Embed Size (px)
DESCRIPTION
WEBS01 Drug Resistance: A Bridge from Basic to Operations Research . Pathogenesis of HIV Resistance: current knowledge and new methodologies Francesca Ceccherini Silberstein Cattedra di Virologia Università di Roma Tor Vergata. - PowerPoint PPT Presentation
Citation preview

www.ias2011.org
WEBS01 Drug Resistance: A Bridge from Basic to Operations Research
Pathogenesis of HIV Resistance: current knowledge and new methodologies
Francesca Ceccherini SilbersteinCattedra di Virologia
Università di Roma Tor Vergata

www.ias2011.org
The emergence of resistance is the inevitable consequence of incomplete suppression of HIV replication by the current antiretroviral drugs, and is a frequent and major limitation of antiviral therapy.

www.ias2011.org
A total of 207 deaths were identified among 1,138 participants over the followup period, with an all cause mortality rate of 18.2%. Among the 679 patients with HIV-drug resistance genotyping done before initiating HAART, HIV-drug resistance to any class was observed in 7.8% of the patients. During follow-up, HIV-drug resistance to any class was observed in 302 (26.5%) participants. Emergence of any resistance was associated with mortality (hazard ratio: 1.75 [95% CI: 1.27, 2.43]). When considered each class of resistance separately, persons who exhibited resistance to non-nucleoside reverse transcriptase inhibitors had the highest risk: mortality rates were 3.02 times higher (95% CI: 1.99, 4.57) for these patients than for those who did not exhibit this type of resistance.

www.ias2011.org
Similarly…..
Logistic regression Multivariate P
CD4 time-dependent(per 50 cells increase)
0.79 (0.66-0.93) 0.006
Plasma HIV-RNA time-dependent(per 1 log10 increase)
1.14 (0.76-1.71) 0.539
Previous AIDS 2.29 (0.86-6.12) 0.098
LPV after GRT 0.57 (0.19-1.67) 0.302
3 drug class multi-resistance (DCMR) 12.29 (3.00-50.28) <0.001
Poor survival in drug-class multi-resistance
Days from GRT
16001400120010008006004002000
Cum
ulat
ive
prop
ortio
n su
rviv
ing
1,0
,9
,8
,7
,6
,5
,4
3 DCMR
2 DCMR
1 DCMR
0 DCMR
P at log-rank <0.001
Zaccarelli,et al., AIDS 2005

www.ias2011.org
Zaccarelli,et al., AIDS 2007
Poor survival in drug-class multi-resistance
And…..
www.ias2011.orgKozal,et al., HIV Clin Trials 2007
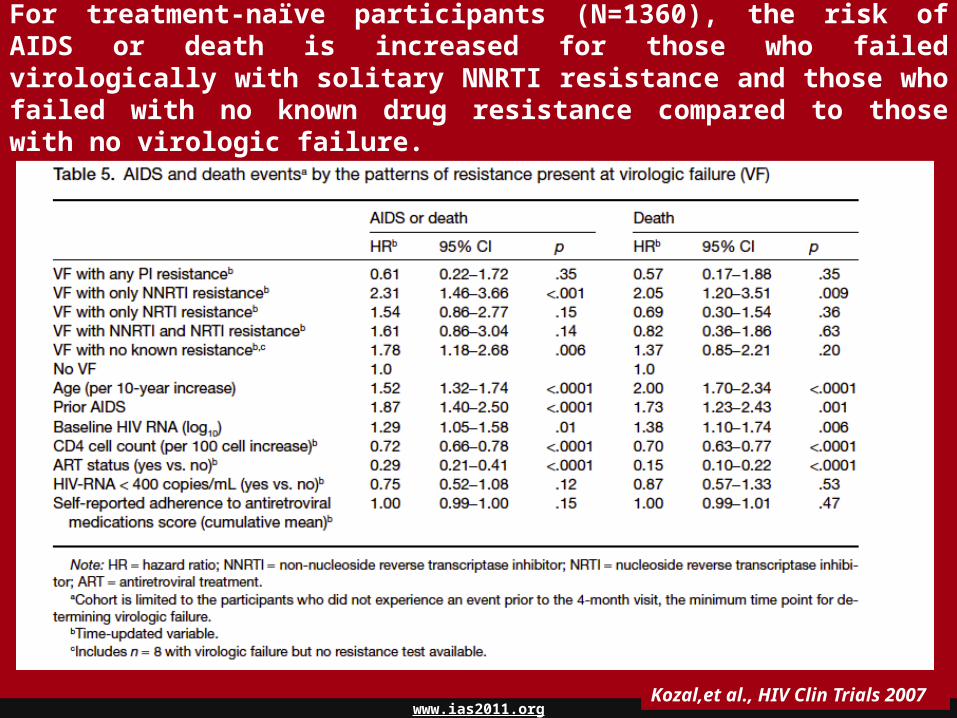
And…..For treatment-naïve participants (N=1360), the risk of AIDS or death is increased for those who failed virologically with solitary NNRTI resistance and those who failed with no known drug resistance compared to those with no virologic failure.

www.ias2011.org
And…..
2007

www.ias2011.org
June 2011

www.ias2011.org
In 1989 ….
4 RT mutations were associated
with drug-resistance

www.ias2011.org
IAS Dec 2010
Today more than 100 mutations…
Johnson VA, et al. Top HIV Medicine 2010

www.ias2011.org
2006 IAS
2010 IAS and Novel
L K L D V L M M I G I F I L A G V V I N L10 20 24 30 32 33 36 46 47 48 50 53 54 63 71 73 77 82 84 88 90F R I N I F I I V V L L L P V S I A V S MI M L V V T A T DR M FV S
2002 IAS
T W R L V T I K I G Q K A L L D V L E E M N R K K M I G I G F I K R Q D Q I L I I C H K A I G T V L V P V N I I N L L T Q I C L4 6 8 10 11 12 13 14 15 16 18 20 22 23 24 30 32 33 34 35 36 37 41 43 45 46 47 48 50 52 53 54 55 57 58 60 61 62 63 64 66 67 69 70 71 72 73 74 75 76 77 79 82 83 84 85 88 89 90 91 92 93 95 97P R Q F I I V R A E ins R V I I N I I Q G I D K T I I V V L S L L R K E E D V P L F F K E V T C P I V I A A D V V S V M S K L F V
I A V A M ins V F K D L T R L A M V Y V N H Q M N R I R S A T T L D I I R MR K X I V V V V L M Y V Y T M T S F G MV V T Q L V A I TC T A X L S
S LCG
L V I G K L D V L E E M K M I G I F I Q D I L I H A G T L V V N I I N L L I10 11 13 16 20 24 30 32 33 34 35 36 43 46 47 48 50 53 54 58 60 62 63 64 69 71 73 74 76 77 82 83 84 85 88 89 90 93F I V E R I N I I Q G I T I V V L L L E E V P L K V C P V I A D V V S V M LI M F L L A M V Y V M I S T D MR I V V M V T T FV V T L A SC T A I
S L
During the years, with the increasing number of new PIs, the number of PR mutations associated with PI-resistance is highly increased.
Knowledge of HIV-1 resistance is continuously evolving
Evolution of HIV-1 resistance profiles follows improvements in regimens’
settings

www.ias2011.org
• More targets
Improved genotypic drug resistance testing
Update from Ceccherini Silberstein, et al. Clin Microbiol Infect. 2010
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 20100
500
1000
1500
2000
2500
3000
138360
539738
906
13371499
1665 1560 1476
1868
2622
gp41 Integrase V3 Pol (PR/RT) Overall
Gen
otyp
ing
resi
stan
ce te
sts,
N

www.ias2011.org
Testing for minority resistant variants
Paredes and Clotet, Eur Infect Dis 2008
• More sensitive approaches• New technologies

www.ias2011.org
• Due to the intrinsic characteristics of HIV, the selection of the first therapeutic regimen is crucial for the success of the following regimens
Remember…..

www.ias2011.org
Virological factors to be considered for a correct approach to first line therapies
Limit as much as possible the use of drugs against whom the virus has already selected primary mutations

www.ias2011.org
Transmitted drug resistance• Studies report prevalence of drug resistance in ARV-naïve patients
in USA and Europe:– 5 to 15% in newly diagnosed persons– 10 to 25% in acutely infected persons
• Persistence of transmitted resistant virus (median follow-up 2.1 years)– NNRTI resistance in 10/14 patients– Resistant virus persistently detectable in 13/14 patients– Mean time to first detectable wt/resistant mixture was 103 weeks (95% CI: 49–
216)• Response to therapy in patients with transmitted resistance
– NNRTI (n=67), PI (n=18), NRTI (n=25): some with MDR virus– 45% (38/84) failed to suppress, best response in those receiving >2 active
drugs (p=0.01)
Little S, et al. 14th CROI, Los Angeles 2007, #60

www.ias2011.org
Time to first virologic failure in the subcohort was substantially shorter for subjects with preexisting NNRTI-resistant virus than
for those without
Weighted Cox proportional hazard models including baseline NNRTI resistance showed a significantly increased risk of virologic failure for subjects with NNRTI-resistant virus at baseline compared with those without (intent-to-treat: HR, 2.27 [95% CI, 1.15–4.49]; P .018) (as-treated: HR, 2.61 [95% CI, 1.30 –5.20]; P .007)
Kuritzkes et al JID 2008

www.ias2011.org

www.ias2011.org
VF rates at M12 were 6.0% (95% confidence interval [CI]: 5.5; 6.5), 6.3% (4.2; 9.3) and 16.2% (13.0; 20.1) for no TDR group, TDR and fully active group and TDR and resistant group, respectively.
Wittkop et al Lancet 2011
TDR was associated with a poorer virological response when patients received cART containing ≥1 drug not fully active

www.ias2011.org
Wittkop et al Lancet 2011
TDR was associated with a poorer virological response when patients received cART containing ≥1 drug not fully active

www.ias2011.org
Wittkop et al Lancet 2011
When an active regimen was used with TDR, the use of a 2NRTI/NNRTI combination was associated with a higher risk for VF, possibly due to the presence of minority resistant species.

www.ias2011.org
Treatment begins
Vira
l loa
d
Time
Selection of resistant quasispecies
Incomplete suppression First-line monotherapy No Adherence Bioavailability Pre-existing resistance Reservoir
Drug-susceptible quasispeciesDrug-resistant quasispecies
Improved detection methods for HIV drug-resistance
Today it is possible to detect resistant quasispecies before the treatment starting. It could be important to detect as soon as possible before starting treatment

www.ias2011.org

www.ias2011.org

www.ias2011.org
www.ias2011.org
While these recently developed methodologies point to the exciting potential for a new quantum of ability in the detection of ARV drug resistance, much work remains to be done to assess the clinical relevance of these “minority” variants…

www.ias2011.org Johnson et al Plos Med 2008
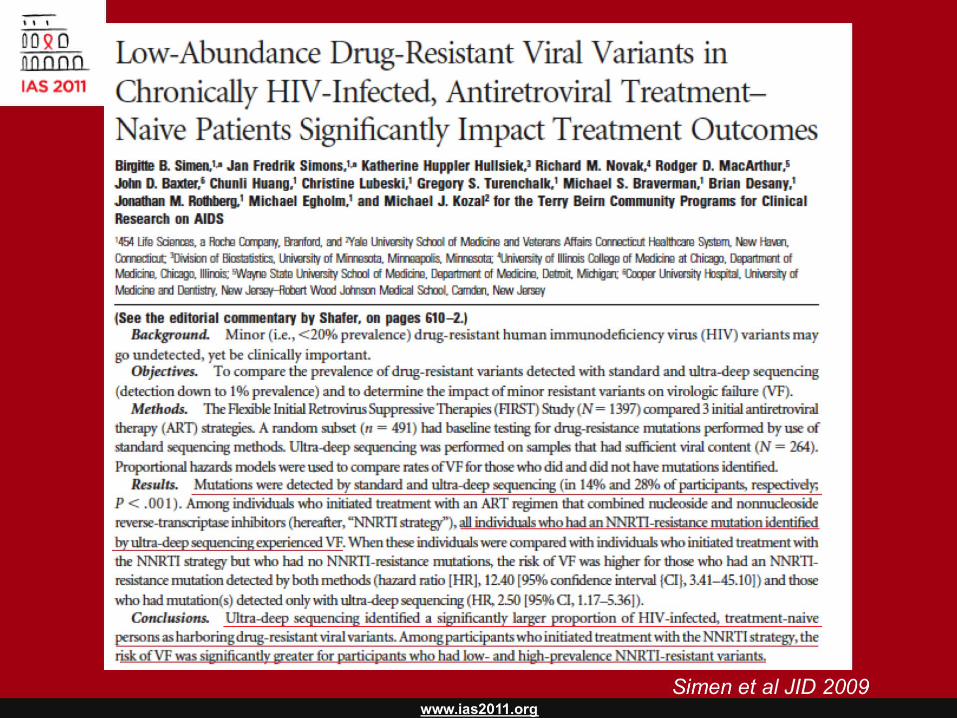
www.ias2011.orgSimen et al JID 2009

www.ias2011.org
Paredes et al., The Journal of Infectious Diseases 2010; 201:662–671
Halvas et al., The Journal of Infectious Diseases 2010; 201:672–680
www.ias2011.org
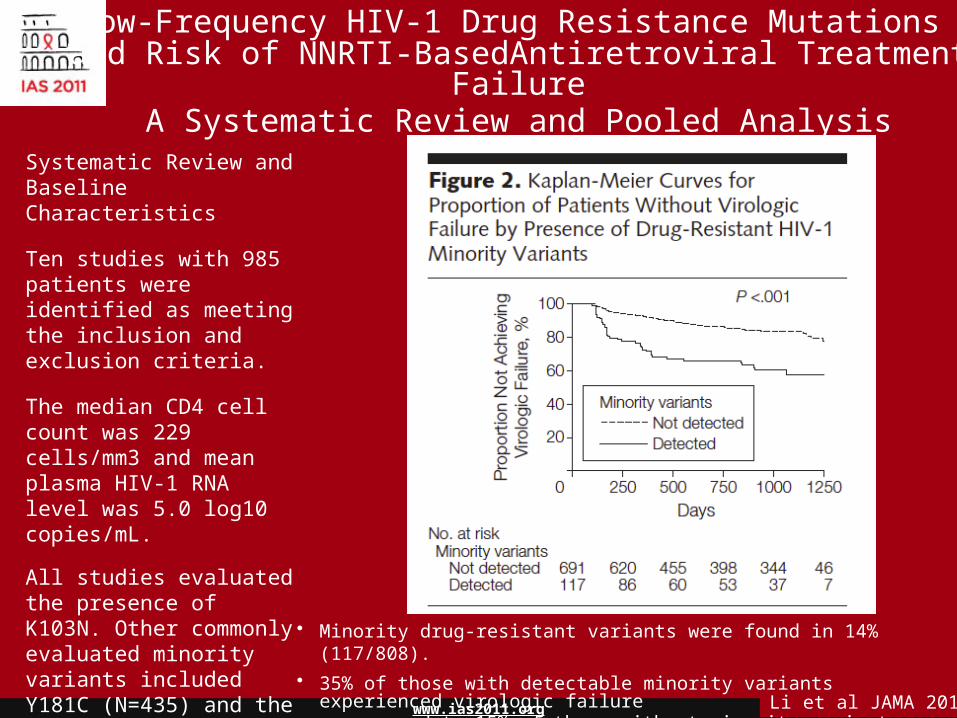
Low-Frequency HIV-1 Drug Resistance Mutations and Risk of NNRTI-BasedAntiretroviral Treatment Failure
A Systematic Review and Pooled Analysis
Systematic Review and Baseline Characteristics
Ten studies with 985 patients were identified as meeting the inclusion and exclusion criteria.
The median CD4 cell count was 229 cells/mm3 and mean plasma HIV-1 RNA level was 5.0 log10 copies/mL.
All studies evaluated the presence of K103N. Other commonly evaluated minority variants included Y181C (N=435) and the NRTI mutations M184V (N=228) and K65R (N=163).
Li et al JAMA 2011
• Minority drug-resistant variants were found in 14% (117/808).• 35% of those with detectable minority variants experienced virologic failure as compared to 15% of those without minority variants.

www.ias2011.org Li et al JAMA 2011
Presence of minority variants at ≥1% conferred a significantly higher risk of virologic failure as compared to minority
variants present at ≤1%.
A dose-dependent effect on the risk of virologic failure was found when subjects were categorized by the absolute copy
numbers of minority variants per mL of plasma.

www.ias2011.org Li et al JAMA 2011
The detection of minority variants was associated with an increased risk of virologic failure at either high or low
levels of medication adherence
www.ias2011.org
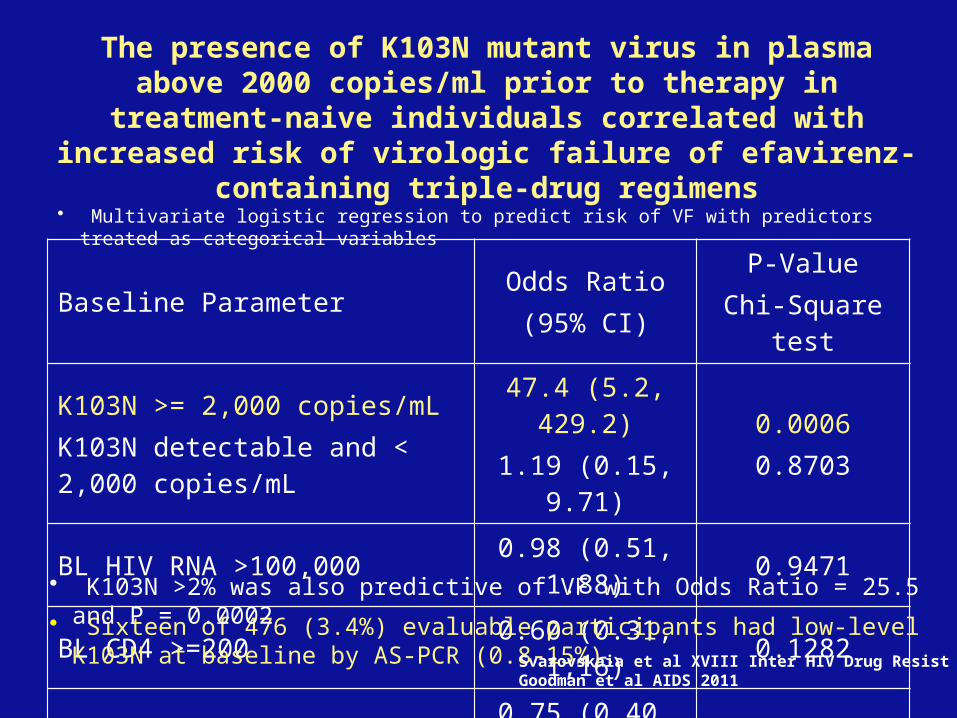
Baseline ParameterOdds Ratio(95% CI)
P-ValueChi-Square test
K103N >= 2,000 copies/mLK103N detectable and < 2,000 copies/mL
47.4 (5.2, 429.2)1.19 (0.15, 9.71)
0.00060.8703
BL HIV RNA >100,000 0.98 (0.51, 1.88) 0.9471
BL CD4 >=200 0.60 (0.31, 1,16) 0.1282
Treatment arm 0.75 (0.40, 1.41) 0.3695
• Multivariate logistic regression to predict risk of VF with predictors treated as categorical variables
• Sixteen of 476 (3.4%) evaluable participants had low-level K103N at baseline by AS-PCR (0.8-15%).
• K103N >2% was also predictive of VF with Odds Ratio = 25.5 and P = 0.0002
Svarovskaia et al XVIII Inter HIV Drug Resist 2009Goodman et al AIDS 2011
The presence of K103N mutant virus in plasma above 2000 copies/ml prior to therapy in treatment-naive individuals
correlated with increased risk of virologic failure of efavirenz-containing triple-drug regimens

www.ias2011.org
Mean virological response of patients Receiving 300mg BID Maraviroc in study 1029
Swenson et al, CROI 2009, Abstract 680 % X4 using PSSM -6.95 cut-off
Change in viral
load10-30% X4>30% X4
<10% X4

www.ias2011.org
Summary• HIV drug-resistance is both a major consequence and cause of
HIV treatment failure.

www.ias2011.org
Summary• HIV drug-resistance is both a major consequence and cause of
HIV treatment failure.• Drug resistance (NNRTI and 3-class) is associated with HIV
disease progression and death.

www.ias2011.org
Summary• HIV drug-resistance is both a major consequence and cause of
HIV treatment failure.• Drug resistance (NNRTI and 3-class) is associated with HIV
disease progression and death.• Transmitted drug resistance is associated with a poorer virological
response, particularly for NNRTI mutations.

www.ias2011.org
Summary• HIV drug-resistance is both a major consequence and cause of
HIV treatment failure.• Drug resistance (NNRTI and 3-class) is associated with HIV
disease progression and death.• Transmitted drug resistance is associated with a poorer virological
response, particularly for NNRTI mutations.
• The presence of minority HIV-1 drug-resistance mutations is associated with more than a two times the risk of virologic failure in patients receiving an initial NNRTI-based ART regimen.

www.ias2011.org
Summary• HIV drug-resistance is both a major consequence and cause of
HIV treatment failure.• Drug resistance (NNRTI and 3-class) is associated with HIV
disease progression and death.• Transmitted drug resistance is associated with a poorer virological
response, particularly for NNRTI mutations.
• The presence of minority HIV-1 drug-resistance mutations is associated with more than a two times the risk of virologic failure in patients receiving an initial NNRTI-based ART regimen.
• The association with virologic failure was most prominent for NNRTI-resistance mutations and was dose-dependent:
- ≥1% conferred a significantly higher risk of virologic failure as compared to minority variants present at ≤1%.
- when subjects were categorized by the absolute copy numbers of minority variants per
mL of plasma (>1000/>2000 copies/ml).

www.ias2011.org
• The upcoming routine availability of new and exciting technologies, such as the deep sequencing, may let scientists and clinician improve the tailoring of therapy to each single patient, by selecting those drugs and strategies able to hit at best the virus of each particular patient.
• Quantity, rather than just presence, of minority resistant (or X4) quasispecies, plays a game in regulating the efficacy of NNRTI-based first line therapies (or CCR5 antagonists).
Conclusions
www.ias2011.org
A. Antinori P. NarcisoC. Gori R. d’Arrigo F. ForbiciM.P. TrottaA. AmmassariR. BellagambaM. ZaccarelliG. LiuzziV. TozziP. SetteN. PetrosilloF. AntonucciE. BoumisE. NicastriU. ViscoP. De LongisG. D’OffiziM.R. CapobianchiI. AbbateG. RozeraA. BrusellesB. BartoliniG. Ippolito
INMI “L. Spallanzani”
C. MussiniV. BorghiL. Sighinolfi
Modena and Ferrara Infectious Diseases Center
G. RizzardiniV. MicheliA. CapettiP. MeravigliaM. Moroni
L. Sacco University Hospital
- The I.CO.N.A. Study Group A. d’Arminio Monforte
ACKNOWLEDGEMENTSUniversity of Rome “Tor
Vergata”C.F. PernoV. SvicherM.M. SantoroA. BertoliD. ArmeniaS. DimonteV. CentoC. AlteriL. FabeniR. CammarotaR. SalpiniF. StaziF. MercurioM. Andreoni
Max Planck Institute of SaarbruckenT. SingN. BeerenwinkelT. Lengauer
University of CatanzaroS. AlcaroA. Artese
Catholic University of Rome, Sacro CuoreA. De LucaR. Cauda
Infectious Diseases Unit FlorenceS. Lo CaputoF. Mazzotta
San Gallicano HospitalG. PalamaraM. Giuliani
University of TurinG. Di PerriS. BonoraV. Ghisetti
European Project CHAIN, No. 223131
Hôpital Pitié-Salpetrière, Paris, FranceV. Calvez A.G. MarcelinI. MaletP. Flandre
San Martino Hospital, GenoaB. BruzzoneA. Di Biagio
ISS RomeM. CiccozziG. RezzaS. Vella
K. Van Baelen, I. VandenbrouckeH. Van Marck, V. Van EygenM. Van Houtte, L. Stuyver, M. Tuohy
Virco BVBA
Resistance StudyGroup
Thank you for your attention !
CHU de Bordeaux, FranceB. Masquelier




















![Highway Bridge Loads and Load Distributionfreeit.free.fr/Bridge Engineering HandBook/ch06.pdf · Load and Resistance Factor Design (LRFD) Specifications [1]. Stream flow, ice loads,](https://img.dokumen.tips/doc/110x75/5a7013757f8b9a9d538b9e27/highway-bridge-loads-and-load-distributionfreeitfreefrbridge-engineering-handbookch06pdfpdf.jpg)








