Embed Size (px)
Citation preview

Welcome to Boot Camp 6
Preventing Complications & Exercise
Summer / Fall 2020Beverly Dyck Thomassian, RN, MPH, BC-ADM, CDE
President, Diabetes Education Services

Diabetes – Microvascular
Complications
Objectives:� Discuss the importance of
oral care
� Eye, kidney and nerve
complications
� Describe modifiable and non-
modifiable risk factors for
diabetes complications
� List screening guidelines
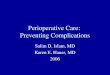
Eye Disease and Education
� Diabetes Retinopathy
� Other Diabetes Eye Complications
� Prevention and Treatment
� Promoting Self-Care

Eye Disease Overview� Leading cause of adult
blindness � Retinopathy and Diabetic Macular
Edema
� DM = 25x’s risk of ocular complications � Including cataracts
� 20% of type 2 have retinopathy at diagnosis
� Only 60% receive appropriate treatment

Quick question 1
�Which of the following describes
proliferative retinopathy?
A. Cotton wool spot and
hemorrhages
B. Increased lens opacity
C. Stiffening of the lens
D. New blood vessel growth

Fundus Geography
Macula
The retina is the only portion of the central nervous system visible from the exterior. Likewise the fundus is the only location where vasculature can be visualized.
Fundoscopy

What is Retinopathy?
� Retina – layer of nerve tissue in back of eye responsible for processing images and light
� Damage to the microvascularlayer that nourishes the retina
� Leads to leakage of blood components through vessel walls and creation of unstable blood vessels hypoxia
� Disturbance in nerve layer = visual symptoms

Non - Proliferative to Proliferative
Diabetic Retinopathy

Proliferative retinopathy
New blood vessel formation on surface of retina or the optic nerve. Severe visual loss can occur due to vitreous hemorrhage and retinal detachment. Note fine network of new blood vessels on the surface of the optic nerve
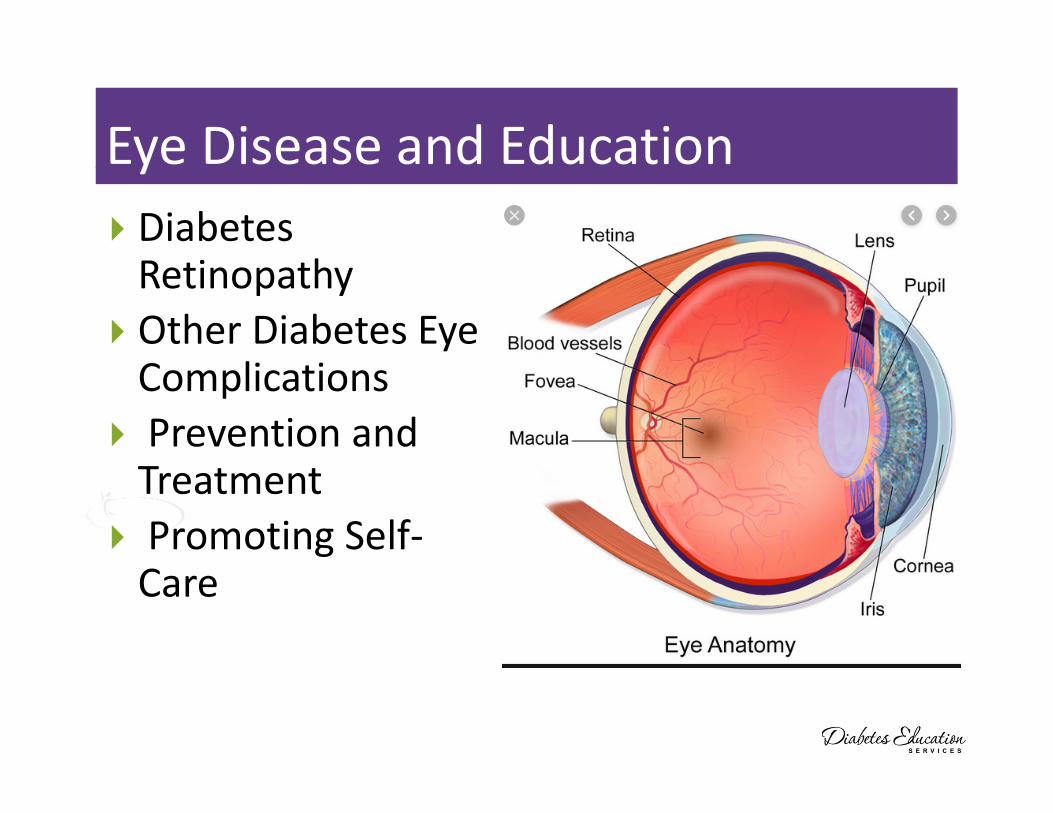
Retinopathy Changes How We See
View of boys by person with normal vision
View of boys by person with diabetic retinopathy.

Pan Retinal Photocoagulation
Decreases risk of severe vision
loss by 50% or more
Destroys 12% of retina and loss of
visual field.
Once stabilized, can achieve
excellent control of PDR
if B/P and BG well controlled.
Injections with Vascular
Endothelial Growth Factor (VEGF)
Inhibitors may also be considered
Treatment for Retinopathy

Retinopathy Prevention
� To reduce the risk
or slow the
progression of
retinopathy
� Optimize
glycemic control
� Optimize blood
pressure control

Quick Question 2
� Which of the following is correct
regarding eye screening for people with
diabetes?
A. All people with diabetes must get a
complete eye exam every year
B. All people diagnosed with type 1 and type 2
need an immediate eye exam.
C. All people diagnosed with type 2 need an
immediate eye exam.
D. People with diabetes over age of 60 should
receive an eye exam every 6 months.

Retinopathy Screening
� Screen with initial dilated and
comprehensive eye exam by
ophthalmologist or optometrist
� Type 2 at diagnosis, then every 1 to 2 yrs
� Type 1 within 5 yrs of dx, then every 1-2 yrs
After initial exam, then…
� Annual exam
� Less frequent (every 2-3) yrs can be considered
if 1 or more normal eye exam
� More frequent if retinopathy progressing
� Refer pts with macular edema, and severe
non-proliferative disease to trained specialist

Assess adaptation to low vision
� necessary vision to perform self-care skills?
� Insulin, Blood glucose monitoring
� shopping/home safety/transportation
� refer to rehab education (800-AFBLINE) or
website www.afb.org

Tools for People with limited vision
� Reading glasses from the dollar store
� Magni-Guide by BD from pharmacy

Prodigy Voice Meter – A+ Access Award
Am Fed Blind
Prodigy Meter only completely
accessible meter for sale in
U.S. - independent access for
visually impaired -
•www.prodigymeter.com
•800-243-2636
•Independent set up
•Self coding
•Audible Memory and error

Diabetes Kidney Disease
� Diagnostic tests to assess
and monitor renal function
� Screening and prevention

Quick Question 3
� John’s dad had diabetes and kidney failure. He
wants to learn the risk factors for kidney
disease. Which of the following describe those
at increased risk for kidney disease?
A. Excessive alcohol intake and daily Tylenol
B. Family history of kidney disease, smoking
C. High protein diet and excessive trans-fat
intake
D. Diet high in processed foods and sodium

Diabetes and Chronic Kidney Disease
(CKD) Considerations
� CVD leading cause of death in CKD
� microalbuminuria = increased risk of CVD
� 1/4 to 1/3 of insulin cleared by kidney
� renal retinal syndrome
� 70 - 80% of people with diabetes
DON’T get kidney disease
� Early and aggressive intervention
crucial

Keep Kidneys Healthy
To reduce the risk or slow
the progression of
nephropathy
� Optimize glucose
control
� Optimize blood
pressure control

Screening for Kidney Disease
Screen who?� Type 2 at dx then yearly
� Type 1 with diabetes for 5 years, then yearly
� For all with diabetes with hypertension
� Screen what?� Urinary albumin - Spot urine Albumin-
Creatinine Ratio (UACR) and
� Glomerular Filtration Rate (GFR):
� Assess Yearly� Measure urinary albumin, serum and
estimated GFR

Definitions of Abnormalities in Albumin
Excretion
� Urine albumin – creatinine ratio (spot
collection)
Category mg/g creatinine
� Bormal <30
� Moderately increased urinary albumin 30-299
� Severely increased urinary albumin >300
� 2 of 3 tests w/in 3-6 mo abnormal to confirm
� If greater than 30 with elevated B/P, consider treatment ACE or ARB
� Also consider using SGLT-2 or GLP-2 to protect kidney

GFR + Albuminuria - CKD Stages and Care
Microvascular Complications and Foot Care:
Standards of Medical Care in Diabetes - 2018. Diabetes Care 2018; 41 (Suppl. 1): S105-S118
ADA Standards 2020 – Standard 11 Microvascular Complications

� Refer for evaluation for renal replacement treatment if eGFR <30
� Promptly refer to a physician experienced in the care of kidney disease for uncertainty about the etiology of kidney disease, difficult management issues, and rapidly progressing kidney disease.
Microvascular Complications and Foot Care:
Standards of Medical Care in Diabetes - 2018. Diabetes Care 2018; 41 (Suppl. 1): S105-S118
Diabetes Kidney Disease (DKD)Treatment

Treatment of Chronic Kidney
Disease (CKD)
There are four primary treatment options for individuals who experience ESRD:
1. Hemodialysis
2. Peritoneal Dialysis
3. Kidney Transplantation
� 120, 000 Americans waiting for kidney
� Only 17,000 receive one each year
� Every day, 12 people die waiting for a kidney
4. No treatment

Psychosocial Issues associated with
Chronic Kidney Failure
� depression
� stress
� anxiety
� support groups,
counseling and coping
skills

Diabetes Nerve Disease Objectives
� Causes of
neuropathy
� Different types of
neuropathy
� Detection,
prevention and
treatment
� Key info to teach
about neuropathy

Quick Question 4
� What 2 office tests can be used to detect
diabetes neuropathy?
A. Pin prick and electrophysiology
testing
B. Monofilament and tuning fork
C. Hot/Cold discrimination testing
D. Babinski reflex assessment

Nerve disease Screening
� Screen all people with diabetes for nerve disease using simple tests, such as a monofilament
� Type 2 at diagnosis, then annually
� Type 1 diabetes at 5 years, then annually
� Tight glycemic control is the only
strategy shown to prevent or
delay the development and
progression of neuropathy.
� Assess and treat patients to reduce pain and symptoms to improve quality of life.

Skin Biopsy to Assess Neuropathy

3 Types of Neuropathy
� Generalized Symmetrical
Polyneuropathy
� Acute sensory
� Chronic sensory (distal)
� Small fiber
� Large fiber
� Autonomic Neuropathy
� Focal and Multifocal
Neuropathy

Generalized Symmetrical Polyneuropathy
Chronic Sensorimotor NeuropathySmall Nerve Fiber
� Sensory deficits in distal portions, spreading medially “stocking-glove”
� Small Nerve Fiber Neuropathy� C-fiber pain = burning and superficial
� Allodynia (all stimuli interpreted as painful)
� Later, loss of pressure and temp sensation
� Decrease blood flow, sweating
� Detect w/ Monofilament
� High risk for ulceration, Charcot, gangrene

Generalized Symmetrical Polyneuropathy
Chronic Sensorimotor Neuropathy – Large Nerve Fiber
� Involve sensory and/or motor nerves
� Fibers are myelinated, rapid conductors
� Can detect destruction w/ nerve testing
� Symptoms may be minimal:
� Impaired vibration perception/position sense
� Ataxia “moon-walking”, in-coordination
� Pain described as deep-seated gnawing
� Shortening of Achilles tendon and claw foot
� Increased blood flow “hot foot”

Treating Neuropathy
� Improve glycemic control
� Control pain
� Relief from depression from
chronic pain
� Massage, stretching,
� Pain control clinic,
� Transcutaneous Electrical Nerve
Stimulation (TENS)
� Avoid alcohol
� Relaxation exercises....

Pharmacologic Therapy for Neuropathy
Try Alpha lipoic acid: 600 – 1,800mg /day. B12 deficiency?
Prescription Therapy
1st line
• Tricyclic antidepressants (ie amitriptyline, nortriptyline
• Calcium channel modulators (ie gababentin, pregabalin)
• Serotonin Norepinephrine Reuptake Inhibitors (SNRI)
2nd line• Topical Capsaicin Cream
• Opioids (tramadol, oxycodone)
Reasons for treatment failure:
• Dose too low, inadequate trial, pt expecting elimination of symptoms, not changing class when no response
Ziegler, D Painful diabetic neuropathy. Diabetes Care, 2009
Other strategies to help ease the pain
� Music
� Podcasts
� Movies
� Pet’s
� Massage
� Touch
� Topical creams
� Lidocaine patches
� Mineral salts baths
� Tylenol / Ibuprofen
� Earthing
� Sleep
� Hobbies
� Aromatherapy
� Time with special people
� Work / volunteering

Fancy Creams and Stuff

Quick Question 14
� Which of the following are at most risk
for developing diabetes autonomic
neuropathy?
A. Diabetes for 1 year with A1c of 7.6%
B. Person with diabetes for 16 years
with A1c never above 6.9%
C. Person with type 1 diabetes for 8
years with retinopathy
D. Person with type 2 for 19 years with
A1c less than 7.5%

“DAN” Diabetic Autonomic
Neuropathy
� 50% of ind’s with peripheral neuropathy also have DAN
� DAN increases M & M rates
� neurogenic bladder, sexual dysfunction
� GI related disorders / gastroparesis
� orthostatic hypotension
� fixed heart rate, silent MI, sudden death
� hypoglycemia unawareness
� sudomotor, pupillary
Who is DAN?

Sexual Functions as We Age
� 20-30 years trice daily
� 30-40 years tri weekly
� 40-50 years try weekly
� 50-60 years try weakly
� 60-70 years try oysters
� 70-80 years try anything
� 80-90 years try to remember
A touch of humor from AADE-New Perspectives on Erectile Dysfunction, 1999

Improving Sex Life for WomenTreatment
� Lower blood glucose / blood pressure
� Treat vaginal infections and UTI’s
� Water based lubricants for vaginal dryness
� Hormone replacement therapy
� Eat to prevent lows during intimacy
� Allow time, touching and romance
� Women with diabetes get more vaginal and bladder infections
� Difficulty achieving orgasm due to neuropathy
� Painful intercourse due to lack of vaginal lubrication

Erectile Dysfunction
� Affects about 50% of men with diabetes
� Loss of erections sufficient for intercourse
� Due to combo of vascular and nerve damage
� Tests: penile tumescence to eval if organic or
psychogenic
� Treatment:
� Sildenafil (Viagra), Vardenafil (Levitra), Tadalfil
(Cialis)
� Use caution if taking nitrate drugs. Check w/ MD first
� Other meds, vacuum devices, prosthetics
� HRT- testosterone gel, patches, injections, pills
Men with Diabetes 2x’s risk for low
testosterone� Symptoms include low sex drive,
ED, depression, lack of energy and vitality
� Low T easily diagnosed and managed, only 10% of men currently treated
� Initial Screening:� Total testosterone: if < 300 ng/dl =
hypogonadal
� am testing preferred, repeat to confirm
� Treatment: determine cause, testosterone replacement therapy

Neuropathy Key Considerations
� Very common long-term complication often not recognized and treated
� Management / treatment complex
� Thorough history /assessment critical
� Treatment based on underlying process, presentation, and cost effectiveness
� Treatable condition with new therapies on horizon.

The ABC’s of Diabetes Management
A - A1c less than 7%
B - Blood pressure
C - Cholesterol HDL > 40, Triglycerides < 150
D - Drugs- Keep list for emergencies/ MD
E - Exercise and Eyes
F - Food and Feet
G – Glucose checks and goals
H- Healthy Coping - Hoorah for your hard work!

Getting Active Objectives
� Current state of exercise in U.S.
� Benefits of exercise
� Listening to the exercise story
� Re-igniting or finding the spark
� Integrating activity into our daily lives a step at a time
� Teaching strengthening exercises

Physical Activity – Key areas
� Physical Activity/ Exercise and
Diabetes Position Statement
� Benefits, barriers precautions
� Exercise and activity plan
(aerobic, resistance training,
etc)
� Adjustment and monitoring of
food and/or meds
Definitions
� Physical activity� Bodily movement produced by the
contraction of skeletal muscle that requires more energy than when resting
� Exercise� Subset of physical activity that is planned,
structured and includes repetitive body movements
� Performed to improve or maintain physical fitness
� Sedentary behavior� Little on no movement or physical activity

Benefits of Exercise
� Increase muscle glucose uptake 5-fold
� Glucose uptake remains elevated for 24 - 48 hours (depending on exercise duration)
� Increases insulin sensitivity in muscle, fat, liver.
� Reduce CV Risk factors (BP, cholesterol, A1c)
� Maintain wt loss
� Contribute to well being
� Muscle strength
� Better physical mobility

Exercise decreases:
� Sleep apnea
� Diabetic kidney disease, retinopathy
� Depression
� Sexual dysfunction
� Urinary incontinence
� Knee pain
� Need for medications
� Health care costs
Importance of Exercise with Diabetes
� Vital component of prevention as
well of the management of type 2
diabetes
� Greatest impact in decreasing
insulin resistance and preventing
prediabetes to diabetes
� Type 1 – emphasis on adjusting
insulin to allow for safe
participation in all forms of
activity.
Exercise Standards
� Get up and move every 30
minutes! Encourage to limit sit
time to 30 minutes and to
accumulate 150 minutes of
exercise a week.
� Flexibility and balance training
2-3 xs weekly for older adults.
� Yoga and tai chi are good options to
increase flexibility, strength and
balance.

Physical Activity - Kids� Children should be
encouraged to engage
in at least 60 minutes
of moderate/vigorous
physical activity a day.
� Plus bone/muscle
strengthening 3 times
a week

Where are we on this continuum?
Only about 50% of us are
meeting activity goals

After dinner stroll “Passegiatta”
� Walk 10-15 minutes after
dinner (and other meals if
possible)
� Maximize the walking benefit
� Get the most BG lowering
effect
� Especially after high carb meals
Diabetologia, Oct 2016.

Best Medicine
� Exercise is the best medicine. Structured
exercise of 8 weeks duration, has been
shown to lower A1c by and average of
0.66% in people with type 2, even
without a significant change in BMI.

Poll question 6
� According to ADA guidelines, who most needs medical clearance before starting to exercise?
a. 25 year old, BMI 28, diabetes 5 yrs who wants to walk 30 minutes a day
b. 30 yr old male, type 1, BMI of 31 who wants to start swimming
c. 38 yr old male, type 1 for 10 yr, hx of retinopathy who wants to do triathlons
d. 38 yr old woman, BMI 32, with history of GDM who wants to start weight lifting

When to Consider Stress TestingPre-exercise medical clearance is
generally unnecessary for asymptomatic
individuals prior to beginning
low- or moderate-intensity
physical activity not exceeding the
demands of brisk walking or everyday
living.

Pre-exercise evaluation T2� In asymptomatic pts, routine
screening for CAD is not recommended.� Does not improve outcome as long as CVD
risk factors are treated.
� Assess CV risk factors annually� Dyslipidemia, HTN, smoking, positive
family history of premature coronary disease, and + albuminuria
� Candidates for advanced or invasive cardiac testing include:� Typical or atypical cardiac symptoms
� Abnormal resting ECG

People with diabetes to discuss these symptoms
with provider before starting exercise
� Chest pain and/or shortness of
breath
� Leg cramps that go away with rest
� Head, shoulder, neck and or back
aches.
� Any unexplained pain above the belt
line should be considered cardiac in
origin until proven otherwise.

Poll question 7
� What best describes normal hormone response during exercise?
a. Insulin and counter regulatory hormones are suppressed
b. Insulin levels increase, gluconeogenesis decreases
c. Insulin action is suppressed, increased gluconeogenesis
d. Increase in insulin, uptake of glycogen

Exercise effects on BG – No Diabetes
� Insulin action suppressed
� Counter regulatory hormones
� Release stored glycogen from
muscle and liver
� Increase gluconeogenesis
� To replace glycogen stores
� Glucose uptake continues for up to
48 hours

Hormone Response –Type 1
� Exogenous insulin remains high
� Increased insulin sensitivity
� Increased insulin absorption
What is this group at risk for?
What strategies to stay safe
before, during and after
exercise?

What about hyperglycemia risk?
� Type 1 – Yes
� Due to too little insulin on board
and excessive stress hormones
� Problem solving
� Inadequate insulin
� High intensity exercise
� Competitive sports
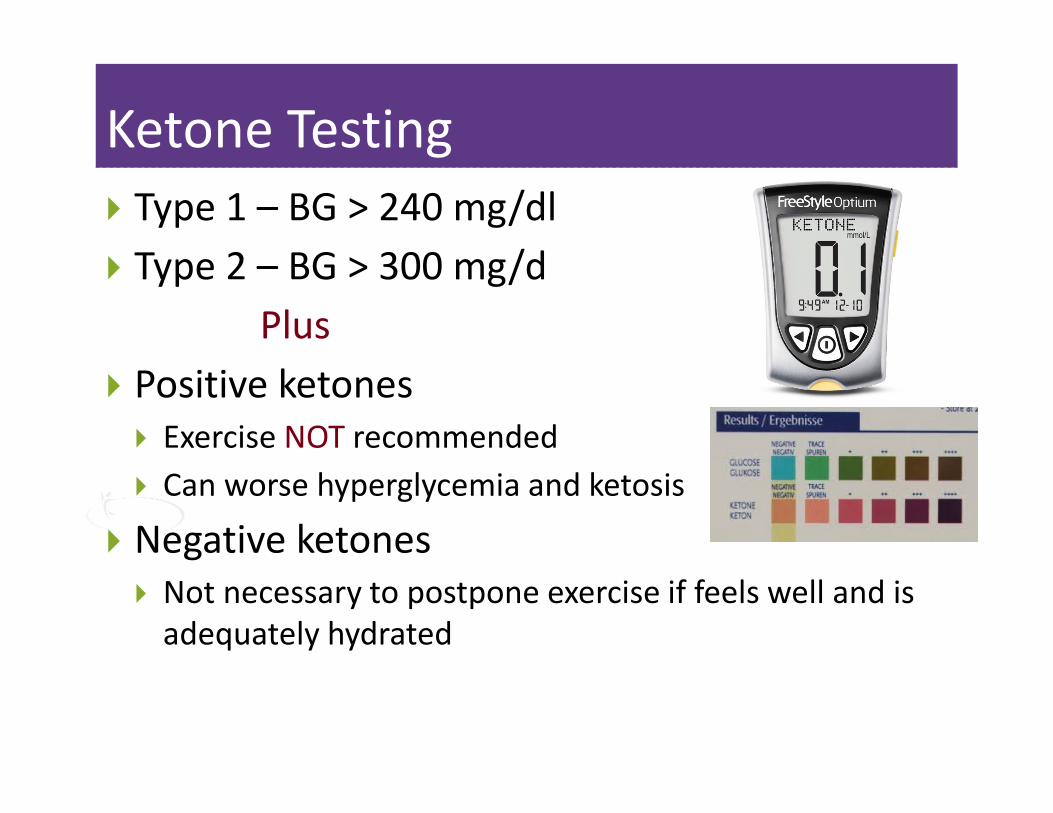
Ketone Testing
� Type 1 – BG > 240 mg/dl
� Type 2 – BG > 300 mg/d
Plus
� Positive ketones
� Exercise NOT recommended
� Can worse hyperglycemia and ketosis
� Negative ketones
� Not necessary to postpone exercise if feels well and is
adequately hydrated

Hormone Response –Type 2
� Decreased secretion of
endogenous insulin
� Increased insulin sensitivity
� Increased glucose disposal
What is this group at risk for?
What strategies to stay safe
before, during and after
exercise?

Hypoglycemic Risk
� Type 1
� Activity increases exogenous insulin
sensitivity and may block
glycogenolysis
� Type 2
� Same concern as above is on insulin
and sulfonylureas
� Low risk if treated by diet, exercise or
medications that do not cause
hypoglycemia.

Duration of Hypoglycemia Risk
� During exercise
� Immediately after exercise
� Post exercise late onset hypo
� More often in type 1
� More often at night
� Moderate to high intensity exercise
> 30 min
� 4 to 15 hours following an exercise
session

Hypoglycemia Prevention Strategies
� If planned activity, adjust insulin
in anticipation of activities
� Reduce insulin in post exercise
period
� Frequent monitoring in post
exercise period
� Pt to keep log to determine how
responds to different activities,
duration and intensity.
Poll question 8
� Adam ate breakfast, took 1000 mg of
metformin, check his BG – 98, and is going to
take a brisk 45 minutes walk. How much carb
should he eat prior to exercise to prevent
hypo?
� 15 gms
� 30 gms
� 5 gms
� none

Hypoglycemia Prevention Strategies
for Patients on Insulin/Secretagogues
� Carry carb snack/ glucagon ER Kit
� Extra Carb in post exercise period
� Caution with alcohol post exercise
� Adjust carbohydrate prior to
planned activity:
� If using insulin and /or secretagogues
� BG < 90, consume 15 -30 gms
� BG 90-150, may need ~ 15gms

Poll question 9
� Adam has type 1 diabetes. Gave 4 units bolus
insulin to cover 60gms of carb, ate breakfast,
BG 107, and is going to take a brisk 30 minutes
walk.
A. 15 gms
B. 30 gms
C. 5 gms
D. A or B

Know these Facts
� Fat - 9 cals per gm
� Carb – 4 cals per gm
� Protein – 4 cal per gm
� Alcohol - 7cals per gm
� Common food carb
count
� Milk is 12 gms of carb
� 1 lb = 3,500 cals
� 7,500 to 10,000 steps
recommended a day
� 2000 steps – 1 mile
� Alcohol serving sizes

Expert Team Toolkit
� Provides in depth
coverage of:
� MNT
� Carb counting
� CV disease
management
� Technology – from
Pumps to Sensors