, whether or nt th ae has su_cie to rqern th rag of socLo-econmc grops and ecoogil o fd In th pwvine
CQtl Jina. Th prefrd sit id hs prvine would be theon joand woud extd field activi sate In 1989 by t m m Cliical Ep oloyand B Unit, Universiy of Gdjab MaL Sdelon of ths ite would grety faciltth estbl of th rDe ar allowigteproectto rcni staffwh a ined andeqwkced In do h of blongldind commovity halt reseach and In pariuarwith tw prposed poputi monitig malods. F _*ere, t stff would be faiarwt the loca condio and the loca MO staff. gm daa co9llecod Ind Mokts TrI would
Am for the fiel arabcue to d wavi ae used tho etird po frombowiufofdlfidambecmDwwoto aTholbsusdodre from

- 103 - A XE7Page 4 of 7
just 31 vlaes. Thee vies are fom two subdisictas are all loca on te coatal rlcepli. Te ew fildd area wod gretly educe the sampling fat fm eh vilae, Inceasethe umber of vilages and the nmber of sbdiicts Involved.
A further avantage of sdectog the Moi tam tlD Impl the Ceta Javasurvla area would beth consiabl number of te sal sf locaed in Yogyaar whowoud be available to spport the fidd area Ths staff indea nutritonst, nmuses,
ao is , amreshasts and computerprogr_T.he latter wouldbepatularyImorn for th dvlopment ad rmaea of the proposed compteizd reilflancesystem. Te curat Morvita comput team include a part-tm senior rogmmr who is alecrr in compute scin at the Universt of Gadjk Mada, a full-tme prgmmer who ia reon UGM couter scie graduate, a fill-tm statcl astat who is a recet UG1Mbtatisc graduaes, two fll-tm grduate research a seor datab mangr andsve d operiene computer opersator. hi team woud play a kwy role at al the fel sitesby developAg the progms for the urveace systom and tig staff from odher sites.
Alteative sites will be cona ered gSi tht the inal four prority disticts for theCommunity Health and Nuition M project actes wil be Gobogan, Wonosobo, Jepar andMagelang. Th fina decison would be mad once dth prvincil aioy cmmittee IestablUxshe
Nusm Temgpa ln M). The prdemd si in n Idoneia would be inthe NTT povince. This province was the site of a project in t late 1980s dut aimed todevlp to capacity of the povici Health Dt o plan sa eat hea services(CHPS project). Ihese earlier inputs place the prvIn A srn posion to z thoIhnfmation th would be gat from a lontd community health resea laboratory.Alo here Is no eisting longitudinal field activity In this pvc h is lconsdrablebasedine he survey data to assist in the selecdo of a iabl distict for die fidd monitoringarea. Furhemor the ologia settg of this prin contrasts sharply wih the prposedsit in Java. It has a low populaton density, a poorer econOmy, less he adrer clInato and dffert agri sysms.
The province has a tota population of 3.3 mifllon iving on 42 idands, although thmajority live on three ildands, namedy Timor, Sumba nd Fiores. Tlere ar 12 disticts and twoof the iwr prior d c slectd for the Cmmunt Healnd Nutiion IR projet arlocatd on Flores. Ihe disict of End and Slka ae poslesites for t community healthrsrch lborty. Each has a ppu of about 200,000 and both can be ased by airdity frm eiter Denpar or Kupong via Maume Both hav hIfant m flt raes ofawound 100 per 1,000 lIv birts with malari, diarrh and acute lnwr epary tract
con begtS prmay ce of deah i ildeL Slkahas lestaamay t for be the mr fesb of the two sie. Final d about wher to loat thocommuniy halt reseac laboroy woud be made once the prvinca advisoy commitis fomed and once the dicts are viited.
Te fie laotor wowUd be managed dict by the Univetdq of Gadjah Mdasincether a eo local Flom with S eperie or sistode wd dththelaboratoy. UGM would place staff on the site on a rotating ba to establish the fild area ndto mor ngoig acv .

- 104 - AN 7Page 5 of 7
S~ of Conmnity Bedlh Research a Manmt of thmjor actvitis of the commun_ y heo research laboratoris wold be aived by a sedes ofcOe_ktM lie to leuk site
Natind Advsoy CQI_ttee. hi committe would have the role of monotonh owea progres of So community halth nd nutrition research labo ries, ensuricoord binatio of poect aciities fom different scdons of the MOB, ad proviig thelabo1a-ories with a widet die withn t MOB. The committee might consi ofegg e senudm of die National stt for Health Research and Deeopment, the Dkicr
fr Infcio Diea Contro nluding te national office of the Fidd logTningProgram and the Surveiln Program office, B e, the prvinces involved and senor
es of th univsity managg the field reseach and t programs. iscommitte would meet once a year to review anmn work plans, mor research findings andprgrs with the training program
!ovha Advisoy Committe. Ihi committee would be the key to link theunivety based research and traiing teams with the MOB. It would consst of a seniorrpvopnpntat, of the MOH from theprvinc,senior rve of te university managing-h field area, the dirct of t fidd sw, and of te aWlied rseach and traing progms.This commite would meet two orree tim per year to review planed actvities, to estahresearch and tainng proi.
uvila A an Committee. Membership of this cmmit wouldconist of direcr of the ace ea and the leads of each of the tm working inthe fied. Primay ivewith projecs acdve in the field would also Tis teamwould med once or twice a week to review field avies, resolve problm and fa liaisobetwe tam.
Apped Reach C _omie. Me of this committee wouldconsi of te directo f the appd research program and the surveiln aa, and the=Pesvnoative of the MOH. t would be reponsible for revieg reseCh proocols forprojec which would be conducted in the fied area. The commtitee would be responsible f1rensurig ta the research projec conducted meet propae etical and scientific standards.This wold meet twice or three time a yea dpending on the nuber of protocl.The cmmitte might sponsor protocol deveopmt semina if necesary.
Hmuanm _----
smTraining d d o ad Commity ealt Prog Ma e.To meet the need fr MOH ditrict staff skilled in survella metods ad prgm
it i prposed to provi scholarships for S2 taning at the Univeriq of GadjahMada in he id d gy Tining Proga hese t ees wodu rte part of thrS2 taig at one ofthcommunity health rarch laboratodes. Ihere wouldbe approximatyya tot of 10 scdolaships per year f1r staff fom the participating pwvic.
Develpment oftF at UGML Resources ae needd to support te deveopnmtof k TP progam at U(M Tbese include funds for devdopment of the lIby resocesfr Pstudn, the productin of an 1dn_ lanqg version of the EPI-INFOpid oogical analdys progra, reorces fr v for field spervision of trainees,
Ift,II1 hh[tki1I I bi�fIfI 'if Iihi till' qII II ipil �iI iii0'
fIji 14� ;i�I j1IflIIUIijUt 1 IIijji. hull"I iji K[I1R�4jI di1111 � hil��� UP

' Ii l,l,ii 1i11i i 11,,[I~~~~~~~~~~~~~~~~~~~~~~~~~~o

DiDONFID ZCOMMUNrTY HEALT AND NUTRMON FROJBC
IPROJBCt MONIrOlRNG AND EVALUATION43ENEAL INDICA1O)RS
SAUl MOI D, ? .oI .r .
__-. _ _ _ ___ _ ,, 8Al!lB IIIE07IIRIOD
mdasgDofDda Wm oam aasoh.ca.beusMs.waagIsrqad.aal I I X I .~~~~~suoU a_D isi bmM uabL Xss~sl Xea X. X XX
M,tesliealy MsaIMeat Theuwsr. yn nshMbkUA p^si OwOmbospiya. ha X X X X.~~~~~~~ssu _bduk dao p_hil,a epamafnaodaotss r ogM
l p. yIsV . hiss b- Ms o ljeb_wahda0 ao t a d cthdtsMsuby Th U*s ddsEms-2Setbtidynomadda( ?hapr X X X X
~ __
Fe_1*_ h_idd>-1to_4r X XX
: :zaz~~qoe 4s*f paU1dsdby amb*e ebo.ahd beaMd toEm x im
. , t ^ = * _ . . . ; . .. .
,V~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~a
1i_ V~~-Ndon I P.Pdd I _ ._ _. _.

AV . pP_eotbebonom6_<20yoateapi>m 34yawop X X X X XYAg. dl h_et3hab<sestsdaas2jecaq X X X X X XPokytad oh& _ippodmof" _ _ d _ _dis x x x xxlqSihdYOasI ~~~~~~~~~~~~~~~~~~Iru~~~~~~~ hcicmiaa~~~~~~~~~obdlM A orkat
S~m Koala = Z_tWm d_1.off FU9gI V Wit nacelY adspaisdsamp at Ulemm isami
P_~~~ib ebim eatp Xtas tmuu1eaew D X X X- ANb -ot et_x__ewoopwommU80 s x Y§WbDmUs . -oigtf wmanu nepmdmWm# ae rp*W isIufx mauaonb bcd I X
_ _ _ _ _ ___e_,_ X X X SXYT_iiem -is Iao
Qz*y 1 tEM t ud _lismslasd NMAy I _ wa S X X X X.~~~~~~~o d TtlZdioh
. AIhtfUsalia ftApada.of agw osinbab idu o X X X
.04a4ametbaftwadmi I. d_
CHRD SURVIVAL
oaN..uWealy KI
Mcsmby ~ dbalmim heft amd a wkauuga moipkdan urn..
Meabby IAWI I-. luc" toumn first yewoarf a0nd sCul be .lided is qosi I X I I
._~~~Cmo .au.oda -f .tctih A. i a. c_esI tee
Oalib(cusyI Ths. osm adtIk Ghhuam gsln ymci haiaeino
O ____ _____________I________ _____Pb_ q ltmmatut llzeldhcehndisld bmhaedaszuc X % X SM_ S_S__~~~~~~~~~~~~~~~~~~~~~~.
_-_ 1~~~~~~~~~~~~~~~0

~~~~~~~~~~Moi"wdAnw 1: - . 6- tve U
as - w
-Z_~~kw Ihabiwaaamauuis4wahabtmmhaaU.oqul K I_ X X X X
lb& ~~&s toztu Moeam la ve m- atdicmat mabdg)m ityjirau_~~~a sZAl* *oDknbyWeamso3M=hr >pneSax x x zcx
Z- bidumt. ID _eynitggd ak . ____________
UD_D_ mas .mcDGmduI&sm.rw ui. X X X X XAn It I_ x sx x x
111~~uhqsu ltwsm(i usqizasas Xadn Smuul, S X ShEwm
bah_ _el D_t W _g_XX x X X
lAmbhwaa..tdmb4musaqest III
i_ __ -md _iD bw6X X X X tww
Lo Ma w s qi|
& cos Ammo -mob
Amme, Pdsn.fm,dbad_ s.oMoabdbdsidnamnk X X X X K
SX~~M"atoetw
8~~~~~~~~~bsi gui_e ammuaisrXX X X
I-.a
AwmUiIIyt of Mmuavwaqtim K K X I1QamiyHel Awailbuliy eof athi dais
ibuulad at Cam ihhmE mubl asgaessig I X I
0
savim~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~H
a'

x x ~~~~~~~~~x x x
_________ ________ h.u1.-ssdammuudm Sgai.bodmadipom I I I I
N"=Pnp YhwAUtaahdgbg 91.fabIss aumim) mItha In isj Is x I
gndAs x__ S_S_~addd3daimbsdb i X X S X I
hamss pwu&mbdi X X X X XNaio11pa~ aah a ala.wo _wSS dahsda X X I X X X
__________ _____bu__ _sddaidssmah Xfd o XI _ _ % X x
_______ Msaigafmlsa X
~~~~"MA100 -As WoInq a.hpma u aahsdI_j p-_vs_4 ia.aaasarba X I X
x ~ h S h " b abaft x x
N _idiau ~ Kiw-hdp.hs. *mm bal Ass, M_ kagd aX bailvo ia d X X X XI
mowob _t bo di E " Xdd I I aXii h .NW X x
usi gaasihemANodbs*nd .,aIstamawboll., TM, hiss a ahws__________ .AUWho* . _bd ed..S , X X X X X
LTXI IBllPlUSON~I I
Wpj80pdsgdamt Aim&g - X X X.msmaal.v*abahsbm X
__ h_ahmobo
Atdbt AMbitdH B_ pWu1.wa h __mbl,aasandpobk. x X X I1 1.sJin. _ _ _ _ _ _ _ X X X X
.. ... _ - ~~~~~~~~~~~~~~~~~~~~~~i

.~~Pstoa . id _islsMwd u. d&dm. DI _n _~,l XX
I~ ~ ~~PshI UatI _ _ ud _ _*Gssd1satU jumwaa, dwlie X X X X
commHoBh
______ ______ ~COWMUMIW AND D3&CKGR~OMI HIC~Ic __
AsUmlUd by SO of bXwasme Xn s X fAly XO.iiA.Uac Wie aie Asusmb nod b1t.t m wia b am aeiMbmau adUn . rn.o
huJwungi rs- -ar afuu... .......... ... k d. omayS b nethe._ _e___l ~~ .. f CO Mfed u's aWtUN lusUMe etc.. ,_____________Uuheeamst hwwsow Asl thm tdas atmlMmsiofwanabopoih X X % X X
b _udm Sobd_ e
CmdMarnwdas .. ha at bea of beam&ul anpod MA Craw e avbuaawd aaldbbasx C_Z ~~emgb ?h_Ie' 4. isusam as.. X X X X X
_gi.tjhamtr a____d antdseutismmh Ac Was lbimte wlnM X IK X XOrna,.mdic Tanqast Sam Urs a1 aupau Is as m iay w A mtebdhA iAgat.Isaaheavihsn s.ady X X X X X
CandblAW W$Mndo..~~~~uhucsmI egblm ndt
_ _ _ _ .. .nlhi e Xaon X__ _ _ _ _ _ _ X_X_ _
cwodwmad K ds,ISEK Ihto*.Kdz wgqbahM.a&eahnlhd and tumidg Ilrstdmis
0_eri c aq sb y fdo _m1ub adx x X X X
Cu~~~~SbkTe atg odm &"*In _ o x X X X .~~~~~~muha o _dk oomA m*- cut Xdaoc x x "I mq IN
Ommisudofmdw=01mVitlap lewd fd= loo NU*ITAJIPIA,II..D11ag#0 high MA& diwiss end SaOdib hw II
VbemW N _ S_wpaf XrUluu Xaagupg.de. X X -__ _ _,__ - __
o l

W ~syaids Nuadm,psmuuuhap, ~qmAuhe. t ff 4VobbW*y 9"4u ad - I X X
DighPi_ Ahv. NhhCds ~_ pJ_K X X X
caadie__, htdz pea, aNU 1, U3PFSIYUS(Wl aidimimr f d _p-it-vS HCd aid asimievg,aver ed.Mw iMeW dDaSat
_ cub1 .. r o d cs
., | ---1*1 COD -- :iir l -c p - - -- r am E4w of i
mmbu dudw am am" in im rw~~~~Z1

NONESTEID COMMONTfY HEALTH AND NUTRITION PROJECT
Expeniftur Aamat by Yeanre A _ wY~~~~~~~~~~~~~~~~~~~~.n-
no mu 9188 Tai an88 low 9m Te
A. ak*Wmab1Wh_oft PSA 14,1 IIJ,i .M 4w3 4,3 4.9 73 s8 22 IA DA-sWl. 'SW 1.. 24 17 163. 1 . 19 IS Ss J Sa88aaa.sv.beAN I"" mu Lw 26la U SA 2U 3 la ad
-_ 182.2 i.ma 28 -$26. 063 J 04 LS81__ el~ - - 11,2120 11,838 12.4M 1e" so" M s 42 62 4 a s*~~~~~~~~~~~~~= Umb 4i 29 Si W" LO DA 7
Ciu -"~I 2. 1.5168 5638 1U ,73 t A 22,1* .9 0.6 W W1 7 U 0 2. ID.4_t_ ~ ~ WI
IfE w iiM 6 U
I__ Om fts 16 4114.1 7.1s1 403 0.S 6t * S tf11_~~~~~~~~~~~A Am Am am tam am Id ad R Li a tj w_tJ_kuwp %42 . SLI 1316 348. 1m 856A Lo 19 I ; 88 1 1 2IL1. _ .1L 38 1.2 282 441 358. Ut I S I. . . .
P. a_ US_ - 2,40 1,*. 64 4454 81. 25184 * 1.9 27 36 23 04 81_ S^4 431 44113 5,1 1,102 2lA A L4 2. 361 is 0. 3IM" SAM Ilam Ama ? ,sA a110 * 42 34 4. 42 t .ma f 2.03¶' S M18* %M18 V= 140 t 0W 1 LI IA Lo Lo is
- - a aS u tO U at ii tJs__~~~m i7u s.m 248 g,6 23Y 1893* &1 68 15 12 J2 10t1
_~~~~~~~~~S 1*0 2A 264s *o 2u WA" 04 u la S LO tSAA. mnf
11 * au. iiS 3.5 282 VO8 * 0. 0. 01 la 0.1 tC __
__.9 96* *8mlots * 1413 1.6%4 6M1 0.4 * 68 1Si L3 42~~m & * 1.28.9~~~~~~M low3. 2.1I.1 1,A2 1,882.2 9,83. 0. s1 IA OA la 6VaWl - 21.2 6* t,9 au is M. 28 IMS IL. 0.1 0.1 03- Lw #w Lw 1N tL uat * .* 1 * LI Qt 5! 2
00
mm Z.0 Nat £mm AmdA am Id ae ad &I u to

TfIID COOMUNITY UDALTI AND NtURITION PROZC
AcNm IR CwcDfl
_a -
-od smb -- fw =-- & mPAO s o
L e-
_~~~$ 49S - . 03 04 1 . . . 33 .IJ1 0t 4 * 04 d es * 1- * a * oomminva_ U At ml U2 AlaiZ * U
s_ . . .~ ~ ~ . . . 1* . * . * * . OJ1
C a__F ~~~A 0,2 di,,,, 4t
_w4 *A O. I u 3 4 . *4 4 * - 2f_. 4..4 * LI * *4 as - -04U IZ U U U U Ad~1 IL ILu
F. #I_O0 03 03 * 04 1 0 - * 03
t__~~~~~~~* 53 4 * 11 * 4 * 24 3.49tS *
_Aw A . . . 0.1 l a 04 t 04 13 -_t _ SJ QX EJ ;7 QU 49 02 * 9
0411 -OA a a O 62 e j 1
_ 9 S ~ ~ ~~ ~~~~ I& JA 2 21 im u Au ji ad du
0, a~* 1. Al LiA Ad A U -
IL _ -aA. _t _
SAN" * 4 L I4 0 o3 03 . 102
M L U 0t2* * OA* 0, 02. 0.?S. 4. 0.? .4 .4 0, . 0. .3 . . *
- _ ~ ~~ I? Ad Ad A U 12U AS -d '6 U
4 .2 I e * «a Yl 1? A 1 4.5C ea
*6 AU A 2AZ la Rt AL Ri U m
__l S S t la 9 u u aa& W ula, us 4ad In. am la am ui UA nu

- 115 - AN N1
THR COMMrUNT HEALTH AND NTTO OJECT
ESIIAI Sca OF Dsm
IBRD ywscal year An er Ig p
2 6.0 6.0 6 0
1 4.5 10.5 11 22 4.5 15.0 16 2
1 8.0 23.0 25 42 8.0 31.0 33 8
1 9.5 40.5 43 182 9.5 50.0 54 28
1 8.5 58A 63 432 8.5 67.0 72 60
ma1 7.5 74.5 so 652 7.5 82.0 88 79
1 6.0 88.0 94 902 53 93.5 100 92
Pect Closa g Date: March 31, 1999
Ia ts dad disbur-unt pri hr PHN pojcts ia Jadosa (Jn 11, 1991).

INDONESIATHIRD COMMUNITY HBALTH AND NUIMMOlONPROJECT
_siaf TA DIT!RRATIONALTECHICALASSIWANC ESCHEDULB
Ustda(TA UPImpe. 9 O StatbsecTOP SL D FaCcmtvAc/M Pme bartie - Aaenm Total SPA Pftc. Em B Ea PM Dip fr e
A. Prepwda*W
1. Hah B c MS& AE. & Caw PM $ 7n0 60 yes , o 1292 No 1W53 No 4D13Adv.(Ph m) HEAkdv.2.HeahtEdw.Ma. Adv.A Cwd, PM S 450 36 Ye No 2WZ No 43 NoAdb.(C Ot HEAdet.3I me& Dmp Deug Mei VIM S225 I6 Yss y No 12/3( No 41193 No 41U9Spc Pai*agm4. Halth 1Iaal Damlop&Taaii
Bpeia*t kiin HeatA-Maaiaa Plaing Du= $16 is Yes No VUS3 No 4V3 NobMabbldw
S. HM AlM fa *M3. FamIy S $10 12 No 120M No 41113 No q13 No f13Sa*ea blaDeaop. MCH Heatrt l. raM
6 iN_an Imoleot AsbalPa. O0I1 S 75 6 No M93 No 5113 No 461 No 3Mvlmya NLA. Aada
7.UACHSenAduie,y ce AsnailSalk Dq $ 151 1 12 No YU93 No SW" No 7AM No 153
D_wl8&MISSpdiSts A_isDevhop. pan S 300 24 No W13 NO N No 4N1VS3 No 4113
aWlS Daa
I.HBE apiVTU CadThV mIm S 156 12 Yes - No mm No TA1 No ff252. Nurim Pli Fe" Ad*ce IP8 S 15 12 No 12/02 No 46/3 No 71W) No 51W
Mamam Spec. Advbe. DWer S 75 6 No Ylfl3 No 4110 No 51153 No 415Weati DlurltLAw
C PoliyMudwA_iesLLoolta Bht2aW DO Cm S $87 30 Yes Y n o NO 4So ae LMmbn Helth (5H)
D. MahmalM Ad" Advceoevr* DO CanaManageom Health $750 60 No 1Z3W No 12/ No 4V No 411/ISB. PAadSp%Wab*d
LCifdaii S al(28M) PtowAdeOn e DO Co. S 750 60 No MM13 No 7/153 No NM13 No N13 M2Mwm_ MHeab(12Sb) for pc.je Hlte
4lidafts8) ,ala SUaWt*aSHealab Jftmma(t2SM) Pas
C*as EBtilmu are lo $4

- 1171- &k~U1
COIbWNTrY HEALTf AND NUTfRION PROJET
SUMAXYOF 0TaCbAJ. ASSMAN
§ANX OM
Waa., . _ _ = = _ _ -
wodu m
F-rn
R.e.had $NO".-
£qulpuataa mwea _ su_ ___ __.
"W _&$U* + ___d
-as". met" Is"_ -.m In _ g_ __d _I.__.
.qJen 0* _oIm t a__pl_t __ , Ia.. ,. w" T__====I
Ornien w __r =_==e _==
£a*meat1 1o i4h eung_ _ i__t ___ V_de I -
bAU. 1 1et t @0*6 ,, , E
Reae _n 111dIes Pe_b e Ip180- ,,, nIa WolbI t_ e ___ t ___
am~~~~ 1=_===_1 New .O-We an 1eeiU _ ___I_ __1
C_ o *

- 118 -
DWDONUIUD COMMUTff EMALTff AND NUTRIMION PlOJECT
--VATOF OZISOMPS *W
--- - ~~-SL-W -aamma am F0 am
a s X s 4 4 t32 ~ ~ ~ ~ ~ ~ ~ 111 1 2
sa.t.om I St- I 2 2 t4z s 4 * 5
S2 4 1 2 2 2n~~ a i a a a ;
9bf 1_ 1 2 2 2 to 1 2
81 1 152 1d 1 2 2 1 1 14 1 de
81 1 2 2 2 S 1282 SU U 1 I
2 S 4 4 1 14 4 6 4 24
_ _am 4 10 tO 26 4 4 4 1dff _~~~ ~ ~ ~~~~~~~~~~ S 1 0 24
m 1~~~~~~~~~~~~~~~~~3 0 so so
S1t 8 50 47 9052 4 4 I 4 8 22 14 41
65.gam s s 4 4 4 82
Di 18 10 10 10 to soDt tO is tO le to So
St 4 4 4 S S 2S52 1 2 , 9 . 4 . s s 24
8_ins S S 2 2 le t 2 2 2 8DS ~~~ ~~~~~~ ~~ ~~~~~22 is 14 5 S a0
S1 is is i5s Stn S 2 s 8 S 4 S 12
wl 10 * tso iso tao 0sS 10 12 14 44
1 2 2 S S 5 6 9 4 5 2t0 9t 82 U s0 4 13 6 In 254 45 404 216 1452
_1 _L ml a _ _ _ L _ A iL IsI .j Alla I

* -119- AEX 13Page 2 of 3
.1 I I 1 I IgeI eI m I I I I I l,
S | | ~~~~~~~~~~~~~~U |2 a a tO 64
11 2j2j I 4 I I 2_S~~~~~~~~ A
St to .| X | _ ___s_LL_ LLU~LIIf-~~~~~~~~~~~~~~~~~~~~~~~~~~i
I s ~ ~ ~ -*-
Abt. 1. - - - - - -_ u - -} - v - ~- -0t
_ .. A .ILJI 1 1 L..t~ZA..d I u..l_IJI 1
____lLI~ _J .L. Li zLI 4z1 |S_ ~ ~ ~ I I UI -l f-I -lt 1 11 12
I I I - ? I 'I I 2I I 1 I
Dll-~ I I I 2121t 1sl11 1211 1'
_* ~~ | - -l - - - p -, I - l I - tO
I 2 2 2 6 1~~~~~ 2 2
usma I I I I IU I_ U S 4~5||oia __ | | X 0 | | U14 | | | Ms 4 s 7
___
81 1to to 0 21i- I-; I ,LI I v v l s I s I @ I * * 2 2 1
~~~~~~~~ 2 2 2 lo I 2121 |t
__ - ii.. . ....n,. I X| X| § §1
8t 1 1 1 1 1 1 1 1 1 1 1 } t | X | X | ~~~..JD Z.

an at Ltw m do - o on a "9 GTu MR * OW OD F o-D WF T us W -W WrU
uu-v- -- T-r -r- -1--' 0- -T "- -Ir-- Is ~-P-
a s~~ 9 P 9_.
--- t ---------
CTZMW ~~~~~- OZT-

ANNEX 14
-121 -Pagel1of 2
I~~ I
_~~~i ., 1
I H t l a R' Xi a 'I + t
.1 .i a a 1 6 i # g g
^ ,,l0,...II,i_ ... ' IR'-'g_ S i

ANNEX 14
-122 -Page 2of 2
|! i I
11111 Ii1 11 1,1 |1
ht V X 11~t 1 l,.tI,,,,,,,,.,,,,..

- 123 - ANNEX 1SPage 1 of 3
W)ONESIATHID COMMUNITY HEALTH AND NUTRITMON PROJECT
SCzXCtED DOCuMENtS IN ftOjC FaLx
I. Domnts and Studies for Projed Prepraton
1. Berg, Ala. The Challenges of Upgrading Quality and Increasing Relevnc: SomeThoughts on Niarieion Work In Indonesia. March, 1992
2. Bostn University and Deloite Haskins & Sells with Dr. Hms Kartibaadi and Co.Aution trategy Sdy to Develop an Integrated Health IMbrmaton System. VolsI and IH. The Health Policy Institute: Boston University, September, 1989.
3. Grffiths, Marcia and Terry Scott. Healh and Nrion Education in Indonesia:Capacty BuUding and DecentraliAton. March, 1992
4. Heywood, Peter. Assessment of he Role of Instes of IIgher E4ucaton in Healthand Nuition Capcy Building. Repoxt on a Consultancy to the World Bank, Apri1992.
S. Khanna, Dr. S. Mona (ed) Public Hah and Soio Economi Ohanges at the Dawnof the 21st Ceny; Impleatons for Pubic Health Academic Educaton, Facuty ofPublic Health University of Indonesia and Ministry of Heath, Republic of IndonesiaDraft Report, May, 1992.
6. Koblinsky, Madorie A., A. rmker, P. Daly, C. Rooney et. al maUng MothrhodS*. Wshington: World Bank (Draft) June, 1992.
7. Mevin, Cathy. The h,Fmado CoMonent of the IW Cmmuniy Health andMtrton Project. June, 1992.
8. Ministry of Health. An Eecdv Swnmary ofAssessme and Rewmende NatonalSrafoegres fr MotWhhd. Vol IV, 17 December 1991.
9. MInist of Health, Bureau of Planming. Isdonesia Community Heal aid Nutrionm: Project Proposal Provincal Copone. (Naative) June, 1992.
10. World Bank. Aide Memoire: Third Community Health and Nutrition Project: Pre-Appraisal Mission June 20July 15, 1991.
11. World Bank Aide Menolre: Second Pre-Appra-a Follow-up Miion: January 27-Febra 11, 1992.
12. . Irian Jaya: Budget Proposal (Revised) June 25, 1992.
13. __. Maluku: Budget Proposa (Revised) June 25, 1992.

- 124 - A 15Page 2 of 3
14. . Nusa Teogua Timur: Budget Proposal (Revised) June 25, 1992.
iS. . Central Java: Budget Proposal (Revised) June 25, 1992.
16. . West Java: Budget Prwposal (Reised) June 25, 1992.
I. Other Documents
1. Carolina Population Cenlter, pdeogrqc Survelance.: A SymposIum. 1971.Chapel Hill: UNC at Chapel Hill. (Pages Cover, Contet, 1-28, 43-65, and 94-98)
2. Freymann, M. W, Impac Indkator Systems In Famiy Planing Programs: A NewLook, Discuwion Outline for RAPID meeting, June 19, 1992, Research TaglePark, NC. 7 pp.
3. Stinivasan, KI, P.C. Saxena and A. Pandey, Bbih Order and ih Inel Saikcs.Use in Assessing Lewls and Changes in Ferility, by Draft 6/11192. (Not forquotation) 29 pp.
M. material for Project Pie
1. Brooks, Marl. Bacrund Prfor Projet Polt Asseane. hsues concerningDee lization and Ieg Planming and Budgeting for THP". PaV prared forMOH, Bureau of Plannig. Draft. August 30, 1991.
2. Bossert, Thomas. Chipps Final Evaluation. Phase I: Decentrlon Lessons.Prepared for Biro Perc_aa, Depkes and USAD/Jakrta Univ. Rsearch Corp.,October, 1988.
3. Bureau of Plaming, Secretaiat General, MOH. Cwep of Basc Healh ServesPrAea jbr Acivites Condcted at Co wy Health Centers (ukea) and
Wstabismentof Ditct Sub Projects. Deember, 1992.
4. Formlir Tinak Lanjut, *IBU HamiP (SKRT 1992). (i Bahasa Indomesia). (12pages).
S. Malison, M.D., et al. E*Iatng Use of ORS, Vaccne Coverage, and CildhoodMortality: A New approadfrom Fperkence In Uganda, May, 1986. Draft. Atanta:Centers for Diee Contrl. 8 pages.
6. Survei Kesdisn Rumah Tangga, 1992, DAFTAR I: Ketangn Seb Kmai *Bahasa Indnesia). 12 pages.
7. Survei Keseata Rumah Tangga, 1992, DAFrAR I I: Keshatan lbuHamil (in Bahasa Indonesia). 9 pages.

- 125 - ANX1Page 3 of 3
8. lhe Evluaton Project: Service Ddivery Working Group, Miutes of Meetig: June34, 1992.
9. The 1992 NbaonalHowehld H h S&M (andonesia), 13 pages (-17 in English; 9-13 in Bahasa Indonsia).
10. . Sub-Commitee on Quality Assurace Service Delivery WorkingGroup Miu of Meeing, June 17, 1992.

INDONESIATHIRD COMMUNITY HEALTH AND NUTRrITON PROJECT
Ministry of Health Organizational Structure
PM"w Pemonm Fkalm ScrtaiatGenra
hspetote hsaphectoa ra6te Buroau of iBureau of Burfeau ot ufi Burau ol Bureau odd Perl od Finance di Laistica Pllalns | Porsormel Fiac . . Istks cr OrgaUzaior Burea off
wome 3erene | r Diretorae Genra Direotorte Gnenraid o| irectorate Geal off olCommt Illy Healez j | of M cal Care Comm. Disase Corold° Food & Drug Coro
d~~~~~~~~~~~~~~~~~~~~~~~ertta SecrebtIat
Dietrt i Drcoaeo ietrt fDirectorate o Directorate of Directorate df o etoae f"~~a,eoFamily Healh Heoah C|te General Sc V r oe
Directorate Dlrectoratedo Diractorated | | Directobate o rectorate o Dir Iectorateo Direca te O Dctoate ICommunity Community ~ ~ ~ ~ wwmm &r.& ofm~
Gs o, s,nation DcrStation. tfe|tthl Equip. cont_ _
I M@d I I mter I ~~~~~~~~~~I Na¢"0 ttcs I
| CenXrEduc |1 E @du arflo of pb¢h
HoOh Doa HekhI
Center of r-,L ' :]~~~~~~~~~~~~~~~~~~~PamU
| C*er rT-| cer9rly | . | -,---- h C-nterl r . * F . l -- .SMAS

CHART II
INDONESIATHIRD COMMUNITY HEALTH AND NUTRITION PROJECT
Provincial Health Organizational Structure
MINISTER OF MINISTER OFHEALTH HOME AFFAIRS
Provine GOVERNOR
PROVINOFF ICE INCIAL GOVERNMENTMINISTRY OF HEALrH -HEALTH OFFICE
BUP ATI(MAY'OR)
DiSct DISTRICT OFFICE GOVERNMENT MOH HEALTH OFFICEI
Subdistdct HISLR ICT
SUB HEALTH HEAD OFCENTER VILAGE
POSYANDU |POSYANDU POSYANDU

CHART III
INDONESIATHIRD COMMUNITY HEALTH AND NUTRMON PROJECT
PROJECT MANAGEMENT STRUCTURE
CENTRAL ADVISO PROJECTLEVEL BOAR DIRECTOR
TASKFORCE
STEERING PROJECTCOMMITTEE I MANGER
I PROJECT MANAGEMENAI SECRETARIAT ADVISER
. 2 ~~~~~~~!
PROVINCIAL _-I!ILEVEL rSTEERJN I RJC
=~~~~~~~~ !.~~~ ~~~~ IILLEN G3 PROJECT
COMMni TT.E DIRECTO I
DISTFUCTLEVELv
W.~~~~~~~~~~~~~~~~~

18/ta+ND , 1t INDONESIA ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~IBRD 247D
°\- "d PI/PNS'-.W... A'.
THIRD COMMUNITY HEALTH
%g15 7/ | A ~~~~~~soundJ CHINA SEA - X) v AND NUTRITION7 PROJECT
< p <|~~~~~~~~~~~~~~~~~~~BUE AT> 8NUMr
OF YM IN FPOJECT 8ATNY
'-,< ~~~ALYSA I*UO
oN °/SFif}'
~~~~~_X; ,, __ NI=ALW tj
2 YER
1':,'"w$~~~~~~~~~~~~~~~~~~~MLY Se tkE
23+ NUiAIENGC/aA8ARAr INDIAN OCEAN _ 24~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~DrRCTWAPAENBONDM
^ 7 77X1UR~~~~~~Q~ A N3'47 0 8XZ9
17. 7W,At7R v~~~~~~~~~~~~~~~~t,,,,5tzf l thw- G i
,m 4\g D v~~~~~~~~~~~~~~~~~INERATON SUNAFE
lowt l8P 17,2$ . IlIP 1;14° 1;9 AUt~~~~~~~~~~~~-


![Untitled-6 [] yamato.pdf · tis 1390-2539 (1996) tis 1390-2539 (1996) tis 1227-2539 (1996) tis 1227-2539 (1996) tis 1227-2539 (1996) tis 1227-2539 (1996)](https://img.dokumen.tips/doc/110x75/5f7cd919128bf72d7a0d9590/untitled-6-yamatopdf-tis-1390-2539-1996-tis-1390-2539-1996-tis-1227-2539.jpg)


























![Untitled-6 [] · tis 1227-2539 (1996) tis 1390-2539 (1996) tis 1227-2539 (1996) tis 1390-2539 (1996) tis 1227-2539 (1996)](https://img.dokumen.tips/doc/110x75/5e1a6a0f6b8d9f48bd19bcad/untitled-6-tis-1227-2539-1996-tis-1390-2539-1996-tis-1227-2539-1996-tis.jpg)