Embed Size (px)
Citation preview

Where does Child Psychiatry fit into paediatric practice? UCT Paediatric Refresher Course February 2010
Dr Rene NassenChild and Adolescent PsychiatryDept of PsychiatryStellenbosch University/Tygerberg Hospital

This presentation
A brief history and overview of relationship between Paediatrics and C-L Psychiatry
Red Cross Children’s Hospital Consultation-Liaison service
Case examples Conclusion

What is consultation liaison psychiatry? Consultation:
Services performed for physically ill patients and families, often at the bedside in a general hospital, upon referral of the attending physician or other health care professional
Liaison:
Services provided for the physician and staff, tying together the treatment of the patient and family, using educational conferences, psychosocial teaching rounds and holistic treatment plans
Involves collaboration between two teams who differ in their main focus of interest and methods of working.

Paediatrician- established a physician-patient relationship - primary case manager
Psychiatrist -brief consultations -acute setting -distressed child -communication problems -absence of parent
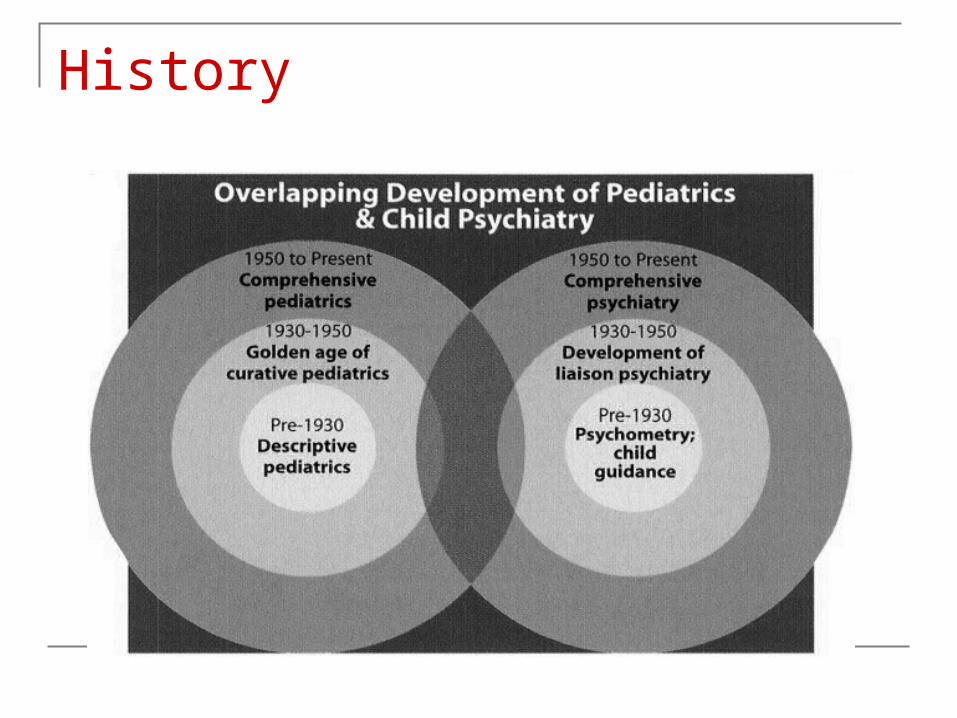
History

Paediatrics and Child psychiatry: 6 decades of the relationship 1937-Kanner L ‘The development and present status of psychiatry and pediatrics’ Pediatrics 11:418-435
1946-Senn M ‘The relationship of pediatrics and psychiatry’ Am j Dis Child 71;537-549
1959-Creak M ‘Child health and child psychiatry, neighbours or colleagues? Lancet 7;481-485
1967-Eisenberg L’The relationship between psychiatry and pediatrics, a disptable view’ Pediatrics 39;645-647
1977-Anders T ‘ Child psychiatry and pediatrics: the state of the relationship’ Pediatrics 60;616-620
1982-Jellinek M ‘The present status of child psychiatry in pediatrics’ N Engl J Med 306;1227-1230
1990-Fritz Gk ‘consultation Liaison in child psychiatry and the evolution of pediatric psychiatry’ Psychosomatics 31;85-90

Donald Winnicott (1896 - 1971)
‘Common Ground’
Collaboration around common goals Clinical population at psychological risk Holistic treatment Prevention Multidisciplinary models of care
Red Cross Children’s Hospital Consultation-Liaison Service Team Services Teaching Research Future- training?

Role of liaison team
Diagnostic Psychosocial meetings/ward rounds Multidisciplinary team meetings Psychological management- group therapy - individual Psychotropic medication Staff support Family support Transition to adult services

Common reasons for referral
Critically ill child ?Depression,?Psychosis (delirium), ?PTSD Behaviourly disturbed, unmanageable child Clinical presentations for which no medical
explanation (? Conversion) The non compliant teenager Transplant assessment
Case 1: The critically ill child
Reason for referral: Referred by S/W on the ICU team 2/52 after admission Extensive burns following fire at home ?PTSD ?Depression
Identifying data: Pearl 10yr 10 month old girl Xhosa and English-speaking Grade 5
Medical Details
Admitted 13/8/05 with >70% burns following fire at home
Most of body affected, face & head spared Multiple operations, including colostomy and many
skin grafts Multiple visits to theatre for change of dressings Septicaemia Significant to severe pain No previous medical/surgical history; no previous
admissions
Medications & Management
Panado Methadone Clonidine Modazolam Amitryptiline Antibiotics Multiple vitamins Nutritional supplementation
Tube-fed Colostomy IV lines Extensive dressings Multiple and regular visits to theatre for grafting or dressing changes
Staff involved
Nursing staff Social worker Medical: Burns team, ICU team, Pain team Physiotherapist Occupational therapist Dietitian Aromatherapist Volunteers Psychiatry
Mental State Examination
Appearance, behaviour, speech Lying on back in bed in ICU almost covered in bandages and
with multiple tubes Engaged well, good eye contact Soft speech, not spontaneous
Mood and affect Objectively sad, but came across as optimistic Subjectively: “happy because my face is not burnt” restrictedAnxiety/PTSD symptoms: Nightmares at night that woke her Thought about the fire and could sometimes ‘see’ fire
Vegetative symptoms: Difficult to assess in view of medical condition, but difficulty
sleeping noted
Thoughts and perceptions: No abnormalities
Cognitions: Alert Orientated to month and year
Insight: Fair

Summary
10yr old girl admitted after severe burns injury
In a critical medical condition
No past medical/psychiatric history
Good family support
Symptoms of acute stress disorder (later PTSD) and possibly depression

Multiaxial Diagnoses
Axis I: PTSD Depressive disorderAxis II: nilAxis III: Severe burns septicaemia GIT complications/ colostomyAxis IV: Medical condition HospitalisationAxis V: 60
Management
Biological:Optimal pain management?Rationalisation of medsFluoxetine 5mg/dayPsychological:Provide source of support to patient & familyEncourage ongoing regular visitsSuggest routine in terms of staff visitsDealing with death and dyingSocial:Contacting school and parents work

Outcome
Patient died 17/10/05 due to overwhelming sepsis, 1 week prior to her 11th birthday
CASE 2: Symptoms for which no medical cause foundReason for referral: Recurrent, unexplained vomiting Referred by neurology registrar during admission for
further investigationsIdentifying data 10yr old girl Saldanha Bay Grade 4 English-speaking Muslim

Medical Details
2yr history of recurrent vomiting severe enough to cause oesophageal tears, oesophagitis and dehydration with electrolyte abnormalities
Associated headaches and abdominal pain Admitted now with severe dehydration, acute renal
failure and for further investigations 1 previous documented UTI No other medical/surgical history No psychiatric history Multiple admissions to RXH and local hospital

Investigations
Blood: FBC & Diff, LFT’s normal U&E abnormal 2° vomiting and dehydration,
otherwise normal Endocrine Metabolic screens Amino acid analysis VMA’sUrine: 1 episode E.coli UTI, otherwise normal VMA’s and NMA’s

Imaging: CT x 2 MRI Ultrasound UKB
EEG: normal
Muscle Biopsy: normal
GIT Endoscopy: normal
Treatment
Admissions for IV fluids
Medication:
Omeprazole, anti-emetics,Carbamazepine
Mental state examination
Appearance, behaviour, speechSitting up in bed, drip IV, relaxed, playing with puzzleAppeared young for age, shyEngaged poorly, unconcernedSpoke softly, answered “I don’t know” or shrugged
shoulders frequentlyGave poor account of illnessMood and affectEuthymic , not anxiousAffect: Inappropriate
Thoughts: No abnormalities Couldn’t think of 3 wishes
No perceptual disturbances
Cognitive function: Orientated, alert, poor cooperation
Insight poor

Summary
10 year old girl from a large nuclear family, presents with long history of unexplained vomiting. History of 1° nocturnal enuresis and shy and nervous temperament.
Maternal history of depression Marital discord Possible abuse

Differential Diagnosis
Axis I: Conversion disorder? Undifferentiated somatoform disorder? Factitious disorder? V code: ??sexual abuseAxis II: deferAxis III: Recurrent vomiting Axis IV: ?Axis V: ?60-70
Outcome
Admission to child psychiatry Selectively mute Emotional distress expressed via somatization Uncooperative parents Several transfers to medical ward Further multidisciplinary meetings Long term admission vs ‘removal’ from parents care Settled after admission to St Josephs Children’s
Home

Ethical dilemmas/end of life decisions 11yo male MVA pedestrian C2 resection, paralysed, ventilator Cognitively intact and alert Prognosis very poor Withdrawal of treatment
Child psychiatry consult
What to tell the child? Right to be informed? Consent/assent Counselling: death/dying Parent’s wishes
Outcome
Met with parents Multidisciplinary team meeting Ethical principle of ‘best interest of the child’,
non maleficence, benificance Sedation maintained and ventilator turned off Follow up sessions with family
Conclusion
End of life Hospital environment Multiple drug regimens Tolerating diagnostic uncertainty

C-L/ Paediatrics
Limited human resources Effective Collaboration Multidisciplinary approach Collaborative clinical services Teaching and training Collaborative research
“Child psychiatry and Paediatrics have enjoyed a long flirtation. It is high time they were married if only for the sake of the children”
(Apley, 1984)

THANK YOU





























