Embed Size (px)
Citation preview

Jules Millogo, MD, MSc Director, Public Health Partnerships Merck & Co, Inc. North Wales, PA, USA
WHO-MSD Collaboration to Bring an Ebola Vaccine to the Populations in Need

V920: rVSVΔG-ZEBOV-GP Vaccine
2
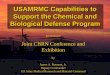
• V920 is a recombinant, replication-competent, vesicular
stomatitis virus (VSV)-vectored-vaccine containing only
the GP protein of Ebola virus (no live Ebola virus)
• The Zaire Ebola virus (ZEBOV) glycoprotein (GP) antigen
is displayed in native conformation on the surface of VSV
•VSV WT •VSVΔG/ZEBOV-GP
•Glycoproteins switched

The International Partnerships Facilitating V920 Clinical Trial Evaluation
3
Study Sponsors and Sites
N vaccinated with
V920
Phase I – Safety and Immunogenicity Trials Using
Varying Vaccine Dose Levels
U. Dalhousie – Halifax, Canada 30
WRAIR – Silver Spring, MD, USA 30
NIAID – Bethesda, MD, USA 30
NewLink – USA 422
WHO – Geneva, Switzerland 100
WHO – Hamburg, Germany 30
WHO – Kilifi, Kenya 40
WHO – Lambarene, Gabon 115 adults/40 pediatric
Phase II/III - Safety, Immunogenicity/Efficacy Trials
at the Selected Vaccine Dose Level of ≥ 2x107 pfu
WHO – Guinea Ring Trial (Ebola ça
Suffit) ~5800
WHO/MSF – Guinea FrontLine
Workers ~1800
CDC/COMAHS – Sierra Leone
(STRIVE) ~8000
NIH/Liberian Partnership – Liberia
(PREVAIL I) ~500
MSD – US / Canada / Europe (V920-
012) ~1060
• 13 trials (one conducted by MSD)
• ~18,000 total vaccinated for all doses
combined (~17,000 subjects vaccinated at ≥ 2x107 dose)
• Efficacy was demonstrated in WHO’s
Ring Vaccination Trial

V920 Overall Safety Conclusions to Date
4
• Preliminary data in healthy, non-pregnant adults suggest an acceptable safety profile that in the context of demonstrated efficacy supports a positive benefit-risk ratio:
– V920 is generally well tolerated.
– Few vaccine-related SAEs reported to date
– Injection-site reactions very common; majority mild to moderate
– Common systemic AEs include headache, fatigue, myalgia, shivering/chills, subjective or objective fever, arthralgia, feeling unwell, nausea, influenza-like illness, and pain. Majority mild to moderate, short duration.
– Joint pain (arthralgia) has been seen in 5%-50% of participants, but joint swelling (arthritis) has been less common (<5% in most studies to 24% in one study).
– Majority of joint events were mild to moderate and resolved within several days (arthralgia) to weeks (arthritis); some subjects reported arthritis of prolonged duration, recurrence and/or sequelae for up to 2 years after vaccination, the longest duration of follow-up to date.
– Rash (with or without vesicles) and mouth ulcers have also been reported.
– Vaccine virus shedding is not frequent in adults and is more frequent in children; secondary transmission has not been demonstrated to date.
– Additional studies in children and HIV+ adults/adolescents have started but data from these studies are not yet available.

Summary of the V920 Product Profile (for Licensure)
5
Description • Live, attenuated vesicular stomatitis (VSV) recombinant
vaccine expressing Ebola Zaire surface glycoprotein
• Generic: Ebola Zaire vaccine (rVSVΔG-ZEBOV-GP, live
attenuated)
Proposed
Indication
Prevention of Ebola-Zaire related disease
• Initial indication: Reactive use
• Eventual indication: General use prophylaxis
Regimen Single dose
Administration Intramuscular (IM) injection of 1mL
Image • Single-dose, liquid-frozen vial (1.2mL)
• Multi-dose available as pre-licensure emergency-use
doses only
Storage • 60oC storage, could be kept up to two weeks at 2-8oC
after thawing.
• Shelf life 3 years; (5 years data TBD)
Target
population
• Initial: ≥ 18 years of age (~2019)
• Eventual: ≥ 1 year of age (~2022)

Regulatory Strategy
6
• Objective: Obtain approval in African countries, facilitated by WHO Prequalification after approval by a stringent regulatory authority (e.g., EMA and/or U.S. FDA).
• Indication: Active immunization of at-risk subjects ≥ 18 years of age to
protect against disease caused by Zaire ebolavirus.
U.S. Food and Drug Administration (FDA)
European Medicines Agency (EMA)
World Health Organization Pre-Qualification
Priority African countries (list being finalized)
Four top priorities

• Expanded Access Clinical Protocols
– Designed to allow use in advance of product licensure under strict protocols requiring informed consent, adherence to GCP, collection of safety data, etc.
• Emergency Use Assessment and Listing (EUAL)
– Mechanism introduced by WHO to allow deployment of a vaccine outside of clinical trials prior to licensure in the context of Public Health Emergency of International Concern
– MSD filed an EUAL application for V920 with WHO in December 2015, with amendments submitted in 2016 -2018; application is currently under review and could be activated/approved if needed
Pre-licensure Deployment Mechanisms
•7

• Regular and transparent Consultations, including ad hoc
emergency meetings to address pressing issues
• Advance exchange of agenda and pending issues to
address
• Leveraging each other’s strengths- for instance WHO has
frequent interactions with African NRAs
• Common voice when approaching regulatory agencies and
associations: FDA, EMA, AVAREF
The Way We Work With WHO PQ Team
8

• Shared Priorities
• Mutual trust that both sides have the best intentions
• Mutual understanding of partner’s constraints
• Willingness to adjust schedules in order to address priorities
• Defined roles and responsibilities and tacit commitment to
implement agreed upon activities in allotted time
Pillars of the Collaboration
9

• Technical Skills: WHO PQ Team has proven to be very
knowledgeable in the regulatory area.
• Understanding of Manufacturing Environment: there is
visible effort to understand Industry’s compliance, legal and
business environment.
• Willingness to Address Challenges- by adopting a
common problem-solving attitude.
How WHO PQ Team Won MSD’s Trust
10

Illustrative Examples of Results of Collaboration
1
1
Addressing programmatic suitability challenges
(thermostability, label, etc.)
Developing a strategy to facilitate African country
registration
Bringing on board AVAREF
Liaison with countries
.

MSD-WHO Collaboration Challenges
• No clear demand size for Ebola vaccine
• Occasional lack of consistency of messages from WHO
• Continued need to overcome cultural barriers between
Industry and WHO
12