Embed Size (px)
Citation preview

Working Paper Series 2017/77/MKT
A Working Paper is the author’s intellectual property. It is intended as a means to promote research to interested readers. Its content should not be copied or hosted on any server without written permission from [email protected]
Find more INSEAD papers at https://www.insead.edu/faculty-research/research
Which Healthy Eating Nudges Work Best? A Meta-Analysis of Field Experiments
Romain Cadario
IESEG, [email protected]
Pierre Chandon INSEAD, [email protected]
December 18, 2017
We examine the effectiveness in field settings of seven healthy eating nudges, classified according to whether they influence 1) cognition, via “descriptive nutritional labeling,” “evaluative nutritional labeling,” or “salience enhancements”; 2) affect, via “hedonic or sensory cues” or “healthy eating prods”; or 3) behavior, via “convenience enhancements” or “plate and portion size changes.” Compared with existing univariate meta-analyses, our multivariate three-level meta-analysis of 277 effect sizes controlling for eating behavior, population, and study characteristics yields smaller effect sizes overall. These effect sizes increase as the focus of the intervention shifts from cognition (d=.08, equivalent to -45 kcal/day) to affect (d=.22, -121 kcal) to behavior (d=.35, -186 kcal). Interventions are more effective at reducing unhealthy eating than at increasing healthy eating or reducing total eating. Effect sizes are larger in the US than in other countries, in restaurants or cafeterias than in grocery stores, and in studies including a control group. Effect sizes are similar for food selection vs. consumption, for children vs. adults, and are independent of study duration. Compared to the typical study, one testing the best nudge scenario should expect a fourfold increase in effectiveness, with half due to switching from cognitive to behavioral nudges. Keywords: Meta-Analysis; Health; Food; Field Experiment; Nudge; Choice Architecture
Electronic copy available at: http://ssrn.com/abstract=3090829
Healthy eating nudges: A « living » meta-analysis
We have created an online tool to allow researchers to correct and update
our data, turning it into a “living” meta-analysis that can be continuously
updated. Do not hesitate to share this URL to your colleagues! We will
periodically update the meta-analysis to include the most recent results. The
updated results will be posted online, available to all.
Helpful comments on various aspects of this research were provided by Janet Schwartz, Alexander Chernev, Maria Langlois, Yann Cornil, Gareth Hollands, and those who participated when the authors presented this research at the TCR conference, the BSPA conference, the SJDM conference, the University of Toronto and the University of British Columbia.

1
1. Introduction
Unhealthy eating is a key risk factor in non-communicable diseases such as cardiovascular
disorders and diabetes, which account for 63% of all deaths worldwide and will cost an estimated
US$30 trillion in the next 20 years (Bloom et al. 2012). Traditional approaches to promote healthier
eating include economic incentives, such as soda taxes (for a recent review, see Afshin et al. 2017)
and nutrition education (for a recent review, see Murimi et al. 2017).
More recently, interest has grown in nudge interventions as a spur to healthier eating.
Disappointingly, existing meta-analyses have only found average effect sizes ranging from weak or
null (e. g., Cecchini and Warin 2016; Littlewood et al. 2016; Long et al. 2015) to moderate (e.g.,
Arno and Thomas 2016; Hollands et al. 2015). However, these were based on a small number of
studies (e.g., 19 for Long et al. 2015), specific foods (e.g., vegetables for Broers et al. 2017), specific
settings (e.g., catering outlets for Nikolaou et al. 2014), or included online or laboratory studies
(e.g., Sinclair et al. 2014) where effect sizes tend to be different than in field studies (Holden et al.
2016; Long et al. 2015). The field still lacks a comprehensive meta-analysis that attests to the
effectiveness of a broader range of healthy eating nudges in field settings. More important, it lacks
a conceptual framework within which to categorize interventions and predict their effectiveness for
different consumption behaviors (e.g., healthy eating, unhealthy eating, or total eating) and different
consumption settings (e.g., restaurants, cafeterias, or grocery stores), as well as for different
populations and study characteristics.
Our study examines the effectiveness of interventions aimed at promoting healthy eating
without resorting to either economic incentives or nutrition or health education. These simple,
inexpensive, freedom-preserving modifications to the choice environment, defined as “nudges” by
Thaler and Sunstein (2009, p.6), refer to “any aspect of the choice architecture that alters people’s
behavior in a predictable way (1) without forbidding any options or (2) significantly changing their

2
economic incentives. Putting fruit at eye level counts as a nudge; banning junk food does not.”
According to this definition, which has been adopted by other influential review papers (e.g.,
Hollands et al. 2013; Skov et al. 2013), healthy eating nudges encompass a wide variety of
interventions, including nutrition labeling in supermarkets, healthy eating cues in cafeterias, and
plate and portion size changes in restaurants, but excluding financial incentives like price changes
or sales promotions.
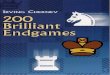
Figure 1: Conceptual framework
To achieve this goal, we identify seven types of healthy eating nudges classified in three
categories: cognitive, affective, and behavioral. As shown in Figure 1, our framework also accounts
for the type of eating behavior (food selection or actual consumption) and distinguishes between
healthy eating, unhealthy eating, and total energy intake. It also considers population characteristics
such as age (children vs. adults), consumption setting (onsite cafeterias vs. offsite restaurants, cafes
vs. grocery stores), and location of the study (US vs. other countries), as well as characteristics such
as the duration of the study and its design. We test this framework with a three-level meta-analysis
of 277 effect sizes from 81 articles and 87 field studies published until the end of 2016.
Intervention
effectiveness (effect size)
Population characteristics Grocery stores vs. offsite eateries vs.
onsite cafeterias Children vs. adults
Americans vs. others
Study characteristics Study duration
Double difference vs. single
treatment-control vs. single pre-post
Selection vs.
consumption
Intervention type
Cognitive nudges (knowing) Descriptive nutrition labeling Evaluative nutrition labeling
Salience enhancements
Affective nudges (feeling) Hedonic or sensory cues
Healthy eating prods
Behavioral nudges (doing) Convenience enhancements
Plate and portion size changes
Total eating vs.
healthy eating vs. mixed eating
vs. unhealthy
eating
Behavior
characteristics

3
Table 1: Comparing Meta-Analyses of Healthy Eating Nudges
Scale and scope Method Categorization of predictors
Reference
Effect
sizes
(K)
Articles
(N) Setting
Hypo-
theses
Accounting
for repeated
observations Model
Intervention
type
Consump-
tion vs.
selection
Healthy
vs. un-
healthy
Other control
variables
This meta-
analysis 277 81
Field
only Yes
Yes
(3 levels)
Multivariate
(16 df)
3 pure and 2
mixed types,
(7 subtypes) Yes Yes
5 study &
population
characteristics
Arno and
Thomas (2016) 42 36
Field &
lab No No
Intercept
only 1 No No None
Broers et al.
(2017) 14 12
Field &
lab No No
Intercept
only 1 No No None
Cecchini and
Warin (2016) 31 9
Field &
lab No No Univariate
1 (only
labeling) No Yes None
Holden et al.
(2016) 56 20
Field &
lab No No Univariate
1 (only size
studies) Yes No
Manipulation
type, field vs. lab
Hollands et al.
(2015) 135 69
Field &
lab No No Univariate
1 (only size
studies) Yes Yes
Manipulation
type, age, design
Littlewood et
al. (2016) 20 14
Field &
lab No No Univariate
1 (only
labeling) Yes No None
Long et al.
(2015) 23 19
Field &
lab No No Univariate
1 (only
labeling) No No Design
Nikolaou et al.
(2014) 10 6
Field
only No No Univariate
1 (only
labeling) No No None
Robinson et al.
(2014) 15 7
Field &
lab No No
Intercept
only
1 (only size
studies) No No None
Sinclair et al.
(2014) 42 17
Field &
lab No No Univariate
2 (desc. vs.
eval. label.) Yes No None
Zlatevska et al.
(2014) 104 30
Field &
lab No No Univariate
1 (only size
studies) No Yes
Field vs. lab, age,
sex, BMI

4
As shown in Table 1, our work contributes to the many useful existing meta-analyses in
terms of (1) scale and scope, (2) method, and (3) categorization of predictors. In terms of scale and
scope, we examine more than twice as many effect sizes as the largest existing meta-analysis. This
is achieved despite focusing only on field experiments involving actual food choices (vs.
perception, evaluation, or choice intentions) and conducted in field settings (onsite cafeterias,
offsite eateries, or grocery stores) rather than in a laboratory or online. This allows us to offer
guidance to restaurants, supermarket chains, and foodservice companies who want to help their
customers eat more healthily but do not know which intervention will work best in their particular
context; and to provide guidance for policy makers who need to forecast the effects that these
nudges would have in real-world settings.
Methodologically, our meta-analysis differs from earlier ones on three levels. First, we
formulate hypotheses about which healthy eating nudges work best and about the effects of eating
behavior and of population and study factors. Second, to reduce the risk of confounds from
univariate analyses, we employ a multivariate model incorporating all predictors simultaneously.
Third, we include a three-level analysis to take into account the hierarchical structure of our data.
Finally, Table 1 shows that we use a more granular predictor structure compared to existing
meta-analyses, which either estimated the effect size of a single type of healthy eating nudge or
compared the effect of one single difference (say, descriptive vs. evaluative labeling) and which
rarely incorporated behavior, population, and study characteristics.
2. Conceptual framework
2.1. Classifying interventions
The many existing classifications of healthy eating interventions tend to be ad hoc, focusing
on mnemonic acronyms rather than theoretical grounding. They have also shown a tendency
towards category inflation over the years. For example, Chance et al. (2014) suggested four P’s

5
(possibilities, process, persuasion, and person) where Kraak et al. (2017) recommended eight P’s
(place, profile, portion, pricing, promotion, healthy default picks, prompting or priming, and
proximity). Hollands et al. (2013) initially distinguished three nudge categories, but even the
simplified version of their more recent TIPPME typology contains 18 categories (Hollands et al.
2017). Unlike the other classifications, Wansink’s (2015) CAN model is based on three
hypothesized mechanisms of action (convenience, attractiveness, or norms). Unfortunately, many
interventions operate via multiple mechanisms, making the CAN model less suitable for a
classification than for a conceptual framework. Moreover, none of the existing classifications makes
predictions about which type of intervention is most effective.
We draw on the classic tripartite classification of mental activities into cognition, affect, and
behavior (or conation), which dates back to eighteenth-century German philosophy (Hilgard 1980).
The trilogy of mind has long been adopted in psychology and marketing, both to understand
consumer behavior and to predict the effectiveness of marketing actions (Barry and Howard 1990;
Breckler 1984; Hanssens et al. 2014; Oliver 1999; Srinivasan et al. 2010). We distinguish between
1) cognitive interventions that seek to influence what consumers know; 2) affective interventions
that seek to influence how consumers feel, without necessarily changing what they know; and 3)
behavioral interventions that seek to influence what consumers do, without necessarily changing
what they know or how they feel.
Within each type of intervention, we further distinguish two or three subtypes that share
similar characteristics and that have been tested by enough studies to enable a meaningful meta-
analysis at their level. This subcategorization is based on existing classifications, such as the
distinction between descriptive and evaluative nutritional labeling (Fernandes et al. 2016; Sinclair
et al. 2014). Table 2 provides definitions and illustrations of the seven types of intervention and

6
lists the studies that tested them. In the analysis section, we explain how we account for the fact
that some studies implemented multiple types of interventions at once.
Cognitive interventions. As described in Table 2, we first grouped the three types of
cognitive interventions that aim to nudge consumers by informing them about the healthiness of
their food options. The first type, “descriptive nutritional labeling,” provides calorie count or
information about other nutrients, be it on menus or menu boards in restaurants, or on labels on the
food packaging or near the foods in self-service cafeteria and grocery stores. The second type,
“evaluative nutritional labeling,” typically (but not always) provides nutrition information but also
helps consumers interpret it through color coding (e.g., red, yellow, green as nutritive value
increases) or by adding special symbols or marks (e.g., heart-healthy logos or smileys on menus).
Although the third type, “salience enhancement,” does not directly provide health or nutrition
information, it is a cognitive intervention because it informs consumers about the availability of
healthy options by increasing their visibility on grocery or cafeteria shelves (e.g., by placing healthy
options at eye level and unhealthy options on the bottom shelves) or on restaurant menus (e.g., by
placing healthy options on the first page and burying unhealthy ones in the middle).
Affective interventions. The first type of affective interventions, dubbed “hedonic or
sensory cues,” seeks to increase the hedonic or sensory appeal of healthy options by using vivid
sensory descriptions (e.g., “amazing broccoli”) or attractive displays, photos, or containers (e.g.,
“pyramids of fruits”). To date, no field experiment has sought to reduce hedonic or sensory
expectations for unhealthy options by using disparaging descriptions or unattractive photos. These
interventions are affective because, rather than focusing on informing consumers about the
nutritional quality of food options or their likely health impact, they focus on the more affective
hedonic or sensory consequences of eating the food.

7
Table 2: Categorization of nudge interventions
Intervention Target: Healthy eating (k = 170) Target: Unhealthy eating (k = 71)
Knowing: Cognitive interventions
Descriptive
nutritional
labeling (k = 31)
Calorie or nutrition labeling (Auchincloss et al. 2013; Bollinger et al. 2011; Brissette et al. 2013; Chu
et al. 2009; Downs et al. 2013; Dubbert et al. 1984; Dumanovsky et al. 2011; Elbel et al. 2011; Elbel et
al. 2009; Elbel et al. 2013; Ellison et al. 2013; Finkelstein et al. 2011; Krieger et al. 2013; Pulos and
Leng 2010; Roberto et al. 2010; Tandon et al. 2011; Vanderlee and Hammond 2014; Webb et al. 2011)
Evaluative
nutritional
labeling
(k = 34)
Green stickers, smileys, “heart healthy” logos
(Cawley et al. 2015; Ensaff et al. 2015; Gaigi et al.
2015; Hoefkens et al. 2011; Kiesel and Villas-Boas
2013; Levin 1996; Levy et al. 2012; Ogawa et al.
2011; Olstad et al. 2015; Reicks et al. 2012;
Thorndike et al. 2014; Thorndike et al. 2012)
Red stickers next to unhealthier options
(Crockett et al. 2014; Hoefkens et al. 2011;
Levy et al. 2012; Olstad et al. 2015; Shah et al.
2014; Thorndike et al. 2014; Thorndike et al.
2012)
Salience
enhancements
(k = 25)
Healthier options more visible: e.g., eye-level shelf
position, transparent containers, placed near cash
register (Bartholomew and Jowers 2006; Cohen et
al. 2015; Ensaff et al. 2015; Foster et al. 2014;
Gamburzew et al. 2016; Geaney et al. 2016; Hanks
et al. 2013; Kroese et al. 2016; Levy et al. 2012;
Meyers and Stunkard 1980; Perry et al. 2004;
Policastro et al. 2017)
Unhealthier options less visible (not eye-level
shelf positions, middle of the menu), previous
unhealthier consumption more visible: e.g.,
leftover chicken wings un-bussed
(Bartholomew and Jowers 2006; Baskin et al.
2016; Dayan and Bar-Hillel 2011; Meyers and
Stunkard 1980; Wansink and Payne 2007)
Feeling: Affective interventions
Hedonic or
sensory cues
(k = 12)
Vivid hedonic descriptions (e.g., “amazing
broccoli”) or attractive displays, photos, or
containers (Cohen et al. 2015; Ensaff et al. 2015;
Hanks et al. 2013; Morizet et al. 2012; Olstad et al.
2014; Perry et al. 2004; Wansink et al. 2012; Wilson
et al. 2016b)
Healthy eating
prods
(k = 35)
Written or oral injunction to choose healthier
options: e.g., “Make a fresh choice” or “Revitalize
yourself” (Buscher et al. 2001; Cohen et al. 2015;
Ensaff et al. 2015; Hanks et al. 2013; Hubbard et al.
2015; Perry et al. 2004; Schwartz 2007; van Kleef et
al. 2015)
Written or oral injunctions to change unhealthy
choices: e.g., “Your meal doesn’t look
balanced” or “Would you like to take a half
portion?” (Freedman 2011; Miller et al. 2016;
Mollen et al. 2013; Schwartz et al. 2012)
Doing: Behavioral interventions
Convenience
enhancements
(k = 56)
Healthier options are easier to select or consume:
e.g., default choice, convenient utensils, “grab and
go” line, placed earlier in cafeteria line, pre-sliced,
pre-portioned, or pre-served (Adams et al. 2005;
Buscher et al. 2001; Cohen et al. 2015; de Wijk et al.
2016; Elsbernd et al. 2016; Goto et al. 2013; Hanks
et al. 2012; Lachat et al. 2009; Olstad et al. 2014;
Redden et al. 2015; Rozin et al. 2011; Steenhuis et
al. 2004; Tal and Wansink 2015; Wansink et al.
2016; Wansink and Hanks 2013; Wansink et al.
2013; Wilson et al. 2016b)
Unhealthier options are less convenient to
select or consume: e.g., placed later in cafeteria
line when tray is fuller, less accessible or
harder to reach, less convenient serving utensils
(Hanks et al. 2012; Mishra et al. 2012; Rozin et
al. 2011; Wansink and Hanks 2013)
Plate and
portion size
change (k = 17)
Larger plates for healthier options (DiSantis et al.
2013)
Smaller plates or portions for unhealthy options
(Diliberti et al. 2004; DiSantis et al. 2013;
Freedman and Brochado 2010; van Ittersum and Wansink 2013; Wansink and Kim 2005;
Wansink and van Ittersum 2013; Wansink et al.
2006; Wansink et al. 2014)

8
The second type of affective interventions, dubbed “healthy eating prods,” provides direct
injunctions, orally or in writing, to eat better. This can be done either by prodding people to choose
a healthy option (e.g., “Make a fresh choice” or “Revitalize yourself by snacking on a fresh basket
of crisp red peppers, juicy tomatoes, and crunchy carrots. Easy to eat on the run!”) or to change
their unhealthy choices (e.g., “Your meal doesn’t look like a balanced meal” or “Would you like to
take half a portion of your side dish?”). These interventions are affective because, rather than
changing beliefs, they seek to directly change people’s eating goals from taste to health through
injunctions. By asking lunch ladies or cashiers to comment on people’s food choices, healthy eating
prods also rely on the power of interpersonal communication and norms.
Behavioral interventions. The third group consists of two types of interventions that aim to
impact people’s eating behaviors without necessarily influencing what they know or how they feel,
and therefore often without people being aware of their presence. “Convenience enhancements”
make it easier for people to select healthy options (e.g., by making them the default option or placing
them in faster “grab & go” cafeteria lines) or to consume them (e.g., by pre-slicing fruits or pre-
serving vegetables), or make it more cumbersome to select or consume unhealthy options (e.g., by
placing them later in the cafeteria line when trays are already full or by providing less convenient
serving utensils). The second type, which we call “plate and portion size changes,” modifies the
size of the plate, bowl, or glass, or the size of pre-plated portions, either increasing the healthy
options they contain or, most commonly, reducing unhealthy options.
Hypotheses. The tripartite categorization of healthy eating nudges allows us to make
predictions about their effectiveness. First, in the domain of food, cognitive factors tend to be less
predictive of choice than affective factors, which have been shown to strongly influence even
restrained eaters who eat according to cognitive rules (Macht 2008). For example, when asked about
what drives their food choices, American and European consumers place affective factors like taste

9
in first position, well ahead of cognitive factors like nutrition or weight control (Glanz et al. 1998;
Januszewska et al. 2011). Even interventions that successfully change beliefs about the health
consequences of behaviors often fail to lead to meaningful behavioral changes (Carpenter 2010;
Sniehotta et al. 2014).
Second, because eating is largely habitual and prone to self-regulation failures, affective
factors tend to be less predictive of food choices than behavioral factors (Herman and Polivy 2008;
Ouellette and Wood 1998). For example, directly changing the eating environment (e.g., avoiding
exposure to tempting food) is a more successful self-control strategy than cognitive strategies (e.g.,
not looking at the food, thinking about its nutrition content) or affective strategies such as relying
on willpower (Duckworth et al. 2016; Wansink and Chandon 2014). Similar conclusions were
reached in a large study of the drivers of the sales elasticity for 74 mostly food brands (Srinivasan
et al. 2010). This study found that changes in distribution (a behavioral intervention) have a larger
impact than changes in advertising (a cognitive or affective intervention) and that affective changes
in liking are more predictive of brand choice than cognitive changes in awareness. We therefore
expect that the effectiveness of healthy eating interventions increases as their focus switches from
cognition to affect and to behavior.
2.2. The role of eating behavior type
As shown in Figure 1, we differentiate between different types of eating behaviors. First,
some studies measure actual food consumption whereas others only capture food selection (e.g., the
purchase of food in a grocery store, cafeteria, or restaurant) without knowing whether the food was
entirely consumed. One may expect larger effect sizes for selection than for consumption if some
consumers, after being nudged to try a healthier food, are disappointed by its taste and only consume
part of it. On the other hand, people usually have a stronger preference for what to eat relative to
how much to eat (Wansink and Chandon 2014). Interventions aiming to influence consumption once

10
the food has already been selected, like plate and portion size changes, may be more effective than
those that attempt to influence what food is selected. This would imply larger effect sizes when
measuring actual consumption than selection. For these reasons, we expect similar effect sizes for
food selection and consumption. This hypothesis is consistent with existing meta-analyses of
specific types of healthy eating nudges, which found no differences between studies measuring
selection and those measuring actual consumption (Holden et al. 2016; Hollands et al. 2015;
Littlewood et al. 2016; Sinclair et al. 2014).
The second aspect of eating behavior that we examine is whether studies measure total
eating (e.g., the total number of calories of the food selected or consumed) or focus on the selection
or consumption of healthy or unhealthy foods. We expect smaller effect sizes when the dependent
variable is total amount of food ordered or consumed for two reasons. The first is that people must
eat—it is difficult, psychologically and physiologically, to sustain an imbalance between energy
intake and energy expenditure. In contrast, people have more flexibility in choosing how to allocate
their total calorie intake between healthy and unhealthy foods. Furthermore, healthy foods have
calories too, so replacing unhealthy food with healthier options—although clearly a form of
healthier eating—does not necessarily mean a reduction in the total quantity of food ordered or
consumed. Total eating therefore underestimates certain forms of healthier eating that are better
captured by measuring changes in healthy and unhealthy eating separately. This hypothesis is
consistent with an existing meta-analysis of interpretive nutrition labels, which found that they are
more effective in helping consumers in choosing healthier products than in changing total intake
(Cecchini and Warin 2016).
Finally, we hypothesize that interventions aimed at reducing unhealthy eating have a
stronger effect size than those aimed at promoting healthy eating. This prediction is based on the
fact that more than two thirds of Americans are overweight or obese, and about half of the latter are

11
actively trying to lose weight in any given year (Snook et al. 2017). Dieters should therefore be
particularly receptive to interventions that help reduce calorie intake, which is most effectively
accomplished by reducing the consumption of unhealthy foods rather than by increasing healthy
food consumption. Indeed, dieters and overweight consumers may be wary of increasing their
intake of foods presented as “healthy,” which often actually have a high energy density (Chernev
2011; Wansink and Chandon 2006). More generally, people often exhibit dynamically inconsistent
preferences, choosing unhealthy food in the short term and regretting it later (Prelec and
Loewenstein 1998; Wertenbroch 1998). Interventions that help people resist the temptation of
unhealthy food should therefore be particularly attractive to the large number of people who have
a long-term healthy eating goal and are aware that they need help resisting unhealthy foods despite
their best intentions. Our hypothesis is consistent with the results of two existing meta-analyses,
which found that the effectiveness of plate and portion size changes is higher for unhealthy foods
compared to healthy foods (Hollands et al. 2015; Zlatevska et al. 2014).
2.3. The role of population characteristics
We consider the influence of three population characteristics. We distinguish between
studies conducted in onsite eating settings (e.g., university or worksite cafeterias), offsite eating
eateries (e.g., restaurants, cinemas, cafes), and grocery stores. We expect weaker effects in grocery
stores compared to the other two settings. This is because it should be easier to respond to healthy
eating nudges when choosing for oneself, from among a limited number of options, and for a single
immediate consumption in a cafeteria or a restaurant, than when choosing for the entire family,
from among a huge variety of tempting options, and for multiple consumption occasions in a
grocery store. This hypothesis is consistent with research showing that uncertainty about future
preferences (when buying for the entire family, for example) increases the variety of choices (Walsh
1995), thereby mitigating the effects of nudges. It is also consistent with the systematic review

12
conducted by Seymour et al. (2004), which concluded that healthy eating nudges have weaker
effects in grocery stores than in restaurants or in university or worksite cafeterias.
Second, prior research has established that adults are more interested in nutrition than
children (Croll et al. 2001). Adults are also more sensitive than children to portion size changes
(Hollands et al. 2015; Zlatevska et al. 2014). We thus expect them to be more responsive to all types
of interventions than children. Finally, we expect to find higher effect sizes in studies conducted in
the US than in other countries. The higher proportion of overweight people in the US, the larger
size of portions there (Rozin et al. 2003), Americans’ higher interest in and knowledge of the health
consequences of eating (Rozin et al. 1999), and their greater reliance on external than internal cues
when making food decisions (Wansink et al. 2007) should all make interventions more effective in
the US than in the other Western countries in our sample.
2.4. The role of study characteristics
We expect two study characteristics to influence the effectiveness of healthy eating nudges.
First, food interventions vary in duration from single-exposure studies of one consumption occasion
to longitudinal interventions lasting several months. In field experiments, treatment effects usually
decay over time as people revert to habitual behavior (Brandon et al. 2017). We therefore expect to
find larger effect sizes for shorter studies than for longer ones.
Finally, we distinguish between studies using a pre-post design without control, those using
a single-difference treatment-control design, and those using a double-difference design. Although
designs with stronger levels of control should have a lower statistical bias in the estimation of the
effect size, the type of design itself should not influence the size of the effect. Therefore, we cannot
formulate hypotheses about the effect of design on effect sizes, and include this factor simply as a
control variable.

13
3. Data collection
3.1. Inclusion criteria
Appendix A provides detailed information on the search strategy, including the SPICE
(Setting, Population, Intervention, Comparison, Valuation) framework (Booth 2006) for the
selection of keywords and the PRISMA (Preferred Reporting Items for Systematic Reviews and
Meta-Analyses, Moher et al. 2009) flow diagram showing the number of articles included and
excluded. Briefly, we searched for relevant articles published in scholarly journals until December
2016 through keyword searches on Science Direct, PubMed, and Google Scholar. We also
examined all the references from 11 meta-analyses (Arno and Thomas 2016; Broers et al. 2017;
Cecchini and Warin 2016; Holden et al. 2016; Hollands et al. 2015; Littlewood et al. 2016; Long et
al. 2015; Nikolaou et al. 2014; Robinson et al. 2014; Sinclair et al. 2014; Zlatevska et al. 2014) and
7 systematic reviews (Bucher et al. 2016; Hollands et al. 2013; Nornberg et al. 2016; Roy et al.
2015; Skov et al. 2013; Thapaa and Lyford 2014; Wilson et al. 2016a). Both authors developed the
protocol detailing the search and inclusion criteria, coding categories for predictors, and
computation rules. The first author was trained to code all the studies and was responsible for
extracting data. The second author checked the results, and disagreements were solved through
discussion.
To be included in the meta-analysis, the study had to test a nudge intervention consistent
with our definition (e.g., not a price change nor a nutrition education campaign). Since our focus
was on pure nudges, studies (or conditions in studies) combining nudges with changes in economic
incentives or education efforts were not included. The intervention had to be tested in a field
experiment in which participants were not aware of the intervention, and thus not in a laboratory or
online setting. This is important because previous reviews found marked differences between
studies conducted in the field and those conducted in a laboratory or online (Long et al. 2015), and

14
between studies conducted with aware or unaware participants (Holden et al. 2016). Finally, the
dependent variable of the study had to provide an objective measure of food selection or
consumption (either in weight or energy). We rejected studies relying on consumption intentions.
Overall, the meta-analysis includes 277 effect sizes derived from 87 studies published in 81
articles. The number of observations per study ranged from 36 to 100 million, with a median of
1,168. Even after excluding the two outlier studies, one with 100 million transactions (Bollinger et
al. 2011) and one with 29 million transactions (Nikolova and Inman 2015), the meta-analysis
represents more than 4.1 million observations.
3.2. Effect sizes calculations
We calculated the effect sizes of studies with a binary outcome, such as the number of
participants who chose a healthy option, by computing the log odds ratio or by obtaining it directly
from the paper in the few cases when it was available. We computed the odds ratio as the odds of a
healthy selection in the treatment group divided by the odds of a healthy selection in the control
group. We then computed its standard error. We calculated the effect sizes of studies with a
continuous dependent variable, such as unhealthy food intake, by computing the standardized mean
difference, except in the few instances when the standardized mean difference, also known as
Cohen’s (1988) d, was already reported in the paper. We computed the d value as the mean
difference in consumption between the treatment and control condition, divided by the pooled
standard deviation. Given that we had two different effect-size metrics, we converted the log odds
ratio into d using the formula proposed by Borenstein et al. (2009). After the conversion, the 135
effects sizes originally calculated as log odds ratio were not statistically different from the 142 effect
sizes computed as d (p = .30). Hence, we report Cohen’s d in the paper because it is the most
common measure and because it allows direct comparisons with other meta-analyses.

15
The most common unreported data was the sample size per experimental condition (e.g.,
intervention vs. control). When only the total sample was reported, we divided the total number of
observations by the number of conditions. When only the number of observations in the control
group or in the intervention group was reported, we used the same number for the other group.
Whenever several assumptions were possible, we conservatively chose the assumption that yielded
the smaller effect size or the largest standard error.
When results were reported separately for each food in the same study (e.g., Ensaff et al.
2015), we calculated separate effect sizes per food and accounted for their dependence in the
statistical analysis. We also computed separate effect sizes for the few studies (e.g., Schwartz 2007)
that measured both food selection (e.g., putting a food item on a cafeteria tray) and consumption
(e.g., how much of it was consumed). When a study had a two-phase intervention (e.g., one
intervention during the first phase and then another intervention during a later phase, Thorndike et
al. 2012), we computed separate effect sizes for each phase and compared both phases to the
baseline period. When a study tested multiple interventions separately (e.g., Mollen et al. 2013), we
computed separate effect sizes for each intervention. Because only two studies reported results
separately for men and women (Baskin et al. 2016; Wansink and Payne 2007), we could not
examine the role of gender in the meta-analysis and calculated the average effect size for these two
studies.
3.3. Coding
Each intervention was categorized into one of the seven types discussed earlier. Field
experiments that implemented multiple interventions at once were treated separately. There are not
enough studies testing each possible combination of cognitive, affective, and behavioral
interventions (for example, only one study mixed a cognitive and a behavioral intervention), and so
we had to rely on an ad hoc coding of “mixed interventions” based on their frequency in our sample.

16
The first type of mixed intervention consists of studies mixing cognitive interventions with affective
and/or behavioral interventions (e.g., descriptive nutrition labeling and hedonic or sensory cues).
We named them “mixed: cognitive present.” The second type of mixed interventions consists of
studies combining affective and behavioral interventions. We named them “mixed: cognitive
absent.” We therefore have five categories for behavioral interventions: three for pure cognitive,
affective, and behavioral interventions and two for mixed interventions (mixed: cognitive present
and mixed: cognitive absent).
When the dependent variable of the study was the total amount of food selected or
consumed, it was categorized as “total eating.” When it was the selection or consumption of fruits,
vegetables, and water, or foods color-coded green in the study, we categorized it as “healthy eating.”
We categorized the selection or consumption of calorie-dense and nutrient-poor foods such as
desserts or sodas and those color-coded red in studies as “unhealthy eating.” We created a fourth
category (“mixed eating”) for foods that could not be categorized as healthy or unhealthy or which
were color-coded yellow by the researcher (rather than green or red). Because our goal is to examine
healthy eating, we reverse coded the effect sizes for unhealthy eating and for total eating.
We coded population characteristics according to where the study was conducted (school or
workplace onsite cafeterias; offsite restaurants, cinemas, or cafes; or grocery stores). We coded
whether the participants were children or adults. Finally, we distinguished between studies
conducted in the United States and those conducted in other countries (Belgium, Canada, France,
Ireland, Israel, Japan, Netherlands, and the United Kingdom). The number of studies in these other
countries was too low to enable a more refined level of analysis.
Regarding study characteristics, we measured the duration of the treatment as the number
of weeks of the intervention period. For example, if a study with a pre-post design measured food
choices in the 4 weeks prior to the intervention and in the 2 weeks after the intervention was

17
implemented, study duration is coded as 2 weeks. Because all the interventions that we studied were
applied continuously, duration captures—in the extreme case—the difference between the effects
of a single exposure to the nudge on a single food choice and the effects of repeated exposures to
the nudge over multiple food choices over time.
We distinguished between “double-difference” designs (which assigned participants to two
independent control and treatment conditions, with observations before and after the intervention),
“single-difference treatment-control” designs (which assigned respondents to two independent
control and treatment conditions), and “single-difference pre-post” designs (which used a pre-post
study design without a control group, comparing observations before and after the intervention).
Note that all are quasi-experiments because the randomization was not done at the participant level
but at the level of the store, restaurant, cafeteria, or at best, cafeteria line.
4. Analyses and results
As indicated in Table 1, the 11 existing meta-analyses used a standard two-level meta-
analytical model (Borenstein et al. 2009). In contrast, we used a three-level model (Cheung 2014),
which accounts for the fact that some observations come from the same field experiment (e.g.,
studies testing two types of interventions or measuring their impact on healthy and unhealthy foods
separately). We estimated a mixed-effects three-level meta-analytic model with the “metafor” R
package provided in Viechtbauer (2010), via maximum likelihood.
4.1. Average meta-analytical effect: Intercept-only model
Let 𝑦𝑖𝑗 be the 𝑖𝑡ℎ effect size in the 𝑗𝑡ℎ study. The equations from the three levels are:
𝑦𝑖𝑗 = 𝜆𝑖𝑗 + 𝑒𝑖𝑗 (1)
𝜆𝑖𝑗 = 𝜅𝑗 + 𝑢(2)𝑖𝑗 (2)
𝜅𝑗 = 𝑑0 + 𝑢(3)𝑗 (3)

18
where 𝜆𝑖𝑗 is the true effect size and Var(𝑒𝑖𝑗) = 𝑣𝑖𝑗 is the known sampling variance in the 𝑖𝑡ℎ
effect size in the 𝑗𝑡ℎ study. 𝜅𝑗 is the average effect size in the 𝑗𝑡ℎ study and Var(𝑢(2)𝑖𝑗) = 𝜏(2)2
captures the heterogeneity in effect sizes between different eating behaviors (e.g., selection or
consumption, healthy or unhealthy food) within the same study, when more than one outcome
was measured. 𝑑0 is the meta-analytic effect size estimated across all studies, and Var(u(3)j) =
τ(3)2 captures the heterogeneity between studies after controlling for the presence of multiple
observations at level 2. The three equations can be combined as follows:
𝑦𝑖𝑗 = 𝑑0 + 𝑢(2)𝑖𝑗 + 𝑢(3)𝑗 + 𝑒𝑖𝑗 (4)
We assessed the magnitude of effect size heterogeneity through the 𝐼2 index (Higgins and
Thompson 2002). We also report the decomposition of heterogeneity within-studies 𝐼(2)2 and
between-studies 𝐼(3)2 as derived in Cheung (2014). Heterogeneity is considered to be low if the 𝐼2
index is below 25%, medium if it is between 25% and 75%, and high if it is above 75% (Higgins
and Thompson 2002).
The standard two-level model yields a statistically significant average effect size (d = .22, z
= 13.05, p < .001) with a very large amount of heterogeneity (𝐼2 = 99.9%). The proposed three-
level model fits the data significantly better than the two-level model (2(1) = 81, p < .001) and
yields a slightly larger estimate of the average effect size (d = .27, z = 9.31, p < .001). This effect
size is considered small as per Cohen’s (1988) definition. The three-level random-effects model
shows that the total heterogeneity is lower within studies (𝐼(2)2 = 32.4%) than between studies (𝐼(3)
2 =
67.5%). Additional analyses reported in detail in Appendix B (p-curve, trim and fill, sensitivity
analyses) suggest minimal publication bias (Rothstein et al. 2006).

19
4.2. Influence of predictors: univariate vs. multivariate model selection
As shown in Table 1, the 11 existing meta-analyses on healthy eating nudges use univariate
meta-analyses (i.e., they separately test the impact of each predictor/outcome). Univariate analyses
exclude control variables and increase the possibility that significant differences are due to potential
confounds. Multivariate models help to provide estimates with better statistical properties, as well
as reduce the risk of bias such that a significant result in univariate analyses may not hold using the
multivariate model (Jackson et al. 2011). We performed both univariate and multivariate analyses
and confirm that the latter lead to a higher model fit as well as more conservative average effect
sizes (Figure 2, Appendix C).
Univariate models. We estimated one univariate meta-regression for each predictor x. These
univariate analyses provide benchmark values which can be compared to the estimates obtained in
the full multivariate model. When the predictor is categorical (for intervention type, for example),
the univariate model in Equation 5 estimates S coefficients 𝛽𝑠 corresponding to each level of the
categorical predictor, without any covariate. The third and fourth column of Figure 2 show,
respectively, the mean and standard errors of the 𝛽𝑠 coefficients, which capture the effect size for
each level of the categorical variables as estimated in a univariate regression.
𝑦𝑖𝑗 = ∑ 𝛽𝑠𝑥𝑖𝑗
𝑆
1
+ 𝑢(2)𝑖𝑗 + 𝑢(3)𝑗 + 𝑒𝑖𝑗
(5)
For study duration, which is a continuous variable measured in weeks, the univariate model
estimated one intercept and one parameter, as shown in Equation 6. To provide a point estimate for
short and long study durations, Figure 2 shows the model’s intercept estimated at the first quartile
(1 week) and third quartile (15 weeks) of the distribution of duration.
𝑦𝑖𝑗 = 𝑑0 + 𝛽𝐷𝑢𝑟𝑎𝑡𝑖𝑜𝑛𝐷𝑢𝑟𝑎𝑡𝑖𝑜𝑛𝑖𝑗 + 𝑢(2)𝑖𝑗 + 𝑢(3)𝑗 + 𝑒𝑖𝑗 (6)

20
Univariate analyses suggested that the effectiveness of healthy eating nudges varies by
intervention type (R2 = 29%, 𝜒2(4) = 35, p < .001). Figure 2 shows, for example, that the estimated
effect sizes in the univariate analysis of intervention type vary between d = .12 for cognitive
interventions and d = .48 for behavioral interventions, and are all statistically different from zero.
Univariate analyses found no difference between selection and consumption (R2 = 4%, 𝜒2(1) = 2.8,
p = .09) but significant effect depending on the behavior measured (total eating, healthy eating,
mixed eating, or unhealthy eating: R2 = 17%, 𝜒2(3) = 26, p < .001). They found no differences
between adults and children (R2 = 2%, 𝜒2(1) = 1.1, p = .29); between grocery stores, offsite eateries,
or onsite cafeterias (R2 = 7%, 𝜒2(2) = 5.5, p = .07), or between studies conducted in the US and
outside the US (R2 = 2%, 𝜒2(1) = 2.9, p = .09). Finally, they found a significant effect of duration
(R2 = 13%, 𝜒2(1) = 10.9, p = .02) and study design (R2 = 9%, 𝜒2(2) = 7.0, p = .03).
Multivariate model. We estimated a full model with all the predictors entered
simultaneously as shown in equation 7, where s corresponds to the categories for each predictor k.
The multivariate model explained 46% of the variance, a significant improvement over the
intercept-only model (𝜒2(15) = 70, p < .001). It is also a significant improvement over the best
univariate model, the one with intervention type (𝜒2(7) = 35, p < .001). This suggests that our
overall conceptual framework captured a substantial variation in the effect sizes, much more than
any separate univariate model.
𝑦𝑖𝑗 = 𝑑0 + ∑ ∑ 𝛽𝑘𝑠𝑥𝑘𝑖𝑗
𝐾
𝑘
𝑆−1
𝑠
+ 𝑢(2)𝑖𝑗 + 𝑢(3)𝑗 + 𝑒𝑖𝑗
(7)
The fifth and sixth columns in Figure 2 show the multivariate effect sizes estimated for each level
of a given predictor, when all the other predictors are at their mean value. Overall, the multivariate
model yielded effect sizes that are 16.4% smaller than those of the univariate models.

21
Figure 2: Effect sizes in the univariate and full multivariate models
Univariate Multi-
variate
Forrest plot (mean and 95% confidence
interval from the multivariate model)
k d se d se
Intervention type
Cognitive 113 .12* .04 .08 .05
Affective 47 .33* .06 .22* .06
Behavioral 73 .48* .05 .35* .06
Mixed: cognitive present 37 .20* .08 .20* .08
Mixed: cognitive absent 7 .30* .10 .23* .10
Eating behavior type
Selection 231 .25* .03 .20* .04
Consumption 46 .34* .05 .23* .06
Eating behavior measure
Total eating 22 .04 .06 .06 .08
Healthy eating 170 .27* .03 .26* .04
Mixed eating 14 .24* .06 .22* .07
Unhealthy eating 71 .39* .04 .33* .05
Population setting
Grocery stores 38 .12 .08 .11 .08
Offsite eateries 67 .24* .05 .29* .05
Onsite cafeterias 172 .32* .04 .25* .05
Population age
Children 96 .31* .05 .18* .06
Adults 181 .25* .04 .25* .05
Population country
Other countries 66 .18* .06 .15* .05
US 211 .30* .03 .28* .05
Study duration
Short (1 week) 277 .32* .05 .24* .04
Long (15 weeks) 277 .24* .05 .21* .04
Study design
Single pre-post 151 .24* .04 .13* .05
Single treatment-control 71 .38* .05 .28* .06
Double-difference 55 .19* .06 .25* .06
Average effect 277 .27* .03 .22* .04 * p < .05.
-0.1 0 0.1 0.2 0.3 0.4 0.5

22
Table 3: Parameter estimates of the multivariate model
𝜷 se Z
Intercept .22*** .04 5.00
Intervention type
Cognitive (ref)
Affective .14* .06 2.26
Behavioral .26*** .06 4.44
Mixed: cognitive present .12 .08 1.42
Mixed: cognitive absent .14 .10 1.39
Eating behavior type
Selection (ref)
Consumption .03 .05 .70
Eating behavior measure
Total eating -.20** .08 -2.58
Healthy eating (ref)
Mixed eating -.03 .07 -.54
Unhealthy eating .08* .04 2.18
Population setting
Grocery stores (ref)
Offsite eateries .18* .08 2.23
Onsite cafeterias .15* .07 2.10
Population age
Children (ref)
Adults .07 .06 1.30
Population country
Other countries (ref)
US .13* .05 2.49
Study duration
Intervention length (week) -.002 .001 -1.59
Study design
Single-difference pre-post (ref)
Single-difference treatment-control .14** .05 2.78
Double-difference .12 .06 1.95
K (observations) 277
N (studies) 87
𝑅2 .46
LR test vs. intercept-only model 70***
***p < .001, **p < .01, *p < .05.
Note: Each coefficient is interpreted as the difference with the reference category, denoted as “(ref).”

23
After controlling for all covariates, the average effect size computed across all 277 observations
shrinks slightly, from d =.27 to d = .22, but remains significantly different from zero (z = 5.00, p
< .001). Other effect sizes show stronger reductions. Importantly, the effect size for cognitive
intervention shrinks from .12 to .08 and is no longer statistically significant. The reduction is
particularly strong for the largest effect sizes, like behavioral interventions (which shrinks from .48
to .35). In the next section, we examine whether these smaller differences are still statistically
significant.
4.3. Hypothesis testing
To test our hypotheses, we estimated the full multivariate model (equation 7). We used
ANOVA coding (e.g., consumption = ½, selection = -½) so that the coefficients of the categorical
predictors represent a contrast with the reference category (see Table 3).
Effect sizes vary significantly between the three types of interventions. As hypothesized,
cognitive interventions are significantly less effective than affective (β = -.14, z = -2.26, p = .02)
or behavioral interventions (β = -.26, z = -4.44, p < .001). As expected, affective interventions are
less effective than behavioral interventions (β = -.12, z = -1.97, p = .049). Note that we chose to
report two-tailed p-values throughout the paper to avoid confusion and to be conservative, but that
a one-tailed test (yielding p = .025) would also be appropriate given that our hypothesis is about the
ordering of cognitive, affective, and behavioral interventions. Finally, mixed interventions are not
more effective than pure cognitive interventions, whether they include a cognitive intervention or
not (respectively, β = .12, z = 1.42, p = .15 and β = .14, z = 1.40, p = .16).
As expected, effect sizes are similar for food selection and actual consumption (β = .03, z
= .70, p = .48). However, effect sizes are significantly lower for total eating compared with healthy
eating (β = -.20, z = -2.58, p = .01) or unhealthy eating (β = -.28, z = -3.58, p < .001). As

24
hypothesized as well, effect sizes are significantly higher for unhealthy eating than for healthy
eating (β = .08, z = 2.18, p = .03).
As expected, and in contrast to what the univariate analyses suggested, effect sizes are
significantly lower for grocery stores compared to offsite eateries (β = -.18, z = -2.23, p = .03) or
onsite eateries (β = -.15, z = -2.10, p = .04). There are no differences between onsite and offsite
eateries (β = -.03, z = -.54, p = .60). As expected, and contrary to the univariate results, effect sizes
are significantly higher in the US than in other countries (β = .13, z = 2.50, p = .01). Contrary to
our hypothesis, there is no difference between children and adults (β =.07, z = 1.30, p = .19).
Similarly, effect sizes are unrelated to study duration (β = -.002, z = -1.60, p = .11), contrary to our
hypothesis and to the univariate results. Last, effect sizes are significantly lower in pre-post studies
than in double-difference studies (β = -.14, z = -2.78, p < .01), and (marginally) lower than in
single-difference studies (β = -.12, z = -1.95, p = .051). There is no difference between studies
using a single- and double-difference design (β = -.03, z = -.42, p = .67).
5. Discussion
It is easy to understand the growing enthusiasm for healthy eating nudges in academic and
policy circles. They promise to improve people’s diet at a fraction of the cost of economic incentives
or education programs and without imposing new taxes or constraints on businesses or consumers.
But do they really deliver on this promise? The encouraging results of existing reviews and meta-
analyses are derived from analyses of only a subset of interventions, and often include results from
studies conducted in favorable laboratory or online settings. More important, existing meta-analyses
relied on univariate comparisons between two or three groups of studies and failed to control for
important differences in eating behaviors, population, and studies in their sample or for the fact that
some studies yielded multiple effect sizes.

25
5.1. Do healthy nudges work, and to what extent?
Our analysis of 277 effect sizes derived from 81 articles and 87 field experiments shows
that the average effect size of healthy eating nudges is d = .217, with a 95% confidence interval of
[.132; .302]). Although this number is lower than what would have been obtained without
controlling for the characteristics of the eating behaviors, population, and studies, it is still
considered “small” (Cohen 1988).
In order to provide a more intuitive grasp of what this means, we computed the daily energy
equivalent that one would expect from such an effect size using the method described in Hollands
et al. (2015). Since d is the standardized mean difference, a d of .217 means that, on average, healthy
eating nudges increase healthy eating by .217 standard deviations. Assuming that the standard
deviation in daily energy intake is 537 kcal for an adult (Hollands et al. 2015), the average effect
size of .217 translates into a .217*537 = 117 kcal change in daily energy intake (-6.8% of the 1,727
kcal average energy intake). Given that a teaspoon of sugar contains 16 kcal, this is equivalent to
about 7 fewer teaspoons of sugar per day (see Table 4).
Table 4: Expected daily energy equivalents by intervention type
Effect sizes Daily equivalents a
Cohen’s d
(SMD)
Energy intake
change (kcal)
Energy intake
change (%)
Teaspoons
sugar b
Cognitive interventions .084 -45 -2.6% -2.8
Affective interventions .225 -121 -7.0% -7.5
Behavioral interventions .346 -186 -10.8% -11.6
Overall meta-analytical effect .217 -117 -6.8% -7.3
Notes: a The daily equivalents are computed using the mean and standard deviation in daily energy intake
of 1,727 ± 537 kcal reported in Hollands et al. (2015). b One teaspoon of sugar contains 16 kcal.
5.2. Which type of healthy eating nudge works best?
Table 4 provides the daily equivalents, in calories and teaspoons of sugar, of the average
effect sizes of cognitive, affective, and behavioral interventions. It shows that effect sizes increase

26
by 168% between cognitive and affective interventions (reducing daily energy intake from 45 kcal
to 121 kcal). Even more remarkable, moving from a cognitive to a behavioral intervention is
estimated to increases effect sizes by a factor of 4 (reducing daily energy intake from 45 to 186 kcal
per day).
There are also important differences between each type of cognitive, affective, and
behavioral nudges. As detailed in Appendix C, we estimated another regression which, instead of
estimating five effect sizes (for the three pure types and the two mixed types), estimated a separate
effect size for each of the seven subcategories, for the two mixed types of intervention, and for a
tenth subcategory consisting of studies combining multiple cognitive interventions (e.g., evaluative
nutrition labeling and salience enhancements). There were no studies combining the two types of
affective interventions or the two types of behavioral interventions. Figure 3 plots the univariate (x-
axis) and multivariate (y-axis) estimates of these ten effect sizes.
Figure 3: Effect sizes of intervention types estimated by univariate and multivariate models
Note: Effect sizes in parentheses are those estimated by the multivariate model.
Descriptive labeling
(d = .05)
Evaluative
labeling
(d = .13)Salience enhancements
(d = .10)
Combined
cognitive
nudges
(d = .18)
Healthy eating
prods (d = .25)
Hedonic or sensory
cues (d = .22)
Convenience enhancements
(d = .33)
Plate & portion
size changes
(d = .56)
Mixed:
cognitive
present
(d = .24)
Mixed:
cognitive
absent
(d = .25)
0
0,2
0,4
0,6
0,8
0 0,2 0,4 0,6 0,8
Mu
tliv
ari
ate
est
imate
s
Univariate estimates
Behavioral
interventions
Affective
interventions
Mixed-type
interventions
Best fitting line
(linear)
Cognitive
interventions

27
As Figure 3 shows, effect sizes are smaller (by 12% on average) in the multivariate analyses
and the magnitude of the reduction increases with the size of the effect. For example, the univariate
average effect size for plate and portion size shrinks by 22% (from d = .72 to d = .56). Note that
this univariate estimate (d = .72) is very similar to the value (d = .76) reported by Holden et al.
(2016) for studies with unaware participants (e.g., excluding laboratory or online studies),
suggesting that the reduction found by our multivariate model would apply also to the sample of
studies examined in prior meta-analyses. In addition to overestimating effect sizes, the univariate
analysis incorrectly ranks some of the interventions, suggesting, for example, that salience
enhancements are more effective than evaluative labeling, when they are not.
5.3. Which other factors influence the effectiveness of healthy eating nudges?
By explaining 46% of the variance among effect sizes, our study shows that some of the
characteristics of the eating behavior, population, and study significantly impact the effectiveness
of healthy eating nudges. First, we find that interventions more easily reduce unhealthy eating than
improve healthy eating or decrease total eating. In other words, it is easier to make people eat less
chocolate cake than to make them eat more vegetables, and the most difficult is to make them
generally eat less. Indeed, the effect size of healthy eating nudges on total eating (d = .06, z = .73,
p = .46) is not statistically different from zero. This finding is consistent with what we know about
the difficulty—perhaps even pointlessness—of hypocaloric diets.
Our result of a 33% stronger effect size for reducing unhealthy eating than for increasing
healthy eating is consistent with prior self-control research (Prelec and Loewenstein 1998;
Wertenbroch 1998). Dynamically inconsistent preferences and self-control lapses can explain why
people would particularly welcome interventions that reduce unhealthy eating and help them stick
to their long-term goals and avoid regret (Schwartz et al. 2014). However, future research is
necessary to test the robustness of this finding, which may be explained, at least in part, by the fact

28
that the most effective interventions (plate and portion size changes) have been disproportionally
implemented to reduce unhealthy eating rather than to promote healthy eating.
On the other hand, we replicate prior findings of similar effect sizes for food selection rather
than actual consumption. This is an important result because it suggests that researchers or
practitioners may not need to measure actual consumption to test the impact of their interventions,
which is usually considerably more onerous to measure than just the number of consumers picking
healthier options.
Importantly, and contrary to what we expected and to what had been reported in the
literature, effect sizes are unaffected by the duration of the study. Although it is a reassuring result
for anyone concerned about the long-term effectiveness of healthy eating nudges, we should note
that the trend is nevertheless toward smaller effects for longer studies. Figure 2 shows that our
model predicts that increasing the duration of the study from 1 week to 15 weeks would reduce
effect size by 12% (from d = .24 to d = .21). It remains to be seen by how much effect size would
change if a nudge were conducted over a longer period.
We also find that effect sizes increase with the level of control in the design of the study.
On average, effect sizes are 98% larger in studies with a control group compared with those with a
simple pre-post design without a control group. This suggests that researchers should use stronger
controls as much as possible. It also provides a way to correct the effect sizes found in pre-post
studies and to forecast what they might have been in a more controlled setting.
Turning to population characteristics, effect sizes are 60% smaller on average among
grocery shoppers than among cafeteria or restaurant eaters. This is consistent with our hypothesis
and with the literature, although more research is needed to determine if it is because of the
differences between choosing for immediate or future consumption, because of different levels of
competition, or because different goals are salient when grocery shopping vs. eating. Also

29
consistent with our hypothesis, effect sizes are 85% larger in studies conducted in the US than in
other countries. This may be because Americans focus less on the experience and more on the health
effects of eating (Rozin et al. 1999) or because they rely more strongly on external eating cues than
internal ones (Wansink et al. 2007). It could also be caused by the higher proportion of overweight
people in the US and the larger size of portions (Rozin et al. 2003). On the other hand, the difference
in effect sizes between adults and children is not statistically significant. Still, compared to the
univariate analyses which suggest larger effects for children than for adults, our results are in the
direction (smaller effects for children) that we hypothesized and that is consistent with the literature.
To determine conclusively whether children and adults respond differently to healthy eating nudges,
more research is needed, especially on cognitive interventions which have, so far, been tested
primarily with adults.
Table 5: Expected effectiveness increase between typical and best nudge study
Predictor Typical
scenario Best scenario
Increase
(d)
Increase
(contribution)
Intervention type Cognitive Behavioral .26 50%
Eating behavior type Selection Consumption .03 6%
Eating behavior measure Healthy Unhealthy .08 15%
Study Duration 6 weeks 1 week .01 2%
Study Design Pre-post Single-difference .14 27%
Population: Country US US
Population: Location Onsite cafeterias Onsite cafeterias
Population: Age Adults Adults
Effect Size (d) .17 .70 .53 100%
Our analysis allows us to predict what effect size one could expect when conducting a field
experiment with any combination of predictors, including the most typical and the most effective
combination. Table 5 summarizes the typical and best scenarios, while Figure 4 shows the
contribution of the different predictors. Table 5 shows that researchers choosing the most typical
level of each predictor (studying the effects of a cognitive intervention on the healthy food selection

30
of US adult cafeteria eaters for a pre-post 6-week study) could expect an effect size of only d = .17,
95% CI [.07, .28]). In contrast, researchers choosing the best combination of predictors (studying
the effects of a behavioral intervention on the unhealthy food consumption of adult cafeteria eaters
for a single-difference 1-week study) could expect an effect size four and a half times larger (d =
.70, 95% CI [.56, .84]). Computing the daily energy equivalents, we get a reduction by 94 kcal for
the typical nudge study, and a reduction by 374 kcal for the best one.
Figure 4: Expected effectiveness in typical vs. best nudge scenarios
5.4. Directions for future research
Our findings offer insights into where more research is needed and where it is not. Table 2
shows the number of observations by intervention type and target eating behavior (healthy or
unhealthy). This table makes it immediately apparent that no field experiment has tested the
effectiveness of displaying unattractive product descriptions or photos of unhealthy foods, like the
dissuasive photos used on cigarette packs in some countries (Kees et al. 2006). Although degrading
other brands may be difficult because of trademark laws, it has shown promise in laboratory studies
(Hollands et al. 2011), and retailers or restaurants could test this strategy with their own unhealthy
products. It would also seem important to run more studies increasing portion, plate, or glass size
for healthy foods and beverages, rather than for unhealthy ones. Further studies are needed to
examine the effectiveness of hedonic sensory cues, for which we only have 12 effect sizes.
Precedence should be given to testing interventions in grocery stores and outside the US, and for
.70
.17
0,0 0,1 0,2 0,3 0,4 0,5 0,6 0,7 0,8
Standardized mean difference
Intervention
type
Eating
behavior type
Eating
measure
Study
design
Study
duration
Typical
scenario
Best
scenario

31
unhealthy foods. These issues should have priority over other well-researched topics, such as
studying the effects of cognitive interventions on healthy eating in cafeterias using a pre-post
design.
Beyond filling out the underpopulated cells of the framework, three research areas appear
particularly fruitful. The first is to study interaction effects. Because of lack of data in our sample,
it is not possible to estimate interactions effects between each intervention type and the other
predictors. In Appendix D, we report the results of a simplified model using linear coding for
intervention type and eating behavior (from total eating to healthy eating). This preliminary analysis
suggests that shifting from cognitive to behavioral interventions is particularly impactful on
consumption (vs. selection), for adults (vs. children), and in the US (vs. in other countries). These
results qualify the lack of main effect for eating behavior and for participant age reported in the
main results. However, additional field experiments orthogonally manipulating intervention type
and population or study characteristics would be necessary to confirm these results.
Second, it would be important to study the interplay between interventions and economic
incentives. One would hope to find synergies between the two that allow, for example, reduction in
the magnitude of economic incentives. Similarly, it would be interesting to compare behavioral and
economic interventions, both in terms of their effects on healthy eating and in terms of their cost
effectiveness.
Finally, the prevalence and severity of non-communicable diseases is strongly associated
with socioeconomic and cultural factors such as income, education, gender, ethnicity, and culture
(Bartley 2017). Surprisingly, this data was almost never available in the studies that we analyzed.
Future research should therefore measure socioeconomic data, as well as biomarkers such as body
mass or diabetes diagnoses, and traits such as cognitive restraint or impulsivity that strongly
influence food choices and health (Ma et al. 2013; Sutin et al. 2011). Such information should be

32
provided, at a minimum, to better characterize the respondent population; it would be even better
to report results separately for different population types. This should be done systematically even
in the absence of significant differences. When prior research or theory predicts an effect, finding
none can be informative.
More broadly, future research should expand the dependent variables beyond purchase and
consumption. To encourage the adoption of healthy eating nudges in commercial operations, it is
important to measure their impact on the consumer’s experience, satisfaction, and perception of
value, as well as on the company’s top and bottom lines. Even interventions that lead to a reduction
in consumption can be good for business if they attract new consumers who value their ability to
nudge them away from unhealthy choices that they will later regret. Similarly, one of the core tenets
of nudges is that they improve consumer welfare as judged by consumers themselves (Sunstein
2017). Future studies should therefore measure whether making the intervention more salient, by
alerting consumers to it, for example, would influence its effectiveness. It would be important to
know whether people, upon learning that they have been subject to an intervention, would agree
that it led them to make better decisions compared to the status quo ante, but also compared to other
interventions such as taxes and other economic incentives. This is important because, while they
preserve freedom of choice, the interventions analyzed here are nevertheless paternalistic. Finding
that consumers welcome these interventions, and that they are compatible with commercial goals,
would go a long way to encourage their adoption in multiple contexts.
5.5. Toward a “living” meta-analysis
One of the biggest challenges of studying healthy eating nudges is the exponential increase
in the studies carried out. Of the 277 effect sizes we analyzed, 166 (60%) were published in the past
5 years, a 133% increase over the previous 5 years. By simple extrapolation, we can predict that
222 new effect sizes will be estimated between 2017 and 2021. This upsurge makes meta-analyses

33
even more valuable but also means that they rapidly become out of date. Compounding the problem,
research on healthy eating nudges is published in a wide variety of scientific publications in
marketing, nutrition, psychology, and health sciences, which are indexed in different databases and
not always available to all researchers. To mitigate these problems, encourage the diffusion of our
results, and correct possible categorization errors, the spreadsheet containing the raw data will be
made available online (post publication). In addition, we have created a simple survey (available at
http://tinyurl.com/healthy-eating-nudge) to allow researchers to correct and update the database by
entering information about their study. We hope that this “living” meta-analysis will encourage the
consolidation and diffusion of knowledge and contribute to making science more open.

34
6. References
* Adams, M.A., R.L. Pelletier, M.M. Zive, J.F. Sallis. 2005. Salad bars and fruit and vegetable
consumption in elementary schools: A plate waste study. J Am Diet Assoc. 105(11) 1789-
1792.
Afshin, A., J.L. Peñalvo, L. Del Gobbo, J. Silva, M. Michaelson, M. O'Flaherty, S. Capewell, D.
Spiegelman, G. Danaei, D. Mozaffarian. 2017. The prospective impact of food pricing on
improving dietary consumption: A systematic review and meta-analysis. PLoS One. 12(3)
e0172277.
Arno, A., S. Thomas. 2016. The efficacy of nudge theory strategies in influencing adult dietary
behaviour: A systematic review and meta-analysis. BMC Public Health. 16(1) 676.
* Auchincloss, A.H., G.G. Mallya, B.L. Leonberg, A. Ricchezza, K. Glanz, D.F. Schwarz. 2013.
Customer responses to mandatory menu labeling at full-service restaurants. Am J Prev
Med. 45(6) 710-719.
Barry, T.E., D.J. Howard. 1990. A review and critique of the hierarchy of effects in advertising.
Int J Advert. 9(2) 121-135.
* Bartholomew, J.B., E.M. Jowers. 2006. Increasing frequency of lower-fat entrees offered at
school lunch: An environmental change strategy to increase healthful selections. J Acad
Nutr Diet. 106(2) 248-252.
Bartley, M. 2017. Health inequality : An introduction to concepts, theories and methods. Polity,
Cambridge, UK ; Malden, MA, USA.
* Baskin, E., M. Gorlin, Z. Chance, N. Novemsky, R. Dhar, K. Huskey, M. Hatzis. 2016.
Proximity of snacks to beverages increases food consumption in the workplace: A field
study. Appetite. 103 244-248.
Bloom, D., E. Cafiero, E. Jané-Llopis, S. Abrahams-Gessel, L. Bloom, S. Fathima, A. Feigl, T.
Gaziano, A. Hamandi, M. Mowafi. 2012. The global economic burden of
noncommunicable diseases. Program on the Global Demography of Aging.
* Bollinger, B., P. Leslie, A. Sorensen. 2011. Calorie posting in chain restaurants. Am Econ J
Econ Policy. 3(1) 91-128.
Booth, A. 2006. Clear and present questions: Formulating questions for evidence based practice.
Library Hi Tech. 24(3) 355-368.
Borenstein, M., L.V. Hedges, J.P.T. Higgins, H.R. Rothstein. 2009. Introduction to meta-analysis.
John Wiley & Sons, Chichester, U.K.
Brandon, A., P.J. Ferraro, J.A. List, R.D. Metcalfe, M.K. Price, F. Rundhammer. 2017. Do the
effects of social nudges persist? Theory and evidence from 38 natural field experiments.
NBER Working Paper Series. No. 23277.
Breckler, S.J. 1984. Empirical validation of affect, behavior, and cognition as distinct components
of attitude. J Pers Soc Psychol. 47(6) 1191-1205.
* Brissette, I., A. Lowenfels, C. Noble, D. Spicer. 2013. Predictors of total calories purchased at
fast-food restaurants: Restaurant characteristics, calorie awareness, and use of calorie
information. J Nutr Educ Behav. 45(5) 404-411.
Broers, V.J., C. De Breucker, S. Van den Broucke, O. Luminet. 2017. A systematic review and
meta-analysis of the effectiveness of nudging to increase fruit and vegetable choice. Eur J
Public Health. 27(5) 912-920.
Article included in the meta-analysis.

35
Bucher, T., C. Collins, M.E. Rollo, T.A. McCaffrey, N. De Vlieger, D. Van der Bend, H. Truby,
F.J. Perez-Cueto. 2016. Nudging consumers towards healthier choices: A systematic
review of positional influences on food choice. Br J Nutr. 115(12) 2252-2263.
* Buscher, L.A., K.A. Martin, S. Crocker. 2001. Point-of-purchase messages framed in terms of
cost, convenience, taste, and energy improve healthful snack selection in a college
foodservice setting. J Acad Nutr Diet. 101(8) 909-913.
Carpenter, C.J. 2010. A meta-analysis of the effectiveness of health belief model variables in
predicting behavior. Health Communication. 25(8) 661-669.
* Cawley, J., M.J. Sweeney, J. Sobal, D.R. Just, H.M. Kaiser, W.D. Schulze, E. Wethington, B.
Wansink. 2015. The impact of a supermarket nutrition rating system on purchases of
nutritious and less nutritious foods. Public Health Nutr. 18(01) 8-14.
Cecchini, M., L. Warin. 2016. Impact of food labelling systems on food choices and eating
behaviours: A systematic review and meta-analysis of randomized studies. Obesity
Reviews. 17(3) 201-210.
Chance, Z., M. Gorlin, R. Dhar. 2014. Why choosing healthy foods is hard, and how to help:
Presenting the 4ps framework for behavior change. Customer Needs and Solutions. 1(4)
253-262.
Chernev, A. 2011. The dieter's paradox. J Consum Psychol. 21(2) 178-183.
Cheung, M.W.L. 2014. Modeling dependent effect sizes with three-level meta-analyses: A
structural equation modeling approach. Psychol Methods. 19(2) 211-229.
* Chu, Y.H., E.A. Frongillo, S.J. Jones, G.L. Kaye. 2009. Improving patrons' meal selections
through the use of point-of-selection nutrition labels. Am J Public Health. 99(11) 2001-
2005.
Cohen, J. 1988. Statistical power analysis for the behavioral sciences. Lawrence Erlbaum
Associates, Hillsdale, NJ.
* Cohen, J.F., S.A. Richardson, S.A. Cluggish, E. Parker, P.J. Catalano, E.B. Rimm. 2015. Effects
of choice architecture and chef-enhanced meals on the selection and consumption of
healthier school foods: A randomized clinical trial. JAMA Pediatr. 169(5) 431-437.
* Crockett, R.A., S.A. Jebb, M. Hankins, T.M. Marteau. 2014. The impact of nutritional labels
and socioeconomic status on energy intake. An experimental field study. Appetite. 81 12-
19.
Croll, J.K., D. Neumark-Sztainer, M. Story. 2001. Healthy eating: What does it mean to
adolescents? J Nutr Educ. 33(4) 193-198.
* Dayan, E., M. Bar-Hillel. 2011. Nudge to nobesity ii: Menu positions influence food orders.
Judgm Decis Mak. 6(4) 333.
* de Wijk, R.A., A.J. Maaskant, I.A. Polet, N.T. Holthuysen, E. van Kleef, M.H. Vingerhoeds.
2016. An in-store experiment on the effect of accessibility on sales of wholegrain and
white bread in supermarkets. PLoS One. 11(3) e0151915.
* Diliberti, N., P.L. Bordi, M.T. Conklin, L.S. Roe, B.J. Rolls. 2004. Increased portion size leads
to increased energy intake in a restaurant meal. Obesity. 12(3) 562-568.
* DiSantis, K.I., L.L. Birch, A. Davey, E.L. Serrano, J. Zhang, Y. Bruton, J.O. Fisher. 2013. Plate
size and children’s appetite: Effects of larger dishware on self-served portions and intake.
Pediatrics. 131(5) e1451-e1458.
* Downs, J.S., J. Wisdom, B. Wansink, G. Loewenstein. 2013. Supplementing menu labeling with
calorie recommendations to test for facilitation effects. Am J Public Health. 103(9) 1604-
1609.
* Dubbert, P.M., W.G. Johnson, D.G. Schlundt, N.W. Montague. 1984. The influence of caloric
information on cafeteria food choices. J Appl Behav Anal. 17(1) 85-92.

36
Duckworth, A.L., T.S. Gendler, J.J. Gross. 2016. Situational strategies for self-control.
Perspectives on Psychological Science. 11(1) 35-55.
* Dumanovsky, T., C.Y. Huang, C.A. Nonas, T.D. Matte, M.T. Bassett, L.D. Silver. 2011.
Changes in energy content of lunchtime purchases from fast food restaurants after
introduction of calorie labelling: Cross sectional customer surveys. BMJ. 343.
Duval, S., R. Tweedie. 2000. Trim and fill: A simple funnel‐plot–based method of testing and
adjusting for publication bias in meta‐analysis. Biometrics. 56(2) 455-463.
* Elbel, B., J. Gyamfi, R. Kersh. 2011. Child and adolescent fast-food choice and the influence of
calorie labeling: A natural experiment. Int J Obes. 35(4) 493-500.
* Elbel, B., R. Kersh, V.L. Brescoll, L.B. Dixon. 2009. Calorie labeling and food choices: A first
look at the effects on low-income people in new york city. Health Aff. 28(6) w1110-1121.
* Elbel, B., T. Mijanovich, L.B. Dixon, C. Abrams, B. Weitzman, R. Kersh, A.H. Auchincloss, G.
Ogedegbe. 2013. Calorie labeling, fast food purchasing and restaurant visits. Obesity.
21(11) 2172-2179.
* Ellison, B., J.L. Lusk, D. Davis. 2013. Looking at the label and beyond: The effects of calorie
labels, health consciousness, and demographics on caloric intake in restaurants. Int J
Behav Nutr Phys Act. 10(1) 21.
* Elsbernd, S., M. Reicks, T. Mann, J. Redden, E. Mykerezi, Z. Vickers. 2016. Serving vegetables
first: A strategy to increase vegetable consumption in elementary school cafeterias.
Appetite. 96 111-115.
* Ensaff, H., M. Homer, P. Sahota, D. Braybrook, S. Coan, H. McLeod. 2015. Food choice
architecture: An intervention in a secondary school and its impact on students’ plant-based
food choices. Nutrients. 7(6) 4426-4437.
Fernandes, A.C., R.C. Oliveira, R.P.C. Proença, C.C. Curioni, V.M. Rodrigues, G.M.R. Fiates.
2016. Influence of menu labeling on food choices in real-life settings: A systematic
review. Nutr Rev. 74(8) 534-548.
* Finkelstein, E.A., K.L. Strombotne, N.L. Chan, J. Krieger. 2011. Mandatory menu labeling in
one fast-food chain in king county, washington. Am J Prev Med. 40(2) 122-127.
* Foster, G.D., A. Karpyn, A.C. Wojtanowski, E. Davis, S. Weiss, C. Brensinger, A. Tierney, W.
Guo, J. Brown, C. Spross. 2014. Placement and promotion strategies to increase sales of
healthier products in supermarkets in low-income, ethnically diverse neighborhoods: A
randomized controlled trial. Am J Clin Nutr. 99(6) 1359-1368.
* Freedman, M.R. 2011. Point-of-selection nutrition information influences choice of portion size
in an all-you-can-eat university dining hall. Journal of Foodservice Business Research.
14(1) 86-98.
* Freedman, M.R., C. Brochado. 2010. Reducing portion size reduces food intake and plate waste.
Obesity. 18(9) 1864-1866.
* Gaigi, H., S. Raffin, M. Maillot, L. Adrover, B. Ruffieux, N. Darmon. 2015. Expérimentation
d’un fléchage nutritionnel dans deux supermarchés à marseille «le choix vita+». Cahiers
de Nutrition et de Diététique. 50(1) 16-24.
* Gamburzew, A., N. Darcel, R. Gazan, C. Dubois, M. Maillot, D. Tomé, S. Raffin, N. Darmon.
2016. In-store marketing of inexpensive foods with good nutritional quality in
disadvantaged neighborhoods: Increased awareness, understanding, and purchasing. Int J
Behav Nutr Phys Act. 13(1) 104.
* Geaney, F., C. Kelly, J.S. Di Marrazzo, J.M. Harrington, A.P. Fitzgerald, B.A. Greiner, I.J.
Perry. 2016. The effect of complex workplace dietary interventions on employees' dietary
intakes, nutrition knowledge and health status: A cluster controlled trial. Prev Med. 89 76-
83.

37
Glanz, K., M. Basil, E. Maibach, J. Goldberg, D.A.N. Snyder. 1998. Why americans eat what they
do: Taste, nutrition, cost, convenience, and weight control concerns as influences on food
consumption. J Am Diet Assoc. 98(10) 1118-1126.
* Goto, K., A. Waite, C. Wolff, K. Chan, M. Giovanni. 2013. Do environmental interventions
impact elementary school students' lunchtime milk selection? Appl Econ Perspect Policy.
35(2) 360-376.
* Hanks, A.S., D.R. Just, L.E. Smith, B. Wansink. 2012. Healthy convenience: Nudging students
toward healthier choices in the lunchroom. J Public Health. 34(3) 370-376.
* Hanks, A.S., D.R. Just, B. Wansink. 2013. Smarter lunchrooms can address new school
lunchroom guidelines and childhood obesity. J Pediatr. 162(4) 867-869.
Hanssens, D.M., K.H. Pauwels, S. Srinivasan, M. Vanhuele, G. Yildirim. 2014. Consumer
attitude metrics for guiding marketing mix decisions. Marketing Sci. 33(4) 534-550.
Herman, C.P., J. Polivy. 2008. External cues in the control of food intake in humans: The sensory-
normative distinction. Physiol Behav. 94(5) 722-728.
Higgins, J., S.G. Thompson. 2002. Quantifying heterogeneity in a meta‐analysis. Stat Med. 21(11)
1539-1558.
Hilgard, E.R. 1980. The trilogy of mind: Cognition, affection, and conation. J Hist Behav Sci.
16(2) 107-117.
* Hoefkens, C., C. Lachat, P. Kolsteren, J. Van Camp, W. Verbeke. 2011. Posting point-of-
purchase nutrition information in university canteens does not influence meal choice and
nutrient intake. Am J Clin Nutr. 94(2) 562-570.
Holden, S.S., N. Zlatevska, C. Dubelaar. 2016. Whether smaller plates reduce consumption
depends on who’s serving and who’s looking: A meta-analysis. Journal of the Association
for Consumer Research. 1(1) 134-146.
Hollands, G., G. Bignardi, M. Johnston, M. Kelly, D. Ogilvie, M. Petticrew, A. Prestwich, I.
Shemilt, S. Sutton, T. Marteau. 2017. The tippme intervention typology for changing
environments to change behaviour. Nature Human Behaviour.
Hollands, G.J., A. Prestwich, T.M. Marteau. 2011. Using aversive images to enhance healthy food
choices and implicit attitudes: An experimental test of evaluative conditioning. Health
Psychol. 30(2) 195.
Hollands, G.J., I. Shemilt, T.M. Marteau, S.A. Jebb, M.P. Kelly, R. Nakamura, M. Suhrcke, D.
Ogilvie. 2013. Altering micro-environments to change population health behaviour:
Towards an evidence base for choice architecture interventions. BMC Public Health. 13(1)
1218.
Hollands, G.J., I. Shemilt, T.M. Marteau, S.A. Jebb, H.B. Lewis, Y. Wei, J.P. Higgins, D. Ogilvie.
2015. Portion, package or tableware size for changing selection and consumption of food,
alcohol and tobacco. Cochrane Database Syst Rev. 9 CD011045.
* Hubbard, K.L., L.G. Bandini, S.C. Folta, B. Wansink, M. Eliasziw, A. Must. 2015. Impact of a
smarter lunchroom intervention on food selection and consumption among adolescents
and young adults with intellectual and developmental disabilities in a residential school
setting. Public Health Nutr. 18(2) 361-371.
Jackson, D., R. Riley, I.R. White. 2011. Multivariate meta‐analysis: Potential and promise. Stat
Med. 30(20) 2481-2498.
Januszewska, R., Z. Pieniak, W. Verbeke. 2011. Food choice questionnaire revisited in four
countries. Does it still measure the same? Appetite. 57(1) 94-98.
Kees, J., S. Burton, J.C. Andrews, J. Kozup. 2006. Tests of graphic visuals and cigarette package
warning combinations: Implications for the framework convention on tobacco control. J
Public Policy Mark. 25(2) 212-223.

38
Kiesel, K., S.B. Villas-Boas. 2013. Can information costs affect consumer choice? Nutritional
labels in a supermarket experiment. Int J Ind Organ. 31(2) 153-163.
Kraak, V.I., T. Englund, S. Misyak, E.L. Serrano. 2017. A novel marketing mix and choice
architecture framework to nudge restaurant customers toward healthy food environments
to reduce obesity in the united states. Obesity Reviews. 18(8) 852-868.
* Krieger, J.W., N.L. Chan, B.E. Saelens, M.L. Ta, D. Solet, D.W. Fleming. 2013. Menu labeling
regulations and calories purchased at chain restaurants. Am J Prev Med. 44(6) 595-604.
* Kroese, F.M., D.R. Marchiori, D.T. de Ridder. 2016. Nudging healthy food choices: A field
experiment at the train station. J Public Health. 38(2) e133-e137.
* Lachat, C.K., R. Verstraeten, B. De Meulenaer, J. Menten, L.F. Huybregts, J. Van Camp, D.
Roberfroid, P.W. Kolsteren. 2009. Availability of free fruits and vegetables at canteen
lunch improves lunch and daily nutritional profiles: A randomised controlled trial. Br J
Nutr. 102(07) 1030-1037.
* Levin, S. 1996. Pilot study of a cafeteria program relying primarily on symbols to promote
healthy choices. J Nutr Educ. 28(5) 282-285.
* Levy, D.E., J. Riis, L.M. Sonnenberg, S.J. Barraclough, A.N. Thorndike. 2012. Food choices of
minority and low-income employees: A cafeteria intervention. Am J Prev Med. 43(3) 240-
248.
Littlewood, J.A., S. Lourenço, C.L. Iversen, G.L. Hansen. 2016. Menu labelling is effective in
reducing energy ordered and consumed: A systematic review and meta-analysis of recent
studies. Public Health Nutr. 19(12) 2106-2121.
Long, M.W., D.K. Tobias, A.L. Cradock, H. Batchelder, S.L. Gortmaker. 2015. Systematic
review and meta-analysis of the impact of restaurant menu calorie labeling. Am J Public
Health. 105(5) e11-e24.
Ma, Y., K.L. Ailawadi, D. Grewal. 2013. Soda versus cereal and sugar versus fat: Drivers of
healthful food intake and the impact of diabetes diagnosis. J Marketing. 77(3) 101-120.
Macht, M. 2008. How emotions affect eating: A five-way model. Appetite. 50(1) 1-11.
* Meyers, A.W., A.J. Stunkard. 1980. Food accessibility and food choice: A test of schachter's
externality hypothesis. Arch Gen Psychiatry. 37(10) 1133-1135.
* Miller, G.F., S. Gupta, J.D. Kropp, K.A. Grogan, A. Mathews. 2016. The effects of pre-ordering
and behavioral nudges on national school lunch program participants’ food item selection.
J Econ Psychol. 55 4-16.
* Mishra, A., H. Mishra, T.M. Masters. 2012. The influence of bite size on quantity of food
consumed: A field study. Journal of Consumer Research. 38(5) 791-795.
Moher, D., A. Liberati, J. Tetzlaff, D.G. Altman, P. Group. 2009. Preferred reporting items for
systematic reviews and meta-analyses: The prisma statement. PLoS Med. 6(7) e1000097.
* Mollen, S., R.N. Rimal, R.A. Ruiter, G. Kok. 2013. Healthy and unhealthy social norms and
food selection. Findings from a field-experiment. Appetite. 65 83-89.
* Morizet, D., L. Depezay, P. Combris, D. Picard, A. Giboreau. 2012. Effect of labeling on new
vegetable dish acceptance in preadolescent children. Appetite. 59(2) 399-402.
Murimi, M.W., M. Kanyi, T. Mupfudze, M.R. Amin, T. Mbogori, K. Aldubayan. 2017. Factors
influencing efficacy of nutrition education interventions: A systematic review. J Nutr
Educ Behav. 49(2) 142-165.e141.
Nikolaou, C.K., C.R. Hankey, M.E.J. Lean. 2014. Calorie-labelling: Does it impact on calorie
purchase in catering outlets and the views of young adults? Int J Obes. 39 542.
* Nikolova, H.D., J.I. Inman. 2015. Healthy choice: The effect of simplified pos nutritional
information on consumer food choice behavior. J Marketing Res. 7(December) 817–835.

39
Nornberg, T.R., L. Houlby, L.R. Skov, F.J. Perez-Cueto. 2016. Choice architecture interventions
for increased vegetable intake and behaviour change in a school setting: A systematic
review. Perspectives in public health. 136(3) 132-142.
* Ogawa, Y., N. Tanabe, A. Honda, T. Azuma, N. Seki, T. Suzuki, H. Suzuki. 2011. Point-of-
purchase health information encourages customers to purchase vegetables: Objective
analysis by using a point-of-sales system. Environ Health Prev Med. 16(4) 239-246.
Full publication date: 1999 Oliver, R.L. 1999. Whence consumer loyalty? J Marketing. 63 33-44.
* Olstad, D.L., L.A. Goonewardene, L.J. McCargar, K.D. Raine. 2014. Choosing healthier foods
in recreational sports settings: A mixed methods investigation of the impact of nudging
and an economic incentive. Int J Behav Nutr Phys Act. 11(1) 6.
* Olstad, D.L., J. Vermeer, L.J. McCargar, R.J. Prowse, K.D. Raine. 2015. Using traffic light
labels to improve food selection in recreation and sport facility eating environments.
Appetite. 91 329-335.
Ouellette, J.A., W. Wood. 1998. Habit and intention in everyday life: The multiple processes by
which past behavior predicts future behavior. Psychol Bull. 124(1) 54-74.
* Perry, C.L., D.B. Bishop, G.L. Taylor, M. Davis, M. Story, C. Gray, S.C. Bishop, R.A.W.
Mays, L.A. Lytle, L. Harnack. 2004. A randomized school trial of environmental
strategies to encourage fruit and vegetable consumption among children. Health Educ
Behav. 31(1) 65-76.
* Policastro, P., Z. Smith, G. Chapman. 2017. Put the healthy item first: Order of ingredient
listing influences consumer selection. J Health Psychol. 22(7) 853-863.
Prelec, D., G. Loewenstein. 1998. The red and the black: Mental accounting of savings and debt.
Marketing Sci. 17(1) 4-28.
Pulos, E., K. Leng. 2010. Evaluation of a voluntary menu-labeling program in full-service
restaurants. Am J Public Health. 100(6) 1035-1039.
* Redden, J.P., T. Mann, Z. Vickers, E. Mykerezi, M. Reicks, S. Elsbernd. 2015. Serving first in
isolation increases vegetable intake among elementary schoolchildren. PLoS One. 10(4)
e0121283.
* Reicks, M., J.P. Redden, T. Mann, E. Mykerezi, Z. Vickers. 2012. Photographs in lunch tray
compartments and vegetable consumption among children in elementary school cafeterias.
JAMA. 307(8) 784-785.
* Roberto, C.A., P.D. Larsen, H. Agnew, J. Baik, K.D. Brownell. 2010. Evaluating the impact of
menu labeling on food choices and intake. Am J Public Health. 100(2) 312-318.
Robinson, E. 2017. The science behind smarter lunchrooms. PeerJ Preprints. 5 e3137v3131.
Robinson, E., S. Nolan, C. Tudur‐Smith, E.J. Boyland, J.A. Harrold, C.A. Hardman, J.C. Halford.
2014. Will smaller plates lead to smaller waists? A systematic review and meta‐analysis of
the effect that experimental manipulation of dishware size has on energy consumption.
Obes Rev. 15(10) 812-821.
Rothstein, H.R., A.J. Sutton, M. Borenstein. 2006. Publication bias in meta-analysis: Prevention,
assessment and adjustments. John Wiley & Sons.
Roy, R., B. Kelly, A. Rangan, M. Allman-Farinelli. 2015. Food environment interventions to
improve the dietary behavior of young adults in tertiary education settings: A systematic
literature review. J Acad Nutr Diet. 115(10) 1647-1681.e1641.
Rozin, P., C. Fischler, S. Imada, A. Sarubin, A. Wrzesniewski. 1999. Attitudes to food and the
role of food in life in the u.S.A., japan, flemish belgium and france: Possible implications
for the diet-health debate. Appetite. 33(2) 163-180.

40
Rozin, P., K. Kabnick, E. Pete, C. Fischler, C. Shields. 2003. The ecology of eating: Smaller
portion sizes in france than in the united states help explain the french paradox. Psychol
Sci. 14(5) 450-454.
* Rozin, P., S. Scott, M. Dingley, J.K. Urbanek, H. Jiang, M. Kaltenbach. 2011. Nudge to
nobesity i: Minor changes in accessibility decrease food intake. Judgm Decis Mak. 6(4)
323-332.
Schwartz, J., D. Mochon, L. Wyper, J. Maroba, D. Patel, D. Ariely. 2014. Healthier by
precommitment. Psychol Sci.
* Schwartz, J., J. Riis, B. Elbel, D. Ariely. 2012. Inviting consumers to downsize fast-food
portions significantly reduces calorie consumption. Health Aff. 31(2) 399-407.
* Schwartz, M.B. 2007. The influence of a verbal prompt on school lunch fruit consumption: A
pilot study. Int J Behav Nutr Phys Act. 4(1) 6.
Seymour, J.D., A. Lazarus Yaroch, M. Serdula, H.M. Blanck, L.K. Khan. 2004. Impact of
nutrition environmental interventions on point-of-purchase behavior in adults: A review.
Prev Med. 39(2) 108-136.
* Shah, A.M., J.R. Bettman, P.A. Ubel, P.A. Keller, J.A. Edell. 2014. Surcharges plus unhealthy
labels reduce demand for unhealthy menu items. J Marketing Res. 51(6) 773-789.
Simonsohn, U., L.D. Nelson, J.P. Simmons. 2014a. P-curve and effect size: Correcting for
publication bias using only significant results. Perspect Psychol Sci. 9(6) 666-681.
Simonsohn, U., L.D. Nelson, J.P. Simmons. 2014b. P-curve: A key to the file-drawer. J Exp
Psychol Gen. 143(2) 534.
Sinclair, S.E., M. Cooper, E.D. Mansfield. 2014. The influence of menu labeling on calories
selected or consumed: A systematic review and meta-analysis. J Acad Nutr Diet. 114(9)
1375-1388.e1315.
Skov, L.R., S. Lourenco, G.L. Hansen, B.E. Mikkelsen, C. Schofield. 2013. Choice architecture
as a means to change eating behaviour in self‐service settings: A systematic review. Obes
Rev. 14(3) 187-196.
Sniehotta, F.F., J. Presseau, V. Araújo-Soares. 2014. Time to retire the theory of planned
behaviour. Health Psychol Rev. 8(1) 1-7.
Snook, K.R., A.R. Hansen, C.H. Duke, K.C. Finch, A.A. Hackney, J. Zhang. 2017. Change in
percentages of adults with overweight or obesity trying to lose weight, 1988-2014. JAMA.
317(9) 971-973.
Srinivasan, S., M. Vanhuele, K. Pauwels. 2010. Mind-set metrics in market response models: An
integrative approach. J Marketing Res. 47(4) 672-684.
* Steenhuis, I., P. van Assema, G. van Breukelen, K. Glanz, G. Kok, H. de Vries. 2004. The
impact of educational and environmental interventions in dutch worksite cafeterias. Health
Promot Int. 19(3) 335-343.
Sunstein, C.R. 2017. 'Better off, as judged by themselves': A comment on evaluating nudges.
International Review of Economics. In press.
Sutin, A.R., L. Ferrucci, A.B. Zonderman, A. Terracciano. 2011. Personality and obesity across
the adult life span. J Pers Soc Psychol. 101(3) 579.
* Tal, A., B. Wansink. 2015. An apple a day brings more apples your way: Healthy samples prime
healthier choices. Psychol Mark. 32(5) 575-584.
* Tandon, P.S., C. Zhou, N.L. Chan, P. Lozano, S.C. Couch, K. Glanz, J. Krieger, B.E. Saelens.
2011. The impact of menu labeling on fast-food purchases for children and parents. Am J
Prev Med. 41(4) 434-438.
Thaler, R.H., C.R. Sunstein. 2009. Nudge: Improving decisions about health, wealth, and
happiness. Penguin Books, New York.

41
Thapaa, J.R., C.P. Lyford. 2014. Behavioral economics in the school lunchroom: Can it affect
food supplier decisions? A systematic review. Int Food Agribus Man. 17(A) 187-208.
* Thorndike, A.N., J. Riis, L.M. Sonnenberg, D.E. Levy. 2014. Traffic-light labels and choice
architecture: Promoting healthy food choices. Am J Prev Med. 46(2) 143-149.
* Thorndike, A.N., L. Sonnenberg, J. Riis, S. Barraclough, D.E. Levy. 2012. A 2-phase labeling
and choice architecture intervention to improve healthy food and beverage choices. Am J
Public Health. 102(3) 527-533.
* van Ittersum, K., B. Wansink. 2013. Extraverted children are more biased by bowl sizes than
introverts. PLoS One. 8(10) e78224.
van Kleef, E., O. van den Broek, H.C.M. van Trijp. 2015. Exploiting the spur of the moment to
enhance healthy consumption: Verbal prompting to increase fruit choices in a self-service
restaurant. Appl Psychol Health Well Being. 7(2) 149-166.
* Vanderlee, L., D. Hammond. 2014. Does nutrition information on menus impact food choice?
Comparisons across two hospital cafeterias. Public Health Nutr. 17(06) 1393-1402.
Viechtbauer, W. 2010. Conducting meta-analyses in r with the metafor package. J Stat Softw.
36(3) 1-48.
Viechtbauer, W., M.W.L. Cheung. 2010. Outlier and influence diagnostics for meta‐analysis. Res
Synth Methods. 1(2) 112-125.
Walsh, J.W. 1995. Flexibility in consumer purchasing for uncertain future tastes. Marketing Sci.
14(2) 148-165.
Wansink, B. 2015. Change their choice! Changing behavior using the can approach and activism
research. Psychol Mark. 32(5) 486-500.
* Wansink, B., H. Bhana, M. Qureshi, J.W. Cadenhead. 2016. Using choice architecture to create
healthy food interventions in food pantries. J Nutr Educ Behav. 48(7) S35-S36.
Wansink, B., P. Chandon. 2006. Can 'low-fat' nutrition labels lead to obesity? J Marketing Res.
43(4) 605-617.
Wansink, B., P. Chandon. 2014. Slim by design: Redirecting the accidental drivers of mindless
overeating. J Consum Psychol. 24(3) 413-431.
* Wansink, B., A.S. Hanks. 2013. Slim by design: Serving healthy foods first in buffet lines
improves overall meal selection. PLoS One. 8(10) e77055.
* Wansink, B., D.R. Just, A.S. Hanks, L.E. Smith. 2013. Pre-sliced fruit in school cafeterias:
Children's selection and intake. Am J Prev Med. 44(5) 477-480.
Wansink, B., D.R. Just, C.R. Payne. 2012. Can branding improve school lunches? Arch Pediatr
Adolesc Med. 166(10) 967-968.
* Wansink, B., J. Kim. 2005. Bad popcorn in big buckets: Portion size can influence intake as
much as taste. J Nutr Educ Behav. 37(5) 242-245.
* Wansink, B., C.R. Payne. 2007. Counting bones: Environmental cues that decrease food intake.
Percept Mot Skills. 104(1) 273-276.
Wansink, B., C.R. Payne, P. Chandon. 2007. Internal and external cues of meal cessation: The
french paradox redux? Obesity. 15(12) 2920-2924.
* Wansink, B., K. van Ittersum. 2013. Portion size me: Plate-size induced consumption norms and
win-win solutions for reducing food intake and waste. J Exp Psychol Appl. 19(4) 320-332.
* Wansink, B., K. van Ittersum, J.E. Painter. 2006. Ice cream illusions: Bowls, spoons, and self-
served portion sizes. Am J Prev Med. 31(3) 240-243.
* Wansink, B., K. van Ittersum, C.R. Payne. 2014. Larger bowl size increases the amount of
cereal children request, consume, and waste. J Pediatr. 164(2) 323-326.

42
* Webb, K.L., L.S. Solomon, J. Sanders, C. Akiyama, P.B. Crawford. 2011. Menu labeling
responsive to consumer concerns and shows promise for changing patron purchases.
Journal of Hunger and Environmental Nutrition. 6(2) 166-178.
Wertenbroch, K. 1998. Consumption self-control by rationing purchase quantities of virtue and
vice. Marketing Sci. 17(4) 317-337.
Wilson, A.L., E. Buckley, J.D. Buckley, S. Bogomolova. 2016a. Nudging healthier food and
beverage choices through salience and priming. Evidence from a systematic review. Food
Qual Prefer. 51 47-64.
* Wilson, N.L., D.R. Just, J. Swigert, B. Wansink. 2016b. Food pantry selection solutions: A
randomized controlled trial in client-choice food pantries to nudge clients to targeted
foods. J Public Health. fdw043.
Zlatevska, N., C. Dubelaar, S.S. Holden. 2014. Sizing up the effect of portion size on
consumption: A meta-analytic review. J Marketing. 78(May) 140-154.

43
Online Appendix to
“Which Healthy Eating Nudges Work Best?
A Meta-Analysis of Field Experiments”
This online appendix contains the following sections:
Appendix A. Search strategy and flow chart
Appendix B. Publication bias
Appendix C. Subcategory analyses
Appendix D. Interaction analyses

44
Appendix A: Search strategy, keyword selection, and flow diagram
This meta-analysis focuses on articles describing nudge interventions, without restriction on
the population. Specific search terms were developed in accordance with the SPICE (Setting,
Population, Intervention, Comparison, Evaluation) framework (Booth 2006) (see Table A1). We
mainly searched for interventions that involved nudging, choice architecture, or behavioral
economics. We considered all articles published in the English language that reported a nudge
intervention in a field setting. As shown in Table A2, key terms within the SPICE framework were
combined using the Boolean operators “AND” and “OR.”
Table A1: Application of the SPICE framework for keyword selection
SPICE Keywords
Setting Food; eat*; fruit; vegetable; drink; beverage; diet; nutriti*; (un)healthy; calorie
Population None assigned, interested in all populations
Intervention Nudg*; choice architect*; behavioral economics; behavioral intervention
Comparator Field study; field experiment
Evaluation Selection; consumption; sales; choice
Table A2: Specific keywords used in database search using Boolean operators Database Keywords
Science Direct ("food" OR "eat" OR "fruit" OR "vegetable" OR "drink" OR "beverage" OR "diet" OR
"nutriti" OR "calorie") AND ("nudg" OR "choice architect" OR "behavioral economics" OR
"behavioral intervention") AND ("field study" OR "field experiment") AND NOT ("lab
study" OR "lab experiment") AND ("selection" OR "consumption" OR "sales" OR "choice")
PubMed ("food" OR "eat*" OR "fruit" OR "vegetable" OR "drink" OR "beverage" OR "diet" OR
"nutriti*" OR "calorie") AND ("nudg*" OR ("choice" AND "architect*"))
Google Scholar "Nudge behavioral intervention food selection consumption choice"

45
Figure A1 reports the PRISMA (Preferred Reporting Items for Systematic Reviews and
Meta-Analyses, Moher et al. 2009) flow diagram. The search strategy was first applied to three
electronic databases: PubMed, Science Direct, and Google Scholar. The search was initially
conducted in January 2016 and updated on October 2017. Within these first 854 articles, we focused
on intervention-based articles as well as review-based articles. In fact, we found 7 systematic
reviews and 11 meta-analyses on topic. We included in our identification base all 559 references
cited in these review-based articles. Last, we also included 9 other references identified through
other sources. After removing duplicates and references based on titles, we evaluated 223 articles.
Of these, 142 articles were excluded for various reasons (see Figure 1), and 81 articles were
included in the meta-analysis.
Figure A1: PRISMA flow diagram
Records identified through
PubMed (159), Science Direct
(195) and Google Scholar (500) N = 854
Iden
tifi
cati
on
Records identified through
7 systematic reviews and 11
meta-analyses N = 559
Scr
een
ing
Eli
gib
ilit
y
Incl
ud
ed
Records (after duplicates
were removed) screened
based on title N = 1,160
Articles assessed for
eligibility based on
abstract or full text N = 223
Articles included in the
meta-analysis N = 81
N = 142 articles excluded,
reasons for exclusion: N = 18: Intervention type N = 95: Study design N = 19: Outcomes & data N = 9: Paper not available
N = 1: Publication retraction
N = 262 duplicates removed
Records identified
though other sources
(reviewers, colleagues) N = 9

46
Appendix B: Publication bias
In Figure A2, the funnel plot displays each observation as a function of the effect size
(standardized mean difference or Cohen’s d) and the standard error. Several observations appeared
outside of the funnel on the right-hand side, suggesting a potential publication bias.
Figure A2: Funnel plot
First, using Duval and Tweedie’s (2000) trim and fill method (not available for a three-level
analysis), we included 8 missing studies (represented by the white dots in Figure 2), resulting in a
slightly lower estimated effect size (d = .21, se = 0.2, p < .001) than in the unadjusted two-level
analysis (d = .22, se = .02, p < .001). However, both estimated effect sizes are positive, considered
of medium magnitude, and significantly different from zero.
Second, following Viechtbauer and Cheung (2010), we performed sensitivity analyses by
removing 30 (30) observations for which the leverage (Cook’s distance) was more than twice the
average leverage (Cook’s distance) in the overall sample. In both cases, the adjusted effect size is
only slightly lower (respectively d = .27, se = .03, p < .001; and d = .23, se = .03, p < .001) compared
to the original three-level analysis (d = .27, se = .03, p < .001).
0
0,1
0,2
0,3
0,4
0,5
0,6
-2 -1 0 1 2
Sta
nd
ard
err
or
Standardized mean difference (Cohen's d)

47
Figure A3: P-curve
Third, we also produced the p-curve (Simonsohn et al. 2014b) for all effect sizes included
in our sample. As shown in Figure F3, the p-curve is strongly right-skewed (p < .001) and indicates
the presence of evidential value. Note that 119 out of 277 effect sizes (43%) were not significant.
A closer examination of non-significant effects shows that only 16 out of 81 articles (19%)
published only non-significant results, 31 papers (38%) published significant and non-significant
effect sizes (e.g., the effect size is significant for fruits but not significant for vegetables) and 31
papers (38%) published only significant results. Using the procedure presented in Simonsohn et al.
(2014a), we also estimated the corrected p-curve effect size on the sample of 158 significant effect
sizes. The corrected effect size estimated through bootstrap (d = .21, se = .03, p < .001) was lower
than the “naïve” estimate on the 158 significant effect sizes without the p-curve correction (d = .39,
se = .03, p < .001), and lower than the “earnest” overall average effect size including all observations

48
(d = .27, se = .03, p < .001). Last, the p-curve effect size is similar to the average effect size from
the overall model including all observations and covariates (d = .22, se = .04, p < .001). All four
estimates are positive, considered of medium magnitude, and significantly different from zero.
Last, in light of the criticisms regarding some of the studies conducted by the Cornell
Food and Brand Lab (Robinson 2017) included in this meta-analysis, we added to the multivariate
model a binary variable controlling for the 32 observations originating from this lab. This variable
was highly insignificant (p = .75). Moreover, we do not include Wansink et al. (2012) in our
meta-analysis because the paper was recently retracted. Including the study would not affect the
results in any way.

49
Appendix C: Subcategory analyses
In Table A3, we report the estimates for the multivariate model using the detailed
categorization for intervention type. On average, the estimates of effect sizes are 12% lower in the
multivariate analysis than in the univariate ones.
Table A3: Estimates for detailed intervention types Univariate Multivariate Difference
k d se d se Raw Percent
Cognitive interventions
Descriptive labeling 31 .05 .06 .05 .09 -.01 -17%
Evaluative labeling 34 .14* .06 .13* .06 -.01 -6%
Salience enhancements 25 .19* .08 .10 .08 -.09 -46%
Mixed: Cognitive only 23 .15* .06 .18* .08 .02 14%
Affective interventions
Healthy eating cues 35 .32* .06 .25* .07 -.07 -21%
Sensory cues 12 .29* .10 .22* .10 -.07 -23%
Behavioral interventions
Convenience enhancements 56 .41* .05 .33* .06 -.08 -18%
Plate & portion size changes 17 .71* .09 .55* .10 -.16 -22%
Mixed interventions
Mixed: Cognitive present 37 .20* .07 .24* .08 .04 20%
Mixed: Cognitive absent 7 .29* .10 .25* .11 -.04 -14%
Weighted average 277 -.04 -12% *p < .05

50
Appendix D: Interaction analyses
The multivariate model shown in equation 7 and Table 4 does not lend itself to interaction
analyses because it already requires estimating 16 coefficients. Adding interactions would require
estimating more than 30 coefficients, which would quickly exhaust the available degrees of
freedom, especially for some combinations with few or no data. Hence, we added interactions to a
simplified model with only one coefficient for each of the 8 types of predictors. Essentially, we
recoded or grouped categories together to provide a single (linear or binary) coefficient per
predictor.
Simplified model. First, we used linear coding for intervention type (-1 = cognitive, 0 =
affective, and 1 = behavioral). We included the mixed interventions into the cognition-affect-
behavior categorization according to the first stage that they sought to influence. Hence, mixed
interventions including at least one cognitive intervention (“mixed: cognitive present”) were
included among cognitive interventions. Mixed interventions excluding a cognitive one (“mixed:
cognitive absent”) were included among affective ones (no study used a mixed intervention of
behavioral nudges). We also used a linear coding for outcome measure (-1 = total eating, 0 = healthy
eating and mixed eating, and 1 = unhealthy eating), while healthy and mixed eating were grouped
together because of a small difference in effect sizes (see Table 2). Third, location was ANOVA
coded (-½ for grocery stores vs. ½ for onsite or offsite cafeterias), while offsite and onsite locations
were grouped together because of a small difference in effect sizes (see Table 2). Fourth, study
design was ANOVA coded (-½ for pre-post and ½ for single and double difference), while single
and double difference were grouped together because of a small difference in effect sizes (see Table
2). The rest of the variables were unchanged; that is, outcome behavior (selection vs. consumption),
age (children vs. adults), and country (other vs. US) were ANOVA coded, while duration was
measured in weeks and mean centered.

51
Results. We first estimated a model with only main-effects (Model 1). Its 𝑅2 decreased only
slightly compared to the model with the categorical coding reported in the main text (from .46 to
.44), and none of the hypotheses tests changed. To examine when each type of intervention is most
effective, we included an interaction term between intervention type and all the other predictors.
Table A4 shows that the effects of intervention type are stronger 1) for consumption than for
selection, 2) for adults than for children, and 3) in the US than in other countries.
Table A4: Interactions analyses
Model 1 Model 2
Predictor 𝜷 se 𝜷 se
Constant .21*** .04 .20*** .04
Intervention type (cognitive to affective to behavioral) .12*** .03 .10* .05
Outcome behavior (selection vs. consumption) .02 .04 .05 .04
Outcome measure (total to healthy/mixed to unhealthy) .11*** .03 .08* .04
Population setting (cafeterias vs. grocery stores) .13* .06 .09 .07
Population age (adults vs. children) .04 .05 .07 .04
Population country (US vs. other) .11* .05 .13** .05
Study duration (duration in weeks, mean centered) -.002 .001 -.004 .003
Study design (single & double difference vs. pre-post) .12** .04 .09* .04
Outcome behavior × intervention type .14** .05
Outcome measure × intervention type -.02 .04
Population setting × intervention type -.06 .07
Population age × intervention type .16*** .05
Population country × intervention type .16** .06
Study duration × intervention type -.003 .003
Study design × intervention type -.01 .05
K (observations) 277 278
N (studies) 87 87
𝑅2 44% 56%
LR test vs. intercept-only model 65*** 87***
***p < .001, **p < .01, *p < .05.

52
References
Booth, A. 2006. Clear and present questions: Formulating questions for evidence based practice.
Library hi tech. 24(3) 355-368.
Duval, S., R. Tweedie. 2000. Trim and fill: A simple funnel‐plot–based method of testing and
adjusting for publication bias in meta‐analysis. Biometrics. 56(2) 455-463.
Moher, D., A. Liberati, J. Tetzlaff, D.G. Altman, P. Group. 2009. Preferred reporting items for
systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6(7)
e1000097.
Robinson, E. 2017. The science behind smarter lunchrooms. PeerJ Preprints. 5 e3137v3131.
Simonsohn, U., L.D. Nelson, J.P. Simmons. 2014a. P-curve and effect size: Correcting for
publication bias using only significant results. Perspect Psychol Sci. 9(6) 666-681.
Simonsohn, U., L.D. Nelson, J.P. Simmons. 2014b. P-curve: A key to the file-drawer. J Exp
Psychol Gen. 143(2) 534.
Viechtbauer, W., M.W.L. Cheung. 2010. Outlier and influence diagnostics for meta‐analysis. Res
Synth Methods. 1(2) 112-125.
Wansink, B., D.R. Just, C.R. Payne. 2012. Can branding improve school lunches? Arch Pediatr
Adolesc Med. 166(10) 967-968.

















![Irving Chernev[1]](https://img.dokumen.tips/doc/110x75/55cf8fc2550346703b9f883c/irving-chernev1.jpg)