Embed Size (px)
Citation preview
1
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use PROCRIT safely and effectively. See full prescribing information for PROCRIT.
PROCRIT® (epoetin alfa) injection, for intravenous or subcutaneous useInitial U.S. Approval: 1989
WARNING: ESAs INCREASE THE RISK OF DEATH, MYOCARDIAL INFARCTION, STROKE, VENOUS THROMBOEMBOLISM, THROMBOSIS OF VASCULAR
ACCESS AND TUMOR PROGRESSION OR RECURRENCESee full prescribing information for complete boxed warning.
Chronic Kidney Disease:• In controlled trials, patients experienced greater risks for death,
seriousadversecardiovascularreactions,andstrokewhenadministerederythropoiesis-stimulating agents (ESAs) to target a hemoglobin level of greater than 11 g/dL (5.1).
• No trial has identified a hemoglobin target level, ESA dose, or dosingstrategythatdoesnotincreasetheserisks.
• UsethelowestPROCRITdosesufficienttoreducetheneedforredbloodcell (RBC) transfusions (5.1).
Cancer:• ESAs shortened overall survival and/or increased the risk of tumor
progression or recurrence in clinical studies of patients with breast, non-smallcelllung,headandneck,lymphoid,andcervicalcancers(Table2, 5.3).
• PrescribersandhospitalsmustenrollinandcomplywiththeESAAPPRISEOncology Program to prescribe and/or dispense PROCRIT to patients withcancer(5.2).
• UsethelowestdosetoavoidRBCtransfusions(2.4).• UseESAsonlyforanemiafrommyelosuppressivechemotherapy(1.5).• ESAs are not indicated for patients receivingmyelosuppressive chemo-
therapywhentheanticipatedoutcomeiscure(1.5).• Discontinuefollowingthecompletionofachemotherapycourse(2.4).Perisurgery:• Duetoincreasedriskofdeepvenousthrombosis(DVT),DVTprophylaxisis
recommended (5.1).
--------------------------------RECENT MAJOR CHANGES---------------------------------• DosageandAdministration:PatientsonCancer
Chemotherapy(2.4) 12/2013
--------------------------------INDICATIONS AND USAGE----------------------------------PROCRITisanerythropoiesis-stimulatingagent(ESA)indicatedfor:• Treatmentofanemiadueto - ChronicKidneyDisease(CKD)inpatientsondialysisandnotondialysis(1.1). - ZidovudineinHIV-infectedpatients(1.2). - The effects of concomitant myelosuppressive chemotherapy, and
upon initiation, there isaminimumof twoadditionalmonthsofplannedchemotherapy(1.3).
• Reduction of allogeneicRBC transfusions in patients undergoing elective,noncardiac,nonvascularsurgery(1.4).
LimitationsofUsePROCRIThasnotbeenshownto improvequalityof life, fatigue,orpatientwell-being(1.5).PROCRITisnotindicatedforuse:• In patients with cancer receiving hormonal agents, biologic products,
or radiotherapy, unless also receiving concomitant myelosuppressivechemotherapy(1.5).
• Inpatientswithcancerreceivingmyelosuppressivechemotherapywhentheanticipatedoutcomeiscure(1.5).
• In patients scheduled for surgery who are willing to donate autologousblood(1.5).
• Inpatientsundergoingcardiacorvascularsurgery(1.5).• As a substitute for RBC transfusions in patients who require immediate
correctionofanemia(1.5).
----------------------------DOSAGE AND ADMINISTRATION------------------------------• CKD Patients: Initial dose: 50 to 100 Units/kg 3 timesweekly (adults) and
50Units/kg3timesweekly(childrenondialysis).Individualizemaintenancedose.Intravenousrouterecommendedforpatientsonhemodialysis(2.2).
• Zidovudine-treatedHIV-infectedPatients:100Units/kg3timesweekly(2.3).• Cancer Patients on Chemotherapy: 40,000 Units weekly or 150 Units/kg
3 times weekly (adults); 600 Units/kg intravenously weekly (children≥5years)(2.4).
• SurgeryPatients:300Units/kgperdaydailyfor15daysor600Units/kgweekly(2.5).
----------------------------DOSAGE FORMS AND STRENGTHS---------------------------• Single-dosevial:2000,3000,4000,10,000,and40,000Units/1mL(3).• Multidosevialcontainingbenzylalcohol:20,000Units/2mLand20,000Units/
1mL(3).
----------------------------------CONTRAINDICATIONS------------------------------------• Uncontrolledhypertension(4).• Pure redcell aplasia (PRCA) that begins after treatmentwithPROCRITor
othererythropoietinproteindrugs(4).• SeriousallergicreactionstoPROCRIT(4).• Use of the multi-dose vials in neonates, infants, pregnant women, and
nursingmothers(4).
-----------------------------WARNINGS AND PRECAUTIONS-----------------------------• IncreasedMortality,Myocardial Infarction,Stroke,andThromboembolism:
UsingESAstotargetahemoglobin levelofgreaterthan11g/dL increasesthe risk of serious adverse cardiovascular reactions and has not beenshown toprovideadditional benefit (5.1 and 14.1).Usecaution in patientswithcoexistentcardiovasculardiseaseandstroke(5.1).
• Increased Mortality and/or Increased Risk of Tumor Progression orRecurrenceinPatientsWithCancer(5.2and5.3).
• Hypertension:Controlhypertensionprior to initiatingandduring treatmentwithPROCRIT(5.4).
• Seizures:PROCRITincreasestheriskforseizuresinpatientswithCKD(5.5).Increasemonitoringof thesepatients forchanges inseizure frequencyorpremonitorysymptoms(5.5).
• PRCA:IfsevereanemiaandlowreticulocytecountdevelopduringPROCRITtreatment,withholdPROCRITandevaluateforPRCA(5.7).
------------------------------------ADVERSE REACTIONS-----------------------------------• PatientswithCKD:Adversereactions in≥5%ofPROCRIT-treatedpatients
in clinical studies were hypertension, arthralgia, muscle spasm, pyrexia,dizziness, medical device malfunction, vascular occlusion, and upperrespiratorytractinfection(6.1).
• Zidovudine-treated HIV-infected Patients: Adverse reactions in ≥ 5% ofPROCRIT-treatedpatientsinclinicalstudieswerepyrexia,cough,rash,andinjectionsiteirritation(6.1).
• CancerPatientsonChemotherapy:Adversereactionsin≥5%ofPROCRIT-treated patients in clinical studies were nausea, vomiting, myalgia,arthralgia,stomatitis,cough,weightdecrease,leukopenia,bonepain,rash,hyperglycemia, insomnia, headache, depression, dysphagia, hypokalemia,andthrombosis(6.1).
• Surgery Patients: Adverse reactions in≥ 5% of PROCRIT-treated patientsinclinicalstudieswerenausea,vomiting,pruritus,headache,injectionsitepain,chills,deepveinthrombosis,cough,andhypertension(6.1).
To report SUSPECTED ADVERSE REACTIONS, contact Janssen Products, LP at 1-800-JANSSEN (1-800-526-7736) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
------------------------------USE IN SPECIFIC POPULATIONS-----------------------------• Pregnancy, nursingmothers, neonates, and infants: Use single-dose vials
onlyanddonotmixwithbenzylalcohol.Basedonanimaldata,PROCRITmaycausefetalharm(8.1,8.3,and8.4).
• PediatricUse:Safetyandeffectivenesshavenotbeenestablished inCKDpatientsundergoingdialysiswhoarelessthan1monthold,pediatricpatientswithcancerlessthan5yearsold,pediatricpatientswithCKDnotondialysis,andpediatricpatientswithHIVinfection(8.4).
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide. Revised: 12/2013
PROCRIT® (epoetin alfa)

2
FULL PRESCRIBING INFORMATION
WARNING: ESAs INCREASE THE RISK OF DEATH, MYOCARDIAL INFARCTION, STROKE, VENOUS THROMBOEMBOLISM, THROMBOSIS OF VASCULAR ACCESS AND TUMOR PROGRESSION OR RECURRENCEChronic Kidney Disease:• In controlled trials, patients experienced greater risks for death,
seriousadversecardiovascularreactions,andstrokewhenadministerederythropoiesis-stimulating agents (ESAs) to target a hemoglobin level of greater than 11 g/dL.
• No trial has identified a hemoglobin target level, ESA dose, or dosingstrategythatdoesnotincreasetheserisks.
• UsethelowestPROCRITdosesufficienttoreducetheneedforredbloodcell (RBC) transfusions [see Warnings and Precautions (5.1)].
Cancer: • ESAs shortened overall survival and/or increased the risk of tumor
progression or recurrence in clinical studies of patients with breast,non-smallcelllung,headandneck,lymphoid,andcervicalcancers[see Table 2, Warnings and Precautions (5.3)].
• Because of these risks, prescribers and hospitals must enroll in andcomply with the ESA APPRISE Oncology Program to prescribe and/ordispensePROCRITtopatientswithcancer.ToenrollintheESAAPPRISEOncologyProgram,visitwww.esa-apprise.comorcall1-866-284-8089 forfurther assistance [see Warnings and Precautions (5.2)].
• To decrease these risks, as well as the risk of serious cardiovascularandthromboembolicreactions,usethelowestdoseneededtoavoidRBCtransfusions [see Dosage and Administration (2.4)].
• Use ESAs only for anemia from myelosuppressive chemotherapy [see Indications and Usage (1.3)].
• ESAs are not indicated for patients receivingmyelosuppressive chemo-therapy when the anticipated outcome is cure [see Indications and Usage (1.5)].
• Discontinue following the completion of a chemotherapy course [see Dosage and Administration (2.4)].
Perisurgery: • DuetoincreasedriskofDeepVenousThrombosis(DVT),DVTprophylaxis
is recommended [see Dosage and Administration (2.5) and Warnings and Precautions (5.1)].
1 INDICATIONS AND USAGE1.1 Anemia Due to Chronic Kidney DiseasePROCRITisindicatedforthetreatmentofanemiaduetochronickidneydisease(CKD),includingpatientsondialysisandnotondialysistodecreasetheneedforredbloodcell(RBC)transfusion.1.2 Anemia Due to Zidovudine in HIV-infected PatientsPROCRITisindicatedforthetreatmentofanemiaduetozidovudineadministeredat≤4200mg/weekinHIV-infectedpatientswithendogenousserumerythropoietinlevelsof≤500mUnits/mL.1.3 Anemia Due to Chemotherapy in Patients With CancerPROCRIT is indicated for the treatment of anemia in patientswith non-myeloidmalignancieswhereanemiaisduetotheeffectofconcomitantmyelosuppressivechemotherapy,anduponinitiation,thereisaminimumoftwoadditionalmonthsofplannedchemotherapy.1.4 ReductionofAllogeneicRedBloodCellTransfusionsinPatientsUndergoingElective, Noncardiac, Nonvascular SurgeryPROCRITisindicatedtoreducetheneedforallogeneicRBCtransfusionsamongpatients with perioperative hemoglobin > 10 to≤ 13 g/dL who are at high riskfor perioperative blood loss from elective, noncardiac, nonvascular surgery.PROCRITisnotindicatedforpatientswhoarewillingtodonateautologousbloodpre-operatively.1.5 Limitations of Use PROCRIThasnotbeenshowntoimprovequalityoflife,fatigue,orpatientwell-being.PROCRITisnotindicatedforuse:• In patients with cancer receiving hormonal agents, biologic products,
or radiotherapy, unless also receiving concomitant myelosuppressivechemotherapy.
• Inpatientswithcancerreceivingmyelosuppressivechemotherapywhentheanticipatedoutcomeiscure.
• In patients scheduled for surgery who are willing to donate autologousblood.
• Inpatientsundergoingcardiacorvascularsurgery.• As a substitute for RBC transfusions in patients who require immediate
correctionofanemia[see Clinical Pharmacology (12.2)].
PROCRIT® (epoetin alfa)
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: ESAs INCREASE THE RISK OF DEATH, MYOCARDIAL INFARCTION, STROKE, VENOUS THROMBOEMBOLISM, THROMBOSIS OF VASCULAR ACCESS AND TUMOR PROGRESSION OR RECURRENCE1 INDICATIONS AND USAGE 1.1 AnemiaDuetoChronicKidneyDisease 1.2 AnemiaDuetoZidovudineinHIV-infectedPatients 1.3 AnemiaDuetoChemotherapyinPatientsWithCancer 1.4 ReductionofAllogeneicRedBloodCellTransfusionsinPatients
UndergoingElective,Noncardiac,NonvascularSurgery 1.5 LimitationsofUse2 DOSAGE AND ADMINISTRATION 2.1 EvaluationofIronStoresandNutritionalFactors 2.2 PatientswithChronicKidneyDisease 2.3 Zidovudine-treatedHIV-infectedPatients 2.4 PatientsonCancerChemotherapy 2.5 SurgeryPatients 2.6 PreparationandAdministration3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS 5.1 IncreasedMortality,MyocardialInfarction,Stroke,and
Thromboembolism 5.2 PrescribingandDistributionProgramforPROCRITinPatients
WithCancer 5.3 IncreasedMortalityand/orIncreasedRiskofTumorProgression
orRecurrenceinPatientsWithCancer 5.4 Hypertension 5.5 Seizures 5.6 LackorLossofHemoglobinResponsetoPROCRIT 5.7 PureRedCellAplasia 5.8 SeriousAllergicReactions
5.9 Albumin(Human) 5.10 DialysisManagement 5.11 LaboratoryMonitoring6 ADVERSE REACTIONS 6.1 ClinicalTrialExperience 6.2 PostmarketingExperience 6.3 Immunogenicity7 DRUG INTERACTIONS8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy 8.3 NursingMothers 8.4 PediatricUse 8.5 GeriatricUse10 OVERDOSAGE11 DESCRIPTION12 CLINICAL PHARMACOLOGY 12.1 MechanismofAction 12.2 Pharmacodynamics 12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis,Mutagenesis,ImpairmentofFertility 13.3 ReproductiveandDevelopmentalToxicology14 CLINICALSTUDIES 14.1 PatientsWithChronicKidneyDisease 14.2 Zidovudine-treatedPatientsWithHIVInfection 14.3 CancerPatientsonChemotherapy 14.4 SurgeryPatients16 HOW SUPPLIED/STORAGE AND HANDLING17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are notlisted.
PROCRIT® (epoetin alfa)

3
2 DOSAGE AND ADMINISTRATION2.1 Evaluation of Iron Stores and Nutritional FactorsEvaluatetheironstatusinallpatientsbeforeandduringtreatmentandmaintainironrepletion.Correctorexcludeothercausesofanemia(e.g.,vitamindeficiency,metabolic or chronic inflammatory conditions, bleeding, etc.) before initiatingPROCRIT[see Warnings and Precautions (5.11)].2.2 PatientswithChronicKidneyDiseaseIncontrolledtrials,patientsexperiencedgreaterrisksfordeath,seriousadversecardiovascular reactions, and stroke when administered erythropoiesis-stimulating agents (ESAs) to target a hemoglobin level of greater than 11 g/dL. No trialhas identifiedahemoglobin target level,ESAdose,ordosingstrategythatdoesnotincreasetheserisks.IndividualizedosingandusethelowestdoseofPROCRITsufficienttoreducetheneedforRBCtransfusions[see Warnings and Precautions (5.1)].Physiciansandpatientsshouldweighthepossiblebenefitsofdecreasingtransfusionsagainsttheincreasedrisksofdeathandotherseriouscardiovascular adverse events [see Boxed Warning and Clinical Studies (14)].
Forall patientswithCKD:Wheninitiatingoradjustingtherapy,monitorhemoglobinlevelsatleastweeklyuntil stable, thenmonitor at leastmonthly.When adjusting therapy considerhemoglobinrateofrise,rateofdecline,ESAresponsivenessandhemoglobinvariability.Asinglehemoglobinexcursionmaynotrequireadosingchange. ◦ Do not increase the dose more frequently than once every
4weeks.Decreasesindosecanoccurmorefrequently.Avoidfrequentdoseadjustments.
◦ If the hemoglobin rises rapidly (e.g., more than 1 g/dL in any2-weekperiod),reducethedoseofPROCRITby25%ormoreasneededtoreducerapidresponses.
◦ Forpatientswhodonotrespondadequately,ifthehemoglobinhasnotincreasedbymorethan1g/dLafter4weeksoftherapy,increasethedoseby25%.
◦ For patients who do not respond adequately over a 12-weekescalation period, increasing the PROCRIT dose further isunlikely to improve responseandmay increase risks.Use thelowestdosethatwillmaintainahemoglobin levelsufficient toreduce the need for RBC transfusions. Evaluate other causesof anemia. Discontinue PROCRIT if responsiveness does notimprove.
ForpatientswithCKDon dialysis: • Initiate PROCRIT treatment when the hemoglobin level is less than
10g/dL. • If the hemoglobin level approaches or exceeds 11 g/dL, reduce or
interruptthedoseofPROCRIT. • The recommended starting dose for adult patients is 50 to
100 Units/kg 3 times weekly intravenously or subcutaneously. Forpediatric patients, a starting dose of 50 Units/kg 3 times weeklyintravenously or subcutaneously is recommended. The intravenousrouteisrecommendedforpatientsonhemodialysis.
ForpatientswithCKDnot on dialysis: • ConsiderinitiatingPROCRITtreatmentonlywhenthehemoglobinlevel
islessthan10g/dLandthefollowingconsiderationsapply: ◦ The rate of hemoglobin decline indicates the likelihood of
requiringaRBCtransfusionand, ◦ Reducing the risk of alloimmunization and/or other RBC
transfusion-relatedrisksisagoal • Ifthehemoglobinlevelexceeds10g/dL,reduceorinterruptthedoseof
PROCRIT,andusethelowestdoseofPROCRITsufficienttoreducetheneedforRBCtransfusions.
• Therecommendedstartingdoseforadultpatientsis50to100Units/kg3timesweeklyintravenouslyorsubcutaneously.
Whentreatingpatientswhohavechronickidneydiseaseandcancer,physiciansshouldrefertoWarnings and Precautions (5.1 and 5.3).Refer patientswho self-administer PROCRIT to the Instructions forUse [see Patient Counseling Information (17)].
2.3 Zidovudine-treated HIV-infected PatientsStartingDoseThe recommended starting dose in adults is 100 Units/kg as an intravenous orsubcutaneousinjection3timesperweek.DoseAdjustment • Ifhemoglobindoesnotincreaseafter8weeksoftherapy,increasePROCRIT
dose by approximately 50 to 100 Units/kg at 4- to 8-week intervals untilhemoglobinreachesalevelneededtoavoidRBCtransfusionsor300Units/kg.
• Withhold PROCRIT if hemoglobin exceeds 12 g/dL. Resume therapy ata dose 25% below the previous dosewhen hemoglobin declines to lessthan11g/dL.
DiscontinuePROCRIT ifan increase inhemoglobin isnotachievedatadoseof300Units/kgfor8weeks.2.4 PatientsonCancerChemotherapyInitiate PROCRIT in patients on cancer chemotherapy only if the hemoglobin islessthan10g/dL,andifthereisaminimumoftwoadditionalmonthsofplannedchemotherapy.UsethelowestdoseofPROCRITnecessarytoavoidRBCtransfusions.
RecommendedStartingDoseAdults: • 150Units/kgsubcutaneously3timesperweekuntilcompletionofachemo-
therapycourseor • 40,000 Units subcutaneouslyweekly until completion of a chemotherapy
course.
PediatricPatients(5to18years): • 600 Units/kg intravenously weekly until completion of a chemotherapy
course.
DoseReductionReducedoseby25%if: • Hemoglobinincreasesgreaterthan1g/dLinany2-weekperiodor • HemoglobinreachesalevelneededtoavoidRBCtransfusion.
Withholddose if hemoglobinexceedsa level needed toavoidRBC transfusion.Reinitiateatadose25%belowthepreviousdosewhenhemoglobinapproachesalevelwhereRBCtransfusionsmayberequired.
DoseIncreaseAftertheinitial4weeksofPROCRITtherapy,ifhemoglobinincreasesbylessthan1g/dLandremainsbelow10g/dL,increasedoseto: • 300Units/kgthreetimesperweekinadultsor • 60,000Unitsweeklyinadults • 900Units/kg(maximum60,000Units)weeklyinchildren
After8weeksoftherapy,ifthereisnoresponseasmeasuredbyhemoglobinlevelsorifRBCtransfusionsarestillrequired,discontinuePROCRIT.2.5 Surgery PatientsTherecommendedPROCRITregimensare:• 300Units/kgperdaysubcutaneouslyfor15daystotal:administereddailyfor
10daysbeforesurgery,onthedayofsurgery,andfor4daysaftersurgery.• 600 Units/kg subcutaneously in 4 doses administered 21, 14, and 7 days
beforesurgeryandonthedayofsurgery.
Deep venous thrombosis prophylaxis is recommended during PROCRIT therapy[see Warnings and Precautions (5.1)].2.6 Preparation and Administration • Donotshake.DonotusePROCRITthathasbeenshakenorfrozen.• Protectvialsfromlight.• Parenteraldrugproductsshouldbeinspectedvisuallyforparticulatematter
and discoloration prior to administration. Do not use any vials exhibitingparticulatematterordiscoloration.
• Discard unused portions of PROCRIT in preservative-free vials. Do notre-enterpreservative-freevials.
• StoreunusedportionsofPROCRITinmultidosevialsat36°Fto46°F(2°Cto8°C).Discard21daysafterinitialentry.
• Donotdilute.Donotmixwithotherdrugsolutionsexcept foradmixingasdescribedbelow:
◦ Preservative-free PROCRIT from single-use vials may be admixedinasyringewithbacteriostatic0.9%sodiumchlorideinjection,USP,withbenzylalcohol0.9%(bacteriostaticsaline) ina1:1 ratiousingaseptictechniqueatthetimeofadministration.Risksareassociatedwith benzyl alcohol in neonates, infants, pregnant women, andnursingmothers[see Use in Specific Populations (8.1, 8.3, 8.4)].
3 DOSAGE FORMS AND STRENGTHSSingle-dosevials:2000,3000,4000,10,000,and40,000UnitsPROCRIT/1mLMultidose vials (contains benzyl alcohol): 20,000 Units PROCRIT /2 mL and20,000UnitsPROCRIT/1mL
4 CONTRAINDICATIONSPROCRITiscontraindicatedinpatientswith:• Uncontrolledhypertension[see Warnings and Precautions (5.4)]• Pure redcell aplasia (PRCA) that begins after treatmentwithPROCRITor
othererythropoietinproteindrugs[see Warnings and Precautions (5.7)]
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

4
• SeriousallergicreactionstoPROCRIT[see Warnings and Precautions (5.8)]PROCRITfrommultidosevialscontainsbenzylalcoholandiscontraindicatedin:• Neonates, infants, pregnantwomen, and nursingmothers. Benzyl alcohol
has been associated with serious adverse events and death, particularlyin pediatric patients.When therapywith PROCRIT is needed in neonatesand infants, use single-dose vials; donot admixwithbacteriostatic salinecontainingbenzylalcohol[see Use in Specific Populations (8.1, 8.3, 8.4)].
5 WARNINGS AND PRECAUTIONS5.1 IncreasedMortality,MyocardialInfarction,Stroke,andThromboembolism• In controlled clinical trials of patients with CKD comparing higher
hemoglobin targets (13 -14g/dL) to lower targets (9 -11.3g/dL),PROCRITandother ESAs increased the risk of death,myocardial infarction, stroke,congestiveheart failure, thrombosisofhemodialysisvascularaccess,andotherthromboemboliceventsinthehighertargetgroups.
• UsingESAstotargetahemoglobin levelofgreaterthan11g/dL increasesthe risk of serious adverse cardiovascular reactions and has not beenshowntoprovideadditionalbenefit[see Clinical Studies (14.1)].Usecautioninpatientswithcoexistentcardiovasculardiseaseandstroke[see Dosage and Administration (2.2)].PatientswithCKDandaninsufficienthemoglobinresponse to ESA therapy may be at even greater risk for cardiovascularreactions and mortality than other patients. A rate of hemoglobin rise ofgreaterthan1g/dLover2weeksmaycontributetotheserisks.
• Incontrolledclinicaltrialsofpatientswithcancer,PROCRITandotherESAsincreasedtherisksfordeathandseriousadversecardiovascularreactions.Theseadversereactionsincludedmyocardialinfarctionandstroke.
• In controlled clinical trials, ESAs increased the risk of death in patientsundergoingcoronaryarterybypassgraftsurgery(CABG)andtheriskofdeepvenousthrombosis(DVT)inpatientsundergoingorthopedicprocedures.
Thedesignandoverall resultsof the3 large trialscomparinghigherand lowerhemoglobintargetsareshowninTable1.
Table 1: Randomized Controlled Trials Showing Adverse CardiovascularOutcomes in Patients With CKD
Normal Hematocrit Study (NHS)
(N = 1265)
CHOIR(N=1432)
TREAT(N=4038)
Time Period of Trial 1993to1996 2003to2006 2004to2009
Population
CKDpatientsonhemodialysiswithcoexistingCHForCAD,hematocrit
30±3%onepoetinalfa
CKDpatientsnotondialysiswithhemoglobin<11g/dLnotpreviously
administeredepoetinalfa
CKDpatientsnotondialysiswithtypeIIdiabetes,hemoglobin
≤11g/dL
Hemoglobin Target;Highervs.Lower
(g/dL)14.0vs.10.0 13.5vs.11.3 13.0vs.≥9.0
Median (Q1, Q3)Achieved
Hemoglobin level (g/dL)
12.6(11.6,13.3)vs.10.3(10.0,10.7)
13.0(12.2,13.4)vs.11.4(11.1,11.6)
12.5(12.0,12.8)vs.10.6(9.9,11.3)
Primary EndpointAll-causemortalityornon-fatalMI
All-causemortality,MI,
hospitalizationforCHF,orstroke
All-causemortality,MI,myocardialischemia,heart
failure,andstrokeHazardRatioorRelativeRisk
(95% CI)1.28(1.06-1.56) 1.34(1.03-1.74) 1.05(0.94-1.17)
Adverse Outcome for Higher
Target Group
All-causemortality
All-causemortality Stroke
HazardRatioorRelativeRisk
(95% CI)1.27(1.04-1.54) 1.48(0.97-2.27) 1.92(1.38-2.68)
PatientswithChronicKidneyDiseaseNormalHematocritStudy(NHS):Aprospective,randomized,open-labelstudyof1265patientswithchronickidneydiseaseondialysiswithdocumentedevidenceof congestive heart failure or ischemic heart diseasewas designed to test thehypothesisthatahighertargethematocrit(Hct)wouldresultinimprovedoutcomescompared with a lower target Hct. In this study, patients were randomized toepoetinalfatreatmenttargetedtoamaintenancehemoglobinofeither14±1g/dLor10±1g/dL.Thetrialwasterminatedearlywithadversesafetyfindingsofhighermortalityinthehighhematocrittargetgroup.Highermortality(35%vs.29%)wasobservedfor thepatientsrandomizedtoatargethemoglobinof14g/dLthanfor
thepatientsrandomizedtoatargethemoglobinof10g/dL.Forall-causemortality,theHR=1.27;95%CI(1.04,1.54);p=0.018.Theincidenceofnonfatalmyocardialinfarction, vascular access thrombosis, and other thrombotic events was alsohigherinthegrouprandomizedtoatargethemoglobinof14g/dL.CHOIR: A randomized, prospective trial, 1432 patientswith anemia due to CKDwhowerenotundergoingdialysisandwhohadnotpreviouslyreceivedepoetinalfatherapywererandomizedtoepoetinalfatreatmenttargetingamaintenancehemoglobinconcentrationofeither13.5g/dLor11.3g/dL.Thetrialwasterminatedearlywithadversesafetyfindings.Amajorcardiovascularevent(death,myocardialinfarction,stroke,orhospitalizationforcongestiveheartfailure)occurredin125ofthe715patients(18%)inthehigherhemoglobingroupcomparedto97ofthe717patients(14%)inthelowerhemoglobingroup[hazardratio(HR)1.34,95%CI:1.03,1.74;p=0.03].TREAT:Arandomized,double-blind,placebo-controlled,prospective trialof4038patientswith:CKDnotondialysis(eGFRof20–60mL/min),anemia(hemoglobinlevels ≤ 11 g/dL), and type 2 diabetes mellitus, patients were randomized toreceiveeitherdarbepoetinalfatreatmentoramatchingplacebo.Placebogrouppatientsalsoreceiveddarbepoetinalfawhentheirhemoglobinlevelswerebelow9g/dL.The trialobjectiveswere todemonstrate thebenefitofdarbepoetinalfatreatmentoftheanemiatoatargethemoglobinlevelof13g/dL,whencomparedtoa“placebo”group,byreducingtheoccurrenceofeitheroftwoprimaryendpoints:(1) a composite cardiovascular endpoint of all-cause mortality or a specifiedcardiovascularevent(myocardialischemia,CHF,MI,andCVA)or(2)acompositerenalendpointofall-causemortalityorprogressiontoendstagerenaldisease.Theoverallrisksforeachofthetwoprimaryendpoints(thecardiovascularcompositeandtherenalcomposite)werenotreducedwithdarbepoetinalfatreatment(seeTable1),buttheriskofstrokewasincreasednearlytwo-fold inthedarbepoetinalfa-treatedgroupversustheplacebogroup:annualizedstrokerate2.1%vs.1.1%,respectively,HR1.92;95%CI:1.38,2.68;p<0.001.Therelativeriskofstrokewasparticularlyhighinpatientswithapriorstroke:annualizedstrokerate5.2%inthedarbepoetinalfa-treatedgroupand1.9% in theplacebogroup,HR3.07;95%CI:1.44, 6.54. Also, among darbepoetin alfa-treated subjectswith a past history ofcancer,thereweremoredeathsduetoallcausesandmoredeathsadjudicatedasduetocancer,incomparisonwiththecontrolgroup.
PatientswithCancerAn increased incidence of thromboembolic reactions, some serious and life-threatening,occurredinpatientswithcancertreatedwithESAs.In a randomized, placebo-controlled study (Study 1 in Table 2 [see Warnings and Precautions (5.3)]) of 939 women with metastatic breast cancer receivingchemotherapy,patientsreceivedeitherweeklyepoetinalfaorplaceboforuptoayear.Thisstudywasdesignedtoshowthatsurvivalwassuperiorwhenepoetinalfawas administered to prevent anemia (maintain hemoglobin levels between12and14g/dLorhematocritbetween36%and42%).Thisstudywasterminatedprematurely when interim results demonstrated a higher mortality at 4 months(8.7%vs.3.4%)andahigherrateoffatalthromboticreactions(1.1%vs.0.2%)inthefirst4monthsofthestudyamongpatientstreatedwithepoetinalfa.BasedonKaplan-Meierestimates, at the timeof study termination, the 12-month survivalwaslowerintheepoetinalfagroupthanintheplacebogroup(70%vs.76%;HR1.37,95%CI:1.07,1.75;p=0.012).
PatientsHavingSurgeryAn increased incidence of deep venous thrombosis (DVT) in patients receivingepoetinalfaundergoingsurgicalorthopedicprocedureswasdemonstrated [see Adverse Reactions (6.1)]. In a randomized, controlled study, 680 adult patients,not receivingprophylacticanticoagulationandundergoingspinal surgery,wererandomized to 4 doses of 600 Units/kg epoetin alfa (7, 14, and 21 days beforesurgery,andthedayofsurgery)andstandardofcare(SOC)treatment(n=340)or toSOCtreatmentalone(n=340).Ahigher incidenceofDVTs,determinedbyeither color flow duplex imaging or by clinical symptoms,was observed in theepoetin alfa group (16 [4.7%] patients) comparedwith the SOC group (7 [2.1%]patients).Inadditiontothe23patientswithDVTsincludedintheprimaryanalysis,19[2.8%]patients(n=680)experienced1otherthrombovascularevent(TVE)each(12[3.5%]intheepoetinalfagroupand7[2.1%]intheSOCgroup).Deepvenousthrombosis prophylaxis is strongly recommended when ESAs are used for thereduction of allogeneic RBC transfusions in surgical patients [see Dosage and Administration (2.5)].Increased mortality was observed in a randomized, placebo-controlled studyof PROCRIT in adult patients who were undergoing CABG surgery (7 deathsin 126 patients randomized to PROCRIT versus no deaths among 56 patientsreceivingplacebo).Fourofthesedeathsoccurredduringtheperiodofstudydrugadministrationandall4deathswereassociatedwiththromboticevents.5.2 Prescribing and Distribution Program for PROCRIT in Patients With CancerInordertoprescribeand/ordispensePROCRITtopatientswithcancerandanemiadue to myelosuppressive chemotherapy, prescribers and hospitals must enrollin and comply with the ESA APPRISE Oncology Program requirements. Toenroll, visitwww.esa-apprise.com or call 1-866-284-8089 for further assistance.Additionally, prior to each new course of PROCRIT in patients with cancer,prescribersandpatientsmustprovidewrittenacknowledgmentofadiscussionoftherisksofPROCRIT.
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)
5
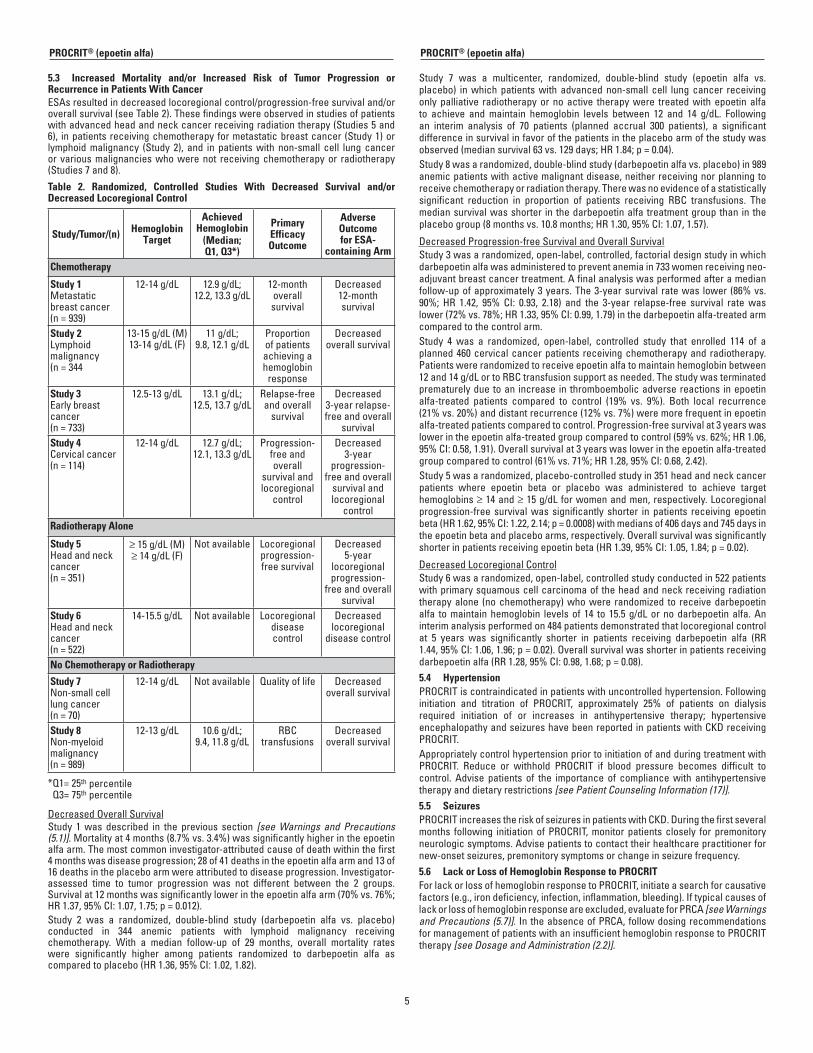
5.3 Increased Mortality and/or Increased Risk of Tumor Progression orRecurrence in Patients With CancerESAsresultedindecreasedlocoregionalcontrol/progression-freesurvivaland/oroverallsurvival(seeTable2).Thesefindingswereobservedinstudiesofpatientswithadvancedheadandneckcancerreceivingradiationtherapy(Studies5and6), inpatientsreceivingchemotherapyformetastaticbreastcancer(Study1)orlymphoidmalignancy (Study 2), and in patientswith non-small cell lungcanceror variousmalignancieswhowerenot receivingchemotherapyor radiotherapy(Studies7and8).
Table 2. Randomized, Controlled Studies With Decreased Survival and/orDecreased Locoregional Control
Study/Tumor/(n) Hemoglobin Target
Achieved Hemoglobin
(Median; Q1, Q3*)
Primary Efficacy Outcome
Adverse Outcome for ESA-
containing ArmChemotherapy
Study 1Metastaticbreastcancer(n=939)
12-14g/dL 12.9g/dL;12.2,13.3g/dL
12-monthoverallsurvival
Decreased12-monthsurvival
Study 2Lymphoidmalignancy(n=344
13-15g/dL(M)13-14g/dL(F)
11g/dL;9.8,12.1g/dL
Proportionofpatientsachievingahemoglobinresponse
Decreasedoverallsurvival
Study 3Earlybreastcancer(n=733)
12.5-13g/dL 13.1g/dL;12.5,13.7g/dL
Relapse-freeandoverallsurvival
Decreased3-yearrelapse-freeandoverall
survivalStudy4Cervicalcancer(n=114)
12-14g/dL 12.7g/dL;12.1,13.3g/dL
Progression-freeandoverall
survivalandlocoregional
control
Decreased3-year
progression-freeandoverallsurvivalandlocoregional
controlRadiotherapy Alone
Study 5Headandneckcancer(n=351)
≥15g/dL(M)≥14g/dL(F)
Notavailable Locoregionalprogression-freesurvival
Decreased5-year
locoregionalprogression-
freeandoverallsurvival
Study 6Headandneckcancer(n=522)
14-15.5g/dL Notavailable Locoregionaldiseasecontrol
Decreasedlocoregional
diseasecontrol
No Chemotherapy or Radiotherapy
Study 7Non-smallcelllungcancer(n=70)
12-14g/dL Notavailable Qualityoflife Decreasedoverallsurvival
Study 8Non-myeloidmalignancy(n=989)
12-13g/dL 10.6g/dL;9.4,11.8g/dL
RBCtransfusions
Decreasedoverallsurvival
*Q1=25thpercentileQ3=75thpercentile
DecreasedOverallSurvivalStudy 1was described in the previous section [see Warnings and Precautions (5.1)].Mortalityat4months(8.7%vs.3.4%)wassignificantlyhigherintheepoetinalfaarm.Themostcommoninvestigator-attributedcauseofdeathwithinthefirst4monthswasdiseaseprogression;28of41deathsintheepoetinalfaarmand13of16deathsintheplaceboarmwereattributedtodiseaseprogression.Investigator-assessed time to tumor progression was not different between the 2 groups.Survivalat12monthswassignificantlylowerintheepoetinalfaarm(70%vs.76%;HR1.37,95%CI:1.07,1.75;p=0.012).Study 2 was a randomized, double-blind study (darbepoetin alfa vs. placebo)conducted in 344 anemic patients with lymphoid malignancy receivingchemotherapy. With a median follow-up of 29 months, overall mortality rateswere significantly higher among patients randomized to darbepoetin alfa ascomparedtoplacebo(HR1.36,95%CI:1.02,1.82).
Study 7 was a multicenter, randomized, double-blind study (epoetin alfa vs.placebo) inwhichpatientswithadvancednon-small cell lungcancer receivingonlypalliative radiotherapyornoactive therapywere treatedwithepoetinalfato achieve andmaintain hemoglobin levels between 12 and 14 g/dL. Followingan interim analysis of 70 patients (planned accrual 300 patients), a significantdifferenceinsurvivalinfavorofthepatientsintheplaceboarmofthestudywasobserved(mediansurvival63vs.129days;HR1.84;p=0.04).Study8wasarandomized,double-blindstudy(darbepoetinalfavs.placebo)in989anemicpatientswithactivemalignantdisease,neitherreceivingnorplanningtoreceivechemotherapyorradiationtherapy.Therewasnoevidenceofastatisticallysignificant reduction in proportion of patients receiving RBC transfusions. Themediansurvivalwasshorter inthedarbepoetinalfatreatmentgroupthanintheplacebogroup(8monthsvs.10.8months;HR1.30,95%CI:1.07,1.57).
DecreasedProgression-freeSurvivalandOverallSurvivalStudy3wasarandomized,open-label,controlled,factorialdesignstudyinwhichdarbepoetinalfawasadministeredtopreventanemiain733womenreceivingneo-adjuvantbreastcancertreatment.Afinalanalysiswasperformedafteramedianfollow-upofapproximately3years.The3-yearsurvivalratewas lower(86%vs.90%; HR 1.42, 95% CI: 0.93, 2.18) and the 3-year relapse-free survival ratewaslower(72%vs.78%;HR1.33,95%CI:0.99,1.79)inthedarbepoetinalfa-treatedarmcomparedtothecontrolarm.Study 4 was a randomized, open-label, controlled study that enrolled 114 of aplanned460cervicalcancerpatientsreceivingchemotherapyandradiotherapy.Patientswererandomizedtoreceiveepoetinalfatomaintainhemoglobinbetween12and14g/dLortoRBCtransfusionsupportasneeded.Thestudywasterminatedprematurelyduetoan increase inthromboembolicadversereactions inepoetinalfa-treated patients compared to control (19% vs. 9%). Both local recurrence(21%vs.20%)anddistantrecurrence(12%vs.7%)weremorefrequentinepoetinalfa-treatedpatientscomparedtocontrol.Progression-freesurvivalat3yearswaslowerintheepoetinalfa-treatedgroupcomparedtocontrol(59%vs.62%;HR1.06,95%CI:0.58,1.91).Overallsurvivalat3yearswaslowerintheepoetinalfa-treatedgroupcomparedtocontrol(61%vs.71%;HR1.28,95%CI:0.68,2.42).Study5wasarandomized,placebo-controlledstudyin351headandneckcancerpatients where epoetin beta or placebo was administered to achieve targethemoglobins≥14and≥15g/dLforwomenandmen,respectively.Locoregionalprogression-free survivalwas significantly shorter in patients receivingepoetinbeta(HR1.62,95%CI:1.22,2.14;p=0.0008)withmediansof406daysand745daysintheepoetinbetaandplaceboarms,respectively.Overallsurvivalwassignificantlyshorterinpatientsreceivingepoetinbeta(HR1.39,95%CI:1.05,1.84;p=0.02).
DecreasedLocoregionalControlStudy6wasarandomized,open-label,controlledstudyconductedin522patientswithprimarysquamouscellcarcinomaoftheheadandneckreceivingradiationtherapyalone (nochemotherapy)whowere randomized to receivedarbepoetinalfa tomaintainhemoglobin levelsof 14 to15.5g/dLornodarbepoetinalfa.Aninterimanalysisperformedon484patientsdemonstratedthatlocoregionalcontrolat 5 years was significantly shorter in patients receiving darbepoetin alfa (RR1.44,95%CI:1.06,1.96;p=0.02).Overallsurvivalwasshorterinpatientsreceivingdarbepoetinalfa(RR1.28,95%CI:0.98,1.68;p=0.08).5.4 HypertensionPROCRITiscontraindicatedinpatientswithuncontrolledhypertension.Followinginitiation and titration of PROCRIT, approximately 25% of patients on dialysisrequired initiation of or increases in antihypertensive therapy; hypertensiveencephalopathyandseizureshavebeenreportedinpatientswithCKDreceivingPROCRIT.AppropriatelycontrolhypertensionpriortoinitiationofandduringtreatmentwithPROCRIT. Reduce or withhold PROCRIT if blood pressure becomes difficult tocontrol. Advise patients of the importance of compliancewith antihypertensivetherapyanddietaryrestrictions[see Patient Counseling Information (17)].5.5 SeizuresPROCRITincreasestheriskofseizuresinpatientswithCKD.Duringthefirstseveralmonths following initiationofPROCRIT,monitorpatientsclosely forpremonitoryneurologicsymptoms.Advisepatientstocontacttheirhealthcarepractitionerfornew-onsetseizures,premonitorysymptomsorchangeinseizurefrequency.5.6 LackorLossofHemoglobinResponsetoPROCRITForlackorlossofhemoglobinresponsetoPROCRIT,initiateasearchforcausativefactors(e.g.,irondeficiency,infection,inflammation,bleeding).Iftypicalcausesoflackorlossofhemoglobinresponseareexcluded,evaluateforPRCA[see Warnings and Precautions (5.7)]. IntheabsenceofPRCA,followdosingrecommendationsformanagementofpatientswithaninsufficienthemoglobinresponsetoPROCRITtherapy[see Dosage and Administration (2.2)].
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

6
5.7 Pure Red Cell AplasiaCasesofPRCAandofsevereanemia,withorwithoutothercytopeniasthatarisefollowingthedevelopmentofneutralizingantibodiestoerythropoietinhavebeenreportedinpatientstreatedwithPROCRIT.ThishasbeenreportedpredominantlyinpatientswithCKDreceivingESAsbysubcutaneousadministration.PRCAhasalsobeen reported inpatients receivingESAs foranemia related tohepatitisCtreatment(anindicationforwhichPROCRITisnotapproved).If severe anemia and low reticulocyte count develop during treatment withPROCRIT,withholdPROCRITandevaluatepatients forneutralizingantibodies toerythropoietin.ContactJanssenProducts,LPat1-800-JANSSEN(1-800-526-7736)toperformassaysforbindingandneutralizingantibodies.PermanentlydiscontinuePROCRITinpatientswhodevelopPRCAfollowingtreatmentwithPROCRITorothererythropoietinproteindrugs.DonotswitchpatientstootherESAs.5.8 Serious Allergic ReactionsSerious allergic reactions, including anaphylactic reactions, angioedema,bronchospasm,skinrash,andurticariamayoccurwithPROCRIT.ImmediatelyandpermanentlydiscontinuePROCRITandadministerappropriatetherapyifaseriousallergicoranaphylacticreactionoccurs.5.9 Albumin (Human)PROCRIT contains albumin, a derivative of human blood [see Description (11)].Based on effective donor screening and product manufacturing processes, itcarriesanextremelyremoteriskfortransmissionofviraldiseases.Atheoreticalrisk for transmission of Creutzfeldt-Jakob disease (CJD) also is consideredextremely remote.Nocasesof transmissionofviraldiseasesorCJDhaveeverbeenidentifiedforalbumin.5.10 Dialysis ManagementPatientsmayrequireadjustmentsintheirdialysisprescriptionsafterinitiationofPROCRIT.PatientsreceivingPROCRITmayrequireincreasedanticoagulationwithheparintopreventclottingoftheextracorporealcircuitduringhemodialysis.5.11 Laboratory Monitoring Evaluate transferrin saturation and serum ferritin prior to and during PROCRITtreatment.Administersupplementalirontherapywhenserumferritinislessthan100mcg/Lorwhenserumtransferrinsaturationislessthan20%[see Dosage and Administration (2.1)].ThemajorityofpatientswithCKDwillrequiresupplementaliron during the course of ESA therapy. Following initiation of therapy and aftereachdoseadjustment,monitorhemoglobinweeklyuntil thehemoglobin level isstableandsufficienttominimizetheneedforRBCtransfusion.
6 ADVERSE REACTIONSThefollowingseriousadversereactionsarediscussed ingreaterdetail inothersectionsofthelabel:• IncreasedMortality,Myocardial Infarction, Stroke, and Thromboembolism
[see Warnings and Precautions (5.1)]• Increasedmortalityand/orincreasedriskoftumorprogressionorrecurrence
inPatientsWithCancer[see Warnings and Precautions (5.3)]• Hypertension[see Warnings and Precautions (5.4)]• Seizures[see Warnings and Precautions (5.5)]• PRCA[see Warnings and Precautions (5.7)]• Seriousallergicreactions[see Warnings and Precautions (5.8)]
6.1 ClinicalTrialExperienceBecauseclinical trials areconductedunderwidely varyingconditions, adversereactionratesobservedintheclinicaltrialsofadrugcannotbedirectlycomparedtoratesintheclinicaltrialsofotherdrugsandmaynotreflecttheratesobservedinpractice.
PatientswithChronicKidneyDiseaseAdult PatientsThreedouble-blind,placebo-controlledstudies,including244patientswithCKDondialysis,wereusedtoidentifytheadversereactionstoPROCRIT.Inthesestudies,themeanageofpatientswas48years(range:20to80years).Onehundredandthirty-three(55%)patientsweremen.Theracialdistributionwasasfollows:177(73%) patientswerewhite, 48 (20%) patientswere black, 4 (2%) patientswereAsian,12(5%)patientswereother,andracialinformationwasmissingfor3(1%)patients.Two double-blind, placebo-controlled studies, including 210 patients with CKDnotondialysis,wereusedtoidentifytheadversereactionstoPROCRIT.Inthesestudies,themeanageofpatientswas57years(range:24to79years).Onehundredandtwenty-one(58%)patientsweremen.Theracialdistributionwasasfollows:164(78%)patientswerewhite,38(18%)patientswereblack,3(1%)patientswereAsian,3(1%)patientswereother,andracial informationwasmissingfor2(1%)patients.The adverse reactions with a reported incidence of ≥ 5% in PROCRIT-treatedpatientsand thatoccurredat a≥ 1%higher frequency than inplacebo-treatedpatientsareshowninthetablebelow:
Table 3. Adverse Reactions in Patients With CKD on Dialysis
Adverse Reaction PROCRIT-treated Patients(n=148)
Placebo-treated Patients(n = 96)
Hypertension 27.7% 12.5%
Arthralgia 16.2% 3.1%
Musclespasm 7.4% 6.3%
Pyrexia 10.1% 8.3%
Dizziness 9.5% 8.3%
MedicalDeviceMalfunction(artificialkidneyclottingduringdialysis)
8.1% 4.2%
VascularOcclusion(vascularaccessthrombosis)
8.1% 2.1%
Upperrespiratorytractinfection 6.8% 5.2%
Anadditionalseriousadversereactionthatoccurred in lessthan5%ofepoetinalfa-treated dialysis patients and greater than placebo was thrombosis (2.7%PROCRITand1%placebo)[see Warnings and Precautions (5.1)].The adverse reactions with a reported incidence of ≥ 5% in PROCRIT-treatedpatientsand thatoccurredat a≥ 1%higher frequency than inplacebo-treatedpatientsareshowninthetablebelow:
Table4.AdverseReactionsinPatientsWithCKDNotonDialysis
Adverse Reactions PROCRIT-treated Patients(n = 131)
Placebo-treated Patients(n = 79)
Hypertension 13.7% 10.1%
Arthralgia 12.2% 7.6%
Additionalseriousadversereactionsthatoccurredinlessthan5%ofepoetinalfa-treatedpatients not ondialysis andgreater thanplacebowereerythema (0.8%PROCRIT and 0% placebo) and myocardial infarction (0.8% PROCRIT and 0%placebo)[see Warnings and Precautions (5.1)].
Pediatric Patients InpediatricpatientswithCKDondialysis, thepatternofadversereactionswassimilartothatfoundinadults.
Zidovudine-treatedHIV-infectedPatientsAtotalof297zidovudine-treatedHIV-infectedpatientswerestudiedin4placebo-controlledstudies.Atotalof144(48%)patientswererandomlyassignedtoreceivePROCRIT and 153 (52%) patients were randomly assigned to receive placebo.PROCRITwasadministeredatdosesbetween100and200Units/kg3timesweeklysubcutaneouslyforupto12weeks.ForthecombinedPROCRITtreatmentgroups,atotalof141(98%)menand3(2%)womenbetweentheagesof24and64yearswereenrolled.TheracialdistributionofthecombinedPROCRITtreatmentgroupswasasfollows:129(90%)white,8(6%)black,1(1%)Asian,and6(4%)other.In double-blind, placebo-controlled studies of 3 months duration involvingapproximately 300 zidovudine-treated HIV-infected patients, adverse reactionswithanincidenceof≥1%inpatientstreatedwithPROCRITwere:
Table 5. Adverse Reactions in Zidovudine-treated HIV-infected Patients
Adverse Reaction PROCRIT(n=144)
Placebo(n = 153)
Pyrexia 42% 34%
Cough 26% 14%
Rash 19% 7%
Injectionsiteirritation 7% 4%
Urticaria 3% 1%
Respiratorytractcongestion 1% Notreported
Pulmonaryembolism 1% Notreported
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

7
CancerPatientsonChemotherapyThe data belowwere obtained in Study C1, a 16-week, double-blind, placebo-controlledstudythatenrolled344patientswithanemiasecondarytochemotherapy.Therewere333patientswhowereevaluableforsafety;168of174patients(97%)randomized to PROCRIT received at least 1 dose of study drug, and 165 of 170patients (97%) randomized toplacebo receivedat least1placebodose.For theonceweekly PROCRIT-treatment group, a total of 76men (45%) and 92women(55%)betweentheagesof20and88yearsweretreated.TheracialdistributionofthePROCRIT-treatmentgroupwas158white(94%)and10black(6%).PROCRITwasadministeredonceweeklyforanaverageof13weeksatadoseof20,000to60,000IUsubcutaneously(meanweeklydosewas49,000IU).The adverse reactions with a reported incidence of ≥ 5% in PROCRIT-treatedpatientsthatoccurredatahigherfrequencythaninplacebo-treatedpatientsareshowninthetablebelow:
Table 6. Adverse Reactions in Cancer Patients
Adverse Reaction PROCRIT(n = 168)
Placebo(n = 165)
Nausea 35% 30%
Vomiting 20% 16%
Myalgia 10% 5%
Arthralgia 10% 6%
Stomatitis 10% 8%
Cough 9% 7%
Weightdecrease 9% 5%
Leukopenia 8% 7%
Bonepain 7% 4%
Rash 7% 5%
Hyperglycemia 6% 4%
Insomnia 6% 2%
Headache 5% 4%
Depression 5% 4%
Dysphagia 5% 2%
Hypokalemia 5% 3%
Thrombosis 5% 3%
SurgeryPatientsFour hundred sixty-one patients undergoing major orthopedic surgery werestudied in a placebo-controlled study (S1) and a comparative dosing study(2dosingregimens,S2).Atotalof358patientswererandomlyassignedtoreceivePROCRIT and 103 (22%) patients were randomly assigned to receive placebo.PROCRITwasadministereddailyatadoseof100to300IU/kgsubcutaneouslyfor15daysorat600IU/kgonceweeklyfor4weeks.For thecombinedPROCRIT treatmentgroups,a total of 90 (25%)and268 (75%)womenbetweentheagesof29and89yearswereenrolled.Theracialdistributionof thecombinedPROCRITtreatmentgroupswasasfollows:288(80%)white,64(18%)black,1(<1%)Asian,and5(1%)other.The adverse reactions with a reported incidence of ≥ 1% in PROCRIT-treatedpatientsthatoccurredatahigherfrequencythaninplacebo-treatedpatientsareshowninthetablebelow:
Table 7. Adverse Reactions in Surgery Patients
Adverse Reaction Study S1 Study S2
PROCRIT300U/kg
PROCRIT100U/kg
Placebo 600U/kgx4weeks
300U/kgx15 days
(n = 112)a (n = 101)a (n = 103)a (n = 73)b (n = 72)b
Nausea 47% 43% 45% 45% 56%
Vomiting 21% 12% 14% 19% 28%
Pruritus 16% 16% 14% 12% 21%
Headache 13% 11% 9% 10% 18%
Injectionsitepain 13% 9% 8% 12% 11%
Chills 7% 4% 1% 1% 0%
Adverse Reaction Study S1 Study S2
PROCRIT300U/kg
PROCRIT100U/kg
Placebo 600U/kgx4weeks
300U/kgx15 days
(n = 112)a (n = 101)a (n = 103)a (n = 73)b (n = 72)b
Deepveinthrombosis
6% 3% 3% 0%c 0%c
Cough 5% 4% 0% 4% 4%
Hypertension 5% 3% 5% 5% 6%
Rash 2% 2% 1% 3% 3%
Edema 1% 2% 2% 1% 3%
aStudyincludedpatientsundergoingorthopedicsurgerytreatedwithPROCRITorplacebofor15days.
bStudy included patients undergoing orthopedic surgery treatedwith PROCRIT600U/kgweeklyfor4weeksor300U/kgdailyfor15days.
cDVTsweredeterminedbyclinicalsymptoms.
6.2 PostmarketingExperienceBecause postmarketing reporting of adverse reactions is voluntary and from apopulation of uncertain size, it is not always possible to reliably estimate theirfrequencyorestablishacausalrelationshiptodrugexposure.The followingadverse reactionshavebeen identifiedduringpostmarketinguseofPROCRIT:• Seizures[see Warnings and Precautions (5.5)]• PRCA[see Warnings and Precautions (5.7)]• Seriousallergicreactions[see Warnings and Precautions (5.8)]• Injectionsitereactions,includingirritationandpain• Porphyria
6.3 Immunogenicity Aswithalltherapeuticproteins,thereisapotentialforimmunogenicity.Neutralizingantibodies to epoetin alfa that cross-reactwith endogenous erythropoietin andotherESAscanresultinPRCAorsevereanemia(withorwithoutothercytopenias)[see Warnings and Precautions (5.7)].The incidence of antibody formation is highly dependent on the sensitivity andspecificityoftheassay.Additionally,theobservedincidenceofantibody(includingneutralizingantibody)positivityinanassaymaybeinfluencedbyseveralfactors,including assay methodology, sample handling, timing of sample collection,concomitantmedications,andunderlyingdisease.Forthesereasons,comparisonoftheincidenceofantibodiestoPROCRITwiththeincidenceofantibodiestootherproductsmaybemisleading.
7 DRUG INTERACTIONSNoformaldruginteractionstudieshavebeenconductedwithPROCRIT.
8 USE IN SPECIFIC POPULATIONS8.1 PregnancyThe multidose vials are formulated with benzyl alcohol. Do not administerPROCRIT frommultidosevials,orPROCRIT fromsingle-dosevialsadmixedwithbacteriostaticsalinecontainingbenzylalcohol,topregnantwomen.WhentherapywithPROCRITisneededduringpregnancy,useabenzylalcohol-freeformulation[see Dosage and Administration (2) and Contraindications (4)].PregnancyCategoryC(single-dosevialsonly)There are no adequate and well-controlled studies of PROCRIT use duringpregnancy.TherearelimiteddataonPROCRITuseinpregnantwomen.Inanimalreproductiveanddevelopmental toxicity studies,adverse fetaleffectsoccurredwhen pregnant rats received epoetin alfa at doses approximating the clinicalrecommended starting doses. Single-dose formulations of PROCRIT should beusedduringpregnancyonly if thepotentialbenefit justifies thepotential risk tothefetus.Thereare reportsof at least 33pregnantwomenwithanemiaaloneor anemiaassociated with severe renal disease and other hematologic disorders whoreceived PROCRIT. Polyhydramnios and intrauterine growth restriction werereported in women with chronic renal disease, which is associated with anincreasedriskfortheseadversepregnancyoutcomes.Therewas1infantbornwithpectusexcavatumandhypospadiasfollowingexposureduringthefirsttrimester.Due to the limited number of exposed pregnancies and multiple confoundingfactors(suchasunderlyingmaternalconditions,othermaternalmedications,andgestationaltimingofexposure),thesepublishedcasereportsandstudiesdonotreliablyestimatethefrequencyorabsenceofadverseoutcomes.WhenhealthyratsreceivedPROCRITatdosesof100Units/kg/dayduringmatingand through early pregnancy (dosing stopped prior to organogenesis), therewere slight increases in the incidences of pre- and post-implantation loss,
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)
Table 7. Adverse Reactions in Surgery Patients (continued)

8
and a decrease in live fetuses. This animal dose level of 100Units/kg/daymayapproximatetheclinicalrecommendedstartingdose,dependingonthetreatmentindication.Whenhealthypregnantratsandrabbitsreceivedintravenousdosesofupto500mg/kg/dayofPROCRITonlyduringorganogenesis,noteratogeniceffectswereobservedintheoffspring.WhenhealthypregnantratsreceivedPROCRITatdosesof500Units/kg/daylateinpregnancy(aftertheperiodoforganogenesis),offspringhaddecreasednumberofcaudalvertebraeandgrowthdelays[see Nonclinical Toxicology (13.3)].8.3 Nursing MothersThe multidose vials of PROCRIT are formulated with benzyl alcohol. Do notadminister PROCRIT from multidose vials, or PROCRIT from single-dose vialsadmixedwithbacteriostaticsalinecontainingbenzylalcohol,toanursingwoman.WhentherapywithPROCRITisneededinnursingwomen,useabenzylalcohol-freeformulation[see Dosage and Administration (2) and Contraindications (4)].ItisnotknownwhetherPROCRITisexcretedinhumanmilk.Becausemanydrugsare excreted in humanmilk, caution should be exercisedwhen PROCRIT fromsingle-dosevialsisadministeredtoanursingwoman.8.4 PediatricUseThe multidose vials are formulated with benzyl alcohol. Do not administerPROCRIT frommultidosevials,orPROCRIT fromsingle-dosevialsadmixedwithbacteriostatic saline containing benzyl alcohol, to neonates or infants. WhentherapywithPROCRITisneededinneonatesandinfants,useabenzylalcohol-freeformulation[see Dosage and Administration (2) and Contraindications (4)].Benzyl alcohol has been associated with serious adverse events and death,particularly in pediatric patients. The “gasping syndrome,” (characterized bycentralnervoussystemdepression,metabolicacidosis,gaspingrespirations,andhighlevelsofbenzylalcoholanditsmetabolitesfoundinthebloodandurine)hasbeen associatedwith benzyl alcohol dosages > 99mg/kg/day in neonates andlow-birthweightneonates.Additionalsymptomsmayincludegradualneurologicaldeterioration, seizures, intracranial hemorrhage, hematologic abnormalities,skin breakdown, hepatic and renal failure, hypotension, bradycardia, andcardiovascularcollapse.Although normal therapeutic doses of this product deliver amounts of benzylalcohol thataresubstantially lower than those reported inassociationwith the“gaspingsyndrome”,theminimumamountofbenzylalcoholatwhichtoxicitymayoccur isnot known.Prematureand low-birthweight infants,aswellaspatientsreceiving high dosages, may be more likely to develop toxicity. Practitionersadministering this and other medications containing benzyl alcohol shouldconsiderthecombineddailymetabolicloadofbenzylalcoholfromallsources.
PediatricPatientsonDialysisPROCRIT is indicated in pediatric patients, ages 1 month to 16 years of age,for the treatment of anemia associatedwith CKD requiring dialysis. Safety andeffectivenessinpediatricpatientslessthan1montholdhavenotbeenestablished[see Clinical Studies (14.1)].Thesafetydatafromthesestudiesaresimilartothoseobtainedfromthestudiesof PROCRIT in adult patientswith CKD [see Warnings and Precautions (5) and Adverse Reactions (6.1)].PediatricCancerPatientsonChemotherapyPROCRITisindicatedinpatients5to18yearsoldforthetreatmentofanemiadueto concomitant myelosuppressive chemotherapy. Safety and effectiveness inpediatricpatientslessthan5yearsofagehavenotbeenestablished[see Clinical Studies (14.3)].Thesafetydata fromthesestudiesaresimilar to thoseobtainedfrom the studies of PROCRIT in adult patients with cancer [see Warnings and Precautions (5) and Adverse Reactions (6.1)].PediatricPatientsWithHIVInfectionReceivingZidovudinePublished literature has reported the use of PROCRIT in 20 zidovudine-treated,anemic,pediatricpatientswithHIVinfection,ages8monthsto17years,treatedwith 50 to 400Units/kg subcutaneously or intravenously 2 to 3 timesperweek.Increases in hemoglobin levels and in reticulocyte counts and decreases in oreliminationofRBCtransfusionswereobserved.
PharmacokineticsinNeonatesLimited pharmacokinetic data from a study of 7 preterm, very low birthweightneonates and 10 healthy adults given intravenous erythropoietin suggestedthat distribution volumewasapproximately 1.5 to 2 timeshigher in thepretermneonates than in the healthy adults, and clearancewas approximately 3 timeshigherinthepretermneonatesthaninthehealthyadults.8.5 Geriatric UseOfthe4553patientswhoreceivedPROCRITinthe6studiesfortreatmentofanemiaduetoCKDnotreceivingdialysis,2726(60%)wereage65yearsandover,while1418(31%)were75yearsandover.Ofthe757patientswhoreceivedPROCRITinthe3studiesofCKDpatientsondialysis,361(47%)wereage65yearsandover,while100(13%)were75yearsandover.Nodifferencesinsafetyoreffectivenesswere observed between geriatric and younger patients. Dose selection andadjustmentforanelderlypatientshouldbeindividualizedtoachieveandmaintainthetargethemoglobin[see Dosage and Administration (2)].
Among778patientsenrolledinthe3clinicalstudiesofPROCRITforthetreatmentof anemia due to concomitant chemotherapy, 419 received PROCRIT and 359receivedplacebo.Ofthe419whoreceivedPROCRIT,247(59%)wereage65yearsandover,while78(19%)were75yearsandover.Nooveralldifferencesinsafetyoreffectivenesswereobservedbetweengeriatricandyoungerpatients.ThedoserequirementsforPROCRIT ingeriatricandyoungerpatientswithinthe3studiesweresimilar.Among1731patientsenrolledinthe6clinicalstudiesofPROCRITforreductionofallogeneicRBCtransfusionsinpatientsundergoingelectivesurgery,1085receivedPROCRIT and 646 received placebo or standard of care treatment. Of the 1085patientswhoreceivedPROCRIT,582(54%)wereage65yearsandover,while245(23%)were75yearsandover.Nooveralldifferences insafetyoreffectivenesswereobservedbetweengeriatricandyoungerpatients.Thedose requirementsforPROCRITingeriatricandyoungerpatientswithinthe4studiesusingthe3timesweeklyscheduleand2studiesusingtheweeklyscheduleweresimilar.Insufficient numbers of patients age 65 years or olderwere enrolled in clinicalstudies of PROCRIT for the treatment of zidovudine in HIV-infected patients todeterminewhethertheyresponddifferentlyfromyoungerpatients.
10 OVERDOSAGEPROCRIToverdosagecancausehemoglobinlevelsabovethedesiredlevel,whichshouldbemanagedwithdiscontinuationorreductionofPROCRITdosageand/orwith phlebotomy, as clinically indicated [see Pharmacodynamics (12.2)]. Casesofseverehypertensionhavebeenobserved followingoverdosewithESAs [see Warnings and Precautions (5.4)].
11 DESCRIPTIONPROCRIT(epoetinalfa)isa165-aminoaciderythropoiesis-stimulatingglycoproteinmanufactured by recombinant DNA technology. It has a molecular weight ofapproximately 30,400 daltons and is produced by mammalian cells into whichthe human erythropoietin gene has been introduced. The product contains theidenticalaminoacidsequenceofisolatednaturalerythropoietin.PROCRITisformulatedasasterile,colorlessliquidinvialsinmultipleformulations.Single-dose vials, formulated with an isotonic sodium chloride/sodium citrate-buffered solution, are supplied in multiple strengths. Each 1 mL vial contains2000,3000,4000,or10,000Unitsofepoetinalfa,Albumin(Human)(2.5mg),citricacid(0.06mg),sodiumchloride(5.9mg),andsodiumcitrate(5.8mg)inWaterforInjection,USP(pH6.9±0.3).Single-dose1mLvials formulatedwithan isotonicsodium chloride/sodium phosphate buffer contain 40,000 Units of epoetin alfaalbumin(human)(2.5mg),citricacid(0.0068mg),sodiumchloride(5.8mg),sodiumcitrate (0.7 mg), sodium phosphate dibasic anhydrate (1.8 mg), and sodiumphosphatemonobasicmonohydrate (1.2mg) inWater for Injection,USP (pH6.9± 0.3).Multidose, 2mL vials contain 10,000Units epoetin alfa, albumin (human)(2.5 mg), benzyl alcohol (1%), sodium chloride (8.2 mg), and sodium citrate(1.3mg) per 1mLWater for Injection, USP (pH 6.1 ± 0.3).Multidose 1mL vialscontain20,000Unitsepoetinalfa,albumin(human)(2.5mg),benzylalcohol(1%),sodiumchloride(8.2mg),citricacid(0.11mg),andsodiumcitrate(1.3mg),per1mLinWaterforInjection,USP(pH6.1±0.3).
12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionPROCRIT stimulates erythropoiesis by the same mechanism as endogenouserythropoietin.12.2 PharmacodynamicsPROCRIT increases the reticulocyte countwithin 10 days of initiation, followedby increases in theRBCcount, hemoglobin, andhematocrit, usuallywithin 2 to6 weeks. The rate of hemoglobin increase varies among patients and isdependentuponthedoseofPROCRITadministered.Forcorrectionofanemia inhemodialysis patients, a greater biologic response is not observed at dosesexceeding300Units/kg3timesweekly.12.3 PharmacokineticsInadultandpediatricpatientswithCKD, theeliminationhalf-life (t1/2)ofplasmaerythropoietin after intravenous administration of PROCRIT ranged from 4 to13 hours. After subcutaneous administration, Cmax was achieved within 5 to24 hours. The t1/2 in adult patientswith serum creatinine greater than 3mg/dLwassimilarbetweenthosenotondialysisandthosemaintainedondialysis.ThepharmacokineticdataindicatenoapparentdifferenceinPROCRITt1/2amongadultpatientsaboveorbelow65yearsofage.Apharmacokineticstudycomparing150Units/kgsubcutaneous3timesweeklyto40,000Unitssubcutaneousweeklydosingregimenwasconductedfor4weeksinhealthysubjects(n=12)andfor6weeksinanemiccancerpatients(n=32)receivingcyclicchemotherapy.Therewasnoaccumulationofserumerythropoietinafterthe2dosingregimensduringthestudyperiod.The40,000UnitsweeklyregimenhadahigherCmax(3-to7-fold),longerTmax(2-to3-fold),higherAUC0-168h(2-to3-fold)oferythropoietinandlowerclearance(CL)(50%)thanthe150Units/kg3timesweeklyregimen. Inanemiccancerpatients, theaverage t1/2wassimilar (40hourswithrangeof16to67hours)afterbothdosingregimens.Afterthe150Units/kg3timesweeklydosing, thevaluesofTmaxandCLweresimilar (13.3±12.4vs.14.2±6.7hours,and20.2±15.9vs.23.6±9.5mL/hr/kg)betweenweek1whenpatientswere
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

9
receivingchemotherapy (n= 14) andweek3whenpatientswerenot receivingchemotherapy (n=4).Differenceswereobservedafter the40,000Unitsweeklydosingwith longerTmax (38±18hours)and lowerCL (9.2±4.7mL/hr/kg)duringweek1whenpatientswerereceivingchemotherapy(n=18)comparedwiththose(22±4.5hours,13.9±7.6mL/hr/kg,respectively)duringweek3whenpatientswerenotreceivingchemotherapy(n=7).The pharmacokinetic profile of PROCRIT in children and adolescents appearedsimilartothatofadults.The pharmacokinetics of PROCRIT has not been studied in patients with HIVinfection.
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenicityThecarcinogenicpotentialofPROCRIThasnotbeenevaluated.
MutagenicityPROCRITwasnotmutagenicorclastogenicundertheconditionstested:PROCRITwas negative in the in vitro bacterial reverse mutation assay (Ames test), inthe in vitro mammalian cell gene mutation assay (the hypoxanthine-guaninephosphoribosyltransferase[HGPRT]locus),inanin vitrochromosomalaberrationassayinmammaliancells,andinthein vivomousemicronucleusassay.ImpairmentofFertilityWhen administered intravenously to male and female rats prior to and duringmating,and to females through thebeginningof implantation (up togestationalday7;dosingstoppedpriortothebeginningoforganogenesis),dosesof100and500 Units/kg/day of PROCRIT caused slight increases in pre-implantation loss,post-implantationlossanddecreasesintheincidenceoflivefetuses.Itisnotclearwhethertheseeffectsreflectadrugeffectontheuterineenvironmentorontheconceptus.Thisanimaldose levelof100Units/kg/dayapproximates theclinicalrecommendedstartingdose,dependingonthepatient’streatmentindication,butmaybelowerthantheclinicaldoseinpatientswhosedoseshavebeenadjusted.13.3 ReproductiveandDevelopmentalToxicologyWhenpregnant ratswere administered intravenousPROCRIT, 500Units/kg/day,after the period of organogenesis (from day 17 of gestation through day 21 oflactation),theirpupsexhibiteddecreasednumberofcaudalvertebrae,decreasedbodyweightgain,anddelayedappearanceofabdominalhair,eyelidopening,andossification. This animal dose level of 500 Units/kg/day is approximately 5-foldhigher than theclinical recommendedstartingdose,dependingon thepatient’streatmentindication.WhenPROCRITwasadministeredintravenouslyduringtheperiodoforganogenesistopregnantrats(gestationaldays7to17)andpregnantrabbits(gestationaldays6to18),noevidenceofteratogenicoutcomewasobservedatthedosestested,upto500Units/kg/day.Theoffspring(F1generation)ofthetreatedratswereobservedpostnatally; rats from the F1 generation reached maturity and were mated; noPROCRIT-relatedeffectswereapparentfortheiroffspring(F2generationfetuses).
14 CLINICALSTUDIES14.1 PatientsWithChronicKidneyDiseaseAdultPatientsonDialysisPatients with chronic kidney disease on dialysis: ESA effects on rates of transfusionIn clinical studies of CKD patients on dialysis, PROCRIT increased hemoglobinlevels and decreased the need for RBC transfusion. Overall, more than 95%of patients were RBC transfusion-independent after receiving PROCRIT for3months.Inclinicalstudiesatstartingdosesof50to150Units/kg3timesweekly,adultpatientsrespondedwithanaveragerateofhemoglobinriseaspresentedinTable8.
Table8.AverageRateofHemoglobinRisein2Weeks
Starting Dose(3TimesWeeklyIntravenously) HemoglobinIncreasein2Weeks
50Units/kg 0.5g/dL
100Units/kg 0.8g/dL
150Units/kg 1.2g/dL
ThesafetyandefficacyofPROCRITwereevaluatedin13clinicalstudiesinvolvingintravenousadministrationtoatotalof1010anemicpatientsondialysis.Overall,morethan90%ofthepatientstreatedwithPROCRITexperiencedimprovementinhemoglobinconcentrations.Inthe3largestoftheseclinicalstudies,themedianmaintenancedosenecessarytomaintainthehemoglobinbetween10to12g/dLwasapproximately75Units/kg3timesweekly.Morethan95%ofpatientswereabletoavoidRBCtransfusions.InthelargestUSmulticenterstudy,approximately65%ofthepatientsreceiveddosesof100Units/kg3timesweeklyorlesstomaintaintheir hemoglobinat approximately 11.7g/dL.Almost 10%ofpatients receivedadoseof25Units/kgorless,andapproximately10%receivedadoseofmorethan200Units/kg3timesweeklytomaintaintheirhemoglobinatthislevel.
IntheNormalHematocritStudy,theyearlytransfusionratewas51.5%inthelowerhemoglobingroup(10g/dL)and32.4%inthehigherhemoglobingroup(14g/dL).
Other ESA trialsIn a 26-week, double-blind, placebo-controlled study, 118 patients on dialysiswithanaveragehemoglobinofapproximately7g/dLwererandomized toeitherPROCRITorplacebo.By theendof thestudy,averagehemoglobin increasedtoapproximately11g/dLinthePROCRIT-treatedpatientsandremainedunchangedinpatientsreceivingplacebo.PROCRIT-treatedpatientsexperiencedimprovementsin exercise toleranceandpatient-reportedphysical functioningatmonth 2 thatweremaintainedthroughoutthestudy.A multicenter, unit-dose study was also conducted in 119 patients receivingperitoneal dialysis who self-administered PROCRIT subcutaneously. Patientsresponded to PROCRIT administered subcutaneously in a manner similar topatientsreceivingintravenousadministration.
PediatricPatientsonDialysisThe safety and efficacy of PROCRIT were studied in a placebo-controlled,randomized study of 113 children with anemia (hemoglobin ≤ 9 g/dL)undergoing peritoneal dialysis or hemodialysis. The initial dose of PROCRITwas 50 Units/kg intravenously or subcutaneously 3 times weekly. The dose ofstudy drug was titrated to achieve either a hemoglobin of 10 to 12 g/dL or anabsoluteincreaseinhemoglobinof2g/dLoverbaseline.Attheendoftheinitial12weeks,astatisticallysignificantriseinmeanhemoglobin(3.1g/dLvs.0.3g/dL)wasobservedonly in thePROCRITarm.Theproportionofchildrenachievingahemoglobinof10g/dL,oranincreaseinhemoglobinof2g/dLoverbaseline,atanytimeduringthefirst12weekswashigherinthePROCRITarm(96%vs.58%).Within12weeksofinitiatingPROCRITtherapy,92.3%ofthepediatricpatientswereRBCtransfusionindependentascomparedto65.4%whoreceivedplacebo. Among patients who received 36 weeks of PROCRIT, hemodialysispatientsreceivedahighermedianmaintenancedose[167Units/kg/week(n=28)vs.76Units/kg/week (n=36)]and took longer toachieveahemoglobinof10 to12g/dL (mediantimetoresponse69daysvs.32days) thanpatientsundergoingperitonealdialysis.
AdultPatientsWithCKDNotRequiringDialysisFourclinicalstudieswereconductedinpatientswithCKDnotondialysisinvolving181patientstreatedwithPROCRIT.ThesepatientsrespondedtoPROCRITtherapyinamannersimilartothatobservedinpatientsondialysis.PatientswithCKDnotondialysisdemonstratedadose-dependentandsustainedincreaseinhemoglobinwhen PROCRIT was administered by either an intravenous or subcutaneousroute,withsimilarratesofriseofhemoglobinwhenPROCRITwasadministeredbyeitherroute.
Patients with chronic kidney disease not on dialysis: ESA effects on rates of transfusionIn TREAT, a randomized, double-blind trial of 4038 patients with CKD and type2 diabetes not on dialysis, a post-hoc analysis showed that the proportion ofpatientsreceivingRBCtransfusionswaslowerinpatientsadministeredanESAtotargetahemoglobinof13g/dLcomparedtothecontrolarminwhichanESAwasadministered intermittently if hemoglobin concentration decreased to less than9g/dL(15%versus25%,respectively). InCHOIR,arandomizedopen-labelstudyof1432patientswithCKDnotondialysis,useofepoetinalfa to targetahigher(13.5g/dL)versuslower(11.3g/dL)hemoglobingoaldidnotreducetheuseofRBCtransfusions. In each trial, no benefits occurred for the cardiovascular or end-stagerenaldiseaseoutcomes.Ineachtrial,thepotentialbenefitofESAtherapywasoffsetbyworsecardiovascularsafetyoutcomesresultinginanunfavorablebenefit-riskprofile[see Warnings and Precautions (5.1)].ESAEffectsonratesofdeathandotherseriouscardiacadverseeventsThree randomized outcome trials (Normal Hematocrit Study [NHS], Correctionof Anemia with Epoetin Alfa in Chronic Kidney Disease [CHOIR], and Trial ofDarbepoetin Alfa in Type 2 Diabetes and CKD [TREAT]) have been conductedin patients with CKD using Epogen/PROCRIT/Aranesp to target higher vs.lower hemoglobin levels. Though these trials were designed to establish acardiovascular or renal benefit of targeting higher hemoglobin levels, in all 3studies,patientsrandomizedtothehigherhemoglobintargetexperiencedworsecardiovascular outcomes and showed no reduction in progression to ESRD. Ineachtrial,thepotentialbenefitofESAtherapywasoffsetbyworsecardiovascularsafetyoutcomesresultinginanunfavorablebenefit-riskprofile[see Warnings and Precautions (5.1)].14.2 Zidovudine-treatedPatientsWithHIVInfectionThe safety and efficacy of PROCRIT were evaluated in 4 placebo-controlledstudiesenrolling 297anemicpatients (hemoglobin< 10g/dL)withHIV infectionreceivingconcomitanttherapywithzidovudine.Inthesubgroupofpatients(89/125PROCRIT and 88/130 placebo)with pre-study endogenous serum erythropoietinlevels≤500mUnits/mL,PROCRITreducedthemeancumulativenumberofunitsofbloodtransfusedperpatientbyapproximately40%ascomparedtotheplacebogroup.AmongthosepatientswhorequiredRBCtransfusionsatbaseline,43%ofpatientstreatedwithPROCRITversus18%ofplacebo-treatedpatientswereRBCtransfusion-independentduringthesecondandthirdmonthsoftherapy.PROCRIT
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

10
therapy also resulted in significant increases in hemoglobin in comparison toplacebo.Whenexaminingtheresultsaccordingtotheweeklydoseofzidovudinereceivedduringmonth3oftherapy,therewasastatisticallysignificantreduction(p < 0.003) in RBC transfusion requirements in patients treated with PROCRIT(n = 51) compared to placebo-treated patients (n = 54) whose mean weeklyzidovudinedosewas≤4200mg/week.Approximately17%of thepatientswithendogenousserumerythropoietin levels≤ 500mUnits/mLreceivingPROCRITindosesfrom100to200Units/kg3timesweeklyachievedahemoglobinof12.7g/dLwithoutadministrationofRBCtransfusionsorsignificantreductioninzidovudinedose.Inthesubgroupofpatientswhosepre-study endogenous serumerythropoietin levelswere> 500mUnits/mL,PROCRITtherapy did not reduce RBC transfusion requirements or increase hemoglobincomparedtothecorrespondingresponsesinplacebo-treatedpatients.14.3 CancerPatientsonChemotherapyThe safety and effectiveness of PROCRIT was assessed in two multicenter,randomized (1:1), placebo-controlled, double-blind studies (Study C1 and StudyC2)andapooledanalysisofsixadditionalrandomized(1:1),multicenter,placebo-controlled, double-blind studies. All studies were conducted in patients withanemia due to concomitantly administered cancer chemotherapy. Study C1enrolled344adultpatients,StudyC2enrolled222pediatricpatients,andthepooledanalysiscontained131patientsrandomizedtoepoetinalfaorplacebo.InStudiesC1andC2,efficacywasdemonstratedbyareductionintheproportionofpatientswhoreceivedanRBCtransfusion,fromweek5throughendofthestudy,withthelast-knownRBCtransfusionstatuscarriedforwardforpatientswhodiscontinuedtreatment. In thepooledanalysis, efficacywasdemonstratedbya reduction intheproportionofpatientswhoreceivedanRBCtransfusionfromweek5throughendofthestudyinthesubsetofpatientswhowereremainingontherapyfor6ormoreweeks.
StudyC1StudyC1wasconducted inanemicpatients (hemoglobin< 11.5g/dL formales;<10.5g/dLforfemales)withnon-myeloidmalignanciesreceivingmyelosuppressivechemotherapy. Randomization was stratified by type of malignancy (lung vs.breastvs.other),concurrentradiationtherapyplanned(yesorno),andbaselinehemoglobin (< 9 g/dL vs. ≥ 9 g/dL); patients were randomized to epoetin alfa40,000Units (n = 174) or placebo (n = 170) as aweekly subcutaneous injectioncommencingonthefirstdayofthechemotherapycycle.Ninety-onepercentofpatientswerewhite,44%weremale,andthemedianageofpatientswas66years(range:20to88years).Theproportionofpatientswithdrawnfromthestudypriortoweek5waslessthan10%forplacebo-treatedorepoetin-treatedpatients.Perprotocol,thelastavailablehemoglobinvaluesfrompatientswho dropped out were included in the efficacy analyses. Efficacy results areshowninTable9.
Table 9. Study C1: Proportion of Patients Transfused
Week5ThroughWeek16orEndofStudya
Chemotherapy Regimen PROCRIT (n=174)
Placebo (n = 170)
AllRegimens 14%(25/174)b 28%(48/170)
Regimenswithoutcisplatin 14%(21/148) 26%(35/137)
Regimenscontainingcisplatin 15%(4/26) 39%(13/33)
aLast-knownRBCtransfusionstatuscarriedforwardforpatientswhodiscontinuedtreatment.
bTwo-sidedp<0.001, logisticregressionanalysisadjustingforaccrualrateandstratificationvariables
StudyC2Study C2 was conducted in 222 anemic patients, ages 5 to 18, receivingchemotherapyforthetreatmentofvariouschildhoodmalignancies.Randomizationwasstratifiedbycancertype(solidtumors,Hodgkin’sdisease,acutelymphocyticleukemia, vs. non-Hodgkin’s lymphoma); patients were randomized to receiveepoetinalfaat600Units/kgmaximum40,000Units(n=111)orplacebo(n=111)asaweeklyintravenousinjection.Sixty-ninepercentofpatientswerewhite,55%weremale,andthemedianageofpatientswas12years(range:5to18years).Two(2%)ofplacebo-treatedpatientsand3(3%)ofepoetinalfa-treatedpatientsdroppedoutofthestudypriortoweek5.Therewere fewerRBC transfusions fromweek5 through theend-of-study inepoetin-alfatreatedpatients[51%(57/111)]comparedtoplacebo-treatedpatients[69%(77/111)].Therewasnoevidenceofanimprovementinhealth-relatedqualityoflife,includingnoevidenceofaneffectonfatigue,energy,orstrengthinpatientsreceivingPROCRITascomparedtothosereceivingplacebo.
PooledAnalysis(ThreeTimesPerWeekDosing)The results of 6 studies of similar design and that randomized 131 patients toepoetin alfa or placebowere pooled to assess the safety and effectiveness ofepoetin alfa. Patients were randomized to receive epoetin alfa at 150 Units/kg(n=63)orplacebo(n=68),subcutaneously three timesperweek for12weeksineachstudy.Acrossallstudies,72patientsweretreatedwithconcomitantnoncisplatin-containing chemotherapy regimens and 59 patientswere treatedwithconcomitantcisplatin-containingchemotherapyregimens.Twelvepatients(19%)intheepoetinalfaarmand10patients(15%)intheplacebo-armdroppedoutpriortoweek6andareexcludedfromefficacyanalyses.
Table 10: Proportion of Patients Transfused in the Pooled Analysis for Three Times PerWeekDosing
Week5ThroughWeek12orEndofStudya
Chemotherapy Regimen PROCRIT Placebo
AllRegimens 22%(11/51)b 43%(25/58)
Regimenswithoutcisplatin 21%(6/29) 33%(11/33)
Regimenscontainingcisplatin 23%(5/22) 56%(14/25)
aLimited to patients remainingon studybeyondweek 6 and includesonlyRBCtransfusionsduringweeks5-12.
bTwo-sidedp<0.05,unadjusted
14.4 SurgeryPatientsThe safety and efficacy of PROCRIT were evaluated in a placebo-controlled,double-blind study (S1) enrolling 316 patients scheduled for major, electiveorthopedichiporkneesurgerywhowereexpectedtorequire≥2unitsofbloodandwhowerenotableorwillingtoparticipateinanautologousblooddonationprogram.Patientswerestratifiedinto1of3groupsbasedontheirpretreatmenthemoglobin [≤ 10g/dL (n= 2), > 10 to≤ 13g/dL (n= 96), and> 13 to≤ 15g/dL(n = 218)] and then randomly assigned to receive 300 Units/kg PROCRIT,100Units/kgPROCRIT,orplacebobysubcutaneous injection for 10daysbeforesurgery,onthedayofsurgery,andfor4daysaftersurgery.Allpatientsreceivedoralironandalow-dose,postoperativewarfarinregimen.TreatmentwithPROCRIT300Units/kgsignificantly(p=0.024)reducedtheriskofallogeneicRBCtransfusioninpatientswithapretreatmenthemoglobinof>10to≤13g/dL;5/31(16%)ofpatientstreatedwithPROCRIT300Units/kg,6/26(23%)ofpatients treatedwithPROCRIT100Units/kg,and13/29 (45%)ofplacebo-treatedpatientswere transfused.Therewasno significantdifference in thenumberofpatients transfused between PROCRIT (9% 300 Units/kg, 6% 100 Units/kg) andplacebo(13%) in the>13 to≤15g/dLhemoglobinstratum.Therewere too fewpatientsinthe≤10g/dLgrouptodetermineifPROCRITisusefulinthishemoglobinstrata. In the>10 to≤ 13g/dLpretreatmentstratum, themeannumberofunitstransfusedperPROCRIT-treatedpatient(0.45unitsbloodfor300Units/kg,0.42unitsblood for 100Units/kg)was less than themean transfusedper placebo-treatedpatient (1.14units) (overallp=0.028). Inaddition,meanhemoglobin,hematocrit,and reticulocyte counts increased significantly during the presurgery period inpatientstreatedwithPROCRIT.PROCRITwasalsoevaluatedinanopen-label,parallel-groupstudy(S2)enrolling145patientswithapretreatmenthemoglobinlevelof≥10to≤13g/dLwhowerescheduledformajororthopedichiporkneesurgeryandwhowerenotparticipatingin an autologous program. Patients were randomly assigned to receive 1 of 2subcutaneousdosingregimensofPROCRIT(600Units/kgonceweeklyfor3weekspriortosurgeryandonthedayofsurgery,or300Units/kgoncedailyfor10dayspriortosurgery,onthedayofsurgery,andfor4daysaftersurgery).Allpatientsreceivedoralironandappropriatepharmacologicanticoagulationtherapy.From pretreatment to presurgery, the mean increase in hemoglobin in the600 Units/kg weekly group (1.44 g/dL) was greater than that observed in the300Units/kgdailygroup.Themean increase inabsolutereticulocytecountwassmallerintheweeklygroup(0.11x106/mm3)comparedtothedailygroup(0.17x106/mm3). Mean hemoglobin levels were similar for the 2 treatment groupsthroughoutthepostsurgicalperiod.TheerythropoieticresponseobservedinbothtreatmentgroupsresultedinsimilarRBC transfusion rates [11/69 (16%) in the 600 Units/kgweekly group and 14/71(20%) inthe300Units/kgdailygroup].Themeannumberofunitstransfusedperpatientwasapproximately0.3unitsinbothtreatmentgroups.
16 HOW SUPPLIED/STORAGE AND HANDLINGStoreat36°Fto46°F(2°Cto8°C).Donotfreeze.Donotshake.Protectfromlight;storePROCRITinthecartonuntiluse.DonotusePROCRITthathasbeenshakenorfrozen.
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

11
Single-dose, Preservative-free Vial: Each 1 mL of solution contains 2000(NDC59676-302-01),3000(NDC59676-303-01),4000(NDC59676-304-01),or10,000Units (NDC 59676-310-01) of epoetin alfa. Each strength is supplied in cartons,eachcartoncontaining6single-dosevials.Single-dose,Preservative-freeVial (Tray):Each1mLofsolutioncontains10,000Units (NDC 59676-310-02) of epoetin alfa and is supplied in dispensing packscontaining25single-dosevials.Single-dose,Preservative-freeVial(inphosphate-bufferedformulation):Each1mLofsolutioncontains40,000Units(NDC59676-340-01)ofepoetinalfaandissuppliedindispensingpackscontaining4single-dosevials.Multidose,PreservedVial:2mL(20,000Unitstotal;10,000Units/mL).Each1mLofsolutioncontains10,000Units(NDC59676-312-04)ofepoetinalfaandissuppliedindispensingpackscontaining4multidosevials.Multidose,PreservedVial:1mL(20,000Units/mL).Each1mLofsolutioncontains20,000Units(NDC59676-320-04)ofepoetinalfaandissuppliedindispensingpackscontaining4multidosevials.
17 PATIENT COUNSELING INFORMATIONSee Medication Guide.Priortotreatment,informpatientsoftherisksandbenefitsofPROCRIT.Informpatientswithcancer that theymustsign thepatient-healthcareprovideracknowledgment formbefore the start of each treatmentcoursewithPROCRITand that healthcare providers must enroll and comply with the ESA APPRISEOncologyPrograminordertoprescribePROCRIT.
Informpatients:• ToreadtheMedicationGuide.• Of the increased risks of mortality, serious cardiovascular reactions,
thromboembolicreactions,stroke,andtumorprogression[see Warnings and Precautions (5.1, 5.3)].
• To undergo regular blood pressure monitoring, adhere to prescribed anti-hypertensiveregimenandfollowrecommendeddietaryrestrictions.
• Tocontact theirhealthcareprovider fornew-onsetneurologicsymptomsorchangeinseizurefrequency.
• Oftheneedtohaveregularlaboratorytestsforhemoglobin.• Risks are associated with benzyl alcohol in neonates, infants, pregnant
women,andnursingmothers[see Use in Specific Populations (8.1, 8.3, 8.4)].
Instructpatientswhoself-administerPROCRITofthe:• ImportanceoffollowingtheInstructionsforUse.• Dangersofreusingneedles,syringes,orunusedportionsofsingle-dosevials.• Properdisposalofusedsyringes,needles,andunusedvials,andof the full
container.
PROCRIT®(epoetinalfa)
Manufactured by:AmgenInc.OneAmgenCenterDriveThousandOaks,CA91320-1799U.S.A.
Manufactured for:JanssenProducts,LPHorsham,Pennsylvania19044
©JanssenProducts,LP2000PrintedinU.S.A.
Patent:www.procrit.com/patents/
MEDICATION GUIDEPROCRIT® (PRO’−KRIT)
(epoetin alfa)
ReadthisMedicationGuide: • beforeyoustartPROCRIT. • ifyouaretoldbyyourhealthcareproviderthatthereisnew
informationaboutPROCRIT. • if you are told by your healthcare provider that you may
injectPROCRITathome, read thisMedicationGuideeachtimeyoureceiveanewsupplyofmedicine.
This Medication Guide does not take the place of talking toyour healthcare provider about your medical condition or yourtreatment.TalkwithyourhealthcareproviderregularlyabouttheuseofPROCRITandaskifthereisnewinformationaboutPROCRIT.
What is the most important information I should know aboutPROCRIT?PROCRITmaycauseserioussideeffectsthatcanleadtodeath,including:Forpeoplewithcancer: • Yourtumormaygrowfasterandyoumaydiesoonerifyou
choose to take PROCRIT. Your healthcare provider hasreceivedspecialtraininginordertoprescribePROCRITandwilltalkwithyouindetailabouttheserisks.
ForallpeoplewhotakePROCRIT,includingpeoplewithcancerorchronickidneydisease: • Serious heart problems, such as heart attack or heart
failure, and stroke. Youmaydie sooner if youare treatedwithPROCRITtoincreaseredbloodcells(RBCs)tonearthesamelevelfoundinhealthypeople.
• Blood clots.BloodclotsmayhappenatanytimewhiletakingPROCRIT.IfyouarereceivingPROCRITforanyreasonandyouaregoingtohavesurgery,talktoyourhealthcareprovideraboutwhether or not you need to take a blood thinner tolessenthechanceofbloodclotsduringorfollowingsurgery.Clots can form in blood vessels (veins), especially in yourleg(deepvenousthrombosisorDVT).Piecesofabloodclotmaytraveltothelungsandblockthebloodcirculationinthelungs(pulmonaryembolus).
• Callyourhealthcareproviderorgetmedicalhelprightawayifyouhaveanyofthesesymptoms:
• Chestpain • Troublebreathingorshortnessofbreath • Paininyourlegs,withorwithoutswelling • Acoolorpalearmorleg • Sudden confusion, trouble speaking, or trouble
understandingothers’speech • Suddennumbnessorweaknessinyourface,arm,orleg,
especiallyononesideofyourbody • Suddentroubleseeing • Sudden trouble walking, dizziness, loss of balance or
coordination • Lossofconsciousness(fainting) • Hemodialysisvascularaccessstopsworking
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

12
See“What are the possible side effects of PROCRIT?”belowformoreinformation.
If youdecide to takePROCRIT, yourhealthcareprovider shouldprescribe the smallest dose of PROCRIT that is necessary toreduceyourchanceofneedingRBCtransfusions.
What is PROCRIT?PROCRITisaprescriptionmedicineusedtotreatanemia.Peoplewithanemiahavealower-than-normalnumberofRBCs.PROCRITworks like thehumanprotein callederythropoietin to help yourbodymakemoreRBCs.PROCRIT isusedtoreduceoravoid theneedforRBCtransfusions.
PROCRITmaybeusedtotreatanemiaifitiscausedby:
• Chronickidneydisease(youmayormaynotbeondialysis). • Chemotherapythatwillbeusedforatleasttwomonthsafter
startingPROCRIT. • A medicine called zidovudine (AZT) used to treat HIV
infection.
PROCRITmayalsobeused toreducethechanceyouwillneedRBCtransfusionsifyouarescheduledforcertainsurgerieswherealotofbloodlossisexpected.
Ifyourhemoglobinlevelstaystoohighorifyourhemoglobingoesup too quickly, thismay lead to serious health problemswhichmayresult indeath.TheseserioushealthproblemsmayhappenifyoutakePROCRIT,evenifyoudonothaveanincreaseinyourhemoglobinlevel.
PROCRITshouldnotbeusedfortreatmentofanemia:
• If you have cancer and youwill not be receiving chemo-therapythatmaycauseanemia.
• Ifyouhaveacancerthathasahighchanceofbeingcured.Talkwithyourhealthcareprovideraboutthekindofcanceryouhave.
• In place of emergency treatment for anemia (RBCtransfusions).
PROCRIThasnotbeenprovento improvequalityof life, fatigue,orwell-being.
PROCRIT should not be used to reduce the chance of RBCtransfusionsif:
• Youarescheduledforsurgeryonyourheartorbloodvessels. • Youareableandwillingtodonatebloodpriortosurgery.
WhoshouldnottakePROCRIT?DonottakePROCRITifyou:
• Have cancer and have not been counseled by yourhealthcareproviderabouttreatmentwithPROCRIT.
• Havehighbloodpressurethatisnotcontrolled(uncontrolledhypertension).
• HavebeentoldbyyourhealthcareproviderthatyouhaveorhaveeverhadatypeofanemiacalledPureRedCellAplasia(PRCA) that starts after treatment with PROCRIT or othererythropoietinproteinmedicines.
• HavehadaseriousallergicreactiontoPROCRIT.
DonotgivePROCRITfrommultidosevialsto: • Pregnantorbreastfeedingwomen • Babies
WhatshouldItellmyhealthcareproviderbeforetakingPROCRIT?PROCRITmaynotberightforyou.Tell your healthcare provider about all your health conditions,includingifyou:
• Haveheartdisease. • Havehighbloodpressure. • Havehadaseizure(convulsion)orstroke. • Haveanyothermedicalconditions. • Are pregnant or planning to become pregnant. It is not
knownifPROCRITmayharmyourunbornbaby.Talktoyourhealthcare provider about possible pregnancy and birthcontrolchoicesthatarerightforyou.
• Arebreastfeedingorplanningtobreastfeed.ItisnotknownifPROCRITpassesintobreastmilk.
Tell your healthcare provider about all themedicines you take,including prescription and nonprescriptionmedicines, vitamins,andherbalsupplements.
Knowthemedicinesyoutake.Keepalistofyourmedicineswithyouandshowittoyourhealthcareproviderwhenyougetanewmedicine.
HowshouldItakePROCRIT? • IfyouoryourcaregiverhasbeentrainedtogivePROCRIT
shots(injections)athome: ◦ Be sure that you read, understand, and follow the
“InstructionsforUse”thatcomewithPROCRIT. ◦ TakePROCRITexactlyas yourhealthcareprovider tells
youto.DonotchangethedoseofPROCRITunlesstoldtodosobyyourhealthcareprovider.
◦ Your healthcare provider will show you how muchPROCRITtouse,howto inject it,howoftenitshouldbeinjected, and how to safely throwaway the used vials,syringes,andneedles.
◦ If you miss a dose of PROCRIT, call your healthcareproviderrightawayandaskwhattodo.
◦ IfyoutakemorethantheprescribedamountofPROCRIT,callyourhealthcareproviderrightaway.
• During treatment with PROCRIT, continue to follow yourhealthcareprovider’sinstructionsfordietandmedicines.
• Have your blood pressure checked as instructed by yourhealthcareprovider.
What are the possible side effects of PROCRIT?PROCRITmaycauseserioussideeffects.
• See“WhatisthemostimportantinformationIshouldknowabout PROCRIT?”
• High blood pressure.HighbloodpressureisacommonsideeffectofPROCRIT inpatientswithchronickidneydisease.Yourbloodpressuremaygouporbedifficulttocontrolwithblood pressure medicine while taking PROCRIT. This canhappen even if you have never had high blood pressurebefore. Your healthcare provider should check your bloodpressure often. If your blood pressure does go up, yourhealthcare provider may prescribe new or more bloodpressuremedicine.
• Seizures.IfyouhaveanyseizureswhiletakingPROCRIT,getmedicalhelprightawayandtellyourhealthcareprovider.
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

13
• Antibodies to PROCRIT.YourbodymaymakeantibodiestoPROCRIT.Theseantibodiescanblockorlessenyourbody’sabilitytomakeRBCsandcauseyoutohavesevereanemia.Callyourhealthcareproviderifyouhaveunusualtiredness,lackofenergy,dizziness,orfainting.YoumayneedtostoptakingPROCRIT.
• Serious allergic reactions. Serious allergic reactions cancause a rash over your whole body, shortness of breath,wheezing,dizzinessandfaintingbecauseofadropinbloodpressure,swellingaroundyourmouthoreyes,fastpulse,orsweating.Ifyouhaveaseriousallergicreaction,stopusingPROCRITandcall yourhealthcareproviderorgetmedicalhelprightaway.
• Dangers of using PROCRIT from multi-dose vials in newborns, infants,andpregnantorbreastfeedingwomen.Do not use PROCRIT from multi-dose vials in newborns,infants, pregnant or breastfeeding women because thePROCRIT in these vials contains benzyl alcohol. Benzylalcohol has been shown to cause brain damage, otherserioussideeffects,anddeath innewbornandprematurebabies. PROCRIT that comes in single-dose vials doesnot contain benzyl alcohol. See “Who should not takePROCRIT?”
CommonsideeffectsofPROCRITinclude: • joint,muscle,orbonepain • fever • cough • rash • nausea • vomiting • sorenessofmouth • itching • headache • redness and pain in the skin where PROCRIT shots were
given
These are not all of the possible side effects of PROCRIT. Yourhealthcareprovidercangiveyouamorecompletelist.Tellyourhealthcareprovideraboutanysideeffectsthatbotheryouorthatdonotgoaway.
Callyourdoctor formedicaladviceaboutsideeffects.YoumayreportsideeffectstoFDAat1-800-FDA-1088.
HowshouldIstorePROCRIT? • DonotshakePROCRIT. • ProtectPROCRITfromlight. • Store PROCRIT in the refrigerator between 36°F to 46°F
(2°Cto8°C). • DonotfreezePROCRIT.DonotusePROCRITthathasbeen
frozen. • Throw away multidose vials of PROCRIT no later than
21daysfromthefirstdaythatyouputaneedleintothevial. • Single-dosevialsofPROCRITshouldbeusedonlyonetime.
Throwthevialawayafteruseevenifthereismedicineleftinthevial.
Keep PROCRIT and all medicines out of the reach of children.
General information about PROCRIT Medicines are sometimes prescribed for purposes other thanthose listed in a Medication Guide. Use PROCRIT only for theconditionforwhichithasbeenprescribed.DonotgivePROCRITtootherpatientsevenif theyhavethesamesymptomsthatyouhave.Itmayharmthem.
ThisMedicationGuidesummarizesthemostimportantinformationaboutPROCRIT.IfyouwouldlikemoreinformationaboutPROCRIT,talk to your healthcare provider. You can ask your healthcareprovider or pharmacist for information about PROCRIT that iswrittenforhealthcareprofessionals.Formoreinformation,gotothefollowingwebsite:www.PROCRIT.comorcall1-800-JANSSEN(1-800-526-7736).
What are the ingredients in PROCRIT?Active Ingredient:epoetinalfa
Inactive Ingredients: • Multidosevialscontainbenzylalcohol. • All vials contain albumin (human), sodium citrate, sodium
chloride,andcitricacid. • Single-dose vials containing 40,000Units of PROCRIT also
contain sodium phosphate monobasic monohydrate andsodiumphosphatedibasicanhydrate.
ThisMedicationGuidehasbeenapprovedbytheU.S.FoodandDrugAdministration.
Manufactured by:AmgenInc.OneAmgenCenterDriveThousandOaks,CA91320-1799U.S.A.
Manufactured for:JanssenProducts,LPHorsham,Pennsylvania19044
©JanssenProducts,LP2000PrintedinU.S.A.
Revised:12/2013
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

14
Instructions for UsePROCRIT® (PRO’−KRIT)
(epoetin alfa)
UsetheseInstructionsforUseifyouoryourcaregiverhasbeentrainedtogivePROCRITinjectionsathome.Donotgiveyourselftheinjectionunlessyouhavereceivedtrainingfromyourhealthcareprovider.Ifyouarenotsureaboutgivingtheinjectionoryouhavequestions,askyourhealthcareproviderforhelp.
Before reading these Instructions forUse, read theMedicationGuidethatcomeswithPROCRITforthemostimportantinformationyouneedtoknow.
When you receive your PROCRIT vial and syringesmake surethat: • ThenamePROCRITappearsonthecartonandviallabel. • Theexpirationdateontheviallabelhasnotpassed.Donot
useavialofPROCRITaftertheexpirationdateonthelabel. • ThedosestrengthofthePROCRITvial(numberofUnitsper
mLontheviallabel)isthesameasyourhealthcareproviderprescribed.
• YouunderstandwhatthedosestrengthofPROCRITmeans.PROCRITvialscomeinseveraldosestrengths.Forexample,the dose strength may be described as 10,000 Units/mLon the vial label. This strengthmeans that 10,000Units ofmedicinearecontainedineach1mL(milliliter)ofliquid.YourhealthcareprovidermayalsorefertoamLasa“cc.”OnemListhesameasone“cc.”
• The PROCRIT liquid in the vial is clear and colorless. DonotusePROCRITiftheliquidintheviallooksdiscoloredorcloudy,oriftheliquidhaslumps,flakes,orparticles.
• ThePROCRITvialhasacolorcaponthetopofthevial.DonotuseavialofPROCRITifthecolorcaponthetopofthevialhasbeenremovedorismissing.
• Useonlythetypeofdisposablesyringeandneedlethatyourhealthcareproviderhasprescribed.
• DonotshakePROCRIT.ShakingcouldcausePROCRITnottowork.IfyoushakePROCRIT,thesolutioninthevialmaylookfoamyandshouldnotbeused.
• DonotfreezePROCRIT.DonotuseavialofPROCRITthathasbeenfrozen.
• StorePROCRITintherefrigeratorbetween36°Fto46°F(2°Cto8°C).
• KeepPROCRITawayfromlight. • Single-dosevialsofPROCRITshouldbeusedonlyonetime.
Throwthevialawayafteruseevenifthereismedicineleftinthevial.
• Afterremovingadosefromthemultidosevial,storethevialintherefrigerator(butnotthefreezer).Donotstorethevialformorethan21days.
• Throwawaythemultidosevialasdirectedbyyourhealthcareprovider:
◦ ifthereisnotenoughmedicineleftinthemultidosevialforanotherdose,or
◦ if ithasbeenmorethan21dayssinceyoufirstputaneedleintothemultidosevial.
HowshouldIprepareforaninjectionofPROCRIT? • Alwayskeepanextrasyringeandneedleonhand. • Follow your healthcare provider’s instructions on how to
measureyourdoseofPROCRIT.ThisdosewillbemeasuredinUnitspermLorcc(1mListhesameas1cc).UseasyringethatismarkedintenthsofmL(forexample,0.2mLor0.2cc).UsingthewrongsyringecanleadtoamistakeinyourdoseandyoucouldinjecttoomuchortoolittlePROCRIT.
Only use disposable syringes and needles. Use the syringes and needles only one time and then throw them away as instructed by your healthcare provider.
What do I need to know about the different types of PROCRITvials?PROCRITcomesintwodifferenttypesofvials.
• Single-doseVials • MultidoseVials
ThemultidosevialofPROCRITcontainsthepreservativebenzylalcohol.Benzylalcoholhasbeenshowntocausebraindamage,otherserioussideeffects,anddeathinnewbornandprematurebabies.PROCRITthatcomesinsingle-dosevialsdoesnotcontainbenzylalcohol.
Important: Follow these instructions exactly to help avoidinfections.
Preparing the dose: 1. Remove thevialofPROCRIT from therefrigerator.During
thistime,protectthesolutionfromlight.
2. Donotuseasingle-dosevialofPROCRITmore thanonetime.
3. DonotshakePROCRIT.
4. Gathertheothersuppliesyouwillneedforyour injection(vial, syringe,alcoholwipes,cottonball,andapuncture-proofcontainerforthrowingawaythesyringeandneedle).SeeFigure1.
Figure 1
5. CheckthedateonthePROCRITvialtobesurethatthedrughasnotexpired.
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

15
6. Wash your hands well with soap and water beforepreparingthemedicine.SeeFigure2.
Figure 2
7. Flipofftheprotectivecolorcaponthetopofthevial.Donotremovethegreyrubberstopper.Wipethetopofthegreyrubberstopperwithanalcoholwipe.SeeFigures3and4.
Figure 3 Figure4
8. Checkthepackagecontainingthesyringe.Ifthepackagehas been opened or damaged, do not use that syringe.Throwawaythesyringeinthepuncture-proofdisposablecontainer.Ifthesyringepackageisundamaged,openthepackageandremovethesyringe.
9. Usingasyringeandneedle thathasbeen recommendedbyyourhealthcareprovider, carefully remove theneedlecover. See Figure 5. Then draw air into the syringe bypullingbackontheplunger.Theamountofairdrawnintothesyringeshouldbeequaltotheamount(mLorcc)ofthePROCRITdoseprescribedbyyourhealthcareprovider.SeeFigure6.
Figure 5 Figure 6
10. With the vial on a flat work surface, insert the needlestraight down through the grey rubber stopper of thePROCRITvial.SeeFigure7.
11. Pushtheplungerofthesyringedowntoinjecttheairfromthesyringe into thevialofPROCRIT.Theair injected intothevialwillallowPROCRITtobeeasilywithdrawnintothesyringe.SeeFigure7.
Figure 7
12. Keep theneedle inside thevial.Turn thevialandsyringeupsidedown.BesurethetipoftheneedleisinthePROCRITliquid.Keepthevialupsidedown.SlowlypullbackontheplungertofillthesyringewithPROCRITliquidtothenumber(mLorcc)thatmatchesthedoseyourhealthcareproviderprescribed.SeeFigure8.
Figure 8
13. Keep the needle in the vial. Check for air bubbles in thesyringe.Asmallamountofairisharmless.ToolargeanairbubblewillgiveyouthewrongPROCRITdose.Toremoveairbubbles,gently tap thesyringewithyourfingersuntiltheairbubblesrisetothetopofthesyringe.Slowlypushtheplungeruptoforcetheairbubblesoutofthesyringe.Keep the tipof theneedle in thePROCRIT liquid.Pull theplungerback to thenumberon the syringe thatmatchesyour dose. Check again for air bubbles. If there are stillairbubbles, repeat thestepsabove to remove them.SeeFigures9and10.
Figure 10Figure 9
14. Double-check that you have the correct dose in thesyringe.Laythevialdownonitssidewiththeneedlestillinituntilafteryouhaveselectedandpreparedyoursiteforinjection.
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)

16
Selecting and preparing the injection site: PROCRITcanbeinjectedintoyourbodyusingtwodifferentways(routes) as described below. Follow your healthcare provider’sinstructionsabouthowyoushouldinjectPROCRIT.Inpatientsonhemodialysis,theintravenous(IV)routeisrecommended.
1. Subcutaneous Route: • PROCRITcanbeinjecteddirectlyintoalayeroffatunder
yourskin.Thisiscalledasubcutaneousinjection.Whengiving subcutaneous injections, follow your healthcareprovider’s instructionsaboutchanging thesite foreachinjection.Youmaywishtowritedownthesitewhereyouhaveinjected.
• Do not inject PROCRIT into an area that is tender,red, bruised, hard, or has scars or stretch marks.RecommendedsitesforinjectionareshowninFigure11below,including:
◦ Theouterareaoftheupperarms ◦ Theabdomen(except for the2-inchareaaround the
navel) ◦ Thefrontofthemiddlethighs ◦ Theupperouterareaofthebuttocks
Figure 11
• Cleantheskinwithanalcoholwipewheretheinjectionistobemade.Becarefulnottotouchtheskinthathasbeenwipedclean.SeeFigure12.
Figure 12
• Double-check that thecorrectamountofPROCRIT is inthesyringe.
• RemovethepreparedsyringeandneedlefromthevialofPROCRITandholditinthehandthatyouwillusetoinjectthemedicine.
• Usetheotherhandtopinchafoldofskinatthecleanedinjectionsite.Donottouchthecleanedareaofskin.SeeFigure13.
Figure 13
• Holdthesyringelikeyouwouldholdapencil.Useaquick“dart-like” motion to insert the needle either straightup and down (90-degree angle) or at a slight angle(45 degrees) into the skin. Inject the prescribed dosesubcutaneously as directed by your doctor, nurse orpharmacist.SeeFigure14.
Figure14
• Pulltheneedleoutoftheskinandpressacottonballorgauzeovertheinjectionsiteandholditthereforseveralseconds.Donotrecaptheneedle.
• Dispose of the used syringe and needle as describedbelow.Donotreusesyringesandneedles.
2. Intravenous Route: • PROCRITcanbe injected inyourveinthroughaspecial
access port placed by your healthcare provider. Thistype of PROCRIT injection is called an intravenous (IV)injection.Thisrouteisusuallyforhemodialysispatients.
• If you have a dialysis vascular access,make sure it isworkingbychecking itasyourhealthcareproviderhasshownyou.Besuretoletyourhealthcareproviderknowrightawayifyouarehavinganyproblems,orifyouhaveanyquestions.
• Wipeoffthevenousportofthehemodialysistubingwithanalcoholwipe.SeeFigure15.
Figure 15
PROCRIT® (epoetin alfa) PROCRIT® (epoetin alfa)
17
• Inserttheneedleofthesyringeintothecleanedvenousportandpushtheplungerall thewaydownto injectallthePROCRIT.SeeFigure16.
Figure 16
• Removethesyringefromthevenousport.Donotrecaptheneedle.
• Dispose of the used syringe and needle as describedbelow.
HowshouldIdisposeofthevials,syringes,andneedles?Donot reuse thesingle-dosevials, syringes,orneedles. Throwaway the vials, syringes, and needles as instructed by yourhealthcareproviderorbyfollowingthesesteps:
• Do not throw the vials, syringes, or needles in thehouseholdtrashorrecycle.
• Donotputtheneedlecoverbackontheneedle. • Placeallusedneedlesandsyringesinapuncture-proof
disposablecontainerwithalid.Donotuseglassorclearplasticcontainers,oranycontainerthatwillberecycledorreturnedtoastore.
• Keepthepuncture-proofdisposablecontaineroutofthereachofchildren.
• When the puncture-proof disposable container is full,tapearoundthecaporlidtomakesurethecaporliddoesnotcomeoff.Throwawaythepuncture-proofdisposablecontainer as instructed by your healthcare provider.Theremaybespecialstateandlocallawsfordisposingofusedneedlesandsyringes.Donotthrowthepuncture-proof disposable container in the household trash. Do not recycle.
Keep PROCRIT and all medicines out of reach of children.
TheseInstructionsforUsehavebeenapprovedbytheU.S.FoodandDrugAdministration.
Manufactured by:AmgenInc.OneAmgenCenterDriveThousandOaks,CA91320-1799U.S.A.
Manufactured for:JanssenProducts,LPHorsham,Pennsylvania19044
©JanssenProducts,LP2000PrintedinU.S.A.
Revised:05/2012
008342-150209
PROCRIT® (epoetin alfa)





























