Embed Size (px)
Citation preview

Why the New Hypertension Guidelines Matter
Putting Them Into Practice
Topics in the Tropics 2018
07 December 2018

Robert Jay Amrien, PA-C
Founding Program Director & Clinical Associate Professor Bryant University School of Health Sciences
Clinical Physician Assistant
Massachusetts General Hospital

Disclosure
American Heart Association Council on Hypertension
Organizational Reviewer, 2017 AHA/ACC Guideline for High Blood Pressure in Adults
Board, AHA Southern New England
American College of Cardiology
Cardiovascular Team Member
Legal Consultant

Fair Winds & Following Seas
Dr. Martin J. Nemiroff, M.D. USPHS 16 December 1940 - 28 November 2018
President George H.W. Bush
12 June 1924 – 30 November 2018
In memory of 2403 lives lost in Pearl Harbor on this day 77 years ago

Objectives
Discuss hypertension as a critical disease in the US Understand how the new guidelines came into place, and why they are necessary Understand the role of every provider in recognizing and treating hypertension

This talk brought to you courtesy of:
6

7
How many of you are familiar with the 2017 AHA/ACC Hypertension
Guidelines?
8
Which beta blocker should be used to treat hypertension?

9
You have newly diagnosed a patient with hypertension. What is the first
line medication you should prescribe?
Definition A progressive cardiovascular syndrome with many causes that results in both functional and structural changes to the heart and vascular system.
http://www.ash-us.org/about_hypertension/index.htm

"A man's health can be judged by which he takes two at a time - pills or stairs." -Joan Welsh

Epidemiology 2018
Centers for Disease Control
•Prevalence: •46% if the population •Increased from 31% under new guidelines
•80% know they have hypertension •Improved from 70%
•73% are prescribed medication •Improved from 60%
•47% are controlled on medication (US Only) •Includes non-compliance •Improved, especially in ACO model v. Fee for Service
12
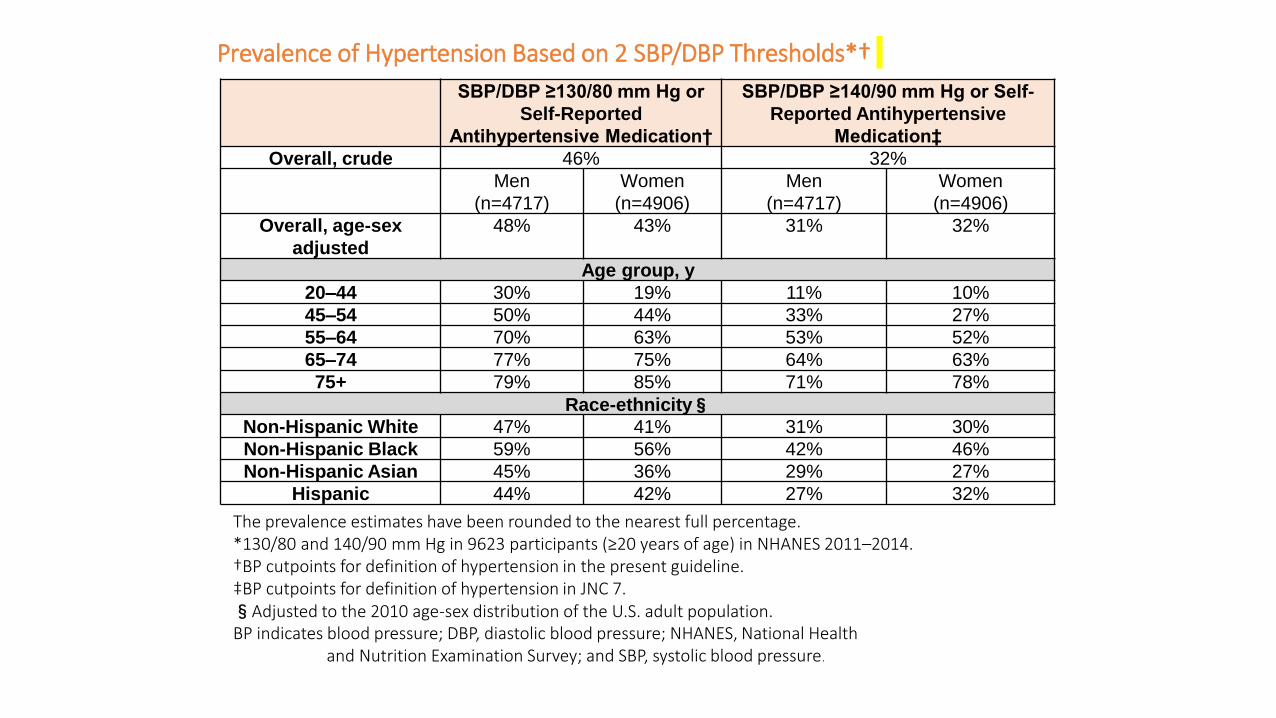
Prevalence of Hypertension Based on 2 SBP/DBP Thresholds*†
SBP/DBP ≥130/80 mm Hg or
Self-Reported
Antihypertensive Medication†
SBP/DBP ≥140/90 mm Hg or Self-
Reported Antihypertensive
Medication‡
Overall, crude 46% 32%
Men
(n=4717)
Women
(n=4906)
Men
(n=4717)
Women
(n=4906)
Overall, age-sex
adjusted
48% 43% 31% 32%
Age group, y
20–44 30% 19% 11% 10%
45–54 50% 44% 33% 27%
55–64 70% 63% 53% 52%
65–74 77% 75% 64% 63%
75+ 79% 85% 71% 78%
Race-ethnicity§
Non-Hispanic White 47% 41% 31% 30%
Non-Hispanic Black 59% 56% 42% 46%
Non-Hispanic Asian 45% 36% 29% 27%
Hispanic 44% 42% 27% 32%
The prevalence estimates have been rounded to the nearest full percentage. *130/80 and 140/90 mm Hg in 9623 participants (≥20 years of age) in NHANES 2011–2014. †BP cutpoints for definition of hypertension in the present guideline. ‡BP cutpoints for definition of hypertension in JNC 7. §Adjusted to the 2010 age-sex distribution of the U.S. adult population. BP indicates blood pressure; DBP, diastolic blood pressure; NHANES, National Health and Nutrition Examination Survey; and SBP, systolic blood pressure.

Epidemiology
Centers for Disease Control
•Prevalence confounders: •Increased prevalence
•Black Americans: 34% •Decreased control
•Mexican Americans •Men •Elderly (>65) •Lack of PCM
•Better control •Insurance •PCM with continuity of care (medical home!)
14

History
ESH Guidelines 2018 *AHA/ACC Guidelines 2017* JNC 8: Published 2013 JNC7: published 2003 (ALLHAT) JNC6: published 1997 JNC 5: published 1992 JNC 4: published 1988 JNC 3: published 1984 JNC 2: published 1980 JNC 1: published 1976 (NHANES)
15

Epidemiology
Centers for Disease Control
•Other facts to consider: •Up to 5% of children and adolescents have primary hypertension •Hypertension is the most common cause for an office visit in non-pregnant adults
16

17

Etiology
18

Why we treat?
LVH Heart Failure
Ischemic Stroke Intracerebral Hemorrhage
Ischemic Heart Disease Chronic Kidney Disease
19

Classification
20
Normal: Less than 120/80 mm Hg; Elevated: Systolic between 120-129 and diastolic less than 80 Stage 1: Systolic between 130-139 or diastolic between 80-89 Stage 2: Systolic at least 140 or diastolic at least 90 mm Hg Hypertensive crisis: Systolic over 180 and/or diastolic over 120

Classification
Pediatrics: HTN: >95th percentile value for age, height & gender
Pre-HTN: >90th percentile value for age, height & gender
21

“…the risk of cardiovascular disease doubles with every 20mmHg increase in systolic blood
pressure…”
22

Secondary Hypertension
Renal • RAS (atherosclerosis, FMD) • RPD (DM, Renal Cystic Disease)
Adrenal • Cushing’s • Pheochromocytoma • Hyperaldosteronism
Medications • NSAIDS, OCPs, Ephedrine, MAOI
Others: • Pregnancy, Coarctation of the aorta, OSA, Thyroid disease
ETOH, Drugs
23

White Coat Hypertension
“Legitimate” diagnosis ICD9: 796.2 (no ICD 10)
Definition: clinic BP >140/90 on 3 occasions, less than 140/90 on 2 non-clinic visits Increased risk of progression to hypertension No proven increased risk in cardiovascular mortality or stroke Increased lifestyle modifications, yearly follow up No medications! 24

Masked Hypertension
No ICD 10
Definition: Normal clinic BP with elevated ambulatory BP Up to 10% of general population Usually diagnosed after high home BP Increased EOD, CV mortality, Stroke
25

Ambulatory Monitoring
• Required for dx in NICE guidelines • White coat hypertension • Masked Hypertension • Drug resistance • Hypotensive symptoms • Episodic dysfunction
May improve patient compliance This is a mainstay of the new guidelines
26

Ambulatory Monitoring
A 24 hour mean of 125/75 A daytime (awake) mean of 130/80 A nighttime (asleep) mean of 110/65
27

Self Monitoring ”Giving the patient power over their disease process is likely
to have better results.”
28

Home BP Testing
29
Screening
• USPSTF
• Screen all adults aged 18 and over • Annual for normal readings • Semi-annual for high risk or elevated BP
• AAP:
• Screen children over 3 annually in conjunction with routine health care
30

Diagnosis
Diagnosis: • Elevated blood pressure on at least two separate
occasions (unless EOD) • Ideal settings • Multiple readings
• Consider secondary causes
• Document: • Elevated blood pressure without diagnosis of
hypertension (ICD10 R03.0) • Pre-Hypertension • Compelling indications
31

Diagnosis
Elevated: What should we do? • 120-129 systolic
• MISSED OPPORTUNITY ALERT
32

Diagnosis
Diagnosis: • BP repeated:
• Manual cuff • Baumanometer • Both arms (on the first visit) • Consider lower extremity • Ambulatory BP monitoring
33
Risk Factors Hypertension
• Genetics
• Family History
• Environment: • Inactivity
• Stress
• Obesity
• Tobacco
• Age
• Menopausal meds
• High NA Diet
• ETOH

Evaluation
Work up: • Complete history & focused physical examination
• Concentrate on end-organ-damage • Risk factors • Secondary causes • Erectile dysfunction
• Labs: CBC, BMP, Lipid Panel, UA • Other labs for secondary causes (TSH) • 12 lead ECG • 10 year ASCVD risk score
• Always ask:
• OTC Medications (NSAIDS) • OCP • ETOH/Drugs
35

Evaluation
36
http://tools.acc.org/ASCVD-Risk-Estimator-Plus/#!/calculate/estimate/

Evaluation Work up:
http://ecg.bidmc.harvard.edu/maven/dispcase.asp?rownum=49&ans=1&caseid=240
37

Evaluation
Work up:
• Other considerations • Urine microalbumin • Urine albumin to creatinine ratio • Lab: TSH, HgA1C, secondary causes • CXR • Echocardiogram • Ambulatory BP Monitoring • Fundoscopic exam
38

Evaluation
Work up:
The ideal blood pressure reading: • Patient seated for 5 minutes
• Feet flat on floor • Arm supported at heart level
• Appropriate sized cuff for patient • At least two readings • Ideally ½ hour after eating, drinking or tobacco • Empty bladder
39

Evaluation
40

Management
ACC/AHA
41

42

Management
Lifestyle Modifications • No trials on hard outcomes (just numbers)
• Dose and time dependent • Everyone should be encouraged despite numbers
• Evidence suggests
• Delayed onset of hypertension • Cost effective • Good for overall cardiovascular health
• Individual results may vary
43

44
Management
Lifestyle Modifications
Weight Reduction: 5-20 mm Hg per 10kg • Goal BMI <25 kg/m2
45

DASH Eating Plan: 8-14 mm Hg • 8 weeks • 8-10 servings per day • Low fat dairy • Reduced fat & cholesterol
Management
Lifestyle Modifications
46

Management
Lifestyle Modifications
Cal: 4210 Fat: 228 Na: 6545 1930 mg
3000 mg
47

48

Management
Lifestyle Modifications
Dietary Sodium Reduction: 2-8 mm Hg • Conflicting evidence • Risk reduction in non-hypertensive patients • Less than 1.5 gm per day (Na)
49

50

Management
Lifestyle Modifications
Physical Activity: 4-9 mm Hg • 30 minutes a day most days of the week
51

Management
Lifestyle Modifications
52

Management Lifestyle Modifications
53

The Push away plan!
National Cholesterol Education Program (Adult Treatment Panel III Guidelines)

Management
Lifestyle Modifications
Moderate Alcohol Consumption: 2-4 mm Hg • <2 drinks per day for males • <1 drink per day for females
55

Management
Other Lifestyle Modifications
• Smoking cessation • Patient education • Relaxation/Meditation
Lifestyle modifications!
Stop all the bad stuff & start all the
good stuff!!!
56

Management
Other Lifestyle Modifications
57

Management
Other Lifestyle Modifications
Actigraphy

Management
Renal Denervation: • Simplicity 3 no long term benefit
• SPYRAL HTN-ON MED underway
59
Management
Stretch Break!
60

Management
Other Lifestyle Modifications
61

Management
Other Lifestyle Modifications Avoid NSAIDS Consider stopping OCP Avoid cough and cold medication, especially long term
62

63

Current Management
Pharmacology
Compelling indications are no longer a consideration. Treat hypertension as hypertension & confounding diseases as their own entity
64

Current Management
Pharmacology
65

*Management*
Pharmacology
Stage I: Lifestyle Modifications and/or Pharmacologic Monotherapy Lifestyle modifications are the mainstay of treating Stage 1 HTN Consider pharmacologic therapy for Stage 1 HTN if: • Established cardiovascular disease • Type II Diabetes Mellitus • Patients over 65 years old • *An estimate 10 year risk of ASCVD of at least 10%*
Caution in patients over 75 or CVD risk over 10% but no CVD Withhold in the very frail or end of life
66

Management
Pharmacology
Stage I: Pharmacologic Monotherapy Low doses of • ARB • ACE • DHP CCB • Diuretic
67

Management
Pharmacology
Stage I: Monotherapy • Diuretic/ACE/ARB
• <55 yo • Non-black
• CCB • >55 • Black
68

Management
Pharmacology
Stage II: Dual Therapy • Diuretic (chlorthalidone) + DHP CCB (amlodipine) • ACE1/ARB + DHP CCB (amlodipine) • ACE1/ARB + diuretic (chlorthalidone) Treatment failures on two drug therapy
• ACE1/ARB + DHP CCB + Diuretic
NO ACE1/ARB/Aliskiren combinations 69

Management
Pharmacology
Resistant or Difficult to Treat Hypertension • Add aldosterone antagonist (spironolactone or eplerenone) Then consider direct vasodilator
70

Management
Pharmacology
Others: • Direct Vasodilators • Aldosterone Antagonists • Non Dihydropyridine CCB (bradycardia) • Alpha Blockers (syncope) • Centrally acting medications (clonidine) • Direct Renin Inhibitor • Loop diuretics • Methyldopa (pregnant)
71

Management
Pharmacology
Combination pills improve tolerance
• Sequential monotherapy: • Start one medicine @ low dose • Consider only one dose increase • If treatment failure, stop medication and
switch class • Try ACE1, ARB, amlodipine, chlorthalidone
72

Management
Pharmacology
Goals: <130/80 Consider <140/90 if hypotensive, symptomatic, or complications Consider <150/90 if frail elderly or over 80
• Accept higher systolic to maintain diastolic*
73

Management
Pharmacology
• Focus on BP reduction! • All first line drugs confer the same
outcomes • Evidence based • Specific drug effect! • Compelling indications in line with BP
reduction
74

Management
Pharmacology
• Drugs trump lifestyle modifications • Lifestyle modifications still imperative • Medications confer: • 35-40% stroke reduction • 20-25% MI reduction
• NNT: 100 patients for 5 years to prevent 2 CV mortalities
75

Management
Pharmacology
• “2 or 3 medications at lower doses have better hypertension reduction with less side effects”
76

Management
Pharmacology
• Consider using 1 antihypertensive at night. Especially in patients who are on 3 or more medications.
• Dippers vs. Non-Dippers
77

78

Follow up
Patients should be followed monthly until BP is at goal. Once goal is met, patients should be followed quarterly to semiannually. One lifestyle modification should be discussed at each visit. Motivational interviewing
79
Children & Adolescents
No clear guidance from AAP, AHA FOCUS ON LSM Consider secondary causes in all! Refer (most do well on ACE1 and CCB)
80

Children & Adolescents
• Childhood obesity and hypertension are on the rise.
• All children over three years of age who present for medical care should have their blood pressure checked using an appropriately sized cuff. • Measurement is also appropriate in certain younger
children.

Children & Adolescents
• Hypertension is diagnosed based on repeat measurements (on three or more separate occasions) that are at the 95th percentile or higher for age, height, and sex.
• Children are considered pre-hypertensive if their blood pressure reached the 90th percentile, and in adolescents, blood pressure over 120/80 mm Hg is considered prehypertension no matter what percentile he or she reaches

Children & Adolescents
• LIFESTYLE MODIFICATIONS!
• Prevention is the key factor.
• Weight loss • Smoking cessation • Increased fruits, vegetables, fiber, and low-fat dairy in
the diet • Limited salt.
• These recommendations are family-centered and apply
to prevention as well as treatment

Children & Adolescents
• ACE Inhibitors • Angiotensin Receptor Blockers • Calcium Channel Blockers • Diuretics

Take Home Messages
85
Take Home Messages
1. Focus on recognizing patients with hypertension 2. Make the diagnosis! 3. Don’t hesitate to order an echocardiogram for LVH
• Look for all End Organ Damage 4. Get your patient to goal!
• <130/80 • Focus more on the numbers • ACE1, DHP CCB, Thiazide, ARB
5. Avoid BB and most Non-DHP CCB
6. Don’t miss an opportunity!
86

Take Home Messages
!!!Getting your patient to goal is the standard of care!!!
Your reimbursement will be tied to success
Patients want to comply & are more willing to do so with an invested provider! Education is imperative! HTN does not hurt (until it becomes substernal crushing chest pain, the worst headache of their life, or when the left side of the body becomes numb!
87
Take Home Messages
“LIFE STYLE MODIFICATIONS are a must for children. Eliminating Hypertension in the future should based on the elimination of risk factors and early application of life style
modifications”
88

Thank you for your attention & thank you for all of the hard work you put forth in taking the best care of your patients!
89

90