Embed Size (px)
Citation preview

Journal of Clinical Neuroscience 18 (2011) 916–921
Contents lists available at ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Clinical Study
Voxel-based morphometric study of brain volume changes in patients withAlzheimer’s disease assessed according to the Clinical Dementia Rating score
SangYun Kim a, Young Chul Youn b,⇑, Ging-Yuek Robin Hsiung c, Sam-Yeol Ha b, Kwang-Yeol Park b,Hae-Won Shin b, Don-Kyu Kim d, Sung-Su Kim e, Baik Seok Kee f
a Department of Neurology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam-si, South Koreab Department of Neurology, Chung-Ang University College of Medicine, Heukseok-dong, Dongjak-gu, Seoul 156-755, South Koreac Division of Neurology, Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canadad Department of Physical Medicine and Rehabilitation, Chung-Ang University College of Medicine, Seoul 156-755, South Koreae Department of Anatomy and Cell Biology, Chung-Ang University College of Medicine, Seoul 156-755, South Koreaf Department of Psychiatry, Chung-Ang University College of Medicine, Seoul 156-755, South Korea
a r t i c l e i n f o a b s t r a c t
Article history:Received 17 May 2010Accepted 9 December 2010
Keywords:Alzheimer’s diseaseClinical Dementia RatingGray matter volume reductionVoxel-based morphometryWhite matter volume reduction
0967-5868/$ - see front matter � 2011 Elsevier Ltd. Adoi:10.1016/j.jocn.2010.12.019
⇑ Corresponding author. Tel.: +82 2 6299 1501; faxE-mail address: [email protected] (Y.C. Youn).
We evaluated the volume reduction of gray matter (GM) and white matter (WM) in patients with an Alz-heimer’s disease (AD) assessment based on the Clinical Dementia Rating (CDR) score. Patients with AD(n = 61), with no subcortical WM ischemia, and healthy control patients (n = 33) underwent T1-weightedspoiled gradient echo sequences, which were analyzed using voxel-based morphometry. Global GM vol-ume reduction was observed in patients with a CDR score of 1 or a CDR score of 2, and WM volume reduc-tion was observed in patients with a CDR score of 2. Regional GM volume reduction was found in the rightinferior frontal gyrus, bilateral dorso-lateral and medial temporal lobes; WM volume reduction wasfound in the bilateral temporal subcortex (family-wise error, p < 0.01). A CDR score of 0.5 was associatedwith volume reduction in the left olfactory gyrus. The peak z-score and spatial extent of volume reductionincreased with increasing CDR score and were higher on the left side. GM volume reduction increasedwith increasing CDR scores and suggests a possible pathomechanism of AD.
� 2011 Elsevier Ltd. All rights reserved.
1. Introduction
Alzheimer’s disease (AD), the most common cause of seniledementia, is diagnosed as ‘‘definite AD’’ by specific neuropatho-logic changes, that is, the presence of neurofibrillary tanglesand amyloid plaques in brain tissue.1 These changes are associ-ated with neuronal and volume loss of the cerebral cortex.2,3
Clinically, efforts are being made to evaluate AD severity basedon other indicators such as the Mini-Mental State Examination(MMSE), the Clinical Dementia Rating (CDR) score and the GlobalDeterioration Scale. Due to technical limitations of whole brainanalyses and the analyses of certain regions, early quantitativestudies, using structural MRI, have focused on regions of interestsuch as the medial temporal lobe.4,5 Recently, many studies haveutilized voxel-based morphometry (VBM), an automated volu-metric analysis that is faster than previously used volumetricanalysis tools. Providing the study design and data parametersremain unaltered, VBM minimizes human error in the analytic
ll rights reserved.
: +82 2 6299 1493.
process, generating consistent results irrespective of the dataanalyst.6,7
Most studies using VBM have compared adults with mildcognitive impairment or patients with AD to control patients.Interestingly, some studies have found that changes in corticalatrophy in AD correlate with AD severity, as determined by theMMSE.8,9 Age and education level can impact MMSE scores.Accordingly, the clinical severity of AD is more strongly correlatedwith the CDR score than it is with the MMSE. In this study, wequantified differences in overall and regional brain volume basedon the CDR score, which is commonly used to evaluate dementiaseverity.
It is difficult to differentiate between subcortical ischemicvascular dementia and AD because the clinical symptoms progressslowly. In addition, many patients with AD show ischemic vascu-lar pathology. To improve dementia classifications, we semi-quantitatively evaluated the severity of white matter (WM)ischemia, using a modified version of the criteria used by Fazeka10
and Shelten.11
To evaluate the volume change of each tissue, we recruitedhealthy control patients (HC) and patients with AD who showedno more than minimal WM ischemic change. Patients were classi-fied according to dementia severity based on the CDR score.

S. Kim et al. / Journal of Clinical Neuroscience 18 (2011) 916–921 917
2. Materials and methods
2.1. Patients
We recruited patients with AD with memory and cognitionimpairment who visited the memory clinic in Chung-Ang Univer-sity Hospital between March 2008 and August 2009. All patientsand HC completed a standardized assessment protocol, which in-cluded history-taking, physical and neurological examinationsand blood tests (including hemoglobin, white cell count, serumelectrolytes, glucose, urea, creatinine, liver function tests, thyroidstimulating hormone and free thyroid hormone, and vitamins B1,B6 and B12). Patients also completed the NeuropsychologicalScreening Battery, the Korean version of the MMSE (K–MMSE)and the CDR score and underwent a brain MRI scan. All study par-ticipants provided their written informed consent to allow theirclinical data to be used for research purposes. This study was ap-proved by the Institutional Review Board.
The inclusion criteria for patients with AD were: (i) aged 60 orolder; (ii) a diagnosis of AD by a neurologist; (iii) probable AD diag-nosed using guidelines from the National Institute of NeurologicalDisorders and Stroke and the Association Internationale pour laRecherché et l’Enseignement en Neurosciences12; (iv) a K–MMSEscore between 10 and 26; (v) a CDR score between 0.5 (sum ofbox score [SOB] 3.5) and 2; and (vi) an MRI showing no specific le-sion capable of causing any significant cognitive impairment. Pa-tients with AD were further categorized into three levels basedon impairment severity using the CDR score: CDR scores of 0.5, 1and 2. We used the CDR (SOB) scores because: (i) although mostpatients with a CDR score of 0.5 fall within a category of ‘‘question-able’’ AD and have a high likelihood of converting to AD over time,diagnosing all patients who have a CDR score of 0.5 with AD is notrecommended13; (ii) most patients with a CDR score of 0.5 are con-sidered to have progressive dementia, but there are some whosedementia severity never worsens; and (iii) the likelihood of pro-gression to AD is strongly related to the SOB score.14
The inclusion criteria for HC were as follows: (i) aged 60 or old-er; (ii) no complaints of memory impairment by the individuals ortheir first-degree relatives; (iii) no functional impairment that af-fected daily living; (iv) a K–MMSE score between 27 and 30; and(v) no evidence of diabetes mellitus or other concurrent diseasecapable of causing cognitive impairment.
Table 1Characteristics of patients with Alzheimer’s Disease compared to healthy controlpatients
Classification Number Age� K–MMSE� Education (year)
HC 33 70.0 ± 4.7 27.4 ± 1.8 7.4 ± 5.6AD 61 – – –CDR 0.5 31 70.1 ± 5.0 20.8 ± 4.0 5.8 ± 5.2CDR 1 20 71.1 ± 6.1 16.4 ± 4.5 6.5 ± 5.4CDR 2 10 73.9 ± 5.5 12.2 ± 5.7 7.1 ± 6.1
All data represent mean ± standard deviation.AD = Alzheimer’s disease patients, CDR = Clinical Dementia Rating, Education =education duration, HC = healthy control patients, K–MMSE = Korean version of theMini-Mental State Examination.� AD versus HC (p = 0.239).� Each CDR group versus HC (p < 0.01).
2.2. Data acquisition and analysis
MRI were acquired using T1-weighted axial, T2-weighted axial,fluid-attenuated inversion recovery (FLAIR) and T1-weightedthree-dimensional (3D) volumetric spoiled gradient echo (SPGR)sequences on a Philips Intera Achieva 3.0 T scanner (Philips:Amsterdam, Netherlands).
Consecutive T1-weighted 3D volumetric SPGR sequences wereobtained with a 1 mm gap. Radiologists assessed the MRI of all pa-tients with AD and HC. For FLAIR images, we semi-quantitativelyevaluated the severity of WM ischemia using criteria modifiedfrom Fazeka10 and Shelten11, as proposed by the Clinical Researchfor Dementia committee of South Korea. Periventricular hyperin-tensities and deep WM hyperintensities (DWH) were evaluatedseparately. We recruited patients and HC whose MRIs demon-strated DWH with maximum diameters of less than 10 mm,including those adjacent to the anterior and posterior horns (cap-ping) or the lateral ventricles (bands).
Images were analyzed using MATLAB 7.5.0 (Mathworks, Natick,MA, USA) and Statistical Parametric Mapping 5 (SPM 5, WellcomeDepartment of Imaging Neuroscience, London, UK). For quantita-tive analysis of the whole brain, the images were reconstructed
using the standard VBM protocol: spatial normalization, segmenta-tion, and smoothing.5,15 Differences between the MRIs of each pa-tient were corrected according to the International Consortium forBrain Mapping template for East Asian Brains during normaliza-tion. Images were grouped by cerebrospinal fluid (CSF), gray mat-ter (GM) and WM based on standard SPM 5 tissue probabilitymaps. Subsequently, all custom options for normalization were leftunaltered. We checked image homogeneity using the VBM5toolbox (http://dbm.neuro.uni-jena.de/vbm/vbm5-for-spm5/). Allimages were smoothed with a 12-mm, full width-at-half-maxi-mum, isotropic Gaussian kernel to minimize cortical variation ofthe gyrus, which depends on the individual characteristics of thepatient.
2.3. Statistical global analysis
The total intracranial volume (TIV) of each patient was deter-mined from modulated GM, WM and CSF volumes. To analyze glo-bal volume changes, each tissue volume was normalized using theTIV, which was calculated as the sum of the GM, WM and CSF vol-umes. The normalization of tissue volumes was calculated bydividing the GM, WM and CSF volume by the TIV.
2.4. Statistical parametric maps
To detect GM and WM volume reductions in patients with AD,Student’s t-tests comparing patients with AD to HC were con-ducted on the processed images. We corrected for small meanage differences between the AD and HC groups when performingstatistical tests, assuming that the results of the cognitive testsand brain volume deteriorated with age. While it is well knownthat the extent of cortical atrophy varies with age, it is not clearwhether factors such as gender, education and environment im-pact cortical atrophy.16,17 Age and TIV were classified as nuisancecovariates in the comparisons of GM volumes between studygroups. The absolute threshold masking was 0.1. Results were con-sidered statistically significant at p < 0.01 and were corrected forfamily-wise error (FWE) or false discovery rate (FDR). This is anexploratory study; therefore, we used both types of corrections,and FWE is stricter than FDR.
3. Results
We enrolled 33 HC patients (mean age = 70.0 ± 4.7 years old)and 61 patients with AD (Table 1). Of the patients with AD, 31had a CDR score of 0.5 (mean age = 70.1 ± 5.0 years), 20 had aCDR score of 1 (mean age = 71.1 ± 6.1 years), and 10 had a CDRscore of 2 (mean age = 73.9 ± 5.5 years). Only patients with a CDRscore of 2 differed significantly from the HC group in age

918 S. Kim et al. / Journal of Clinical Neuroscience 18 (2011) 916–921
(p = 0.29, p = 0.47 and p = 0.02 for controls compared to CDR scoreof 0.5, 1 and 2, respectively).
3.1. Global changes in volume of GM, WM and CSF
Data are expressed as the mean volume (cm3) ± standard devi-ation (SD) (Fig. 1). The normalized GM volumes (GM/TIV) of HC,and those with a CDR score of 0.5, 1 and 2 were 0.384 ± 0.026,0.386 ± 0.023, 0.364 ± 0.035 and 0.351 ± 0.028, respectively. Thenormalized WM volumes (WM/TIV) were 0.281 ± 0.028, 0.288 ±0.025, 0.269 ± 0.032 and 0.258 ± 0.025, respectively. The GMvolumes were significantly reduced in patients with a CDR scoreof 1 (p = 0.032), a CDR score of 2 (p = 0.006), and the WM volumesof patients with a CDR score of 2 (p = 0.023) compared to HCpatients.
The normalized CSF volumes for HC patients, and those withCDR scores of 0.5, 1, and 2 were 0.336 ± 0.046, 0.326 ± 0.037,0.367 ± 0.058 and 0.392 ± 0.033, respectively. These data showedsignificantly increased CSF volumes in patients with CDR scoresof 1 (p = 0.04) and 2 (p = 0.00) compared to HC patients. However,there was no significant difference in TIV between any AD group(CDR scores of 0.5, 1502 ± 113.88; CDR score of 1,1513.46 ± 158.62; and CDR score of 2, 1506.47 ± 139.86) comparedto HC patients (1526.53 ± 121.56).
3.2. Voxel-based morphometry of GM and WM
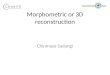
Overall GM and WM volume reductions in patients with ADare shown in Fig. 2 and statistically significant atrophic areashave been overlaid onto a normal brain template in MRIcron(http://www.cabiatl.com/mricro/mricron/index.html) using SPM 5.Regardless of their CDR score, patients with AD showed globalreductions in GM volume in the temporal, frontal, parietal andbasal ganglia (FDR < 0.05) compared to HC patients. When usingthe FWE correction, patients with AD showed GM reductions inthe left inferior and superior temporal lobes, right inferior frontal
Fig. 1. The normalized (A) gray matter (GM), (B) white matter (WM), (C) cerebrospinal flupatients with Alzheimer’s disease Clinical Dementia Rating (CDR) scores of 0.5, 1, and 2. ⁄pWM volume to TIV; CSFv/TIV = normalized CSF volume to TIV.
gyrus and several other areas (Fig. 2, Table 2). Patients with AD alsoshowed significant bilateral volume reduction, including the para-hippocampal gyrus, amygdala and hippocampus, though the re-sults were more intense in the left medial temporal structures.Additionally, WM volume reductions were observed in the subcor-tical WM of the bilateral temporal lobes, insula and cerebralpeduncles (FWE < 0.01) of patients with AD.
Regional GM volume reductions associated with dementiaseverity were found in the patients with AD compared to the HCgroup. The CDR 0.5 group showed volume reduction in the leftolfactory gyrus, left amygdala, left inferior temporal gyrus, rightsuperior temporal gyrus and bilaterally in the putamen (correctedFDR p < 0.01). When using the more strict FWE correction(p < 0.05), few regions showed differences between patients indifferent CDR groups.
The group with a CDR score of 1 showed greater volume reduc-tions in the left superior temporal gyrus, bilateral inferior temporalgyrus, right inferior frontal gyrus, bilateral parahippocampal gyrus,left uncus, left insula, right middle frontal gyrus and several otherareas (corrected FWE, p < 0.01; see Fig. 2, Table 3) compared to thepatients with a CDR score of 0.5. The group with a CDR score of 2showed bilateral cortical volume reduction in the uncus and supe-rior frontal gyrus, and their z-values were higher on the right sidethan on the left. This group also showed volume reduction of theright insula and inferior temporal and fusiform gyri. Finally, thegroup with a CDR score of 2 showed greater z-values of GM volumereductions in the medial temporal regions compared to patientswith a CDR score of 1.
4. Discussion
We focused on GM volume changes in patients with AD whoshowed clinically different states of deterioration compared tothose of healthy controls. We found global GM volume reductionsin patients with AD and also noted reductions in a number of
id (CSF) and (D) total intracranial volume (TIV) of healthy control patients (HC) and< 0.05. ⁄⁄p < 0.01. GMv/TIV = normalized GM volume to TIV; WMv/TIV = normalized

Fig. 2. Statistical parametric maps of (A, C) gray matter (GM) and (B) white matter (WM) volume reductions in Alzheimer’s disease. FWE = family-wise error.
Table 2Area of grey matter density reduction in Alzheimer’s disease (family-wise errorcorrected p < 0.01)
Coordinates x, y, z Anatomical location z-score
�33 �13 �40 Left inferior temporal gyrus Positive infinite�17 �10 �27 Left parahippocampal gyrus 7.7730 20 �15 Right inferior frontal gyrus 7.66�42 7 �18 Left superior temporal gyrus 7.4923 �17 �23 Right parahippocampal gyrus 7.29�21 �5 �23 Left amygdala 7.04�26 �18 �18 Left hippocampus 6.90�16 12 8 Left caudate 6.4021 �5 �19 Right amygdala 5.7432 �19 �17 Right hippocampus 5.51
S. Kim et al. / Journal of Clinical Neuroscience 18 (2011) 916–921 919
specific regions. As expected, the global volumes of GM and WMwere reduced in the AD cohort, but TIV was not changed withCDR score. The global volume reductions in GM and WM werenot noted in the patients with a CDR of 0.5, but rather were slightlyincreased. When considering the focal volume changes, such asmedial, temporal and related tissues after normalization, these re-sults suggest that a structural and/or functional compensatorymechanism could be present in uninvolved regions of thebrain.18–20
In particular, we found GM volume reductions in the left infe-rior and superior temporal, right inferior frontal and bilateral med-ial temporal lobes, including the parahippocampal gyrus, amygdalaand hippocampus. The WM volume reductions were also mostprominent in their related subcortical areas: the bilateral temporaland insula. This is consistent with previous studies that also foundatrophy in these areas in patients with AD.4,8,9,21–23 We did not findany GM volumetric differences in the sensorimotor and visualcortices, consistent with previously published reports.24,25
GM volume reductions were not found in the lower parietal,cingulate or precuneus areas, even in patients with a CDR scoreof 2, possibly due to the recruitment of patients over 60 years ofage with late-onset AD. One previous study found that patientswith early-onset AD showed bilateral reductions in the medialtemporal lobes, inferior parietal lobules, the precuneus and perisyl-vian cortices, the right inferior frontal gyrus and bilaterally in thecingulate cortices, whereas late-onset patients with AD showedatrophy in only the bilateral medial temporal cortices.26
Consistent with previous studies examining the early stages ofAD, our patients exhibited significant GM reductions in the hippo-campus, parahippocampal gyrus, amygdala and superior/inferiortemporal gyrus. The patients with a CDR score of 0.5 showedreductions in the left olfactory gyrus, amygdala and entorhinal cor-tex (a cluster within the inferior temporal gyrus). Damage to theentorhinal cortex, which projects to the hippocampus from neocor-tical inputs, interferes with episodic memory consolidation in pa-tients with AD. The volumetric reductions seen in this regionmay help explain reports of episodic memory loss in early stagesof AD.27,28 The patients with a CDR score of 0.5 also showed re-duced volume in the left putamen, an area involved in reinforce-ment learning and implicit learning. This finding is supported byprevious studies suggesting the involvement of the putamen andcaudate nucleus in AD pathology. Although dopamine and tonicallyactive neurons have a key role in learning and memory, the exactmechanisms are not known.29,30 Taken together, our findings sug-gest that structural differences might underlie the cognitive andbehavioral deficits observed in patients with AD.
Compared to patients with a CDR score of 0.5, the patients witha CDR score of 1 showed atrophy of the medial temporal lobe, spe-cifically in the uncus, hippocampus, parahippocampal gyrus, olfac-tory gyrus and entorhinal cortex. The present study also delineatedthe order of hippocampal atrophy, which progressed from the

Fig. 3. Areas of statistically significant volume reduction of gray matter in patients with Alzheimer’s disease with Clinical Dementia Rating (CDR) scores of (A) 0.5, (B) 1and (C)2. FDR = false discovery rate, FWE = family-wise error.
Table 3Area of grey matter density reduction in patients with Alzheimer’s disease as assessed by Clinical Dementia Rating score (corrected for family-wise error p < 0.05; or ⁄falsediscovery rate p < 0.01)
CDR score of AD Coordinates x, y, z Anatomical location z-score
0.5⁄ �20 7 15 Left putamen 5.28�21 8 �15 Left olfactory gyrus 5.2142 8 �20 Right superior temporal gyrus 5.11�31 �1 �43 Left inferior temporal gyrus 4.4417 12 3 Right putamen 4.28�21 �5 �23 Left amygdala 4.23
1 �42 8 �17 Left superior temporal gyrus 6.2731 20 �19 Right inferior frontal gyrus 5.80�65 �13 �24 Left inferior temporal gyrus 5.80�18 �9 �19 Left parahippocampal gyrus 5.63�62 �20 �27 Left fusiform gyrus 5.58�43 �11 2 Left insula 5.5225 �20 �17 Right parahippocampal gyrus 5.5067 �18 �23 Right inferior temporal gyrus 5.41�13 �5 �26 Left uncus 5.2229 �21 �14 Right hippocampus 5.2055 3 41 Right middle frontal gyrus 5.17
2 16 �10 �31 Right uncus 6.5525 60 25 Right superior frontal gyrus 6.29�19 �14 �30 Left uncus 5.9819 8 �19 Right inferior frontal gyrus 5.6642 2 �6 Right insula 5.3667 �18 �18 Right inferior temporal gyrus 5.30�17 37 50 Left superior frontal gyrus 5.2962 �9 �29 Right fusiform gyrus 5.24�61 �13 �30 Left fusiform gyrus 5.23�26 �18 �18 Left hippocampus 5.2132 �19 �17 Right hippocampus 5.15�40 6 �15 Left superior temporal gyrus 5.00
AD = Alzheimer’s disease, CDR = Clinical Dementia Rating score.
920 S. Kim et al. / Journal of Clinical Neuroscience 18 (2011) 916–921
uncus, olfactory and entorhinal gyri to the middle and entire hip-pocampus. This finding supports the theory that AD-related hippo-campal atrophy, which may be due to extra-hippocampal fiberdegeneration converging on the hippocampus rather than neuronal
loss in the hippocampus, is secondary to entorhinal cortical degen-eration.27 However, because this study was cross-sectional, we donot know if these volumetric differences were caused by the pro-gression of AD.

S. Kim et al. / Journal of Clinical Neuroscience 18 (2011) 916–921 921
Even though we found GM reductions in patients with AD com-pared to HC, some of our measurements within the AD group didnot appear to support our hypothesis of reduced GM volume corre-lating with AD deficits. The patients with a CDR score of 2 showedgreater peak z- scores of GM volume reduction in the medial tem-poral area, which is related to memory and other cognitive func-tions, than the patients with a CDR score of 1. However, theextent of spatial distribution of the clinical deterioration effecton other areas was limited in the group with a CDR score of 2 com-pared to the CDR 1 group. One possible explanation is that this wascross-sectional rather than longitudinal study. Patients in the sameCDR cohort have heterogeneous clinical and cognitive impairmentsthat are not continuous through CDR ratings. Additionally, care-giver behavior could affect the characteristics of patients with aCDR score of 1. Caregivers are typically more concerned aboutabnormal non-cognitive behavior than general cognitive declinein the early stages of AD. This could impact volume changes inthe right frontal lobe in patients with moderate dementia(Fig. 3B). We did not find progressive deterioration of the basalganglia with increasing CDR score and this may be explained inseveral ways. First, as previously discussed, this result could bedue to our study being a cross-sectional study and not a longitudi-nal study. Second, we used different statistical cut-off values forSPM 5 between CDR scores of 0.5 and 1. Additionally, becausewe applied TIV as a covariate to correct for global effects and the‘‘normalization process’’ in the VBM protocol, all brains had equaldistributions of volume throughout, except for focally atrophicareas. Thus, a diffuse atrophic brain, even if more severe globalatrophic changes exist, will be reported as having a greater volumethan a focally atrophic brain. Furthermore, if the volume reductionrate differs or follows non-linear patterns in each region, thenprobability maps and z-scores could vary among the CDRgroups.17,31,32 To evaluate the progression of cortical volumereduction with clinical deterioration, further longitudinal studiesare needed.
In conclusion, we found global and regional volume reductionsin GM and WM across CDR scores in patients with AD, excludingthose patients with potential subcortical ischemic vascular demen-tia. Longitudinal follow-up studies are needed to determinewhether these volumetric differences can be attributed to the pro-gression of AD.
Acknowledgement
This research was supported by a Chung-Ang UniversityResearch Grant in 2008.
References
1. Parihar MS, Hemnani T. Alzheimer’s disease pathogenesis and therapeuticinterventions. J Clin Neurosci 2004;11:456–67.
2. Bell-McGinty S, Lopez OL, Meltzer CC, et al. Differential cortical atrophy insubgroups of mild cognitive impairment. Arch Neurol 2005;62:1393–7.
3. Mouton PR, Martin LJ, Calhoun ME, et al. Cognitive decline strongly correlateswith cortical atrophy in Alzheimer’s dementia. Neurobiol Aging 1998;19:371–7.
4. Whitwell JL, Przybelski SA, Weigand SD, et al. 3D maps from multiple MRIillustrate changing atrophy patterns as subjects progress from mild cognitiveimpairment to Alzheimer’s disease. Brain 2007;130:1777–86.
5. Villemagne VL, Rowe CC, Macfarlane S, et al. Imaginem oblivionis: the prospectsof neuroimaging for early detection of Alzheimer’s disease. J Clin Neurosci2005;12:221–30.
6. Whitwell JL, Jack Jr CR. Neuroimaging in dementia. Neurol Clin 2007;25:843–57[viii].
7. Ashburner J, Friston KJ. Why voxel-based morphometry should be used.Neuroimage 2001;14:1238–43.
8. Apostolova LG, Lu PH, Rogers S, et al. 3D mapping of mini-mental stateexamination performance in clinical and preclinical Alzheimer disease.Alzheimer Dis Assoc Disord 2006;20:224–31.
9. Frisoni GB, Testa C, Zorzan A, et al. Detection of grey matter loss in mildAlzheimer’s disease with voxel based morphometry. J Neurol NeurosurgPsychiatry 2002;73:657–64.
10. Fazekas F, Chawluk JB, Alavi A, et al. MR signal abnormalities at 1.5 T inAlzheimer’s dementia and normal aging. AJR Am J Roentgenol 1987;149:351–6.
11. Scheltens P, Barkhof F, Leys D, et al. A semiquantative rating scale for theassessment of signal hyperintensities on magnetic resonance imaging. J NeurolSci 1993;114:7–12.
12. McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’sdisease: report of the NINCDS-ADRDA Work Group under the auspices ofDepartment of Health and Human Services Task Force on Alzheimer’s Disease.Neurology 1984;34:939–44.
13. Saxton J, Snitz BE, Lopez OL, et al. Functional and cognitive criteria producedifferent rates of mild cognitive impairment and conversion to dementia. JNeurol Neurosurg Psychiatry 2009;80:737–43.
14. Daly E, Zaitchik D, Copeland M, et al. Predicting conversion to Alzheimerdisease using standardized clinical information. Arch Neurol 2000;57:675–80.
15. Ashburner J, Friston KJ. Voxel-based morphometry–the methods. Neuroimage2000;11:805–21.
16. Abe O, Yamasue H, Yamada H, et al. Sex dimorphism in gray/white mattervolume and diffusion tensor during normal aging. NMR Biomed2010;23:446–58.
17. Allen JS, Bruss J, Brown CK, et al. Normal neuroanatomical variation due to age:the major lobes and a parcellation of the temporal region. Neurobiol Aging2005;26:1245–60 [discussion 79–82].
18. Guedj E, Barbeau EJ, Didic M, et al. Effects of medial temporal lobe degenerationon brain perfusion in amnestic MCI of AD type: deafferentation and functionalcompensation? Eur J Nucl Med Mol Imaging 2009;36:1101–12.
19. Qi Z, Wu X, Wang Z, et al. Impairment and compensation coexist in amnesticMCI default mode network. Neuroimage 2010;50:48–55.
20. Stott J, Spector A. A review of the effectiveness of memory interventions in mildcognitive impairment (MCI). Int Psychogeriatr 2010;15:1–13.
21. Fotenos AF, Snyder AZ, Girton LE, et al. Normative estimates of cross-sectionaland longitudinal brain volume decline in aging and AD. Neurology2005;64:1032–9.
22. Karas G, Sluimer J, Goekoop R, et al. Amnestic mild cognitive impairment:structural MR imaging findings predictive of conversion to Alzheimer disease.AJNR Am J Neuroradiol 2008;29:944–9.
23. Chetelat G, Fouquet M, Kalpouzos G, et al. Three-dimensional surface mappingof hippocampal atrophy progression from MCI to AD and over normal aging asassessed using voxel-based morphometry. Neuropsychologia 2008;46:1721–31.
24. Postiglione A, Lassen NA, Holman BL. Cerebral blood flow in patients withdementia of Alzheimer’s type. Aging (Milano) 1993;5:19–26.
25. Blesa R, Mohr E, Miletich RS, et al. Cerebral metabolic changes in Alzheimer’sdisease: neurobehavioral patterns. Dementia 1996;7:239–45.
26. Ishii K, Sasaki M, Kitagaki H, et al. Reduction of cerebellar glucose metabolismin advanced Alzheimer’s disease. J Nucl Med 1997;38:925–8.
27. Mizutani T, Kasahara M. Hippocampal atrophy secondary to entorhinal corticaldegeneration in Alzheimer-type dementia. Neurosci Lett 1997;222:119–22.
28. Lehmann M, Crutch SJ, Ridgway GR, et al. Cortical thickness and voxel-basedmorphometry in posterior cortical atrophy and typical Alzheimer’s disease.Neurobiol Aging in press, 2009 [Epub ahead of print].
29. Cross AJ, Crow TJ, Ferrier IN, et al. Striatal dopamine receptors in Alzheimer-type dementia. Neurosci Lett 1984;52:1–6.
30. Dai W, Lopez OL, Carmichael OT, et al. Mild cognitive impairment andalzheimer disease: patterns of altered cerebral blood flow at MR imaging.Radiology 2009;250:856–66.
31. Grieve SM, Clark CR, Williams LM, et al. Preservation of limbic and paralimbicstructures in aging. Hum Brain Mapp 2005;25:391–401.
32. Mechelli A, Friston KJ, Frackowiak RS, et al. Structural covariance in the humancortex. J Neurosci 2005;25:8303–10.