Embed Size (px)
Citation preview

WHEN THE BODY SPEAKS: TUMMY RUMBLINGS IN THETHERAPEUTIC ENCOUNTER
Angela King
abstract Historically there has been a struggle to understand the role of the body ina psychotherapeutic context and, although the status of bodily communications is anarea of increasing interest and study, it remains one of the least understood aspects oftherapy practice. Yet even when therapist and client ignore the body in their interaction,they are still confronted with the body as a metaphor for the whole self; as Freud stated:‘The ego is first and foremost a bodily ego’ (Freud, 1923, p. 26) so therapy with no bodyis impossible. Drawing on ideas from practice, theory and research this paper focusesspecifically on borborygmi (tummy rumbling), a bodily phenomenon often consideredinconsequential and intrusive in the therapeutic encounter. Data from a groundedtheory study is presented offering a framework which reflects the processes involved inacknowledging and bringing embodied experiences into an open therapeutic dialogue.Aclinical example is then given.bjp_1233 156..174
Key words: body, psychotherapy, embodied, research, relational psychoanalysis, coun-tertransference, borborygmi, tummy rumbling
Science above all, teaches us to doubt – to question our conceptions of the world.It is an institutional embodiment of Freud’s reality principle.
(Marshall Edelson, 1988, p. 231)
IntroductionAlthough the spoken word dominates psychotherapeutic interaction thereremains the issue of how to work with bodily phenomena, and how to makesense of such bodily information. Borborygmi are the sudden rumbling orgurgling noises occurring spontaneously as our bodies respond to the desire orneed for food. Likewise, because the same reflex is involved with digestion,borborygmi also occur after meals as a result of peristaltic contractions in theintestines. From a medical viewpoint, they serve an important function of equi-librium of the system, which is best understood as a global state transitioninvolving all parts of the brain and body acting in concert. Generally they aremostly heard through use of a stethoscope.
Intuitively we understand that there is a link between the mind and the gutand this is supported by research which shows that gut feelings are not meremetaphors, but do, in fact, have a biological basis (Gershon, 1998). Underlyingthis sensation is an often overlooked extensive network of neurons lining ourguts known as the Enteric Nervous System or ‘Gut Brain’. Previously thought ofas simply relay ganglia, this Enteric Nervous System comprises two autonomic(sympathetic) ganglia; the myenteric and the submucosal plexuses which areresponsible for control of gut motility and regulation of the gut’s luminalenvironment. Although ultimately under control of the central nervous system
ANGELA KING is a Senior Accredited Member of the British Association of Coun-selling and Psychotherapy. She is an Embodied Relational Psychotherapist workingmainly in private practice. She also works in an NHS brief therapy setting as well assupervising in both individual and group settings. Address for correspondence: HeathHouse, 156a Sandridge Road, St Albans, AL1 4AP. [[email protected]]
156
© The authorBritish Journal of Psychotherapy © 2011 BAP and Blackwell Publishing Ltd, 9600
Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA.

this neural network is able to act autonomously, to sense stimuli and to react tothem in various ways. Literally, it learns from experiences, remembers pastactions and events, and produces an entire range of ‘gut feelings’ that caninfluence our actions.
Interestingly, within a psychotherapeutic context, although Scott (1958) sug-gests that the frequently mentioned countertransference reactions to borbo-rygmi might well lead to co-operative research among analysts, an extensivesearch of mainstream psychoanalytic literature returned sparse results. Da Silva(1990) contends that borborygmi of both therapist and client, at certain thera-peutic moments, may be seen as markers of psychic work. He makes a strongcase for viewing the phenomenon within the primitive maternal transference inwhich borborygmi are often accompaniments to the illusion of being fed by theanalyst. He also purports that free association encourages therapeutic explora-tion of the meaning of these occurrences. Sussman (2001), using the termpsycho-peristalsis, presents the findings from a heuristic study suggesting linksto synchronicity, empathy and countertransference.
Body psychotherapy approaches, however, yield more references:
As the belly wakes up in bodywork we hear all sorts of gurglings and rumblings –usually a sign of healthy activity as it resumes its functions of absorption anddischarge. Gerda Boyesen worked for many years with the belly’s wisdom. Shefound – as we have experienced for ourselves – that, whenever the belly emits aparticularly energetic gurgle, it signals some important thought, feeling or memorywhich may be below the threshold of awareness unless we take up the belly’s cueand look within. (Totton & Edmondson, 2009, p. 48)
Indeed, Gerda Boyesen (1980) developed biodynamic psychotherapy aroundthe discovery that peristaltic sounds are part of the self-healing or self-regulatingability of the body. Using a stethoscope to differentiate a multiplicity of peristal-tic noises, she made inferences on the subconscious processes of the clients.
Background to Present StudyMy own interest in this phenomenon has grown as I have increasinglynoticed, with clients, at times of seemingly intense emotion, significant insightor deep connection, that either mine or the clients’ borborygmi (whetherprivate or aloud) are more distinct. For example, in one notable session witha client I had been seeing weekly for six years, she began talking of unre-solved issues. I was fleetingly aware of a sinking feeling in my stomach as Ithought about how stuck we seemed to be. At that precise moment, mystomach gave what can only be described as a loud groan. Her response wasto look, not at my face but at my tummy and state: ‘And you can keep quiet’.I was curious about her response which seemed to be giving my tummy rum-bling an identity of its own, so I asked what she thought it might be saying,and she not only gave an accurate account of what had passed throughmy mind, but also went on to own feelings, ideas and fantasies about hersituation in far more depth than previously. Finally she fell silent, at whichpoint her stomach made its own contribution. ‘Oh, mine’s doing it now,’ she
ANGELA KING 157

commented. Asked to reflect on her own rumbling, she replied that it hadsounded ‘hollow, yet sort of contented’. This comment enabled further explo-ration and processing of what she was now experiencing and the meaning thatshe had attributed to our exchange. It certainly seemed that the advent of theborborygmi joining in had advanced the therapeutic endeavour.
Cole (2002) suggests that at the heart of counselling is the process of listeningand ‘creation of meaning in the moment’. The study presented here ‘listens’ totherapists’ experiences of borborygmi and offers an interpretive frameworkwhich reflects the processes involved in acknowledging and bringing embodiedexperiences into an open therapeutic dialogue.
Underlying the study are three main assumptions:
1) Verny (1981) draws attention to the fact that the unborn child listensall the time, with his mother’s stomach rumblings being the loudestthing he hears. Linked to Stern’s (1985) observations about the devel-opment of visual, tactile and auditory perceptions in creating a two-waycommunication, this suggests that borborygmi are part of a lifelong‘background relational communication’.
2) The digestive tract is not only concerned with the processing of food. Insimilar vein to Bion (1962), Gershon (1998, pp. 16–17) states: ‘Certainly,the voice of the brain is heard in the bowel . . . nor does it inevitably sendthe information it receives back . . . it can, when it chooses, process dataits sensory receptors pick up all by themselves’.
3) Schachter (1997) points out that the body or else one particular organ issaid to offer a privileged medium for the symbolic expression of uncon-scious conflict. Seen from this perspective, borborygmi could be consid-ered a marker of dysfunctional emotional processes and unconsciousmaterial.
My strategy in this study was to encourage articulation and sharing of experi-ences of borborygmi, so contributing to a wider understanding of this embodiedphenomenon.
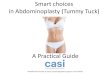
MethodQualitative orientations are particularly well suited to counselling research(Gama, 1992). A grounded theory approach (Strauss & Corbin, 1990), whichaims to unravel the elements of an experience and create a framework forunderstanding how those elements fit together to embody the process of under-going that experience, was used to inform the process of sampling, data collec-tion and data analysis. It is based on the principle of ‘constant comparativeanalysis’ and ‘saturation of data’ (see Figure 1).Three stages are apparent in thistype of data analysis namely, Open Coding,Axial Coding and Selective Coding.This involves gathering evidence through the generation of conceptual categor-ies, which then lead to generalized relations between the categories and theirproperties. The analysis is essentially interpretative, a method that allows theresearcher to dissect the raw data and to organize meaning derived from it in a
158 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)

systematic way until all data is accounted for. Thus it is a method for generatingempirical generalizations rather than universal facts.
McLeod (2001) suggests that grounded theory research should be carried outwith between eight and 20 participants. Fewer than eight results in somethingsimilar to a case study, whereas involving more than 20 participants can produceredundant data. According to Strauss and Corbin (1998), microscopic inspec-tion of 10 high-quality interviews can usually provide the skeleton for a theor-etical structure. In Grounded Theory, however, the ultimate criterion for thefinal sample size is theoretical saturation (Strauss & Corbin, 1998). Theoreticalsaturation employs the general rule that, when building theory, data should begathered until each category is saturated. This means that the category is welldeveloped in terms of its properties and dimensions, demonstrating variationwith no new information emerging.
Background to ResearchThe research was carried out in 2004 as part of an M.Sc. in Counselling Studies.The research proposal was assessed and the research given approval by theUniversity’s ethics committee. Specific ethical considerations included respectfor the confidentiality of the individuals who participated in the study, and forthose individuals and experiences they related. Written consent was obtainedfrom all participants, at time of interview, including the possibility of futurepublication. As the study progressed specific permission was also sought forquotes used. Pseudonyms have been used for all clients and some biographicaldetails have been altered.
Figure 1. Diagrammatic view of Constant Comparison Method
ANGELA KING 159

ParticipantsParticipants self-selected by responding to letters or e-mails sent to two localcounselling centres and a random selection of counselling websites. The 12participants in the study were all practising counsellors and psychotherapistsfrom Psychodynamic, Humanistic and Body Psychotherapy orientations, eachwith between three and 14 years’ clinical experience. Although not intentional,it can be assumed that only those interested in borborygmi took part.
ProceduresSemi-structured interviews were used to provide the raw data, generating aconsiderable amount of data. Each interview was transcribed verbatim withparticipants checking the context and content accuracy of transcriptions prior todata analysis. This allowed the ‘presence of voice’ in the text (Eisner, 1991, p.36), helping validation and emphasizing the rich narrative description ratherthan quantifiable answers. Transcripts were coded into meaning units using anapproach described by Rennie and Fergus (2001, p. 12) as ‘embodied categor-ization’. This means ‘the iteration between the constructed category and themeaning unit is mediated by gut feeling’, which seemed particularly apt for thisstudy on ‘gut noises’. In this way theory generation was inductive, with categor-ies emerging from the data and becoming more focused as the research pro-gressed. Saturation of categories and theoretical constructs occurred after 10interviews when no new conceptual information provided new codes or theexpansion of existing and integrated ones.To validate this sense of closure of theanalytic process two final interviews confirmed established categories whilst notidentifying any new themes. Copies of the completed study were returned toparticipants for member checking. The comments received back supported theview that the findings were compatible with their own perceptions on the topicarea.
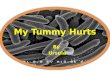
ResultsAfter careful consideration, the central category that emerged and became thetitle of the theoretical model was ‘Rumbling Exposure – Revealing Responses’(see Figure 2).
A storyline approach (Strauss & Corbin, 1998, p. 146) is employed in pre-senting these findings. It highlights the features of the identified theory andreveals how four sequential stages are inextricably interwoven with each otheras well as through the core category.
Although the framework presented here investigates therapists’ responses toborborygmi, it has transferability in that it could just as easily explain theprocess around any other phenomenon occurring within the psychotherapeuticsetting.
Stage One: Being OpenThe definition of ‘Being Open’ emerged from the data to describe the open andreceptive stance of the therapist from which later knowledge will suddenly
160 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)

emerge. It involves a type of listening attention that therapists engage in neces-sitating the setting aside of conscious expectation thus maximizing the potentialfor curiosity, surprise and discovery.
Three sub-categories are identified;
1) Drawing attention represents a prompt to notice something happeningin the moment, drawing the therapists’ attention to selective anddetailed information about their physiological responses, subjectiveexperiences and expressive behaviours. The category is broad enoughto encompass obvious rumbles, private rumbles or ones occurring atspecific moments:
You know in theatres they have a whisperer, hidden, well sometimes it’s like thewhisperer reminding of the importance in our narrative. (P6)
They rumble inside you and I tend to think they are for me to note . . . it could besomething very intimate or just a pull up, just a reminder. (P4)
Rumbling Exposure – Revealing Responses
Being Open Drawing attention
Differentiating Focusing and filtering
Deciding on Significance Rationalizing Questioning Validatin
Making Meaning Playing with ideas
Interpreting
Reflecting on Practice Sharing experiences Identifying training
needs
Figure 2. Diagrammatic representation of identified theory: Rumbling Exposure– Revealing Responses
ANGELA KING 161

2) Focusing and filtering illustrates a contrasting awareness of borborygmieither as a specific focus or a background feature:
So if it’s out of the ordinary then I’ll become aware of it but there’s the backgroundlevel and it’s like traffic or birds, sometimes you notice it but normally it’s justthere in the background. (P8)
Yes, sometimes I notice it in the silences with clients, but then I haven’t reallythought it happens in silences, I’ve just thought that it’s more obvious. (P3)
Implicit in these quotes is the notion that the division of attention betweenrelatively strong and weak stimuli, and a heightened degree of self-awarenessseem to increase the salience of borborygmi. Moreover, borborygmi appearmore obvious when the therapeutic space is not being filled with other sounds.The theme of heightened awareness to borborygmi in the absence of distrac-tions also held true for the intimacy of the shared moment. Although borbo-rygmi could be considered a distraction, in this instance client and therapistweave it almost effortlessly into the relational dynamic:
As soon as we were doing therapy once again from a shared space, her stomachstarted rumbling and quite closely afterwards, mine too, and both of us laughedbecause it’s been quite a theme . . . frequently, and she said, ‘Oh so now we arewelcome’ or something like that. (P6)
3) Differentiating highlights how borborygmi are experienced as havingdifferent tones and qualities at different times with participants identi-fying different nuances:
It is fascinating how they do alter with my mood and my feelings. (P10)
The sound reflects the feeling. (P2)
Indeed, participants imagined borborygmi as a kind of internalized body sensoroffering an additional means of cultivating mindful listening, as illustrated in thefollowing transcript extract showing the transition of the counsellor’s thinkingfrom an initial assumption about digestive processes to an acceptance of adeeper process:
I initially just assumed they were to do with being hungry, [pause] but I did noticethat [pause] that given that I’m seeing my clients at the same time every week itstarted to dawn on me that there was something not just about being hungry becauseotherwise you’d expect it to be the same sort of the same type of tummy rumbling ateach session and it’s not like that at all . . . It’s more in difficult sessions which is whyI’ve put it down to my anxiety . . . so yes maybe it is around deeper things. (P9)
Stage Two: Deciding on SignificanceDeciding on significance brings into focus how therapists consciously respondto borborygmi informed by personal and professional attitudes and values. Itconcerns the transformation of thoughts, feelings and ideas as therapists decideif and how borborygmi can be of value within the therapeutic process:
162 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)

They are quite congruent with something concrete happening in the therapy roomor within the client process and I think these are quite distinctively different andunlike the occasional tummy rumble but again I can tell you that I can pick it up,but I don’t know how to explain it. (P6)
Three sub-categories are defined:
1) Rationalization emerged out of the data as participants described howtummy rumbles are frequently accompanied by an affect of some nature.Feelings of embarrassment and anxiety were the most frequently men-tioned with a tendency to ignore or apologize; also evident were humourand relief:
But there’s something about – I know mine will want to reply and I’m embarrassedby this. (P8)
But it’s another thing like what I wear or the room that can be picked up by theclient. (P3)
Even in the research interviews it was hard to break the habit of rationalizing:[Tummy rumble followed by laugh] Sorry, I haven’t had any breakfast yet. (P9)
Despite the obvious amusement, consider how often in therapy laughterdisguises other emotions! When faced with the difficult task of thinking abouthow physical and somatic aspects contribute to a therapy, it appears a morecomfortable option to avoid mentioning these aspects altogether:
I think it’s the tactlessness somehow, when they’re deep in their sadness or theirpain or whatever, I hope they haven’t heard it because it does seem intrusivestamping your own physiological noises on their pain. (P11)
It certainly seems there is an implicit taboo about openly discussing bodilyattributes. Yet even if it is possible to accurately distinguish ‘food relatedrumbles’ these are still events occurring in the therapeutic space about whichboth participants will have some thoughts, feelings and/or fantasies:
I think probably, what, certainly the obese client thinks, always thinks that I’mempty. (P1)
Considering that personal experiences of borborygmi within the therapeuticsetting were acknowledged in every interview, it is perhaps surprising that acommon theme was that these aspects often go unmentioned. Why?
I think that’s because it’s not really knowing how to use it. (P2)
It’s not culturally acceptable to talk about tummy rumblings. (P4)
We’re all of us in denial anyway about what happens in our bodies. (P10)
I thought it was the time of day I saw the client and my own sort of dietary habits.(P7)
No wonder then it is easier to just rationalize borborygmi as a digestive func-tion. This is not to say that borborygmi might not, at times, be attributable todigestive phenomena separate from psychosomatic causes, but if we do notallow ourselves to consider the possibility, we may be missing rich material.
2) Validating articulates how it is possible to consider borborygmi as aninterface between the psyche and a somatic response:
ANGELA KING 163

It’s only the body language actually gives you the indication of whether you aregetting anywhere, because the body language quite often gives you the truth whenwords may not. (P2)
Therapeutic change can be quite gradual and slow and it’s really good, both for meas a therapist and for a client to have somatic confirmation that something ishappening. (P6)
So, here (in the body) there is material that needs to be taken into account andelaborated!
3) Questioning highlights a number of processes ranging from identifyingmeanings, significance, timing, and impact, to concerns about therapists’somatic responses:
Well, when it happens in sessions, for the client or for myself, I wonder what itmeans and why it’s happening at that time. (P1)
So the cynic might say its purely physiological but no, I think there is definitely alink there and my body was picking up my wanting to show a very sympatheticfeeling. (P3)
This questioning attitude adds a valuable dimension to the therapeutic relation-ship that advances the clinical work, as illustrated here:
So I wondered about what was going on between her and I or what was going onin her material that might have been responsible for my tummy rumbling . . . andin fact what she brought to the session was she was really anxious that her mum wasgoing to leave and send her away . . . but on this particular occasion she was cryingwhich she hadn’t really done before . . . And what I thought about after that . . . be-ing aware of the tummy rumbling, was her hunger for her mum, to be understoodand to have a relationship with mum. (P5)
Prompted by the borborygmi this participant moves through progressive stagesof reflection allowing understanding of the client’s distress to deepen. It is thispurposeful use of borborygmi that aids assimilation of new material.
Stage Three: Making MeaningMaking meaning captures the essence of the interactive and creative process bywhich client and therapist ascribe meaning to borborygmi. Two sub-categoriesilluminate these processes:
1) Playing with ideas makes explicit how both metaphorical and narrativeexplorations become part of a contemplative process. Participantsaccredited borborygmi with an ability to communicate and inform,complementing speech, in the fullest sense of the word, drawing atten-tion to what was variously described as mimicry, an empathic response,coincidence and mirroring. Moreover, tummy rumbling conversationswere attributed to acknowledge, reflect back, or repeat emotionalresponses evoked by the client material:
I couldn’t say that, but my stomach at exactly the moment that I was feeling aah,my stomach made this absolutely aah sound. (P7)
164 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)

It’s as if you know your emotions are being mirrored in and by your tummy. (P11)
However, it is acknowledged that these are subjective views. In spite of theinevitable consequences of becoming ‘immersed’ in the topic and the need to beon ‘intimate’ terms with the question, Moustakas (1990) emphasizes the needfor personal responsibility during the exploratory process of research to checkand judge the evidence. Borborygmi in this instance spoke for itself, literallyjoining in:
I am talking about my stomach so why shouldn’t it want to be involved in theconversation? (P9)
2) Interpreting makes explicit how participants attribute existing theoreticalconstructs to borborygmi. Various theoretical constructs including coun-tertransference, empathy, intersubjectivity and projective identificationwere identified by participants:
And that is quite important to the extent that transference and countertransfer-ence are not things you can see . . . and tummy rumblings are really good becausesometimes they just make that visible. (P6)
But my client’s stomach started rumbling and I started to do the same . . . it wasalmost like a sort of empathic sort of response. (P10)
In my countertransference I was quite concerned for her and that was when mytummy started to get really noisy. (P11)
It’s not that she made my tummy rumble . . . I don’t think she evoked that in mebut her reaction, what she made of it was a projection. (P1)
I use them, you know whether it comes from me or the client because it is in thespace between us, it’s in the intersubjectivity. (P4)
Therapists inevitably have a shaping influence on clinical material, especially asthere are no ‘time outs’ in the session and everything a therapist does, says, ordoes not say affects how clients talk, think, feel and act. If therapists ‘accept’borborygmi as a natural, valid part of the therapeutic discourse, so will theclients giving another perspective:
I have a client who calls it something like ‘Bullshit detector’. (P6)
Stage Four: Reflecting on PracticeThis stage explicates the ongoing process by which therapists reflect on andadvance their professional practice. Two sub-categories are delineated:
1), 2) Sharing experiences and Identifying training needs. Developing reflec-tive practice both in and on practice (Schon, 1983) enables the practi-tioner to respond to the unique challenges of practice. However, itwould seem,even when borborygmi do inform the therapeutic process,they are omitted when writing notes or presenting in supervision:‘I’veused it but then I’m not sure that I recorded it in my notes’. (P1)
This lack of recording instances of borborygmi may reflect a wider concernconnected with the low priority given to bodily issues in training. Therapists
ANGELA KING 165

need to feel confident working with bodily phenomena if the possible signifi-cance of borborygmi ‘joining in’ can be explored:
They do affect me, but I’m listening out for them now to see if I can tell what theyare saying. (P7)
Within this particular sample it is notable that, unless body psychotherapy wasthe main modality, the majority of participants acknowledged that their formaltraining did not include the use of embodied phenomena such as borborygmiand were also unaware of written material on the subject:
In fact I didn’t even know it had a name. (P5)
I think possibly the sort or a lot of the training was that if you’re interested in thatthen you go ahead and you do it and you look it up. (P8)
However, an example of borborygmi as a contributor to sessions was given inevery interview and was also an active contributor in 10 of the 12 interviews.One might ask why the absence of borborygmi in two interviews? Theresearcher only assumes it was absent, as it was only acknowledged if heard:
I am talking about my stomach so why shouldn’t it want to be involved in theconversation? (P7)
So the explicit findings in this study are that borborygmi are not isolatedincidents. Some participants use it for reflection about the client and the thera-peutic situation, some use it instinctively to play with something in the sessionbringing richness to the therapeutic work, and some ignore it perceiving it as adisruption to the therapeutic space. Several admitted that it was only because ofthis research that they had given it any serious thought:
I was aware of it in a more conscious way than I would normally have been againbecause I knew I was coming here. (P5)
Clarkson (1995, p. 75) states that countertransference, like transference, iseverywhere and unavoidable but countertransference that is likely to causetrouble is the unconscious one on the analyst’s side. Problems occur whensuch feelings are out of awareness, chronic or repetitive, detrimental to thetherapeutic work, or persistently distressing to the therapist. These pointssound remarkably similar to some of the participants’ views expressed aboutborborygmi. If borborygmi should be viewed as mentioned in this study atdifferent times as countertransference, projective identification, intersubjectiv-ity, empathy or synchronicity, then it is imperative that more attention is givento this embodied phenomenon in training.
Discussion and Implications for PracticeOverall, the findings fit with existing views which privilege the importance ofborborygmi as highlighted by Boyesen (1980), Da Silva (1990) and Sussman(2001). The central process identified in the model is the development of adynamic integration of cognitive, psychosocial and interpersonal behaviourstowards a therapeutic orientation.
166 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)

The study indicates the importance of the therapist’s stance. The analyticattitude, first described by Freud (1912), is that suspended free-floating atten-tion is the basis of all settings. Others have characterized this therapeuticlistening as an analytic ‘reverie’ while Fordham (1993), referring to Reik (1949),talks of listening with the ‘third ear’. However, whilst these recognized conceptsof listening accept that the empathic and emotional dimension of listening hasa bodily and physiological dimension, very little attention is paid to the embod-ied presence of the practitioner and their capacity to be fully there as a body, notjust as a disembodied mind or consciousness.
In this study the category ‘Being Open’ stresses a capacity for attunement toour body’s own wordless, felt sense of experiencing similar to Gendlin’s (1996)focusing-based therapeutic approach or Wilberg’s (1998) maieutic listening.Listening in this way, when borborygmi catch a counsellor unawares, as high-lighted here: ‘Well, it was a surprise to me because it came so suddenly’ (P3), itmay be easier to accept them as markers of psychic significance (Da Silva,1990), or metaphorical slips of the tongue, rather than just a tummy rumble.
An implication of the findings shows how developing the capacity to be withmoment to moment awareness, to tolerate ambiguities and unexpected phe-nomena without judgement, can enhance awareness of the sensory, somatic,intuitive and emotional background of experience:
It is almost an invitation to shift position and then usually when I am shiftingposition I also engage with some kind of recursive process of what’s going on orthat I’m not comfortable with, or what is it that the client’s not comfortable with atthat thing. (P6)
Furthermore, as attachment theory attests, the nonverbal communication ofaffect is fundamental to all forms of social interaction and serves to regulate thebiological functioning of both people in a dyad. Even if nonverbal events inpsychotherapy are overlooked or not consciously noticed, they occur, and rela-tional mutual influence happens largely on a bodily level.
Recent work in neuroscience suggests that emotion functions to co-ordinatethe mind and the body.According to Regina Pally (1998, p. 349), who is workingon bridging psychoanalysis and the neurosciences: ‘Emotion connects not onlythe mind and body of one individual but minds and bodies between individuals’.
Findings in this study show how putting the body on the map of psycho-therapy helps psychotherapists to perceive and to use the bodily information.Body-oriented interventions can be woven into the verbal dialogue and becomeone of many possible interventions therapists have at their disposal at any onemoment. Awareness of body reactions and nonverbal cues makes room for thefreshness of the moment; it invokes the actual and it makes one alert to what isrelevant.
As shown in this study, it facilitates affective contact in the client and itprovides a ground for deeper exploration. Certainly previous research revealsthat a high degree of self-awareness increases the relative salience of all aspectsof the self, including somatic information (Duval & Wicklund, 1972; Wegner &Giuliano, 1982). Further, Gendlin (1991) stresses the primacy of the body as a
ANGELA KING 167

prelinguistic source of language that continues to speak in the midst of speak-ing. It could therefore be argued that borborygmi are joining in the conversa-tion as many of the participants in this study suggested:
Our tummies rumble together so it’s like a conversation at a deeper level. (P2)
Findings also suggest that, when we can pay attention and listen in a moreintimate, bodily way, we are able to recognize the nuances of our own experi-ence and in turn are increasingly able to recognize the nuanced communicationof our clients. So, paying attention to bodily information also gives access todysfunctional emotional processes and unconscious material. Although manytherapists may have either tacit or explicit knowledge of empathic resonance, Iwonder how many are aware of its somatic aspects. Indeed, Hanna (2000) pointsout that empathy is a somatic response, and suggests that the therapist’s body isenacting the themes and conflicts on a subconscious level. Casement (1985) hassuggested that patients not only communicate by words, they also communicateby impact, a suggestion several participants seemed to affirm:
I think in hindsight it’s always when there is something very disturbing. (P2)
Viewed in this way, the therapist’s capacity to contain the feelings aroused inhim by the client can be seen as equivalent to the function of a mother con-taining the infant projections, to use Bion’s model (1967). From this viewpoint,if the projection is preverbal when no words were available to distinguishbetween body and psyche, bodily symptoms in the therapist may provide thefirst clue to understanding. The following quote seems comparable to thisconcept:
But it’s interesting because you can think of words like digesting and processingyou know which are words that I would commonly use to interpret it, but in factthey wouldn’t have been right because it was something about taking it in but notdigesting until then, and that puts the sort of slight distaste of something beingunpalatable in the mouth because her story was . . . it’s something I didn’t want totolerate. (P5)
For decades the body-oriented tradition has been working with the notionthat memory is not at all an exclusively cerebral process. Where does arepressed memory get stored? Reich’s (1943) explanation, as extended byGerda Boyesen (1980), implies that emotionally significant interactions becomeinternalized in a variety of ways. Boyesen contends that these repressed memor-ies are regulated by the dual biological and psychological function of the gastro-intestinal tract. She came to the conclusion that certain massage techniquescould bring to completion the expression of unwanted feelings, and this wouldentail similar noises from the intestines as during digestion of food. She claimedthat this function of digesting psychological problems which she termed‘psycho-peristalsis’ is identifiable by a multiplicity of different tonalities andtypes of tummy rumblings, and is often accompanied by new insights.
In this study participants expressed similar observations:
I know this sounds a bit mad, but it’s not always the same sound and I think thesound can actually reflect how I’m feeling about something. (P10)
168 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)

Sussman (2001) has also drawn attention to this property linking it to synchro-nicity. Notably, Williams (1957) points out that a common reaction when asynchronistic event occurs is to construct a linear causal explanation or, con-versely, in the absence of a satisfactory explanation, dismiss the experiencealtogether as coincidental. For Jung, a tireless champion of open-mindedness,calling an event coincidence did not automatically shut the door on any furtherexamination of the facts. Consider Jung’s description of synchronicity: ‘Thecoincidence of a psychic state . . . with a simultaneous, objective, external eventthat corresponds to the psychic state or content’ (Jung, 1997, p. 97). Borborygmicertainly seem to be compatible with the concept of synchronicity:
My tummy just rumbled [said with a sense of amazement] so suggestive. (P10)
But there is, I know there is I want to say a co-incidence rather than a coincidence.(P8)
The noise that came from my tummy perfectly mimicked what I was feeling andwhat I would have wanted to vocalize. (P4)
Seen in this context, borborygmi could be considered as a mode of interper-sonal communication.
So the study emphasizes the dual physiological and psychological ability ofthe digestive system. This is consistent with Bion’s (1967) theory of thinkingwhich is based on the centrality of the ‘digestion’ of emotional experience. Heargues that a failure in the maternal containment of an infant’s experiences canlead to problems for the individual in their ability to transform internal andexternal events into digestible elements. Clearly, for Bion, thinking emergesfrom bodily events and the experience of satisfaction is the substance of newself-understanding. Participants in this study highlighted how borborygmi atcertain times seemed to be an audible acknowledgement of this:
And you reach that point when you think gosh maybe, maybe just maybe there’s abit of movement here then there’ll be a deep gurgle of almost contentment. (P11)
Thus the framework identified in the study gives a clear message; for thepsychotherapist, cultivation of deep listening facilitates the free flow of clinicalcreativity and engages the wisdom of the embodied heart–mind. This goesbeyond mere technique to understanding how the therapist becomes a rela-tional presence in the interior life of the client (and vice versa), dynamicallyco-arising in intimate dialogue. Indeed, several participants reported how asession comes alive when borborygmi is explored in metaphorical or narrativeterms:
So when there are tummy rumblings I ask, ‘Aah, so what is it like?’ and then it givesan opening for whatever a client’s metaphor for this, often it is a conversation. . . sometimes it’s nice to give it a voice, and then I want to know who is it that’strying to talk and how old is he, or how old is she? (P6)
What the results do not adequately explain, however, is specific context andtiming in relation to the whole psychotherapeutic context. Participants had noclear answers to these conundrums:
ANGELA KING 169

I don’t know, maybe I notice it more as time goes by. There are certainly a fewclients where it’s very poignant and natural part of our work whereas with othersit’s just an occasional thing. (P6)
Short and long term I can’t honestly say that I can remember any difference. I thinkit happens across both. (P8)
I don’t know if this is about people who are certain personality styles, or is it aboutpeople who are very anxious and people talking about very difficult material? (P9)
Maybe it happens at the beginning because they’re nervous, or it happens when wego deeper into the issues, or is it both? (P3)
However, this study did not attempt to discover the prevalence of borbo-rygmi or to explain it, merely to describe the processes involved. Furtherstudy may be indicated to explore these specific questions in relation to thequality and length of the relationship, personality types, client history orsubject matter.
In summary, being open to the significance of borborygmi (as with any otherembodied reaction) has the potential to both widen and deepen the therapeuticprocess.Whether considered as countertransference (Da Silva, 1990), synchron-icity (Sussman, 2001), or intersubjectivity (Shaw, 2003) it is important that thetherapist recognizes and is able to utilize them. The danger, it seems, is pointedout by this participant:
It’s interesting that it seems to coincide with what’s happening with the client butunless you disclose that or bring it into therapy then how the hell do we know.(P10)
LimitationsDespite the steps which were taken to enhance the trustworthiness of the study,the subjective nature inherent in this research needs to be acknowledged.Criticism could be directed toward the sample size. However, as Morse (1994)suggests, smaller sample sizes may afford researchers opportunities to get adeeper understanding of participants’ experiences. No claim to universal gen-eralizability of the results can be made.
Clinical Example‘Gwen’, 50 years old, had begun counselling following the distress of a diagnosisof cancer necessitating a hysterectomy and the breakdown of her marriage. Ourearly work was definitely about containment. Initially she was not able to thinkabout or begin to process anything, and I wondered how I would survive thesheer force of her anger, which was a tangible presence in the room.
Gwen had few, if any happy memories. Adopted when she was 18 months oldshe has no direct memory of her real mother.The betrayal by her husband whenhe left her for another woman reinforces her inner belief that she is not lovable– a belief that has come from her birth mother’s total abandonment and the lackof either physical or emotional nurturance from her adoptive parents. Her earlyexperiences of deprivation and aggression have been so intense that as a child
170 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)

she never felt safe enough to bring good and bad experiences of self and othertogether into an integrated whole.All the suffering Gwen endured as a child sitsinside and engulfs her, much like the cancer threatened to do – both arepotential killers.
Six months into our work together Gwen had arrived for a session in aparticularly distraught state following an unsatisfactory encounter with herex-husband. For several minutes, as the full weight of her fury spilled out, I wasaware of my stomach silently rumbling. As her angry outburst subsided shecollapsed into tears, unable to look at me. Listening in an embodied way (beingopen) it was as if my borborygmi were vicariously experiencing, for a momen-tary period of time, what it is like to be Gwen. I decided that in this instance mygut feelings were of significance. The analytic dyad, according to Schore (2009),intensifies the client’s (as well as the analyst’s) experience of dissociated dys-regulated emotions and defensive adaptations. As they become part of anenmeshed interaction within the intersubjective field, they constitute not only apowerful mode of non-conscious communication, but through the analyst’saffect tolerance they also become an important means towards affect regula-tion. My response therefore aimed to give attention and interpretation to thoseregressive aspects of Gwen’s emotional experience that could be thought aboutand integrated.
I said I was remembering her talking about her childhood and how she hadnot been able to express herself as a child; I made an analogy about a pressurecooker suggesting that, when there is no outlet for steam, the contents becomemore pressurized and dangerous to manage. She told me it was not so much thatshe wasn’t allowed to shout but that she had had so many reasons to scream andshout. She wasn’t listened to. I suggested it was like that small child is stillscreaming to be heard. She agreed and asked me: ‘But why is it so active, whydoes it make everything so difficult, why does it take over?’
I reflected that it felt as if it was difficult to trust that anyone would beinterested in her needs and suggested that, in asking that question, part of herbecomes like mum ignoring ‘the child’ and she is unable to hear her until sheshouts. My interpretation was met with a momentary silence followed by a loudrumble as her stomach loudly joined in. With a little laugh she put her hand toher mouth as she stated:‘Well, I certainly heard her this time!’ When she told meit had felt like something had shifted, I asked if she could say a bit more. ‘It’strue,’ she reiterated, ‘I get so caught up in all the shit that keeps getting thrownat me I expect the worst all the time and I just don’t expect anyone to under-stand.’ Now we were able to consider her inner resources acknowledging that,as well as the vulnerable inner child, there was an inner strength that she hadbeen able to call on when necessary.
I think what this brief example from my practice illustrates is the reparativepossibility in working with embodied phenomena in the therapeutic endeavour.As Resneck-Sannes (2003) writes:
Our ability to be empathic and attuned to the client is what is healing in therelationship . . . The current research utilizing brain imaging is finding that this
ANGELA KING 171

somatic, empathic attunement appears to be necessary for developing attachmentin infants and for any therapy process. (pp. 16–17)
The therapist needs to be attuned to such an extent that the material is within thetherapeutic window . . . Our body interventions should become an invitation forthe client to explore somatically (sensate) feelings, meaning, imagistic representa-tion, and internal object representations.We then become the mirroring, empathic,attuned other that hopefully will begin to live inside our client’s body/mind andsupport them in being who they are. (p. 20)
ConclusionsThis study explored experiences of borborygmi in order to ascertain theirsignificance and impact within the therapeutic space. Certainly participants inthis study did have many examples of significant experiences involving borbo-rygmi as a way of further understanding something happening in the therapeu-tic relationship.
I do not assume that the findings are specific to borborygmi but suggest thatthey might also be instructive about other similar ‘meaning moments’ andembodied responses. Indeed most participants had also experienced otherembodied responses including tears, tingling sensations and drowsiness.
The study unavoidably carries the ‘voice’ of the researcher. Borborygmi ofboth researcher and ‘participant’ have been active contributors in all but two ofthe interviews, which highlight the interactive and affective nature of the inter-views whilst also illuminating the process being uncovered.
If therapists are to avoid missing part of the picture it is necessary to respectthe idiosyncratic situation; it is also necessary to honour the individual mean-ings applied to such situations. I feel that my offering of this grounded theorystudy does just that. It is simply an attempt to challenge my own assumptions,tacit knowledge, preconceptions and misconceptions.
Hopefully, the persuasiveness of the finished study lies in its value for guidingpractice. As such it highlights important implications for practice, training andsupervision. Previous studies provide support for expanding our ideas aboutembodied knowledge, especially borborygmi, to include more careful consider-ation of the role a therapist’s body plays. If these bodily issues were addressedin training and supervision then maybe therapists would give embodied reac-tions such as borborygmi a more prominent and acceptable role?
ReferencesBion, W.R. (1967) Second Thoughts. London: Heinemann.Bion, W.R. (1962) Learning from Experience. London: Heinemann.Boyesen, G. (1980) Collected Papers of Biodynamic Psychology, vols 1 & 2. London:
Biodynamic Publications.Casement, P. (1985) On Learning from the Patient. London: Tavistock.Clarkson, P. (1995) The Therapeutic Relationship. London: Whurr.Cole, S. (2002) The creation of meaning in the moment. Counselling and Psychotherapy
Journal 13(3): 10–13.Da Silva, G. (1990) Borborygmi as markers of psychic work during the analytic session.
International Journal of Psychoanalysis 71: 641–59.Duval, S. & Wicklund, R. (1972) A Theory of Self-Awareness. New York, NY: Academic
Press.
172 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)

Edelson, M. (1988) Psychoanalysis: A Theory in Crisis. Chicago, IL: University ofChicago Press.
Eisner, E.W. (1991) The Enlightened Eye: Qualitative Inquiry and the Enhancement ofEducational Practice. New York, NY: Macmillan.
Fordham, M. (1993) On not knowing beforehand. Journal of Analytic Psychology 38(2):127–36.
Freud, S. (1912) Recommendations to physicians practising psychoanalysis. SE 12, pp.109–20. London: Hogarth.
Freud, S. (1923) The Ego and the Id. SE 19, pp. 1–66. London: Hogarth.Gama, J. (1992) Toward science–practice integration: Qualitative research in counselling
psychology. Journal of Counselling and Human Development 25: 1–12.Gendlin, E.T. (1991) Thinking beyond patterns: Body, language and situations. In: den
Ouden, B. and Moen, M. (eds), The Presence of Feeling in Thought, pp. 21–151. NewYork, NY: Peter Lang.
Gendlin, E.T. (1996) Focusing-oriented Psychotherapy. New York, NY: Guilford.Gershon, M.D. (1998) The Second Brain. New York, NY: Harper Perennial.Hanna, E.C. (2000) Somatic psychology for psychotherapists. Somatics 12(4): 28–31.Jung, C.G. (1997) On synchronicity. In: Main, R. (ed.), Jung on Synchronicity and the
Paranormal, pp. 93–103. Princeton, NJ, London: Princeton University PressMcLeod, J. (2001) Qualitative Research in Counselling and Psychotherapy. London: Sage,
2006.Morse, J. (1994) Designing funded qualitative research. In: Denzin, N.K. and Lincoln,
Y.S. (eds), Handbook of Qualitative Research, pp. 220–35. Thousand Oaks, CA:Sage.
Moustakas, C. (1990) Heuristic Research: Design, Methodology and Applications. Thou-sand Oaks, CA: Sage.
Pally, R. (1998) Emotional processing:The mind–body connection. International Journalof Psychoanalysis 79: 349–62.
Reich, W. (1943) Character Analysis. 3rd edn. New York, NY: Orgone Institute Press.Reik, T. (1949) The Inner Experience of a Psychoanalyst. London: Allen & Unwin.
[Quoted in Fordham (1993).]Rennie, D. & Fergus, K. (2001) It rises from my gut: Embodied categorizing in grounded
theory analysis. Paper presented at Annual Meeting of International Society forTheoretical Psychology, Calgary, Alberta, June 2001.
Resneck-Sannes, H. (2003) Bioenergetics: Past, present and future. Keynote address,IIBA Conference, Bahia, Brazil.
Schon, D. (1983) The Reflective Practitioner: How Professionals Think in Action. NewYork, NY: Basic Books.
Scott, C.M. (1958) Noise, speech and technique. International Journal of Psychoanalysis39: 108–11.
Schachter, J. (1997) The body of thought: Psychoanalytic considerations on the mind–body relationship. Psychoanalytic Psychotherapy 11(3): 211–19.
Schore, A.N. (2009) Right brain affect regulation: An essential mechanism of develop-ment, trauma, dissociation and psychotherapy. In: Fosha, D., Solomon, M. and Siegel,D. (eds), The Healing Power of Emotion: Integrating Relationship, Body, and Mind, pp.1–54. New York, NY: Norton.
Shaw, R. (2003) The Embodied Psychotherapist: The Therapist’s Body Story. Hove:Brunner Routledge.
Stern, D. (1985) The Interpersonal World of the Infant. New York, NY: Basic Books.Strauss, A. & Corbin, J. (1990) Basics of Qualitative Research:Techniques and Procedures
for Developing Grounded Theory. Thousand Oaks, CA: Sage.Strauss, A. & Corbin, J. (1998) Basics of Qualitative Research. Thousands Oaks, CA:
Sage.Sussman, S. (2001) The significance of psycho-peristalsis and tears within the therapeutic
relationship. Counselling and Psychotherapy Research 1(2): 90–100.Totton, N. & Edmondson, E. (2009) Reichian Growth Work: Melting the Blocks to Life
and Love. 2nd edn. Ross-on-Wye: PCCS Books.
ANGELA KING 173

Verny, T. (1981) The Secret Life of the Unborn Child. London: Sphere.Wegner, D. & Giuliano, T. (1982) Arousal-induced attention to the self. Journal of
Personality and Social Psychology 38: 719–26.Wilberg, P. (1998) Listening as bodywork: Therapy, philosophy and maieutic listening.
Energy and Character 30(1): 77–94.Williams, M. (1957) An example of synchronicity. Journal of Analytic Psychology 2: 93–5.
174 BRITISH JOURNAL OF PSYCHOTHERAPY (2011) 27(2)