Embed Size (px)
Citation preview

1
Quality Payment Program Final Rule Year 2:What’s Coming in the New Year!
Michelle Brunsen and Sandy Swallow
December 6, 2017
This material was prepared by Telligen, the Medicare Quality Innovation Network Quality Improvement Organization, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 11SOW-QIN-D1-12/04/17-2481

2
• Overview of 2018 Quality Payment Program (QPP)
– Key changes to the Merit-Based Incentive Payment System (MIPS) for 2018
– Retroactive changes for 2017
– Eligibility and participation options
– Timelines and important dates
– Incentives and penalties
– Significant Hardship Exceptions
• Your questions!
Today’s Agenda

3
• Proposed Rule published 6/30/2017• Final Rule Year 2 released 11/2/2017• Effective January 1, 2018• Comments accepted through 5 pm EST January 2,
2018– Submit electronic comments to http://www.regulations.gov– Follow the “Submit a comment” instructions– Refer to CMS-5522-FC when commenting on issues in the Final
Rule– Refer to CMS-5522-IFC when commenting on issues in the
interim final rule
Quality Payment Program Year 2 Timeline

4
Quality Payment Program Year 2 (2018)
A Second Year to Ramp UpBuild upon the iterative learning of year 1
Prepare for more robust year 3

5
MIPS Eligible Clinicians 2018
MIPS Eligible Clinicians
• Physicians– MD, DO
– Dentist
– Podiatrist
– Optometrist
– Chiropractor
• Physician Assistants
• Nurse Practitioners
• Clinical Nurse Specialists
• Certified Registered Nurse Anesthetists
Eligible Clinicians Excluded from MIPS
• Clinicians at or below the Low Volume Threshold
• Eligible Clinicians newly enrolled with Medicare
• aAPM Qualified Participants (QPs)• aAPM Partial QPs who choose not
to report• Temporary Excluded Credentials
– Certified Nurse Midwife– Clinical Social Worker– Clinical Psychologist– Registered Dietician or Nutritionist– Physical or Occupational Therapist– Speech-Language Pathologist– Audiologist

6
Low-Volume Threshold (LVT) Exclusion and Opt-In Option
• < $90,000 Medicare Allowable Charges OR
• < 200 Part B-enrolled beneficiaries
• Excludes an additional 134k Clinicians
• Two data runs to determine eligibility– Each period Sept. 1 – Aug. 31 with 30-day claims run out
– 1st period ending in the calendar year 2 years prior to performance year
– 2nd period ending in the calendar year 1 year prior to performance year
• Applied at the submitting entity level: individual or group
• LVT Opt-in option for 2019 not finalized– Concerns CMS may not be ready to operationalize
– Revisit in 2018 NPRM
MIPS Eligible Clinicians 2018

7
MIPS Reporting Options 2018

8
Inclusion of Virtual Groups
• Additional participation option• Solo practitioners and groups of < 10 clinicians come together to
participate as a group regardless of location or specialties• Qualified non-patient facing clinicians eligible• Most MIPS group policies apply
– Must exceed the LVT to participate
• Elect to participate and go through an election process– Election period Oct. 1 – Dec. 31, 2017– Submit application– Establish a formal written agreement
• Resources on QPP website– Virtual Group Toolkit– Virtual Group Fact Sheet
MIPS Reporting Options for 2018

9
MIPS Incentives and Penalties 2018
10
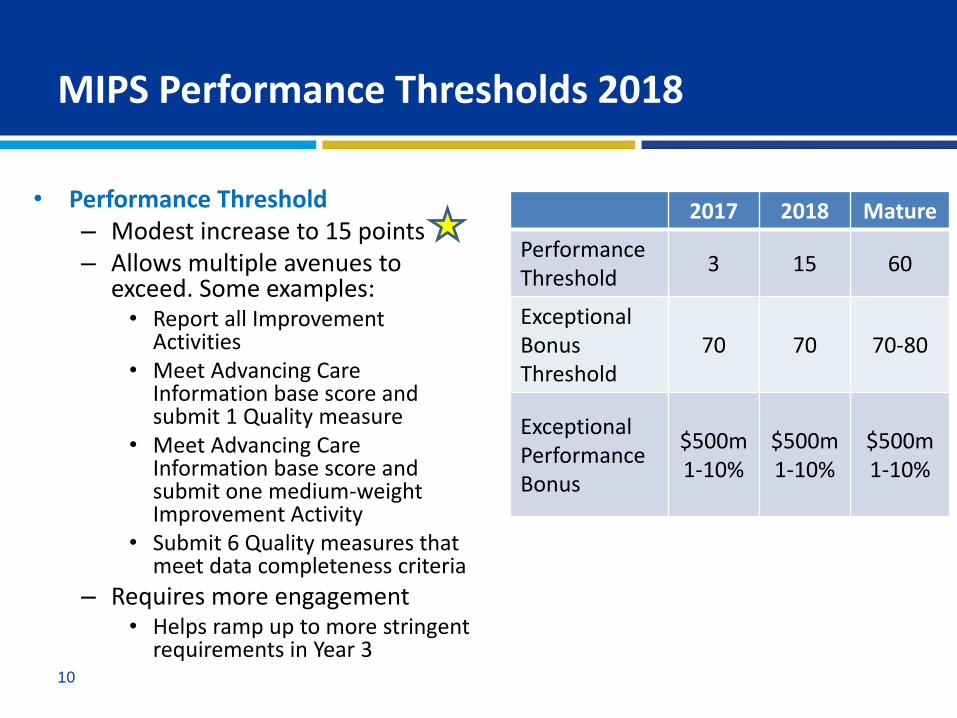
MIPS Performance Thresholds 2018
• Performance Threshold– Modest increase to 15 points– Allows multiple avenues to
exceed. Some examples:• Report all Improvement
Activities• Meet Advancing Care
Information base score and submit 1 Quality measure
• Meet Advancing Care Information base score and submit one medium-weight Improvement Activity
• Submit 6 Quality measures that meet data completeness criteria
– Requires more engagement• Helps ramp up to more stringent
requirements in Year 3
2017 2018 Mature
PerformanceThreshold
3 15 60
Exceptional BonusThreshold
70 70 70-80
Exceptional PerformanceBonus
$500m1-10%
$500m1-10%
$500m1-10%

11
• Only allowed 1 data submission mechanism per performance category
• Multiple submission mechanism options starting in 2019
MIPS Submission Mechanisms and Deadlines
Mechanism Deadline
Qualified Registry
March 31QCDR
EHR/Data Submission Vendor
Attestation (ACI and IA)
Claims March 1 (60 day claims run-off)
Web Interface 8 week submission window between Jan. 2 and Mar. 31 TBD

12
MIPS Performance Category Weights 2018
Performance Year
Quality Cost Advancing Care
Information
ImprovementActivities
2017 60% 0% 25% 15%
2018 50% 10% 25% 15%
2019 30% 30% 25% 15%
2020 30% 30% 25% 15%
• Complex re-weighting protocols
• Hardship Exemption Applications can now apply to any/all Categories

13
Performance Category Performance Period
Quality 1 Full Year
Cost 1 Full Year
Advancing Care Information 90-Day Minimum to 1 Full Year
Improvement Activities 90-Day Minimum to 1 Full Year
MIPS Performance Period Requirements 2018

14
Performance Category Requirements 2018

15
Quality Measure Submission Requirements
• 6 measures including 1 Outcome or High Priority Measure– Fewer than 6 measures?
• Partial credit awarded for partial submission• Measure groups still available
– Claims/Qualified Registry Only– Eligible Measure Applicability (EMA) the new MAV test
– Or Web Interface Submission (groups 25 or more)– If a quality submission is made
• 1 Administrative Claims Measure: All Cause Readmissions– Medicare Calculates from claims– Only if Group size >15 and > 200 attributed hospitalizations
MIPS Quality Performance Category 2018

16
Data Completeness
• > 60% reporting rate required• All payer data for: (at least one measure must contain data
on one Medicare patient)– Registry– QCDR– EHR
• Medicare beneficiary data only for:– Claims– Web Interface
• Finalized the same criteria for 2019
MIPS Quality Performance Category 2018

17
Expanded the Measure Stratification Classes
• Class 1 – Complete: 3-10 points– 60% reporting rate
– 20 case minimum
– Has a benchmark
• Class 2 – < 20 Cases or No Benchmark: 3 points
• Class 3 – < 60% Reporting Rate: 1 point (3 for small practices)
MIPS Quality Performance Category 2018

18
New Scoring Language
• Measure Achievement Points
• Total Measure Achievement Points (TMAP)
• Measure Bonus Points
• Total Measure Bonus Points (TMBP)
• Total Available Measure Achievement Points (TAMAP)
• Scoring equation– (TMAP + TMBP)/TAMAP = Total Quality Performance Category Score
– Quality Performance Category Percent Score when expressed as a percent
MIPS Quality Performance Category 2018

19
Topped Out Measures
• Defined:
– Majority of clinicians near top of the distribution
• Little room for improvement
• Little basis for comparison
– 45% of measures are topped out
• 6 measures identified
• 4-year lifecycle protocol
MIPS Quality Performance Category 2018

20
MIPS Quality Performance Category 2018
• 4-year lifecycle years
1. Identify as TOM
2. Special scoring applied7-point Cap
3. Consider removal through rulemaking
4. Removal decisions made through rulemaking
Measure #
Preoperative Care: Selection of Prophylactic Antibiotic
21
Melanoma: Overutilization of Imaging Studies in Melanoma
224
Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis
23
Image Confirmation of Successful Excision of Image-Localized Breast Lesion
262
Optimizing Patient Exposure to Ionizing Radiation:
359
Chronic Obstructive Pulmonary Disease (COPD): Inflated Bronchodilator Therapy
52
21
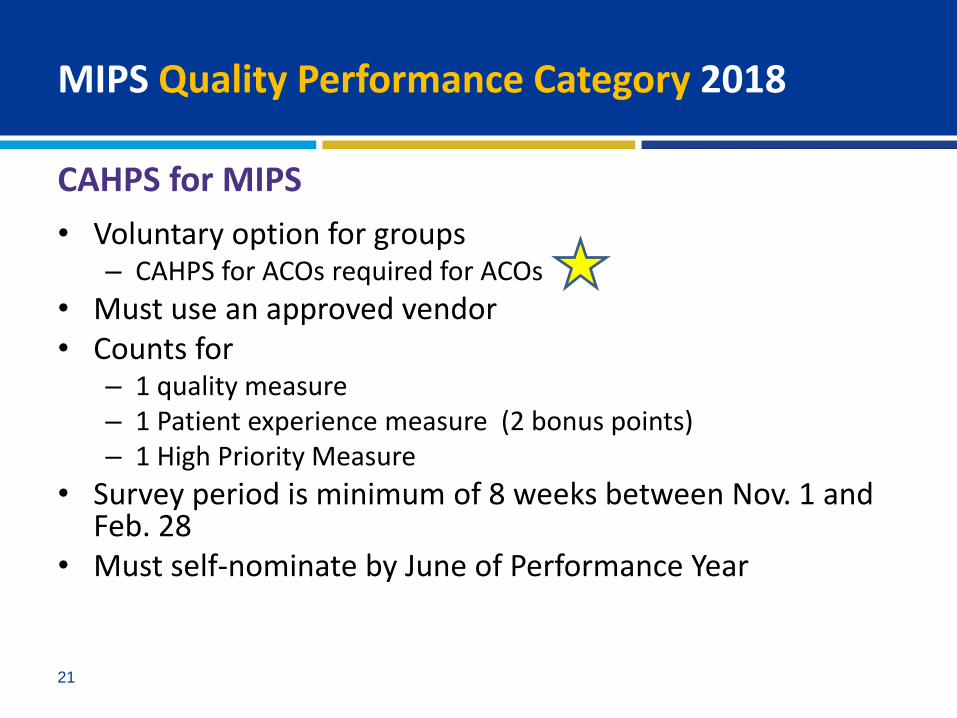
CAHPS for MIPS
• Voluntary option for groups– CAHPS for ACOs required for ACOs
• Must use an approved vendor• Counts for
– 1 quality measure– 1 Patient experience measure (2 bonus points)– 1 High Priority Measure
• Survey period is minimum of 8 weeks between Nov. 1 and Feb. 28
• Must self-nominate by June of Performance Year
MIPS Quality Performance Category 2018

22
Quality Category Improvement Bonus
• Full current year participation required• Comparison only to previous year data at category level
– If previous year Quality score < 30, then 30% is used as comparison
– Will convert data for comparison if entities do not match
• Calculated as– Capped at 10% points– Category Percentage Scores without Bonus Points– Based on statistically significant changes
• (This Yr. Score – Last Yr. Score/Last Yr.)
MIPS Quality Performance Category 2018

23
Cost Category Dynamics
• 10% weight; 30% 2019• 2 Cost Measures
– Total per capita costs for all attributed beneficiaries• Attributed to the Provider/Practice source of Plurality of Primary Care
Services• All Part A and Part B costs• 20 Case Minimum
– Medicare Spending per Beneficiary (Inpatient)• Attributed to the Provider/Practice source of the Plurality of Inpatient
Services• Costs included 30 days pre-admission to 30 days post-admission• 35 Case Minimum
– NO Episode Measures
MIPS Cost Performance Category 2018

24
Cost Category Improvement Bonus
• Measure level analysis• Must have data in prior year
– Same measure– Same entity level– Both sets meet data sufficiency minimums
• Can only be positive• Max of 1% point• Cost improvement score = (measures with significant
improvement-measures with significant decline)/measures) *1% point
• (Cost Achievement Points/Available Cost Achievement Points) + (Cost Improvement Score) = (Cost Performance Category Percent Score)
MIPS Cost Performance Category 2018

25
ACI Category Dynamics
• Maintains a 25% weight
• Scoring the same: Base + Performance + Bonus
• Reporting period: minimum of continuous 90-day up to full year
• Allow use of 2014 or 2015 CEHRT or combination
– 10% point bonus for exclusive use of 2015 CEHRT
• Rule is silent on CEHRT requirements for 2019
MIPS Advancing Care Information Performance Category 2018

26
ACI Category Exceptions
• Hospital-based clinicians
• Non-patient facing clinicians
• Ambulatory Surgery Center (ASC)-based clinicians
MIPS Advancing Care Information Performance Category 2018

27
ACI Category Clarification/Corrections
• Meaningful user = any provider with an ACI Category Score > 75%• Timely for Patient Access = 4 business days after data available to
EC• Applied Retroactively to 2017
– VDT action – clarified the actions in the measure as being taken by the patient or the patient-authorized representatives rather than the MIPS EC
– Summary of Care document can be generated by any support staff, not just clinician
– Minor verbiage corrections to: Patient Access, Patient Education, Health Information Exchange & Medication Reconciliation
MIPS Advancing Care Information Performance Category 2018

28
ACI Category Clarifications/Corrections
• Same minimum for any reporting period – 90 to 365 days• Specific exceptions to e-Prescribing and HIE Base Point
Measures - Retroactive to 2017– Generate fewer than 100 prescriptions in a reporting period– Generate fewer than 100 outgoing transitions of care in a
reporting period– Receive fewer than 100 incoming TOC in a reporting period
• 2015 CEHRT measures• Applies to never-before-encountered patients
MIPS Advancing Care Information Performance Category 2018

29
ACI Category Dynamics
• Reporting to Public Health Agency (PHA) or Clinical Data Registry (CDR)– 10% points for electronically reporting to any
single PHA or CDR
– Bonus score of 5% points for reporting to at least one additional PHA or CDR
– Bonus registry must be different than the performance registry
MIPS Advancing Care Information Performance Category 2018

30
IA Category Dynamics
• Maintains 15% weight
• Finalized more activities (112) and changes to existing activities – 30 CEHRT IA measures available (extra credit in ACI)
• Performance period minimum of continuous 90-day up to including full year
• Continue double points for small practices, rural or HPSA and non face-to-face
MIPS Improvement Activities Performance Category 2018

31
IA Category PCMH Adjustment
• Language adjusted to include status of “Recognized” as equivalent to “Certified”
• 50% threshold for number of practice sites within TIN with PCMH recognition for full credit
• Must attest to receive credit
MIPS Improvement Activities Performance Category 2018

32
New Bonus opportunities!
• Improvement Bonus – Quality: applies to category-level (1-10% points)– Cost: applies to measure-level (1% point)
• Applies at Final Score Level– Add 5-point Small Practice bonus (< 15 clinicians)– Add 5-point Complex Patient bonus (dual eligibility ratio and HCC risk
score)• Based on Risk Score year prior to performance period• Patient attribution overlapping performance year (Sept.- Aug.)
• Electronic Flow – Limit to 10% of denominator– Scoped for the first 2 years only– All but Claims Submission Measure
MIPS Scoring Additions for 2018

33
• Significant Hardship Exception by Application– Due by December 31st starting in 2017– Applicable to Individuals, Groups, Virtual Groups– Expanded to apply to any one or more performance categories– Results in Re-weighting – 5 year limitation removed– Supported reasons for approval include:
• Significant hardship for small practice• Insufficient internet connectivity• Extreme and uncontrollable circumstances• Lack of control over the availability of CEHRT• Lack face-to-face patient interaction• Decertified EHR technology
– Good faith effort to migrate to CEHRT– Annual Renewal limitation to 5 years
MIPS Hardship Exceptions

34
• Automatic Extreme and Uncontrollable Circumstance Policy– Interim (emergency) final rule
• Automatic exception without having to submit an application
– “The Hurricanes – Harvey, Irma and Maria Rule”
– “Northern California Wildfires – Disaster Exceptions/Exemptions”
– Final Score = Performance Threshold
– Data accepted and scored if submitted
Significant Hardship Exceptions

35
Automatic Identification
• CMS will automatically identify the following status with access through QPP website:– Low Volume– Small Practice– Rural and HPSA Clinicians and Practices– Non-Patient Facing Clinicians and Practices– Hospital Based Clinicians and Practices– Ambulatory Surgical Center Based Clinicians and Practices– Facility-Based Clinicians and Practices (not available until 2019) – Extreme and Uncontrollable Circumstances
MIPS Special Provider Populations for 2018

36
Small Practices Status Applicable to:
• Eligibility for technical assistance
• Improvement Activity requirement
• ACI Hardship Exception
• Small Practice Bonus
• Low Volume Exclusion if meet criteria
• Virtual Group option if meet criteria
• 3 Point floor on Quality Measures
MIPS Special Provider Populations for 2018

37
Special Status Applicable to:
Special Status Activity
Rural and HPSA • Improvement Activity Points doubled
Non-Patient Facing
• Improvement Activity Points doubled• Advancing Care Information (ACI)
• Automatically reweighted• Scored if submitted
Hospital-Based• Advancing Care Information (ACI)
• Automatically reweighted• Scored if submitted
ASC-Based
• Advancing Care Information (ACI)• Automatically reweighted• Scored if submitted
MIPS Special Provider Populations for 2018

38
More than one Final Score is associated with a TIN/NPI?
Example Final Score Used to Determine Payment Adjustments
TIN/NPI has more than one APM Entity final scoreThe highest of the APM Entity final scores
TIN/NPI has an APM Entity final score and also has an individual score
APM Entity final score
TIN/NPI has an APM Entity final score that is not a virtual group score and also has a group final score
APM Entity final score
TIN/NPI has an APM Entity final score and also has a virtual group score
APM Entity final score
TIN/NPI has a virtual group score and an individual final score
Virtual group score
TIN/NPI has a group final score and an individual final score, but no APM Entity final score and is not in a virtual group
The highest of the group or individual final score
Hierarchy for Final Score

39
No Final Score is associated with a TIN/NPI?
MIPS EC (NPI1) Performance Period Final
Score
TIN/NPI Billing in MIPS Payment Year
(yes/no)
Final Score Used to Determine Payment
Adjustment
TIN A/NPI 1 90Yes(NPI 1 is still billing under TIN A in the MIPS payment year)
90
TIN B/NPI 170
No (NPI 1 has left TIN B and no longerbills under TIN B in the MIPS payment year)
N/A (No claims are billed under TIN B/NPI 1)
TIN C/NPI 1N/A (NPI 1 was not part of TIN C during the performance period)
Yes (NPI 1 has joined TIN C and is billing under TINC in the MIPS payment year)
90 (No final score for TIN C/NPI 1. Use the highest final score associated with NPI 1 from the performance period)
Hierarchy for Final Score
Table 31; page 778

40
• CMS wants to hear from you!
• How to comment on the Final Rule:
– Electronically through Regulations.gov
– Regular mail
– Express/overnight mail
– Hand or courier
• Submit comments by Jan. 2, 2018
• QPP Final Rule Year 2
Continue the Dialogue

41
✓ Create a strategy to manage Cost in 2018✓ If you are in a small practice, check the revised low-
volume thresholds and learn more about virtual groups before deadline.
✓Understand the changes to the categories/weighting, the increase in minimum participation to avoid a penalty, the new data completeness threshold and more.
✓ Plan to continuously improve. Scores in the 70-80 range may not exceed the performance threshold in the future.
✓ Reach out to Telligen QIO or SURS for assistance• CMS continues to support these programs
Takeaways for You!

42
Telligen
Sandy Swallow
515.223.2105
Michelle Brunsen
515.453.8180
Websites
• www.telligenqinqio.com
• www.telligenqpp.com
• www.qpp.cms.gov
THANK YOU!





























