Embed Size (px)
Citation preview

What’s New In Neurology?
Evie Marcolini, Assistant ProfessorEmergency Medicine and Neurology
Medical Director, SkyHealth Critical CareYale University School of Medicine
Tuesday, May 10, 16
We make a difference
Tuesday, May 10, 16

•Subarachnoid hemorrhage
• Best practices
• Intracerebral hemorrhage
• Blood pressure
•Traumatic brain injury
• Are we chillin’ yet?
• Stroke
• Interventional madness?
What’s new?
Tuesday, May 10, 16

SAHTuesday, May 10, 16

Exam, exam, examHunt/Hess
Intubate if needed Reverse coagulopathy
Manage blood pressureTreat pain
Think about hydrocephalusAntifibrinolytic agentsSeizure prophylaxis
Tuesday, May 10, 16

Tuesday, May 10, 16

Tuesday, May 10, 16

Exam, exam, examHunt/Hess
Tuesday, May 10, 16

Hunt and Hess Classification
Grade 1Asymptomatic, minimal headache slight nuchal
rigidity
Grade 2Moderate to severe headache, nuchal rigidity; no
neurological deficit (except 3rd n. Palsy)
Grade 3 Drowsiness, confusion, or mild focal deficit
Grade 4 Stupor, moderate to severe hemiparesis; possible early decerebrate posturing
Grade 5 Deep coma, decerebrate posturing, moribund
Tuesday, May 10, 16

Exam, exam, examHunt/Hess
Intubate if needed Reverse coagulopathy
Manage blood pressureTreat pain
Think about hydrocephalusAntifibrinolytic agentsSeizure prophylaxis
rebleedTuesday, May 10, 16

Tuesday, May 10, 16
Tuesday, May 10, 16

We make a difference
Tuesday, May 10, 16
Tuesday, May 10, 16

Malhotra:CT/LP most effective in most settings .
Acad Emerg Med. 2016 Jan 4 (epub ahead of print)
Wu:CT/CTA not effective
Emerg Med J 2016;33:30-36
Martin:LP is a useful “rule-out”
Br J Neurosurg 2015;16:1-5
Sayer:LP has low diagnostic yield
Acad Emerg Med 2015;22:1267-‐1273
Dubosh:CT is extremely sensitive in certain cases
Stroke 2016;47:00-‐00
Meurer:CT/CTA is reasonable approachhemorrhage J Emerg Med 2016 (epub ahead of print)
Tuesday, May 10, 16
Take this home
Exam, exam, examHunt/Hess
Intubate if needed Reverse coagulopathy
Manage blood pressureTreat pain
Think about hydrocephalusAntifibrinolytic agentsSeizure prophylaxis
CT/LP is still the standard...but not for long
rebleedTuesday, May 10, 16

ICHTuesday, May 10, 16

Tuesday, May 10, 16

Tuesday, May 10, 16
We make a difference
Tuesday, May 10, 16

Airway Imaging
Blood pressure managementAnticoagulation reversal
Osmotic therapyTransfer to appropriate level of care
Surgical interventionsGoals of care
Airway
Tuesday, May 10, 16

NICU Intubation - Nursing checklist
Tuesday, May 10, 16

Airway Imaging
Blood pressure managementAnticoagulation reversal
Osmotic therapyTransfer to appropriate level of care
Surgical interventionsGoals of care
Tuesday, May 10, 16

Tuesday, May 10, 16

Airway Imaging
Blood pressure managementAnticoagulation reversal
Osmotic therapyTransfer to appropriate level of care
Surgical interventionsGoals of care
rebleedTuesday, May 10, 16

Tuesday, May 10, 16

J Hypertens 2008;26:1446-52
HemorrhagicIschemic
Tuesday, May 10, 16

Tuesday, May 10, 16

NOACSTuesday, May 10, 16

Glund S Lancet 2015;386:680-90
Idarucizumab reverses dabigatran
Tuesday, May 10, 16

Siegal DM N Engl J Med 2015 Nov 11 [Epub ahead of print]
Andexanet reverses apixaban and rivaroxaban
Tuesday, May 10, 16

Airway Imaging
Blood pressure managementAnticoagulation reversal
Osmotic therapyTransfer to appropriate level of care
Surgical interventionsGoals of care
Tuesday, May 10, 16
Airway Imaging
Blood pressure managementAnticoagulation reversal
Osmotic therapyTransfer to appropriate level of care
Surgical interventionsGoals of care
Tuesday, May 10, 16

Neurosurgical considerations
VentriculostomyClot evacuation
Craniectomy
Tuesday, May 10, 16
Tuesday, May 10, 16

Tuesday, May 10, 16

Airway Imaging
Blood pressure managementAnticoagulation reversal
Osmotic therapyTransfer to appropriate level of care
Surgical interventions
Goals of care
Take this home
rebleedTuesday, May 10, 16

TBITuesday, May 10, 16

Tuesday, May 10, 16

Tuesday, May 10, 16

Avoid hypotension and hypoxia
Tuesday, May 10, 16

Tuesday, May 10, 16

Avoid hypotension and hypoxiaC-spine precautions
Head of bed up 30 degreesAirway
Hyperventilation?Osmotics
Anticoagulation reversalSeizure prophylaxis
Consider ventriculostomy
Tuesday, May 10, 16

Adult-Salvageable TBI -GCS 3-8 after resuscitation-Abnormal CT
-TBI with normal CT with:-Age > 40-Posturing-SBP < 90
Tuesday, May 10, 16

Tuesday, May 10, 16

HyperventilationMannitol
Hypertonic salineVentriculostomy/drainage
Maintain CPP>50Vasoactives as needed
CraniectomyParalytics
Phenobarbitol burst suppressionTherapeutic hypothermia
Increasing ICP treatment
Tuesday, May 10, 16

N Engl J Med 2015;373(25):2402-12
Standard therapy favored over therapeutic hypothermia
Tuesday, May 10, 16

Tuesday, May 10, 16

Fever is BAD
Tuesday, May 10, 16

Tuesday, May 10, 16
Avoid hypotension and hypoxiaCPP = MAP - ICP
Dont hyperventilateOsmotics
Anticoagulation reversalSeizure prophylaxis
Consider ventriculostomy
Take home
Tuesday, May 10, 16

Acute Ischemic Stroke
Tuesday, May 10, 16
Rapid assessment and treatmentBlood pressure = perfusion
Endovascular therapy is an optionConsider Goals of Care
Tuesday, May 10, 16

Advance hospital notification by EMSRapid triage protocol and stroke notification
Single call activation systemStroke tools
Rapid acquisition/interpretation of imagingRapid lab testing
Mix tPA ahead of timeRapid access to IV tPATeam-based approachPrompt data feedback
JAMA 2014;311(16):1632-40
Tuesday, May 10, 16

JAMA 2014;311(16):1632-40Tuesday, May 10, 16

Tuesday, May 10, 16

J Hypertens 2008;26:1446-52
HemorrhagicIschemic
Tuesday, May 10, 16

Tuesday, May 10, 16

Tuesday, May 10, 16
Tuesday, May 10, 16

N Engl J Med 2013;368:952-5
Tuesday, May 10, 16

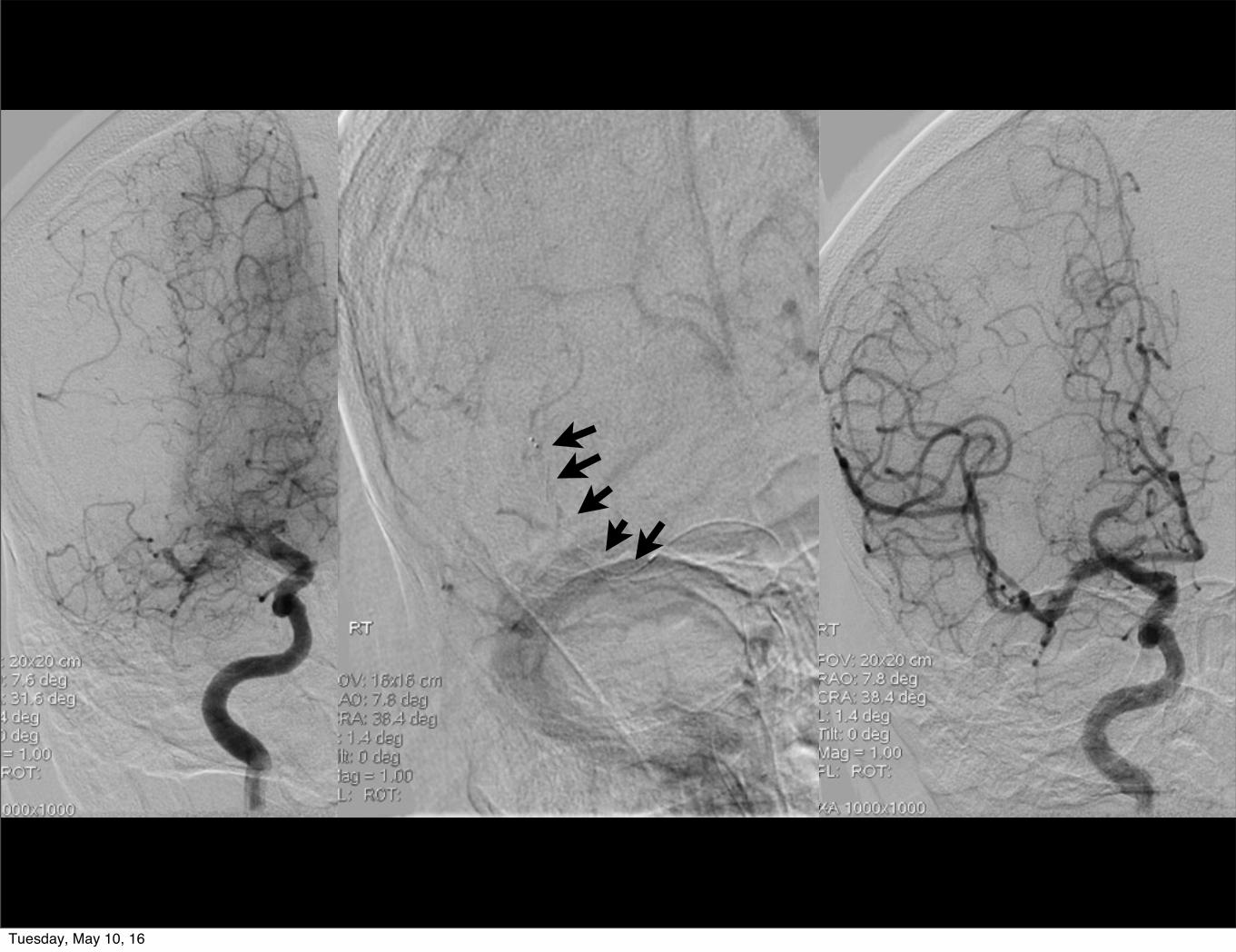
N Engl J Med 2015;372:11-20
MR-CLEAN Investigators
Absolute difference 13.5%mRS 0-2
Tuesday, May 10, 16

Tuesday, May 10, 16

Tuesday, May 10, 16

N Engl J Med 2015;372
Tuesday, May 10, 16

Who is appropriate for endovascular thrombectomy?
-55 yo, stage IV metastatic disease, spontaneously resolving and then undergoing thrombectomy with TICI 3 reperfusion, a month more
before hospice?
-58 yo with no history, NIHSS 15 to 1, TICI 3 reperfusion and discharged to home with slight facial droop?
Tuesday, May 10, 16

Rapid assessment and treatmentBlood pressure = perfusion
Endovascular therapy is an optionConsider Goals of Care
Take this home
Tuesday, May 10, 16

Airway - fine tune itHyperventilation - don’t
Exam - repeat itBlood pressure - manage itCoagulopathy - reverse it
Osmotics - use themTransfer -slow down to speed upSeizure prophylaxis - consider it
Surgical/endovascular options - consider them
We make a difference
Goals of CareTuesday, May 10, 16

















![REVIEW ARTICLE / ПРЕГЛЕД ЛИТЕРАТУРЕ Imaging of the ... · soft tissue pathology [17, 18]. Imaging of the TMJ requires a dedicated pa - tient posturing. Adequate mandible](https://img.dokumen.tips/doc/110x75/60327b08e2249856f20cd09e/review-article-imaging-of-the-soft-tissue.jpg)