Embed Size (px)
Citation preview
Webinar SURGICAL OBJECT SURVEILLANCE
Kyung Jun, RN, MSN, CNOR
January 22, 2014

• Please vote for best title regarding
preventing retained surgical item
– “SOS”: Surgical Object Surveillances?
– “What Goes In Must Come Out”?
– “Seek and Sweep”?
– FOFO: Free of Foreign Object?
TITLE

• Share our journey of what has worked and
what has not…
• Provide opportunity to network with other
hospitals on this issue
• Allow time for feedback and questions
OBJECTIVES

• 950 beds
• Teaching hospital with both faculty and
private physicians
• Over 43 operating rooms on 8 separate
locations
• Over 30,000 surgeries per year
OUR JOURNEY

Increased Risk
Emergency surgeries
Unplanned changes in procedure (e.g. intraoperative hemorrhage, code blue)
Increased body-mass index
Multiple surgical specialties
Multiple nursing staff hand-offs
Intervention Anticipate cases with high probability of RFO
Call out packed items and write on the board
Surgeon to surgeon report
RN to RN report using SBAR
Sweep or Peep (visual/manual inspection of site) prior to closure
X-ray
For incorrect count or missing item
Inform radiologist: item in question, operative area, drains, and lines
Radiologist must speak to the Surgeon to convey the result
Do not close skin until x-ray is negative
Surgery end time is defined as “last stitch in”
Adapted from Gawande, Risk factors for retained instruments and sponges after surgery. N Engl J Med. 2009; 35 (3): 229-35
EARLY ON

• In 2008, had a peak in RSI
• Initiated RFO Oversight Committee
• Importance of Oversight Committee
– Multidiscipline
– Physician & nurse involvement
– PI facilitator keep project on tract
– Aimed to achieve goal within 12-18 months
HISTORY
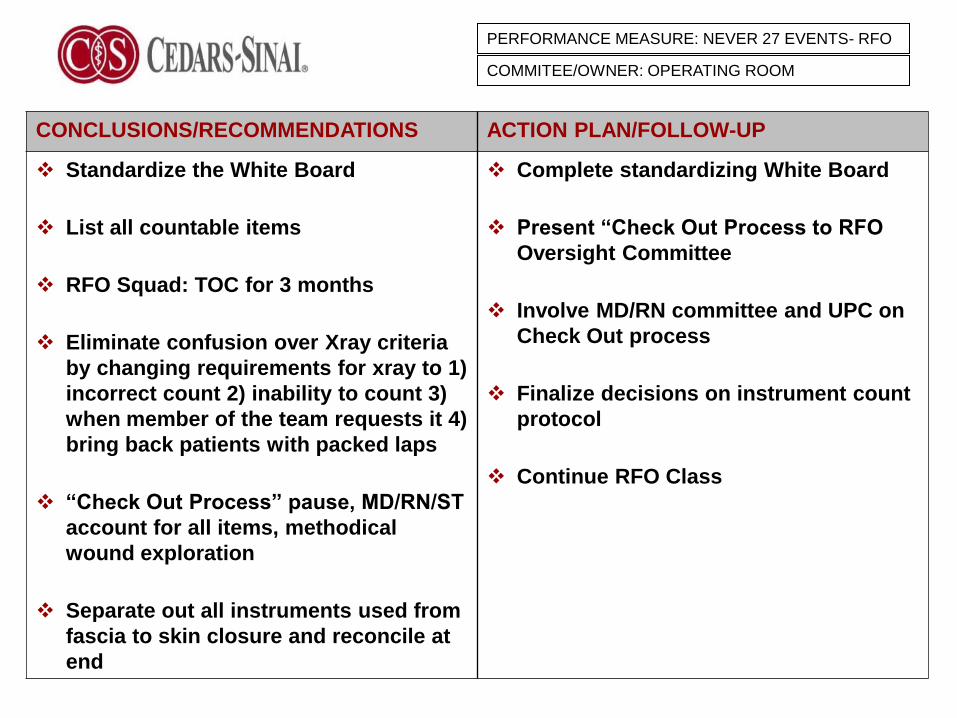
CONCLUSIONS/RECOMMENDATIONS ACTION PLAN/FOLLOW-UP
Standardize the White Board
List all countable items
RFO Squad: TOC for 3 months
Eliminate confusion over Xray criteria
by changing requirements for xray to 1)
incorrect count 2) inability to count 3)
when member of the team requests it 4)
bring back patients with packed laps
“Check Out Process” pause, MD/RN/ST
account for all items, methodical
wound exploration
Separate out all instruments used from
fascia to skin closure and reconcile at
end
Complete standardizing White Board
Present “Check Out Process to RFO
Oversight Committee
Involve MD/RN committee and UPC on
Check Out process
Finalize decisions on instrument count
protocol
Continue RFO Class
PERFORMANCE MEASURE: NEVER 27 EVENTS- RFO
COMMITEE/OWNER: OPERATING ROOM

0
1
2#
o
f R
FO
s
Sep-08 Oct-08 Nov-08 Dec-08 Jan-09 Feb-09
Never 27
Events
(RFO)Target 0
PERFORMANCE MEASURE: NEVER 27 EVENTS- RFO
COMMITEE/OWNER: OPERATING ROOM
RFO
Oversight
CTE
OR RFO CTE

TASK FORCE STRUCTURE
Clinical Improvement Committee
RFO Taskforce Oversight Committee
(Meets Monthly)
RFO Prevention in
the O.R.
Team Leaders:
OB, MD,
Surgery, MD,
OR, RN
RFO Prevention in
other Procedural
Areas
Team Leaders:
ED, MD
Medicine, MD
Med-Surg. Adm., RN
New Technology to
Prevent RFO
Team Leaders:
Surgery, MD
Clinical Engineering
Education &
Communication
Team Leaders:
OB, MD
Nursing Adm. PhD
Nursing Ed.
RFO Integration Team
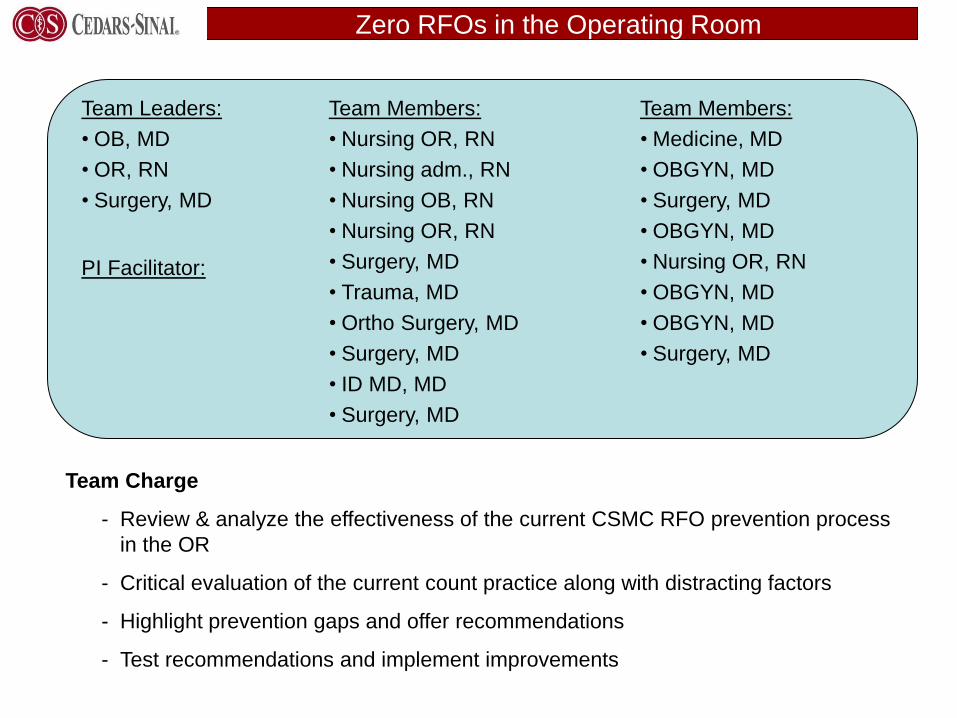
Zero RFOs in the Operating Room
Team Leaders:
• OB, MD
• OR, RN
• Surgery, MD
Team Members:
• Nursing OR, RN
• Nursing adm., RN
• Nursing OB, RN
• Nursing OR, RN
• Surgery, MD
• Trauma, MD
• Ortho Surgery, MD
• Surgery, MD
• ID MD, MD
• Surgery, MD
Team Charge
- Review & analyze the effectiveness of the current CSMC RFO prevention process
in the OR
- Critical evaluation of the current count practice along with distracting factors
- Highlight prevention gaps and offer recommendations
- Test recommendations and implement improvements
PI Facilitator:
Team Members:
• Medicine, MD
• OBGYN, MD
• Surgery, MD
• OBGYN, MD
• Nursing OR, RN
• OBGYN, MD
• OBGYN, MD
• Surgery, MD

• 12 questions to test staff, surgeons, and
anesthesiologists knowledge about the count
process, when to take an x-ray and to get input
on what we need to change
• Survey sent to OR nurses, techs, surgeons,
OBGYN, anesthesiologists, interventionalists
SURVEY

• Most valuable questions asked were:
• What distractions interfere with the count? Rank 1-5 with
1 being the most distracting
– Multitasking
– Music
– Computer entry
– Too many people in the room
– other
• If you had one suggestion to reduce the risk of retained
foreign objects in the OR, what would it be?
SURVEY

Documentation Standardization
Whiteboard Standardization in the Operating Room
• Larger whiteboards installed
• First test: magnet standardization, magnets finalized on May 18
• Other considerations: add permanent lines, add permanent item locations
• Next steps: collect feedback from the staff and follow-up on best practices
from the Patient Room Whiteboard Standardization Project
BEFORE AFTER

Angiocath Cottonoid fred Iodoform gauze
Penrose drain Safety pins Sternal wires Umbilical tapes
Cottonballs House Mayfield pins Q-tips
shoestring Bulldog reels CiP
Fish hooks Pacing wires Rubber band Alcohol wipes
ENT gauze Hypo needles Stapler
cartridge
Vessel loop
Mayfield pins Suction tips Suture boots Weck cell
Shoe strings Throat packs shods Vag packs
Bovie scratch Instrument
caps
Peanuts seprafilm
Surgical Items

• In-service for every one
• Small groups
• “RFO Prevention Month” in October
• Audits
EDUCATION

• Survey the room: remove labels, remove opened sutures, clear whiteboard, check kick bucket and sharps container
• Count instruments/ sponges/ needles BEFORE pt enters
• Use standardized board (needles, micro-needle) no exception
PRIOR TO SURGERY

• Count from surgical field (pick up laps, open
them), mayo stand, back table, to sponge
counter bag
• Circulating RN calls out items to be counted
• Pick up laps, open them, insert into bag
with radiopaque string visible
• Create distraction free environment during
counts- stop the music, etc..
COUNTING PROCESS
• Keep tally of needles and sponges throughout case
• NO ST and RN should break at the same time
• Only primary circulator gives countable item
• Use Sponge counter bags (5 laps with blue tag showing, 10 raytecs)
DURING SURGERY
• Must use for every case (no exception)
• Show blue radiopaque tags
• 5 laps; 10 raytecs
• “show me” Pass off all sponges and raytecs
to fill the sponge counter bags
• See it; touch it; open it; feel it
SPONGE COUNTER BAGS

“Show
Me” from
Dr Verna
Gibbs

• X-ray criteria
– Incorrect count
– After removal of packed sponges
– Inability to count for any reason
– When a member of surgical team requests it
X-RAY

• Avoid cutting cottonoids, tapes, and sponges
• Tapes, cottonoids are cut, all portions must be accounted for
• When cutting gauze, vag pack and molding cotton or others, have a count of 5’s
• Put this on the board
• When packing (throat, abdomen, chest, vagina) put this on the board
• Other methods (clamp on your gown)
PACKED ITEMS

• Count done by RN & ST for open cavity and
vaginal cases
• RN/ST count BEFORE the patient enters
room: nurse with protocol reads, ST counts
• Instrument count should be included in
the FINAL count
• Most commonly left item: sponge, needle,
clamps, retractors, malleable
INSTRUMENTS

• Surgeons busy operating
• Accounting was sole nursing responsibility
• Must have joint accountability through Check Out
– Methodical Wound Exam
– Count uninterrupted
– Closing suture
JOINT ACCOUNTABILITY

Defining Methodical Wound Examination
A methodical wound examination is necessary to prevent RFO
Minimum requirements for a methodical wound exam:
Space to be closed must be carefully examined
Special focus should be given to closure of a cavity within a cavity
(heart, major vessel, stomach, bladder, uterus, vagina)
Strive to see & touch – reliance on one element of sensory
perception is insufficient
Look and feel in the recesses of the wound and examine under
fatty protuberances and soft-tissues appendages
If the surgeon is informed of a missing object, while the OR staff
are looking for the surgical item, the surgeon should stop closing &
repeat the methodical wound exam
We need your help to define the methodical wound exam in your
discipline
Goal: define methodical wound exam for each discipline

Defining Methodical Wound Examination
Goal: define methodical wound exam for each discipline
Samples Abdomen and Pelvis
Definition should not be complicated. Definition must be easy to remember while in the OR.

Defining Methodical Wound Examination
Goal: define methodical wound exam for each discipline
Samples Mediastinum or Thorax
Definition should not be complicated. Definition must be easy to remember while in the OR.

PAUSE for the Check Out !
Process Start: Surgeon announces he / she is ready to close
Surgeon Nurse & Scrub Tech
• Perform methodical wound
examination
• Verbally attest to
completion of wound exam
• Close wound
• Perform sponge and sharps
accounting
• Verbally attest to completion of
sponge and sharps accounting
• Perform instrument accounting
Process End: Nurse documents completion of the Check Out process

• X-ray must be taken if broken inside patient
• Chain of command
• Midas: name of item, manufacturer, catalog
number, lot number, contact person for
company
BROKEN INSTRUMENTS
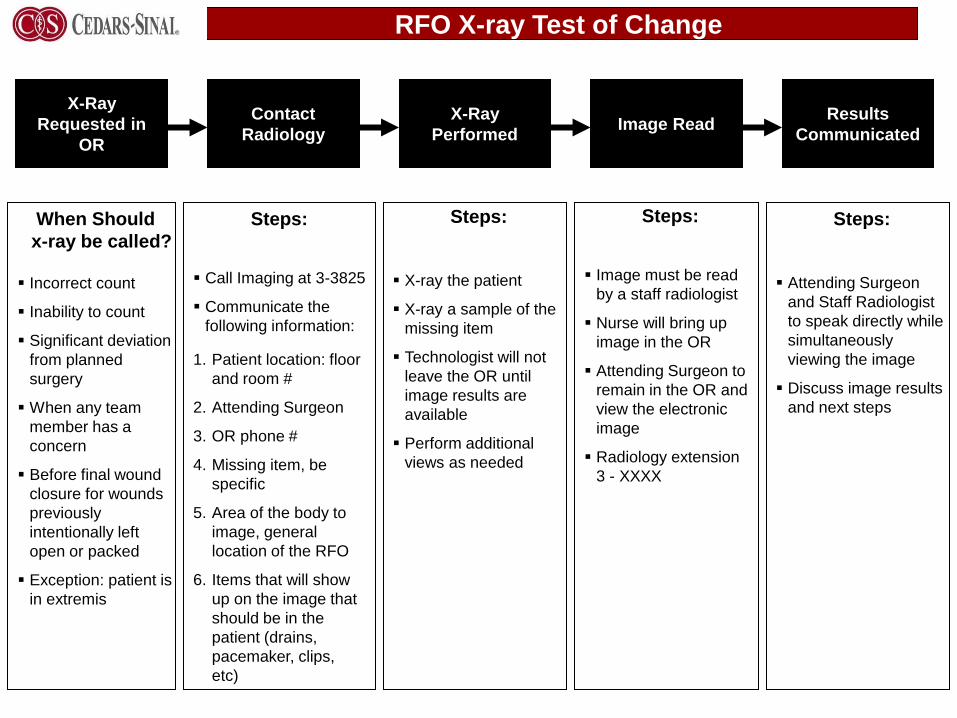
RFO X-ray Test of Change
X-Ray
Requested in
OR
Contact
Radiology
X-Ray
Performed Image Read
Results
Communicated
When Should
x-ray be called?
Incorrect count
Inability to count
Significant deviation
from planned
surgery
When any team
member has a
concern
Before final wound
closure for wounds
previously
intentionally left
open or packed
Exception: patient is
in extremis
Steps:
Call Imaging at 3-3825
Communicate the
following information:
Steps:
X-ray the patient
X-ray a sample of the
missing item
Technologist will not
leave the OR until
image results are
available
Perform additional
views as needed
Steps:
Image must be read
by a staff radiologist
Nurse will bring up
image in the OR
Attending Surgeon to
remain in the OR and
view the electronic
image
Radiology extension
3 - XXXX
Steps:
Attending Surgeon
and Staff Radiologist
to speak directly while
simultaneously
viewing the image
Discuss image results
and next steps
1. Patient location: floor
and room #
2. Attending Surgeon
3. OR phone #
4. Missing item, be
specific
5. Area of the body to
image, general
location of the RFO
6. Items that will show
up on the image that
should be in the
patient (drains,
pacemaker, clips,
etc)

RFO X-ray Process

• Criteria
• Inability to count for any reason
• When an item is unaccounted for
• After packed item is removed
• When anyone requests it
X-RAY

Technology Evaluation (2010)
Counts High Tech Option Status
Instruments X-ray • time consuming, dollar impact, not always a reliable
method of detection
Sponges Wand (RF Surgical) • Pilot to begin Jun 2
• 20 wands to be tested on 3 OR, 5 OR, 6OR
• Meeting on May 21st to determine needed supplies
Barcode (Surgicount) • Focus groups did not endorse this product
Wand + Bucket
(Clearcount)
• Question as to whether they can handle our size
Needles • No high-tech option available

Surgical Safety Checklist
Sign In Time Out Check out
Before induction of anesthesia Before skin incision Before wound closure
Patient has confirmed:
Site Marked / Not Applicable
Anesthesia Safety Checklist Completed
Pulse Oximeter on Patient & Functioning
No
Yes
No
Yes, and equipment / assistance available
No
Yes, and adequate intravenous access
and fluids planned
• Identity • Site • Procedure • Consent
Does Patient Have:
Known Allergy?
Difficult Airway / Aspiration Risk?
Risk of > 500ML Blood Loss?
Confirm all team members have
introduced themselves by name and role
Surgeon, Anesthesia Professional, and
Nurse Verbally Confirm:
• Patient • Site • Procedure
Anticipated Critical Events
Surgeon reviews: what are the critical or
unexpected steps, operative duration,
anticipated blood loss?
Anesthesiologist reviews: are there any
patient-specific concerns?
Nursing Team reviews: has sterility
(including indicator results) been
confirmed? Are there equipment issues or
any concerns?
Has antibiotic prophylaxis been given
within the last 60 minutes?
Yes
Not Applicable
Is essential imaging displayed?
Yes
Not Applicable
Name of the procedure recorded
Sponge and sharp counts are correct
How the specimen is labeled (including
patient name)
Whether there are any equipment
problems to be addressed
Surgeon, Anesthesiologist, and Nurse
review the key concerns for recovery and
management of this patient
Surgeon performs methodical wound exam
Visual inspection of sponge tree
Nurse verbally attests to completion of
sponge and sharp accounting
Surgeon begins wound closure
Sign out
Do you have a specific concerns to note
prior to the procedure?
Surgeon verbally attests to completion of
methodical wound exam
Nurse and Scrub Tech perform sponge
and sharp accounting
Nurse and Scrub Tech perform instrument
accounting
Instrument counts are correct
Nurse verbally
confirms:
Not Applicable (spine, hip case)
Yes

RFO PREVENTION AUDIT
Date: Date: Date
Unit/Rm: Unit/Rm: Unit/Rm
Physician : Physician: Physician:
Circulating RN Circulating RN Observed
MRN: MRN: MRN:
Audit #1 Audit #2 Audit #3
YES NO N/A COMMENTS YES NO N/A COMMENTS YES NO N/A COMMENTS
1. survey room: check sharp
container, pharm bin, kick
bucket, clear board, remove all
labels
3. keep sponge counter bags
up
4. The Check Out
Addressed the following:
a. Pause by all
b. Count by RN and ST
c. Methodical Wound
Exploration by MD
d. Attestation of count status by
RN
e. Attestation of MWE by MD
5. Include instrument count at
final count for open cavity and
vaginal case
6. Protocol sheet used for
instrument count
7. "Show Me"- fill all spaces in
sponge counter bags and show
MD

• Process of looking at “other” retained
items (guide-wires,
• Always audit everything
– Sponge counter bags
– Methodical Wound Exam
• Study trends of near misses
– When are we doing x-rays
– Hand offs
WHERE ARE WE NOW

DAYS WITHOUT
RETAINED SPONGE
797





























