Embed Size (px)
Citation preview

What Might Cause Postural Tachycardia Syndrome (POTS)? &
What Might we Learn from Research to Benefit Patients?
Satish R Raj MD MSCI FACC FHRSProfessor of Cardiac Sciences
Libin Cardiovascular Institute of AlbertaAdjunct Associate Professor of MedicineVanderbilt University Medicine Center
Heart Rhythm Congress, Birmingham, UKOctober 2018

POTS is the‘final common pathway’of hundreds of genetic and acquired
autonomic and cardiovascular entities- David Robertson
David Robertson
What Causes POTS?

Pathophysiology of POTS
Satish

Multiple Pathophysiologies in POTS
• Mast Cell Activation
• Partial Autonomic Neuropathy
• Leg Blood Flow Abnormalities
• Hypovolemia
• Hyperadrenergic
– Increased Release
– Decreased Clearance
• Antibodies are Evil…

Blood Volume & Renin-Angiotensin-
Aldosterone System in POTS
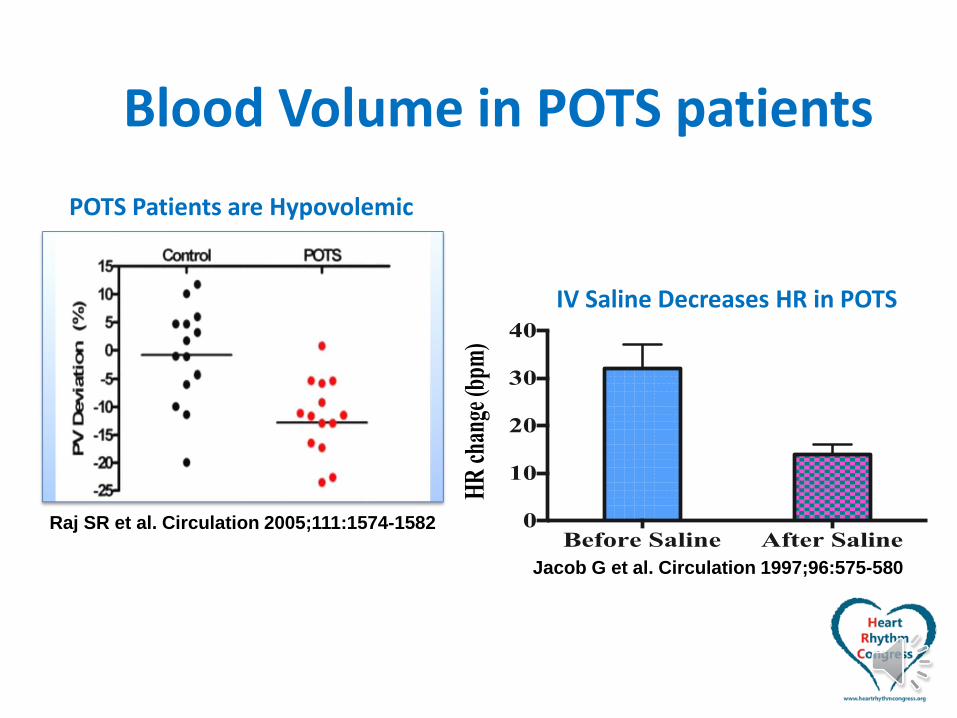
Blood Volume in POTS patients
Raj SR et al. Circulation 2005;111:1574-1582
POTS Patients are Hypovolemic
HR
cha
nge
(bpm
)
Before Saline After Saline0
10
20
30
40
Jacob G et al. Circulation 1997;96:575-580
IV Saline Decreases HR in POTS
Water and Salt Intake: Common Advice
• Increase salt intake
– Up to 10g/day
– Dietary if possible
– Tablets as needed
• NaCl 1gm tablets
• Salt Stick 250mg buffered tablets
• Increase fluid intake
– 2-3 Liters (8-12 cups) per day
“In God we Trust; All others must bring data.”
- Unknown
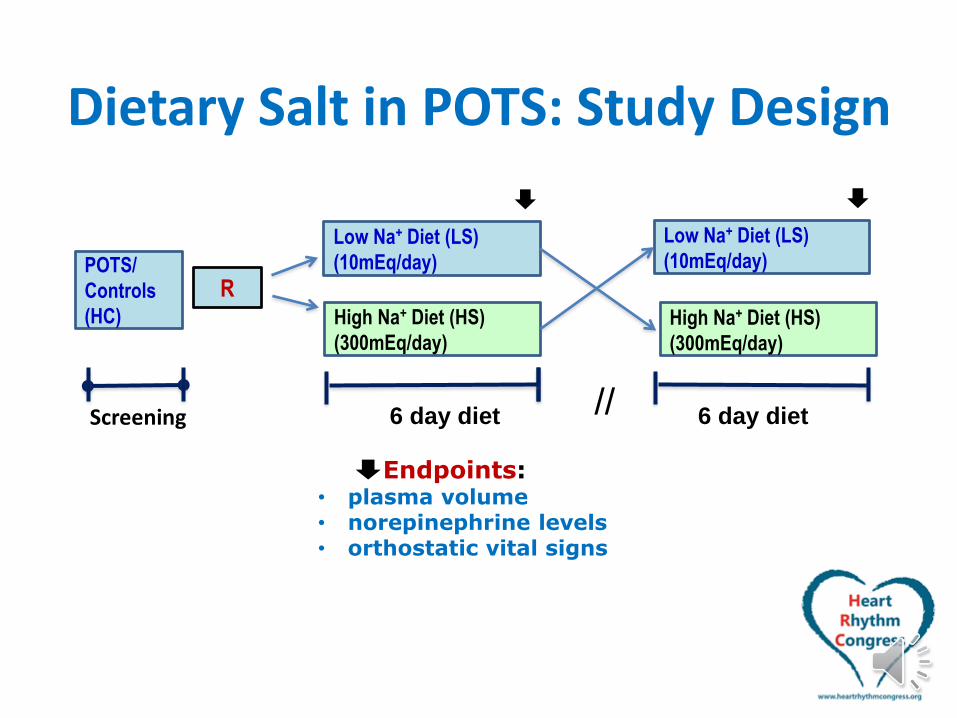
Dietary Salt in POTS: Study Design
Low Na+ Diet (LS)
(10mEq/day)
High Na+ Diet (HS)
(300mEq/day)
Low Na+ Diet (LS)
(10mEq/day)
R
ScreeningH&PPlasma Volume
6 day diet 6 day diet//
POTS/
Controls
(HC)
Endpoints: • plasma volume• norepinephrine levels • orthostatic vital signs
High Na+ Diet (HS)
(300mEq/day)

Dietary Salt in POTS: Demographics
POTS(n=14) Controls(n=13) P Value
Age, years 35±2 31±2 0.98
BMI, kg/m2 23±1 24±1 0.577
Na, mEq/l 140±0.29 138±0.42 0.002*
K, mEq/l 3.80±0.07 3.95±0.07 0.082
Cl, mEq/l 107±0.55 106±0.43 0.141
Glucose, mg/dl 87.8±5.38 82.2±2.94 0.512
BUN, mg/dl 10.8±0.73 11.1±0.87 0.883
Cr, mg/dl 0.74±0.02 0.74±0.03 0.789
Hematocrit, % 39±0.76 40±0.45 0.17
Hemoglobin, g/dl 13.1±0.25 13.3±0.15 0.511
Carbon Monoxide-technique Blood Volume
Total blood volume, ml 5139±283 5804±237 0.031*
Red blood cell volume, ml 1951±115 2133±77 0.031*
Plasma volume, ml 3188±174 3671±167 0.02*
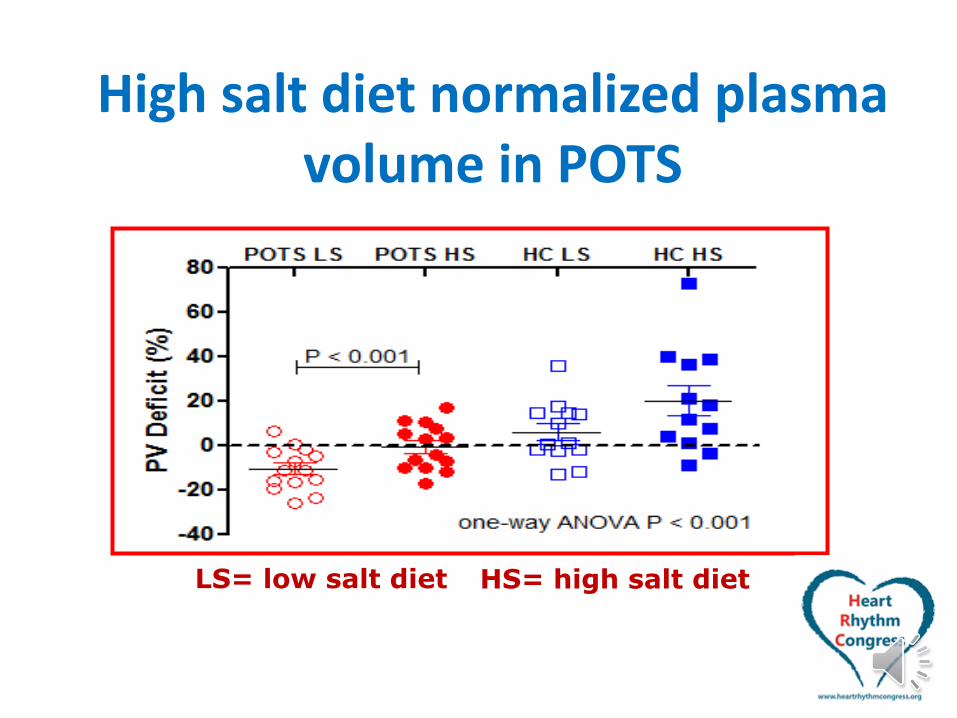
High salt diet normalized plasma volume in POTS
HS= high salt dietLS= low salt diet
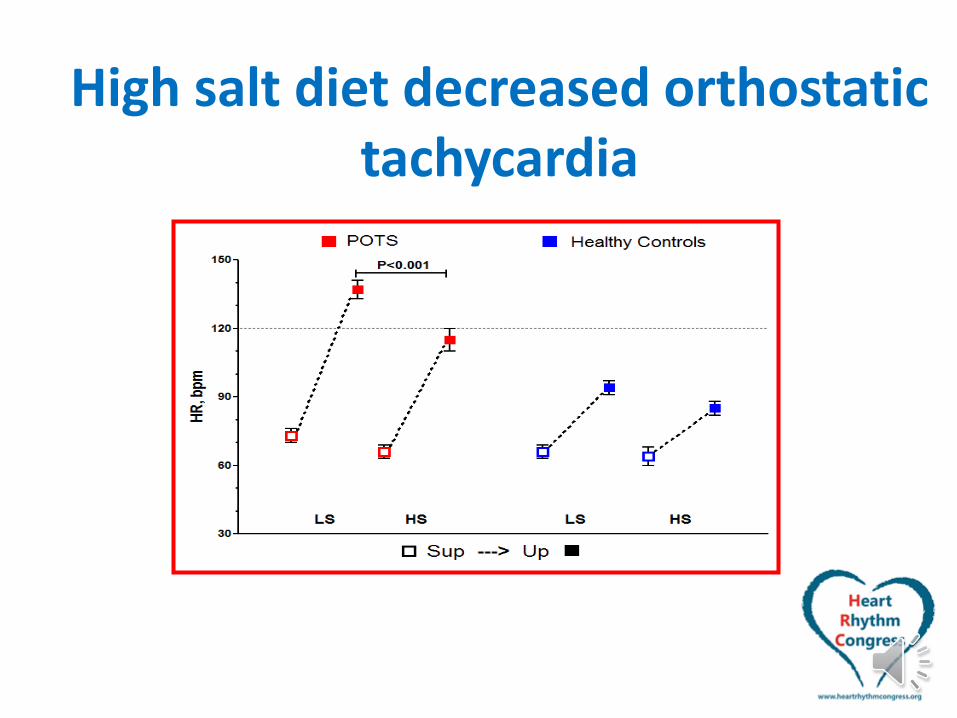
High salt diet decreased orthostatic tachycardia
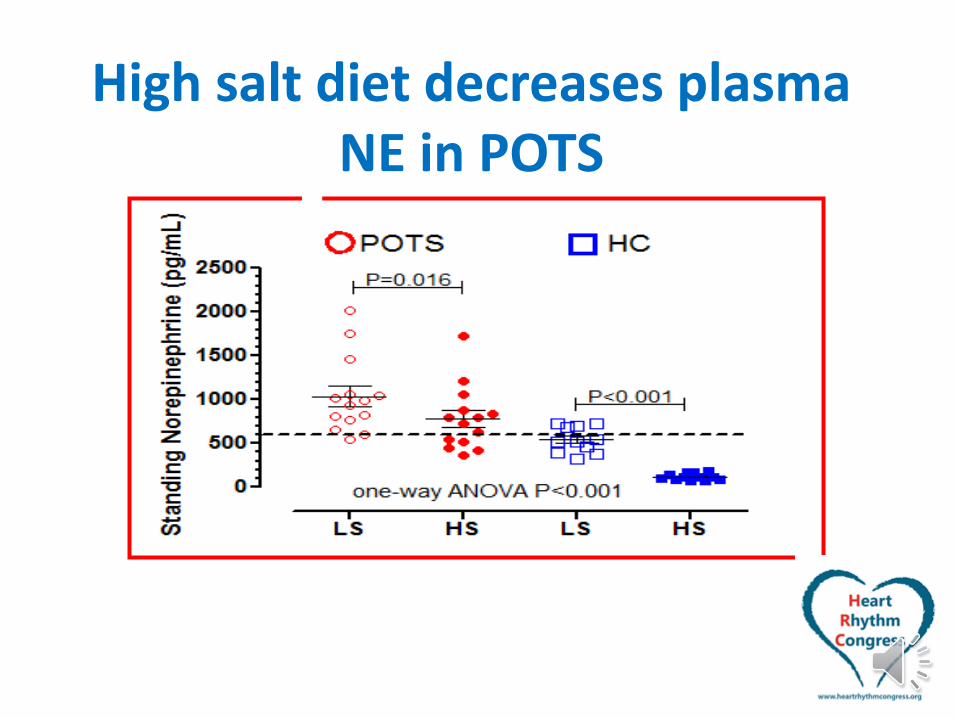
High salt diet decreases plasma NE in POTS
Dietary Salt in POTS: Summary• In POTS patients, a HIGH SALT DIET
– Increases plasma volume
– Decreases standing plasma norepinephrine
– Decreases orthostatic tachycardia
• HOWEVER, this did not normalize POTS patients
• POTS patients on a HIGH SALT DIET physiologically resemble Healthy subjects on a LOW SALT DIET

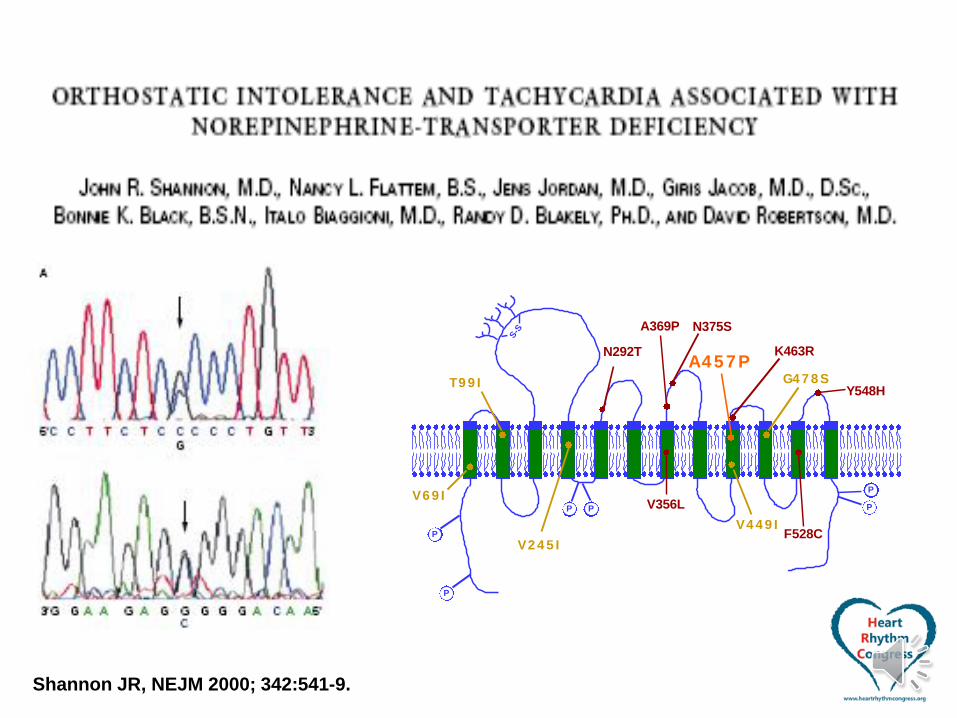
Hyperadrenergic POTS – Decreased NE Clearance
Shannon JR, NEJM 2000; 342:541-9.

Muscle Sympathetic Nerve Activity and Plasma NE
Shannon JR, NEJM 2000; 342:541-9.
Electrochemical Dissociation%
of
Su
pin
e V
alu
e
MSNA [NE] MSNA [NE]0
100
200
300
400
500
Supine
Upright
Normal Patient
Shannon JR, NEJM 2000; 342:541-9.
.
P
P P P
P
S-S
P
V6 9 I
T9 9 I
V2 4 5 I
V4 4 9 I
G4 7 8 S
A4 5 7 PN292T
V356L
A369P N375S
K463R
F528C
Y548H
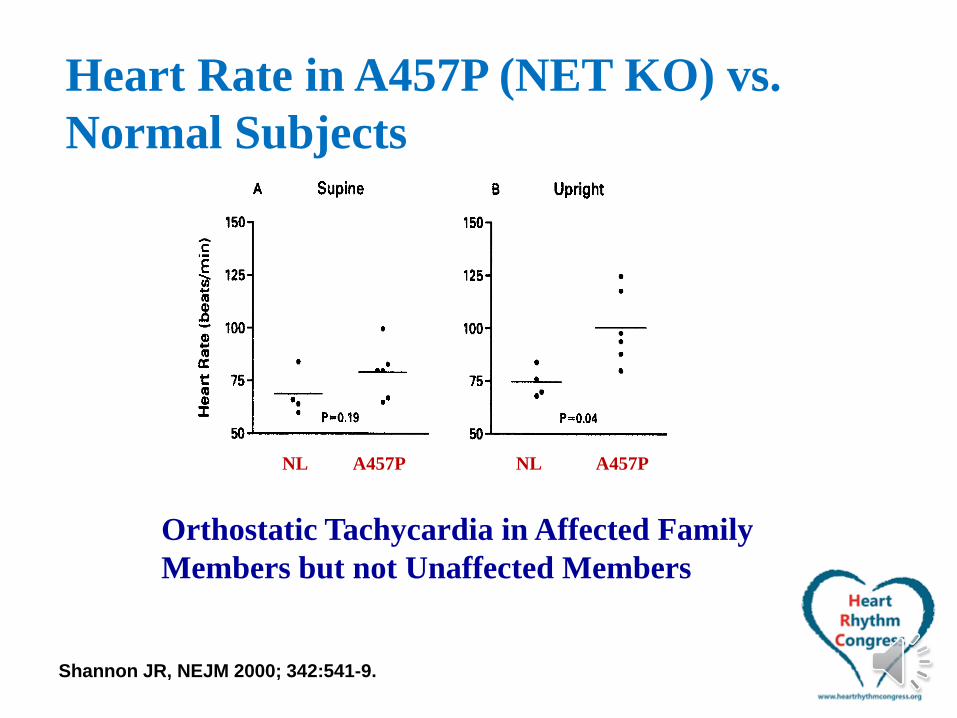
NL A457P NL A457P
Heart Rate in A457P (NET KO) vs.
Normal Subjects
Orthostatic Tachycardia in Affected Family
Members but not Unaffected Members
Shannon JR, NEJM 2000; 342:541-9.

A Norepinephrine Synapse
NET
Slide courtesy of
Alex Nackenoff
(Vanderbilt)

A Norepinephrine Synapse
NET
Slide courtesy of
Alex Nackenoff
(Vanderbilt)
SNS
Tone
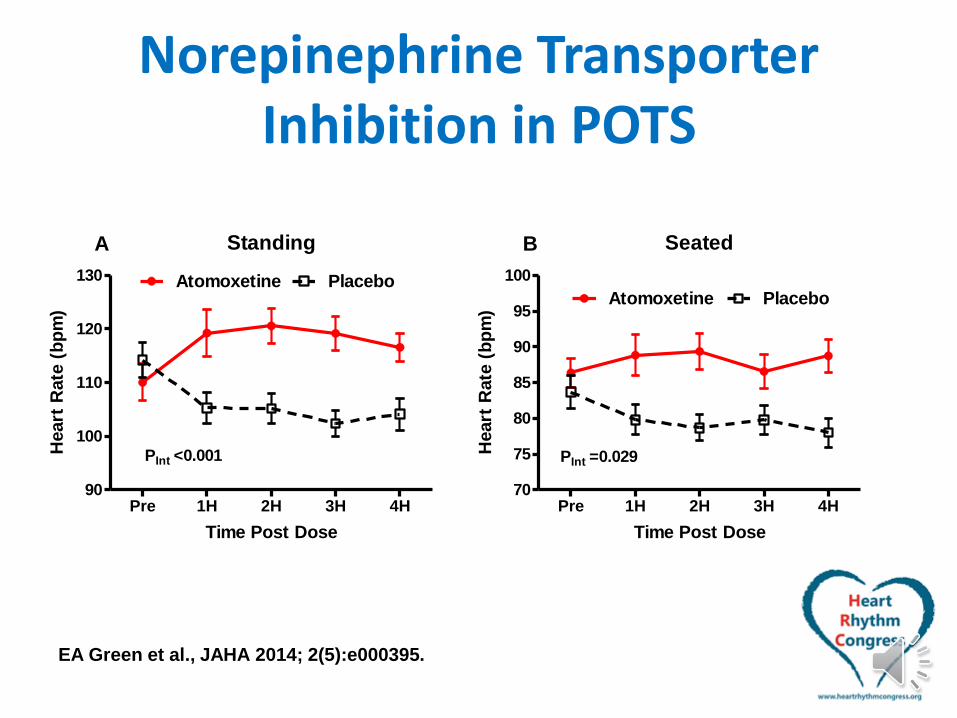
Norepinephrine Transporter Inhibition in POTS
Standing
Pre 1H 2H 3H 4H90
100
110
120
130 Atomoxetine Placebo
PInt <0.001
A
Time Post Dose
Heart
Rate
(b
pm
)
Seated
Pre 1H 2H 3H 4H70
75
80
85
90
95
100
PInt =0.029
B
PlaceboAtomoxetine
Time Post Dose
Heart
Rate
(b
pm
)
EA Green et al., JAHA 2014; 2(5):e000395.

Norepinephrine Transporter Inhibition in POTS
Orthostatic Change
Pre 1H 2H 3H 4H15
20
25
30
35
40 Atomoxetine Placebo
PInt =0.001
C
Time Post Dose
H
eart
Rate
(b
pm
)
Symptoms: 0 to 2h
Atomoxetine Placebo
-8
-6
-4
-2
0
2
4
6
P =0.028
Sym
pto
ms S
co
re (
a.u
.)
EA Green et al., JAHA 2014; 2(5):e000395.
Role of Adrenergic Autoantibodies in POTS
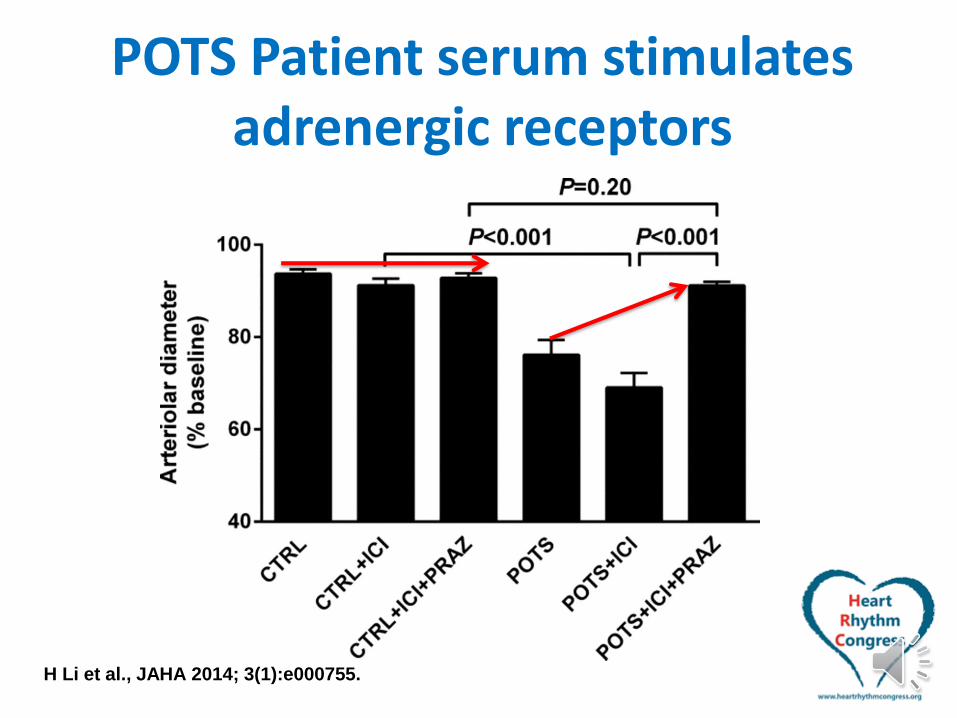
POTS Patient serum stimulates adrenergic receptors
H Li et al., JAHA 2014; 3(1):e000755.
POTS Adrenergic Ab - Summary
• POTS IgG in vitro has:
– Alpha-1 Partial Agonist
– Beta-1 Agonist
– Beta-2 Agonist
• This has now been repeated in a different patient cohort
• Do these antibodies have activity in vivo?
– Ongoing Study; Enrollment now open

POTS – Take Home Messages• Research in POTS
– Helps us to understand WHAT IS
WRONG
– Sometimes leads to RATIONAL
TREATMENTS
• Treatment
– High Salt Diet can make things better
– NET inhibitors can make things worse
– Autoantibodies MAY be bad for you

Questions?





























