Embed Size (px)
Citation preview

What If Everything You Are Doing About Physician Compensation Is Wrong?
Vision for Aligned Physician Compensation
Michael Connolly, DOSenior Vice President, Quality Management
Nevada Health CentersRobert Bauer
Senior Vice PresidentNavvis Healthways

2
COMPENSATION V 1.0 FEE FOR SERVICE

3
If It Isn’t Wrong, It’s Not Optimal
• Most physician compensation models are primarily productivity (wRVU) or cash collection based
• These fee for service models incent quantity over quality• If we do not FUNDAMENTALLY transform our system of
payment and compensation, we will continue to have:– Poor physician morale– Unsatisfactory experience: customer service and access– Slow progress towards a value-based system

4
Are Current Compensation Models to Blame?
Physician Morale• According to a Wall Street
Journal survey of 12,000 physicians in 2012, only 6% described morale as positive• The greatest area of
dissatisfaction is not having enough time to spend with patients and feeling that they cannot meet patients’ needs.
• According to a 2014 Medscape/WebMD survey, only 46% would choose medicine as a career again and only 45% would encourage a younger person to enter medicine.
Patient Perception• Dissatisfied with access to
providers• Dissatisfied with communication
and follow-up by physicians• Generally confident in the quality
of their providers and care• Generally dissatisfied with
customer service and access to care

5
Current Comp Models: Sustainable Results?
Hospital Owned Average Loss per Physician
Family Practice ($127,535)
Internal Medicine ($182,999)
Pediatrics ($24,882)
Source: 2012 MGMA Cost Survey Data
6
Are You Really Patient Centered?
• Most health systems prominently state their desire to be patient centered.
• Are you patient centered if you:– Pay physicians based on volume instead of quality?– Do not provide multiple venues of access?– Do not provide care when the patient wants it?– Do not have a system that enables a physician
to spend meaningful time with patients?

7
Is Compensation Aligned with the Triple Aim?
IMPROVING THE PATIENT
EXPERIENCE OF CARE
IMPROVING THE
HEALTH OF POPULATIO
NS
REDUCING THE PER CAPITA
COST OF HEALTH
CARE

8
What Does FFS Incent? V 1.0 (FFS)Productivity Office Based Visit Volume YesPanel Size NoPatient Satisfaction Time with Provider NoEasy Access NoChronic Condition Management NoCommunication with Provider NoPhysician Satisfaction Satisfaction with Job NoTop of License Practice NoProfessional Pride NoQuality Reward for Quality NoAccess Non-Visit Based Care Incentive NoExtended Hours Incentive NoPopulation Focused Coordinated Care NoDisease Management Focused NoEfficiency Total Cost of Care NoOffice Staff Efficiency No

9
Relationship of FFS to the Triple Aim
IMPROVING THE PATIENT
EXPERIENCE OF CARE
IMPROVING THE
HEALTH OF POPULATIO
NS
REDUCING THE PER CAPITA
COST OF HEALTH
CARE
V 1.0 FFS

10
Shift From Volume To Value: The Train Has Left The Station
• In January, 2015 the Department of Health and Human Services announced performance goals and timelines for the transition of Medicare payments from volume to value.
• They also introduced a partnership to encourage private payers, employers, hospitals and physicians to adopt similar goals.
“We are dedicated to using incentives for higher-value care, fostering greater integration and
coordination of care and attention to population health, and providing access to information that
can enable clinicians and patients to make better-informed choices.” – Sylvia Burwell, HHS
Secretary

11
CMS Provider Payment Reform Goals

12
COMPENSATION V 2.0 FEE FOR SERVICE + PAY FOR QUALITY
13
Typical P4Q Constructs
• Process measures have evolved to performance measures• Typical rewards based on:
– Preventive measures– Chronic disease measures– Generic drug utilization– Off-hours care – Decreased ER visits– Decreased admissions/readmissions
Can be PCMH based, which does emphasize care coordination.

14
Challenges with P4Q
• # measures; generally too many– Peanuts effect
• Different measures for different payors• Physician line of sight and involvement in negotiating• IT systems to prompt closing gaps in care • Workflow for non physician providers and staff
– Standing orders– Incentives for staff
• Transparency and reporting to physicians: clinical and financial
• System and culture of accountability

15
Challenges with P4Q
• Lack of alignment between comp model and P4Q programs– Are P4Q incentives passed directly to the physician?– In whole or in part?
• Timing and form of reward: not just about remuneration• Reward and recognition issues:
– Included in normal pay?– Paid periodically and in special setting?
• Quarterly quality meeting?– Special recognition and designation for high performance?

16
Challenges with P4Q
• Undercuts the intrinsic professional and moral responsibility to provide high quality care into an economic transaction.
• Addressing a problem; not fixing the system.
A band aid at best.
17
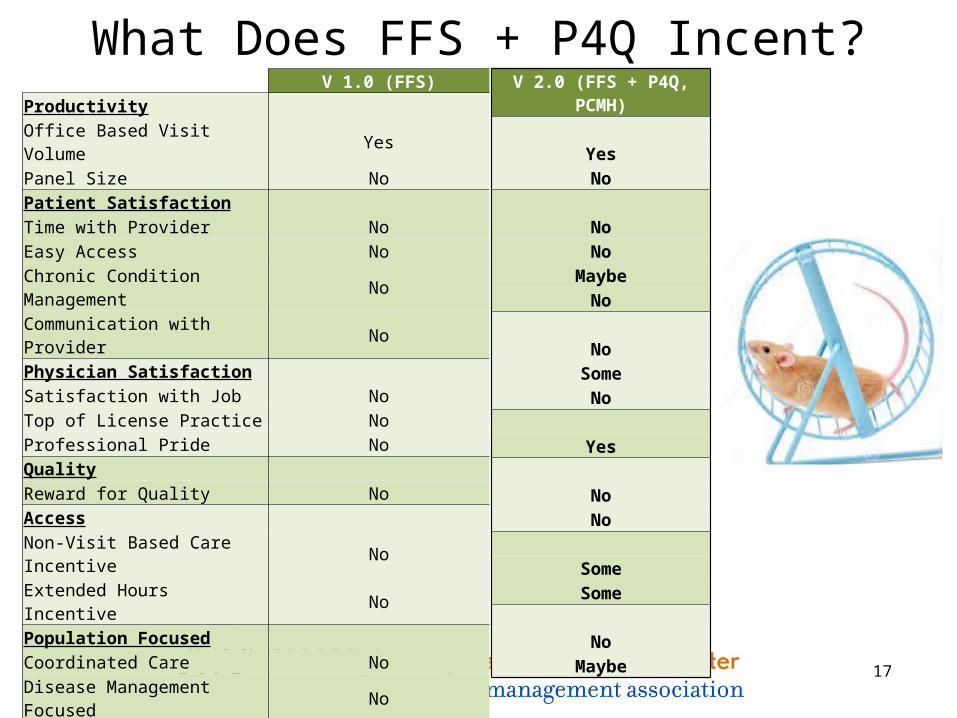
What Does FFS + P4Q Incent? V 1.0 (FFS)Productivity Office Based Visit Volume YesPanel Size NoPatient Satisfaction Time with Provider NoEasy Access NoChronic Condition Management NoCommunication with Provider NoPhysician Satisfaction Satisfaction with Job NoTop of License Practice NoProfessional Pride NoQuality Reward for Quality NoAccess Non-Visit Based Care Incentive NoExtended Hours Incentive NoPopulation Focused Coordinated Care NoDisease Management Focused NoEfficiency Total Cost of Care NoOffice Staff Efficiency No
V 2.0 (FFS + P4Q, PCMH)
YesNo
NoNo
MaybeNo
No
SomeNo
Yes
NoNo
SomeSome
No
Maybe

18
Relationship of FFS+P4Q to the Triple Aim
IMPROVING THE PATIENT
EXPERIENCE OF CARE
IMPROVING THE
HEALTH OF POPULATIO
NS
REDUCING THE PER CAPITA
COST OF HEALTH
CARE
V 1.0 FFS
V 2.0 FFS
+P4Q, PCMH

19
COMPENSATION V 3.0 IT’S THE ALIGNMENT ………

20
What Patients Really Want From Healthcare
PATIENT WANTS CURRENT REALITY
Restoring health when illThis is what our health system is built around
Reassurance and hope of options, even in dire circumstances
Our system has the most readily available treatment options
Highly qualified providersMost extensive system of medical education in the world
Maintain wellness Not a focus
Immediate availabilityNot current reality; Access is the new black
Ease of communication and follow-up after visits Severely lacking
Source: Detsky AS. What Patients Really Want From Health Care. JAMA. 2011;306(22):2500-2501. doi:10.1001/jama.2011.1819.
F

21
Meeting Patient Needs: How We’re Doing
Prevention & Well-Being
Acute/Episodic Care
Chronic Disease
Management
Advanced Care
Current Payment & Delivery System
• Preventive care• Community based
services and infrastructure to address upstream determinants of health & well-being
• Care coordination• Regular access to
provider team• Medication
adherence• Lifestyle
modifications• Behavioral health
• Care as needed• Coordination across
providers and facilities
• Follow-up and prevention of recurrence
• Advanced care planning
• Supportive care – patient and family
• Timely hospice referral

22
Access is the “New Black”
• Access– Access does not need to be in the form of an appointment with a
physician– True open access: today, tomorrow, evening, weekend
• In-person• Email• Phone• Tele visits• Text

23
Communication And Follow-Up
50% of patients report no follow-up at all after a visit. Only 5% of patients report not wanting any follow-up
43% of patients prefer to be contacted by phone
25% of patients prefer to be contacted by Email
50% of patients report not knowing if their physician has a portal. Only 9% of patients report using a patient portal at any time in the past
96% of physicians view medication adherence as very important but less than half include adherence counseling when prescribing a new medication
Source: http://technologyadvice.com/medical/blog/study-patient-portal-communication-2014/ https://healthprize.com/wp-content/uploads/2015/02/Doc-Survey-Release_FINAL.pdf
Rapid communication and preferred
method of communication
are highly important to
patients

24
Not Currently Paid For Or Incentivized Under FFS
• Phone management• Tele-health visits• Emails• Texts• Patient navigators• Patient portal and supporting technology (except via MU and
some PCMH contracts)
DIFFICULT TO ALIGN INCENTIVES OF PHYSICIANS AND PATIENTS WITHOUT THESE
COMPONENTS

25
What We Need: A Transformational Payment Model
Prevention andWell-Being
Acute/EpisodicCare
Chronic DiseaseManagement
AdvancedCare
System That Meets All Members’ Health And Healthcare Needs
Current Payment And Delivery System
Prevention andWell-Being
Acute/EpisodicCare
Chronic DiseaseManagement
AdvancedCare
Next Generation Physician Compensation Model Goal: To design and implement a transformational, member-centered payment model for providers that encourages high-quality, coordinated care, patient
engagement and a focus on well-being and prevention, and bends the cost growth curve.
26
This Transformational Model…
Is designed to meet member needs
Embraces health and healthcare needs
Recognizes socio-economic status
Pays for outcomes and value
Incorporates behavioral economics
Is not fee-for-service driven
REPRESENTS AN EVOLUTION FROM A TRANSACTIONAL RELATIONSHIP TO A VALUE-BASED COMPACT

27
The Transformational Payment Model
• Physicians receive a core patient management fee, PMPY/PMPM:– Management fee based on:
• Number of attributed patients• Adjusted for age, gender, disease burden
– Incentive compensation• Patient satisfaction• Outcome measures
– ER visits, admissions, clinical measures, wellness measures• Adherence to evidence-based guidelines• Total Cost of Care
– Capitation model with a difference!
28
How to get from here to there…..
• Payer contracts must be restructured:– Minimum Required Change: Convert historic FFS PCP payments into
a guaranteed base capitation• Need adjustments for changes to attributed members
– More aggressive change: Convert entire contract to a global cap• Need specific strategies and infrastructure for success
• Creating aligned compensation model– PCP compensation model is converted to a PMPM management fee– Protection for transition periods– The right performance metrics – Ecosystem of care support
Caution: Not for the faint of heart!

29
Case Study for Payment Transformation
HMSA (Blue Cross of Hawaii)
Premise: FFS payment model is major contributor to unsustainable growth in health care costs.
Solution: Totally eliminate FFS payments for all PCPs.
Specifics:• Current FFS payments and % of PCMH $s rolled into a cap
payment level• In office visits with a physician no longer core to patient access
• Protection for transition year• Specific performance measures to protect against
disadvantages of a cap model
30
Incentive Measures
• Principles– Focus on outcomes and value vs. process measures
– Manageable number
– Meaningful to both the physician and the patient
– Clinical goals evidence-based with built-in clinical support via the EHR
– Pay for improvement
– Checks and balances for cost, quality, and access

31
Sample Primary Care Performance MetricsDOMAIN MEASURE(S)
1 PreventionAge and gender appropriate cancer screenings bundle: - Breast, Colon, Cervical
2 Prevention Flu and pneumonia vaccine bundle
3 Behavioral Health Screening for clinical depression and anxiety (PHQ4)
4 Population Management (Well-being)
BMI control/obesity - all members
5Population Management (Well-being)
WB5 completion rate
6 Patient Experience- Patient-reported satisfaction or PCP rating - Patient-reported access to care
7 Shared Decision Making Patient-reported SDM measure
8 Patient Experience/SDM Advance Care Planning
9 Chronic Condition Management
Diabetes Care Management bundle: - HbA1c Control - Eye Exam - Medical Attention for Nephropathy - Blood Pressure Control
10 Population Management (well-being)
Smoking cessation & follow-up
32
Key Success Factors
ENGAGE • Incentivize financially
ENABLE• Information (business intelligence platform)
– provide real time data and analytics
EMPOWER • Ecosystem/Infrastructure

33
Individual Physician Payment Illustration
PMPM $Per-member-
per-month base
Engagement $ and Triggers
Performance improvement -based $ and Triggers
Total potential primary care compensation
TCOC bonus
Current PCP FFS and PCMH reimbursement
80% 20%
Performance Incentive
25%Shared Savings

34
Evolution of Compensation V 1.0 (FFS)Productivity Office Based Visit Volume YesPanel Size NoPatient Satisfaction Time with Provider NoEasy Access NoChronic Condition Management NoCommunication with Provider NoPhysician Satisfaction Satisfaction with Job NoTop of License Practice NoProfessional Pride NoQuality Reward for Quality NoAccess Non-Visit Based Care Incentive NoExtended Hours Incentive NoPopulation Focused Coordinated Care NoDisease Management Focused NoEfficiency Total Cost of Care NoOffice Staff Efficiency No
V 2.0 (FFS + P4Q, PCMH) YesNo NoNo
MaybeNo NoSomeNo Yes NoNo
SomeSome No
Maybe
V 3.0 (Population Health)
NoYes
YesYesYesYes
YesYesYes
Yes
YesYes
YesYes
YesYes

35
Evolution of Compensation V 1.0 (FFS)Productivity Office Based Visit Volume YesPanel Size NoPatient Satisfaction Time with Provider NoEasy Access NoChronic Condition Management NoCommunication with Provider NoPhysician Satisfaction Satisfaction with Job NoTop of License Practice NoProfessional Pride NoQuality Reward for Quality NoAccess Non-Visit Based Care Incentive NoExtended Hours Incentive NoPopulation Focused Coordinated Care NoDisease Management Focused NoEfficiency Total Cost of Care NoOffice Staff Efficiency No
V 2.0 (FFS + P4Q, PCMH) YesNo NoNo
MaybeNo NoSomeNo Yes NoNo
SomeSome No
Maybe
V 3.0 (Population Health)
NoYes
YesYesYesYes
YesYesYes
Yes
YesYes
YesYes
YesYes

36
Aligned Compensation Model & the Triple Aim
IMPROVING THE PATIENT
EXPERIENCE OF CARE
IMPROVING THE
HEALTH OF POPULATIO
NS
REDUCING THE PER CAPITA
COST OF HEALTH
CARE
V 1.0 FFS
V 3.0 Population
Health
V 2.0 FFS
+P4Q, PCMH

37
Summary• Our current compensation models:
– do not support the move to population health
– Are inconsistent with the triple aim
• Current models do not meet the needs of either physicians or patients;
• The current model drives unprofitable volume:– Physicians spend too much time on unnecessary visits– Do not practice at the top of their license
• Our failure to meet member needs, especially related to Access, is evidenced by the growth of disruptive competitors;

38
Michael J. Connolly, DO
Dr. Connolly is the Sr. VP for Quality Management at Nevada Health Centers based in Las Vegas, Nevada. Prior to joining Nevada Health Centers Dr. Connolly served as the Chief Medical Officer for Carondelet Medical Group (CMG) in Tucson, Arizona. He has extensive experience in practice operations, physician compensation, contracting, chronic disease management, and value based purchasing. He remains an active clinician with a primary care practice.
Dr. Connolly’s formal training includes a fellowship in Geriatric Medicine at SUNY Stony Brook and a residency in Internal Medicine at Yale University. He has worked in a wide variety of clinical and administrative environments, including academic positions at SUNY Stony Brook and clinical positions with the US Indian Health Service on the San Carlos Apache Indian Reservation.
While working with the Indian Health Service he recognized the need for a coordinated team approach to the management of Diabetes. He developed the San Carlos interdisciplinary Diabetes team that ultimately led to one of the Indian Health Services first ADA recognized Diabetes care programs. He has continued to work extensively in the Diabetes arena and has developed clinical programs that have been featured by The Health Care Advisory Boards publications as one of the nation’s most successful and innovative approaches to Diabetes care and reimbursement.
Dr. Connolly has served on the Pima County Medical Society’s Board of Directors. He was also the chairperson for the Quality Committee of Mercy care plan, Arizona’s largest and highest clinically rated Medicaid plan. He also served on Mercy care Plans Board of Directors. Dr. Connolly has received multiple awards for excellence and compassion in patient care.

39
Robert Bauer
Bob Bauer is a Senior Vice President for Navvis Healthways, a boutique consulting firm that specializes in payment transformation and the strategic evolution to Population Health Management. He has over 30 years of consulting and executive leadership experience in the health care industry. He has served as the V.P. Finance/CFO for community, multi-hospital, teaching and faith based health systems. Bob is known for his strategic approach to financial leadership and has led numerous acquisition, affiliation and financing transactions.
Bob has extensive experience in PHO and integrated health system development. He implemented a Core Competency Development Process to accelerate physician leadership development. He has served as Sr. Vice President/COO for a network of ten hospitals and their respective PHOs or IPAs involved in risk based managed care contracting. Bob is also an innovator in ambulatory care strategies. He created the nationally recognized Health and Wellness Center by Doylestown Hospital, an experientially designed comprehensive outpatient campus.
Bob graduated from Villanova University with a Bachelor of Science degree in accounting. He is a member of the Healthcare Financial Management Association and the Pennsylvania Institute of Certified Public Accountants, where he has served on the statewide Health Care Committee.





























