Embed Size (px)
Citation preview

What do we know?
Suicide on UK roads in context
Subtitle
Ann JohnProfessor of Public Health and PsychiatryChair of the NAG to WG on Suicide and self harm prevention
Whistle stop tour
Key facts and issues
Global and national suicide rates
Methods used-in relation to RTIs
An example from Wales

Suicide – key facts
Approximately 800 000 people die by suicide every year globally
For every suicide there are many more people who attempt suicide-1: 20
A prior suicide attempt is the single most important risk factor for suicide
in the general population.
Suicide is the second leading cause of death among 15–29-year-olds.
Ingestion of pesticide, hanging and firearms are among the most
common methods of suicide globally.
1.4% of all deaths worldwide, 17th leading cause of death in 2015.

Suicide –key issues
Potentially preventable
Ambivalence, response to a crisis, impulsive, planned
Only ¼ are known to MH services in the year before they die
Inequalities- Men lower socio-economic backgrounds, living in deprived areas, 10x more likely to take their own lives than those living in affluent areas
0
5
10
15
20
25
30
35
40
2003-05 2004-06 2005-07 2006-08 2007-09 2008-10 2009-11 2010-12
EASR
per
100
,000
Least deprived Most deprived
Suicides, European age-standardised rate (EASR) per 100,000, by least and most
deprived fifth (WIMD 2011), males aged 15+, Wales, 2003-2012Produced by Public Health Wales Observatory, using ADDE & MYE (ONS), WIMD (WG)
95% confidence interval

Many different risk factors interacting in complex ways
Risk Factors for Suicide(non-exhaustive)INDIVIDUAL
Sex - male
Low socio-economic status
Restricted educational achievement
Previous suicide attempt or self harm
Mental disorder (including those unrecognised or untreated)
Bullying- victim/ perpetrator
Alcohol or substance misuse
Family history of suicide
History of trauma or abuse
Sense of isolation
Personality traits-hopelessness, low self esteem, external locus of control,
aggression, introversion
Restricted help seeking
SITUATIONAL
Job and financial losses
Stressful life events (including divorce/ separation)
Relational or social losses or discord
Easy access to lethal means
Clusters of suicide that have an element of contagion
Family history of suicidal behaviour (modelling or
inheritance)
Parental psychopathology- depression, substance
misuse, anti social behaviour, non-intact homes
SOCIO-CULTERAL
Exposure to suicidal behaviours
Stigma associated with poor help seeking behaviour
Barriers to accessing healthcare, particularly mental health and
substance misuse treatment
Suicide by adolescent peer
Media coverage of a suicide
No single organisation, everybodys’ business
National strategies to co-ordinate action, PH, collaborative

Quality of suicide data
60/172 WHO Member states have good-quality death registration data
Legality, stigma, under reporting
Coroners court ‘beyond a reasonable doubt
Probable, possible
-Suicide, deaths of undetermined intent (open)
-Narrative verdicts as accidental death
-Accidental hanging and poisonings, single vehicular accidents, unknown cause
X81.0 intentional SH jumping or lying in front of a motor vehicle
X82 intentional SH by crashing a motor vehicle
Suicide excluded from road traffic data, Stats 19, validated DfT figures
‘clear evidence injury was self-inflicted, that the deceased intended to kill
himself. If there is any doubt about the intentions of the deceased either an
accidental or open verdict’



Age standardised suicide rates
UK:1981-2014
1932–33 increase due to recession
1939–45 decrease due to WWII
1950–63 increase (post war,
austerity)
1963–74 decrease
1975–90 increase
1991 – decrease2009-upturn
2016 registrations

15.7 29.1 31.6 19.4 17.44.8 10.0 9.3 4.8 5.3
England Scotland† Northern Ireland Wales UK*
Males Females
Suicides, European age-standardised rates (EASR) per 100,000, males and females
aged 15+, UK Nations, 2009-2011 Produced by Public Health Wales Observatory, using data from ONS, GROS & NISRA
95% confidence interval
*UK is derived from the sum of England, Scotland, Northern Ireland and Wales and does not include deaths of non-residents †Denominator used to calculate 2011 rate is based on 2010 MYEs as Scottish MYEs have not been revised to reflect Census 2011 populations

Males, females and age
2nd leading cause of death 10-29 year olds
Lethality

Proportion of suicide by method and
sex, Great Britain, registered in 2016
Jumping from a high
place
Jumping or lying in
front of a moving
object
Hanging
Isolated rural lay-bys,
- car exhaust
Rural lanes
Single vehicle
collisions
Do we know more? 2% of single vehicle RTAs are suicidal behaviours (Pompilli 2012)
2.8% fatal RTAs suicides, Scottish study (1792 road fatalities ONS bulletin)
Under reporting, as accidents, ambivalence, risk taking behaviour and suicide spectrum, impulsivity
Males, 25-34 years
Risk factors- previous attempts, mental disorder, alcohol
Little known re determinants of choice of method- ease of access, acceptability, occupation
Roads- Financial benefits, reduction of stigma
Community survey 14.8% who reported planning a suicide thought of having an RTA ( Murray and De Leo 2007)
Lethality
1/3 left a note: hardly any in RT- ? Impulsive, alcohol
Proximity to psychiatric hospitals
Single car, single occupant collision, head on collision single occupant heavy goods lorry, pedestrian accidents

Interventions to prevent suicides on roads
-4 ways
RESTRICT ACCESS TO THE SITE AND THE MEANS OF SUICIDE
① Closing all or part of the site ✔
② Installing physical barriers to prevent jumping or access ✔
③ Introduce other deterrents- boundary markings or lighting
④ Alcohol interlocks?
⑤ Intelligent speed adaptation
⑥ Car bonnet design, air bags

Interventions to prevent suicides on
roads-4 ways Increase opportunity and capacity for human intervention
① Improve surveillance- CCTV, staffing, foot patrols
② Suicide awareness staff, community ✔ (gatekeeper)
③ Car braking, lights, speed etc for pedestrian injuries
Increase opportunities for help seeking
① Samaritans signs (✓) / phones (✔)
② Signpost to staffed sanctuary
Change public image of site
① Appropriate media reporting
② Think about memorials

Other considerations RTAs and ED staff
Single vehicle single occupant accidents, PM, psychological
autopsies, inquests
Staff
Data collection- need more
Who? How? Where? When?
Real time surveillance
Attempts
ONS method and place of death
Since Stats 19 does not record suicide as a cause of death difficult for the highways agency to do national analysis or strategic prevention
Incident logs

In Wales
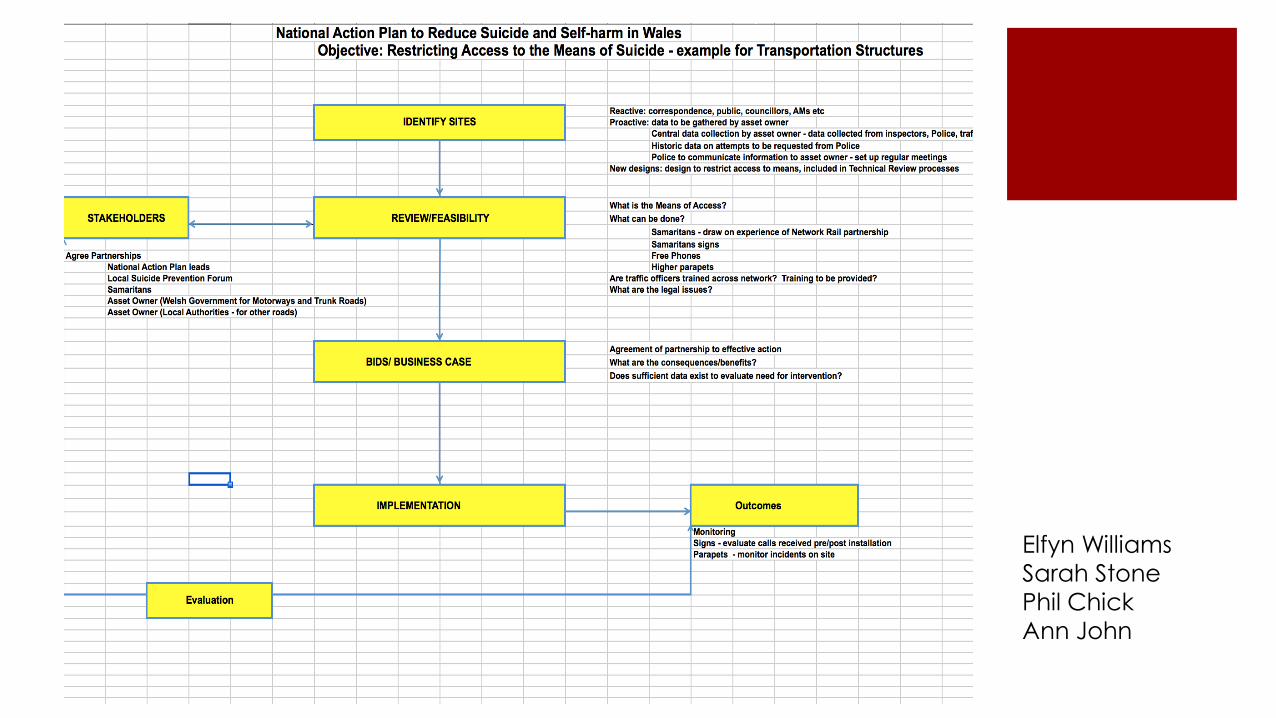
Elfyn Williams
Sarah Stone
Phil Chick
Ann John

Diolch yn fawr – Thank you
It’s a team and collaborative effort……………
TeamLloyd, Dennis, John, Tan, Delpozobanos, McGregor, Marchant, Brown, Kandalama, Andrews, Okolie, Daniels, Loxton, Basu, Wood, Glenndinig, Lacey, Thomas, Thomas, Lee.
ActivitiesLloyd- Samaritans Cymru BoardJohn- Chair National Advisory Group to WG on S&SH Prevention, APCO UK Suicide Prevention, HQIP Advisory Board NCISH, MHRN SSH RDG England, WISPLoxton- CASIP
UK and international collaborationsOxford (Hawton), Bristol (Gunnell), Cardiff (Scourfield, Jones, Owens, Walters,Kemp), Leeds (Owens), Manchester (Kapur) Scotland (Platt), Ireland (Arensman), Australia (Beautrais, Pirkis), Canada (Hatcher,
Lesage)
National Confidential Enquiry into Patient Outcomes and DeathsSwansea University Human and Health Sciences (SWISH)Farr InstituteNCPHWR-Lyons, Fone, Roberts, Brophy
National Centre for Mental HealthPRIME- paramedics, Snooks, Rees
Public Health Wales 3rd sector- Samaritans, Papyrus, Cruse, Hafal, Casip





























