Embed Size (px)
Citation preview

British Journal of Industrial Medicine 1988;45:14-18
Welders' pneumoconiosis: tissue elementalmicroanalysis by energy dispersive x ray analysisA FUNAHASHI, DPSCHLUETER, K PINTAR, EL BEMIS,*K A SIEGESMUND
From the Departments ofMedicine and Pathology of the Clement J Zablocki Veterans Administration MedicalCenter, Milwaukee, Wisconsin, and the Departments ofMedicine, Pathology, and Anatomy of the MedicalCollege of Wisconsin, Wisconsin, USA
ABSTRACT Histological examination on lung tissue obtained from 10 symptomatic welders was
performed by two certified pathologists without the knowledge of the patients' clinical condition. Inall cases, there was some degree of interstitial fibrosis; in five the degree of fibrosis was consideredto be moderate to pronounced. The tissue was also analysed by energy dispersive x ray analysis andelemental contents were compared with age matched controls. There was a large amount of iron inthe lungs of welders but the silicon content did not differ from the control subjects. No specificforeign element was detected. It is concluded that (1) interstitial pulmonary fibrosis is seen in somewelders and (2) the cause of fibrosis does not appear to be coexisting silicosis.
Since the first description by Doig in 1936, welders'pneumoconiosis has been considered to be benign.12Nevertheless, in several reports welders' pneu-moconiosis has been associated with clinical symp-toms and physiological abnormalities.38 Sincewelders are often exposed to a variety of inorganicmaterials including silica, which is known to be highlyfibrogenic to the lung, coexisting silicosis has beensuggested as an aetiological factor in symptomaticwelders. There are few data, however, regarding theactual dust burden in the lungs of welders. Energydispersive x ray analysis (EDXA) is a relatively newmethod of elemental analysis which allows a simulta-neous, multi-elemental analysis while samples arebeing examined by either scanning electron micro-scope (SEM) or scanning transmission electronmicroscope (STEM). We have previously used thismethod of analysis to study interstitial pulmonaryfibrosis associated with silicosis and found it to beuseful in discriminating fibrosis secondary fromsilicosis of other causes.9 This report is based on astudy of 10 welders who had respiratory symptomsand abnormal chest radiographs. Nine had open lungbiopsies for diagnosis and in one case the tissue wasobtained at necropsy. The tissue specimens were thenprocessed for tissue elemental analysis by EDXA.
*Dr Bemis died on 13 January 1984.
Accepted 9 March 1987
Material and methods
All 10 cases had been seen at one of the metropolitanMilwaukee hospitals. Clinical records and the resultsof pulmonary function studies were available. In mostcases the chest radiographs were avaiable for review,in the remainder official interpretations by the radiol-ogist were used. Forced expiratory spirograms wereperformed on a Stead-Wells spirometer and lung vol-ume measurements were performed by the heliumdilution method. Diffusing capacity (DLCO) wasmeasured by a single breath holding method. Pre-dicted values for spirometry were taken from Morriset al, 0 lung volumes from Boren et al, " and DLCOfrom Burrows et al."2 The decision for biopsy wasmade by the attending physicians and pulmonaryconsultants concerned. No biopsy was performed forthe purpose of this investigation.
Histological specimens were stained byhaematoxylin-eosin and Prussian blue and examinedindependently by two certified pathologists with noprior knowledge of the clinical history. They wereasked to grade the pathological findings into six cate-gories: (1) fibrosis, (2) alveolar wall thickening, (3)cellular infiltrates, (4) iron content, (5) bronchiolarchanges, and (6) vascular changes. The pathologicalchanges were graded as absent, minimal, slight, mod-erate, or pronounced. The method of study by SEMand EDXA has been reported.'3 Briefly, paraffinembedded specimens were cut at 40 ,im thickness and
14
copyright. on F
ebruary 15, 2021 by guest. Protected by
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.45.1.14 on 1 January 1988. D
ownloaded from

Table 1 Individual patient profiles, chest x ray abnormalities, andpulmonary function results
Pulmonaryfunction
Duration Radiograph FVC FEVI FEV1/FVC DLCOAge Sex Occupation (years) Symptoms report (% predicted)
1 36 M Welder 12 Cough, dyspnoea Diffuse nodular 76 72 76 562 56 M Welder 26 Dyspnoea Diffuse nodular 67 64 71 803 55 M Gas Cutter 24 Dyspnoea Reticulonodular 58 64 79 844 36 M Welder 15 Dyspnoea Diffuse nodular 73 72 78 735 31 M Gas Cutter 8 Dyspnoea Diffuse nodular 86 93 87 936 47 M Welder 23 Cough Reticulonodular 67 68 81 727 60 M Welder 40 Dyspnoea Diffuse nodular 82 87 80 1048 60 M Welder 30 Cough Diffuse nodular 91 77 64 -
9 49 M Gas cutter 10 Dyspnoea Diffuse nodular 87 86 78 9510 63 M Welder 40 Dyspnoea Diffuse nodular 76 70 68 113
deparaffinised by passage through graded alcoholsand finally floated in water. The specimens were thenplaced on an electromagnetically pure carbon stuband air dried. They were examined by a JSM-35Cscanning electron microscope equipped with an OrtecSI solid state detector. The analyses were performedwith magnification of 100 which allowed an analysisof 1 mm in each area. A total of five area analyses wasperformed and the results were expressed aselement/sulphur ratio, as described previously, inorder to compensate for differences in tissue mass ineach area of analysis."3 Si/S and Fe/S ratio were then
compared with 10 age matched controls and 10 casesof well established silicosis previously studied in ourlaboratory. Student's t test was used for statisticalanalysis.
Results
Table I shows individual patient profiles, chest radio-graphic abnormalities, and pulmonary functionresults. Age ranged from 31 to 63 (mean 49 3) and theduration of welding from eight to 40 years (mean22-8). All were symptomatic and complained of dys-
Ak,~~~~s:
4,P
.... ~~'''' wabs;,.;' . ,."r , ..,X
.4~~~~~~~~~~~~~~.d^ > < t . . R <a sj; <stt
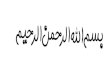
'~~~~""A~i*ii^ E+L>Fig 1 Lower magni~fication shows lung periphery with pleura. Delicate intra-alveolar septa are next tothickened septa with deposition of iron andfibroplasia. There isfocalfibrosis ofpleura and thickening ofblood vessels (arrowheads). (Haematoxylin-eosin stain, original magnification x 50.)
Welders'pneumoconiosis 15
copyright. on F
ebruary 15, 2021 by guest. Protected by
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.45.1.14 on 1 January 1988. D
ownloaded from

Funahashi, Schlueter, Pintar, Bemis, Siegesmund
8
Fig 2 Higher magnif-ication showsfocalfibrosis ofsepta andpleura with iron deposition.(Haematoxylin-eosin stain, original magnification x 160.)
Table 2 Main pathological changes
Min Slight Mod Pronounced
Fibrosis 2 3 4 1Alveolar wall thickening 2 3 4 1Iron content 0 1 4 5
pnoea, except cases 6 and 8 who complained of coughonly. All had abnormal chest radiographs showingdiffuse small nodular densities.
PULMONARY FUNCTION STUDYTable 1 also shows pulmonary function test results.Seven patients showed a restrictive impairmentwhereas two had mild to moderate airways obstruc-tion.8 10 Diffusing capacity was reduced in three ofnine patients who also had restrictive impairment.
PATHOLOGICAL FINDINGSTable 2 shows the main pathological findings in the10 cases. In no case was there a difference in inter-pretation of more than one grade between the twopathologists. When there was a difference in grading,the lower grade was used to express the degree ofpathological changes. All had some degree of fibrosis.In five cases the degree of fibrosis was considered to
be moderate to pronounced. In seven cases alveolarwall thickening was noted to be moderate topronounced.
ILLUSTRATIVE CASEFigures 1 and 2 show lung tissue from one subject(case No 7) in which the degree of fibrosis was consid-ered to be slight. The specimen showed iron pigmentsin the alveolar macrophages and in the alveolar septa.The iron deposition in the tissue is patchy, locatedmainly subpleurally and around blood vessels and thebronchial walls. The deposition of iron in theselocations is associated with a mild lymphocyticinfiltration and with proliferation of myofibroblasts.The resulting small nodularity and fusion of adjacentnodules produced the patchy appearance. The luminaof the affected vessels are often compromised or oblit-erated. The pleura is focally thickened.
ELEMENTAL CONTENT IN TISSUETissue elemental contents expressed as Si/S ratio andFe/S ratio are shown in fig 3. Mean Si/S ratio showedno difference between controls and welders whereaspatients with silicosis had a significantly (p < 0 005)higher ratio than controls and welders. The meanFe/S ratio was slightly higher in patients with silicosis
16
4. i..
A :.4 ..
.04.
i fI.4 wo- itV ,,
copyright. on F
ebruary 15, 2021 by guest. Protected by
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.45.1.14 on 1 January 1988. D
ownloaded from

Welders' pneumoconiosis
I
9-080
7*0
60
5*0
4*0
30
.2
u,) 2 0
1 0
0*5
0*40*30.1
(i
I
ILLKIL~I&1.1
o(' \\F>ge,
1
0
LI
I I
G'4§
140T
Fig 3 Silicon/sulphur ratio (Si/S) and iron/sulphur ratio(Fe/S) in three groups ofsubjects.
than in controls but the difference did not attain sta-tistical significance. The Fe/S ratio is significantlyhigher in welders as compared with controls andpatients with silicosis (p < 0-0025). No other ele-ments were found to be raised in the welders.
Discussion
In 1936 Doig described abnormal chest radiographsin six of 16 welders; all six were asymptomatic. 1 Enzerand Sanders reported the first pathological descrip-tion of welders' pneumoconiosis in a subject who hadan abnormal chest radiograph and died from an acci-dent.14 They found little fibrosis despite a large accu-
mulation of iron in the alveolar spaces. In 1948 Doigreported that the radiographic abnormalities in twoof his original series of patients cleared after they wereremoved from exposure.'5 Morgan and Kerr studiedseven welders with radiographic abnormalities. 16Three of these seven cases had mild respiratory symp-
toms. Histological examination showed a largeamount of iron, primarily in the alveolar space withlittle interstitial fibrosis. In one case there was consid-
17
erable fibrosis but tuberculosis was also present andhe had had exposure to other dusts. Spectrographicstudy of the lung tissue showed an increased amountof silica along with increased iron. The cause offibrosis was attributed to his pulmonary tuberculosis.The authors concluded that welders' siderosis is abenign condition and "those welders described in theliterature, in whom obstructive airway disease andassociated carbon dioxide retention was present, weremost probably suffering from the effect of concomi-tant bronchitis and emphysema." A review of thepublished reports showed that many symptomaticwelders indeed had obstructive ventilatoryimpairment on their pulmonary function studies andhistological examination showed emphysematouschanges.36 In the present series all subjects had clin-ical symptoms of dyspnoea or cough. The most prev-alent pulmonary function abnormality found wasthat of restrictive impairment except in subjects 8 and10 in whom a mildly reduced FEV1/FVC ratio indi-cated some airways obstruction. The degree ofobstruction, however, was not considered severeenough to explain their symptoms and the patientsunderwent open lung biopsies. Furthermore, all oursubjects showed interstitial fibrosis to some degreewhich is not a feature of obstructive airways disease.In 1967 Meyer et al reported a case of pulmonaryfibrosis in arc welders.7 A spectrographic analysis ofthe lung tissue showed that silica was 30% of the totaliron content. Since welding rod coating material maycontain elements such as titanium, silicon, mag-nesium, manganese, calcium, and copper and thepatient had no history of exposure to silica, theauthors concluded that the fibrosis observed was dueto coexisting silicosis from exposure to fumes fromthe electrode coating. This view was supported byPatel and Kumat who also reported a case of welders'pneumoconiosis with interstitial fibrosis.8 In thepresent study the results of elemental analysis byEDXA showed that the silicon content of the welders'lung tissue was similar to that of controls. Thisfinding would support the contention that coexistingsilicosis due to coating material was not the cause ofinterstitial fibrosis. Recently, Stettler et al used anelectron probe microanalyser together with a scan-ning transmission electron microscope to study thelung tissue from two welders.17 The first case hadminimal fibrosis but the second case had "more exten-sive interstitial fibrosis." They analysed particles inthe lung greater than 0 2 gm and found that most par-ticles contained iron, chromium, manganese, ornickel and that a small percentage of these particleswas classified as silicate or silica. In 1978 Guidotti etal also studied the lung tissue of a welder who hadsevere interstitial fibrosis with EDXA together withSEM. 8 They also used a high magnification (2000 x )
copyright. on F
ebruary 15, 2021 by guest. Protected by
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.45.1.14 on 1 January 1988. D
ownloaded from

18
and analysed particles seen inside the individual cellsand found them to contain iron and silicon. BothStettler et al and Guidotti et al emphasised the use-fulness of in situ microanalysis of small particles seenin the lung tissue.17 18 We have used a similar tech-nique to analyse black particles seen in cases of pul-monary interstitial fibrosis, and found that theseparticles contain chromium, iron, cobalt, andnickel.'4 In the present study we used a lowermagnification that allowed us to cover a larger areafor analysis. We believe that the higher magni-fications used by Stettler et al, Guidotti et al, and inour previous study of interstitial fibrosis are useful inidentifying the elemental composition of individualparticle(s) of smaller size (less than I gm) but are notsuitable to estimate the overall dust burden of the tis-sue.9 Interstitial fibrosis is a reaction of lung tissue tovarious insults. Therefore, the interstitial fibrosis seenin our patients is possibly a mere coexistence of weld-ers' siderosis and idiopathic pulmonary fibrosis. If,however, idiopathic pulmonary fibrosis developed inthe lung with benign welders' siderosis in which ironparticles are seen in the alveolar space, one wouldexpect those particles to remain in the alveolar space.The fact that many iron containing particles are seenin the fibrosed alveolar septa would suggest that theobserved fibrosis is a reaction to those particles. Fur-ther investigation is warranted in this interesting clin-ical entity to see if heavy metals contained in ironparticles are indeed responsible for the fibrosis seen inthese patients. From the clinician's standpoint, it isimportant to recognise that welders who have noexposure to silica or asbestos may develop interstitialfibrosis leading to respiratory symptoms and phys-iological abnormalities although it is uncommon. Weconclude therefore that (1) welders' pneumoconiosismay be associated with interstitial fibrosis; (2) theassociation of welders' pneumoconiosis and inter-stitial fibrosis appears to be more than coincidental;and (3) the cause of interstitial fibrosis in this group ofwelders with pneumoconiosis did not appear to bedue to associated silicosis, since silica concentrationsin the lung were within normal limits.
Funahashi, Schlueter, Pintar, Bemis, Siegesmund
This study was supported by a Veterans Adminis-tration research grant.
ReferencesI Doig MB, McLaughlin ALG. X-ray appearance of the lungs of
electric arc welders. LancetI 936;i:771-5.2 Park WR. Occupational lung disease. London: Butterworth,
1982:113-7.3 Charr R. Respiratory disorders among welders. JAMA
1953;132: 1520-2.4 Charr R. Respiratory disorders among welders. Am Rev Respir
Dis 1955;71:877-84.5 Charr R. Pulmonary changes in welders. A report of three cases.
Ann Intern Med 1956;44:806-12.6 Friede E, Rachow DO. Symptomatic pulmonary disease in arc
welders. Ann Intern Med 1961;54:121-7.7 Meyer E, Kratzinger SF, Miller WH. Pulmonary fibrosis in arc
welder. Arch Environ Health 1967;15:462-8.8 Patel KC, Sheth SM, Kamat SR. Arc welders' lung. J Postgrad
Med 1977;23:35-8.9 Funahashi A, Schlueter DP, Pintar K, Siegesmund KA. Value of
in situ elemental microanalysis in the histologic diagnosis ofsilicosis. Chest 1984;85:506-9.
10 Morris JF, Koski A, Johnson LV. Spirometric standard forhealthy non-smoking adults. Am Rev Respir Dis1971;103:57-67.
11 Boren HG, Kory RC, Syner JC. The Veterans Administrations-Army Cooperative study of pulmonary function II. The lungvolume and its subdivision in normal man. Am J Med1966;43:96-1 13.
12 Borrow B, Kask JE, Niden AH. Clinical usefulness of the single-breath pulmonary diffusing capacity test. Am Rev Respir Dis1961 ;84:789-806.
13 Funahashi A, Pintar K, Siegesmund KA. Identification of foreignmaterial in lung by energy dispersive x-ray analysis. Arch Envi-ron Health 1975;30:285-9.
14 Enzer N, Sander OA. Chronic lung changes in electric arc weld-ers. Journal of Industrial Hygiene and Toxicology1 938;20:333-50.
15 Doig AT, McLaughlin ALG. Clearing of x-ray shadows inwelder's siderosis. Lanc et 1948;i:789-91.
16 Morgan WKC, Kerr HD. Pathologic and physiologic studies ofwelder's siderosis.Ann Intern Med 1963;55:293-304.
17 Stettler LE, Groth DH, Mackay GR. Identification of stainlesssteel welding fume particulates in human lung and environ-mental samples using electron probe microanalysis. Am IndHyg Assoc J 1977;39:76-82.
18 Guidotti TL, DeNee PB, Abraham JL, Smith JR. Arc welderspneumoconiosis: application of advanced scanning electronmicroscopy. Arch Environ Health 1978;33:117-24.
19 Siegesmund KA, Funahashi A, Pintar K. Identification of metalin lung from a patient with interstitial pneumonia. Arch Envi-ron Health 1974;28:345-9.
copyright. on F
ebruary 15, 2021 by guest. Protected by
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.45.1.14 on 1 January 1988. D
ownloaded from