Embed Size (px)
Citation preview

Where are the Men: Finding the Missing Link
By: Daniel Were, PhD

Conflict of interest
• No conflicts to declare

Why Men?
• In Africa, HIV prevalence and incidence is higher in women than in men. However…
• Men account for 48% of people living with HIV globally
• Men are consistently less likely to know their HIV status than women
• Men under-utilize HIV prevention and treatment services
• Men contribute to onward transmission of HIV to others
• Men are more likely than women to die of AIDS-related illnesses
UNAIDS data, 2018

Men are Critical in Breaking the Cycle of Heterosexual Transmission
High HIV incidence men Mean age 27 years (range 23-35 years)
High HIV risk women Mean age 18 years (range 16-23 years)
Very young women acquire HIV from men, on average,
8 years older
Men and women > 24 years usually acquire HIV from similarly aged partners
When teen women reach mid-20s they continue the cycle
Dellar R, Tanser F, Abdool Karim Q, et al. Manuscript in preparation
High HIV prevalence womenMean age 26 years(range 24-29 years)

Multiple Combination Prevention Tools for Men

HIV Testing Coverage Lower Among Men
DHS Comparative Reports, 2013
Perc
enta
ge
ever
tes
ted
fo
r H
IV

Variations Between Men & Women in Progress towards 90-90-90
*Consolidated estimates from PHIA Data: Cameroon, Cote D'Ivoire, Ethiopia, Lesotho, Malawi, Namibia, Swaziland, Tanzania, Uganda, Zambia and Zimbabwe
63%
73%
89%
92%
85%
87%
Tested Linked to Care Viral suppression

Intention is not translating to Action in VMMC – Why?
PSI Research & Metrics, “Zimbabwe (2013): Voluntary Medical Male Circumcision TRaC Study among men and women aged 15 – 49 years in Zimbabwe.” PSI Social Marketing Research Series, (2013)
100%
68% 66% 64%
11%
0%
20%
40%
60%
80%
100%
All Men Aware Interest Intention Circumcised
Intention → MCInterest → IntentionAwareness → Interest
Sample of 1,165 men, ages 15-49, conducted in October 2013

Why are men not getting services? What we know…
9
Lack of provider empathy
Fear of social stigma linked to HIV
Fear of pain and/or adverse events
Lost income when seeking services
Being HIV+ feels emasculating
Men deny and externalize risk
Lack of anonymity and confidentiality
Getting services is a time consuming hassle

HIV Testing has More Drawbacks and Fewer Gains for Men
Anticipated loss with no corresponding gain
Fear, not indifference Grief and trauma
Disclosure is frightening
Men are perceived as indifferent; but in reality they are scared, their HIV testing and linkage journey ischaracterized by fear and loss.
Provider empathy is not guaranteed
Testing positive means life collapses
Breaking the cycle of transmission, 2019

Reflections
• The global health field has come a long way in ensuring that services are available, but when it comes to motivating people to be better consumers of treatment and of preventive health services, there are relatively few proven interventions that promote uptake (Sgaier, 2016)
11
Sgaier et al., 2016. Interventions to drive uptake of voluntary medical male circumcision—A collection of impact evaluation evidence. JAIDS.

HIV acquisition is driven by behavior
and uptake of interventions is
driven by behavior
Dr. Nduku Kilonzo, Director, Kenya National AIDS Control Council
12
“

We Must Turn the Tide:
• How might we make HIV prevention services convenient and attractive to men?
• How might we make men CRAVE the services they NEED but FEAR?
• How might we make the benefits to outweigh the costs?
13

A Framework for Reaching Men
Jhpiego, 2018: Reaching Men for an AIDS Free Generation

15
1. Understand Clients

The CUBES Behavioral Framework
Engl E and Sgaier SK. CUBES: A practical toolkit to measure enablers and barriers to behavior for effective intervention design [version 1]. Gates Open Res 2019, 3:886.
Enablers & Barriers Influencers & Channels Enablers & Barriers
KNOWLEDGE INTENTION ACTION REPEAT HABIT

Deeply Understanding Client Perspectives…
17
Human Centered Design Behavioral EconomicsMarket Segmentation
Understand people’s Desires
Design a product or service that responds
Tell people: Make a compelling Promise
Make it easy to get Deliver on the Promise
Marketing:

Behavioral Economics
A data-driven approach to understanding the psychology behind human behaviors and attitudes
While human choices often seem non rational, this can be predicted…

Market Segmentation
• Age• Gender• Income• Marital status• Education
• Social status• Lifestyle• Personality • Values• Emotions
• Habits • Consumption • Loyalty• Frequency • Intent
Demographic Psychographic Behavioral

Market Segmentation for Oral PrEP: MSM Archetypes

SOCIALLY SUPPORTED BELIEVERS
Base: all uncircumcised men, n=1189
SELF-RELIANT BELIEVERS
FRIENDS DRIVEN HESITANTS
INDIFFERENT REJECTERS
SCARED REJECTERS
KNOWLEDGEABLE HESITANTS
TRADITIONAL BELIEVERS
17%
27% 6%
11%
19%
9%
10%
Moderate potential (11% of uncircumcised men), but high commitment and likelihood to advocate to wide audience; need to overcome some dissonance issue.
Moderate potential (9%), but easy conversion to action and highly likely to act as advocates for friends and to some extent other men.
Moderate potential (10%), but the key barrier is concern in safety which reduce motivation – increase of their commitment is relatively easy by addressing their issues.
Large potential (20%), but rather low motivation and need in additional assurance in need of VMMC. But can be easily converted by strong advocacy around them.
Large potential (17%) but low motivation and strong concerns , including fears and embarrassment – need a lot of support.
Large potential (27%), but hard to crack; absence of motivation and almost no concerns or fears, but could be reached via advocates in the community.
Small potential (6%), no need in support; have very high commitment driven by tradition.
Psychographic Segmentation for VMMC: Client Archetypes

Human Centered Design (HCD)
• Predominantly qualitative
• Offers a process, tools and techniques to:› Build programmers’ empathy,
connection, and respect for clients› More deeply understand the human
and emotional dimensions of a problem
› Catalyze an action-oriented creative problem-solving
22
Mindset
Toolset Skillset

The Design Process

The Design Process Yields Insights = Windows of Opportunity!
How Might We…

25
MSM Key Insights for Oral PrEP Demand Creation
“I never see
pictures of people
like me in the
media. Nobody
understands what
it’s actually like"
MSM talking about stigmatizing and
patronizing content
“I don’t trust
many doctors, I
feel judged
about being an
MSM”
MSM talking about not trusting
advice from outside sources
“If a popular MSM
says no, then there's
no point even trying
to speak to any of
his boys.”
MSM talking about the role that peer
influence drives decisions

Clients Perspectives Providers Perspective on Clients
Insights from a PrEP Continuation Design Sprint: Conflicting Narratives
• Rational decisions
• Risk perception equals health seeking behavior
• Futuristic focus
• Risk and consequences
• Guidelines and prescriptive delivery of PrEP
26
• Emotional decisions• Preoccupied with:
o Social perceptiono Stigma o Emotional needs (Love,
fear, respect, hope)o Does this feel good?o Living NOW
• Choices on how, when, where to receive PrEP

Reality Check???
27
MSM - BOLD STAKEHOLDERS - SUBTLE

2. Deliver Blended Program Activities to Achieve Impact

MSM Interventions for PrEP Uptake in Kenya: Jilinde Project
Let’s Get Real
1
Let’s Get Real Digital Media Campaign
5Collaboration with Family
Planning Leveraging current FP efforts
2Let’s Get Real Events
Initiated on PrEP
4,030*
*122% of target 12 months
before end of project
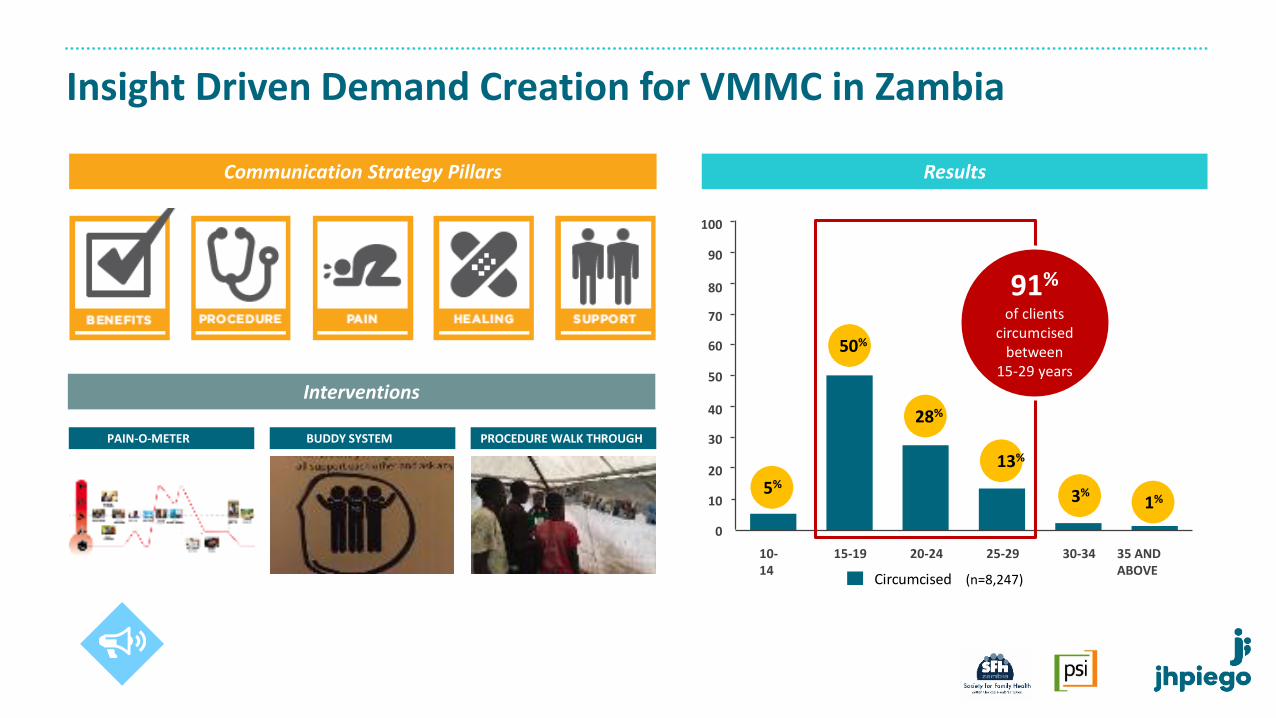
Insight Driven Demand Creation for VMMC in Zambia
Communication Strategy Pillars
Interventions
PROCEDURE WALK THROUGHBUDDY SYSTEMPAIN-O-METER
10-14
15-19 20-24 25-29 30-34 35 ANDABOVE
5%
28%
13%
3%1%
(n=8,247)
91%
of clients circumcised
between15-29 years
50%
Circumcised
0
10
20
30
40
50
60
70
80
90
100
Results

Increasing Uptake of VMMC: AIDS Free Malawi
• Optimization of Community Mobilizers
› Revamped selection criteria › Branded mobilizers› Enlisted satisfied clients › Revised training curriculum› Group incentives

AIDS Free Malawi Performance on 15-29 Age Group
147501 572
1,699
3172 3045
6340
2775 2686
4390
8981
1845
0
10
20
30
40
50
60
70
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
Nu
mb
er o
f V
MM
Cs
VMMCs done in the Month Median Percent of Clients Aged 15-29 Years
Median Before
Median After

The ‘Khotla’ Men's Clinic in Lesotho
• Stand alone male clinic in a public hospital established in 2016
• Comprehensive integrated male friendly services under one roof
• Male service providers
• Clients doubled with over 10,000 clients served annually
• 14% positivity yield, compared to 3% for VMMC clients alone

Note: Yield for partners of FSW = 4.4% & Other Men at Risk = 2.3%
Footballer
1%Religious leaders
5%
Singers/ entertainers
2%
Unskilled laborers
25%
Businessmen
16%Skilled laborers
18%
State Representatives
9%
Drivers
18%
Others
1%
Peers
2%
Older men
3%
Targeting High Risk Men: Sauti Project in Tanzania
• Characterized male typologies (AGYW and FSW sex partners, MSM, General population)
• Mapping of male hotspots and workplaces
• Consultation with men’s sexual partners
• Engaging community leaders and men living/working in hotspots
• Provided male friendly services

180,602 (49.2%)
186,643(50.8%)
Targeting High Risk Men in Tanzania: Sauti Project
2.1%1.6%
6.3% 5.9%
4.4%3.8%
0.0%
4.5%
1.9%
7.7%
5.0%
1.9%2.8%
0.0%1.0%2.0%3.0%4.0%5.0%6.0%7.0%8.0%9.0%
New testersRepeated testers or unknown testing history
Men under 35: Yield by venue (Q1FY18)

Increasing Positive Yield through Index Testing: Kenya
3.3 2.7 2.4 2.4 2.2 2.4 1.5 1.0 1.39
2226
7
27
36
0
10
20
30
40
50
60
70
2011 2012 2013 2014 2015 2016 2017 2018 2019
Posi
tivi
ty r
ate
(%)
Duration (Years)
Routine male Routine male Index male Index female
*Routine testing includes provider and client initiated
Start of
Index Testing

Increasing Access: HIV Self Testing in Kenya
37
34,704sold to dateHIV test kits
17 pharmacies
testing kitsselling HIV self
60of clients are male
%
29 yearsmedian age

Conclusions
• Reaching women with HIV prevention and treatment interventions is not enough to stop the epidemic. We must reach men to reduce incidence among women and protect girls
• Men face numerous complex social challenges that discourage them from seeking HIV prevention services. We need to cultivate a deeper understanding of these challenges
• Innovative tools such as behavioral economics, human-centered design and market segmentation provide new ways of thinking and problem solving
• Jhpiego is applying these tools to catalyze millions of men to access HIV prevention services and address gaps in VMMC targeting, HIV testing, linkage to care, ART retention and PrEP continuation
38

Acknowledgements
• Dr. Sema Sgaier – Surgo Foundation
• Jason Reed, Manya Dotson, Kelly Curran, Zebedee Mwandi, Gideon Mureithi – Jhpiego
• Anabel Gomez – AVAC
39
South Africa
Zambia

Use Format Background to change the image fill





























