Embed Size (px)
Citation preview

What will the Affordable Care Act do for me?!

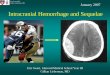
Neuroimaging of
Intracranial Hemorrhage
Lee Madeline, MD
November 2, 2013

Much of this talk pilfered from
◦ The Net

Role of Imaging
To recognize the presence of blood
To localize and differentiate hemorrhages
◦ (SAH, SDH, EDH)
To determine the age of the hemorrhage
To identify the etiology
◦ Exclude stroke mimic (tumor, etc.)
To aid in ascertaining the patient's prognosis

Neuroimaging of ICH
Appearance on CT
Appearance on MRI
Etiology for ICH
◦ Intracerebral
◦ Extracerebral
All in just 30 minutes!

ICH: Appearance on CT
Density of Tissue Gray Scale • air black
• fat darker gray
• CSF gray
• brain lighter gray
• acute blood, contrast white
• bone very white

Hemorrhage on CT
IPH SAH SDH EDH

Mutifocal hemorrhagic contusions

Subacute: Isodense Subdural

ICH: Appearance on MRI
Depend on …
the age of the hematoma
imaging sequence or parameters
site of the hemorrhage (“faster” IPH)
local partial pressure of oxygen in the tissues (hypoxic)
the local pH (acidic)
pt’s hematocrit
local glucose concentration
hemoglobin concentration
integrity of the BBB
the patient's temp (hyper)

Stages of Hemorrhage
As a hematoma ages, hemoglobin changes
through several forms
◦ Oxyhemoglobin
◦ Deoxyhemoglobin
◦ Methemoglobin
◦ Then RBCs are broken down into
Ferritin
Hemosiderin

Stages of Hemorrhage
Phase Time Hemoglobin,
Location
Hyperacute < 24 h Oxyhemoglobin,
intracellular
Acute 1-3 d Deoxyhemoglobin,
intracellular
Early subacute >3 d Methemoglobin,
intracellular
Late subacute >7 d Methemoglobin,
extracellular
Chronic >14 d Ferritin and hemosiderin,
extracellular

Evolution of Hemorrhage on MRI
Phase Time
Hemoglobin,
Location
Appearance
T1-
Weighted
MRI
T2-
Weighted
MRI
Hyperacute < 24 h Oxyhemoglobin,
intracellular
Isointense or
hypointense
Hyperintense
Acute 1-3 d Deoxyhemoglobin,
intracellular
Isointense Hypointense
Early
subacute
>3 d Methemoglobin,
intracellular
Hyperintense Hypointense
Late subacute >7 d Methemoglobin,
extracellular
Hyperintense Hyperintense
Chronic >14 d Ferritin and
hemosiderin,
extracellular
Hypointense Hypointense
“I D / B D / B B / D D”

Hyperacute (<24h)
Right external capsule and insular cortex in a known hypertensive patient
T1 isointense to hypointense
T2 hyperintense
I “B”D / B D / B B / D D

Acute (1-3d)
T1 iso to hypodense
T2 hypointense
I D / B D / B B / D D

Early Subacute (>3d)
T1 hyperintense
T2 hypointense
I D / B D / B B / D D

Late Subacute (>7d)
Late Subacute hemorrhage bithalamic regions in a pt with known cerebral malaria.
T1 hyperintense
T2 hyperintense
T2 (and GRE) hypointense rim due to hemosiderin.
I D / B D / B B / D D

Chronic (>14d)
The hematoma shows a large medial subacute component and a small lateral chronic component.
The chronic component (arrow) is hypointense on both T1 and T2.
This hypointensity is enhanced due to the blooming effect of blood on GRE.
I D / B D / B B / D D

Cavernous Malformation
Characteristic “popcorn appearance” on MRI

Intracranial Hemorrhage
8-13% of all strokes
More likely to result in death or major
disability than ischemic stroke
Annually, more than 20,000 individuals in
the US die from ICH
ICH has a 30-day mortality rate of 44%


ICH: Categorize by Cause
Drug abuse
Moyamoya
Sickle cell disease
Eclampsia or postpartum
vasculopathy
Infection
Vasculitis
Hypertension
Vascular malformations
Aneurysmal SAH
Cerebral amyloid angiopathy
Intracranial neoplasm
Coagulopathy
Hemorrhagic transformation
of an ischemic infarct
Cerebral venous
thrombosis
Trauma (SDH/EDH) > Non Traumatic

Cerebral Hemorrhage Categorized by etiology
Intracranial Bleeds
◦ hypertensive bleeds
◦ hemorrhagic transformation of ischemic infarction
◦ cerebral amyloid angiopathy
◦ aneurysmal SAH
Extraaxial Fluid Collections
◦ EDH / SDH

Hypertensive Bleeds
most common cause of nontraumatic
intraparenchymal hemorrhage in the brain
Chang

Hypertensive Hemorrhage
Pathophysiology
◦ degenerative cerebral microangiopathy
characterized by hyalinization of the walls of small
arterioles and, ultimately, fibrinoid necrosis.
Charcot- Bouchard aneurysms

Hypertensive Bleeds
Location
◦ putamen/external capsule,
60-65%
◦ thalamus, 15- 25%
◦ pons and brainstem, 5-10%
◦ cerebellum, 2-5%
◦ cerebral hemispheres, 1-2%
IV extension in 50%
Men have 5-20% higher
incidence Osborn

HTN Bleed in Cerebellum
62 yo with HTN with acute onset of ataxia and confusion
CT T2
Acute = Dark on T2

47 yo with HTN bleed in BS

Cerebral Hemorrhage
Intracranial Bleeds
◦ hypertensive bleeds
◦ hemorrhagic transformation of ischemic infarction
◦ cerebral amyloid angiopathy
◦ aneurysmal SAH
Extraaxial Fluid Collections
◦ EDH / SDH

Hemorrhagic Transformation of
Brain Infarction
Infarcted brain has a propensity to bleed, particularly
when reperfused in the acute phase.
Hemorrhage due to brain infarction may be recognized
b/o assoc cytotoxic edema that conforms to an arterial
territory.
◦ assoc may be difficult to diagnose when early massive
bleeding obscures the underlying infarct.

Baseline CT < 3 hrs
Hemorrhagic Transformation of
Ischemic Infarction

Day 1 CT s/p TPA
Hemorrhagic Transformation of
Ischemic Infarction

Cerebral Hemorrhage
Intracranial Bleeds
◦ hypertensive bleeds
◦ hemorrhagic transformation of ischemic infarction
◦ cerebral amyloid angiopathy
◦ aneurysmal SAH
Extraaxial Fluid Collections
◦ EDH / SDH

Cerebral Amyloid Angiopathy
Pathophysiology
◦ Deposition of beta-amyloid in the arterial media and/or
adventitia of small arterioles
◦ Cerebrum > cerebellum
◦ Dissection into
SAS is common,
Ventricular extension is uncommon.
◦ In elderly, lobar ICH and multiple microbleeds are highly
suggestive of CAA.
◦ not associated with systemic amyloidosis
◦ although most cases are sporadic, familial forms exist

Amyloid Angiopathy
Amyloid is a protein that infiltrates vessel walls, replaces
smooth muscle cells in the media, and may make the vessel structurally
brittle.

Amyloid Angiopathy
20 months later 6 weeks later
65 yo with multiple intracerebral hemorrhages
Initial

Cerebral Amyloid Angiopathy
Prognosis
◦ Lobar ICH is assoc w a lower mortality rate (11-
32%) and a better functional outcome than
hypertensive deep ganglionic bleeds
◦ Of individuals with CAA-related hemorrhage, 25-40%
have a recurrence
highest risk in the first year
Merino

Cerebral Hemorrhage
Intracranial Bleeds
◦ hypertensive bleeds
◦ hemorrhagic transformation of ischemic infarction
◦ cerebral amyloid angiopathy
◦ aneurysmal SAH
Extraaxial Fluid Collections
◦ EDH / SDH

SAH Etiology
Overall, head trauma is the most common
cause of SAH
80% of nontraumatic SAH results from
ruptured aneurysms
Less common causes:
mycotic aneurysm
AVM
infection
hemorrhagic disease

SAH Presentation
sudden onset of the “worst headache of my life”
frequently followed by photophobia, nausea, and vomiting
most common in those aged 40-65 ◦ blacks have 2.1 times greater risk
◦ slightly higher in women than men
annual incidence of aneurysmal SAH is 6-25 per 100,000
>27,000 Americans suffer ruptured intracranial aneurysms each year

SAH from basilar tip aneurysm
Pattern of SAH:
“Aneurysmal”

SAH from ruptured MCA aneurysm
Pattern of SAH:
“Aneurysmal”

Pattern of SAH:
Perimesencephalic Low rate of re-hemorrhage
Lower rate of Sx vasospasm
Venous hemorrhage

SAH Morbidity/Mortality
10-15% of pts die before reaching hospital
mortality rate reaches as high as 40% within
the first week
Rebleed carries a mortality rate of 75%
about half die in the first 6 mo
> 1/3 have major neurologic deficits
25% multiple

SAH Pathophysiology
Aneurysms are acquired lesions related to
hemodynamic stress on the arterial walls at
bifurcation points and bends
Saccular aneurysms are specific to the
intracranial arteries b/c walls lack an external
elastic lamina and contain a very thin
adventitia—factors that may predispose to
the formation of aneurysms
lie unsupported in the SA space

Mycotic Aneurysms
any aneurysm that results from an infectious
process involving the arterial wall
Bacterial endocarditis 80%
2-4% of all intracranial aneurysms
occur with greater freq in children
often are found on vessels distal to CoW
fusiform morphology and are usually v friable
Peripheral and multiple

Mycotic Aneurysm

SAH
Intracranial aneurysms classified to
according to
◦ gross pathologic appearance
◦ location
3 types
◦ saccular or berry aneuryms
◦ fusiform
◦ dissecting aneurysms
Osborn

Fusiform Aneurysm
Elongated aneurysm caused by
atherosclerotic disease
Usually located in vertebrobasilar system
Present in older patients
Can contain thrombus and calcification
Saccular Fusiform

Dissecting Aneurysm
Following a dissection an intramural hematoma results
in a saclike outpouching
Etiology:
◦ trauma>vasculopathy (SLE, FMD)>spontaneous
dissection
Location: extracranial ICA, VA
High incidence of hemorrhage
Osborn

Dissecting Aneurysm
NANG: elongated contrast collection beyond vessel lumen

SAH and IVH
SAH and IVH differ from IPH, SDH and EDH in that
they are mixed with CSF.
Like EDHs and SDHs, SAHs have high oxygen levels;
therefore, they age more slowly than IPH.
In cases of mild SAH, RBCs may be resorbed by the
time notable methemoglobin formation occurs.
Therefore, T1 shortening is seldom seen.
… CT is advocated for the early diagnosis of SAH.

SAH and IVH

SAH and IVH on MRI
FLAIR is the most sensitive MRI sequence for detecting
SAH.
◦ SAH appears as high SI c/t normally hypointense CSF
T2- and T2* can potentially demonstrate SAH as an area
of low signal in normally hyperintense SA spaces.
On T1, acute SAH may appear as intermediate or high
signal in the SA space. (Less sensitive)
In chronic and repeated SAH, hemosiderin may stain the
leptomeninges, leading decreased signal known as
superficial siderosis.

Hemosiderosis from prior SAH on MRI

SAH and IVH
MRA useful in the evaluation of aneurysms and other
vascular lesions.
CTA may be adequate for identifying and characterizing
lesions without a need for catheter DSA in the acute
phase of the illness.
Primary IVH is rare
◦ HTN
◦ Acomm Aneurysm
◦ Anticoagulation
◦ Vascular malformation
◦ Moyamoya disease
◦ IV tumors

Cerebral Hemorrhage
Intracranial Bleeds
◦ hypertensive bleeds
◦ hemorrhagic transformation of ischemic infarction
◦ cerebral amyloid angiopathy
◦ aneurysmal SAH
Extraaxial Fluid Collections
◦ EDH / SDH

SDH and EDH
Because the dura is well vascularized and because O2 tension
remains high, progression from one stage to another is slower in SDH /
EDH than IPH.
First 4 stages same as those for IPH.
The chronic stage characterized by continued oxidative
denaturation of methemoglobin.
◦ No hemosiderin rim is seen in the surrounding hematoma and
no tissue macrophages are present.
EDHs are differentiated from SDH on the basis of their classic
biconvexity versus medially concavity

SDH dissecting
down from the
head
EDH from
Catheter

SDH – Late Subacute
isodense on CT Bright / Bright

Mimics for Hemorrhage
… hyperintensity on T1 Melanin:
◦ Mets from melanoma less commonly display susceptibility on GRE, and they
typically show some contrast enhancement.
Fat:
◦ Use of fat-suppression techniques can help differentiate fat from hemorrhage.
◦ Presence of a chemical shift artifact may also indicate a fatty lesion.
Hem Mets:
◦ Contrast enhancement, which is not seen in bland hematomas.
Calcification:
◦ Differences in the morphology
◦ CT may also help differentiate these entities
Gadolinium
Diffuse Cerebral Edema

SAH Mimic: Diffuse hypoxic ischemic brain
injury

Conclusion
As hemorrhage evolves, it passes through 5 well-defined and easily
identified stages, as seen on MRI.
◦ Knowledge of these stages may be useful for dating a single
hemorrhagic event or for ascertaining if multiple hemorrhagic
events occurred at different times.
CT more sensitive for detecting hyperacute parenchymal
hemorrhage or early SAH or IVH
MRI more sensitive after 12-24 hours.
MRI is also more specific than CT in determining the age of a
hemorrhage.
Both T1and T2 MRI used to adequately characterize and stage a
hemorrhage.
◦ I D / B D / B B / D D

Thank You!
Photo Bomb