Embed Size (px)
Citation preview

WHO’S WATCHING THE KIDS?
BASIC PEDIATRIC TRAUMA

Michael J. Allshouse, DO, FACS, FAAP
Medical Director
Pediatric Surgery and Trauma Program Valley Children’s Hospital
2017 TUCKER REDFERN PEDIATRIC TRAUMA SYMPOSIUM


I have nothing to disclose

Financial Disclosure: I have nothing to disclose… No financial conflict of interest


WHAT’S NEW FROM THE COT AND ATLS?

PEDIATRIC SURGERY AND ITS ROOTS IN TRAUMA HALIFAX HARBOR EXPLOSION OF A CANADIAN MUNITIONS SHIP RESULTED IN NUMEROUS SERIOUS INJURIES. WILLIAM LADD, MD, LED A GROUP OF AMERICAN PHYSICIANS WHO TRAVELED TO HELP WITH THE FIRST D.M.A.T. DR. LADD LATER INITIATED THE FIRST PEDIATRIC SURGICAL PROGRAM. TODAY, ROUGHLY 75% OF NORTH AMERICAN PEDIATRIC SURGEONS CAN TRACE THEIR PROFESSIONAL LINEAGE TO THAT PROGRAM.

LITTLE HUMANS CAUSING BIG PROBLEMS FOR SOCIETY
• 3 BILLION DOLLARS IN LIFETIME MEDICAL COSTS
• 30 % DROP IN CHILDHOOD DEATHS 2000 – 2009 BUT STILL, > 9000 KIDS DIE EACH YEAR
• 25 DEATHS/ DAY – AGRICULTURE RELATED DEATH EVERY 3
DAYS • 37% OF ALL POST INFANT CHILDHOOD
DEATHS • 47% OF THE YPLL

Pediatric Trauma is an Epidemic
• 12,000 children and teenagers will die as the result of injury – > 60% of all pediatric deaths – For every child who dies, 40 more are
hospitalized and 1120 are treated in EDs
• 50,000 children suffer permanent disabilities each year, most of which are the result of head injuries
• $16 billion are spent annually caring for injuries to children between birth and 16 yrs
Children’s Safety Network, 1996

National & Global Injury Burden
• In US, 12,000 deaths annually – 30 children per
day • >150,000 hospitalizations • 10 – 20% result in permanent disability • Worldwide, each year about 875,000 children are
killed • There are 10 to 30 million non-fatal injuries
globally



Gentlemen, Rest your sphincters!

Mechanism of Injury
• Blunt
• Penetrating

Blunt

Blunt wounding mechanism
• Lap belts, seat belts
• Fists and feet
• Handlebars
• Large angry bovine and equine beasts

Penetrating

How Big is the Problem of penetrating injury?
• 10% of most major pediatric trauma center admissions
• Up to 7% are GSW’s • NTDB 2003 had penetrating mechanism as 20%
of all injuries and led to 20% of deaths in those < 19 years old
• Overall lethality roughly 3X that of blunt mechanism

Wounding Mechanism
• GSW – highest mortality. 10 deaths/day in USA • Shotgun • Air rifles – you can put more than your eye out • Knives • Impalement • Foreign bodies – ingested and inserted • Non accidental trauma • Recreational equipment

RISK FACTORS FOR PEDIATRIC INJURY
• Poverty • Frequent family household moves • Single parent • Household crowding • Other siblings • Child aggression, impulsiveness, ADHD • Poor maternal health – physical and mental • Marital discord • Child abuse and neglect • Inadequate adult supervision linked to 43% of deaths
in Alaska and Louisiana studies

Who is at risk?
• Males – biology, risky behavior, gender socialization, cognitive
• Socioeconomic status more important than race or ethnicity
• Exposure to hazardous activity or environmental circumstances

The INFAMOUS “Y” CHROMOSOME SOURCE OF “FRAGILE Y SYNDROME”

CHILDHOOD INJURY
• PREDICTABLE
• PREVENTABLE – C. EVERETT KOOP MD, 1985:
• “ MOST INJURIES TO PEOPLE, AND NEARLY ALL INJURIES TO CHILDREN, CAN BE PREDICTED AND CAN BE PREVENTED.”

J. CAIRNS SCIENTIFIC AMERICAN 1985
• “The ONLY intervention ever known to reduce the aggregate mortality for a disease – any disease - at a population level was PREVENTION”

BENJAMIN FRANKLIN
“ IN THE FIRST PLACE, AS AN OUNCE OF PREVENTION IS WORTH A POUND OF CURE, I WOULD ADVISE ‘EM TO TAKE CARE HOW THEY SUFFER LIVING COALS IN A FULL SHOVEL, TO BE CARRIED OUT OF ONE ROOM INTO ANOTHER, OR UP OR DOWN STAIRS, UNLESS IN A WARMINGPAN SHUT; FOR SCRAPS OF FIRE MAY FALL INTO THE CHINKS AND MAKE ON APPEARANCE UNTIL MIDNIGHT; WHEN YOUR STAIRS BEING IN FLAMES, YOU MAY BE FORCED, (AS I ONCE WAS) TO LEAP OUT OF YOUR WINDOWS, AND HAZARD YOUR NECKS TO AVOID BEING OVEN-ROASTED.”

HOW ARE WE DOING SO FAR?
• Baldwin et al. “ While child injury death rates declined by 29% from 2000 to 2009, annual number of deaths (9143 in 2009) remains unacceptably high.
• On the rise: suffocation (UP 54%), poisoning (UP 50% - prescription drugs), ATV’s, bounce houses
• Overall injury rates down close to 50% according to SAFEKIDS
• LOWEST DEATH RATES = MA AND NJ < 5 per 100,000
• HIGHEST = MS AND SC > 23 per 100,000

TRAUMA IN CHILDREN WITH DISABILITY What is the problem? • Injury is the leading cause of death in young
people between the ages of 1 and 18. • Approximately 8% of US children are classified
as disabled – As high as 20% of children <18 y.o. have a chronic
physical, developmental, behavioral or emotional condition requiring greater than usual level of health related services!
» Newachek PW et al Pediatrics 1998

Who is at Greatest Risk?
• Disabled children perceived as less valuable and without feelings
• Study ranking order of “acceptability” of disabilities: – Cognitive impairment and CP = least – Blind, speech defect, seizures, LD = medium – Amputations and cognitively competent in
wheelchairs = Most acceptable

Trimodal distribution of trauma related death
• 1st Peak: CNS, Central vasculature injury – Solution = prevention
• 2nd Peak: CNS mass lesion, SOI, Chest injury
– Solution = Resuscitation, definitive care, ATLS
• 3rd Peak: less common in kids. Death from MODS rare. Long term disability is not

Importance of prehospital care
• Injury adjusted death rate for children 2X that for adults
• Survival OOH cardiac arrest ½ that of adults • ET intubation failure as high as 50% • Trauma is the most common reason for
ambulance transport but is <10% of total paramedic volume in most metropolitan regions
• Helicopter over triage is 18 – 20 %

PHYSICAL STIGMATA OF CHILD MALTREATMENT

Background: Golden Hour
• Small infants and children – Platinum half-hour – Initial period of stability is significantly
shorter as age decreases • Primary survey
– Life-threatening events identified and treated
• Resuscitation phase • Secondary survey
– Examination from head to foot • Tertiary examination
– Rehabilitation needs

Mechanism of Injury: effects on injury patterns
Mechanism Patterns of Injury MVC unrestrained multiple trauma, head,
neck air bag head, neck, facial,
ocular restrained torso, head, neck,
spine


Anatomy : Pediatric versus Adult
• Proportionally larger and heavier head • Weaker and underdeveloped neck musculature • Higher center of gravity
– Pediatric : C2-C3 – Adult: lower cervical vertebrae
• Greater elasticity and laxity of ligaments in children
• More horizontal orientation of facet joints

Anatomic Variants in Children
• Airway size, caliber and length • Head/neck size and relationship to airway • Bony thorax • Mediastinum and great vessel mobility • Lung parenchyma • Heart

Physiologic difference too…
• Diminished FRC
• Rapid deoxygenation with apnea
• Increased oxygen consumption
• Rapid development of hypoxemia

Head and Neck Injuries
• TBI is the most common cause of death and in children.
• PTOS study – Kids with ISS > 15 had lower dependency scores
for feeding, locomotion, social interaction and expression categories if treated at PTC compared to ATC AQ

Unique anatomic features of children: effects on injury patterns
• Head – head size is
disproportionately larger – skull and scalp thinner
reduction in head size relative to body size

Injuries Unique to Children
• Central Nervous System – Most common isolated
system injured – The leading cause of
death among injured children
– Principal determinant of outcome
– Mortality from spinal fractures 54.5% in children vs. 20.5% in adults

Injuries Unique to Children
• Thoracic Injuries
– Second leading cause of death in childhood trauma
– Isolated thoracic injuries are relatively uncommon
– Significant intrathoracic injury may exist in the absence of external signs of trauma

Unique anatomic features of children
• Chest – increased flexibility – decreased
ossification – not well
muscularized – permits greater
energy transfer to internal organs

Unique anatomic features of children
• Abdomen – organs are larger,
exposed
– abdominal wall is thinner providing less protection
– reduced perinephric fat

Injuries Unique to Children
• Abdominal Injuries – Abdomen begins at the
nipple in children
– Rib cage does not provide adequate protection
– Underdeveloped abdominal muscles
– A minor force may result in a serious injury
– Relatively high incidence of liver and spleen injuries

Unique anatomic features of children
• Extremities – bones immature and flexible – fx at sites of weakness =
cartilagenous growth plates
fx may be present without deformity

Pelvic Fracture can be Life Threatening
pelvic ring disruption
expanding hematoma
iliac a. bleeding

Unique anatomic features of children
• Skin – surface area greater
in children relative to size and weight
at risk for hypothermia
which mimics hypovolemic shock

Unique anatomic features of children
80-90% of visceral injury due to blunt trauma
and the site of occult blood loss

Unique anatomic features of children
• Spinal Column – high energy transfer with
• axial loading of spine or • extreme flexion /extension
– weak muscles, ligaments lax
young: high cervical fx
adolescent: low cervical fx

What makes children vulnerable?
• Age pattern • Communication skills • Inability to protect themselves • Anatomic and physiologic differences
– Abdominal wall musculature – Lack of protection of visceral contents – Delay in seeking care

Initial Trauma Assessment: ABCDE
• Airway – obstruction
• soft tissue • blood • vomit • loss of reflexes
– immobilize c-spine
Children = increased lymphoid tissue, floppy tongue,
and subglottic narrowing predispose to obstruction

Initial Trauma Assessment: ABCDE
• Breathing – look, listen, feel
• loss of CNS drive – head injury – intoxication
• restriction – rib fractures
• chest injury – pulmonary
contusion – pneumothorax

Hypoxemia
• PaO2/FiO2 < 150 • PaO2 < 60 – 65 or SaO2 < 90% • Apnea or cyanosis • Really a relative term
–The injured brain initially needs all of the oxygen it can get

Initial Trauma Assessment: ABCDE
hildren = significant injury can occur in absence of visible traum



Initial Trauma Assessment: ABCDE
• Circulation – Assessment of
end organ perfusion
• level of consciousness
• skin / cap refill – Heart rate – Blood pressure Children = hypotension is an ominous finding

Primary Survey: ABCs
• A: Airway – Inability to establish and maintain a patent airway is
the most common cause of cardiorespiratory arrest
• B: Breathing • C: Circulation
– Assessing the circulation and obtaining hemorrhage control
– A rapid and accurate assessment of hemodynamic status is essential prior to further secondary evaluations

Background: Children
• Significant physiologic reserve
– Normal blood pressure even after sustaining significant blood loss
• Maintain cardiac output
– Reflex tachycardia
– Peripheral vasoconstriction
• Compensated Shock 0
20
40
60
80
100
120
140
160
0 25 50 75
Percent blood volume deficit
Perc
ent o
f con
trol
Vascular resistance
Blood pressur
e
Cardiac
output

Background: Blood Loss / Shock
• Blood volume of a child
– 80 mL/kg
• Loss of > 25% can cause shock
– 20 mL/kg
– Signs of shock
• Heart rate levels off after 35 - 45% of blood volume loss
– Compensatory mechanisms fail
– Tachycardia Bradycardia
– Hypotension
– Irreversible shock
0
20
40
60
80
100
120
140
160
0 25 50 75
Percent blood volume deficit
Perc
ent o
f con
trol
Vascular resistance
Blood pressur
e
Cardiac
output

Circulation: Hemorrhage Control
• External sources of blood loss
– Direct pressure
– No hemostats • Internal blood loss (occult)
– Chest
– Abdomen
– Long bone fractures
• Surgery is indicated if hemodynamic normality cannot be restored or maintained

Circulation: Response to Resuscitation
• Slowing of heart rate
• Increased pulse pressure
• Return of normal skin color
• Increased warmth of extremities
• Clearing of sensorium
• Increased systolic blood pressure
• Increased urinary output – 2cc/kg/hr in infants – 1cc/kg/hr in adolescents

Hypotension
• Age Dependent –Generally speaking… –70 + (age in years x 2) is the lowest
acceptable systolic pressure –Median (50th Percentile) SBP for
children older than 1 year: 90 + (2 x age in years)

Initial Trauma Assessment: ABCDE
• Disability – AVPU
• Alert • Verbal responsive • Pain responsive • Unresponsive
– Avoid 20 brain injury • oxygen, fluid resuscitation
– Avoid 20 spinal cord injury
• spine immobilization

Initial Trauma Assessment: ABCDE
• Exposure – Identify other major injuries – Control sites of bleeding – Splint Fractures
• Avoid hypothermia
– reduced body temperature impairs
• cognitive function • organ function • coagulation
– maintain temperature >360

The Secondary Survey: CNS
• Head injury most common • Classification
GCS 13-15 mild GCS 9-12
moderate GCS 3-8 severe
• CT scan indicated: – Abnormal GCS – History of loss of
consciousness > 5 min regardless of repeat GCS
• Actions: avoid secondary brain injury – Oxygen, fluid resuscitation – GCS<8 = maintain airway – +/- mannitol (1gm/kg)

TO CT OR NOT TO CT? LESS THAN AGE 2

OVER AGE 2…

The Secondary Survey: C-spine
• Spine injury should always be assumed until proven otherwise
• If head injury present,c-spine can only be cleared radiographically
• In the awake patient, suspect injury if: – guarding, stiffness, pain – tenderness, lateralizing
deficit
• Actions: – Immobilize c-spine – Do not remove helmet

C-spine Fracture is Potentially Lethal
0
20
40
60
80
100
C1-C3 C4-C7 Mortality0-4 years 5-9 years10-14 years 15-18 years

Epidemiology of pediatric cervical spine injury: Age
• Mean age is 8-9 years old, 2:1 male to female • < 8 years old mainly, ligamentous injuries • > 8 years old mainly fractures • Infants under 1 year old with Cervical Spine
Injuries are rare, HOWEVER, they are probably more common in NAT than we originally suspected. Be suspicious

Mechanism
• MVC • Pedestrian struck • Falls • Struck • Hanging/clothesline injury • Sudden hyperextension/flexion • Violent cough, dog lifting, water sports

Who should be screened for cervical CV injury?
• Hemorrhage from mouth, nose ,ears or wounds with potential arterial origin
• Expanding cervical hematoma • Cervical bruit • Cerebral infarction on CT • Unexplained neuro exam, Horner’s, atypical
neuro exam (syndromic cord injury pattern: e.g. Brown-Sequard)

Screening, cont’d
• Asymptomatic – Severe hyperextension/rotation or flexion,
especially with displaced midface or mandibular fracture
– Near hanging – Seatbelt mark

Screening for Vertebral artery injury
• Cervical spine fractures – Subluxation – Fractures extending into the transverse foramen – Upper cervical involvement

The Secondary Survey: Chest
• Significant force can be transferred to intrathoracic structures
• Rib fractures or soft tissue trauma is an ominous finding
• Actions: – Administer Oxygen – ? Pneumothorax
• needle thoracostomy

Chest Injury is Potentially Lethal
0
10
20
30
40
50
Lung PTX/HTX Rib Rx Mediastinum
FrequencyMortality

ED Thoracotomy
• Reserved for two categories of injured children
– Penetrating thoracic trauma and no vital signs in the ED
– Blunt injuries with loss of vital signs in the ED
Beaver et al, J Pediatr Surg, 1987

Thoracic Trauma Strata of Severity
• Immediate death – Cardiac rupture, commotio cordis, aortic rupture with
decompression • Quick death
– Tension pneumothorax, airway obstruction, massive hemothorax, cardiac tamponade, massive air embolism
• Delayed – MOSF/ARDS, Tracheobronchial injury, pulmonary
contusion

Cardiac Injury
• Blunt injury in children is Uncommon • ECHO, Troponin I • Air embolism
• COMMOTIO CORDIS
– Sudden, forceful blunt chest impact leading to dysrhythmia and sudden death

Penetrating Thoracic Trauma
• Vast majority treated by chest tube alone – < 15% require thoracotomy/sternotomy
• CXR is the fundamental examination – Mark entrance and exit sites
• 6-hour rule – Upright CXR after 6hrs with no PTX makes the
likelihood of delayed PTX or occult injury vanishingly small
• Open pneumothorax – Sucking chest wound – Occlusive dressing fixed on 3 sides – Chest tube

Frequency of Thoracic Injuries
Type of Injury Blunt (%) Penetrating (%)
Pulmonarycontusions/lacerations
53 29
Pneumothorax/hemothorax 38 64Rib/sternal fractures 36 8Cardiac 5 13Diaphragm 2 15Major blood vessals 1 10
Cooper et al, J Pediatr Surg, 1994

Musculoskeletal Thoracic Injury
• Rib fractures are indications of high kinetic energy injury
• Markers of severe injury – Greater than 2 ribs, <2 y.o.
• Location and type of fracture give clues to the etiology
• First, second ribs, scapula, sternal, spine fractures all are worthy of intense eval.
• Flail chest is rare in children

Pitfalls in Diagnosis of PTX
• Mainstem intubation
• Lumenal obstruction
• Gastric distention
• Diaphragmatic disruption

TENSION PNEUMOTHORAX AND FLAIL CHEST


Pulmonary Contusion
• Probably the most common thoracic injury in kids • Vehicle passenger restraints reduce prevalence • Lower rate of associated bony injury, HTX or
great vessel injury than in adults • Compliant chest wall efficiently transmits energy
to the lungs • CT is VERY sensitive at identifying these injuries • > 30% lung involvement increases risk for
mechanical ventilation support.

Pulmonary Contusion

Traumatic Diaphragmatic Rupture



Injury to the Diaphragm
• Rare injury in children • Blunt force trauma, Lap-Belt injury, some
penetrating • Blunt injury
– 2/3 are on the Left side – Liver and spleen injuries in 75%
• Diagnosis – CXR, CT, Missed in 40-50% during acute eval

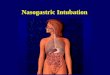
Traumatic Asphyxia
• Kids run over by cars • Closed glottis • Valveless great veins
in chest and neck • Associated chest
injury in 58%, fractures in 34% and abdominal injury in 11%
• CNS manifestations

Traumatic Asphyxia
• Unique injury to children related to compliance of the chest wall
• Dramatic physical presentation
– Cervical and facial petechial hemorrhages – Craniocervical cyanosis associated with
vascular engorgement – Subconjunctival hemorrhage
• Good prognosis

Traumatic Asphyxia
• Most commonly the result of blunt compressing thoracic trauma
– Sudden airway obstruction, closure of glottis – Abrupt retrograde high pressure in SVC
• Common associated injuries
– CNS – Pulmonary contusions – Intra-abdominal injuries
Gorestein et al, J Pediatr Surg, 1986


The Secondary Survey: Abdomen
• Abdominal Injury – 5% of children admitted
with blunt injury mechanism
– Risk Factors • High energy • Seat belt • Unexplained Shock • CNS injury, Pelvic
Fracture – Examination
• abdominal tenderness • hematuria

Mechanisms for Intra-abdominal Trauma
1. Motor vehicle collisions 2. Automobile vs pedestrian accidents 3. Falls 4. ATV 5. Handlebar injury from bicycle 6. Sports 7. Non-accidental trauma

CT is the imaging study of choice in the hemodynamically stable child
Splenic Laceration

CT is the imaging study of choice in the hemodynamically stable child
Liver
Laceration

CT is the imaging study of choice in the hemodynamically stable child
Renal
Injury

CT is the imaging study of choice in the hemodynamically stable child
Hollow Visceral Injury

CT is the imaging study of choice in the hemodynamically stable child
Pancreatic Transection

Take an Unstable Child to CT?

Who needs a CT abdomen?
• No abdominal wall trauma or seat belt sign • GCS > 13 • No abdominal tenderness • No thoracic wall tenderness
– Again the importance of anatomic characteristics • No c/o abdominal pain • No decreased breath sounds • No emesis • PECARN STUDY SAYS NO CT RECOMMENDED

Frequency of Pediatric Blunt Abdominal Injuries
• Spleen 27%
• Kidney 27%
• Liver 15%
• Pancreas 2%

Solid Organ Injury
• Treatment
• > 90% of hemodynamically stable pts successfully managed non-operatively
• Less than 10% require transfusion

AAST Splenic Injury Scale
17-yo boy injured on an ATV. Grade I injury with subcapsular fluid occupying less than
10% of spleen’s surface area.

AAST Splenic Injury Scale
17-yo girl injured in an MVC. Grade II injury with laceration involving less than 3 cm of
parenchymal depth

AAST Splenic Injury Scale
16-yo boy injured playing hockey. Fractured spleen involving more than 25%,
Grade IV splenic laceration

AAST Splenic Injury Scale
12-yo boy pedestrian struck by MV. Fractured spleen with hilar
devascularization. Grade V injury.

Splenic Trauma
• Complications • Pseudoaneurysms
• Often asymptomatic and resolve over time
• If treatment required, angiographic embolization may be used
• Also occur in liver trauma
A. Splenic pseudoaneurysm (arrowheads) after nonoperative treatment of blunt
splenic injury.
B. Successful angiographic embolization The microcatheter
used to deploy the coils is marked by the arrowheads and the embolic
coils are marked by the arrows.

Splenic injury
14 year old male, stepped on by a 1500 lb bull Chest protector

Contrast Blush - Spleen
• 216 Pts – 7 yrs
• 26 Pts – Contrast blush on CT scan
• Lower HgB
• More likely to need op (22% vs 4%) • Not a definite indication for operation, but indicates subset of pts who
have active bleeding and may need transfusion and/or operation
Blunt Splenic Injury

APSA Guidelines
CT GRADE I II III IV Days in ICU None None None 1 day Hospital stay 2 days 3 days 4 days 5 days Predischarge imaging
None None None None
Postdischarge imaging
None None None None
Activity restrictions
3 weeks 4 weeks 5 weeks 6 weeks
From Stylianos S, and APSA Trauma Committee: Evidence-based guidelines for resource utilization in children with isolated spleen or liver injury.
APSA guidelines for hemodynamically stable children with isolated spleen or liver injury
J Pediatr Surg 35:164-169, 2000

• Prospective study all pts with BSLI • No exclusions
• Bedrest : Grade I – II inj – 1 night Grade III – V inj – 2 nights
J Pediatr Surg 46:173-177, 2011

Prospective Study - BSLI
• 131 pts (spleen only 72, liver only 55
• 1 splenectomy (Grade V inj)
• Transfusions – 24 (18 due to BSLI)
• Mean injury grade – 2.6
• Mean bed rest – 1.6 days
• Need for bed rest limiting factor in duration of hospital in 86 pts (66%)
J Pediatr Surg 46:173-177, 2011

Prospective Study – BSLI
An abbreviated protocol of 1 night for Grade I – II
injuries and 2 nights for Grade III or higher in
hemodynamically stable pts is safe and significantly
decreases hospitalization c/w previous APSA
recommendations.

Liver Trauma
• Blunt trauma is most common cause of injury to liver
• High risk due to:
• Large organ, friable parenchyma, ligamentous attachments

Contrast Blush - Liver
• 105 pts – blunt liver injury – 6 yrs • 75 pts – Grade III – V
• 22 pts – Contrast blush • transfusion req.
• mortality (23% vs 4%) • ISS also
• Mortality may be related to the other injuries

Indication for Intervention
• Operate for continued blood loss with hypotension, tachycardia, decreased urine output, decreasing Hg unresponsive to IVF and pRBC
• Operative rates • 3-11% for multiple injuries
• 0-3% for isolated liver injury
• Angioembolization – not used as commonly as in adults

• 72 pts • 30 – Liver
• 44 – Spleen
• Liver vs spleen –
• Longer recovery period
• Nine complications
• Greater use of resources
J Pediatr Surg 43:2264-2267, 2008

Why does NOM fail?
• Shock • Peritonitis • Bleeding • Intestinal injury
– Delay does not typically impact outcome • Pancreatic injury • Diaphragmatic injury


NOM failure Conclusion
• WHO fails: not many. Age and gender don’t matter, pancreas and grade do
• WHAT predicts: bicycle, hypotension, non-responder, high ISS, low GCS
• WHEN do they fail: earlier than adults… typically within the first several hours
• WHERE?: Non pediatric TC, no pediatric surgeon
• WHY: bleeding, peritonitis, pancreatic, intestinal, NOT delayed hemorrhage, lack of protocol

Non Operative Management of BAT
• It works. Uses less blood and is safe. • Age is irrelevant • Delayed operation is not detrimental • Failure most common in the first 12 hours • Failure rates: Kidney 3%, liver 3%, spleen 4%,
pancreas 18% • Bicycles are tough on the pancreas

THE SEAT BELT MECHANICS OF INJURY: ABDOMINAL WALL, VISCERAE AND SPINE

Seat Belt Complex
• Abdominal wall ecchymosis should increase suspicion for blunt intestinal injury as well as injury to the spine
• Triad of lap-belt ecchymosis, intestinal rupture, and Chance fracture of the spine is well-documented – Chance fracture: Fracture of the lower
thoracic or lumbar spine • Oriented transversely through the vertebral
body • Produced by a flexion-distraction mechanism
• Some trauma surgeons advocate the seat-belt complex mandates abdominal exploration without further evaluation due to the risk of intestinal injury
Reid et al, J Trauma, 1990
Sivit et al, AJR, 1996


Lapbelt trauma to sigmoid colon

Laparoscopic view of small bowel injury

Chance fracture FRACTURE THROUGH THE PARS INTERARTICULARIS IN CHILDREN, IT MAY NOT BE A CLASSIC FRACTURE OFTEN A LIGAMENTOUS INJURY MUST BE CONSIDERED UNSTABLE UNTIL ADVANCED IMAGING AND SPINAL SURGEON CONSULTATION

MVC with lapbelt complex
• 12 year old rear seat restrained passenger
• High speed deceleration injury
• Severe abdominal pain and thoracolumbar tenderness

Fixing the Chance fracture

Lap belt complex

Sitting in Auntie’s lap, with the belt across both.

Multiple bowel injuries and renal vascular pedicle injury

Duodenal rupture
16 year old male Calif HS Bull riding champ

DC continued
• Prolonged TPN • External drainage • Gradual resumption
of diet • Slow but steady
improvement. • Nearly 7 week
hospital stay

CT imaging

Handlebars
• Perforation • Transmural injury vs partial thickness • Acute abdominal wall disruption and hernia • Vehicle types
– 60% bicycles – 25% motorcycles – 9% scooters – 4% ATV – 2% others: jet skis, sleds, etc

HANDLEBAR IMPACT MARK


13 year old bicycle handlebar injury. No Free air
Thickened
terminal ileum
surprise!

Duodenal injury
• Penetrating: GSW or stab – Treatment depends on status of pancreas, bile
duct and portal venous injury • Blunt: punch, lap belt, bull, horse, recreational
equipment – Handlebar injury: pancreas vs intestinal
• Severe pancreatico duodenal injury may require exclusion or even pancreaticoduodenectomy (trauma Whipple operation).
• Duodenal hematoma resolves spontaneously in about 2 weeks. BAT vs EGD

Duodenal injury pearl
• Duodenal injury in the very young child, < 2 years old is ALMOST always non accidental trauma.

2 year old kicked by horse First CT No free air

Horse kick Expensive air

16 year old bull rider

5 year old fell on the monkey bars

Duodenal perforation blunt monkey bar impact
Expensive air

BB GUN

Shotguns

Anorectal penetrating injury

NPTR Data
• Head injury remains the major co-morbidity. – The combination of head injury with blunt
abdominal in NAT increases mortality 9 fold per NPTR data.
• Child maltreatment/NAT causing blunt abdominal injury results in 6 fold increased death rate compared to other mechanisms.



Densmore et al.
• KID (Kids Inpatient Database) • Pediatric discharges from community, nonrehab
hospitals • 27 participating states • 2784 hospitals • AHA “universe” of 4839 facilities • 79,673 pediatric injury cases

Case demographics
0-10 y, ISS>15 All patients
Number 7856 79,673
Age (SD) 3.9 +/- 5.0 y 12.2 +/- 6.2 y
Sex 38:62 F:M 31:69
Mean ISS 19.5 +/- 9.6 7.4+/- 7.6
Mean total charges (SD)
$24,435 +/- 59,015 $15,383 +/- 30,494

Site of Care NACHRI designation
0 to 10 y, ISS > 15 (%) All patients (%)
Children’s Hospital 26.8 10.7
Children’s Unit 38.1 23.5
Adult Hospital 35.1 65.8

Outcome by site of care
Mortality (%) LOS > 8 d (%) Charges> $15,000 (%)
A. 0-10 y, ISS>15 Children’s Hosp 4.9 16.8 33.3 Children’s Unit 9.1 25.5 42.2 Adult 7.4 17.7 34.7 B. All patients Children’s Hosp 0.9 8.9 20.2 Children’s Unit 2.4 17.2 32.4 Adult 1.4 9.7 22.2

Mortality differences for injury types by site of care
Fractures (%) Intracranial (%) Internal inj. (%) A. 0-10y, ISS>15 CH 4.7 6.4 1.6 CU 6.9 12.5 8.1 AH 5.2 11.5 5.0 B. All patients CH 0.7 2.7 0.3 CU 1.5 8.5 3.2 AH 0.9 4.9 1.9

Big Picture
• 93 Million admissions from NIS and KID 1988 through 2005
• 2,087,915 surgical admissions in the US • Overall mortality 0.85% • Highest mortality:
– Craniotomy for trauma (26.27%) – Multiple significant trauma (10.69%) – Liver/ Int Tx (11.12%), heart tx (10.94%)

Multivariate results

Future Directions
• Educate • Disseminate APSA, AAP, AAST guidelines • Encourage inclusive, cooperative systems • Transfer agreements • Identify the highest risk groups and injury
patterns • Commitment to research and PI

9th Edition ATLS Circulation
• Blood volume – 70-80 ml/kg
• Transfuse earlier • Vascular access
priority – PIV x 2 – IO – Fem – EJ – cutdown

9th Edition ATLS HEAD INJURY
• Avoid hypoxemia and hypotension • Persistent emesis or Seizure: CT imaging • Options
– Hypertonic saline – Mannitol – Antiepileptic (Keppra vs phenytoin) – ICP monitoring

9th Edition ATLS IMAGING
• Limit CT imaging – ALARA: AS LOW AS REASONABLY
ACHEIVABLE – Do Not scan if planning transfer
• FAST
– Adjunct to physical exam – Not sole diagnostic to rule-out intraabdominal
injury

9th Edition ATLS changes
• Airway – Oral airway
insertion – Cuffed tubes, all
ages • Cuff pressure
monitor – NO NT intubation – LMA option

Radiation Risks
• DLP = dose length product • 5 fold increase use in CT imaging • Risk of leukemia, brain, thyroid and GI
malignancy • Delays definitive care in some cases • Increased Cost • Increased exposure • “Image Gently” • One CT c-spine = 80 chest x-rays

Military lessons learned
• MASSIVE TRANSFUSION PROTOCOLS
• TXA • TOURNIQUET • SPINE
IMMOBILIZATION – VACUUM

Tourniquets in children
• Iraq and Afghanistan • 88 inured kids age 4 – 17 • 67 extremity injuries • Extremity AIS 2 – 4 • 93 % survival • Standard combat application tourniquet • Pediatric concerns
– Skin breakdown, increased ischemic time – Compartment syndrome – Time > 2 hours has increased limb loss risk

COMBAT ACTION TOURNIQUET

MASSIVE TRANSFUSION AND PEDIATRICS
• NATIONWIDE CHILDRENS HOSPITAL – MTP policy 2009 – Goal 1:1:1 ratio
• Results: 55 patients – FFP:PRBC RATION OF 1:3 – No difference in mortality – Decreased thromboembolic events
» J Groner. J Trauma and Acute Care Surg OCT
2012

TXA IN PEDIATRICS
• Cardiac experience with AMICAR • Scoliosis • Craniofacial reconstruction • Traumatic hyphema • Not much published data in pediatric trauma
– PED-TRAX: Joint Theater Trauma Registry • TXA use was independently associated with
decreased mortality • ? Prehospital use



References 1. Cairns J : Treatment of diseases and the war against cancer. Scientific American 1985:253(5) 51-59. 2. Quinlan K. Et al. Using focus groups in pediatric injury prevention research. J Trauma Supp 2007, S6. 3. Haddon WJ. The changing approach to the epidemiology, prevention and amelioration of trauma; the transition to
approaches etiologically rather than descriptively based. Inj Prev 1999; 5: 231-236 4. Meehan WP. Et al. Bicycle helmet laws are associated with a lower fatality rate from bicycle-motor vehicle collisions. J
Pediatr 2013 May 24. Epub 5. Haider AJ. Et al. An evidence-based review: efficacy of safety helmets in the reduction of head injuries in recreational
skiers and snowboarders. J Trauma Acute Care Surg 2012 Nov; 73(5): 1340-7. 6. Spinks A. Et al. The WHO Safe Communities model for the prevention of injury in whole populations. Cochrane
Library 2009, issue 3. 7. Macy M. et al. Availability of child passenger safety resources to Emergency physicians practicing in the ED within
Pediatric, Adult and Nontrauma centers. Pediatr Emerg Care 2013 March 29(3). 8. Macy M. et al. Child passenger safety practices in the United States. Am J Prev Med 2012; 43(3), 272-281. 9. Baldwin G. Fulfilling a promise. The National Action Plan for Child Injury prevention. Inj Prev 2012 June; 18(3) 207. 10. Istre G. Et al. A controlled evaluation of the WHO Safe Communities model approach to injury prevention increasing
child restraint use in motor vehicles. Inj Prev 2011; 17: 3-8 11. Schacter J. Restraint use law enforcement intervention in Latino communities. J Trauma Acute Care Surg 2011;
71(5)S517-521. 12. Bruce B, et al. Group interventions for prevention of injuries in young children: a systematic review. Inj Prev 2005
(11):143-147. 13. Pike I. et al. Developing injury indicators for Canadian children and youth: A modified Delphi approach. Inj Prev 2010 (16):
154-160. 14. Wright S, et al. Childhood Agricultural injury: An update for clinicians. Curr Prob Pediatri Adoles Health Care 2013. 43: 20-
44. 15. Sise M. et al. Measuring trauma center injury prevention activity: An assessment and reporting tool. J Trauma Acute Care
Surg. Feb 2006: 60(2) 444-451. 16. Hirsch M. et al. Injury prevention and the national agenda – can we make America Injury Free? J Tra:uma Acute Care Surg
Aug 2009: 67(2) S91-93. 17. McGuire M .et al. Goods for Guns – the use of a gun buyback as an injury prevention/community education Tool. J Trauma Acute Care Surg Nov
2011 ;71(5)S537-540.

References 18. Coley BD, Mutabagani KH, Martin LC, Zumberge N, Cooney DR, Caniano DA, Besner GE, Groner JI, Shiels WE 2nd. Focused
abdominal sonography for trauma (FAST) in children with blunt abdominal trauma. J Trauma. 2000 May;48(5):902-6.
19. Holcomb GW III, Murphy JP. Ashcraft’s Pediatric Surgery. 5th ed. Philadelphia, PA: Saunders An Imprint of Elsevier, 2010.
20. Lynn KN, Werder GM, Callaghan RM, Sullivan AN, Jafri ZH, Bloom DA. Pediatric blunt splenic trauma: a comprehensive review.
Pediatr Radiol (2009) 39:904-916.
21. Moore EE, Cogbill TH, Jurkovich GJ, et al: Organ injury scaling: Spleen and liver (1994 revision). J Trauma 38:323-324, 1995
22. Sabiston DC II, Townsend CM III. Sabiston Textbook of Surgery. 18th ed. Philadelphia, PA: Saunders An Imprint of Elsevier,
2007.
23. Stylianos S. Evidence-based guidelines for resource utilization in children with isolated spleen or liver injury. The APSA Trauma
Committee. J Pediatr Surg. 2000 Feb;35(2):164-7.
24. Tataria M, Nance ML, Holmes JH 4th, Miller CC 3rd, Mattix KD, Brown RL, Mooney DP, Scherer LR 3rd, Grooner JI, Scaife ER,
Spain DA, Brundage SI. Pediatric blunt abdominal injury: age is irrelevant and delayed operation is not detrimental. J Trauma 2007
Sep;63(3):608-14.
29. Eberhardt CS, Zand T, Ceroni D, et al. The Seatbelt Syndrome – Do we Have a Chance? Ped Emerg Care 2015 on line. 30. Liao W, Wen G and Zhang X. Button Battery Intake as Foreign Body in Chinese Children. Ped Emerg Care 2015 31(6), p. 412-415. 31. De Roo AC, Thompson MC, Chounthirath T, et al. Rare-earth Magnet Ingestion-Related injuries Among Children, 2000-2012. Clin Pediatr. 2013, 52(11), p 1006-1013. 32. Cherniawsky H, Bratu I, Rankin T, et al. Serious Impact of Handlebar Injuries. Clin Pediatr 2014, 53(7), p 672-676.

References 25. Injuries from Batteries among Children agee < 13 years – United States, 1995-2010. MMWR Weekly Report Vol 61(34) Aug 31,2012. 26. Bonnard A, Zamakhshary M and Wales PW. Outcomes and management of rectal injuries in children. Pediatr Surg Int 2007, 23: p 1071-1076 27. Shastri N, Leys C, Fowler M, et al. Pediatric Button Battery and small magnet coingestion. Two cases with different outcomes. Ped Emerg Care 2011, 27(7), p. 642-644. 28.Nataraja RM, Palmer CS, Arul GS, et al. The full spectrum of handlebar injuries in children: a decade of experience.
Injury 2014, 45: p684-689 29. Eckert, MJ, Wertin TM, Tyner SD, et al. Tranexamic acid administration to pediatric trauma patients in a combat
setting: The pediatric trauma and tranexamic acid study (PED-TRAX). J Trauma Acute Care Surg 2014, 77(6) p 852-858.
30. Beno S, Ackery AD, Callum J, et al. Tranexamic acid in pediatric trauma: why not? Critical Care 2014, 18: 313. 31. Kragh JF, Cooper A, Aden JK, et al. Survey of Trauma Registry Data on Tourniquet use in Pediatric War Casualties.
Pediatr Emer Care 2012: 28(12): 1361-1365.

Initial films

6 y.o. vs Manure spreader

Summary
• Identify the level of injury • BEST airway possible - remember it is not always
ET intubation • Oxygenation • Avoid the terrible Triad: Acidosis, hypothermia
and coagulopathy • Transfer as rapidly as possible to definitive care.


How expensive?
• 80.2 Billion dollars in medical care costs • 326 Billion dollars in productivity losses • Of that total, injures in children 0 to 14 account
for 51 Billion dollars • Difficult to calculate the lifetime impact on
children in YPLL and costs of care.

BCR >1 Cost:QALY <$0.00

Epidemiology : Associated Injuries
Of 45 children with Cervical Spine Injuries Pulmonary Contusion 10 Femur Fracture 8 Hemoperitoneum 6 Tibial Fracture 5 Arm Fracture 4 Rib Fracture 3 Splenic Laceration 3 Ruptured Kidney 2 Pelvis Fracture 2 Clavicle fracture, pneumothorax, 1 each hemothorax, flail chest, liver laceration, bowel wall edema, limb amputation
Note: 40% of children with cervical spine injury have no trauma to an other body part
Orestein et al.