Embed Size (px)
Citation preview

Ways of Working in Nursing
Resource Package

NSW DEPARTMENT OF HEALTH
73 Miller Street
NORTH SYDNEY NSW 2060
Tel. (02) 9391 9000
Fax. (02) 9391 9101
TTY. (02) 9391 9900
www.health.nsw.gov.au
Produced by:
Nursing and Midwifery Office
NSW Department of Health
Tel. (02) 9816 0373
Fax. (02) 9816 0240
This work is copyright. It may be reproduced in whole or in part for study
training purposes subject to the inclusion of an acknowledgement of the source.
It may not be reproduced for commercial usage or sale. Reproduction for purposes
other than those indicated above requires written permission from the
NSW Department of Health.
© NSW Department of Health 2011
SHPN (NM) 110125
Further copies of this document can be downloaded from the
NSW Health website www.health.nsw.gov.au
June 2011

WOW Resource Package NSW HealtH PaGe i
Preface
The healthcare environment in which we work is constantly changing and evolving.
Healthcare professionals in hospitals today provide care for an increasing number
of acutely ill patients often with a number of chronic conditions and associated
co-morbidities. Consequently, acute care hospitals are busy places accommodating
sicker patients requiring more intensive treatment and nursing care. Advances in care
have also led to a reduced length of stay and a higher patient turnover as well as an
increase in the complexity of specialist and general medical and surgical nursing care.
At the same time we are experiencing changes in our nursing workforce. Different levels of nurses, an aging workforce
and an increasing number of novice practitioners compel nurses to constantly assess and reassess the way that work is
managed within their wards/units. Nurses today need to support and grow the workforce of the future by ensuring that
not only the “science” but also the “art” of nursing is supported through the way that work is organised. The initial
education we all receive provides a solid foundation on which we build further skills and knowledge through practical
application. This growth in practice is supported by colleagues willing to share their knowledge and skills.
The NSW Department of Health Nursing and Midwifery Office commenced the Ways of Working (WOW) Project in
2010 to explore the ways that nurses organise their clinical work and to develop a suitable framework and guidelines
to support a collaborative nursing model (CNM).
The Project Officer visited many sites and spoke to key stakeholders regarding the way that work is organised on wards
and units across NSW. Many ways of working were observed and discussed but it was identified that a more collaborative
approach would provide support for the development of the workforce into the future and enhance patient care by:
• More efficient use of nursing resources
• Improved communication between staff
• Improved support for staff new to an area of practice
• Improved capacity to effectively utilise different skills within the nursing team.
One of the strategies to assist nurses in working more collaboratively is the WOW Resource.
Nurses throughout the system are encouraged to actively consider their Ways of Working on a regular basis and
to be prepared to change these to better meet the needs of patients and also support a positive work environment.
This Resource recognises that Ways of Working can vary across and within health services and does not seek to suggest
a particular model but provides guidance for wards/units in reviewing their Way of Working and principles that can
guide the ward/unit in developing a collaborative nursing model.
Adjunct Professor Debra Thoms
Chief Nursing and Midwifery Officer
NSW

PaGe ii NSW HealtH WOW Resource Package
Contents
1. WOWResourcePackageOverview....................................................................................................1 Purpose .............................................................................................................................................................. 1
Objectives ........................................................................................................................................................... 1
Background ........................................................................................................................................................ 2
What is a collaborative nursing model? ............................................................................................................... 2
What does working in a CNM look like?.............................................................................................................. 5
2. ImplementingaCNM:GettingStarted...............................................................................................6 Evaluating your efforts ........................................................................................................................................ 7
Impact on nursing staff ....................................................................................................................................... 7
Impact on patient care ........................................................................................................................................ 8
3. ImplementingaCNM:Planning...........................................................................................................9 The implementation plan .................................................................................................................................... 9
Team member roles ............................................................................................................................................ 9
The NUM ............................................................................................................................................................ 9
TeamRoles.........................................................................................................................................12 Role of the RN ...................................................................................................................................................12
Role of the team leader ......................................................................................................................................13
Role of the EN ................................................................................................................................................... 14
Role of the AIN ..................................................................................................................................................15
4. ImplementingaCNM:Whathavewedone?....................................................................................16 Re-evaluating your efforts ................................................................................................................................. 16
Sustaining the work .......................................................................................................................................... 16
Appendices.................................................................................................................................................18Appendix 1: Glossary of terms ...................................................................................................................................... 18
Appendix 2: Useful reading and references – Further help ............................................................................................. 19

WOW Resource Package NSW HealtH PaGe 1
WOW Resource Package Overview
SECTION 1
Purpose
The WOW Resource has been developed to assist nurses1
in their efforts to introduce a collaborative nursing model
(CNM) into their ward/unit. It is envisaged that the NUM
will be coordinating the project and the WOW Resource
has been designed accordingly.
Objectives
The WOW Resource will:
1. Introduce the evidence for considering a CNM in your
ward/unit
2. Provide guidelines for implementing a CNM in your
ward/unit
3. Provide an audiovisual representation of nurses working
collaboratively
4. Provide tools that can be used to support and evaluate
a CNM.
1 Nurse will be used throughout this document.
If you are considering introducing a collaborative midwifery
model refer to midwifery models of care resources:
http://www.health.nsw.gov.au/nursing/midwifery.asp#para_5.
Throughout the WOW Resource the reader is directed to:
Helpful tools
Internet sites
The WOW Film – Making it Real
Note: An internet connection is required to review
these element links of the package. Should you have
any difficulty with the links through this pdf resource,
please access the elements via the website at:
http://www.health.nsw.gov.au/nursing/projects/WOW.asp
To allow the reader to evaluate progress in
implementing a CNM he/she is provided with:
Reflection spaces
Regular checkpoints
Note: This package is designed as an electronic
resource and if printing is necessary it will take
considerable time and paper to print out in its entirety.
The WOW Resource is freely available through the
Department of Health website link at:
http://www.health.nsw.gov.au/nursing/projects/WOW.asp

PaGe 2 NSW HealtH WOW Resource Package
Background
There are a plethora of studies conducted on the
topic of the ways that nurses organise their clinical
care and it is beyond the scope of this package to
provide a comprehensive literature review.
Follow this link to a short summary of the different ways of working nurses use including:
– Patient allocation
– Task/functional
– Team/modular
– Primary nursing and case
management
Apart from the ways that nurses organise their clinical
care, there is considerable literature available regarding
components of a collaborative nursing model (CNM).
A comprehensive list of references and appropriate
web-based documents is provided at the end of the
WOW Resource and some will be discussed under
the appropriate sections of the package.
WhatisaCollaborativeNursingModel?
A collaborative nursing model is:
A model of care delivery based on collaboration
where an appropriately skilled nurse takes
responsibility for leading a team. The team can
accommodate different levels of nurses working
together with a shared goal, to meet the
comprehensive holistic care needs of a
group of patients.
The aim of a CNM is to utilise and develop the skills
of the nurses to the fullest extent by providing a
supportive learning environment. Clear guidelines
and communication and reporting structures are
required to enable the team to function efficiently.

WOW Resource Package NSW HealtH PaGe 3
Table 1
A Collaborative Nursing Model
n Allows nurses at different levels of training and expertise to perform their work more effectively
n Ensures improved supervision and support of nurses transitioning to practice and non permanent members of the nursing team by more senior staff
n Takes advantage of each member’s skills and level of experience – leading to professional development and enhancement of knowledge and skills of junior staff
n Reduces staff isolation and allows for a supportive working environment
n Can improve patient outcomes and satisfaction with care provision
n Allows individual team members to become familiar with all team members’ skills and capacities
n Assists continuity of patient care and support for part time nurses by assigning full-time and part-time nurses to the same team
n Reduces the risk of missed care (any aspect of required patient care that is omitted or significantly delayed)
n Allows for team members to share the burden of ‘difficult’ patients and a heavy workload leading to reduced nurse stress levels and manual handling injuries
n Can improve job satisfaction and lead to increased morale
n Leads to reduced complaints from other healthcare workers and visitors about their inability to seek up-to-date information about the condition of patients. There are more nurses involved in the one patient’s care and less ‘I don’t know. I am not looking after them’ responses for assistance
n Ensures that relief for escort duties and meal breaks is provided by from someone who ‘knows’ the patients
n Should make it easier to have medications and intravenous therapy checked if team members are working together in the same relative location negating the need to search the ward for assistance.
A CNM is based on the principles of teams and teamwork.
Teams are increasingly becoming the format for the way
of working for all healthcare professionals as the nature
of the clinical work is being dramatically transformed.
Simply a team is:
‘….a group of people who are mutually dependent
on one another to achieve a common goal’.
The most common team we hear about in healthcare is the
multidisciplinary team. A multidisciplinary team comprises
all the healthcare workers involved in a particular patient or
a group of patients’ care and might include a number of
doctors, allied health and nursing staff. On a shift to shift
basis there are a number of nurses providing direct patient
care and the emphasis of the WOW Resource is on this
nursing team.
The team can comprise whatever groups or levels of nurses
deemed appropriate by the ward/unit staff. It will depend
on the number of beds on the ward/unit and the level of
staffing and skill mix. A team should consist of a staff
member who takes on the team leader role. This would
commonly be a registered nurse (RN). The NUM will remain
in an overarching coordination role for the combined
nursing teams and the team leaders and NUM will meet
regularly throughout the shift to provide updates on
patient progress and nursing care requirements.
Some teams will be big and some will be small and as
highlighted there is no limit to how the team is configured
as long as the configuration meets the needs of the ward/
unit. There will be more information regarding the makeup
of the teams and how a CNM can be implemented
throughout the WOW Resource.
PaGe 4 NSW HealtH WOW Resource Package
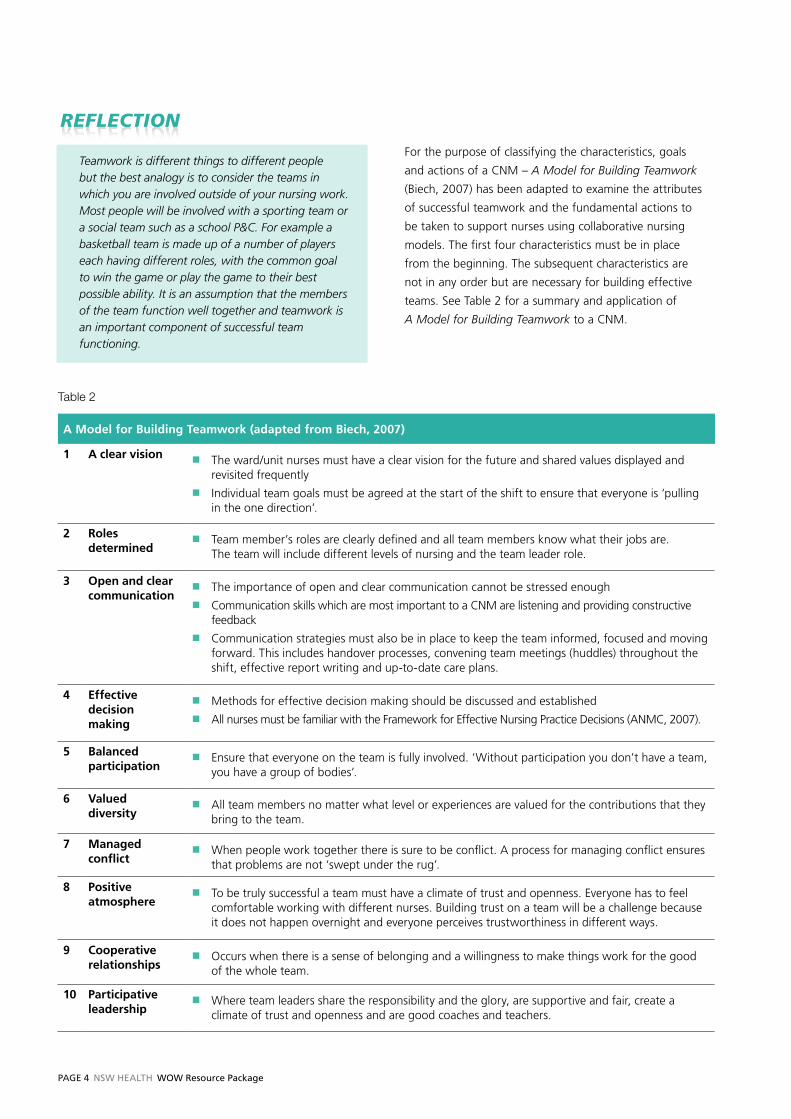
Teamwork is different things to different people but the best analogy is to consider the teams in which you are involved outside of your nursing work. Most people will be involved with a sporting team or a social team such as a school P&C. For example a basketball team is made up of a number of players each having different roles, with the common goal to win the game or play the game to their best possible ability. It is an assumption that the members of the team function well together and teamwork is an important component of successful team functioning.
For the purpose of classifying the characteristics, goals
and actions of a CNM – A Model for Building Teamwork
(Biech, 2007) has been adapted to examine the attributes
of successful teamwork and the fundamental actions to
be taken to support nurses using collaborative nursing
models. The first four characteristics must be in place
from the beginning. The subsequent characteristics are
not in any order but are necessary for building effective
teams. See Table 2 for a summary and application of
A Model for Building Teamwork to a CNM.
Table 2
A Model for Building Teamwork (adapted from Biech, 2007)
1 A clear visionn The ward/unit nurses must have a clear vision for the future and shared values displayed and
revisited frequently n Individual team goals must be agreed at the start of the shift to ensure that everyone is ‘pulling
in the one direction’.
2 Roles determined
n Team member’s roles are clearly defined and all team members know what their jobs are. The team will include different levels of nursing and the team leader role.
3 Open and clear communication
n The importance of open and clear communication cannot be stressed enough n Communication skills which are most important to a CNM are listening and providing constructive
feedback n Communication strategies must also be in place to keep the team informed, focused and moving
forward. This includes handover processes, convening team meetings (huddles) throughout the shift, effective report writing and up-to-date care plans.
4 Effective decision making
n Methods for effective decision making should be discussed and established n All nurses must be familiar with the Framework for Effective Nursing Practice Decisions (ANMC, 2007).
5 Balanced participation
n Ensure that everyone on the team is fully involved. ‘Without participation you don’t have a team, you have a group of bodies’.
6 Valued diversity
n All team members no matter what level or experiences are valued for the contributions that they bring to the team.
7 Managed conflict
n When people work together there is sure to be conflict. A process for managing conflict ensures that problems are not ‘swept under the rug’.
8 Positive atmosphere
n To be truly successful a team must have a climate of trust and openness. Everyone has to feel comfortable working with different nurses. Building trust on a team will be a challenge because it does not happen overnight and everyone perceives trustworthiness in different ways.
9 Cooperative relationships
n Occurs when there is a sense of belonging and a willingness to make things work for the good of the whole team.
10 Participative leadership
n Where team leaders share the responsibility and the glory, are supportive and fair, create a climate of trust and openness and are good coaches and teachers.

WOW Resource Package NSW HealtH PaGe 5
WhatdoesWorkinginaCNMLookLike?Ruth Hansten (2009) suggests that when ‘a bundle of best
bedside practices’ are integrated into practice they become
a shared standard resulting in optimum clinical outcomes.
The ten steps are applicable to the way an ideal shift might
Table 3
Best Bedside Practices – shift steps – based on Hansten (2009)
1 Make assignments for care providers based on the patient’s 4 Ps n purpose, for being engaged in this episode of caren picture, of success including short and long term goalsn plan of caren part each person plays
and the skills and expertise of the nurses in the team.
2 Handover performed at the bedside. This doubles as an Introductory round where the team meets the patients and performs a quick assessment.
3 The team leader in consultation with the team thinks critically about the plan for the shift, prioritising the care and assigning utilising the 5 Rights of Delegation:n right taskn right circumstancesn right personn right direction and communicationn right evaluation
Plans are also made for meal breaks and team checkpoints
4 All team members pitch in and help each other with the work at hand. Priority is given to less experienced staff to allow them to gain competency in the skills required to care for patients during the shift.
5 Throughout the shift care plans are made in partnership with the patient/family.
6 The plan is communicated to all care providers via the team leader. Mechanisms are put in place to ensure that all team members and the NUM are kept up-to-date.
7 Participation in interdisciplinary rounding to share and evaluate progress.
8 Teamwork checkpoints convened at appropriate intervals to evaluate the care.
9 Reciprocal feedback and celebration checkpoint held near the end of the shift to determine whether the goals for the shift have been achieved.
10 Critical thinking and problem solving are used to plan for the next shift and the handover of care.
look when nurses are working in a CNM. The steps are
underpinned by most of the key components of The Model
of Teamwork which include; goal setting, communication,
delegation, support and coaching. The steps have been
modified for our NSW healthcare context and are
summarised in Table 3.

PaGe 6 NSW HealtH WOW Resource Package
SECTION 2
Implementing a CNM – Getting Started
On some wards/units a change to a CNM will be a big adjustment for the staff. The majority of nurses are used to working in a patient allocation model. They value the contribution working in a patient allocation model makes to the level of expert care they provide, although it has been identified that most newly graduated nurses and nurses new to the ward/unit or specialty appreciate a more team approach to care.
Consider your team’s readiness for change and the ways that you might approach this project.
Getting started is the most time consuming phase of
the project and involves lots of discussion and planning.
Encourage all of the nurses to be involved in the CNM
Project by using principles of Practice Development
methodology. Practice Development is gaining momentum
in NSW as clinicians come to appreciate the value of using
a systematic approach to delivering person-centred care
that encompasses the needs of patients, families and staff.
Person-centred care incorporates the Practice Development
principles of inclusiveness, respect for each other, valuing
individual contributions and connecting. If you require
further information on Practice Development please
follow this link.
Link to PD explanation on NaMO website
As highlighted in The Model for Teamwork, the first
place to start is to have a clear vision for the ward/unit.
Everyone needs to have the opportunity to contribute to
the shared vision. It is quite likely that common themes will
arise that indicate support and teamwork are values the
nurses would like to experience on the ward/unit. The vision
for the ward/unit must be displayed where all staff, visitors
and patients can see it. It should also be reviewed and
discussed regularly to ensure that it still represents the
collective values of the current staff.
If your ward/unit is participating in the Essentials of Care
(EOC) Project you should already have a clear vision but
you might like to revisit it before you consider discussing
a CNM. If you need more information regarding values
clarification please discuss with an EOC facilitator or click
on the link below.
Link to values clarification discussion and exercise on the NaMO PD site
You will require the engagement of all nurses on your
ward/unit in understanding that a CNM is the most
effective way for them to practice. The best way to
commence useful discussions is to provide them with the
evidence for change. Perhaps your nurses already work in
a collaborative way and would benefit from discussions on
some of the improvements they could make to that CNM.
To assist you in this process a WOW PowerPoint presentation
containing evidence and information supporting a CNM is
provided. The PowerPoint presentation is available at the
following link.
Link to Powerpoint presentation
Just because a group of people come together as a team,
it does not mean that they function effectively. Teams
develop over time and the project to support a CNM will
also take time to enact.
This would be an appropriate time to encourage staff to
view the WOW film – Making it Real.
Making it Real has been produced to show a nursing team
role modeling the bundle of best bedside practices and
how the shift might look when working in a CNM.
Link to Making it Real

WOW Resource Package NSW HealtH PaGe 7
Take the time to examine how the WOW on your ward/unit might be modified to reflect a CNM
As part of the discussions about the WOW on the ward/
unit it might be useful to conduct an exercise to address
any Claims Concerns and Issues the staff might have about
modifying or changing their current WOW to a CNM.
Information on how to conduct a Claims Concerns and
Issues exercise is found at the following link.
Link to conducting a claims, concerns and issues exercise
Evaluating Your Efforts
When introducing change it is always helpful to know what
difference you have made. You need to know where you
have been and where you are now. Therefore, evaluation
must be established at baseline before the implementation
of the new WOW and followed at regular intervals dependant
on the strategies used. Another reason to evaluate your
efforts is to ensure that the project is on track and moving
toward meeting the project objectives and that CNM
changes are identified and adjusted accordingly on
an ongoing basis:
Evaluation of a CNM at a ward/unit level could:n Identify the effectiveness of a CNM on patient and/or
quality outcomes n Identify the effectiveness of the nurses working within
the team in regard to teamwork and collaborationn Identify nursing and key stakeholder satisfaction with
the model by capturing and comparing:
– Ward unit workforce data
– Nursing satisfaction
– Key stakeholder satisfaction.n Capture the improvements as a result of implementation
of CN modelsn Identify if the CNM is sustained, becoming part of
the culture and the way things are done on a
day-to-day basis.
You will need to consider the evaluation strategies you will
use. The following are some ideas that you might consider.
Impact on nursing staff
Evaluation of the impact of the CNM on nursing staff
can be approached in two ways: the way that the nurse
collaborates and functions within the nursing team and
secondly, the satisfaction of the nurse with the CNM.
Nurse functioning within the team
The Nursing Teamwork Survey (NTS) was developed and
validated for use in the United States (Kalisch, Lee & Salas,
2010). The NTS measures the level of nursing teamwork in
acute care settings. Permission has been sought from the
authors to use this tool with minor demographic changes
required for the Australian context. Follow the links below:
Links to
– A copy of the short survey – A copy of the long survey
– Instructions for using the NTS
– An excel spreadsheet which can be used to enter and analyse the survey responses
Nurse satisfaction
Nurse satisfaction with the model of care is pivotal to
the success of the CNM. The Nursing Workplace
Satisfaction Questionnaire (NWSQ) was developed
specifically to evaluate job satisfaction with a new model
of team nursing within a large Sydney Teaching Hospital
(Fairbrother, Jones & Rivas, 2009). The tool is available
to use for the project with permission from the authors.
Follow the link below to find the tools required to conduct
this questionnaire.
Links to
– A copy of the questionnaire
– Instructions for using the NWSQ
– An excel spreadsheet which can be used to enter and analyse the questionnaire responses
If your ward/unit is involved in EOC the nurses may have
already completed the NWSQ or the Person Centred
Nursing Index (PCNI) and there will be no need to
re-evaluate. Some facilities have their own version of a staff
satisfaction survey but they may not be appropriate because
most do not contain questions about the organisation of
care and collaboration and teamwork which are essential
components of a CNM.

PaGe 8 NSW HealtH WOW Resource Package
Workforce data
Recruitment and retention are often used to identify a work
place or situation which has a positive or negative work
culture. Nurses are more likely to be attracted to a place or
remain on staff in a ward/unit where there is a positive work
environment and supportive team (Duddle & Boughton,
2007; Aiken, Clarke, Sloane, Lake & Cheney, 2008; Kalisch,
Weaver & Salas, 2009). A comparative study of team nursing
vs. allocation nursing was conducted in a large Sydney
Teaching Hospital. The intervention (team nursing) group
had a reduction in vacancy rate below that of the control
group (allocation) following the study by Fairbrother (2010).
ImpactonPatientCare
Teamwork is essential for patient safety and the provision of
quality care (NHS, 2007). Therefore, evaluation could
include nurse sensitive safety and quality outcomes. The
problem is that these outcomes are often difficult to define
as most patient outcomes are not wholly sensitive to the
nursing care provided. There has been considerable work
conducted in the USA which indicates a relationship
between nursing care and some specific indicators including
falls and pressure ulcers (Montalvo, 2007). Fowler, Hardy &
Howarth (2006) attempted to measure the effect of a
collaborative nursing model on clinical outcomes. There was
an increase in incident/accident reports which may be due
to an increased reporting rather than an actual increase.
Heinemann, et al (1996) measured the effect of a project
titled ‘Partners in patient care’ on quality indicators.
Indicators included falls, medication errors and intravenous
device infection rates and found that there was no significant
difference between the pilot wards which instituted a team
based model compared to the control ward.
Data can be sourced from existing systems including the
Incident Information Management System (IIMS), complaints
and compliments and nurse sensitive indicators and audits
deemed appropriate for the ward/unit. Ward/unit staff
could audit the nursing care activities which have meaning
for them in their particular context eg falls in aged care
or line infection in an ICU.
NB: You may have already done this as part of EOC.
Although the evidence is not conclusive it would be
worthwhile investigating whether there is a change
in patient outcomes after introducing a CNM on
your ward/unit.
In addition to the ward/unit nurses, it is always a good idea
to share the evaluation with key stakeholders including
management. This will assist by substantiating the time and
effort put into conducting the CNM project, demonstrating
the impact of your endeavours and hopefully to celebrate
you and your nurses’ success.
Project Checkpoint One
Is Practice Development methodology being used? 3Are regular meetings scheduled? 3Has a values clarification exercise been conducted? 3Do the ward/unit nurses have a clear vision guiding their work? 3Has the WOW PowerPoint Presentation been shown and discussed with all staff? 3Has a Claims, Concerns and Issues exercise been conducted? 3Have all staff seen the WOW Presentation – Making it Real? 3Has pre-evaluation been conducted? 3
If the above are in place, you should be able to progress to Implementing a CNM – Planning.

WOW Resource Package NSW HealtH PaGe 9
SECTION 3
Implementing a CNM – Planning
Again the planning and implementation phase must be a
collaborative effort; all ward/unit nurses should have a clear
understanding of the project. Do not jump in and expect
everyone to work in a CNM. Discussions will need to occur
around how and when. If a Claims Concerns and Issues
exercise has been conducted, revisit the questions which
were formulated and start by addressing them.
The big question is:
What has to be done to Start a CNM on the Ward/Unit?
This will help identify where the deficiencies lie and what
will need to be developed and what education supports
might be required. The next section of the WOW Resource
will provide assistance on aspects of a CNM which might
require development.
TheImplementationPlan
Develop a clear implementation plan and identify an
implementation timeframe. Health is an unpredictable
environment and there will be interruptions and hurdles
along the way. In times of increased workload project work
is often given reduced priority. If you find that there are more
critical priorities, just return to your plan and pick up where
you left off when things settle.
TeamMemberRolesFor a CNM to work effectively everyone needs to
be aware of each other’s roles in the team. This is
emphasised in A model for building teamwork:
‘Defining the team roles lets all team members
know what their jobs are and recognises individual
talent tapping into the expertise each member
brings to the team.’
It also recognises that regardless of how long we have
been in practice we can all be at different stages in our
professional development. The aim is to use the full
capacity of skills and knowledge available in the team.
The team will be constructed of different categories of
nurses including:n NUMn Registered nurses including: – newly registered nurses – agency and casualn Enrolled nurses including agency and casualn Assistants in nursing.
Nursing students should be included in the team providing
the opportunity to experience a CNM.
No matter where a nurse is working he/she must work
within their scope of practice at all times:
A profession’s scope of practice is the full spectrum
of roles, functions, responsibilities, activities and
decision making capacity which individuals within
the profession are educated, competent and
authorised to perform.
Delegation and Supervision for Nurses and Midwives (2007)
TheNUM
It is quite likely that the NUM is overseeing or coordinating
the CNM Project. Whether or not the NUM is the project
coordinator, the NUM will need to have a clear understanding
of the project and be fully involved in its implementation.

PAGE 10 NSW HEAltH WOW Resource Package
Think about how you can achieve this big task.
Try not to tackle it all on your own. Get support of some likeminded colleagues who are also implementing a CNM Project on their ward/unit and also seek out some champions within your ward/unit nursing team.
Consider the skills you may have gained through ‘take the lead’ and how they can be utilised in this project.
It might be possible to allocate some protected time for the CNE or a CNS to coordinate the project. Most of all, remember that the Practice Development principles of inclusiveness, respect for each other, valuing individual contributions and connecting will lead to greater acceptance of the new CNM.
Rostering for appropriate teams
One of the NUM’s major contributions will be rostering for
appropriate teams. The clinical area should be divided
geographically into distinct areas to reduce the amount of
unnecessary travel for the team members. Also take into
consideration the patient mix within these areas. If the
ward/unit has more acutely unwell patients within one area
then the team for that area might be bigger or they might
need to be allocated less patients. The patient load for a
team can be flexible dependent on the skill mix and the
acuity of the patients.
When preparing the rosters it will be important to divide
the roster into levels of expertise. One good way to
determine the level of expertise is to use the framework
proposed by Patricia Benner (1984) – ‘Novice to Expert’.
This framework is used widely and is acknowledged as an
effective way to classify nurse skill acquisition. Click on the
following link to a comprehensive overview of Benner’s
stages of clinical competence.
Link to comprehensive overview of Benner’s stages of clinical competence
Experience as it is used in this resource, does not necessarily
refer to the length of time in a position, rather it refers to a
very active process of refining and changing preconceived
theories, notions and ideas when confronted with actual
situations (Benner, 1984). Some nurses will progress to an
expert in a relatively short period of time while others may
spend ten years on a ward without being classified as expert.
In addition, you do not need to be an RN to be seen as an
experienced nurse.
A proficient/expert nurse must be allocated to each team to
fulfill the team leader role. It is important to be flexible in the
way the team is composed to allow for patient acuity, changes
to skill mix and to cover untoward situations such as sick
leave replacement. Perhaps there will be situations where
there is no proficient/expert RN to lead a team. It might be
necessary to alter team assignments and perhaps one
proficient/expert RN could be allocated to leading the ward/
unit team in its entirety. This might be the option of choice
for some smaller wards/units where the staffing allocation
is less. Sample schemata for the shift staffing have been
developed and can be found at the link below.
Link to
view sample schemata for team assignment
Communication
The NUM will need to organise an appropriate allocation
board which can be hung clearly at the nurses’ station so
that the nurses and other health professionals and visitors
are aware of the team looking after the patient and the
designated team leader.
Another necessary housekeeping duty will be to organise a
communication system for the staff. A comprehensive
and up-to-date care plan will help guide the team in the
goals and activities to be performed for the shift. Regular
team huddles are also a way for the team to communicate
their progress in the shift plan.
Managing conflict
It is not unusual to have conflict in the workplace and
appropriate systems are required to manage it. When
nurses work in a patient allocation model they often do not
have to work together closely with other nurses. In a CNM
team members need to have the skills to approach other
members who are ‘not pulling their weight’. In the event
that conflict occurs in teams there should be a standard
mechanism for dealing with it. The actions to be taken

WOW Resource Package NSW HealtH PaGe 11
when a team member’s behavior diverges from the
group values should have been discussed in the values
clarification exercise.
Check to see if your organisation has a policy for managing
conflict. You might need to draw staff’s attention to this
policy and why it is important in a CNM. One of the key
things to remember is that teams require time to develop.
Do not expect smooth sailing especially when a CNM is
first introduced. Follow the link below to a sample conflict
resolution flow chart which you might consider using if
you do not have one.
Link to view a conflict resolution flowchart

PaGe 12 NSW HealtH WOW Resource Package
TeamRoles
RoleoftheRN
Competencies for entry RN practice in Australia have been
developed. It has been identified through the WOW Project
that not all nursing team members are familiar with these
competencies and it would be beneficial for all staff to
review them in the CNM Project planning stage.
Link to The National Competency Standards for the Registered Nurse can be found on the following web page: http://www.nursingmidwiferyboard.gov.au/Codes-and-Guidelines.aspx
The RN competencies are grouped under four major
domains as set out in the table below. RNs are required
to meet these in order to register. First year RNs will take
time to consolidate these competencies and the specialty
skills required as a new member of staff on the ward/unit.
The first year RN is supported by the CNM to attain
these skills in a supportive learning environment.
Table 4
The National Competency Standards for the RN – Domains
Professional practicen Practices in accordance with legislation affecting nursing practice and health care.n Practices within a professional and ethical nursing framework.
Critical thinking and analysisn Practices within an evidence-based framework.n Participates in ongoing professional development of self and others.
Provision and coordination of caren Conducts a comprehensive and systematic nursing assessment.n Plans nursing care in consultation with individuals/groups, significant others and the interdisciplinary health care team.n Provides comprehensive, safe and effective evidence-based nursing care to achieve identified individual/group health outcomes.n Evaluates progress towards expected individual/group health outcomes in consultation with individuals/groups, significant
others and interdisciplinary health care teams.
Collaboration and therapeutic practicen Establishes, maintains and appropriately concludes therapeutic relationships.n Collaborates with the interdisciplinary health care team to provide comprehensive nursing care.

WOW Resource Package NSW HealtH PaGe 13
There are at least five standards listed in the competency
document that have important significance to a CNM.
These standards have been extracted and highlighted
in Table 5.
Table 5
Standards CNM skills
2.7 Recognises the differences in accountability and responsibility between RNs, ENs and unlicensed care workers. Delegation
4.3 Contributes to the professional development of others. Clinical teaching and coachingSupervision
7.5 Delegates aspects of care to others according to their competence and scope of practice.
Clinical teaching and coaching:SupervisionDelegation
7.6 Provides effective and timely direction and supervision to ensure that delegated care is provided safely and accurately. Delegation
10.3 Facilitates coordination of care to achieve agreed health outcomes. Leadership and collaboration
Delegation, clinical teaching and coaching, supervision,
leadership and collaboration are areas which might need
development in the RNs who work on the ward/unit.
The skills will be required to work effectively as a team
member and as a team leader. To support RNs in
achieving skills in these areas you might direct your
nurses to educational opportunities through the LHD or
other education providers, eg The College of Nursing.
NaMO is also examining other resources to assist nurses
in the acquisition of these skills.
All roles within the team should have a position description
developed incorporating the specific responsibilities and
competencies required for the role.
Roleoftheteamleader
All teams have a designated team leader. Put simply:
The team leader coordinates a small group of nurses
to provide care for a group of patients for the shift.
All efforts should be made to roster a proficient/expert
RN in the team leader role. Some teams might be made
up of more than one RN and negotiation needs to occur
for the opportunity to take on the lead role for the shift
or to accept delegations as a member of the team.
There are specific skills and knowledge required by the
team leader and these are listed in Table 6.

PaGe 14 NSW HealtH WOW Resource Package
Table 6
The Team Leader
n Is familiar with the ward/unit routines
n Is knowledgeable and skilled in care provision for the specific patient group
n Is familiar with the condition and needs of all patients assigned for the team and assists in planning the individualised care for each patient
n Possesses critical decision- making skills
n Is a coach and clinical teacher, skilled in giving feedback
n Encourages a cooperative environment
n Delegates and assigns care according to scope of practice of team members
n Processes good communication skills and maintains clear communication among all team members including convening regular team huddles to communicate progress toward meeting the shift goals
n Is able to use his/her initiative.
As already highlighted, some of the attributes listed above
might not be skills that all RNs in the ward/unit currently
possess. RNs will need support to develop these important
attributes to enable them to function to their full scope and
practice as an RN.
RoleoftheEN
The enrolled nurse is an associate to the registered
nurse who demonstrates competence in the provision
of patient-centred care as specified by the registering
authority’s license to practice, educational preparation
and context of care.
(EN Competency Standards, 2002)
Somebackground
ENs comprise about 14% of the public sector nursing
workforce in NSW. With changes to workforce patterns
and models of care delivery there has been a renewed
interest in the EN position and ENs have been introduced
into a number of acute health care facilities. Recent changes
to National Law have resulted in no endorsement for
medicine administration by ENs as all ENs practicing in
Australia will as part of their education program; have
undertaken the relevant units of study enabling them to
administer medications safely (Nursing & Midwifery Board
Australia, 2010).
In July 2009 there was a major change to the education
model for ENs in NSW with a move to a pre-service course.
Previously, ENs were educated in an apprentice model;
whereby they were employed by their Area Health Service
for 12 months and attended lectures at Technical and
Further Education (TAFE) for 15 weeks. In the new model
EN education continues to be provided by TAFE NSW and
clinical experience is gained from clinical placements in a
variety of health facilities as well as in clinical simulation
laboratories. These changes bring NSW in line with other
Australian States and Territories and provide a more
supportive learning environment for the students as they
are no longer relied on as part of the nursing workforce.

WOW Resource Package NSW HealtH PaGe 15
In general, the role and functions of the enrolled nurse
are not clearly recognised by managers, RNs and ENs
themselves. This has led to the inconsistent application of
the role and functions of the ENs across the public health
sector. There are wards/units where ENs do not work to
their full scope of practice ie they are performing less
functions than the EN is legislated or trained to do and In
some instances ENs are working in advanced roles without
the necessary education and governance to support them.
Changing skill mix and workforce issues require the effective
utilisation of ENs as part of a CNM. Discussions must be
conducted regarding the roles and functions of the EN
within the team before the CNM Project begins. Ambiguity
in roles could lead to conflict between the team members
and this should be avoided if clear roles are established.
Link to The National Competency Standards for the Enrolled Nurse can be found on the following web page: http://www.nursingmidwiferyboard.gov.au/Codes-and-Guidelines.aspx
Link to Australian Nursing Federation Competency Standards for the Advanced Enrolled Nurse are found at: http://www.anf.org.au/pdf/Competency_Standards_Advanced_EN.pdf
RoleoftheAIN
NSW Health released a policy directive in 2010 which
supports the introduction of AINs into acute care units/wards.
The purpose of this policy is to facilitate uniform practices
for employing, expanding and developing the AIN role.
The policy outlines the education, qualification or
equivalency, scope of practice and skills recognition
processes to be applied to those in this employment
category. The policy also refers employers to assessment
processes for identifying the appropriate clinical
environments for AIN allocation in acute care.
Link to Visit the NSW Health Working with AINs Website http://www.health.nsw.gov.au/training/ain/workingwithains.asp for the following documents
n Health Service Implementation Package: Working with
Assistants in Nursing in the acute care environmentn Position Description for Assistant in Nursing –
Acute Caren Delegation and Supervision Guidelines.
Project Checkpoint Two
Is Practice Development methodology being used? 3Are regular meetings scheduled? 3Have the team roles been defined and are staff aware of them? 3Is the allocation board ready? 3Is there a team communication system? 3Has conflict resolution been discussed with staff? 3Are education supports in place? 3Is the implementation plan in place? 3Has a start date been established? – Go for it. 3

PAGE 16 NSW HEAltH WOW Resource Package
Once the CNM has been implemented on the ward/unit
it is time to evaluate what difference it has made, what
further changes need to occur and how you can go
about sustaining the CNM as everyday practice.
Re-evaluating your efforts
As highlighted earlier in the WOW Resource, it is very
important to re-evaluate your efforts to determine whether
the CNM project has resulted in positive outcomes for the
nurses and the patients. A CNM will not ‘fix’ everything
and there might be areas which require further discussion
and action which will not be directly related to the CNM.
Reevaluation should occur around six months to give the
nurses time to settle into the new CNM. The same strategies
should be used as for the initial evaluation so that the
results can be compared. After adding the new data for
the Nursing Teamwork Survey and Nursing Workforce
Satisfaction Survey you will be able to open Sheet 3
where you will find the data has been converted to graphs.
The graphs will compare the outcomes from the first and
second surveys.
You might like to compare your outcomes across the
different wards/units in the hospital. Or perhaps more
importantly showcase your achievements and share
your lessons learnt.
Sustaining the work
There are lots of changes in health and there are lots of
projects that commence and when the initial enthusiasm
dies down so does the action and everyone goes back to
the way it was. For a CNM, like any other initiative to be
sustained, it needs to become part of the culture or the
norm – the way things are done around here. This is
perhaps the hardest part of the project.
Not only have the process and outcome changed,
but the thinking and attitudes behind them are
fundamentally altered and the systems surrounding
them are transformed as well. In other words the
change has become an integrated or mainstream
way of working rather than something ‘added on’.
As a result, when you look at the process or outcome
one year from now or longer, you can see that at a
minimum it has not reverted to the old way or old
level of performance. Further, it has been able to
withstand challenge and variation; it has evolved
alongside other changes and perhaps has continued
to improve over time. Sustainability means holding
the gains and evolving as required – definitely not
going back.
NHS Institute for Innovation and Improvement (2005)
Link to www.institute.nhs.uk/sustainability
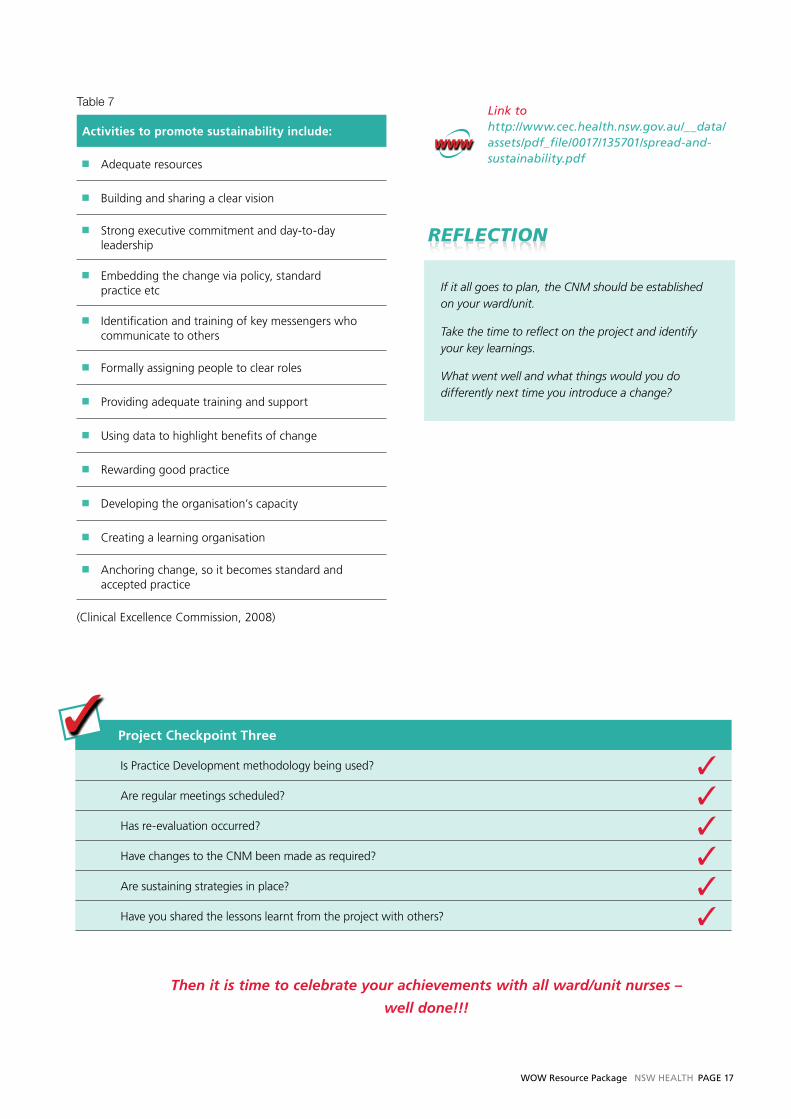
The Clinical Excellence Commission (CEC) suggests that
there are a number of key activities which can assist in
ensuring the sustainability of a project. As you read the
list you will realise that a lot of these activities have already
been instigated within the project if a Practice Development
approach is being used.
Implementing a CNM – What have we done?
SECTION 4
WOW Resource Package NSW HEAltH PAGE 17
Table 7
Activities to promote sustainability include:
n Adequate resources
n Building and sharing a clear vision
n Strong executive commitment and day-to-day leadership
n Embedding the change via policy, standard practice etc
n Identification and training of key messengers who communicate to others
n Formally assigning people to clear roles
n Providing adequate training and support
n Using data to highlight benefits of change
n Rewarding good practice
n Developing the organisation’s capacity
n Creating a learning organisation
n Anchoring change, so it becomes standard and accepted practice
(Clinical Excellence Commission, 2008)
Project Checkpoint Three
Is Practice Development methodology being used? 3Are regular meetings scheduled? 3Has re-evaluation occurred? 3Have changes to the CNM been made as required? 3Are sustaining strategies in place? 3Have you shared the lessons learnt from the project with others? 3
Then it is time to celebrate your achievements with all ward/unit nurses –
well done!!!
Link to http://www.cec.health.nsw.gov.au/__data/assets/pdf_file/0017/135701/spread-and-sustainability.pdf
If it all goes to plan, the CNM should be established on your ward/unit.
Take the time to reflect on the project and identify your key learnings.
What went well and what things would you do differently next time you introduce a change?

PaGe 18 NSW HealtH WOW Resource Package
Accountability: means that nurses must be prepared to
answer to others, such as health care consumers, their
nursing regulatory authority, employers and the public for
their decisions, actions, behaviours and the responsibilities
that are inherent in their roles. Accountability cannot be
delegated. The registered nurse who delegates an activity
to another person is accountable, not only for their
delegation decision, but also for monitoring the standard
of performance of the activity by the other person, and for
evaluating the outcomes of the delegation. Enrolled nurses
are accountable for making decisions about their own
practice and about what is within their own capacity and
scope of practice. See NMBA Decision-making Framework
for further information.
Allocation or assignment: involves asking another person
to care for one or more consumers on the assumption that
the required activities of consumer care are normally within
that person’s responsibility and scope of practice. Many of
the same factors regarding competence assessment and
supervision that are relevant to delegation also need to
be considered in relation to allocation/assignment.
Coaching: focuses on the skills and competencies required
for optimum performance to meet expectations. Coaching
approaches are predominantly facilitating in style using
challenging questions to enable the coachee to ‘grow’
from the experience.
Collaboration: is a process where two or more people
work together to realise shared goals. Collaborative
problem solving relies on sharing knowledge, learning,
and building consensus.
Competency: is the combination of skills, knowledge,
attitudes, values and abilities that underpin effective and/or
superior performance in a profession/occupational area.
Delegation: A delegation relationship exists when one
nurse delegates aspects of patient care, which they are
competent to perform and which they would normally
perform themselves, to a less experienced nurse.
The delegator retains accountability for the decision to
delegate and for monitoring outcomes. Delegation may be
either the: transfer of authority to a competent person to
perform a specific activity in a specific context or conferring
of authority to perform a specific activity in a specific
context on a competent person who does not have
autonomous authority to perform the activity.
Delegation is a two-way, multi-level activity, requiring a
rational decision-making and risk assessment process, and
the end point of delegation may come only after teaching
and competence assessment. To maintain a high standard
of care when delegating activities, the professional’s
responsibilities include: teaching, competence assessment,
providing guidance, assistance, support and clinically-
focussed supervision ensuring that the person to whom the
delegation is being made understands their accountability
and is willing to accept the delegation evaluation of
outcomes reflection on practice. See Decision Making
Framework.
Experience: as it is used in this resource, does not
necessarily refer to the length of time in a position, rather
it refers to a very active process of refining and changing
preconceived theories, notions and ideas when confronted
with actual situations (Benner, 1984). Some nurses will
progress to an expert in a relatively short period of time
while others may spend ten years on a ward without being
classified as expert. In addition, you do not need to be an
RN to be seen as an experienced nurse.
Responsibility: in nursing is the state of being answerable
for one’s performance according to the terms of reference
of the Code of Professional Conduct.
Supervision: in the CNM context is direct. Direct
supervision is when the supervisor is actually present and
personally observes, works with, guides and directs the
person who is being supervised.
APPENDIx 1
Glossary of terms

WOW Resource Package NSW HealtH PaGe 19
FurtherHelp
The following references which are available through CIAP
or assessable on the internet might be helpful in providing
some more information around CNMs. There are some
hospitals/wards/units in NSW where a CNM is working
well and you might like to seek out one of these areas
for support.
Teamwork
Biech, E. ed. (2008). The Pfeiffer Book of Successful Team-
building Tools, second edition. Pfeiffer: San Francisco.
Hansten R (2009) Field evidence for a bundle of best
bedside practices. The Health Care Manager 28(2) 11-116.
Kalisch, B.J., Weaver, S.J. & Salas, E. (2009). What does
nursing teamwork look like? A qualitative study.
Journal of Nursing Care Quality, Oct-Dec, 298-307.
Kalisch, B.J. & Lee, H. (2009). Nursing teamwork,
staff characteristics, work schedules and staffing.
Health Care Management Review, 34(4) 323-333.
Kalisch, B.J., Curley, M. & Stefanov, S. (2007).
An intervention to enhance nursing staff teamwork
and engagement. Journal of Nursing Administration,
37(2) 77-84.
Kalisch, B.J. & Begeny, S.M. (2005). Improving nursing
unit teamwork. Journal of Nursing Administration,
35(12) 550-556.
NHS Institute for Innovation and Improvement &
The Royal College of Nursing. (2007). Developing
and sustaining effective teams – Guides 1-8. Royal
College of Nursing: London.
DelegationandDecisionMaking
Nursing and Midwifery Board of Australia (2007).National
Framework for the Development of Decision-Making Tools
for Nursing and Midwifery Practice (2007). Available at:
http://www.anmc.org.au/userfiles/file/DMF%20
Framework%20Final+watermark.pdf
Nursing and Midwifery Board of Australia (2007).
Nursing Practice Decisions Summary Guide. Available at:
http://www.nursingmidwiferyboard.gov.au/Codes-and-
Guidelines.aspx
Hansten, R. & Washburn, M. (1996). Why don’t nurses
delegate? Journal of Nursing Administration, 26(12) 24-28.
Phoenix Bittner, N. & Gravlin, G. (2009). Critical thinking,
delegation and missed care in nursing practice.
Journal of Nursing Administration, 39(3) 142-146.
Standing, T.S. & Anthony, M.J. (2008). Delegation: what
it means to acute care nurses. Applied Nursing Research,
21(1) 8-14.
General
Benner, P. (1984). From novice to expert: excellence
and power in clinical nursing practice. Menlo Park:
Addison-Wesley.
NSW Health (2008) Profile of the nurses and midwives
workforce in NSW. Available at:
http://www.health.nsw.gov.au/pubs/2009/pdf/nursing_08.pdf
APPENDIx 2
Useful reading and references

PaGe 20 NSW HealtH WOW Resource Package
TeamRoles
Albani, R., Camp, C. & Culver, A. (2006) Celebrating
a partnership of enrolled nurse education and training
in NSW. (1986–2006). Sydney: TAFE NSW.
Nursing and Midwifery Board of Australia. National
Competency Standards for the Enrolled Nurse, (2002).
Available at: http://www.nursingmidwiferyboard.gov.au/
Codes-and-Guidelines.aspx
Nursing and Midwifery Board of Australia. National
Competency Standards for the Registered Nurse, (2006)
Available at: http://www.nursingmidwiferyboard.gov.au/
Codes-and-Guidelines.aspx
Australian Nursing Federation Competency Standards
for the Advanced Enrolled Nurse. Available at:
http://www.anf.org.au/pdf/Competency_Standards_
Advanced_EN.pdf
Blay, N. & Donoghue, J. (2007) Enrolled nurse skill
extension: metropolitan myth or rural reality?
Australian Journal of Advanced Nursing 24(3) 38-42.
Chaboyer, W., Wallis, M., Duffield, C., Courtney, M.,
Seaton, P., Holzhauser, K., Schluter, J. & Bost, N. (2008)
A comparison of activities undertaken by enrolled and
registered nurses on medical wards in Australia: an
observational study. International Journal of Nursing
Studies. 45 1274-1284.
Eagar, S., Cowin, L., Gregory, L. & Firtko, A. (2010)
Scope of practice conflict in nursing: a new war or just
the same battle? Contemporary Nurse 36(1-2) 86-95.
Gibson, T. & Heartfield, M. (2005) Australian enrolled
nurses have their say – Part 2: Scope of practice.
Contemporary Nurse 19(1-2) 126-136.
Milson-Hawke, S. & Higgins, I. (2004) The scope of
enrolled nurse practice: a grounded theory study.
Contemporary Nurse 17(1-2) 44-62.
NSW Health, 2010, PD 2010_059. Employment of
Assistants in Nursing (AIN) in NSW Health Acute Care.
Available at: http://www.health.nsw.gov.au/policies/
pd/2010/pdf/PD2010_059.pdf
NSW Health (2010) Assistants in Nursing working
in the acute care environment health service Health
Service Implementation Package. Available at:
http://www.health.nsw.gov.au/pubs/2010/pdf/ain_
acute_care.pdf
NSW Health Nursing and Midwifery Office (2009)
Enrolled Nurse – Critical Care Units Project Report.
Available at: http://www.health.nsw.gov.au/resources/
nursing/pdf/eval_report_april09_1.pdf
Queensland Health (2010) Enrolled Nurse (Advanced
Practice). Available at: http://www.health.qld.gov.au/
nursing/enrolled_advanced.asp
Sutherland-Fraser, S. (2007) PEPEN: Developing an
educational pathway for the enrolled nurse instrument
nurse in New South Wales. ACORN 20(1) 17-21.
Tranter, S., Westgarth, F. & White, G. (2010). The Scope
of Practice of the Haemodialysis Enrolled Nurse in NSW
Report. Available at http://www.health.nsw.gov.au/
resources/gmct/renal/pdf/moc_report_2009.pdf
WOW
Chavasse, J. (1981). From task assignment to patient
allocation a change evaluation. Journal of Advanced
Nursing, 6 137-145.
Cioffi, J. & Ferguson, L. (2009). Team nursing in acute
care settings; nurses’ experiences. Contemporary Nurse,
33(1) 2-12.
Fairbrother, G., Jones, A. & Rivas, K. (2010). Changing
model of nursing care from individual patient allocation
to team nursing in the acute inpatient environment.
Contemporary Nurse, 35(2) 202-220.
Fowler, J., Hardy, J. & Howarth, T. (2006). Trialing
collaborative nursing models of care: the impact of change.
Australian Journal of Advanced Nursing, 23(4) 40-46.
Gullick, J., Shepherd, M. & Ronald, T. (2004). The effects
of an organisational model on the standard of care.
Nursing Times, 100(10) 36-39.
Hayman, B., Wilkes, L. & Cioffi, J. (2008) Change process
during redesign of a model of nursing practice in a surgical
ward. Journal of Nursing Management, 16 257-265.

WOW Resource Package NSW HealtH PaGe 21
Makinen, A., Kivimaki, M., Elovanio, M. & Virtanen, M.
(2003). Organization of nursing care and stressful work
characteristics. Journal of Advanced Nursing, 43(2) 197-205.
Thomas, J. & Herrin, D. (2009). Care model transformation:
a necessity, not an option. Journal of Nursing Administration,
39(11) 453-456.
O’Connell, B., Duke, M., Bennett, P., Crawford, S. &
Korfiatis, V. (2006). Trials and tribulations of team-nursing.
Collegian, 13 (3) 11-17.
Tiederman, M.E., & Lockinland, S. (2004). Traditional
models of care delivery; what have we learned?
Journal of Nursing Administration, 34(6), 291-297.
Zinsmeister, LB. & Schafer, D. (2009) The exploration
of the lived experience of the graduate nurse making
the transition to registered nurse during the first year of
practice. Journal for Nurses in Staff Development.
25(1) 28-34.
EvaluationandProjectManagement
Aiken, LH., Clarke, SP., & Sloane, DM. (2002) Hospital
staffing, organization, and quality of care: cross-national
findings. Int J Qual Health Care 14:5-13.
Aiken, LH., Clarke, SP., Sloane, DM., Lake, E. & Cheney, T.
(2008) Effects of hospital care environment on patient
mortality and nurse outcomes. Journal of Nursing
Administration 38(5) 223-229.
Amos, M.A., Hu, J. & Herrick, C.A. (2005). The impact of
team building on communication and job satisfaction of
nursing staff. Journal for Nurses in Staff Development,
21(1) 10-16.
Bartram, T., Joiner, T. & Stanton, P. (2004) Factors affecting
the job stress and job satisfaction of Australian nurses:
implications for recruitment and retention. Contemporary
Nurse,17(3) 293-304.
Bureau of Health Information. (2010). Insights into care:
patients’ perspectives on NSW Public Hospitals. Available at:
http://www.bhi.nsw.gov.au/publications/iic-report
Cioffi, J. & Ferguson, L. (2009). Team nursing in acute care
settings; nurses’ experiences. Contemporary Nurse, 33(1) 2-12.
Clinical Excellence Commission (CEC) (2008). Enhancing
project spread and sustainability – A companion to the
‘Easy guide to clinical practice improvement. Sydney: CEC.
Available at: http://www.cec.health.nsw.gov.au/__data/
assets/pdf_file/0017/135701/spread-and-sustainability.pdf
Dougherty, M.B. & Larson, E.L. (2010). The Nurse-Nurse
Collaboration Scale. Journal of nursing Administration,
40(1) 17-25.
Duddle, M. & Boughton, M. Intraprofessional relations
in nursing. Journal of Advanced Nursing 59 (1) 29-37.
Fairbrother, G. (2010). Team-based versus patient
allocation systems in nursing: a comparative evaluation
and socio-cultural discussion. Unpublished thesis.
Fairbrother, G., Jones, A. & Rivas, K. (2009). Development
and validation of the Nursing Workplace Satisfaction
Questionnaire (NWSQ). Contemporary Nurse, 34(1) 10-18.
Kalisch, B.J., Lee, H. & Salas, E. (2010). The Development
and testing of the Nursing Teamwork Survey.
Nursing Research, 59(1) 42-50.
Kalisch, B.J (2009). Nurse and nurse assistant perceptions
of missed nursing care. Journal of Nursing Administration,
39(11) 485-493.
Heinemann, D., Lengacher, C.A., Vancott, M., Mabe,
P. & Swymer, S. (1996). Partners in patient care: measuring
the effects on patient satisfaction and other quality
indicators. Nursing Economics, 14(5) 276-285.
Makinen, A., Kivimaki, M., Elovainio., M, Virtanen,
M. & Bond, S. (2003). Organisation of nursing care as a
determinant of job satisfaction among hospital nurses.
Journal of Nursing Management, 11, 299-306.
NHS Institute for Innovation and Improvement, (2005)
Sustainability model and guide. Available at:
www.institute.nhs.uk/sustainability
Montalvo, I. (2007) The National Database of Nursing
Quality Indicators (NDNQI). The Online Journal of
Issues in Nursing 12(3) 1-11. Available at:
http://www.nursingworld.org/MainMenuCategories/
ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/
Volume122007/No3Sept07/NursingQualityIndicators.aspx

PaGe 22 NSW HealtH WOW Resource Package
Urden, L.D. & Roode, J.I. (1997). Work sampling: a decision
making tool for determining resource and work design.
Journal of Nursing Administration, 27(9) 34-41.
Vancott, M., Lengacher, C.A., Heinemann, D., Mabe, P.,
Swymer, S. & Bistritz, D. (1997). The use of focus groups to
assist in the design and implementation of a new nursing
practice model. Journal of Nursing Staff Development,
13(2) 83-87.
Walker, K., Donoghue, J. & Mitten-Lewis, S. (2007).
Measuring the impact of a team model of nursing
practice using work sampling. Australian Health Review,
13(1) p98-107.
Wu, M., Courtney, M. & Berger, G. (2000).
Models of nursing care: a comparative study of patient
satisfaction on two orthopaedic wards in Brisbane.
Australian Journal of Advanced Nursing, 17(4) 29-34.
PracticeDevelopment
Dewing J. (2008). Implications for nursing managers
from a systematic review of practice development.
Journal of Nursing Management, 2008, 16, 134–140.
Manley, K., McCormack, B. & Wilson, V. (editors) (2008)
International Practice Development in Nursing and
Healthcare. Blackwell.
McCormack, B. & McCance, TV. (2006). Development
of a framework for person-centred nursing. Journal of
Advanced Nursing 56(5): 472-9.
Pryor, J. & Buzio, A. (2010) Enhancing inpatient
rehabilitation through the engagement of patients
and nurses. Journal of Advanced Nursing 66(5),
978–987.
Tranter, S., Burns, T., Dobson, S., Graf, E., Ng, W. &
Martinez, Y. (2007). Practice Development in the
hospital haemodialysis unit: improving calcium and
phosphate management. Renal Society of Australasia
Journal 3(2) 61-64. Available at:
http://findarticles.com/p/articles/mi_6859/is_2_3/ai_
n28558883/?tag=content;col1

SHPN (NM) 110125