Embed Size (px)
Citation preview

WHY THIS BORING TOPIC
Intake of Sick Newborn – at the mercy of neonatologist.
Small amount of fluid can make a big difference.
Fluid Overload - may lead to NEC, PDA, CLD.
HOW WET ARE THE NEWBORN
TBW - 0.7 L/kg in Newborn
0.6 L/kg at 1yr. Age
ECF 40% - Newborn
20% - Older Children

WHO REQUIRE FLUID Infant < 30 wks. & <1250 gm.
Sick Term Newborns
- Severe birth asphyxia
- Apnoea
- RDS
- Sepsis
- Seizure

HOW MUCH FLUID TO BE GIVEN <1 kg 1-1.5 kg. >1.5 kg.
1st day 100 ml/kg. 80 ml/kg. 60 ml/kg.
7th day 190/ml/kg 170 ml/kg 150 ml/kg.
increase 15 ml/kg/day upto 6th day
Add 20 ml/kg/day for Phototherapy & Warmer.
All calculation done on birth wt. till body wt. exceeds birth wt.
Fluid if prematures nursed in Plastic heat Sheild

WHAT FLUID
1st 48 hrs. <1 kg - 5% Dextrose
1-1.5 kg. - 10% Dextrose
>1.5 kg. - 10% Dextrose
After that ISO – P Na+ - 20 mEq / lit
K+ - 20 mEq / lit
Cl - 25 mEq / lit
D - 5%
25ml 25% D+ 75ml
ISO – P Na+ - 22.7 mEq / lit
K+ - 18 mEq / lit
Cl - 22 mEq / lit
D - 10%

LESS FLUID
Birth asphyxia
Meningitis
Pneumothorax
IVH
PDA
CLD
2/3 of Maintenance

EXTRA FLUID
NEC & other condition with loss in 3rd space
May require upto 200ml / kg – repeated 10ml / kg RL/NS bolus.
ELBW / VLBW neonates – Due to high IWL.

KEY POINTS TO REMEMBER IN FLUID THERAPY
Term – 1% Per day
Allow a wt. Loss
Preterm – 2% Per day
1st 48 hrs – no electrolyte required
Replace Gastric fluid loss ½ NS + KCL
Other body fluids NS + KCL
Give fluid direction 8-12 hrly in sick neonates

Premature 1.25 kg. day 1 give fluid direction
10% Dextrose
80 ml / day
20 ml 6 hourly
10% Dextrose 3.5ml / hr = 3 drops / min
A 3 kgs., term sick newborn on 4th day under radiant
warmer & phototherapy, calculate fluid requirement
ISO – P
315 ml + 60 ml + 60 ml = 435 ml
108 ml / 6 hrs.
18 ml / hr. = 18 drops / min.

ELECTROLYTE REQUIREMENT
A. SODIUM :
Add -from day 2 - 3
In VLBW add when lost 6% wt.
Require - Term & LBW 2 - 3 mEq / kg / day
ELBW 3 - 5 mEq / kg / day

ELECTROLYTE REQUIREMENT….
B. POTASIUM :
Add - from day 3
can wait till serum K+ < 4 in small
prematures
Require - 2 - 3 mEq / kg / day

ELECTROLYTE REQUIREMENT....
C. CALCIUM : Give to IDM
Preterm
Birth asphyxia
<1500 gm.
Add from day 1.
36-72 mEq / kg / day
or
4- 8 ml / kg / day of 10% Cal. gluconate

GLUCOSE REQUIREMENT
Optimum requirement 4-6 mg / kg / min
Conc. Used - 5%, 10%, 12.5% (max)
Glucose infuse – (mg / kg / min) = % Gx rate (ml / hr.)
x 0.167 x wt.
Thumb rule – 3 ml / kg / hr of 10% D = 5mg / kg / min
Remain careful about glucose in – LBW
IDM
IUGR

GOALS OF FLUID ELECTROLYTE THERAPY
Urine output 1 – 3 ml/kg/hr.
Allow a weight loss 1 – 2% / day in 1st wk.
(weigh the splint before putting i/v line)
Absence of Edema / Dehydration / Hepatomegaly
Urine Sp. gravity 1005 - 1015
Euglycaemia - 75 – 100 mg / dl
Normonatremia - 135 - 145 mEq / lit
Normokalemia - 4 – 5 mEq / lit

MONITORING FLUID ELECTROLYTE THERAPY Check Daily - Definitely
Wt. - loss > 3% - dehydration
<1% over dehydration
Urine output <1 ml / kg / hr – dehydration or SIADH
(Hourly) >4 ml / kg / hr. – overhydration / dieresis
Napkin weight technique
Collect in syringe from cotton
Urine specific gravity >1015 fluid deficit
(each sample if possible) <1005 fluid overload
Blood Glucose
Clinical Signs

MONITORING FLUID ELECTROLYTE THERAPY …...
Check Daily --- if possible
Serum Na+
Serum K+
Blood Urea
Serum Creatinine




Peripheral lines: Indications & Purpose
• Maintain fluid, electrolyte & acid-base balance in neonate
• Provide IV medications.
• Provide blood or blood components.
• Provide peripheral parenteral nutrition.
• N B: do not try > 2consecutive times by the same person !

Preliminary stepsSteps Rationale
Assemble cleansing supplies, 2 ml syringe filled with N.Saline, over the needle cannula, fixing tapes, cotton, assistant.
Minimises time and hastle. Syringe should be pre-filled.
Prepare neonate after initial stabilization with the help of assistant
Prevents unexpected needle prick or tear of the vein.
Universal asepsis after wash and gloves Prevent nosocomial infections.
Clean local area with alcohol , iodine and alcohol.
Prevents local phlebitis and sepsis.
Ensure skin stretched , but not taught. Prevents rolling of vein, but not flushed

Insertion of Line
Steps RationaleSelect a site in the vein as distal as possible.Insert the needle slowly at 30-40* angle with bevel up. After piercing bring it to skin level.
To keep the proximal vein for future use. Reduce angle of the needle to prevent piercing the vein.
Blood flow observed back in the set. A gentle suck with prefilled syringe may be tried.
If no blood comes, draw needle back and try keeping the tip beneath the skin.
Thread the cannula over the needle forward and remove the stylet after the cannula is advanced .Never reinsurt the needle into the canula
Prevent the cannula emboli as needle may puncture or tear it. Prevents piercing the vessel wall.
Fix with occlusive transparent dressing over the cannula. Wedge cotton fluff under the cannula before fixing.
Leave connection site exposed. Stabilizes needle. Allows slight elevation which helps flow.
Stabilize arm.Start fluid. Settle neonate. Document time, site, size,drugs, fluids & sign.
Protection from accidental dislodgement.
Monitoring & Discontinuation• Observe rate,
patency ,air within the line.
• Observe for local warmth, pain,leak redeness ,edema, blanching.
• Flush with 2 ml N.Saline (with asepsis) if needed to check the line.
• Indication : on order / leak / phlebitis / thrombosis / blanching (except with ionotrope infusion).
• Stop fluid / asepsis / remove dressings / remove cannula / press until bleeding stops / dress with iodine.
• Send cannula tip for culture if phlebitis.

Umbilical venous line• Purpose : Central line for medication, exchange
transfusion, pressure monitoring and fluid (rarely)• Policy : Should be done by a doctor only.• Emphasis : Tip in ductus/IVC, do not advance
once secured, do not keep open, very careful about sepsis.
• Equipment : 5Fr for < 3.5 kg; 8Fr for > 3.5kg.( It should have side holes at tip ), forceps, scalpel,probe, suture, drapes, asepsis utensils, tapes, ties etc. )

UVC Procedure• Estimate length of the catheter(graph), assemble
equipments• Universal asepsis.• Identify UV( patulous, single, bleeding, at 12
o’clock) / grasp cord with toothed forceps / remove clots from vein by iris forcep
• Introduce fluid filled catheter with stop cock 2-3 cm inside vein / suck for blood / remove clot if no free flow of blood /remove, rotate & reinsert until free flow comes / advance to desired length
• Fix UVC once free flow established with tapes. Radiology confirmation (D9-D10 or just above right diaphragm).

Capillary Blood Sampling
• Purpose : heel prick blood sampling
• Emphasis : safe and effective / maxm. 2 pricks per heel (except sick newborn).
• Policy : preferably doctors/ only trained nurse.
• Indications : sugar / blood gas / Hct / sepsis screen / bilirubin / biochemistry.
• Equipment: asepsis utensils, lancet, capillary tubes, gauze.

Procedure of CBS• Ask sister to bundle the neonate. Chose the site
(picture). Warm the area with dry warm cloth.• Universal asepsis. Perform lancet puncture in most
medial or lateral aspect of plantar surface (avoid puncture on previous or previous weight bearing sites of the neonates).
• Discard first drop of blood / hold the site downward / keep gentle continuous pressure /avoid ‘milking’ / Collect in capillary tube /
• Stop bleeding by pressure / apply Iodine / label each tube / send with details quickly / document all details.
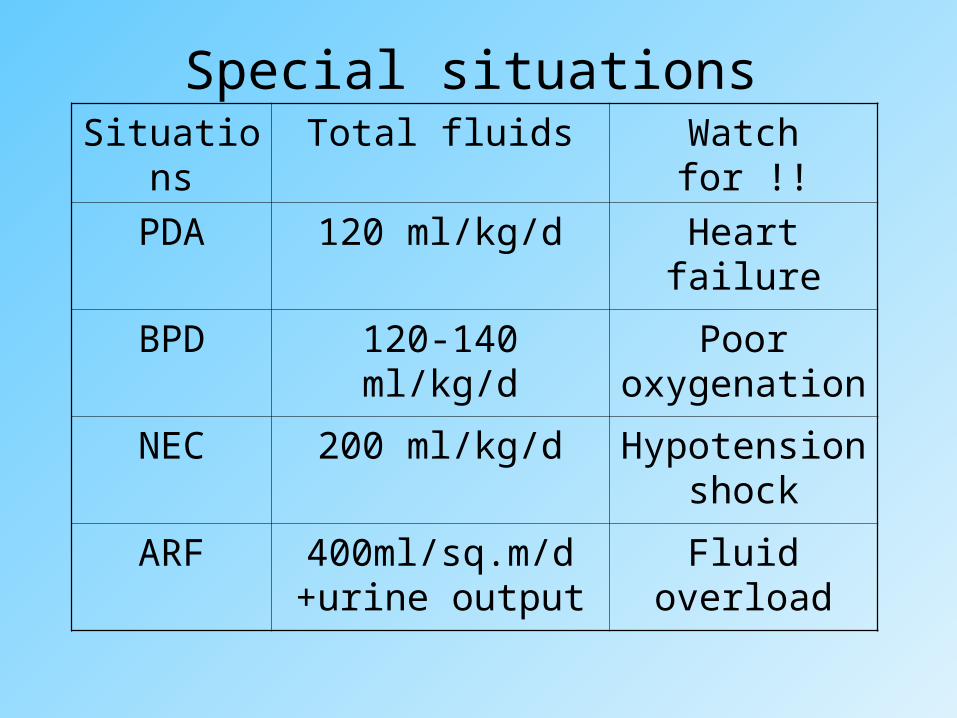
Special situationsSituations Total fluids Watch for !!
PDA 120 ml/kg/d Heart failure
BPD 120-140 ml/kg/d Poor oxygenation
NEC 200 ml/kg/d Hypotension shock
ARF 400ml/sq.m/d +urine output
Fluid overload

CASE
1250 gm. 26 wk. Premature, intubated & Ventilated
dev. apnoea on day 5 started i/v aminophylline
day 15 Switched to oral theophylline
day 20 on EBM 150 ml/kg
day 28 Na+ 133 mEq / lit, K+ 4mEq / lit urine output 2-4 ml / kg / hr
Day 30 Na+ <100 mEq / lit , serum osmola 204 mosm / lit
Urine Sp gr. 1040.
From 28 –30th day gained wt. 25 gm / day despite a fall of
Urine vol from 3 ml / kg / hr. 0.5 ml / kg / hr
Diagnosis
Management

CASE….
- A 30 yrs Woman P2+o taken to labour room
- In last 1 hr of labour woman drunk 3L water + received
5% D i/v
- Delivered male baby 3kg, apgar 18 59
- after 6 hrs. the baby dev. Seizure
What is the most likely cause of seizure?
How to prevent this?

HYPONATREMIA
Serum Na+ <130 mEq / lit
Neurological Signs or Na+ <120 mEq / lit
treat promptly
What to give :
3% Nacl 0.5 mEq Na+ / ml
2 – 3 ml /kg initial dose
use 3% Nacl to raise Na+ upto 125 mEq / lit
NaHco3 7.5% solution 0.9 mEq Na+ / ml
(if 3% Nacl not available)
HYPONATREMIA…….
How to calculate deficit
Na+ deficit (mEq) = (desired Na+ - obs Na+) x wt x 0.6
Add next 2 days daily requirement 2-3 mEq / kg / day
correct in 48 hrs.
Thumb rule - correct 1/3rd 8hr
1/3rd 16 hr
1/3rd 24 - 48 hr.

Male baby of 7 days wt. 1.5 kgs., serum Na+ obs. 122 mEq. / lt.
How to correct the hyponatremia ?
Deficit of Na+ = (135 – 122) x 1.5 x 0.6 = 11.7 mEq.
Maintenance Na+ = 3 x 1.5 x 2 (correction made in 48 hrs.)
= 9 mEq.
Total requirements = 11.7 +9 = 20.7 mEq. = 21 mEq.
Fluid requirements for 48 hrs. = 1.5 x 150 x 2 = 450 ml.
21 mEq Na+ in 450 ml. fluid = 50 mEq. Na+ in 1 lit.
Fluid required = 450 ml. N/3 Solution.

HYPERNATREMIA
Serum Na> 150 mEq / lit
Excess free water loss than Na+
Do not treat with Na+ free water
Fluid therapy -- 2/3 maintenance with N2 / N5 sol. + 5% D.
-- correct Na+ over 24 – 48 hrs. Do not drop >10 mEq / lit / day.
-- May require 3% NaCl if over correctionleads to CNS signs.

SIADH
Predisposing factors present
Feature wt. Gain with out oedema
hypotonic hyponatremia
Urine output
Urine osmolality > plasma osmolality
Treat Water restriction – 2/3 maintenance x 24 hrs
3% Nacl if Na+ <120 mEq / lit or CNS sign
Frusemide Urinary electrolyte free H2o
excretion

HYPOKALEMIA
A Newborn 3kgs on 2nd day developed abdominal distension, NG tube inserted, on 3rd day Serum K+ observed was 2.1 mEq / lit. How to correct.
K+ deficit = (Req K+ - obs K+) x body wt.
3
= (3.5 - 2.1) x 3
3
= 1.4 mEq

HYPOKALEMIA ………
Max K+ i/v without ECG - monitoring – 40 mEq / lit = 2ml 1.5ml KCL / 100ml of Fluid.
Max K+ i/v with ECG – monitoring – 60 - 80 mEq / lit
Signs of hypokalenia in newborn – ileus
Obtundation
QT / ST depression

HYPERKALEMIA
Serum K+ > 6 mEq / lit
How to manage
1. Check Sampling error and Recheck Value
2. Remove all sources of K+
3. Upto 7mEq / lit Kayexelate 1gm / kg at 0.5gm / ml of NS given as enema (upto 1- 3 cm) minimum retention time = 30 min.

HYPERKALEMIA….
4. K+ > 7 mEq / lit - Co – gluconate 1- 2ml / kg over 5 min
- NaHCo3 1 – 2ml / kg slowly
- 2ml / kg of 10% D + 0.05 units / kg regular insulin followed by – infusion
- Kayexelate
- Salbatatnoe Nebalisation 4mcg / kg
5. If above measure fails
Peritoneal dialysis
Exchange transfusion
ECG Tall T / PR / QRS

Solution Concentration Available from Equivalents
Soda bicarb solution
7.5% 10 ml ampoule 1 ml = 1 mEq of HCO3 + 1 mEq of Na
Potassium Chloride 15% w/v 10 ml ampoule 1 ml = 2 mEq of K
Calcium gluconate 10% w/v 10 ml ampoule 1 ml = 9.3 mg of Cal.
Magnesium sulphate
50% and 25% 2 ml ampoule If 25% Mg 4.15 mOsm/dL
Sodium Chloride 3% 10 ml ampoule
50 ml bottle
1 ml = 0.5 mEq of Na
25% Dextrose 25 w/v 25 G/100 ml 10 ml ampoule and
25 ml ampoule
50% Dextrose 50 w/v 50 G/100 ml 25 ml ampoule
Commercial electrolyte and dextrose stock sol.

Dextr. Na K Cl Lactat Ca mOsm/L
G/L
Isotonic NS 154 154 308
RL 131 5 111 29 2 270
½ isotonic ½ NS 77 77 154
Electrolyte free solution
5% 50 278
10% 100 556
Dextrose, electrolyte solution
5% DNS 50 154 154 585
D5 ½ NS 50 77 77 415
D5 0.33% NaCl
50 57 57 381
D5 0.2% NaCl
50 34 34 347
Ped. Maint. Isolyte P 50 25 20 22 368
Composition of commercial I.V. fluid available

HYPOCALCAEMIA
Serum Calcium <7.0 mg / dl Ionised Cal <4.0 mg / dl
Seizure
Treatment of Hypocalcaemic Crisis apnoea
Tetaxy
1 – 2ml Ca-glu. / kg + 5 - 10% D 10ml over 10 min.
No response in 10min REPEAT DOSE
Maintenance Cal 8ml / kg / day x 48 hrs.
Switch to oral therapy

HYPOCALCAEMIA ………
Refactory hypocalcaemia think hypomagnesaemia 0.2ml of 50% mgso4 2 doses 12hr. Apart i/v or deep im
Caution in Ca++ therapy
Rapid i/v infusion - dysrythmia / bradycardia
Extravasation of Ca++ Solution S/C necrosis & Calcification

Thank U





























