Embed Size (px)
Citation preview

PTOC12
CHEST X-RAY INTERPRETATIONAimTo systematicaly and acurately examine a patients chest X-Ray to assist in the diagnosis and treatment of respiratory conditions.
Background
X-rays use electromagnetic energy beams to produce images of internal tissues, bones, and organs for diagnostic purposes. The X-rays pass through body tissues onto specially treated plates (similar to camera film) and a “negative” type digital picture is made, the more solid a structure is, the whiter it appears on the film.
Chest X-rays provide information regarding the size, shape, contour, and anatomic location of the heart, lungs, bronchi, great vessels (aorta, aortic arch, pulmonary arteries), mediastinum, and the bones (cervical and thoracic spine, clavicles, shoulder girdle, and ribs). Changes in the normal structure, position and appearance may indicate disease or other conditions.
Local variations will exist relating to which professions are able to request Chest X-Rays but regardless of practice physiotherapists in On Call situations need to be able to assess and interpret for both normal and abnormal findings as this will imapact on respiratory function and treatment plans.
1. To effectively assess Chest X-Rays physiotherapists require the necessary underpinning knowledge:
An expert knowledge of respiratory anatomy and physiology. An understanding of the indications for performing Chest X-rays and
potential contraindications and risks. Differences between departmental and portable films. The ability to use a System of Scrutiny (SOS) to assess for normal and
abnormal findings. An understanding of the common radiological signs associated with
respiratory pathology. An ability to rationalise findings to assist in formulation of treatment plans
and interventions. An awareness of need to document and report findings.
Indications
Evaluation of signs and symptoms potentially related to the respiratory, cardiovascular, upper gastrointestinal, and musculoskeletal systems of the thorax.
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
Follow-up of known thoracic disease processes to assess improvement,
resolution, or progression. Monitoring of patients with life-support devices and patients who have
undergone cardiac or thoracic surgery or other interventional procedures.
Contraindications
Do not image pregnant women in the area of the foetus due to radiation risk.
Ensure all investigations are necessary to minimise radiation exposure.
Difference between Department and Portable Chest X-Ray
2. Ascertain where the chest X-ray was undertaken and understand the differences between department and portable films. Remember the limitations of portable films but SICK WARD patients need portable films.
Department
• Posterior-Anterior approach (P.A.) • Comparable - always the same circumstances/erect/standard exposure.• Arms internally rotated so no scapulae shadows are visible within the lung
fields.
Portable
• Anterior-Posterior approach (A.P.) - Distance shorter/variable.• Heart and mediastinum are further from the plate therefore they appear
magnified relative to the rib cage.• Not comparable – different patient positions /different exposures.• Scapulae shadows are visible within the lung fields.
REMEMBER:-
The CXR is just part of the patient assessment. Describe using radiological terms not pathological. The CXR is a two dimensional picture of a three dimensional structure. A normal CXR does not rule out disease. Consider trends.
3. Perform Preliminary Checks:-
NameDate and timeProjectionTranslucency - too white = under exposed
- too dark = over exposed
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
SymmetryLines, drains, ETT etc.
4. Undertake a Systematic Examination of the Chest X-Ray (System of Scrutiny). Consider;
Bones ClaviclesAny fractures?Sternal ends equidistant from vertebral spinous process?ScapulaeAre the medial borders in the lung fields?RibsAre they all present i.e. thoracoplasty?Are there any fractures? number? location? flail segment?Do they have normal shape and slope?Do they appear of normal density i.e. osteoporosis?Number visible (9 - 10 ribs on full inspiration visible above diaphragm)
Lung FieldsTranslucencyCompare the two sides; any abnormal shadows? evidence of secretions?Lung markingsDensity (should increase in the lower zones)Do they extend to the periphery?Horizontal fissureVisible in 80% of adults.
DiaphragmCostophrenic and Cardiophrenic angles These should be acute and clear.If the diaphragm is abnormally low, as in asthma or emphysema, the costophrenic angles may be obliterated.The right hemi-diaphragm should be slightly higher than the left.Unilaterally raised when the phrenic nerve is paralysed or there is atelectasis or major collapse.Look for air under the diaphragm (? Perforated gut).
MediastinumThe left hilum should be slightly higher than right.The trachea should be visible and central with a slight deviation to the right in its lower third.Are the left and right main bronchi visible? Can the carina be visualised?Is the heart size within normal limits? It should be less than half the total diameter of the thorax.
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
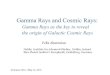
Is the heart shadow in a normal position? It should be a third to the right and two thirds to left.Is the heart shadow normal?
A Normal Chest X-Ray
5. Identify Abnormalities seen on Chest X-Rays and rationalisefindings in relation to the need for physiotherapy interventions.
Chest X-Rays may display;
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
COLLAPSE
Can be caused by compression e.g. Large pleural effusion Tumour Tension pneumothorax Ascites, hepatomegaly, splenomegaly.
The appearance is the same whatever the cause, and is modified by several factors including the degree of shrinkage, accompanying consolidation, state of pleura and pre-existing condition of lung. If the whole of a lung has collapsed, the hemi thorax of the affected side will be radio-opaque (a total whiteout). If the lung is only partially collapsed (lobe, segment, sub-segmental) and there is no accompanying consolidation there will be little increase in radio-opacity. The only evidence will be a shift in normal landmarks such as the position of the fissures, vascular pattern, hilar shadow, etc.
The Chest X-Ray features depend on the degree of lung collapse:
Airlessness with shrinkage. Atelectasis. This is absorption collapse as a sequel to bronchial obstruction
by extrinsic pressure; (tumour, glandular mass, aneurysm, enlarged left atrium, pericardial effusion), or by intrinsic disease; (bronchial Ca, granulation tissue, exudate, sputum or inhaled foreign material such as blood or vomit).
Pulls structures towards the area of collapse i.e. trachea, mediastinal shift, hemi-diaphragm shift etc.
Rib crowding with associated volume loss. Lung markings of the remaining lobes become more wide spaced. Can be sub-segmental, segmental, lobar or whole lung. Produces a total or
partial homogenous shadow of part or whole of the lung field.
Partial Lung Collapses
Right Upper Lobe; The horizontal fissure is pulled upwards and the trachea may be deviated to the right. There is an apical white triangular shadow.
Right Middle Lobe; Either there is a narrow band shadow in the position of the horizontal fissure or the right heart border is obscured.
Right Lower Lobe; The right hemi-diaphragm may be displaced upwards and the heart may be displaced to the right. The right hemi-diaphragm can become obscured with loss of the cardiophrenic angle and there is a shadow adjacent to the right heart border.
Left Upper Lobe; The trachea is displaced to the left .If the lingula is involved the left border of the heart may be obscured.
Left Lower Lobe; The heart may be displaced to the left and the left hemi-diaphragm may be pulled upwards. The left hemi-diaphragm is obscured with loss of the cardiophrenic angle and there is a solid white shadow behind the heart.
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
Physiotherapy techniques to treat lung collapse will differ depending upon the underlying cause, the degree of lung involvement, the level of patient stability and the patient compliance. A complete patient assessment will be necessary to select the most appropriate intervention but consider the usefulness of ACBT, Cough Assist, Manual techniques and Manual hyperinflations.
CONSOLIDATION
With consolidation air in the lungs is replaced by fluid, pus or cells. Consolidation may be lobar, sub-lobar, segmental, or sub-segmental.
Consolidation can be;
COMPLETE All the air in affected area has been replaced. The degree of radio-opacity depends on thickness of the consolidation in the line of the X-Ray beam. Evident on CXR is homogeneous shadowing occupying the anatomical area of the area affected by consolidation with loss of vascular markings. Also although the alveoli contain fluid the bronchi will probably still contain air which contrasts with the shadow producing air bronchograms.
INCOMPLETE Only some of the alveoli are affected and there is only a slight increase in the overall radio-opacity. This may appear on CXR as fine mottling or as a faint ground glass shadowing.
N.B. In many cases a combined collapse/consolidation may occur.
Physiotherapy techniques to treat lung consolidation will differ depending upon the underlying cause, the degree of lung involvement, the level of patient stability and the patient compliance. A complete patient assessment will be necessary to select the most appropriate intervention but consider the usefulness of positioning to decrease the work of breathing and V/Q optimisation, and secretion clearance techniques if the consolidation is secondary to sputum retention.
PLEURAL EFFUSIONS
This is fluid within the pleural cavity which occupies the space in the thorax at the expense of underlying lung which retracts towards the hilum. It appears on CXR as a homogeneous shadow devoid of pulmonary markings. Mostly free fluid gravitates to the dependant part of the thorax and the underlying lung de-aerates. However the presence of pleural adhesions between the visceral and parietal pleura may cause
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
loculations (encystment) of the fluid. The shape of the encystment is most frequently that of flattened biconcave lens.
Effusions are formed by;
Transudate – often bilateral (cardiac failure, ALD, renal disease). Exudate – pulmonary and subphrenic infection (pneumonia, pancreatitis). Haemorrhagic – trauma, post surgery, bleeding disorders. Chylous effusion - obstruction to thoracic ducts e.g. malignant invasion.
Radiological differentiation not possible.
Effusions can be classified by size; Small : 300-500mls. Causes clouding/obscuring of the costophrenic angle. If
the film is taken in the erect position there may be a fluid level. If the film is not fully erect there may not be a level, but the shadow will obscure the costophrenic angle. A small (100 - 200 ml) effusion may be hidden by the diaphragm on a P.A. film and only be seen on a lateral.
Medium : As the effusion increases in size the diaphragm will be obscured. The fluid will tend to track up the pleura giving it an upward going lip. If the film is taken in the supine position the fluid will track up the pleura giving a hazy appearance will be seen on the film at the affected side.
Large : May render the entire hemi-thorax opaque causing a “white out" of the affected side with mediastinal shift to contra lateral side.
Physiotherapy techniques are not useful in the management of pleural effusions other than to maximise healthy lung expansion, and the use of positioning to offset any increased work of breathing. Occasionally CPAP may be helpful for symptom management.
PNEUMOTHORACES
Caused by air in the pleural cavity. They can vary in size from small apical to large tension pneumothoraces, and should not be confused with bullae which also have few lung markings but have no visible lung edge. In the presence of a pneumothorax the underlying lung relaxes and retracts towards hilum leaving a clear radiolucent pleural cavity devoid of vascular markings, separated from lung by delicate white line (lung edge) of visceral pleura. Lobes may tend to separate as fissures allow a little air to enter them. Blood vessels of the affected lung may be of smaller calibre than those of sound lung which receives a preferential pulmonary blood flow. A large pneumothorax may cause mediastinal shift to affected side. Pneumothoraces are best demonstrated on P.A. expiratory radiograph.
Pneumothoraces can be;
Spontaneous; commonly caused by rupture of an emphysematous bullae or sub -pleural bleb.
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
Traumatic; Caused by external entry of air - e.g. penetrating wounds or from
mediastinal rupture of the trachea, bronchus or oesophagus (a pneumomediastinum may result from violent coughing).
Tension; Occurs when there is a valvar tear in the pleura so air enters with each inspiration and cannot escape on expiration. The air distended pleural sac may herniate across mediastinum and compress good lung, increasing mediastinal displacement. This compression of functional lung may precipitate an acute emergency and cause cardiac tamponade.
Physiotherapy techniques are not useful in the management of pneumothoraces other than to maximise healthy lung expansion and the use of positioning to offset any increased work of breathing.
RIB FRACTURES
Consider the number and position of any identified rib fractures. Fractures may be anterior, posterior or most commonly lateral. The possibility of flail segments should be examined for where there is more than one fracture on the same rib/ribs. Large flails will have significant effects on respiratory function. Rib fractures are often associated with underlying lung contusions or pneumothoraces. Old fractures are also often evident on CXR.
Physiotherapy techniques to assist in the treatment of patients with rib fractures will differ depending upon the underlying cause, the degree of lung involvement, the level of patient stability and the patient compliance. A complete patient assessment will be necessary to select the most appropriate intervention but consider optimal pain control as being key in the success of any treatment. Consider the usefulness of ACBT, Cough Assist, Manual techniques and Manual hyperinflations to assist with resolution of any associated secretion retention. Optimal positioning is also essential to reduce any increased work of breathing.
PULMONARY OEDEMA
This is an accumulation of excessive fluid in the interstitial spaces of the lung with subsequent movement of the fluid into the alveolar spaces. On chest X-ray it has a fluffy, usually bilateral shadowing which in its worse state can take on a ground glass appearance. Other features include;
Peripheral septal lines known as Kerley B lines. These are fine linear shadows 2-3cm long at the pulmonary edge perpendicular to the pleural surface. They are most numerous at bases, decreasing in number towards the mid zones.
Large septal lines known as Kerley A lines. These are straight linear shadows from the periphery to hilar that appear to cross vascular markings.
Peri-hilar haze. This is caused by oedema within interstial tissue around the hilum and it can extend from the hilar to the lower zones. This is what is
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
described as ground glass appearance.
Intra alveolar oedema – fluid transudes from the interstial tissues into the alveolar spaces giving fluffy ‘cotton wool’ opacities. A typical diagnostic distribution shows ‘bats wing shadows’ spreading out from the hilar regions.
Many causes;
Heart failure – acute Fluid overload e.g. Excess I.V. fluid Renal failure Cerebral disease e.g. CVA, Trauma ARDS (Adult Respiratory Distress Syndrome).Non-cardiogenic pulmonary
oedema, often associated with multi-organ failure.
Physiotherapy techniques are not useful in the management of pulmonary oedema other than the use of positioning to offset any increased work of breathing. Occasionally CPAP may be helpful for symptom management.
SURGICAL EMPHYSEMA
This is caused by air leaking into subcutaneous tissues which is clearly seen on chest X-Ray. Often muscle striations of the pectorals are visible. It will reabsorb once the air leak has stopped. Commonly associated with misplaced chest drains or large air leaks. It is only serious if it causes airway compromisation.
Physiotherapy techniques are not useful in the management of surgical emphysema.
PERFORATED GUT
This is evidenced on CXR by free air under the right hemi-diaphragm on a pre-operative film. It is an emergency sign which requires surgical intervention.
Physiotherapy techniques are not indicated.
LARGE CIRCULAR / OVAL SHADOWS
Chest X-Ray appearances will be dependent on the underlying cause;
Bronchial Cancer - often presents as a well-defined mass. Secondary deposits- metastatic disease often presents with multiple opacities
throughout the lung fields. It may also be associated with malignant effusions. Cyst – these may be fluid containing. T.B. Focus.
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
Lung abscess; well demarcated, often a fluid level is seen which may be due
to pus. Can be secondary to infections such as Staph pneumonia. Fungus infection – aspergilloma.
Physiotherapy techniques are not indicated.
PNEUMONIA
Many types – lobar, aspiration, hypostatic, atypical etc. and different features are seen with different infections. Typical CXR changes include;
• Air spaces are consolidated or filled with phlegm so an increased white shadowing is seen. This may be ill-defined if the consolidation is incomplete.
• With lobar infection white homogenous shadowing will occur in the anatomical region.
• Atypical infections such as Staph or Strep often cause widespread changes with diffuse patchy shadowing.
Physiotherapy techniques will be directed towards secretion clearance, optimisation of positioning and, respiratory support (CPAP) if presentation is severe.
ASTHMA
With asthma the Chest X-Ray may appear normal, but in acute events patients may show the following radiographic abnormalities;
Airways obstruction may lead to over inflation of lungs, a lowering of level of diaphragm, hyper translucency and a horizontal rib pattern.
Transient areas of consolidation may occur. In chronic cases bronchial wall thickening may be seen with accentuated lung
markings and prominent vascular patterning.
Physiotherapy techniques will be directed towards secretion clearance, optimisation of positioning and, respiratory support if presentation is severe.
EMPHYSEMA
Classified as;
Primary essential emphysema (in the absence of chronic bronchitis). Accompanying chronic bronchitis. Often associated with bulla formation and
progressive destructive changes.
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
Obstructive emphysema. Results from obstruction involving a large bronchus
caused by an inhaled foreign body or mass.
Chest X-Ray changes include;
Emphysema, and therefore some of the changes may be generalised or localised.
A reduction in the calibre and number of small vessels leading to reduced vascular markings, best seen in middle and outer thirds of lungs.
Air trapping which shows as increased lung volume or over inflation, and a flattening of the contours of diaphragm. The heart shadow is often long and narrow with a cardio-thoracic ratio of 1:3 or 1:4.
Lung fields usually appear more translucent. An increase, beyond the normal, in the airspaces distal to the terminal
bronchioles with dilation or destruction of their walls. Large hilar shadows (enlarged pulmonary arteries). Bullae. These are thin walled spherical or oval translucencies, varying in
diameter from a few mm to several cm. They often occur in groups, usually on the lung periphery at the base or apex or along the margins of the fissures. Bullae walls, when visible, are smooth and regular. Some can become huge, occupying most of the hemi-thorax displacing and compressing the rest of the lung tissue which may make them difficult to distinguish from a pneumothorax.
Physiotherapy techniques will be directed towards secretion clearance, optimisation of positioning and, respiratory support if presentation is severe.
COPD
Often there are no specific radiological signs but Chest X-Rays are performed;
To assess for the degree of emphysema. To determine whether cardiovascular changes of corpulmonale are
developing (increase in size of heart and main pulmonary arteries.) To assess for the presence of other disease or infection.
Where seen Chest X-Ray changes include;
Chronic inflammatory changes including small ill-defined opacities may be seen anywhere in lungs. These are small areas of consolidation or scarring from previous inflammation.
Linear shadows may be found which represent old fibrotic areas. Normal vascular pattern replaced by fine linear markings and added mottling.
Physiotherapy techniques will be directed towards secretion clearance, optimisation of positioning and, respiratory support if presentation is severe i.e. BiPAP.
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
CYSTIC FIBROSIS / BRONCHIECTASIS
Chest X-Ray changes include;
Chronic inflammatory changes Dilated airways Pockets of infection
Physiotherapy techniques to treat CF and bronchiectasis are generally directed towards secretion clearance including ACBT, manual techniques, positioning and postural drainage.
6. Document in the patient’s records.
7. Feedback clearly to the medical and nursing team, and physiotherapy colleagues for ongoing management.
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
Physiotherapy On Call Competencies
NAME: TAUGHT MODELLED COMPETENT
PTOC12
Chest X-Ray Interpretation DATE DATE DATE
1 Is able to discuss CXR in relation to:
Indications, Contraindications and risks Local policies and procedure
2 Understands and is able to discuss the differences between departmental and portable CXR’s.
3 Performs preliminary checks on the CXR
4 Uses a Systematic System of Scrutiny (SOS) to assess for normal and abnormal findings.
5 Demonstrates an understanding of the common radiological signs associated with respiratory pathology and shows the ability to rationalise findings to assist in formulation of treatment plans and interventions.
6 Documentation of findings and actions
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder

PTOC12
7
Feedback to medical and nursing team, and physiotherapy colleagues
Sign and date when achieved
Signature of Learner
Signature of Assessor
Date of Review
© Rachael Smith &Jayne Duffy (Effective Workforce Solutions Ltd) All rights reserved. Not to be reproduced, stored or transmitted in whole or part without permission of copyright holder