Embed Size (px)
Citation preview

What Clinicians Should Know
About Hepatitis C Virus
Michael S. Saag, MDAssociate Dean, Global Health
Professor of MedicineDirector, Center for AIDS Research
University of Alabama at BirminghamBirmingham, Alabama
FINAL AS OF: 11/15/17
Slide 3 of 55
Learning Objectives
After attending this presentation,
learners will be able to: Describe the genotypes of HCV and how they relate
to treatment effects
Recognize how to stage HCV infection and why it is important to accurately stage
Recall the clinical presentation of advanced liver disease (cirrhosis)
Describe emerging treatments of HCV and how the changing landscape will impact treatment decisions in the near future
Identify new changes to the HCV Guidelines (Sept 2017)
Slide 5 of 55
Which test most accurately stage liver fibrosis?
1. Fibroscan
2. Fibrosure
3. APRI
4. Liver biopsy
5. Liver percussion
Fibro
scan
Fibro
sure
APRI
Liver
bio
psy
Liver
per
cuss
ion
27%
9%
0%
64%
0%
Louisville, Kentucky, November 17, 2017 1

Slide 7 of 55
What percent of persons with chronic HCV infection develop
cirrhosis over 30 years?
1. 0 – 5%
2. 6% – 20%
3. 21% – 50%
4. 51% – 75%
5. >75%
0 –
5%
6%
– 2
0%
21% –
50%
51% –
75%
>75
%
0%
23% 23%
15%
38%
Slide 9 of 55
What is the most common genotype of HCV in the United
States?
1. Genotype 1
2. Genotype 2
3. Genotype 3
4. Genotype 4
5. Genotype 5–6
Genotype
1
Genotype
2
Genotype
3
Genotype
4
Genotype
5–6
93%
0% 0%0%7%
Slide 10 of 55
Objectives
Epidemiology
Natural History
Staging
Genome and Drug Targets
Viral Kinetics With Therapy
Current Treatments
What Does SVR Really Mean?
Louisville, Kentucky, November 17, 2017 2

Slide 11 of 55
Objectives
Epidemiology
Natural History
Staging
Genome and Drug Targets
Viral Kinetics With Therapy
Current Treatments
What Does SVR Really Mean?
Slide 12 of 55
HCV Research Timeline
Moradpour Nature Reviews 2007; 5:453-463
AIDS
1982
HIV
1984
AZT
1987
Slide 13 of 55
HCV Worldwide
170 million infected
Highest Asia & Africa
Egypt > 15%
USA 1.6%– 3-4 million infected
www.cdc.gov
Louisville, Kentucky, November 17, 2017 3

Slide 14 of 55
Worldwide prevalence of each HCV genotype by GBD
HCV genotype 1 (83.4 million cases: 46.2%)- one-third of which are in East Asia.
Genotype 3 (54.3 million: 30.1%); genotypes 2, 4, and 6 (22.8%); genotype 5 <1%.
While genotypes 1 and 3 dominate in most countries irrespective of economic Status: largest proportions of genotypes 4 and 5 are in lower-income countries.
Slide 15 of 55
The Treatment Cascade of HCV infection in
the US:~3 – 4 million persons infected
Adapted from Holmberg et al. NEJM 2013
0%25%50%75%
100% 100%
50%38%
23%11% 6%
Slide 16 of 55
Future Burden of Hepatitis C Related Morbidity and
Mortality in the US
Markov model of health outcomes
– Of 2.7 M HCV infected persons in primary care
1.47 M will develop cirrhosis
350,000 will develop liver cancer
897,000 will die from HCV-related complications
Rein D, et al. Dig Liver Dis 2010.
05000
10000150002000025000300003500040000
2010
2013
2016
2019
2022
2025
2028
2031
2034
2037
2040
2043
2046
2049
2052
2055
2058
Deaths
DCC
HCC
Nu
mb
er
Louisville, Kentucky, November 17, 2017 4

Slide 17 of 55
Objectives
Epidemiology
Natural History
Staging
Genome and Drug Targets
Viral Kinetics With Therapy
Current Treatments
What Does SVR Really Mean?
Slide 18 of 55
Resolved
Stable
Slowly
Progressive
Transplant/Death
~20%
~15% ~85%
~3%-4%/yr
~80%
~75%
~ 20-year progression rate may beaccelerated with HIV, HBV,
alcohol, and steatosis1,2
Exposure(Acute Phase)
Chronic
Cirrhosis
~4%/yr~6%/yr
ESLD HCC
10 20 30Time(yrs)
5-year survival in patients with HCC is <5%*
ESLD: end-stage liver disease
*NIH Consens Statement. June 10-12, 2002;19(3):1-46. NIH Consens Statement. March 24-26, 1997;15(3):1-41.
1. Di Bisceglie AM. Hepatology. 2000;31(4):1014-1018. 2. Bialek SR, Terrault NA. Clin Liver Dis. 2006;10(4):697-715.
Natural History of HCV Infection
Slide 19 of 55
Objectives
Epidemiology
Natural History
Staging
Genome and Drug Targets
Viral Kinetics With Therapy
Current Treatments
What Does SVR Really Mean?
Louisville, Kentucky, November 17, 2017 5

Slide 20 of 55
Fibrosis/Cirrhosis
Slide 25 of 55
Objectives
Epidemiology
Natural History
Staging
Genome and Drug Targets
Viral Kinetics With Therapy
Current Treatments
What Does SVR Really Mean?
Slide 26 of 55
Translation
HCV NS proteins
NS2
Polyprotein
processing
NS3
NS4B
NS5A NS5B
HCV RNA
Fusion and
uncoating
RNA
replication
NS5A
CypA
NS5B
NS2
NS3
NS4B
Viral
assembly
Transport and
release
NS3/4A protease inhibitors
NS5A inhibitors
NS5B polymerase inhibitors
NS5A inhibitors
Potential Therapeutic Targets in the HCV
Replication Cycle
Adapted from slide courtesy Ray Chung
Louisville, Kentucky, November 17, 2017 6

Slide 27 of 55
NUCLEOSIDEINHIBITORS
Non-NUCLEOSIDEINHIBITORS
“NS5A”INHIBITORS
PROTEASE INHIBITORS
Slide 28 of 55
Suffixes Matter!
- --- PREVIR (Protease / NS3-4a)
- --- ASVIR (NS5a)
- --- BUVIR (NS5b)
Slide 29 of 55
Agents and Regimens: Fall 2017
Antiviral
NS3 NS5ANon-Nuc
NS5BNuc
NS5B
Ledipasvir/sofosbuvir FDC
Paritaprevir/r/ombitasvir FDC + dasabuvir
Simeprevir + sofosbuvir
Glecaprevir / pibrentasvir FDC
Sofosbuvir + daclatasvir
Elbasvir/grazoprevir FDC
Velpatasvir/sofosbuvir FDCVelpat/ Sof / voxilaprevir FDC
Louisville, Kentucky, November 17, 2017 7

Slide 30 of 55
Objectives
Epidemiology
Natural History
Staging
Genome and Drug Targets
Viral Kinetics With Therapy
Current Treatments
What Does SVR Really Mean?
Slide 31 of 55
On Treatment Viral Kinetics
2 log decline
LOD
Slide 32 of 55
Objectives
Epidemiology
Natural History
Staging
Genome and Drug Targets
Viral Kinetics With Therapy
Current Treatments
What Does SVR Really Mean?
Louisville, Kentucky, November 17, 2017 8

Slide 33 of 55
Chronic HCV prior SOC
Pegylated IFN + RBV
48-72 weeks
Significant AEs
Response > GT 2/3SV
R, %
Fried MW, NEJM 2002
Manns MP, Lancet 2001
Slide 34 of 55
Antiviral HCV treatments
(FDA-approved as of September, 2017)
Monotherapies
IFN-2a
IFN-2b
PEG-IFN 2a
PEG-IFN 2b
– IFN-2a + Ribavirin
– IFN-2b + Ribavirin
–PEG-IFN 2a + Ribavirin*
–PEG-IFN 2b + Ribavirin
– PEG-IFN + ribavirin plus either:
– Boceprevir (GT1)
– Telaprevir (GT1)
– Simeprevir (GT1)
–In combination with other
agents:
–Sofosbuvir
• Combination Therapies
Simeprevir + Sofosbuvir (GT1)
Paritaprevir / ritonavir / ombitasvir
(FDC) + dasabuvir (GT1)
Paritaprevir / ritonavir/ ombitasvir
(FDC) (GT4)
–Daclatasvir + Sofosbuvir
–(GT1,3)*§
Elbasvir + Grazoprevir
–(GT 1, 4)Velpatasvir / Sofosbuvir FDC
Voxilaprevir / Velpatasvir /
Sofosbuvir FDC
Glecaprevir / Pibrentasvir FDC
Ledipasvir + Sofosbuvir
(FDC, GT1,4,5,6)
Pangenotypic Regimens
(GT 1 – 6 )
Slide 35 of 70
Slide 35 of 55
Sofosbuvir plus Daclatasvir for GT1
41n=44 20 2141
No documented virologic failures. All failures due to missing sample/lost to follow-up or re-infection.
Louisville, Kentucky, November 17, 2017 9

Slide 36 of 70
Slide 36 of 55
Slide 36 of 70
Slide 37 of 55
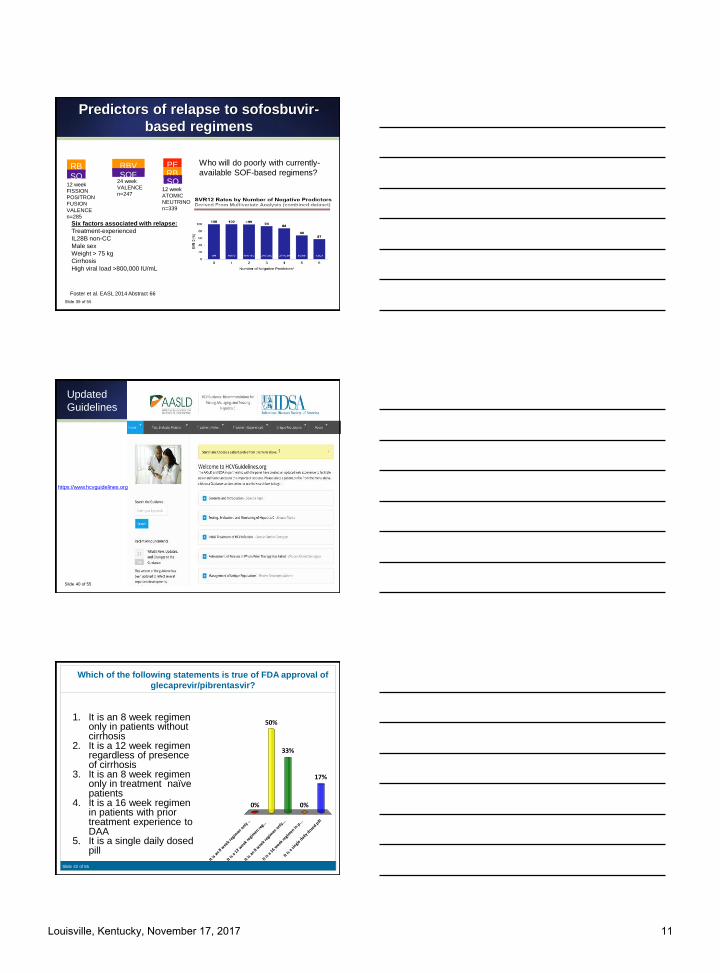
Predictors of relapse to sofosbuvir-
based regimens
RBVSOF
RB
VSO
F12 week
FISSION
POSITRON
FUSION
VALENCE
n=285
24 week
VALENCE
n=247
PE
G RB
VSO
F12 week
ATOMIC
NEUTRINO
n=339
Who will do poorly with currently-
available SOF-based regimens?
Foster et al. EASL 2014 Abstract 66
GT177%
GT29%
GT310%
GT44%
Slide 38 of 55
Predictors of relapse to sofosbuvir-
based regimens
RBVSOF
RB
VSO
F12 week
FISSION
POSITRON
FUSION
VALENCE
n=285
24 week
VALENCE
n=247
PE
G RB
VSO
F12 week
ATOMIC
NEUTRINO
n=339
Who will do poorly with currently-
available SOF-based regimens?
Foster et al. EASL 2014 Abstract 66
Louisville, Kentucky, November 17, 2017 10
Slide 39 of 55
Predictors of relapse to sofosbuvir-
based regimens
RBVSOF
RB
VSO
F12 week
FISSION
POSITRON
FUSION
VALENCE
n=285
24 week
VALENCE
n=247
PE
G RB
VSO
F12 week
ATOMIC
NEUTRINO
n=339
Who will do poorly with currently-
available SOF-based regimens?
Foster et al. EASL 2014 Abstract 66
Six factors associated with relapse:
Treatment-experienced
IL28B non-CC
Male sex
Weight > 75 kg
Cirrhosis
High viral load >800,000 IU/mL
Slide 40 of 55
Updated
Guidelines
https://www.hcvguidelines.org
Slide 42 of 55
Which of the following statements is true of FDA approval of
glecaprevir/pibrentasvir?
1. It is an 8 week regimen only in patients without cirrhosis
2. It is a 12 week regimen regardless of presence of cirrhosis
3. It is an 8 week regimen only in treatment naïve patients
4. It is a 16 week regimen in patients with prior treatment experience to DAA
5. It is a single daily dosed pill
It is
an 8
wee
k reg
imen
only
..
It is
a 12
week
regi
men re
g...
It is
an 8
wee
k reg
imen
only
...
It is
a 16
week
regi
men in
p...
It is
a sin
gle d
aily d
osed p
ill
0%
50%
17%
0%
33%
Louisville, Kentucky, November 17, 2017 11

Slide 43 of 70
Slide 43 of 55
Glecaprevir (NS3)/pibrentasvir (NS5A)
•Co-formulated – 3 pills once daily
•Pangenotypic
•Next generation
–Active vs NS3 RAS at 80, 155, 168 and
NS5A RAS at 28, Q30, 31, 93
–A30K associated with failure in GT3
infection
•Negligible renal excretion
•Contains a protease inhibitor
•Has interaction with acid suppressing meds
Slide 44 of 55
Glecaprevir/pibrentasvir: no cirrhosis
►8 (N=828) vs 12 (N=1076) weeks
►TN and TE
–PEG, RBV, SOF
–No DAA otherwise
►Relapse <1%
►Tx emergent RAS
►TN GT3 may need 12W
►TE GT3 – may need 16 weeks
99 99 99 97100 100 10099 100 100 98 100 100 100
0
10
20
30
40
50
60
70
80
90
100
All GT 1 GT 2 GT 3 GT 4 GT 5 GT 6
8 weeks 12 weeks
Puoti et al. EASL 2017
Which of the following statements is true of FDA approval of sofosbuvir/velpatasvir/voxilaprevir?
1. It is an 8 week regimen only in patients without cirrhosis
2. It is a 12 week regimen regardless of presence of cirrhosis
3. It is an 8 week regimen regardless of prior treatment experience to DAA
4. It is approved for all genotypes across all DAA failures
It is
an 8
wee
k reg
imen
only
..
It is
a 12
week
regi
men re
g...
It is
an 8
wee
k reg
imen
reg.
..
It is
appro
ved fo
r all
genot..
.
8%
58%
0%
33%
Louisville, Kentucky, November 17, 2017 12

Slide 47 of 55
Sofosbuvir/velpatasvir/voxilaprevir: 8 vs 12 weeks of SOF/VEL
►POLARIS 2
– GT 1-6 w/ and w/o cirrhosis
►POLARIS 3
– GT 3 with cirrhosis
– 2 relapses
►Pooled analysis
– N=611
►8 weeks of therapy failed non-inferiority in POLARIS-2
– 3.8% relapse
– 14 GT1a (regardless of cirrhosis)
9297 97 98 94 94 100
0
10
20
30
40
50
60
70
80
90
100
GT 1aGT 1b GT 2 GT 3 GT 4 GT 5 GT 6
Roberts et al. EASL 2017; Jacobson et al. Gastro 2017
Slide 40 of 52
Slide 48 of 55
Sofosbuvir/velpatasvir/voxilaprevirNS5A Inhibitor DAA -Experienced
►POLARIS 1
–GT 1-6 (30% GT3)
►12 weeks of therapy
– vs placebo
►Including compensated cirrhosis (46%)
►2.2% relapse
►4 GT 3 relapse – all 3a and ¾ had BL NS5A RAS
►No treatment emergent RAS
►all VF had cirrhosis (6 R, 1 VBT)
Bourliere et al. NEJM 2017
Slide 49 of 55
Does Failure = Resistance?
Louisville, Kentucky, November 17, 2017 13

Slide 50 of 55
Key HCV Resistance Concepts
HCV resistance associated substitutions (RASs) can
be present without drug exposure
HCV RASs impacts treatment responses in specific
situation
HCV is resistance is NOT absolute
Patient characteristics are just (if not more) important
than RASs
Future regimens appear to obviate the need for most
resistance testing
Slide 51 of 55
Resistance Characteristics of HCV Antiviral Classes
ClassAntiviral Potency
GenotypeActivity
ResistanceBarrier
FDA Approvals
NS3 ProteaseInhibitors
+++ to ++++1, 4
(± 2, 3, 6)
Lowto
High
Simeprevir (2013)Paritaprevir (2014)Grazoprevir (2016)Voxilaprevir (2017)Glecaprevir (2017)
NS5B Nucleotide ++++ 1-6 Very High Sofosbuvir (2013)
NS5BNonnucleoside
++ 1 Low Dasabuvir (2014)
NS5A Inhibitors ++++1, 4, 6
(± 2, 3)
LowTo
High
Ledipasvir (2014)Daclatasvir (2015)Ombitasvir (2014)
Elbasvir (2016)Velpatasvir (2016)Pibrentasvir (2017)
*anticipated US FDA approvals
Slide 52 of 55
Broad Cross-Resistance With “Early Generation” NS5As
Fold Change Genotype 1a Genotype 1b
M28T Q30R L31M/V Y93H/N L31V Y93H/N
Ledipasvir 20x > 100x> 100x/
> 100x
> 1000x/
> 10,000> 100x/--
Ombitasvir > 1000x > 100x< 3x > 10,000x/
> 10,000x< 10x 20x/50x
> 100x
Daclatasvir > 100x > 1000x> 100x/
> 1000x
> 1000x/
> 10,000x< 10x 20x/50x
Elbasvir 20x > 100x> 10x > 1000x/
> 1000x< 10x > 100x/--
> 100x
Velpatasvir < 10x < 3x 20x/50x> 100x/
> 1000x< 3x < 3x/--
Pibrentasvir < 3x < 3x < 3x < 10x/< 10x < 3x < 3x/< 3x
Ruzasvir < 10x < 10x < 10x < 10x < 10x < 10x
Louisville, Kentucky, November 17, 2017 14

Slide 53 of 55
Objectives
Epidemiology
Natural History
Staging
Genome and Drug Targets
Viral Kinetics With Therapy
Current Treatments
What Does SVR Really Mean?
Slide 54 of 55
Long-Term Follow-Up of SOF Phase 3 Studies
Median time to follow-up: 170 days (~ 24 weeks) after SVR24
Of 480 patients with SVR24 from phase 3 trials, 435 (91%) and 90 (19%) had post-treatment week 48 and 72
data, respectively Cheng W, et al. EASL 2014. P1112.
78/78 52/52 88/88 37/37 84/84 185/185 1/1
Slide 55 of 55
JAMA. 2012;308(4):370-378. doi:10.1001/jama.2012.7844
Louisville, Kentucky, November 17, 2017 15

Slide 56 of 55
Clinical Benefits of SVR:
Liver Failure, HCC
Liver Failure
Live
r Fa
ilure
(%
)
Time, y
Hep
ato
cell
ula
rC
arci
no
ma
(%
)
Time, y
Hepatocellular Carcinoma
van der Meer AJ, et al. JAMA. 2012;308(24):2584–2593.
530 Europeans followed for a median 8.4 years after HCV treatment
192 (36%) achieved SVR
Slide 57 of 55
Effects of SVR on the risk of liver transplant, hepatocellular carcinoma,
death and re-infection:
meta analysis, 129 studies, 34,563 patients
Hill AASLD 2014
5-year risk of hepatocellular carcinoma
by SVR
General: 21 stud
n=12,496Avg. FU=6.1 years
Cirrhotic: 18 stud
n=4,987Avg. FU=6.6 years
HIV/HCV: 3 studies
n=2,085Avg. FU=4.7 years
5-year risk of death (all-cause)
by SVR
Gen 18 stud
n=29,269Avg. FU=4.6 years
Cirr 9 stud
n=2,734Avg. FU=6.6 years
HIV/HCV: 5 stud
n=2,560Avg. FU=5.1 years
Slide 58 of 55
Louisville, Kentucky, November 17, 2017 16







![Hepatitis B virus and hepatitis C virus play different ... · alcoholic cirrhosis, hepatitis viruses, tobacco and metabolic diseases[4]. Hepatitis viruses, including hepatitis B virus](https://img.dokumen.tips/doc/110x75/60e46cab5bd9101a6f539e91/hepatitis-b-virus-and-hepatitis-c-virus-play-different-alcoholic-cirrhosis.jpg)





















