Embed Size (px)
Citation preview

Update in Anaesthesia123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901123456789012345678901234567890121234567890123456789012345678901212345678901
A journal for anaesthetists in developing countries
Contents: No 3
EditorialSpinal anaesthesiaPhysiology - Control of Heart RateDrawover anaesthesia - Practical Aspects
- Equipment CarePharmacology - MorphineClinical DilemmaEquipment - Aneroid Sphygmomanometer
EDITORIAL
spinal anaesthesia. There is an art, a skill associatedwith learning to ride a bicycle or learning anyanaesthetic technique. But practice makes perfect.The more spinal anaesthetics one gives, the easierthey are to give and the greater the level of success.Any truly competent anaesthetist, physician orparamedical, must be expert in spinal anaesthesiaas well as in general anaesthesia if the manifestadvantages of spinal anaesthesia are to be providedto all patients. The anaesthetist not fully comfortablewith spinal anaesthesia should attain the requisitelevel of competence by purposefully giving spinalsevery time he or she can reasonably do so, even ifspinal anaesthesia may not be the only anaesthetictechnique indicated. By giving spinal anaesthesiaeven once or, better, twice a week, the anaesthetistwill, by the end of the year, be an expert whose skillis requested for patients in whom spinal anaesthesiais the technique of choice. The anaesthetist whoknows how to give a good spinal will also enjoy amore rewarding and professionally interesting day-to-day practice.
Instead of giving the same general anaesthetic 500times a year, he or she will enjoy the professionalstimulation of varying the type of anaesthesia based
Editors: Drs Iain Wilson, Roger Eltringham Section Editors: Drs Bill Casey, Ian Kestin, Mr Mike YeatsOverseas Editors: Drs Jill Bem (Zambia), Henry Bukwirwa (Uganda) Distribution: Dr Sarah Jane Fearnley
Illustrations & Graphics: Angela Frost
1
The Role of Spinal Anaesthesia in DevelopingCountries.
Professor Nicholas M Greene, Dept. ofAnaesthesiology, School of Medicine, YaleUniversity, USA
Regional anaesthesia, although popular in certaincentres in developing countries, is generally poorlyaccepted in these areas as a reliable, economicalmeans for providing operative anaesthesia. Perhapsthis is understandable in the case of complicatednerve blocks such as ankle blocks and femoral andsciatic blocks for operations below the knee. Thismay also be understandable for blocks of lumbarplexus or of the brachial plexus using thesupraclavicular approach. The same may be saidfor continuous spinal or epidural techniques thatrequire catheters both hard to obtain and expensive.But failure of single-injection spinal anaesthetictechniques to achieve richly deserved popularity isdifficult to understand given the obvious advantageswith which such simple, straightforward, effective,safe and even inexpensive techniques are associated.
The present "mini-review" of spinal anaesthesiaoffered by Drs. Ankorn and Casey is such a paragonof lucidity, completeness, and good common senseas to be beyond the need for trivial tinkering oramplification. It says what needs to be said andleaves unsaid what needs not to be said. It isrecommended for close reading by anaesthetistseverywhere but perhaps especially those indeveloping areas where spinal is so infrequentlyemployed.
There is, undeniably, an art, a skill associated with
UPDATE INANAESTHESIAWORLD
ANAESTHESIA
WA
No 3 1993

Update in Anaesthesia2
on patient condition, type of operation proposed,and the quiet self-confidence that comes withexperience using the champagne of anaesthetics:
spinal anaesthesia. How to attain this requisite levelof skill and art is neatly described in this update onthe subject. Read it and believe it.
SPINAL ANAESTHESIA - A Practical Guide
Dr Chris Ankcorn, Lecturer in Anaesthesia, Kumasi,Ghana
Dr William F Casey FRCA, Consultant Anaesthetist,Gloucestershire Royal Hospital, Gloucester, UK
Spinal anaesthesia is induced by injecting smallamounts of local anaesthetic into the cerebro-spinalfluid (CSF). The injection is usually made in thelumbar spine below the level at which the spinalcord ends (L2). Spinal anaesthesia is easy to performand has the potential to provide excellent operatingconditions for surgery below the umbilicus.
If the anaesthetist has an adequate knowledge ofthe relevant anatomy, physiology andpharmacology, safe and satisfactory anaesthesiacan easily be obtained to the mutual satisfaction ofthe patient, surgeon and anaesthetist.
The Advantages of Spinal Anaesthesia
Cost. Anaesthetic drugs and gases are costly andthe latter often difficult to transport. The costsassociated with spinal anaesthesia are minimal.
Patient satisfaction. If a spinal anaesthetic and theensuing surgery are performed skillfully, themajority of patients are very happy with thetechnique and appreciate the rapid recovery andabsence of side-effects.
Respiratory disease. Spinal anaesthesia producesfew adverse effects on the respiratory system aslong as unduly high blocks are avoided.
Patent airway. As control of the airway is notcompromised, there is a reduced risk of airwayobstruction or the aspiration of gastric contents.This advantage may be lost with too much sedation.
Diabetic patients. There is little risk ofunrecognised hypoglycaemia in an awake patient.Diabetic patients can usually return to their normalfood and insulin regime soon after surgery as thereis less sedation, nausea and vomiting.
Muscle relaxation. Spinal anaesthesia providesexcellent muscle relaxation for lower abdominaland lower limb surgery.
Bleeding. Blood loss during operation is less thanwhen the same operation is done under generalanaesthesia. This is as a result of a decreased bloodpressure and heart rate, and improved venousdrainage which results in less oozing.
Splanchnic blood flow. Because of its effect onincreasing blood flow to the gut, spinal anaesthesiareduces the incidence of anastomotic dehiscence.
Visceral tone. The bowel is contracted by spinalanaesthesia and sphincters relaxed althoughperistalsis continues. Normal gut function rapidlyreturns following surgery.
Coagulation. Post-operative deep vein thrombosesand pulmonary emboli are less common followingspinal anaesthesia.
Disadvantages of Spinal Anaesthesia
1. When an anaesthetist is learning a new technique,it will take longer to perform than when he is morepractised, and it would be wise to let the surgeonknow that induction of anaesthesia may be longerthan usual. Once competent, however, spinalanaesthesia can be very swiftly performed.
2. Occasionally, it is impossible to locate the duralspace and obtain CSF and the technique has to beabandoned. Rarely, despite an apparently faultlesstechnique, anaesthesia is not obtained.
3. Hypotension may occur with higher blocks andthe anaesthetist must know how to manage thissituationsituation with the necessary resuscitativedrugs and equipment immediately to hand. As withgeneral anaesthesia, continuous, close monitoringof the patient is mandatory.
4. Some patients are not psychologically suited tobe awake, even if sedated, during an operation.They should be identified during the preoperativeassessment.
5. Even if a long-acting local anaesthetic is used, aspinal is not suitable for surgery lasting longer thanapproximately 2 hours. If an operation unexpectedlylasts longer than this, it may be necessary to convertto a general anaesthetic.

Update in Anaesthesia 3
6. There is a theoretical risk of introducing infec-tion into the subarachnoid space and causing men-ingitis. This should never happen if equipment issterilised properly and an aseptic technique is used.
7. A postural headache may occur postoperatively.This should be rare: see later.
Indications for Spinal Anaesthesia
Spinal anaesthesia is best reserved for operationsbelow the umbilicus e.g. hernia repairs, gynaeco-logical and urological operations and any operationon the perineum or genitalia. All operations on theleg are possible, but an amputation, though pain-less, may be an unpleasant experience for an awakepatient. In this situation it may be kinder to supple-ment the spinal with generous sedation or a lightgeneral anaesthetic.
Spinal anaesthesia is especially indicated for olderpatients and those with systemic disease such aschronic respiratory disease, hepatic, renal and en-docrine disorders such as diabetes. Most patientswith mild cardiac disease benefit from thevasodilation that accompanies spinal anaesthesiaexcept those with stenotic valvular disease or un-controlled hypertension.
It is suitable for managing patients with trauma ifthey have been adequately resuscitated and are nothypovolaemic. In obstetrics, it is ideal for manualremoval of a retained placenta (again, providedthere is no hypovolaemia). There are definite advan-tages for both mother and baby in using spinalanaesthesia for Caesarean section. However, spe-cial considerations apply to managing spinal an-aesthesia in pregnant patients (see later) and it isbest to become experienced in its use in the non-pregnant patient before using it for obstetrics.
Contra-indications to Spinal Anaesthesia
Most of the contra-indications to spinal anaesthesiaapply equally to other forms of regional anaesthe-sia. These include:
Inadequate resuscitative drugs and equipment.No regional anaesthetic technique should be at-tempted if drugs and equipment for resuscitationare not immediately to hand.
Clotting disorders. If bleeding occurs into theepidural space because an epidural vein has beenpunctured by the spinal needle, a haematoma couldform and compress the spinal cord. Patients with alow platelet count or receiving anticoagulant drugssuch as heparin or warfarin are at risk. Rememberthat patients with liver disease may have abnormalclotting profiles whilst low platelet counts as wellas abnormal clotting can occur in pre-eclampsia.
Hypovolaemia from whatever cause e.g. bleeding,dehydration due to vomiting, diarrhoea or bowelobstruction. Patients must be adequately rehydratedor resuscitated before spinal anaesthesia or theywill become very hypotensive.
Any sepsis on the back near the site of lumbarpuncture.
Patient refusal. Patients may be understandablyapprehensive and initially state a preference forgeneral anaesthesia, but if the advantages of spinalanaesthesia are explained they may then agree tothe procedure and be pleasantly surprised at theoutcome. If, despite adequate explanation, thepatient still refuses spinal anaesthesia, their wishesshould be respected.
Uncooperative patients. Although spinalanaesthesia is suitable for children, their cooperationis necessary and this must be carefully assessed atthe pre-operative visit. Likewise, mentallyhandicapped patients and those with psychiatricproblems need careful pre-operative assessment.
Septicaemia. Due to the presence of infection inthe blood there is a possiblity of such patientsdeveloping meningitis if a haematoma forms at thesite of lumbar puncture and becomes infected.
Anatomical deformities of the patient’s back.This is a relative contraindication, as it will probablyonly serve to make the dural puncture more difficult.
Neurological disease. The advantages anddisadvantages of spinal anaesthesia in the presenceof neurological disease need careful assessment.Any worsening of the disease postoperatively maybe blamed erroneously on the spinal anaesthetic.Raised intracranial pressure, however, is an absolutecontra-indication as a dural puncture may precipitateconing of the brain stem.

Update in Anaesthesia4
Reluctant surgeon. If a surgeon is unhappyoperating on an awake patient or if he is relativelyunskilled, spinal anaesthesia may be better avoided.
Physiology of Spinal Anaesthesia
Local anaesthetic solution injected into thesubarachnoid space blocks conduction of impulsesalong all nerves with which it comes in contact,although some nerves are more easily blocked thanothers.
There are three classes of nerve: motor, sensory andautonomic. The motor convey messages for musclesto contract and when they are blocked, muscleparalysis results. Sensory nerves transmit sensationssuch as touch and pain to the spinal cord and fromthere to the brain, whilst autonomic nerves controlthe calibre of blood vessels, heart rate, gutcontraction and other functions not under consciouscontrol.
Generally, autonomic and pain fibres are blockedfirst and motor fibres last. This has several importantconsequences. For example, vasodilation and adrop in blood pressure may occur when theautonomic fibres are blocked and the patient maybe aware of touch and yet feel no pain when surgerystarts.
There are practical implications associated withthese physiological phenomena.
- The patient should be well hydrated before thelocal anaesthetic is injected and should have anintravenous infusion in place so that further fluidsor vasoconstrictors can be given if hypotensionoccurs.
- The site to be operated on should not be repeatedlytouched and the patient asked "Can you feel this?"as this increases the patient’s anxiety. Often somesensation of touch or movement remains and yetno pain is felt. It is better to pinch the skin gentlyeither with artery forceps or fingers and ask if it ispainful. If it is not then surgery can begin.
Anatomy
The spinal cord usually ends at the level of L2 inadults and L3 in children. Dural puncture abovethese levels is associated with a slight risk ofdamaging the spinal cord and is best avoided. Animportant landmark to remember is that a linejoining the top of the iliac crests is at L4 to L4/5
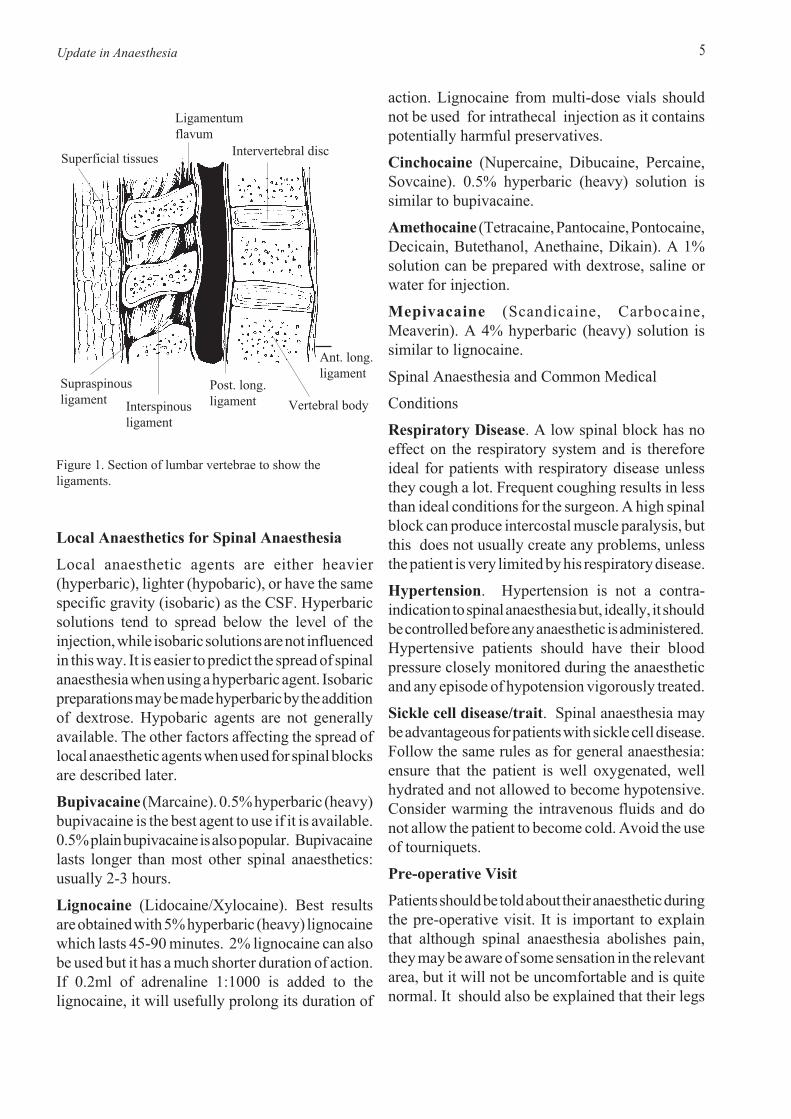
Remember the structures that the needle will piercebefore reaching the CSF (fig 1.).
The skin. It is wise to inject a small bleb of localanaesthetic into the skin before inserting the spinalneedle.
Subcutaneous fat. This, of course, is of variablethickness. Identifying the intervertebral spaces isfar easier in thin patients.
The supraspinous ligament which joins the tips ofthe spinous processes together.
The interspinous ligament which is a thin flatband of ligament running between the spinousprocesses.
The ligamentum flavum is quite thick, up to about1cm in the middle and is mostly composed ofelastic tissue. It runs vertically from lamina tolamina. When the needle is within the ligaments itwill feel gripped and a distinct "give" can often befelt as it passes through and into the epidural space.
The epidural space contains fat and blood vessels.If blood comes out of the spinal needle instead ofCSF when the stylet is removed, it is likely that anepidural vein has been punctured. The needle shouldsimply be advanced a little further.
The dura. After feeling a "give" as the needlepasses through the ligamentum flavum, a similarsensation may be felt when the needle is advanceda short distance further and pierces the dural sac.
The subarachnoid space. This contains the spinalcord and nerve roots surrounded by CSF. Aninjection of local anaesthetic will mix with the CSFand rapidly block the nerve roots with which itcomes in contact.
Update in Anaesthesia 5
Figure 1. Section of lumbar vertebrae to show theligaments.
Ligamentumflavum
Superficial tissuesIntervertebral disc
Ant. long.ligament
Vertebral body
Post. long.ligamentInterspinous
ligament
Supraspinousligament
Local Anaesthetics for Spinal Anaesthesia
Local anaesthetic agents are either heavier(hyperbaric), lighter (hypobaric), or have the samespecific gravity (isobaric) as the CSF. Hyperbaricsolutions tend to spread below the level of theinjection, while isobaric solutions are not influencedin this way. It is easier to predict the spread of spinalanaesthesia when using a hyperbaric agent. Isobaricpreparations may be made hyperbaric by the additionof dextrose. Hypobaric agents are not generallyavailable. The other factors affecting the spread oflocal anaesthetic agents when used for spinal blocksare described later.
Bupivacaine (Marcaine). 0.5% hyperbaric (heavy)bupivacaine is the best agent to use if it is available.0.5% plain bupivacaine is also popular. Bupivacainelasts longer than most other spinal anaesthetics:usually 2-3 hours.
Lignocaine (Lidocaine/Xylocaine). Best resultsare obtained with 5% hyperbaric (heavy) lignocainewhich lasts 45-90 minutes. 2% lignocaine can alsobe used but it has a much shorter duration of action.If 0.2ml of adrenaline 1:1000 is added to thelignocaine, it will usefully prolong its duration of
action. Lignocaine from multi-dose vials shouldnot be used for intrathecal injection as it containspotentially harmful preservatives.
Cinchocaine (Nupercaine, Dibucaine, Percaine,Sovcaine). 0.5% hyperbaric (heavy) solution issimilar to bupivacaine.
Amethocaine (Tetracaine, Pantocaine, Pontocaine,Decicain, Butethanol, Anethaine, Dikain). A 1%solution can be prepared with dextrose, saline orwater for injection.
Mepivacaine (Scandicaine, Carbocaine,Meaverin). A 4% hyperbaric (heavy) solution issimilar to lignocaine.
Spinal Anaesthesia and Common Medical
Conditions
Respiratory Disease. A low spinal block has noeffect on the respiratory system and is thereforeideal for patients with respiratory disease unlessthey cough a lot. Frequent coughing results in lessthan ideal conditions for the surgeon. A high spinalblock can produce intercostal muscle paralysis, butthis does not usually create any problems, unlessthe patient is very limited by his respiratory disease.
Hypertension. Hypertension is not a contra-indication to spinal anaesthesia but, ideally, it shouldbe controlled before any anaesthetic is administered.Hypertensive patients should have their bloodpressure closely monitored during the anaestheticand any episode of hypotension vigorously treated.
Sickle cell disease/trait. Spinal anaesthesia maybe advantageous for patients with sickle cell disease.Follow the same rules as for general anaesthesia:ensure that the patient is well oxygenated, wellhydrated and not allowed to become hypotensive.Consider warming the intravenous fluids and donot allow the patient to become cold. Avoid the useof tourniquets.
Pre-operative Visit
Patients should be told about their anaesthetic duringthe pre-operative visit. It is important to explainthat although spinal anaesthesia abolishes pain,they may be aware of some sensation in the relevantarea, but it will not be uncomfortable and is quitenormal. It should also be explained that their legs

Update in Anaesthesia6
will become weak or feel as if they don’t belong tothem any more. They must be reassured that, if theyfeel pain they will be given a general anaesthetic.
Premedication is not always necessary, but if apatient is apprehensive, a benzodiazepine such as5-10 mg of diazepam may be given orally 1 hourbefore the operation. Other sedative or narcoticagents may also be used. Anticholinergics such asatropine or scopolamine (hyoscine) are unnecessary.
Pre-loading
All patients having spinal anaesthesia must have alarge intravenous cannula inserted and be givenintravenous fluids immediately before the spinal.The volume of fluid given will vary with the age ofthe patient and the extent of the proposed block. Ayoung, fit man having a hernia repair may onlyneed 500 mls. Older patients are not able tocompensate as efficiently as the young for spinal-induced vasodilation and hypotension and mayneed 1000mls for a similar procedure. If a highblock is planned, at least a 1000mls should be givento all patients. Caesarean section patients need atleast 1500 mls.
The fluid should preferably be normal saline orHartmann’s solution. 5% dextrose is readilymetabolised and so is not effective in maintainingthe blood pressure.
Positioning the Patient for Lumbar Puncture
Lumbar puncture is most easily performed whenthere is maximum flexion of the lumbar spine.
Figure 2. Effect of flexion and extension on the lumbarintervertebral space in the lumbar region.
This can best be achieved by sitting the patient onthe operating table and placing their feet on a stool.If they then rest their forearms on their thighs, theycan maintain a stable and comfortable position.
Figure 3. Ideal sitting position for spinal anaesthesia.
Alternatively, the procedure can be performed withthe patient lying on their side with their hips andknees maximally flexed. An assistant may help tomaintain the patient in a comfortable curled position.The sitting position is preferable in the obesewhereas the lateral is better for uncooperative orsedated patients. The anaesthetist can either sit orkneel whilst performing the block.
Flexion
Extension
Crestof
ileumL 5
L 3L 4

Update in Anaesthesia
Figure 4. Note how the level of the subarachnoid spacevaries between male and female
Although the level of injection will obviously effectwhich dermatomes are blocked, spinal injectionstend to be performed only in the lower lumbarregion. The extent of the block is influenced moreby the volume injected and the position of thepatient than the actual interspace at which theinjection occurs.
The speed of injection has a slight effect on theeventual extent of the block. Slow injections resultin a more predictable spread while rapid injectionsproduce eddy currents within the CSF and asomewhat less predictable outcome.
Finally, increased abdominal pressure fromwhatever cause (pregnancy, ascites etc) can lead toengorgement of the epidural veins, compression ofthe dura and hence a reduction in the volume of theCSF. A given quantity of local anaesthetic injectedinto the CSF might then be expected to produce amore extensive block.
7
Hips vertical
Female
Male
Knees drawn up to chestFactors Effecting the Spread of the LocalAnaesthetic Solution
A number of factors effect the spread of the injectedlocal anaesthetic solution within the CSF and theultimate extent of the block obtained. Among theseare:
- the baricity of the local anaesthetic solution
- the position of the patient
- the concentration and volume injected
- the level of injection
- the speed of injection
The specific gravity of the local anaesthetic solutioncan be altered by the addition of dextrose.Concentrations of 7.5% dextrose make the localanaesthetic hyperbaric (heavy) relative to CSF andalso reduce the rate at which it diffuses and mixeswith the CSF. Isobaric and hyperbaric solutionsboth produce reliable blocks. The most controllableblocks are probably produced by injectinghyperbaric solutions and then altering the patient’sposition.
If a patient is kept sitting for several minutes afterthe injection of a small volume of a hyperbaricsolution of local anaesthetic, a classical saddleblock of the perineum will result. The spinal columnof patients lying on their side is rarely trulyhorizontal. Males tend to have wider shouldersthan hips and so are in a slight "head up" positionwhen lying on their sides, whilst for females withtheir wider hips, the opposite is true. Regardless ofthe position of the patient at the time of injectionand whatever the initial extent of the block obtained,the level of the block may change if the patient’sposition is altered within twenty minutes of theinjection.
The quantity of local anaesthetic (in milligrams)injected will determine the quality of the blockobtained whilst its extent will also be determinedby the volume in which it is injected. Large volumesof concentrated solutions will, thus, produce denseblockade over a large area.
Shoulders verticalBack in flexionat edge of table

Update in Anaesthesia8
Quantities of Local Anaesthetics to Use
The degree of spinal blockade needed, as measuredby the height of the block, will depend on theoperation to be performed.
Table 1.
Level Surgical Procedure
T4-5 (Nipple) Upper abdominal surgeryT6-8 (Xiphisternum) Lower abdominal surgery incl.
caesarean section, renalsurgery, hernia
T10 (Umbilicus) Prostatic and vaginal surgeryincl. forceps delivery, hipsurgery
L1 (Groin) Lower limb surgeryS2 (Perineum) Perineal and rectal surgery
For certain blocks, less local anaesthetic is neededwhen hyperbaric rather than plain solutions areused. Special considerations apply to obstetricpatients and so the following chart does not applyto them (see later section).
The volumes of local anaesthetic shown in Table 2should be considered only as a guideline. The lowervolumes suggested should generally be injected inparticularly small people. More may have to begiven if the resultant block is not high enough forthe proposed operation. Hyperbaric agents are morereliable when trying for a mid-thoracic block.
Preparation for Lumbar Puncture
Assemble the necessary equipment on a sterilesurface. It will include:
A spinal needle. The ideal would be 24-25 gaugewith a pencil point tip to minimise the risk of thepatient developing a post-spinal headache.
An introducer, if using a fine gauge needle as theyare thin and flexible, and therefore difficult todirect accurately. A standard 19 gauge (white)disposable needle is suitable for use as an introducer.
A 5ml syringe for the spinal anaesthetic solution.
A 2 ml syringe for local anaesthetic to be used forskin infiltration.
A selection of needles for drawing up the localanaesthetic solutions and for infiltrating the skin.
A gallipot with a suitable antiseptic for cleaningthe skin, eg chlorhexidine, iodine, or methyl alcohol.
Sterile gauze swabs for skin cleansing.
A sticking plaster to cover the puncture site.L5 S1
L5 S1,2
L 2 , 5S 2 , 3
L 1
C8 TH1
C 6 , 7 , 8
C 5 , 6
C8 TH1C 5 , 6
C 2
C 2 , 3C 3 , 4
T H 6T H 5T H 4T H 3T H 2
T H 7TH8T H 9TH10
T H 1 2T H 1 1
C5 , 6
T H 2
T H 1 , 2
L 1 2
L 3 , 4
L4 , 5
S 1 , 2
Figure 5. Diagram of dermatones
Table 2.
Type of block Hyperbaric Plain Hyperbaric Bupivacaine Bupivacaine Lignocaine
Saddle block, 2ml 3ml 1mleg operationson genitalia,perineum
Lumbar block, 3-3.5ml 3-3.5ml 2mleg operationson legs
Mid-thoracic 3-4ml 3-4ml 2mlblock, eg hernia,hysterectomy
Update in Anaesthesia
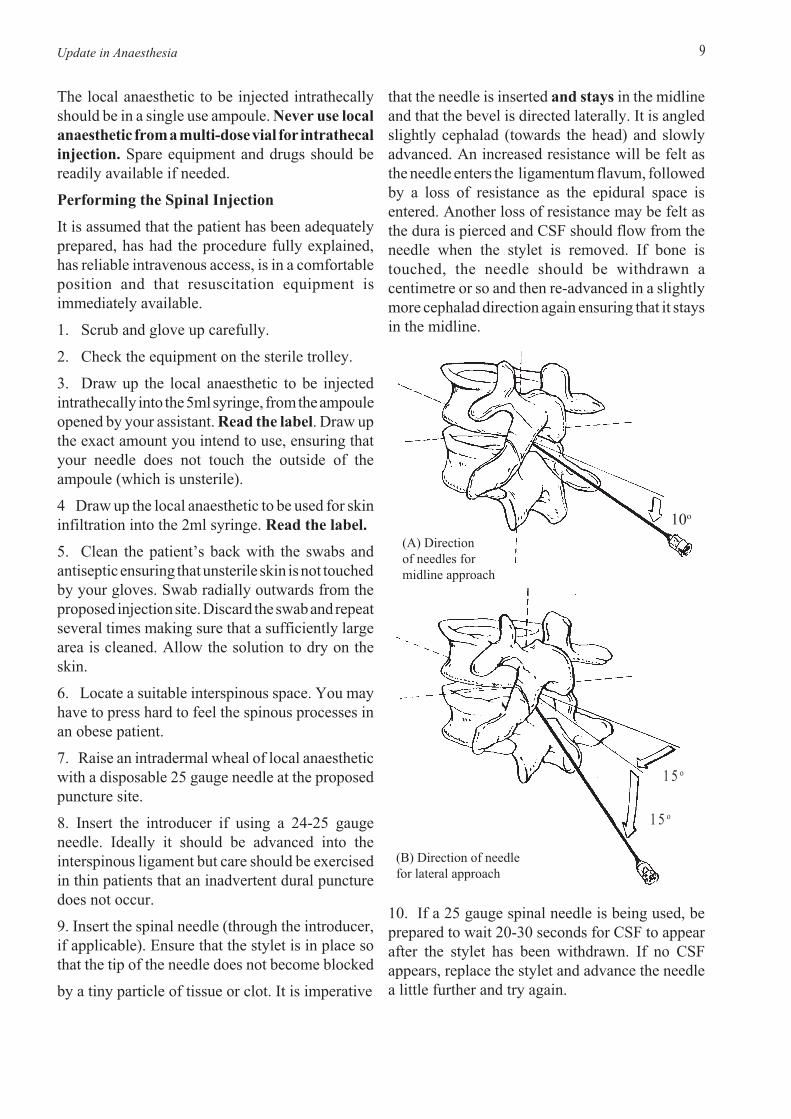
that the needle is inserted and stays in the midlineand that the bevel is directed laterally. It is angledslightly cephalad (towards the head) and slowlyadvanced. An increased resistance will be felt asthe needle enters the ligamentum flavum, followedby a loss of resistance as the epidural space isentered. Another loss of resistance may be felt asthe dura is pierced and CSF should flow from theneedle when the stylet is removed. If bone istouched, the needle should be withdrawn acentimetre or so and then re-advanced in a slightlymore cephalad direction again ensuring that it staysin the midline.
10. If a 25 gauge spinal needle is being used, beprepared to wait 20-30 seconds for CSF to appearafter the stylet has been withdrawn. If no CSFappears, replace the stylet and advance the needlea little further and try again.
9
The local anaesthetic to be injected intrathecallyshould be in a single use ampoule. Never use localanaesthetic from a multi-dose vial for intrathecalinjection. Spare equipment and drugs should bereadily available if needed.
Performing the Spinal Injection
It is assumed that the patient has been adequatelyprepared, has had the procedure fully explained,has reliable intravenous access, is in a comfortableposition and that resuscitation equipment isimmediately available.
1. Scrub and glove up carefully.
2. Check the equipment on the sterile trolley.
3. Draw up the local anaesthetic to be injectedintrathecally into the 5ml syringe, from the ampouleopened by your assistant. Read the label. Draw upthe exact amount you intend to use, ensuring thatyour needle does not touch the outside of theampoule (which is unsterile).
4 Draw up the local anaesthetic to be used for skininfiltration into the 2ml syringe. Read the label.
5. Clean the patient’s back with the swabs andantiseptic ensuring that unsterile skin is not touchedby your gloves. Swab radially outwards from theproposed injection site. Discard the swab and repeatseveral times making sure that a sufficiently largearea is cleaned. Allow the solution to dry on theskin.
6. Locate a suitable interspinous space. You mayhave to press hard to feel the spinous processes inan obese patient.
7. Raise an intradermal wheal of local anaestheticwith a disposable 25 gauge needle at the proposedpuncture site.
8. Insert the introducer if using a 24-25 gaugeneedle. Ideally it should be advanced into theinterspinous ligament but care should be exercisedin thin patients that an inadvertent dural puncturedoes not occur.
9. Insert the spinal needle (through the introducer,if applicable). Ensure that the stylet is in place sothat the tip of the needle does not become blocked
by a tiny particle of tissue or clot. It is imperative
10o
(A) Directionof needles formidline approach
(B) Direction of needlefor lateral approach
1 5 o
1 5 o

Update in Anaesthesia10
This is performed by inserting the spinal needleabout 1cm lateral to the mid line at the level of theupper border of a spinous process, then directing itboth cephalad and medially. If bone is contacted itis likely to be the vertebral lamina. It should then bepossible to "walk" the needle off the bone and intothe epidural space, then advance through it topierce the dura (fig. 6 ).
Assessing the Block
Some patients are very poor at describing what theydo or do not feel, therefore, objective signs arevaluable. If, for example, the patient is unable to lifthis legs from the bed, the block is at least up to themid-lumbar region.
It is unnecessary to test sensation with a sharpneedle and leave the patient with a series of bleedingpuncture wounds. It is better to test for a loss oftemperature sensation using a swab soaked in eitherether or alcohol. Do this by first touching thepatient with the damp swab on the chest or arm(where sensation is normal), so that they appreciatethat the swab feels cold. Then work up from the legsand lower abdomen until the patient againappreciates that the swab feels cold.
If the replies are inconsistent or equivocal, thepatient can be gently pinched with artery forceps orfingers on blocked and unblocked segments andasked if they feel pain. Using this method, there israrely any difficulty in ascertaining the extent of theblock.
Surgeons should be dissuaded from prodding thepatient and asking "can you feel this?". Surgeonsand patients should be reminded that when a blockis successful, a patient may still be aware of touchbut will not feel pain.
Problems with the Block
No apparent block at all. If after 10 minutes thepatient still has full power in the legs and normalsensation, then the block has failed probably becausethe injection was not intrathecal. Try again.
The block is one-sided or is not high enough onone side.
a). When using a hyperbaric solution, lie the patienton the side that is inadequately blocked for a fewminutes and adjust the table so that the patient isslightly "head down".
11. When CSF appears, take care not to alter theposition of the spinal needle as the syringe of localanaesthetic is being attached. The needle is bestimmobilised by resting the back of the non-dominanthand firmly against the patient and by using thethumb and index finger to hold the hub of theneedle. Be sure to attach the syringe firmly to thehub of the needle; hyperbaric solutions are viscousand resistance to injection will be high, especiallythrough fine gauge needles. It is, therefore, easy tospill some of the local anaesthetic unless care istaken.
12. Aspirate gently to check the needle tip is stillintrathecal and then slowly inject the localanaesthetic. When the injection is complete,withdraw the spinal needle, introducer and syringeas one and apply a sticking plaster to the puncturesite.
Practical Problems
The spinal needle feels as if it is in the rightposition but no CSF flows. Wait at least 30seconds, then try rotating the needle 90 degrees andwait again. If there is still no CSF, attach an empty2ml syringe and inject 0.5-1ml of air to ensure theneedle is not blocked then use the syringe to aspiratewhilst slowly withdrawing the spinal needle. Stopas soon as CSF appears in the syringe.
Blood flows from the spinal needle. Wait a shorttime. If the blood becomes pinkish and finallyclear, all is well. If blood only continues to drip,then it is likely that the needle tip is in an epiduralvein and it should be advanced a little further orangled more medially to pierce the dura.
The patient complains of sharp, stabbing legpain. The needle has hit a nerve root because it hasdeviated laterally. Withdraw the needle and redirectit more medially away from the affected side.
Wherever the needle is directed, it seems tostrike bone. Make sure the patient is still properlypositioned with as much lumbar flexion as possibleand that the needle is still in the mid-line. If youthink that you are not in the midline check with thepatient which side they feel the needle. Alternatively,if the patient is elderly and cannot bend very muchor has heavily calcified interspinous ligaments, itmight bebetter to attempt a lateral approach to thedura.

Update in Anaesthesia 1 1
b). When using an isobaric solution, lie the patienton the side that is blocked. (Moving a patientaround in any way at all in the first 10-20 minutesfollowing injection will tend to increase the heightof the block).
Block not high enough.
a). When using a hyperbaric solution, tilt thepatient head down whilst they are supine (lying onthe back), so that the solution can run up the lumbarcurvature. Flatten the lumbar curvature by raisingthe patients knees.
b). When using a plain solution turn the patient acomplete circle from supine to prone (lying on thefront) and back to supine again.
Block too high. The patient may complain ofdifficulty in breathing or tingling in the arms orhands. Do not tilt the table "head up". (See laterunder ‘Treatment of a total spinal.’)
Nausea or vomiting. This may occur with highspinal blocks which may be associated withhypotension. Check the blood pressure and treataccordingly. (See later)
Shivering. This occurs occasionally. Reassure thepatient and give oxygen by mask.
Monitoring
It is essential to monitor the respiration, pulse andblood pressure closely. The blood pressure can fallprecipitously following induction of spinalanaesthesia, particularly in the elderly and thosewho have not been adequately preloaded with fluid.Warning signs of falling blood pressure includepallor, sweating or complaining of nausea or feelinggenerally unwell.
A moderate fall in systolic blood pressure to, say,80mmHg in a young fit patient or 100mmHg in anolder patient is acceptable, provided the patientlooks and feels well and is adequately oxygenated.
Bradycardia is quite common during spinalanaesthesia particularly if the surgeon ismanipulating the bowel or uterus. If the patientfeels well, and the blood pressure is maintained,then it is not necessary to give atropine. If, however,the heart rate drops below 50 beats per minute orthere is hypotension, then atropine 300-600mcgshould be given intravenously.
It is generally considered good practice for allpatients undergoing surgery under spinalanaesthesia to be given supplemental oxygen byface mask at a rate of 2-4 litres/minute, especiallyif sedation has also been given.
Treatment of Hypotension
Hypotension is due to vasodilation and a functionaldecrease in the effective circulating volume. Thetreatment is, therefore, to reverse the vasodilatationwith vasoconstrictor drugs and increase thecirculating volume by giving fluids. All hypotensivepatients should be given OXYGEN by mask untilthe blood pressure is restored.
A simple and effective way of rapidly increasingthe patient’s circulating volume is by raising theirlegs thus increasing the return of venous blood tothe heart. This can either be done manually by anassistant or by tilting the lower half of the operatingtable. Tilting the whole operating table head downwill also achieve the same effect, but is unwise if ahyperbaric spinal anaesthetic has been injected inthe preceding 15 minutes as it will result in theblock spreading higher and the hypotensionbecoming more severe. If an isobaric spinalsolution has been used, tilting the table at any timewill have very little effect on the height of the block.
Increase the speed of the intravenous infusion tomaximum until the blood pressure is restored toacceptable levels and, if the pulse is slow, giveatropine intravenously. Vasoconstrictors should begiven immediately if the hypotension is severe, andto patients not responding to fluid therapy.
Vasopressors
Ephedrine is probably the vasopressor of choice.It causes peripheral blood vessels to constrict andraises the cardiac output by increasing the heart rateand the force of myocardial contraction. It is safefor use in pregnancy as it does not reduce placentalblood flow.
Ephedrine is generally available in 25 or 30 mgampoules. It is best diluted to 10mls with water forinjections and then given in increments of 1-2ml(2.5-6mg) titrated against the blood pressure. Itseffect generally lasts about 10 minutes and it mayneed repeating. Alternatively, the ampoule may beadded to a bag of intravenous fluid and the rate ofinfusion altered to maintain the desired bloodpressure.

Update in Anaesthesia12
It can also be given intramuscularly but its onsettime is delayed although its duration is prolonged.Larger doses are necessary when it is givenintramuscularly.
Other Vasopressors
Metaraminol (Aramine). It is supplied in 10mgampoules and should be diluted and usedincrementally (1-5mg) as with ephedrine. It has aslower onset time (at least 2 minutes afterintravenous injection) but lasts longer (20-60minutes)
Methoxamine (Vasoxine). It is available in 20mgampoules and is best diluted before injection.Suitable adult doses are 2.5-5mg. It is a pureperipheral vasoconstrictor and reflex bradycardia,needing treatment with atropine can occur.
Phenylephrine. A pure peripheral vasoconstrictorwhich is available in 10mg ampoules. Dilute beforeuse. Suitable adult doses for intravenous use are100-200mcg which last about 15 minutes. A reflexbradycardia may occur.
Noradrenaline (Levophed). A powerful vasocon-strictor available in 2mg ampoules which must bediluted in 1000ml of intravenous fluid before use.It is then given at an initial rate of 2-3ml/minute andthereafter titrated against the blood pressure. Controlthe infusion with the utmost care.
Adrenaline/Epinephrine. Available as 1mg/ml(1:1,000) and 1mg/10ml (1:10,000) ampoules.Dilute 1ml of 1:1,000 adrenaline to at least 10mlwith saline and give increments of 50mcg (0.5ml of1:10,000) repeating as necessary. Monitor the effectof adrenaline closely - it is a very powerful drug butonly lasts a few minutes.
Treatment of Total Spinal
Although rare, total spinals can occur withfrightening rapidity and result in the death of thepatient if not quickly recognised and treated. Theyare more likely to occur when a planned epiduralinjection is, inadvertently, given intrathecally. Thewarning signs that a total spinal block is developingare:
Hypotension - treat as detailed above. Rememberthat nausea may be the first sign of hypotension.
Bradycardia - give atropine
Increasing anxiety - reassure.
Numbness or weakness of the arms and hands,indicating that the block has reached the cervico-thoracic junction.
Difficulty breathing - as the intercostal nerves areblocked the patient may state that they can’t take adeep breath. As the phrenic nerves (C 3,4,5) whichsupply the diaphragm become blocked, the patientwill initially be unable to talk louder than a whisperand will then stop breathing.
Loss of consciousness.
Action:
Ask for help - several pairs of hands may be useful!
Intubate and ventilate the patient with 100%oxygen.
Treat hypotension and bradycardia withintravenous fluids, atropine and vasopressors asdescribed earlier. If treatment is not started quicklythe combination of hypoxia, bradycardia andhypotension may result in a cardiac arrest.
Ventilation will need to be continued until thespinal block recedes and the patient is able tobreathe again unaided. The time this will take willdepend on which local anaesthetic has been injected.
Once the airway has been controlled and thecirculation restored, consider sedating the patientwith a benzodiazepine as consciousness may returnbefore muscle power.
General Postoperative Care
The patient should be admitted to the recoveryroom as with any other anaesthetised patient. In theevent of hypotension in the recovery room, thenurses should know to elevate the legs, increase therate at which intravenous fluids are beingadministered, give oxygen and summon theanaesthetist. Further doses of vasoconstrictors orfluids may be required, particularly if surgicalbleeding continues.
Patients should be advised as to how long theirspinal block will last and be told to remain in beduntil full sensation and muscle power has returned.

Update in Anaesthesia
As the sacral autonomic fibres are among the last torecover following a spinal anaesthetic, urinaryretention may occur. If fluid pre-loading has beenexcessive, a painful distended bladder may resultand the patient may need to be catheterised.
Permanent neurological complications areextremely rare. Many of those that have beenreported were due to the injection of inappropriatedrugs or chemicals into the CSF producingmeningitis, arachnoiditis, transverse myelitis orthe cauda equina syndrome with varying patternsof neurological impairment and sphincterdisturbances.
If inadequate sterile precautions are taken, bacterialmeningitis or an epidural abscess may resultalthough it is thought that most such abscesses arecaused by the spread of infection in the blood.
Finally, permanent paralysis can occur due to the"anterior spinal artery syndrome". This is mostlikely to affect elderly patients who are subjectedto prolonged periods of hypotension and may resultin permanent paralysis of the lower limbs.
It used to be thought that bedrest for 24 hoursfollowing a spinal anaesthetic would help reducethe incidence of headache, but this is now no longerbelieved to be the case. Patients may get up oncenormal sensation has returned, if surgicalconsiderations so allow.
Treatment of spinal headache : Pateints withspinal headaches prefer to remain lying flat in bedas this relieves the pain. They should be encouragedto drink freely or, if necessary, be given intravenousfluids to maintain adequate hydration. Simpleanalgesics such as paracetamol, aspirin or codeinemay be helpful as may measures to increase intra-abdominal and hence epidural pressure such aslying prone. Caffeine containing drinks such as tea,coffee or Coca-Cola are often helpful. Prolonged orsevere headaches may be treated with epiduralblood patch performed by aseptically injecting 15-20ml of the pateint's own blood into the epiduralspace. This then clots and seals the hole and preventsfurther leakage of CSF.
1 3
Complications of Spinal Anaesthesia
Headache: a characteristic headache may occurfollowing spinal anaesthesia. It begins within 12-24 hours and may last a week or more. It is postural,being made worse by raising the head and relievedby lying down. It is often occipital and may beassociated with a stiff neck. It is frequentlyaccompanied by nausea, vomiting, dizziness andphotophobia.
It is more common in the young, in females andespecially in obstetric patients. It is thought to becaused by the continuing loss of CSF through thehole made in the dura by the spinal needle. Thisresults in descent of the brain and traction on itssupporting structures.
The incidence of headache is related directly to thesize of the needle used. A 16 gauge needle willcause headache in about 75% of patients, a 20gauge needle in about 15% and a 25 gauge needleabout 3%. It is, therefore, sensible to use thesmallest needle available especially in high riskobstetric patients.
As the fibres of the dura run parallel to the long axisof the spine, if the bevel of the needle is parallel tothem, it will part rather than cut them and therefore,leave a smaller hole. Make a mental note of whichway the bevel lies in relation to the notch on the huband then align it appropriately. It is widelyconsidered that pencil-point needles (Whiteacre orSprotte) make a smaller hole in the dura and areassociated with a lower incidence of headache thanconventional cutting-edged needles (Quincke).
Figure 7. Patterns of spinal needle tips.
Quincke
Pencil

Update in Anaesthesia14
Other Complications In the absence of hypovolaemia due to bleeding,spinal anaesthesia is a simple and safe alternative togeneral anaesthesia for manual removal of a retainedplacenta. It does not produce uterine relaxation andif this is required, a general anaesthetic with avolatile agent may be preferred.
Technique
Spinal anaesthesia is performed and managed inpregnant patients in the same way as in non-pregnantpatients but with a number of special considerations.
It is generally recommended that obstetric patientsshould be pre-loaded with not less than 1500 mls ofa crystalloid solution before the dural puncture isperformed.
Although spinal anaesthesia is not contra-indicatedin the presence of mild pre-eclampsia, rememberthat such patients may have altered clotting functionand are relatively hypovolaemic. There is always achance that a pre-eclamptic patient may suddenlyfit and anticonvulsant drugs (diazepam orthiopentone) must be immediately available. Theadvantages and disadvantages of spinal versusgeneral anaesthesia will have to be carefullyconsidered for each patient.
Pregnant women need smaller volumes of spinalanaesthetic solution than non-pregnant women inorder to obtain a given height of block. For acaesarean section, anaesthesia should extend to T6(about the bottom of the sternum) to be completelysuccessful. This can usually be achieved with thefollowing regimes, although the hyperbaric agentsare more predictable:
2.0-2.5 ml of a hyperbaric solution of 0.5%bupivacaine or
2.0-2.5 ml of an isobaric solution of 0.5%bupivacaine or
1.4-1.6 ml of a hyperbaric solution of 5%lignocaine or
2.0-2.5 ml of an isobaric solution of 2% lignocainewith added adrenaline (0.2 ml of 1:1000)
If anaesthesia is required for a forceps delivery,1.0ml of a hyperbaric solution injected with themother in the sitting position is usually adequate.
As the sacral autonomic fibres are among the last torecover foloowing a spinal anaesthetic, urinaryretention may occur. If fluid pre-loading has beenexcessive, a painful distended bladder may resultand the patient may need to be catherised.
Permanent neurological complications areextremely rare. Many of those that have beenreported were due to the injection of inappropriatedrugs or chemicals into the CSF producingmeningitis, arachnoiditis, transverse myelitis or thecauda equina sundrome with varying patterns ofneurological impairment and sphincter disturbances.
If inadequate sterile precautions are taken bacterialmeningitis or an epidural abscess may resultalthough it is thought that most such abscesses arecaused by the spread of infection in the blood.
Finally, permanent paralysis can occur due to'anterior spinal artery syndrome'. This is most likelyto affect elderly patients who are subjected toprolonged periods of hypotension and may result inpermanent paralysis of the lower limbs.
Spinal Anaesthesia in Obstetrics
There are several reasons for preferring spinalanaesthesia to general anaesthesia for caesareansections. Babies born to mothers having spinal (orepidural) anaesthesia may be more alert and lesssedated as they have not received any generalanaesthestic agents through the placental circulation.As the mother's airway is not compromised, there isa reduced risk of aspiration of gastric contentscausing chemical pneumonitis (Mendelson'ssyndrome).
Many mothers also welcome the opportunity ofbeing awake during the delivery and being able tofeed their child as soon as the operation is complete.
There are, however, also disadvantages. It may bedifficult to perform the spinal injection as lumbarflexion may be impeded by the pregnant uterus and,if labour has started, the mother may be unable toremain still when having contractions. Unless smallgauge needles (25 gauge) are used, the incidence ofpost-spinal headache may be unacceptably high.Spinal anaesthetics for caesarean section shouldnot be performed until the anaesthetist hasaccumulated sufficient experience in theirperformance with non-pregnant patients.

Update in Anaesthesia 1 5
CONTROL OF HEART RATE
Dr I Kestin, Consultant Anaesthetist, DerrifordHospital, Plymouth.
The heart will beat independently of any nervous orhormonal influences. This spontaneous rhythm ofthe heart (called intrinsic automaticity) can bealtered by nervous impulses or by circulatorysubstances, like adrenaline. The muscle fibres ofthe heart are excitable cells like other muscle ornerve cells, but have a unique property. Each cell inthe heart will spontaneously contract at a regularrate because the electrical properties of the cellmembrane spontaneously alter with time andregularly "depolarise". This means the reversal ofthe electrical gradient across the cell membranethat causes muscle contraction or passage of anervous impulse. Muscle fibres from different partsof the heart have different rates of spontaneousdepolarisation; the cells from the ventricle are theslowest, and those from the atria are faster.
The coordinated contraction of the heart is producedbecause the cells with the fastest rate ofdepolarisation "capture" the rest of the heart musclecells. These cells with the fastest rate ofdepolarisation are in the sinoatrial node (SA node),the "pacemaker" of the heart, found in the rightatrium. As the SA node depolarises, a wave ofelectrical activity spreads out across the atria toproduce atrial contraction. Electrical activity thenpasses through the atrioventricular node (AV node)and through into the ventricles via the Purkinjefibres in the Bundle of His to produce a ventricular
contraction. If there is any disease of the conductingsystem of the heart, then this process may beinterfered with and the heart rate altered. If, forexample, there is disease of the AV node, then thereis an electrical block between the atria and theventricles. The ventricles will beat with their owninherent rhythm, which is much slower, usually 30-50 beats per minute.
Aorta
Left bundle branch
Leftposteriorfascicle
Left anteriorfascicle
Purkinje system
Bundle of His
Internodalpathways
Anaesthesia to T10 is needed for removal of aretained placenta. This can be obtained by injecting1.5mls of a hyperbaric solution with the patientsitting and then lying her down.
Positioning of the Pregnant Patient
Pregnant patients should never lie supine as thegravid uterus will compress the vena cava and, to alesser extent the aorta (aorto-caval compression)resulting in hypotension. They should, instead,always lie with a lateral tilt. This can be achievedeither by tilting the whole table or by inserting awedge under the patients right hip. The uterus isdisplaced slightly to the left and the vena cava is notcompressed (see Update No. 2).
As with all patients undergoing surgery under spinalanaesthesia, oxygen should be given during theoperation. As hypotension commonly occurs despitefluid preloading, many anaesthetists routinely givea dose of vasoconstrictor intravenously. Ephedrineis the favoured vasoconstrictor as it does not causeconstriction of the uterine blood vessels. If it is notavailable, one of the other vasoconstrictors discussedpreviously should be used as untreated hypotensioncan seriously damage the unborn infant.
After delivery of the baby, syntocinon is the oxytocicof choice as it is less likely to produce maternalnausea and vomiting than ergometrine.
Superior vena cava
Sinoatrialnode
Atrio-ventricularnode
Right bundle branch
Figure 1. Conducting system of the heart.

Update in Anaesthesia16
are found in the atria. When the atria distend, as inheart failure or overtransfusion, there is a reflexincrease in the heart rate to pump the extra bloodreturning to the heart. When there is a suddenreduction in the pressure in the atria the heart slows.This is called the Bainbridge Reflex and is the causefor the marked bradycardia sometimes seen duringspinal anaesthesia. It is best treated by raising thelegs to increase the venous return.
Circulatory substances can also affect the heartrate. Catecholamines, like adrenaline, are releasedduring stress, and will cause an increase in heartrate. Drugs are another common cause of change inthe heart rate and most anaesthetic drugs can dothis. Halothane affects the SA node and will alsodepress the force of contraction of the heart.Isoflurane, by contrast has little direct affect on theheart, but causes peripheral vasodilation of theblood vessels. This will then decrease the bloodpressure, and hence produce a reflex tachycardia asexplained above. Ketamine causes stimulation ofthe sympathetic nervous system, and thereforeproduces a tachycardia. Other circulating substancesmay also affect the heart rate, acting indirectlythrough the autonomic nervous system. For exampleincreased blood concentrations of carbon dioxidewill cause stimulation of the sympathetic nervoussystem and tachycardia, and is an important sign ofrespiratory failure.
Anaesthetic drugs, like halothane, may depress therate of depolarisation of the SA node, and the AVnode may become the pacemaker of the heart.When this occurs it is frequently termed nodal orjunctional rhythm.
This automatic rhythm of the heart can be altered bythe autonomic nervous system. The sympatheticnervous system supply to the heart leaves the spinalcord at the first four thoracic vertebra, and suppliesmost of the muscle of the heart. Stimulation via thecardiac beta-1 receptors causes the heart rate toincrease and beat more forcefully. The vagus nervealso supplies the atria, and stimulation causes theheart rate to decrease (bradycardia). Surgicalprocedures can cause vagal stimulation and producesevere bradycardia. Examples include pulling onthe mesentery of the bowel, anal dilatation orpulling on the external muscles of the eye. Undernormal conditions the vagus nerve is the moreimportant influence on the heart. This is especiallynoticeable in athletes who have slow heart rates.
There are nervous reflexes that effect heart rate.The afferents are nerves in the wall of the atria oraorta that respond to stretch. The aorta containshigh pressure receptors. When the blood pressure ishigh these cause reflex slowing of the heart toreduce the cardiac output and the blood pressure.Similarly, when the blood pressure is low, the heartrate increases, as in shock. Similar pressure receptors

Update in Anaesthesia 1 7
DRAW-OVER ANAESTHESIA Part 2 -Practical Application
Dr M B Dobson, Consultant Anaesthetist,John Radcliffe Hospital, Oxford OX3 9DU
In the first article on draw-over, Georg Kammdescribed the apparatus used in draw-overanaesthesia. In this issue, I want to describe theways in which draw-over apparatus can be used toprovide safe, high quality anaesthesia. We mustfirst recognise that safe anaesthesia is not producedby apparatus alone!
The essentials for safe anaesthesia in any situationinclude adequate pre-operative assessment,preparation and resuscitation of patients, reliableintravenous access, a pleasant and safe induction, asecure airway, adequate tissue oxygenation,appropriate monitoring, and rapid recovery. Noneof these depends on high cost or high technologyequipment, but all require properly trained andreliable people, on whom primary safety depends.If you are responsible for anaesthesia in a districthospital, and do not have extensive specialisttraining, you are well advised to use a small numberof safe, widely applicable clinical techniques. Thiswill allow you to become thoroughly familiar andconfident with them through regular practice. No-one can be safe or confident when they use anunfamiliar technique. Restricting yourself to a smallnumber of techniques also means that you use alimited number of drugs, and it is easier to makesure that adequate stocks are held in the hospitalwhich do not run out.
A draw-over system is most suitable for the needsof district hospitals. It is simple to understand,robust, independent of compressed gases, and canbe repaired on site if necessary. In a draw-oversystem the carrier gas (air, with or without oxygenenrichment) passes through a low resistancevaporiser, through a self-inflating bag or bellowsand reaches the patient via a universal breathingvalve which ensures that expired gases are directedinto the atmosphere and do not re-enter theanaesthetic system.
Ether as an Anaesthetic Agent
Ether has largely disappeared from anaestheticpractice in Western countries, because of a numberof apparent disadvantages: it has a pungent smell,and this combined with its high blood solubility
prolongs the induction of anaesthesia with etheralone. It has also been associated with post-operativevomiting, and people are concerned about possibledangers of fires and explosions. Nevertheless, etherhas many important advantages - it increases cardiacoutput and is a respiratory stimulant - and is thereforethe only volatile agent which can safely be used forspontaneously breathing patients if oxygen is notavailable. It is certainly the safest volatile anaestheticin the hands of the inexperienced or occasionalanaesthetist, and the experienced anaesthetist caneasily use ether as part of a more sophisticatedtechnique which avoids the problems of slowinduction, vomiting, and delayed recovery.
Most of the disadvantages of ether are seen when itis used alone for induction of anaesthesia. Theyinclude a slow onset, an unpleasant smell for thepatient, with coughing, breath-holding and laryngealirritability, salivation, swallowing and sometimesvomiting. In the vast majority of patients, theseproblems can be easily and safely avoided byintravenous induction of anaesthesia with drugssuch as thiopentone or ketamine. Insertion of anendotracheal tube secures the airway, and allowsthe concentration of ether to be increased rapidly tomaintenance levels with no risk of laryngospasm. Ifa muscle relaxant is used, inhaled etherconcentrations of 3-4% are enough to ensureunconsciousness, and wake up reasonably rapidlyat the end of surgery. Ether also provides aconsiderably longer period of post-operativeanalgesia than other volatile anaesthetics. Thus, theclinical disadvantages of ether can be overcome,allowing us to make use of its advantages in safety,availability and economy. (A summary of a suitabletechnique for ether anaesthesia is shown in Table 1,Page 20 ). The only problem remaining is thequestion of its flammability.
Ether is flammable (will burn, but not explode)when mixed with air. In this respect you can compareit with alcohol, but not with petrol, which willexplode when ignited in air. The addition of oxygen(or nitrous oxide) to ether does produce an explosivemixture, in which ignition could be caused by asource such as surgical diathermy, a sparking electricsocket, or (especially in a dry climate) staticelectricity. Flammable or explosive mixtures musttherefore be separated from possible ignition sources- there are two ways of doing this:-

Update in Anaesthesia18
should be assisted or controlled to prevent hypoxia.Halothane sensitises the heart to adrenaline, andyou should warn the surgeon not to infiltrate thewound with adrenaline-containing solutions whenhalothane is in use. (Some anaesthetists allowinfiltration of up to 20 ml of 1:200,000 adrenalineprovided the pulse is closely monitored).
Halothane may be very useful in combination withother volatile anaesthetics. If you plan aninhalational induction, begin with halothane, thenchange to ether once the patient becomesunconscious - this is much quicker and more pleasantfor the patient - and you will see the contrastbetween the respiratory depression of halothaneand the stimulation of ether!
Halothane has also been used successfully formilitary anaesthesia in combination with trich-loroethylene, using two Oxford MiniatureVaporisers in the "Tri-service" apparatus. The agentscomplement each other, since halothane is a goodhypnotic but a poor analgesic, while the reverse istrue of trichloroethylene. Use 0.5% trichloro-ethylene as a "baseline" and vary the concentrationof halothane to obtain the required depth ofanaesthesia. Turn the trichloroethylene off a fewminutes before the end of the operation as it takesa while to wear off. Once again, added oxygen isnecessary.
Separation in time. Healthy patients are mostlikely to need added oxygen at the beginning ofanaesthesia (before and just after intubation) and atits end (before extubation). At these times surgicaldiathermy is not in use. During the operation useether/air without added oxygen unless the patient isvery sick, old, very young or anaemic, or there areother indications such as pregnancy, cardio-respiratory disease or high altitude.
Separation in space. During the use of flammable/explosive mixtures no source of ignition is permittedin a "zone of risk" which extends 30 cm from allpoints of the breathing system where gas mightescape - thus no diathermy in the thoracic cavity,head and neck, or mouth is permitted, but diathermyin the bladder or abdominal cavity is consideredsafe. A simple scavenging system - a length oftubing to direct the expired gases away from the siteof surgery, is helpful. In dry climates (including airconditioning) anti-static precautions should also beused.
It is worth remembering that Western operatingtheatres are still mostly built with antistaticprecautions, since even without ether there is a riskof fires and explosions with other substances mixedwith oxygen (enflurane, trichloroethylene, alcoholetc.).
Using Other Volatile Anaesthetic Agents
Halothane is widely available, and has a number ofadvantages. It is non-flammable, has a pleasant,non-irritant smell, and induces unconsciousnessmore quickly than ether. Its disadvantages are thatit depresses the cardiovascular and respiratorysystems, resulting in hypotension and hypoxia. It ismore potent than ether, and must never be given by"open drop" techniques. Halothane should never beput in an EMO vaporiser, as it attacks the metalfrom which these vaporisers are made, and thevaporiser will be wrecked! The most suitable draw-over vaporiser for halothane is the Oxford MiniatureVaporiser, which can also be used for other volatileanaesthetics if these are available (e.g.trichloroethylene, enflurane etc.).
Halothane can be used alone for anaesthesia; itsmain disadvantages in this situation is the respiratorydepression which it causes, and supplementaryoxygen should always be used throughout theprocedure. If oxygen is not available, ventilation
Draw-over Without Volatile Anaesthetics
Whichever kind of general anaesthetic you use, thepatient must have a secure airway and adequatebreathing. There is no reason why you should notuse the draw over system to provide these inconjunction with a total intravenous anaesthetic.The invention of electronically controlled infusionpumps leads some to suggest that these may oneday replace vaporisers for most anaesthetics - but inmany situations a carefully regulated and monitoredintravenous infusion of a drug such as ketamine canbe given using an ordinary intravenous drip and awatch with a second hand.
Prepare a solution of intravenous anaesthetic to astandard concentration (e.g. ketamine 1000mg in a500 ml bottle or bag of normal saline, equal toketamine 2mg/ml). You will need to know thenumber of drops/ml of your giving set. Prepareyour apparatus, give oxygen by facemask, andinduce anaesthesia with a fast running infusion

Update in Anaesthesia
etc, use a nasopharyngeal catheter (eg a 8-10FGrubber or plastic catheter) inserted into thenasopharynx with a flow of 1 litre/min for a child or2 litres/min for an adult, giving an inspiredconcentration of about 40% oxygen. It is desirableto humidify the flow of oxygen and vital to checkthat the catheter is not inserted too far (e.g. into theoesophagus) or gastric dilatation could result. Aswell as its economy, this method is preferred bymany patients as it allows them to talk, cough,expectorate and eat - all difficult to do with aconventional facemask!
Other sources of oxygen are worth considering.Industrial (welding) oxygen is normally made bythe same process as "Medical oxygen" - and indeedindustrial oxygen is often made to a higher degreeof purity! You must check your own localspecification!
Oxygen concentrators (see Update No.1) can alsoprovide a supply for draw-over or ward use.Concentrators compress room air to a pressure of 4bar, then pass it though a zeolite column whichabsorbs the nitrogen, leaving up to 96% oxygen(the rest is argon). If excessive flows are demandedthe concentration delivered falls off. Smallconcentrators, which meet the World HealthOrganisation’s (WHO) standards can deliver 4litres/min of oxygen (>90%) with a powerconsumption of around 350 watts (mains electricityor AC generator required). Concentrators are usuallythe cheapest way of getting oxygen - often 30-50%of the cost of cylinders. They require simpleservicing every 5000 hours and an overhaul every20,000 (equivalent in running time to about half amillion miles for a car!). For details of WHOapproved concentrators write to the author.
1 9
(you will need about 120mg of ketamine - 60ml ofthe above dilution). When the patient has lostconsciousness give a muscle relaxant and intubatethe trachea. Reduce the infusion of ketamine toabout 2mg/min of the above dilution according toclinical signs for maintenance, and give furtherdoses of relaxant as necessary. You must monitoryour infusion continuously - if it stops or becomes"tissued" the patient may become aware. At theend of anaesthesia reverse the relaxant, stop theketamine, make sure the patient is breathing welland put them in the recovery position.Benzodiazepine premedication or postmedicationwill prevent dreaming and emergence reactions.The addition of atropine will reduce excessivesecretions.
You can use a similar technique with otherintravenous agents, but be warned that recoveryafter the use of barbiturate infusions may be veryprolonged.
Oxygen Supplies
We have already noted some of the problems ofoxygen supplies: in developing countries hospitalsmay have to purchase their own cylinders, andmany of these go missing when sent for re-filling.With the draw-over system, missing cylinders donot cause the anaesthetic service to collapse, butoxygen is still very desirable, especially if yourpatient is very young, old, anaemic or ill.
The use of a T-piece (see Fig 1) to enrich a draw-over system is very economical and allows you tomake the most of your supplies. A flow of 1 litre/min provides an inspired concentration of 30-40%oxygen; 4 litres/min provides 60-80%. To make thebest use of oxygen post-operatively, or in cases ofbreathing difficulty due to respiratory infections
0
5
Low flow oxygen enrichment
Room air
Open endedoxygen reservoirtube
to Patient
Figure 1. Adding oxygen to a drawover circuit
Vaporiser

Update in Anaesthesia20
Is General anaesthesia required for this case? NO Use regional technique
YES
Is the anaesthetist trained in endotracheal NO Use ketamine or spinalintubation?
YES
Has the patient a difficult airway? YES Use regional or seekexpert help
NO
Table 1. Suggested plan for General Anaesthesia
Proceed as follows:-
¨ Check your apparatus and drugs
¨ Obtain intravenous access and preoxygenate the patient
¨ Give a sleep dose of thiopentone or ketamine
¨ Give 1mg/kg suxamethonium i.v.
¨ Intubate the trachea
¨ Ventilate the lungs manually with 3% ether in air. Increase this during the first 5 minutes to 6-10% to settle the patient. (Halothane 1-1.5% can be used instead of ether).
¨ When breathing returns (usually after 3-5 minutes) allow the patient to breathe 6-8% ether in airor 1-1.5% halothane in oxygen-enriched air or if available give a long term relaxant (egalcuronium or gallamine) and continue to ventilate the lungs manually, at an appropriateconcentration of volatile agent (This technique allows rapid recovery).
¨ At the end of surgery reverse long acting muscle relaxants (if given) with neostigmine andatropine, continuing to ventilate the lungs until breathing resumes; turn the patient on hisside, and remove the tube when the patient is awake.
This "universal" technique can be used for almost all types of surgery, and for both elective andemergency cases.
⇓
⇓
⇓
⇓
⇓
⇓
⇒ ⇒
⇒ ⇒
⇒ ⇒

Update in Anaesthesia 2 1
pulling. Wash the inside and outside of the valvewith warm soapy water, and allow the parts to drythoroughly before carefully re-assembling the valve.Most Ambu valves can be sterilised, either withantiseptics or by autoclaving, but sterilisation isonly necessary if the valve has been contaminatedby use on an infected patient - for example one withtuberculosis.
When using the Oxford inflating bellows with anAMBU (or other universal breathing valve) ensurethat you disable the flap valve nearest the patientusing the magnet provided. This will prevent thevalves from jamming during intermittent positivepressure ventilation.
If your anaesthetic facemasks have an inflatablemargin check the state of the rubber, as it is likelyto perish in time. If the small bung used to retain theair is missing it should be replaced with a suitablesubstitute - do not inflate the mask and tie a knot inthe inflating tube!
Check your stock of endotracheal tubes regularly.Red rubber tubes are liable to deteriorate in hot andhumid conditions. The inflatable cuff is especiallyvulnerable and should be tested before use.
Special Attention for Vaporisers
Drain and discard the contents of your vaporisersonce a week, to avoid the build-up of depositsinside.
Vaporisers are precision instruments and must betreated with care. When complicated repairs areneeded, the machine must be sent to a competentmedical engineer or service centre, but there are anumber of simple problems which you can dealwith yourself. First of all, write to the manufacturersto obtain a service manual and any replacementparts you will need. When these have arrived, setaside a time when the vaporiser will not be neededfor clinical use, and you have time to work on it.Below are brief descriptions of some of theoperations you should be able to manage on Penlonvaporisers (EMO & OMV - the address is PenlonLtd, Radley Road, Abingdon OX14 3PH. Telephone44 235 554222 Fax 44 235 555252). Other brandsof draw-over vaporisers generally need the attentionof a service engineer.
The EMO Vaporiser - Common Faults
Dr M B Dobson, Consultant Anaesthetist,Oxford, UK
If you work in a district hospital it is unlikely thatyou will have the help of a skilled technician to lookafter your apparatus, and the responsibility istherefore yours. No apparatus will work reliablyunless it is properly and regularly inspected andcared for. Draw-over apparatus is not difficult tounderstand, and many simple procedures willprevent or correct breakdown. The first rule is notto interfere with apparatus which is working well!If you do have to make a repair, obtain a copy of theservice manual, and make sure you have all thenecessary spare parts and any special tools beforeyou start.
Routine Care
Like all machines, your draw-over system requiresregular attention to keep it in good, reliable workingorder. One of the main advantages of draw-overapparatus is that it is relatively simple to carry outthese regular checks and simple repairs yourself -but remember that vaporisers and valves areprecision instruments, and need to be handledcarefully. Never use excessive force.
Make sure your apparatus is stored in a clean, dryplace, away from dusty environments. Wipe it overregularly with a soft, moist cloth and a littledetergent. Close off open ends with corks or plasticcaps to prevent dust and insects getting inside.
Black (anti-static) anaesthetic breathing hoses areliable to perish in humid atmospheres; after usethey will be wet inside from the water vapour in thepatient’s breath. After use hang them vertically ina cupboard to allow them to dry. Inspect themregularly looking especially for cracks in betweenthe corrugations - this is where they most oftendevelop leaks. If you do not use ether, you do notneed anti-static hoses, and white polythenecorrugated hoses are both cheaper and more resistantto humidity. Check your inflating bellows or Ambubag for cracks or perishing in the rubber. Theseitems are almost impossible to repair, so it is wiseto have a spare in the supply cupboard.
Regularly inspect your Ambu (or other universalbreathing) valves, and clean them when necessary.The inlet and exhaust ports can be unscrewed byhand, and the valve rubbers removed by gentle

Update in Anaesthesia22
many different models - be sure to specify whichyou want. The air inlet can be on the right (usuallyfor draw-over) or left (for a compressed gasmachine) and the tapers can be either 22mm ISO(draw-over) or 23mm cagemount (compressed gasmachine). Make sure you know what you wantbefore you order!
A video tape of the servicing of EMO and OMVvaporisers can be obtained from Dr RogerEltringham, Department of Anaesthetics,Gloucestershire Royal Hospital, Gloucester, UK.
Technical Queries
Dr Ray Towey from Tanzania writes to ask:-
Q: "Is it possible to connect the outlet of thePuritan Bennett oxygen concentrator to an OxfordMiniature Vaporiser (OMV) to provide a continuousgas flow for an Ayres T-piece paediatric breathingsystem? My concern is that the outlet pressure ofgas from the concentrator is too low to permit IPPVfrom an Ayre’s T-piece".
Short answer: No problem, but the flow from theconcentrator of 4 litres/minute means that with afresh gas requirement of 150ml/kg/min you will belimited to using this system on patients under about20kg - if you exceed this, rebreathing will be aproblem.
Long answer: There are actually 2 questions toanswer:
Q1: Does the OMV work efficiently with acontinuous gas flow of 4 litres/min or less?
Answer: The OMV works best in the intermittentflow of a draw-over system, but with continuousflows its performance at 4 litres/min is satisfactory.If the flow is reduced to 2 litres/min it will givesignificantly less than indicated. I thereforerecommend that you keep the flow at 4 l/min for allsizes of patients up to 20kg.
Q2: Does the back pressure generated by IPPVwith a T-piece reduce the flow from the concentratorsignificantly?
Answer: No. Small concentrators like the PuritanBennett and other WHO-approved models(Healthdyne & DeVilbiss) produce oxygen at apressure of up to 5 p.s.i. (=0.35 bar, 260 mmHg,340cm. water). The back pressure generated byIPPV is unlikely to exceed 30 cm. water, which is
1. The pointer sticks and is difficult or impossibleto move
Cause: build up of sticky deposits around theinternal rotor drum.
Remedy: remove the drum and clean it; re-assemblethe vaporiser.
You will need: Maintenance manual, screwdrivers,artery forceps, penetrating oil, ether, brass polish,vaseline and possibly a new main gasket.
2. The thermocompensator breaks - only themetal disc is visible in the window on top of thevaporiser.
Cause: metal fatigue after 5-10 years use.
Remedy order a replacement unit from themanufacturer. This is very simple to exchange forthe broken unit - only a screwdriver needed toloosen 3 screws.
You will need: Screwdriver, replacement part.
3. Broken window of the filler gauge. Warning:you must not use an EMO with a broken filler gauge- it will give a dangerously high concentration ofether
Cause: accidental breakage.
Remedy: order and fit a replacement from themanufacturer. Fitting is simple - loosen 3 screws,remove the old unit and slot in the replacement.
You will need: screwdriver, replacement part.
Problems with the Oxford Miniature Vaporiser
OMV’s used with halothane gradually become stiffto operate, due to the build-up of thymol (used as apreservative in halothane) in the mechanism. Toclean this off properly you will have to take the topoff the vaporiser. First obtain the service manual;you will almost certainly need to fit new rubberseals, so order these at the same time. A temporary"repair" can be achieved by pouring ether into theinlet and outlet ports, and gently working theconcentration control from side to side. Do not useexcessive force or you will bend it. The thymol willbe dissolved by the ether. Afterwards, tip all theether out, and ventilate with the bellows to dry outthe vaporiser before re-filling it with the correctagent.
If you order a new OMV, remember that there are

Update in Anaesthesia 2 3
only a tenth of that available. I have checked this inthe laboratory using a P-B concentrator, andmeasuring the flow delivered through a highprecision flowmeter while producing back pressureby applying a gate clamp to the oxygen tubing (seefigure 1) with the concentrator flow control set todeliver 4 l/min.
Conclusions:
1. Flow from the concentrator is well maintained
2. Even with significant back pressure, the flowindicated on the concentrator’s flowmeter is areliable guide to the flow actually being delivered.
until back pressure reaches 60-100 mmHg (75-130cm. Water). Results are shown in Table 1 below.
Figure 1.
The results obtained were as follows
Table 1.
Flow from Back pressure Actual flowConcentrator applied delivered
4 0 4.254 15 mmHg 4.254 30 mmHg 4.14 45 mmHg 3.84 60 mmHg 3.83.5 100 mmHg 3.42 200 mmHg 1.751 300 mmHg 1.250 500 mmHg 0
Concentrator ManometerClamp
Flowmeter

Update in Anaesthesia24
emptying of the stomach, constipation, and mayalso lead to urinary retention.
Morphine can also cause histamine release, whichcauses itching of the skin and nose and a mildflushing of the skin. Morphine has little directeffect on the heart or blood pressure. However theblood pressure may fall slightly following the painrelief produced by morphine and also with thesedation which may be produced. Significanthypotension following morphine is usually due toother causes such as hypovolaemia. Occasionallypatients with severe asthma may become wheezy.An unimportant, but early noticeable effect is thatthe pupils become small. This helps to differentiaterespiratory depression caused by morphine fromother causes.
Precautions.
All patients who have been given morphine must becarefully observed for evidence of respiratorydepression. This can be detected as a slow respiratoryrate and a very sleepy patient with pin point pupils.Oxygen should be given by face mask, and positivepressure ventilation of the lungs started if necessary.Naloxone, 100-400 micrograms may be givenintravenously if available.
Dose and Uses
Morphine can be given orally, rectally, byintramuscular or intravenous injection, sub-cutaneously, sublingually, or injection into theepidural or subarachnoid space. The dose foranalgesia by IM injection is 100-150mcg/kg,repeated 2 hourly as required. The dose usedintravenously during anaesthesia depends on thenature and duration of the surgery. The usual dosegiven at the start of surgery when intermittentpositive pressure ventilation is used is 100-200mcg/kg, followed by required additional doses of 1-2mgintravenously when required. After the patient haswoken up further doses of 1-2mg may be givenuntil the patient is free of pain. Much higher dosesare sometimes used during specialist surgery suchas cardiac or neurosurgery.
Morphine can be given to relieve chronic painespecially from cancer. Much higher doses areneeded orally than by injection. The oral dose isvery variable for individual patients; sufficientshould be given to relieve the pain.
MORPHINE
Dr I Kestin, Consultant Anaesthetist, DerrifordHospital, Plymouth.
Structure.
Morphine is obtained from opium, the juice secretedby the seeds of the poppy. It works on several typesof receptors, widely found in nervous tissue."Opioids" is a term used for all drugs that act onthese receptors. These other opioids may be naturaloccurring substances, such as morphine, or madein the laboratory such as pethidine.
Morphine works on receptors in the cell membranes.These are protein-lipid molecules that alter theirshape when stimulated to effect molecular changeswithin cells. There are thought to be three types ofreceptors that respond to opioids, mu, kappa andlambda. Morphine acts mainly on mu receptors tocause a wide variety of effects. The most importantof these are relief of pain and respiratory depression.In anaesthesia morphine is used to relieve pain.This is an effect of its action on the spinal cord todecrease the transmission of painful stimuli frombody to brain, and its action within the brain itself.
Side Effects.
Morphine has many side effects. The mostdangerous is respiratory depression. Minor degreesof respiratory depression may be detected followingstandard doses of morphine, but this is not clinicallyimportant. With higher doses or in frail patients,the respiratory rate decreases, the patient becomesincreasingly sedated, and the pupils very small.Common side effects are nausea and vomiting dueto a central action of morphine stimulating one ofthe centres in the brain concerned with vomitingcalled the chemotactic trigger zone. Other centralnervous system side effects of morphine are coughsuppression, sedation, and dependence leading toaddiction. Addiction is not a problem whenmorphine is used to treat acute pain after surgery;sufficient morphine should always be given torelieve the pain.
Morphine also has an effect on the muscle of thebowel and urinary tract, causing the sphincter tocontract and reduce the peristalsis (the wavelikemovements of the bowel muscle that propel itscontents forwards). This results in a delayed

Update in Anaesthesia 2 5
Morphine can be given into the epidural orsubarachnoid space. This is to deliver the morphineclose to one of its sites of action, the spinal cord. Itis thought that pain relief of long duration can beobtained with very low doses of morphine. A singledose of epidural morphine may relieve pain for 12-24 hours. The usual adult dose for epidural morphineis 3-7 milligrams, and of subarachnoid morphinebetween 250mcg and 1mg. The main risk of thistechnique is that severe respiratory depression mayoccur up to 18 hours after the initial injection
because of the slow circulation of cerebral spinalfluid which carries the morphine up to the brain toact on the respiratory centre. It is vital that all thosecaring for a patient who has had this technique areaware of the potential side effects and watch out forthem. This technique can only be used in specialisthospitals with intensive care facilities. In all otheraspects the side effects of epidural and subarachnoidmorphine are similar to morphine given by anyother route.
Answers
1. The X ray shows a traumatic rupture of the leftdiaphragm with bowel in the chest.
2. The bowel may herniate through the tear as isseen in the X ray. If gastric dilation develops severerespiratory distress may result. If treatment of theherniation is delayed ischaemia may develop in theaffected bowel leading to gangrene.
3. Many cases of ruptured diaphragm are associatedwith other intra-abdominal injuries and it is usuallyrepaired at the same laparotomy.
Treatment should include oxygenation, resuscitationand in the presence of a lot of gastric air the passageof a nasogastric tube. During anaesthesia ventilationshould be controlled due to the inefficient ventilationresulting from this injury.
Comment.
Traumatic diaphragmatic hernias are more oftendescribed on the left than the right. They are usuallythe result of severe blunt trauma which causes a tearin the dome of the diaphragm resulting in herniation.Since the intra-abdominal pressure is higher then,the pleural pressure bowel will tend to move intothe thoracic cavity.
There is often a delay in diagnosis untilbreathlessness results from gastric dilation.Clinically the patient may have reduced air entry onthe effected side, and bowel sounds may be audiblein the left chest. A chest X ray may reveal thecharacteristic changes seen in the example, or maybe misdiagnosed as Penetrating trauma may alsocause lacerations of the diaphragm which are usuallysmall. Herniation is less common at the time ofinjury, but the patient may present years later whena hernia develops.
CLINICAL DILEMMA
A 26 year old man was admitted to your hospitalafter a road traffic accident. He had abdominal painand was found to be breathless and cyanosed onexamination. His chest X ray is seen in figure 1.
1. What is the abnormality seen?
2. What complications may occur with it?
3. What is the treatment?
Figure 1.

Update in Anaesthesia26
showing other changes at the left base such aspleural fluid or basal consolidation. If the stomachis dilated the X ray may suggest a pneumothorax,which if drained would reveal gastric contents. Ifa nasogastric tube has been passed it may be seenin the chest on X ray. The condition is alsosometimes diagnosed at laparotomy performed forother abdominal injuries. In cases of doubt a chest
X ray taken after ingestion of contrast material willconfirm the diagnosis. After diagnosis, treatmentshould not be delayed due to the potentialcomplications discussed earlier. The left diaphragmis usually repaired at laparotomy, right sided injuries(which are uncommon and may be difficult todiagnose) via a thoracotomy.
THE MAINTENANCE OF AN ANEROIDSPHYGMOMANOMETER
Mr Mike Yeats, Derriford Hospital, Plymouth
The first article in this series described themaintenance of a mercury sphygmomanometer,this article describes the maintenance of an aneroidblood pressure apparatus. Aneroid means, in Greek,operating without liquid or containing no fluid.Aneroid blood pressure gauges are generally smallerthan mercury ones but they are easily damaged andcan go out of calibration without detection.
A common type of aneroid apparatus is shown infigure 1. It consists of a dial which normally rises to300mmHg and a thin brass corrugated bellowsinside. There is a shaft which connects two pins atright angles to each other; one of these rests on thebellows, the other is inside a concave sided trianglewhich meshes with a pinion connected to the dialpointer. A thin coiled spring (known as a hairspring) is also connected to the pinion and returnsthe pointer to zero when the pressure is released.
Figure 1. An Aneroid Sphygmomanometer

Update in Anaesthesia
Figure 3. Method of comparing aneroid and mercurysphygmomanometers
2 7
transmitted by the other pin which moves the triangleand therefore the pinion and pointer. This can beseen in figure 2.
Figure 2.
When in use the gauge is connected to a bloodpressure cuff around the patient's arm. As thepressure in the cuff rises, the pin resting on theexpanding bellows is lifted. This movement is
The following errors may occur:
Leaks in the system. If a leak develops in thesystem wrap the cuff around itself and secure theend. Inflate the system to 250mmHg, watch thepointer. If it slowly drops there is a leak - it is mostlikely to be in the cuff or inflation bulb. It is fairlyrare for a leak to occur in the gauge itself. A smallpointed brush with soapy water on it will help findthe smallest leak.
Incorrect zero - the gauge does not return to zeroafter the cuff has been deflated. On some models,such as the example photographed, there is anadjustment screw to set the zero point. Howeverusing this screw requires the instrument to be takenout of the case and the screw may be very stiff. Theeasiest method of adjusting the zero is by removingthe glass from the front of the gauge and carefullytaking off the pointer and replacing it in the correctposition The pointer can usually be taken off usingyour finger and thumb nails. If this is not successfulfind two very small screwdrivers or thin flat piecesof metal and lever the pointer upwards using one oneach side.
Calibration check. Every aneroid blood pressuregauge should be compared with a well maintainedmercury sphygmomanometer on a regular basis.Connect the gauges together with a plastic T-pieceand connect the third arm to an inflation bulb(figure 3).

Update in Anaesthesia28
Inflate the bulb slowly and note the readings showingon each instrument on a piece of paper at intervalsof say, 20mmHg, starting at 40mmHg and going upto 200mmHg. After you have finished the testinspect the figures (example shown below) andnote the difference between them. If the readingsare within a few millimeters of mercury throughoutthe scale this is acceptable for clinical use.
In Table 1 the aneroid is reading 10mmHg higheracross the scale - this is an example of a linear error.
Table 1. Example of a linear errorMercury AneroidSphygmomanometer Sphygmomanometer Difference (mmHg) (mmHg) (mmHg)
40 50 +10 60 70 +10 80 90 +10100 110 +10120 130 +10
Table 2. - Example of a non-linear errorMercury AneroidSphygmomanometer Sphygmomanometer Difference (mmHg) (mmHg) (mmHg)
40 20 -20 60 50 -10 80 80 0100 110 +10120 140 +20
In the example shown in Table 2, at low pressuresthe aneroid sphygmomanometer reads less than themercury sphygmomanometer, becomes the sameat 80mmHg, and then reads higher above 80mmHg.This is an example of a non-linear error.
Correction of calibration. This is requiredoccasionally, usually as result of the gauge beingdropped. It is best done by someone who hasexperience of aneroid blood pressure machines.However, it may be undertaken by carefullyfollowing the instructions below. Each adjustmentshould be made in very small amounts followed bya check to assess the effect.
1. Start by making sure the pointer is on the zeromark.
2. Remove the glass, then carefully remove thepointer and lift off the dial. You should now see thetriangle with concave sides, on one side of which isa pin. In order to correct a non-linear error bendthis pin very slightly away or towards the side of thetriangle, replace the dial and pointer and run thecalibration check again. Repeat this operation untilthe error has gone.
3. When correcting a linear error bend this pinvery slightly along the line of the triangle side. Runthe calibration check again and keep adjusting untilthe error is gone.
4. Broken cover glass. Visit the local watchrepairer or make a glass from a thin plastic sheet.
After making the adjustments apply a little watchoil to the bearing points.
Sponsored by: Overseas Development AdministrationTypset by: Graphic Services, Exeter Postgraduate Medical Centre UK.
Printed in Great Britian by: BPCC Wheatons Ltd, Exeter UK.Correspondence to: Dr I H Wilson, Anaesthetics Dept., Royal Devon & Exeter Hospital, Exeter, EX2 5DW, UK