Embed Size (px)
Citation preview

What works: Advances in Adolescent Substance AbuseTreatment and Research
Michael Dennis, Ph.D.
Chestnut Health Systems,
Bloomington, IL
Presentation for the SAMHSA National Policy Academy on Co-Occurring Mental and Substance Abuse Disorders, April 14-16, 2004, Baltimore, MD. The opinions are those of the author sdo not reflect official positions of the consortium or government . Available on line at www.chestnut.org/li/posters.

Examine the prevalence, course, and consequences of adolescent substance use
Summarize major trends in the adolescent treatment system
Review the current knowledge base on treatment effectiveness
Examine how characteristics and outcomes vary by level of care.
Goals of this Presentation

Change in Past Month Substance Use by Age
Source: Dennis (2002) and 1998 NHSDA.
0
10
20
30
40
50
60
70
80
90
10012
13
14
15
16
17
18
19
20
21
22-2
3
24-2
5
26-2
9
30-3
4
35-3
9
50-6
4
65 +
Age
Alcohol Use
Tobacco Use
Binge Alcohol use
Any Illicit Drug Use
Marijuana Use

Consequences of Substance Use
Source: Dennis, Godley and Titus (1999) and 1997 NHSDA.

Importance of Perceived Risk
Source: Office of Applied Studies. (2000). 1998 NHSDA
Mar
ijua
na
Use
Ris
k &
Ava
ilab
ilit
y

The Adolescent Treatment System
Less than 1/10th of adolescents with substance dependence problems receive treatment
Under 50% stay 6 weeks, 75% stay less than the 3 months recommended by NIDA
From 1992 to 1998, admissions to treatment increased 53% (96,787 to 147,899), but then leveled off in 1999 to 2002
From 1992 to 1998, admissions for treatment of primary, secondary or tertiary marijuana use disorders increased 115% (51,081 to 109,875)
Source: Dennis, Dwaud-Noursi, Muck, & McDermeit, 2003; Hser et al., 2001; OAS, 2000

Change in Adolescent Admissions (1992-1998)
Source: Dennis, Dawud-Noursi, Muck & McDermeit, 2003 and 1992-1998 Treatment Episode Data Set (TEDS)
0
20,00040,000
60,000
80,000
100,000120,000
140,000
160,000
Tot
al
(+53
%)
Mar
ijuan
a(+
115%
)
Alc
ohol
(+20
%)
Stim
ulan
ts(+
146%
)
Hal
luci
noge
ns(-
6%)
Coc
aine
(+35
%)
In
hala
nts
(-
41%
)
Opi
ates
(+13
5%)
Oth
er*
(+15
4%)
Ann
ual A
dmis
sion
s .
1992 admissions
1998 admissions
* including tranquilizers, sedatives and o-t-c

Patterns of Substance Use Problems
Alcohol Only9%
All Other Patterns
16%
Marijuana Only23%
Alcohol and
Marijuana52%
Source: Dennis, Dawud-Noursi, Muck & McDermeit, 2003 and 1998 Treatment Episode Data Set (TEDS)

Sources of Adolescent Referrals
Criminal Justice
System 44%
School/ Community Agency 22%
Self/Family 17%
Other Health Care Provider 5%
Other Substance
Abuse Treatment
Agency 5%
Other16%
Source: Dennis, Dawud-Noursi, Muck & McDermeit, 2003 and 1998 Treatment Episode Data Set (TEDS)

Level of Care at Admission
Intensive Outpatient
11%
Detox. or Hospital
5%
Short-Term Residential
6%
Long-Term Residential
9% Outpatient 68%
Source: Dennis, Dawud-Noursi, Muck & McDermeit, 2003 and 1998 Treatment Episode Data Set (TEDS)

Severity Varies by Level of Care
0%10%20%30%40%50%60%70%80%90%
100%
Weekly use atintake
Dependence First usedunder age 15
Prior Treatment
Outpatient (n=24704)Intensive Outpatient (n=4024)Detoxification or Hospital (n=2062)Short Term Residential (n=2046)Long Term Residential (n=3124)
Source: Dennis, Dawud-Noursi, Muck & McDermeit, 2003 and 1998 Treatment Episode Data Set (TEDS)

Relatively Small And New Literature
With over 65% of the studies first published in the past 5 years and over 3 dozen more currently in the field, we are entering a “renaissance of
knowledge” in this area.
Source: Dennis &, White (2003) at www.drugstrategies.org.

Key Lessons Effectiveness was associated with therapies that:
– were manual-guided and had developmentally appropriate materials– involved more quality assurance and clinical supervision– achieved therapeutic alliance and early positive outcomes– successfully engaged adolescents in aftercare, support groups, positive
peer reference groups, more supportive recovery environments Interventions that are associated with no or minimal change in substance
use or symptoms:– Passive referrals– Educational units alone – Probation services as usual– Unstandardized outpatient services as usual
Interventions associated with deterioration: – treatment of adolescents in “groups including one or more highly
deviant individuals” or that were mismanaged (but NOT all groups)– treatment of adolescents in adult units and/or with adult
models/materials (particularly outpatient)

Limitations of the Literature
Small sample sizes (most under 50) High rates (30-50%) of refusals by eligible people Unstandardized measures, no measures of abuse or
dependence, no measures of comorbidity Unstandardized and minimally-supervised therapies
(making replication very difficult) Minimal information on services received High rates (20-50%) of treatment dropout High rates of attrition from follow-up (25-54%) leading to
potentially large (unknown) bias

NIAAA/NIDA Other Grantees
CSAT/ NEW Adolescent Treatment Program Other Grantees and Collaborators (80+ sites)
CSATCannabis Youth Treatment (CYT)Adolescent Treatment Model (ATM)Strengthening Communities for Youth (SCY)Adolescent Residential Treatment (ART)Effective Adolescent Treatment (EAT)
Other CSAT Grantees
Other Collaborators
RWJF Reclaiming Futures Program
RWJF Other RWJF Grantees
Other Grants/Contracts
Source: www.chestnut.org/li/apss

Key Features
Pooled data over 3,500 and growing at over 1000/year Diverse samples with low (under 15%) refusal and attrition Use a common standardized measure – Global Appraisal of
Individual Needs (GAIN) with explicit measures of abuse, dependence, comorbidity, ASAM criteria and services received
Manualized interventions, including several experiments and replications of the same intervention across states (publicly available at www.chestnut.org/li/apss )
High treatment completion and follow-up rates (generally 80-90%)
Over 3 dozen people doing research on scales, case mix, matching rules, continuing care, and other topics.

Multiple Co-occurring Problems Are the Norm and Increase with Level of Care
Source: CSAT’s Cannabis Youth Treatment (CYT), Adolescent Treatment Model (ATM), and Persistent Effects of Treatment Study of Adolescents (PETS-A) studies
44
2125
21
70
47 43
7880
65
88
56
3635
68
445252
0
20
40
60
80
100
ConductDisorder
ADHD MajorDepressiveDisorder
GeneralizedAnxietyDisorder
TraumaticStress
Disorder
Any Co-OccuringDisorder
Outpatient Long Term Residential Short Term Residential

Severity is Related to Other Problems
71%
57%
25%
42%
30%37%
22%
5%
13%
22%
0%
20%
40%
60%
80%
100%
Health ProblemDistress*
Acute MentalDistress*
AcuteTraumaticDistress*
AttentionDeficit
HyperactivityDisorder*
ConductDisorder*
Past Year Dependence (n=278) Other (n=322)* p<.05
Source: Tims et al 2002

High Rates of Victimization
Source: Dennis (2004)
71
82 84
52
6973
45
5662
2519
37
0
10
20
30
40
50
60
70
80
90
100
OP/IOP (n=560) LTR (n=390) STR (n=594)
Lifetime History of Victimization Acute Victimization
Past Year Victimization Past 90 Day Victimization

Victimization is Related to Severity
Source: Titus, Dennis, et al., 2003

0
5
10
15
20
25
30
35
40
Pre Post
OP - No/Low Victimization OP - Acute Victimization
Resid - No/Low Resid- Acute Victimization
Interaction of Victimization and Treatment Setting on Days of Marijuana Use
Source: Funk, et al., 2003
Traumatized groups have higher severity
Both groups respond to residential treatment
High trauma group does not respond to OP

Illegal Activity (not just possession)
Source: Adolescent Treatment Model (ATM) data
7478
82
69 7168
86
65
8580 81 81
939395
0
10
20
30
40
50
60
70
80
90
100
OP/IOP (n=560) LTR (n=390) STR (n=594)
Any Illegal Activity Property crimes Interpersonal crimes
Drug related crimes Acts of Physical Violence

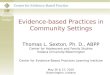
Change in Substance Frequency Indexby Level of Care\a
\a Source: Adolescent Treatment Model (ATM) data; Level of cares coded as Long Term Residential (LTR, n=390), Short Term Residential (STR, n=594), Outpatient/Intensive and Outpatient (OP/IOP, n=560);. T scores are normalized on the ATM outpatient intake mean and standard deviation. Significance (p<.05) marked as \t for time effect, \s for site effect, and \ts for time x site effect.
40
50
60
Intake 3 6 9 12
Months from Intake
STR\t,s,ts
LTR\t,ts
OP\t,s,ts

Change in Substance Problem Indexby Level of Care\a
\a Source: Adolescent Treatment Model (ATM) data; Level of cares coded as Long Term Residential (LTR, n=390), Short Term Residential (STR, n=594), Outpatient/Intensive and Outpatient (OP/IOP, n=560);. T scores are normalized on the ATM outpatient intake mean and standard deviation. Significance (p<.05) marked as \t for time effect, \s for site effect, and \ts for time x site effect.
Change in Substance Problem Index Past Month T-Score (TSPIM) by Level of Care\a
40
50
60
Intake 3 6 9 12
Months from Intake
STR\t,s,ts
LTR\t,s,ts
OP\t,s,ts

Percent in Recovery (no past month use or problems while living in the community)
\a Source: Adolescent Treatment Model (ATM) data; Level of cares coded as Long Term Residential (LTR, n=390), Short Term Residential (STR, n=594), Outpatient/Intensive and Outpatient (OP/IOP, n=560);. T scores are normalized on the ATM outpatient intake mean and standard deviation. Significance (p<.05) marked as \t for time effect, \s for site effect, and \ts for time x site effect.
0%
20%
40%
60%
80%
100%
Intake 3 6 9 12
Months from Intake
STR\t,s,ts
LTR\t,ts
OP\t,s

Change in Emotional Problem Indexby Level of Care\a
\a Source: Adolescent Treatment Model (ATM) data; Level of cares coded as Long Term Residential (LTR, n=390), Short Term Residential (STR, n=594), Outpatient/Intensive and Outpatient (OP/IOP, n=560);. T scores are normalized on the ATM outpatient intake mean and standard deviation. Significance (p<.05) marked as \t for time effect, \s for site effect, and \ts for time x site effect.
40
50
60
Intake 3 6 9 12
Months from Intake
STR\t,s,ts
LTR\t,s,ts
OP\t,s

Change in Illegal Activity Indexby Level of Care\a
\a Source: Adolescent Treatment Model (ATM) data; Level of cares coded as Long Term Residential (LTR, n=390), Short Term Residential (STR, n=594), Outpatient/Intensive and Outpatient (OP/IOP, n=560);. T scores are normalized on the ATM outpatient intake mean and standard deviation. Significance (p<.05) marked as \t for time effect, \s for site effect, and \ts for time x site effect.
40
50
60
Intake 3 6 9 12
Months from Intake
STR\t,s,ts
LTR\t,ts
OP\s

270180900
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.10.0
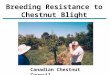
Reducing Relapse After Residential Treatment
Source: Godley et al 2002Days to First Marijuana Use (p<.05)
Per
cent
Rem
aini
ng A
bstin
ent
Usual Continuing Care
Assertive Continuing Care

Concluding Comments
We are entering a renaissance of new knowledge in this area, but are only reaching 1 of 10 in need
Several interventions work, but 2/3 of the adolescents are still having problems 12 months later
We need to move beyond focusing on minor variations in therapy (behavioral brand names) and acute episodes of care to focus on continuing care and a recovery management paradigm
It is very difficult to predict exactly who will relapse so it is essential to conduct aftercare monitoring with all adolescents

Resources Copy of these slides and handouts
– http://www.chestnut.org/LI/Posters/
Assessment Instruments – CSAT TIP 3 at http://www.athealth.com/practitioner/ceduc/health_tip31k.html– NIAAA Assessment Handbook,http://www.niaaa.nih.gov/publications/instable.htm
Adolescent Treatment Manuals– NCADI at www.health.org or www.chestnut.org/li/bookstore– CSAT CYT, ATM and other manuals at www.chestnut.org/li/apss/csat/protocols
Adolescent Treatment Programs and Studies – List of programs by state and summary of pre-2002 studies at www.drugstrategies.com – Cannabis Youth Treatment (CYT) : www.chestnut.org/li/cyt – Persistent Effects of Treatment Study of Adolescents (PETSA):
www.samhsa.gov/centers/csat/csat.html (then select PETS from program resources)– Adolescent Program Support Site (APSS): www.chestnut.org/li/apss
Society for Adolescent Substance Abuse Treatment Effectiveness (SASATE)– Website at www.chestnut.org/li/apss/sasate with bibliography – E-mail Darren Fulmore <[email protected]> to be added to list server– Next conference is June 18, 2004, See website or E-mail Joan Unsicker
<[email protected]> for information about about meeting

ReferencesBukstein, O.G., & Kithas, J. (2002) Pharmacologic treatment of substance abuse disorders. In Rosenberg, D., Davanzo, P., Gershon, S.
(Eds.), Pharmacotherapy for Child and Adolescent Psychiatric Disorders, Second Edition, Revised and Expanded. NY, NY: Marcel Dekker, Inc.Dennis, M.L., (2002). Treatment Research on Adolescents Drug and Alcohol Abuse: Despite Progress, Many Challenges Remain.
Connections, May, 1-2,7, and Data from the OAS 1999 National Household Survey on Drug AbuseDennis, M.L. (2004). Traumatic victimization among adolescents in substance abuse treatment: Time to stop ignoring the elephant in our
counseling rooms. Counselor, April, 36-40.Dennis, M.L., & Adams, L. (2001). Bloomington Junior High School (BJHS) 2000 Youth Survey: Main Findings. Bloomington, IL: Chestnut
Health Systems Dennis, M.L., Dawud-Noursi, S., Muck, R., & McDermeit, M. (2003). The need for developing and evaluating adolescent treatment models.
In S.J. Stevens & A.R. Morral (Eds.), Adolescent substance abuse treatment in the United States: Exemplary Models from a National Evaluation Study (pp. 3-34). Binghamton, NY: Haworth Press and 1998 NHSDA.
Dennis, M. L., Godley, S. H., Diamond, G., Tims, F. M., Babor, T., Donaldson, J., Liddle, H., Titus, J. C., Kaminer, Y., Webb, C., Hamilton, N., & Funk, R. (in press). The Cannabis Youth Treatment (CYT) Study: Main Findings from Two Randomized Trials. Journal of Substance Abuse Treatment.
Dennis, M. L., Godley, S. and Titus, J. (1999). Co-occurring psychiatric problems among adolescents: Variations by treatment, level of care and gender. TIE Communiqué (pp. 5-8 and 16). Rockville, MD: Substance Abuse and Mental Health Services Administration, Center for Substance Abuse Treatment.
Dennis, M. L., Perl, H. I., Huebner, R. B., & McLellan, A. T. (2000). Twenty-five strategies for improving the design, implementation and analysis of health services research related to alcohol and other drug abuse treatment. Addiction, 95, S281-S308.
Dennis, M. L. and McGeary, K. A. (1999). Adolescent alcohol and marijuana treatment: Kids need it now. TIE Communiqué (pp. 10-12). Rockville, MD: Substance Abuse and Mental Health Services Administration, Center for Substance Abuse Treatment.Dennis, M. L., Titus, J. C., Diamond, G., Donaldson, J., Godley, S. H., Tims, F., Webb, C., Kaminer, Y., Babor, T., Roebeck, M. C., Godley,
M. D., Hamilton, N., Liddle, H., Scott, C., & CYT Steering Committee. (in press). The Cannabis Youth Treatment (CYT) experiment Rationale, study design, and analysis plans. Addiction, 97, 16-34..
Dennis, M.L., & White, M.K. (2003). The effectiveness of adolescent substance abuse treatment: a brief summary of studies through 2001, (prepared for Drug Strategies adolescent treatment handbook). Bloomington, IL: Chestnut Health Systems. [On line] Available at http://www.drugstrategies.org

ReferencesDennis, M.L. & White,M.A. (2003). The effectiveness of adolescent substance abuse treatment: a brief summary of studies through
2002. Washington, DC: Drug Strategies. Retrived from www.drugstrategies.com . Funk, R. R., McDermeit, M., Godley, S. H., & Adams, L. (2003). Maltreatment issues by level of adolescent substance abuse treatment
The extent of the problem at intake and relationship to early outcomes. Journal of Child Maltreatment, 8, 36-45.Godley, M. D., Godley, S. H., Dennis, M. L., Funk, R., & Passetti, L. (2002). Preliminary outcomes from the assertive continuing care
experiment for adolescents discharged from residential treatment. Journal of Substance Abuse Treatment, 23, 21-32.Godley, M., Godley, S., Dennis, M., Funk, R. & Passetti, L. (2002). Findings from the Assertive Continuing Care Experiment.
Presentation at the American Public Health Association annual conference, Philadelphia, PA November 11, 2002. Hser, Y., Grella, C. E., Hubbard, R. L., Hsieh, S. C., Fletcher, B. W., Brown, B. S., & Anglin, M. D. (2001). An evaluation of drug
treatments for adolescents in four U.S. cities. Archives of General Psychiatry, 58, 689-695.Lewinsohn, P.M., Hops, H., Roberts, R.E., Seeley, J.R., Andrews, J.A. (1993). Adolescent psychopathology, I: prevalence and
incidence of depression and other DSM-III-R disorders in high school students. J Abn Psychol, 102, 133-144. National Academy of Sciences (1994). Reducing risks for mental disorders: Frontiers for preventive intervention research.
Washington, DC: National Academy Press.Office of Applied Studies. (2000). National Household Survey on Drug Abuse: Main Findings 1998. Rockville, MD: Substance Abuse
and Mental Health Services Administration. Retrieved, from http://www.samhsa.gov/statistics.Office of Applied Studies (OAS) (1999). Treatment Episode Data Set (TEDS) 1992-1997: National admissions to substance abuse
treatment services. Rockville, MD: Author. [Available online at <http://www.icpsr.umich.edu/SAMHDA>.]Office of Applied Studies (OAS) (2000). Treatment Episode Data Set (TEDS) 1993-1998: National admissions to substance abuse
treatment services. Rockville, MD: Author. [Available on line at <http://www.icpsr.umich.edu/SAMHDA.html>.]Office of Applied Studies. (2000). National Household Survey on Drug Abuse: Main Findings 1998. Rockville, MD: Substance Abuse
and Mental Health Services Administration. Retrieved, from http://www.samhsa.gov/statisticsTims, F. M., Dennis, M. L., Hamilton, N., Buchan, B. J., Diamond, G. S., Funk, R., & Brantley, L. B. (2002). Characteristics and
problems of 600 adolescent cannabis abusers in outpatient treatment . Addiction, 97, 46-57.Titus, J. C., Dennis, M. L., White, W. L., Scott, C. K., & Funk, R. R. (2003). Gender differences in victimization severity and outcomes
among adolescents treated for substance abuse. Journal of Child Maltreatment, 8, 19-35.

Contact Information
Michael L. Dennis, Ph.D., Senior Research PsychologistLighthouse Institute, Chestnut Health Systems720 West Chestnut, Bloomington, IL 61701Phone: (309) 827-6026, Fax: (309) 829-4661E-Mail: [email protected]