Embed Size (px)
DESCRIPTION
Week 9 - Joints and Bones Systems I. Dr. Alex Alexander. Next Week: Muscle and Connective Tissue. Tendinitis and Bursitis Epicondylitis Achilles Contracture Carpal Tunnel Torticollis Rhabdomyolysis. Tendinitis and Bursitis. - PowerPoint PPT Presentation
Citation preview

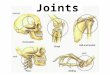
Week 9 - Joints and Bones Systems I
Dr. Alex Alexander

Next Week: Muscle and Connective Tissue
Tendinitis and Bursitis
Epicondylitis
Achilles Contracture
Carpal Tunnel
Torticollis
Rhabdomyolysis

Tendinitis and Bursitis
Tendinitis is a painful inflammation of the tendon-muscle attachment to the bone, usually in the shoulder, achilles or hamstring.
Bursitis is the painful inflammation of one or more bursae--closed sacs lubricated with small amounts of synovial fluid that facilitate the motion of muscles and tendons over bony prominences.

Toma(y)to-Toma(h)toThe term tendinosis was first used in the 1940s by a group of German researchers, however the term did not receive much attention until it was used again in the mid 1980s to describe a non-inflammatory tendon condition. The more commonly used term of tendinitis has since been proven to be a misnomer for several reasons. The first of which is that there is a lack of inflammatory cells in conditions that were typically called a tendonitis. Since inflammation is the key pathological process involved with that term, and the discovery that there in fact were no, or very few, inflammatory cells present in the condition, a new term was adopted tendinosis. This has a much greater impact then just the name one calls a condition, it also has a profound impact on how the condition is treated.

Tendinopathy• Etiology
Although tendinopathy affects millions of people, its etiology is not clear. While multiple factors including age, genetics, body weight, and muscle weakness are believed to be involved, repetitive mechanical loading of tendons is considered the major risk factor in the development of tendinopathy.
Tendons serve several functions including mechanical force transmission, joint stabilization, and shock absorption to limit muscle damage. Tendons consist of collagens, proteoglycans, glycoproteins, water, and cells. They are able to alter their structure and composition in response to mechanical loads. While appropriate mechanical loading of tendons is beneficial, overuse (chronic, repetitive mechanical loading placed on tendons) results in pathologic changes.

Diagnostic Approach
Clinical diagnosis of tendinopathy is based on careful palpation of the tendon in question. Presentation and exam features of tendinopathy at common sites are detailed below.
Imaging is not required to make a diagnosis but may assist in managing recalcitrant cases. It is important to view imaging studies in the context of their clinical findings. •Plain radiographs may show calcium deposits in calcific tendinopathy, but are not useful in soft-tissue evaluation.•Ultrasound and MRI are generally not needed but may be utilized to demonstrate tendinosis in cases that are not straightforward.•Ultrasound is quick and inexpensive, but it is highly operator dependent.•Although MRI is expensive, it allows evaluation of the surrounding structures and may aid in the diagnosis.

Tendinopathy
Treatment Approach
The main goal in the treatment of tendinopathy is to reduce pain and allow return to activity. Tendinopathies are not complicated injuries, but can be difficult to manage. Patients need to be monitored by the physician on a regular basis for response to therapy. General principles of therapy are shared among all tendinopathy sites, but details within each treatment modality vary by anatomic site.
Treatment begins with relative rest and activity modification, with ice and nonsteroidal anti-inflammatory drugs (NSAIDs) for acute pain relief. Physical therapy may be enhanced by corticosteroid injections, topical nitroglycerin, and/or specialized modalities, depending on anatomic site and response to initial therapy.

TendinopathyRelative rest and activity modification
Since tendinopathy is an overuse injury, the main initial treatment is relative rest and activity modification.
• Goal is to decrease the mechanical overload to promote tendon healing and pain relief.
• Also important to evaluate and correct athletic overtraining errors.
• For some anatomic sites, a brace or heel lift may be useful. In epicondylitis, a counterforce brace over the proximal lower arm may decrease pain and improve function. In Achilles tendinopathy, heel lifts help with pain by decreasing the amount of stretch on the Achilles tendon. In cases where dorsiflexion is diminished (tight gastrocnemius-soleus complex), a night splint may be used to hold the foot in neutral to dorsiflexion for 6 to 8 weeks to maintain passive dorsiflexion.

BursitisHistory and exam
Patients with acute bursitis typically complain of pain localized to the site of the bursa, particularly on movement. There may be a history of trauma, repetitive occupational activity, autoimmune disease, or crystal arthropathy. Infection may follow a penetrating injury or foreign body. If the bursa is superficial, swelling and erythema may be evident. In bursitis secondary to crystal deposition, the bursa is usually particularly erythematous, painful, and warm to the touch.
Chronic bursitis may last for several months and flare up many times. If inflammation persists near a joint, the patient is likely to have a limited range of active movement. Typically in bursitis, the passive range of motion is preserved, whereas active movement is limited.
Septic bursitis is most common in the prepatellar and olecranon bursae due to their superficial position. Symptoms suggestive of septic bursitis include a low-grade temperature, local erythema, swelling, and warmth, sometimes with local cellulitis.
Subacromial bursitis: classically in subacromial bursitis, the patient will complain of a painful arc on abduction of the arm due to impingement of the bursa under the coracoacromial arch. This can also occur with rotator cuff tears, and the two conditions may coexist.

BursitisTrochanteric bursitis: there may be risk factors present causing an alteration in gait. Diagnostic criteria have been proposed, but their sensitivity, specificity, and predictive value have not been established. The criteria propose that lateral hip pain and tenderness around the greater trochanter must be present in combination with 1 of the following:
• Pain at the extremes of rotation, abduction, or adduction
• Pain of contraction of the hip abductors against resistance
• Pseudoradiculopathy: pain radiating down the lateral aspect of the thigh.
Bursae of the knee: with anserine bursitis, the patient will typically complain of tenderness on the upper medial tibia at a point 3 cm to 5 cm distal to the medial knee joint line. A valgus deformity may be noted.
With prepatellar and infrapatellar bursitis, the prepatellar bursa is located between the skin and patella, and the infrapatellar bursa is between the skin and tibial tuberosity. Swelling and erythema are common, and the patella may be impalpable if a lot of fluid is present.
Olecranon bursitis: a superficial bursa, susceptible to infection and usually accompanied by significant swelling. The patient may recall direct trauma to the elbow.
Retrocalcaneal bursitis: tenderness along the distal portion of the Achilles tendon associated with swelling is typical. There may be a palpable bump, and poorly fitting shoes may play a role.

Septic Bursitis
•If septic bursitis is suspected, the fluid should be aspirated and sent for laboratory analysis with Gram stain and culture. If fluid is aspirated, it is recommended that some also be sent for crystal analysis, especially if there is a history of gout or pseudogout. Aspiration should be carried out in an aseptic manner. Superficial bursae such as the prepatellar and olecranon bursa can easily be drained, but ultrasound guidance may be useful if the bursa is deeper.

Risk Factors
occupation that causes mechanical stress on bursa
rheumatoid arthritis
gout or pseudogout
penetrating injury
osteoarthritis of the hip
infection in a nearby joint
lower limb length discrepancy
iliotibial band contracture
lumbar spondylosis
valgus knee deformity
low-riding shoes
anatomic or functional impingement within the coracoacromial arch

Key Diagnostic Features
pain at site of bursa
common
tenderness to palpation at site of bursa
common
decreased active range of motion

TreatmentThe first step in the treatment of nonseptic bursitis is to modify activity and lifestyle to minimize mechanical stress on the inflamed bursa. This involves avoiding activities that worsen symptoms (e.g., kneeling with prepatellar bursitis) and protecting the area where possible (e.g., kneepads to help avoid further trauma in prepatellar bursitis). Many patients with trochanteric and infrapatellar bursitis find crutches or a walking stick useful. It is also advisable to try to identify any predisposing risk factors that can be corrected to reduce the chance of recurrence, such as leg length discrepancy in trochanteric bursitis. It is important to rest the affected area to allow the inflammation to settle, but physical therapy may also be of benefit. Evidence from controlled trials is lacking to recommend a particular regimen; the duration of rest, and type and intensity of exercise is patient dependent. This combination of activity modification, intermittent rest, and physical therapy is often effective.
Ice may be used in the first 24 hours to reduce swelling. It can be applied topically to the area for 10 minutes at a time, every few hours (but not directly onto the skin; a thin towel is placed between ice and skin).
Simple analgesia such as acetaminophen or NSAIDs may also be required. Topical NSAIDs may be tried initially in preference to systemic NSAIDs if acetaminophen is insufficient.

EpicondylitisTypically occurs during the 4th and 5th decades of life. Patients describe a history of activities contributing to overuse of the forearm muscles that originate at the elbow.
Patients with epicondylitis report pain during or following elbow flexion and extension.
People with lateral epicondylitis are tender approximately 2 cm distal and anterior to the lateral epicondyle. They report pain during resisted wrist and digit extension, and during passive wrist flexion with the elbow extended.
People with medial epicondylitis have tenderness along the medial elbow, approximately 5 mm distal and anterior to the medial epicondyle. Pain is exacerbated with resisted forearm pronation and resisted wrist flexion.
Most patients will have complete resolution of symptoms with arm rest and nonsteroidal anti-inflammatory drug (NSAID) therapy. Patients with continued symptoms may require further treatment, including physical therapy, injection therapy, or surgical debridement.
The principal complication is continued pain. All other complications may arise from interventions attempting to alleviate the pain.

Epicondylitis
Definition
Epicondylitis of the elbow is a condition associated with repetitive forearm and elbow activities. Both lateral epicondylitis (commonly known as tennis elbow), and medial epicondylitis (commonly known as golfer's elbow), are characterized by elbow pain during or following elbow flexion and extension. A combination of poor mechanics, microtears in areas of hypoperfusion, and a delayed healing response contribute to the pathophysiology of the condition.

Classification
Classification according to anatomic location
Lateral• Prevalence is 1.3% to 3% in people aged 30 to 64 years.• Overuse injury commonly occurs within the origin of the
extensor carpi radialis brevis, but may also originate in the extensor digitorum communis or extensor carpi radialis longus tendon. Associated with activities requiring wrist extension or supination.

Classification
Medial
• Prevalence is 0.4% to 5% in people aged 30 to 64 years.• Overuse injury may occur in the pronator teres, flexor carpi radialis,
palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris. • Associated with activities requiring wrist flexion/pronation, particularly
when there is a valgus strain at the elbow.

Diagnostic Approach
A diagnosis of lateral and medial epicondylitis can be made with a comprehensive history and physical exam.
General findings on clinical evaluation
Pain at either the lateral or medial aspect of the elbow is the main complaint. Patients will report pain during or following elbow flexion and extension.
Typically all patients describe a history of repetitive recreational or occupational activity. These activities exacerbate their pain. Other risk factors strongly associated with the development of epicondylitis may be present and include:
•Age 40 to 60 years
•Past medical history of epicondylitis
•Inadequate physical conditioning for the activities they are undertaking
•Poor mechanics during a repeated activity
•Smoking.
Grip strength may be decreased in either medial or lateral epicondylitis, without pain associated with this function. Additionally, grip strength can be diminished without a change in the typical epicondylitis pain. Therefore, measurement of grip strength may be used as an objective tool to assess recovery. Although a rare finding, if symptoms are severe the patient's elbow may have mild swelling. Checking for Tinel sign is recommended. This is performed by tapping lightly on the medial elbow over the ulnar nerve. It is described as positive if testing generates paresthesia without pain. A negative Tinel sign can help rule out cubital tunnel or other neurologic conditions.

Lateral Epicondylitis
Specific findings in lateral epicondylitis
Lateral epicondylitis is characterized by:•Tenderness over the common extensor tendon typically localized to the extensor carpi radialis brevis; maximal tenderness occurs approximately 2 to 5 cm distal and anterior to the midpoint of the lateral epicondyle •Normal sensation•Complete range of motion at the elbow and wrist, but possibly a weak wrist extension secondary to pain •Pain during resisted wrist and digit extension, and during passive wrist flexion with the elbow extended•Positive extensor carpi radialis brevis stretch test: reproducible pain over the origin of the common extensor mass when the arm is placed in extension while the examiner maximally flexes the wrist.

Medial Epicondylitis
Specific findings in medial epicondylitis
In medial epicondylitis:•The pain may have a more insidious onset •Tenderness is present distal and lateral to the medial epicondyle, over the pronator teres and flexor carpi radialis•Pain may radiate along the medial elbow and be increased with resisted forearm pronation or wrist flexion •Patients will also have normal sensation and strength, and complete range of motion.

Treatment
Rest, Ice, NSAIDS, brace
Steroid injections

Achilles Contracture
Shortening of the achilles tendon that causes foot pain and limits ankle dorsiflexionWomen who wear high heeled shoesJoggers who land on balls of feet and not heels

Signs and Symptoms
Sharp spasmodic pain during dorsiflexion
Treat conservatively: Gradually lower the heels of the patient if that is the etiology.
Surgery is last resort

Carpal Tunnel
Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist.




epidemiology
Affects an estimated 3 percent of adult Americans
Three times more common in women than in men
High prevalence rates have been reported in persons who perform certain repetitive wrist motions (frequent computer users)
• 30% hand paresthesias
• 10% clinical criteria for carpal tunnel syndrome
3.5% abnormal nerve conduction studies


Clinical Features
Pain
Numbness
Tingling
Symptoms are usually worse at night and can awaken patients from sleep.
To relieve the symptoms, patients often “flick” their wrist as if shaking down a thermometer (flick sign).


Clinical Features
Pain and paresthesias may radiate to the forearm, elbow, and shoulder.
Decreased grip strength may result in loss of dexterity, and thenar muscle atrophy may develop if the syndrome is severe.

Atrophy

Physical examination
Phalen’s maneuver
Tinel’s sign
weak thumb abduction.
two-point discrimination

Phalen’s maneuver

Tinel’s sign

Diagnostic
History
Physical examination
Nerve Conduction Study

Differential Diagnostics
Tendonitis
Tenosynovitis
Diabetic neuropathy
Compression of the Median nerve at the elbow

Treatment
CONSERVATIVE TREATMENTS
GENERAL MEASURES
WRIST SPLINTS
ORAL MEDICATIONS
LOCAL INJECTION
ULTRASOUND THERAPY
Predicting the Outcome of Conservative Treatment
SURGERY

GENERAL MEASURES
Avoid repetitive wrist and hand motions that may exacerbate symptoms or make symptom relief difficult to achieve.
Not use vibratory tools
Ergonomic measures to relieve symptoms depending on the motion that needs to be minimized


WRIST SPLINTS
Probably most effective when it is applied within three months of the onset of symptoms
Optimal splinting regimen ?

WRIST SPLINTS

ORAL MEDICATIONS
Diuretics
Nonsteroidal anti-inflammatory drugs (NSAIDs)
pyridoxine (vitamin B6)
Orally administered corticosteroids
Prednisolone
20 mg per day for two weeks
followed by 10 mg per day for two weeks
DO NOT WORK !!!

LOCAL INJECTION
A mixture of 10 to 20 mg of lidocaine (Xylocaine) without epinephrine and 20 to 40 mg of methylprednisolone acetate (Depo-Medrol) or similar corticosteroid preparation is injected with a 25-gauge needle at the distal wrist crease (or 1 cm proximal to it).

LOCAL INJECTION

LOCAL INJECTION

LOCAL INJECTION
Splinting is generally recommended after local corticosteroid injection.
If the first injection is successful, a repeat injection can be considered after a few months
Surgery should be considered if a patient needs more than two injections

ULTRASOUND THERAPY
•May be beneficial in the long term management •More studies are needed to confirm it’s usefulness


SURGERY
Should be considered in patients with symptoms that do not respond to conservative measures and in patients with severe nerve entrapment as evidenced by nerve conduction studies,thenar atrophy, or motor weakness.
It is important to note that surgery may be effective even if a patient has normal nerve conduction studies

SURGERY
Complications of surgery
Injury to the palmar cutaneous or recurrent motor branch of the median nerve
Hypertrophic scarring
laceration of the superficial palmar arch
tendon adhesion
Postoperative infection
Hematoma
• arterial injury
• stiffness



SURGERY

PREGNANCY
Alterations in fluid balance may predispose some pregnant women to develop carpal tunnel syndrome.
Symptoms are typically bilateral and first noted during the third trimester.
Conservative measures are appropriate, because symptoms resolve after delivery in most women with pregnancy-related carpal tunnel syndrome.

ConclusionMost common focal peripheral neuropathy
Pain and paresthesias in the distribution of the median nerve are the classic symptoms.
While Tinel’s sign and a positive Phalen’s maneuver are classic clinical signs of the syndrome, hypalgesia and weak thumb abduction are more predictive of abnormal nerve conduction studies.

Conclusion
Conservative treatment options include splinting the wrist in a neutral position and ultrasound therapy
Orally administered corticosteroids can be effective for short-term management (two to four weeks), but local corticosteroid injections may improve symptoms for a longer period.
If symptoms are refractory to conservative measures or if nerve conduction studies show severe entrapment, open or endoscopic carpal tunnel release may be necessary.

Torticollis - Basics
Neck deformity that involves shortening of the sternocleidomastoid (SCM) muscle resulting in limited neck rotation and lateral flexion.
Infants tilt their head toward the side of the shortened muscle and rotate to the contralateral side.
Plagiocephaly and craniofacial deformities can be associated with congenital muscular torticollis (CMT) and can perpetuate one another.
Developmental hip dysplasia can be associated with CMT.
It is important to rule out nonmuscular causes such as ocular, vertebral, and neurologic.
Treatment includes caregiver education on positioning and physical therapy; botulinum toxin type A injections, or surgery are reserved for recalcitrant cases.

Torticollis
Congenital muscular torticollis (CMT) is a neck deformity that involves shortening of the sternocleidomastoid (SCM) muscle resulting in limited neck rotation and lateral flexion. This results in a head tilt to the affected side and rotation to the contralateral side.

Rhabdomyolysis
Definition
Rhabdomyolysis may result from any traumatic or medical injury to the sarcolemma (the myocyte cell membrane). The subsequent release of intracellular ions, myoglobin, CK, and urates into the circulation results in electrolyte disturbances, disseminated intravascular coagulation (DIC), renal failure, and multiorgan failure. The measurement of serum CK levels at 5 times the upper limit of normal is used as diagnostic criterion.

Rhabdo
Etiology
Rhabdomyolysis is a consequence of different disease entities that cause myonecrosis. These processes may be classified as traumatic or medically induced. Trauma, including overexertional states, results in direct muscle injury. There are various medical causes. Rare, inherited muscle enzyme defect disorders, as well as seizures, infections, metabolic abnormalities, hypoxic conditions, temperature-related entities, and certain immunologic diseases, may result in rhabdomyolysis.

Rhabdo
Numerous prescribed and abused drugs may lead to rhabdomyolysis:
• Cocaine, amphetamines, and phencyclidine may cause hyperdynamic muscular states
• Narcotics and other central nervous system depressants (barbiturates, sedative-hypnotics) may cause tissue hypoperfusion and prolonged immobilization and limb compression
• Salicylate toxicity uncouples oxidative phosphorylation, which inhibits ATP formation
• Diuretics may lead to potassium depletion severe enough to result in rhabdomyolysis
• Statin therapy for cholesterol control has a significant unwanted effect of rhabdomyolysis. The mechanism is not clearly defined.

Rhabdo
Toxins, such as cyanide, mercury, copper, carbon monoxide, and toluene, disrupt ATP use or production at the cellular level and subsequently cause muscle damage.
Envenomation is a form of toxin-induced rhabdomyolysis. It has been documented in bee stings, centipede bites, and snakebites.
In essence, any condition that causes intrinsic or extrinsic damage to myocytes results in release of intracellular contents into the vascular compartment and the ensuing complications. A small proportion of cases are classified as idiopathic. These, however, are thought to be from as yet unrecognized hereditary defects or earlier undiagnosed metabolic causes.

Rhabdo
The diagnosis of rhabdomyolysis is based on presenting complaints and a high index of suspicion if risk factors are present. Obvious presentations include trauma victims with an extremity crush injury or a physically unconditioned person who presents with limb pain after jogging or weightlifting. Patients with medical causes of rhabdomyolysis may present much more insidiously. Complaints may be nonspecific such as generalized malaise or dark urine.
Examination is usually unremarkable, but muscle tenderness may be present and signs of compartment syndrome (cool extremity with diminished circulation) should be looked for in all cases of limb trauma and cases of prolonged limb immobilization.