Embed Size (px)
Citation preview

What is the position of NOACs in
acute coronary syndromes amp
secondary prevention
Ron Peters
Academic Medical Center
Amsterdam
the Netherlands
Part 1
Coronary disease
no other indication
for anticoagulant therapy
50
60
70
80
90
100
0 1 2 3 4 5 6
Months after hospital discharge
S
urv
ivin
g
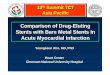
STEMI Non-STEMI UA
Survival Rate 6 Months Post Discharge for
STEMI NSTEMI and UA Patients
Goldberg RJ et alAm J Cardiol 200493288-93
OASIS 5 follow-up
N Engl J Med 2006 3541464-1476
N Engl J Med 2002347969-9
Composite of death reinfarction and stroke
10
Circulation 2002Feb 5105(5)557-63
Haq et al Am J Med 2010123250-258
Sorensen R et al Lancet 2009374 1967-1974
bull During a mean follow-up of 476middot5 days 4middot6 patients were admitted to hospital with bleeding
bull The yearly incidence of bleeding varied from 2middot6 for the aspirin group to 12middot0 for triple therapy
bull Number needed to harm was12middot5 for triple therapy
bull Of 1852 patients with non-fatal bleeding (37middot9) had recurrent MI or died during the study period
Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Part 1
Coronary disease
no other indication
for anticoagulant therapy
50
60
70
80
90
100
0 1 2 3 4 5 6
Months after hospital discharge
S
urv
ivin
g
STEMI Non-STEMI UA
Survival Rate 6 Months Post Discharge for
STEMI NSTEMI and UA Patients
Goldberg RJ et alAm J Cardiol 200493288-93
OASIS 5 follow-up
N Engl J Med 2006 3541464-1476
N Engl J Med 2002347969-9
Composite of death reinfarction and stroke
10
Circulation 2002Feb 5105(5)557-63
Haq et al Am J Med 2010123250-258
Sorensen R et al Lancet 2009374 1967-1974
bull During a mean follow-up of 476middot5 days 4middot6 patients were admitted to hospital with bleeding
bull The yearly incidence of bleeding varied from 2middot6 for the aspirin group to 12middot0 for triple therapy
bull Number needed to harm was12middot5 for triple therapy
bull Of 1852 patients with non-fatal bleeding (37middot9) had recurrent MI or died during the study period
Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

50
60
70
80
90
100
0 1 2 3 4 5 6
Months after hospital discharge
S
urv
ivin
g
STEMI Non-STEMI UA
Survival Rate 6 Months Post Discharge for
STEMI NSTEMI and UA Patients
Goldberg RJ et alAm J Cardiol 200493288-93
OASIS 5 follow-up
N Engl J Med 2006 3541464-1476
N Engl J Med 2002347969-9
Composite of death reinfarction and stroke
10
Circulation 2002Feb 5105(5)557-63
Haq et al Am J Med 2010123250-258
Sorensen R et al Lancet 2009374 1967-1974
bull During a mean follow-up of 476middot5 days 4middot6 patients were admitted to hospital with bleeding
bull The yearly incidence of bleeding varied from 2middot6 for the aspirin group to 12middot0 for triple therapy
bull Number needed to harm was12middot5 for triple therapy
bull Of 1852 patients with non-fatal bleeding (37middot9) had recurrent MI or died during the study period
Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

OASIS 5 follow-up
N Engl J Med 2006 3541464-1476
N Engl J Med 2002347969-9
Composite of death reinfarction and stroke
10
Circulation 2002Feb 5105(5)557-63
Haq et al Am J Med 2010123250-258
Sorensen R et al Lancet 2009374 1967-1974
bull During a mean follow-up of 476middot5 days 4middot6 patients were admitted to hospital with bleeding
bull The yearly incidence of bleeding varied from 2middot6 for the aspirin group to 12middot0 for triple therapy
bull Number needed to harm was12middot5 for triple therapy
bull Of 1852 patients with non-fatal bleeding (37middot9) had recurrent MI or died during the study period
Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

N Engl J Med 2002347969-9
Composite of death reinfarction and stroke
10
Circulation 2002Feb 5105(5)557-63
Haq et al Am J Med 2010123250-258
Sorensen R et al Lancet 2009374 1967-1974
bull During a mean follow-up of 476middot5 days 4middot6 patients were admitted to hospital with bleeding
bull The yearly incidence of bleeding varied from 2middot6 for the aspirin group to 12middot0 for triple therapy
bull Number needed to harm was12middot5 for triple therapy
bull Of 1852 patients with non-fatal bleeding (37middot9) had recurrent MI or died during the study period
Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Circulation 2002Feb 5105(5)557-63
Haq et al Am J Med 2010123250-258
Sorensen R et al Lancet 2009374 1967-1974
bull During a mean follow-up of 476middot5 days 4middot6 patients were admitted to hospital with bleeding
bull The yearly incidence of bleeding varied from 2middot6 for the aspirin group to 12middot0 for triple therapy
bull Number needed to harm was12middot5 for triple therapy
bull Of 1852 patients with non-fatal bleeding (37middot9) had recurrent MI or died during the study period
Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Haq et al Am J Med 2010123250-258
Sorensen R et al Lancet 2009374 1967-1974
bull During a mean follow-up of 476middot5 days 4middot6 patients were admitted to hospital with bleeding
bull The yearly incidence of bleeding varied from 2middot6 for the aspirin group to 12middot0 for triple therapy
bull Number needed to harm was12middot5 for triple therapy
bull Of 1852 patients with non-fatal bleeding (37middot9) had recurrent MI or died during the study period
Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Sorensen R et al Lancet 2009374 1967-1974
bull During a mean follow-up of 476middot5 days 4middot6 patients were admitted to hospital with bleeding
bull The yearly incidence of bleeding varied from 2middot6 for the aspirin group to 12middot0 for triple therapy
bull Number needed to harm was12middot5 for triple therapy
bull Of 1852 patients with non-fatal bleeding (37middot9) had recurrent MI or died during the study period
Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Oldgren J et al Eur Heart J 2013341670-1680
n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

n=7400
Recent ACS + 2 high risk features
apixaban 5 mg BID (or 25 if ecclt40)
19 single APT 81 DAPT
Mortality in placebo 39 in 15 months
(hazard ratio with apixaban 259
95 CI 150 to 446)
HR095 (080 to 111)
n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

n=15500 Recent ACS
If lt 55 years previous MI or DM
Rivaroxaban 25 or 5 mg BID
7 single APT 93 DAPT
Mortality in placebo arm 107 in 2y
HR 396 (246ndash638)
Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Meta-analysis efficacy
all cause mortality MI and stroke
Oldgren J et al Eur Heart J 2013341670-1680
NNT (benefit) on top of DAPT 187
Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Oldgren J et al Eur Heart J 2013341670-1680
Meta-analysis safety
major bleeding
NNT (harm) on top of DAPT 24
What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

What about dose
apixaban in APPRAISE 2 same dose as in afib (5mg BID)
rivaroxaban in ATLAS ACS2 frac14 and frac12 the dose used in afib
(25 and 5 mg vs 10 mg)
unexpectedly
Increase in bleeding similar with both agents
Lower dose rivaroxaban appears more effective than full dose
apixaban
What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

What about newer P2Y12 inhibitors
Replacing clopidogrel with ticagrelor (or prasugrel)
may be a better option than adding an OAC to ASA plus
clopidogrel
ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

ASA + ticagrelor (PLATO)
vs
low dose rivaroxaban +ASA + clopidogrel (ATLAS ACS2-TIMI51)
PLATO ATLAS ACS2
Age (years) 62 62
PCI 61 60
nonSTE-ACS 60 50
Rubboli et al
Intern Emerg Med
20138672-680
individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

individuals at high risk
of thrombotic complications example
At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

At Discharge Risk Model
6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

6 month mortality after ACS
Validity of the GRACE ACS prediction model in an independent data set
P J Bradshaw D T Ko A M Newman and L R DonovanHeart 2006 Jul 92(7) 905ndash909
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey)
Chest 2010138(5)1093-100
TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

TNT and IDEAL trials
atorvastatin 80 mg vs low dose statin
Overall treatment effect RR 078
Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Part 2
coronary artery disease in
patients with atrial fibrillation
At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

At Discharge Risk Model
Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Pisters R Lane DA Nieuwlaat R et al (the Euro Heart Survey) Chest 2010138(5)1093-100
Lip GY Frison L Halperin JL Lane DA J Am Coll Cardiol 201157(2)173-80
Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Selected recommendations
In ACS adding OAC to DAPT doubles the risk of bleeding
In ACS risk stratify with GRACE score
Long term re-assess CHA2DS2-VASc and HAS-BLED annually
In combination with antiplatelet therapy consider lower dose of OAC
In combinations with OAC prefer clopidogrel over newer P2Y12 inhibitors (bleeding risk)
In general continue existing OAC if ACS occurs
Minimize duration of combination therapy
Long term continue OAC in all patients with CHA2DS2-VASc ge2
Very selected cases long term combination with antiplatelet agent
Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Lancet 2013Volume 381 No 9872 p1107ndash1115
Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Measures to reduce the risk of bleeding
Low dose aspirin
Clopidogrel preferred second antiplatelet agent
INR 20 ndash 25
INR in TTR gt 70
Radial approach in PCI
Bare metal stents or new generation drug eluting stents (shorterduration combined therapy)
Avoid routine use of GP2b3a inhibitors
Consider PPI in OAC + antiplatelet therapy
Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

Eur Heart J 2014353155-3179
conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended

conclusions
CAD high risk of recurrent events
No clear evidence of benefit of adding OAC to antiplatelet Rx
clear evidence of increased bleeding risk with adding OAC toantiplatelet Rx
Adding newer P2Y12 antagonists to ASA may be superior to addingOAC to ASA + clopidogrel
Individualization of benefits and bleeding risk is recommended
Please use professional organisation resources (ESC AHAACC) forguidance and local protocols
Explicit documentation and repeated re-assessment is recommended







![Journal Papers [1-44] - biosensors.com · Polymer-Based Biolimus-Eluting Stents Versus Durable Polymer-Based Sirolimus-Eluting Stents in Patients With Coronary Artery Disease: Final](https://img.dokumen.tips/doc/110x75/5fae34968d5e227c587bb762/journal-papers-1-44-polymer-based-biolimus-eluting-stents-versus-durable-polymer-based.jpg)