Embed Size (px)
Citation preview

CURRENT INDIAN EYE RESEARCH 1
Current Indian Eye ResearchJournal of Ophthalmic Research Group
(Peer reviewed open access journal)
Editor:Dr Sambuddha Ghosh
Associate Editor:Dr. Somnath Mukhopadhyay
Editorial Office:16B Prince Golam Mohammad Road,Kolkata- 700026
Contact:Phone: 033 40071886E-mail: [email protected]
Contents
Editorial 2Eye Research in India
Sambuddha GhoshReview ArticlePathogenesis and Management of Diabetic Macular Edema 3
Atul Kumar, Sangeeta Roy, Subijay SinhaOriginal ArticleXeno-Free Autologous Cultivated Oral Mucosal Epithelial Transplantationfor Bilateral Ocular Surface Burns: Clinical Outcomes andImmunohistochemical Analysis 17
Subhash Gaddipati, Sayan Basu, Geeta K Vemuganti, Muralidhar Ramappa,Savitri Maddileti, Virender S Sangwan
Combination of Azathioprine and Corticosteroids in the Treatment ofSerpiginous Choroiditis 25
Aneesha Lobo, Prachir Agarwal, Debmalya Das, Manmath Das,Rupak Roy, Jyotirmay Biswas
Community Based Intervention for Preventing Corneal Injury fromPaddy Grain 30
Asim Kumar SilRetinal Vascular Caliber Measurement through MahalanobisDistance Function based Segmentation 33
Subhamoy Chatterjee, Souvik Dasgupta, Jyotirmoy Chatterjee,Sambuddha Ghosh
Case SeriesMultilayered Amniotic Membrane Transplantation for Mooren's Ulcer – A CaseSeries of Ten Patients 36
Jayanta Dutta, Somnath Mukhopadhyay, Himadri Datta, Tamojit ChatterjeeResearch MethodologyMultivariable Analysis 39
Bijay Prasad MukhopadhyayCommentaryOphthalmology beyond Ophthalmologists and Also Including Ophthalmologists 42
Garga ChatterjeeHistory of OphthalmologyFamous Ophthalmologists Who Suffered from Eye Disorders 44
Debmalya DasAuthor Guideline 46
Cover photo:colourized scanningelectron micrograph of rods and cones
For free circulation
Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH2
EditorialEye Research in India
Ophthalmic research in India has a glorious past1,2 and a vibrant present3.Sushruta, who practiced during the 5th century BC, classified eye diseases in the Uttar Tantram according to signs,symptoms, prognosis, and management. Sushruta’s description of cataract surgical method was probably the first accounton extracapsular cataract surgery1.Indian ophthalmologists inherit the amazing contribution to ophthalmic research by scholars like King Serfoji II of Thaanjavur,who carried out methodical ophthalmic practices between 1798 and 1832 and kept detailed records with the help ofcharts and manuscripts2.In a bibliometric analysis of Indian ophthalmic papers published from 2001 to 2006 in peer-reviewed journals, a neardoubling of the annual output of research articles was observed, two-thirds of these being published in internationaljournals3.However the same study showed that 50% of the publications were contributed by only nine major eye hospitals in Indiaand articles on basic science were the least common type in that series3.Ophthalmic literature from developed and developing countries were compared in a retrospective review of the fivehighest scoring impact factor journals in ophthalmology within the 3 year period 1998-2000. Contribution from the developingworld was only 5.47% of the literature compared to 92.19% from the developed world; only 2.33% being the collaborativeresearch from the two groups4.While developing countries account for the vast majority of world blindness, this inverse relationship between burdenand research contribution demands urgent attention from Indian scientists engaged in ophthalmic research.Only 16.5% of the free papers presented at the All India Ophthalmic Society Annual Conference 2000 were publishedover the next seven years in journals indexed with Pubmed5.Another study showed that only 30% of theses prepared by postgraduate students from a university medical college inIndia were later published6.Current Indian Eye Research plans to publish articles based on researches conducted in the Indian perspective withspecial thrust on inter disciplinary research. Emerging issues in ophthalmology will find special place in this journal. We particularly look forward towards young researchers and trainees toiling hard on their research work. We hope thattheir work may find useful place and recognition in this journal.I thank all contributors for their overwhelming response in our first issue.
References1. Kansupada KB, Sassani JW. Sushruta: the father of Indian surgery and ophthalmology. Doc Ophthalmol 1997; 93:
159-67.2. Biswas J, Badrinath V, Badrinath SS. Ophthalmic contributions of Raja Serfoji II (1798-1832). Indian J Ophthalmol
2012; 60: 297-300.3. Kumaragurupari R, Sieving PC, Lalitha P. A bibliometric study of publications by Indian ophthalmologists and vision
researchers, 2001-06. Indian J Ophthalmol 2010; 58: 275-80.4. Mandal K, Benson S, Fraser SG. The contribution to ophthalmic literature from different regions of the world. Int
Ophthalmol 2004; 25: 181-4.5. Dhaliwal U, Kumar R. An observational study of the proceedings of the All India Ophthalmological Conference, 2000
and subsequent publication in indexed journals. Indian J Ophthalmol 2008; 56: 189–95.6. Dhaliwal U, Singh N, Bhatia A. Masters theses from a university medical college: Publication in indexed scientific
journals. Indian J Ophthalmol 2010;58:101-4.
Sambuddha GhoshEditor
[email protected]@gmai.com
Volume 1, Issue 1, June 2014

CURRENT INDIAN EYE RESEARCH 3
Pathogenesis and Management of Diabetic Macular EdemaAtul Kumar1, Sangeeta Roy1, Subijay Sinha2
Review ArticleReview ArticleReview ArticleReview ArticleReview Article
1. Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi-110029;2. Susrut Eye Foundation and Research Centre, Sector-III, Salt Lake City, Kolkata 700106.Corresponding Author : Dr. Subijay Sinha, E-mail: [email protected] on : 04/05/2014, Accepted on : 30/05/2014Conflict of Interest : None, Financial Disclosure : None
Diabetic macular edema (DME) is one of the majorcauses of vision loss in patients with diabetic
retinopathy. It is defined as retinal thickening in theposterior pole essentially resulting from increasedpermeability of retinal vasculature leading to the disruptionof the blood retinal barrier and other alterations in theretinal micro-environments1.
Though chronic hyperglycemia is the primary factorleading to the development of diabetic retinopathy, themechanisms by which elevated blood sugar levels leadto the development of DME and the histopathologicallyvisible changes are still not clear.
DME may result from leakage of micro aneurysms or itmay be due to diffuse leakage of hyper permeablecapillaries. It may or may not be characterised byintraretinal cyst formation and also sub retinal fluid in thesettings of severe cystic thickening involving the fovea.To characterize the severity of macular edema and fortreatment guidelines, the term clinically significant macularedema (CSME) is used. Macular edema is clinicallysignificant if one of the following conditions is present:retinal thickening at or within 500 um of the center of themacula; and/or hard exudates at or within 500 um of thecenter of the macula if associated with thickening of theadjacent retina; and/or a zone or zones of retinalthickening 1 disk area in size, at least part of which iswithin 1 disk diameter of the macular center2,3.
Pathogenesis of diabetic macular edema
Biomechanical mechanisms in pathogenesis ofdiabetic macular edema
1. The aldose reductase pathway
Aldose reductase uses the reduced form of nicotinamideadenine dinucleotide phosphate as a cofactor to reduce
many aldose sugars into their respective sugar alcohol.Glucose is reduced to sorbitol, which is then oxidised tofructose by sorbitol dehydrogenase. In normoglycemicconditions, the aldose reductase pathway is non-operativeas glucose is a poor substrate for aldose reductasebecause of its high binding constant. Although, in thesettings of hyperglycemia the aldose reductase pathwaysare activated which further lead to osmotic stress due toaccumulation of sorbitol. Increase in the utilisation ofaldose reductase in the hyperglycemic state of diabeteswill result in a decline of intracellular NADPH that altersthe cellular redox balance4. These lead to oxidative stressand result in cellular damage.
2. Advanced glycation protein endproduct theory
Nonenzymatic glycation and cross linking of proteins havebeen proposed as a mechanism to explain thecomplications of diabetes5. Chronic hyperglycemia leadsto the formation and accumulation of AGEs that may be aprimary contributor to diabetic microvasculopathy. AGEsform on the amino groups of proteins, lipids, and DNAwith complex cross-links and lead to modification in thestructure and function of proteins6. Formation of AGEsmay directly damage the cells by impairing the functionof a variety of protein both extracellular and intracellular.The cellular effects of AGEs9ii is also mediated by itsbinding to receptors, namely receptor for AGE (RAGE)are attached to the foot plates of Muller cells. Whenactivated they can initiate a cascade of signal transductioninvolving at least p21, p44/p42 mitogen activated proteinkinase(MAPK) Nuclear factor kappaB(NB-kB) and proteinkinase C which further lead to cellular damage7-9.Upregulation of VEGF is seen in Muller cells along withincreased expression of glial fibrillary acidic protein(GFAP), which causes increased reactive gliosis, whenRAGE is activated10.

CURRENT INDIAN EYE RESEARCH4
3. Reactive oxygen intermediate theory
The byproducts of oxidative phosphorylation includes freeradicals such as superoxide anion, whose production isincreased by high levels of glucose11. Free radicals notonly damage the cellular proteins, it also reduces nitricoxide levels12, promotes leukocyte adhesions to theendothelium and decreases the barrier function ofendothelial cell13. Oxidative stress can also activate PKCby increasing the formation of diacylglycerol.
4. Protein kinase C theory
Activation of PKC by phorbol esters is associated withincreased permeability in epithelial and endothelial culturecells14. It seems that certain PKC isoforms may play animportant role in VEGF induced vasopermeability. PKCinhibitors specific for the PKC-b isoform have been shownto significantly reduce VEGF-induced fluoresceinleakage15.
5. Insulin receptors and glucose transporters
There are at least 5 different types of facilitated cellmembrane glucose transporters designated GLUT 1, GLUT2, GLUT 3, GLUT 4 and GLUT 5 that appear to be themost impoetant for the intracellular transport of glucose inthe tissues like retina that do not require insulin. Of theseGLUT 1 appears to be most prevalent in the retina16,17,occurring in the microvascular and macrovascularendothelial cells and on RPE cells as well as in the Mullercells. These up regulations of the cell membrane glucosetransporters could be a mechanism that initiates glucosemediated damage by permitting a much greater influx ofglucose into cells.
6. Vascular endothelial growth factors:
VEGF-A belongs to a gene family that includes placentalgrowth factor (PGF), VEGF-B, VEGF-C, and VEGF-D.VEGF-A recently has come to be accepted as one of themost potent factors inducing angiogenesis. Six majorisoforms exist: 121, 145,165, 183, 189, and 206. VEGF-Ais a ligand for two receptor tyrosine kinases, VEGFR-1and VEGFR-2,both of which act through downstreamsignalling cascades18. VEGF-A,especially the VEGF-165isoform, is emerging as an important factor in the patho-physiology of DME. VEGF is produced by RPE cells,ganglion cells, Muller cells, pericytes, endothelial cells, glialcells, neurons19,20, and smooth muscle cells of the diabeticretina. Up regulation of VEGF by hypoxia occurs in all ofthese cell types15. Muller cells are the most importantsource of VEGF in the retina due to their high rate of
glycolysis. VEGF produces conformational changes in thetight junctions of retinal vascular endothelial cells15. VEGFinduces phosphorylation of the tight junction proteins,occludin and ZO-1, which leads to increased vascularpermeability by phos-phorylation of adherent junction andcytoskeletal proteins of vascular endothelial cells andinduction of fenestrations in endothelial cell membranes.VEGF also may be associated with the early inflammatorychanges seen with diabetic retinopathy and DME. In earlydiabetes, vitreous levels of VEGF are elevated.
7. Other vasoactive substances
There are other vasoactive substances like histamine,Angiotensin II21, Matrix meta-lloproteinase22, Pigmentepithelium derived growth factor23, Platelet derived growthfactor24 and basic fibroblast growth factor25 also plays animportant role in the pathgenesis of diabetic macularedema.
Anatomical and histological changes responsible forpathogenesis of diabetic macular edema
1. Loss of pericytes:
Loss of pericytes is one of the earliest and most specificsigns of diabetic retinopathy. Pericytes are contractile cellsthat play an important role in the microvascularautoregulation26. Loss of pericytes leads to alteration ofvascular intercellular contacts and impairment of bloodretinal barrier. Loss of intercellular contact also appears topromote endothelial cell proliferation resulting in thedevelopment of microaneurysms27. Two major theories thathave been implicated for the loss of pericytes are aldosereductase pathway and the platelet derived growth factorbeta.
2. Capillary basement membrane thickening
Electron microscopic findings in diabetics show thickeningof the capillary basement membrane along with depositionof fibrillar collagen and swiss cheese vacuolisation of theotherwise homogenous pattern of the basement membranecollagen. Biochemical reactions like aldose reductasepathway, sorbitol pathway28,29 and enzymatic ornonenzymatic glycation of the basement membranecollagen30 have been play important role in the thickeningof the basement membrane.
3. Break down of the blood retinal barrier
Break down of the blood retinal barrier is an importantpathologic factor responsible for the development ofdiabetic macular edema. One mechanism by which thereis a breakdown of the blood retinal barrier is opening of
DME ReviewDME ReviewDME ReviewDME ReviewDME ReviewVolume 1, Issue 1, June 2014

CURRENT INDIAN EYE RESEARCH 5
the tight junctions,also known as zonula occludensbetween the vascular endothelial cell processes31. VEGFalso palys an important role in the breakdown of the innerblood retinal barrier by altering the endothelial cell tightjunctions20. The other mechanism involved the increase inthe vascular permeability is kallikrein kinin system throughthe production of bradykinin which in turn causesvasorelaxation of the retinal arterioles via nitric oxise32.
4. Vitreoretinal interface
Clinical and anatomical evidence indicates thatabnormalities in the structure of the vitreo retinal interfacemay play an important role in the pathogenesis of DME33,34.DME may be exacerbated due to persistent vitreomaculartraction by the residual cortical vitreous on the macula afterPVD, thickened and taut posterior hyaloid that may or maynot be adherent to ILM, macular traction due to tractionalproliferative membranes, or loculation of cytokines in thepre-macular vitreous pocket. A diabetic retina compromiseddue to microvascular abnormalities may be vulnerable toincreased exudation in the presence of any maculartraction.
Classification of diabetic macular edema
The Early Treatment Diabetic Retinopathy Study (ETDRS)defined DME as retinal thickening or presence of hardexudates within 1 disk diameter of the center of the macula.To characterize the severity of macular edema and fortreatment guidelines, the term clinically significant macularedema (CSME) is used. Macular edema is clinicallysignificant if one of the following conditions is present:retinal thickening at or within 500 µm of the center of themacula and/or hard exudates at or within 500 µm of thecenter of the macula if associated with thickening of theadjacent retina; and/or a zone or zones of retinal thickening1 disk area in size, at least part of which is within 1 diskdiameter of the macular center2,3. On optical coherencetomography the DME can be classified into central involvingand noncentral involving macular edema based on thepresence or absence of cystic spaces at the central foveathereby increasing the central foveal thickness. It isimportant to differentiate DME into central involving or noncentral involving as the treatment protocol for the each isdifferent.(Figure 1a and b)
Extrafoveal foci of retinal thickening and hard exudatesmay not cause any symptoms or affect visual acuity butDME that involves or threaten the centre of the maculacause significant vision loss. In the ETDRS, the 3 year
risk of moderate vision loss among untreated DME isaround 32%2. In focal CSME, discrete points of retinalhyperfluorescence are present on the FA due to focalleakage of micro-aneurysms35. The discrete leakingmicroaneurysms are thought to cause retinal thickening.Commonly, these leaking microaneurysms are surroundedby circinate rings of hard exudates. The exudates arelipoprotein deposits in outer retinal layers. In diffuse DME,areas diffuse leakage are noted on the FA due intraretinalleakage from a dilated retinal capillary bed and/orintraretinal microvascular abnormalities RMA), and/or (insevere cases) from arterioles and venules without discretefoci of leaking microaneurysms .There may be associatedcystoid macular edema (CME). Cystoid macular edemaresults from a generalized breakdown of the inner BRBwith fluid accumulation, primarily in the outer plexiformlayer36.
Management of diabetic macular edema
Diagnostic imaging techniques
1. Fundus fluorescein angiography
Fluorescein angiography is a standard method used toevaluate patients with DME that is sensitive for qualitativedetection of fluid leakage37. The DME can be classified asfocal and diffuse with the help of fundus fluoresceinangiography. It also helps us to diagnose macular ischemia.Fundus photography is an important tool to look for theprogression of the retinopathy in individual patients.
Figure 1a: Optical Coherence tomographyshowing noncentre involving DME
Figure 1b: Optical Coherence tomographyshowing centre involving DME
DME ReviewDME ReviewDME ReviewDME ReviewDME Review Volume 1, Issue 1, June 2014

CURRENT INDIAN EYE RESEARCH6
2. Optical coherence tomography
OCT has been used for high-resolution imaging of the retinaand detection of increased retinal thickness. OCT hasseveral advantages as a retinal imaging technique: 1) it isnon-invasive (no injected dye involved) and well tolerated(especially important in children); 2) it provides quantitativeinformation regarding retinal thickness with a high degreeof accuracy and reproducibility; 3) it clearly reveals thepresence and extent of vitreomacular traction. As shownby Chan and Duker, central macular thickness on OCT isa highly useful method for evaluation and comparison ofthe different therapeutic modalities for DME38.
Treatment
Systemic therapy for DME
The main aims of systemic therapy in DR/DME are toreduce the risk of diabetic patients developing theseconditions in the first place and to reduce the risk ofprogression of existing retinopathy or maculopathy to moresevere, sight-threatening forms.
Modifying metabolic control
Improving glycemic control and lowering the level ofglycosylated hemoglobin (HbA1c) is, at present, the mosteffective medical treatment to slow the progression ofDR.This was proven by the Diabetes control andcomplications trial (DCCT) in type 1 diabetics39 and theUnited Kingdom prospective diabetes study40. As per DCCTthere was a 35%-40% reduction in the risk of retinopathyprogression for every 10% decrease in HbA1C39. Accordingto UKPDS for every percentage point decrease in HbA1Cthere was a 35% decrease in the risk of microvascularcomplications40. Intensive glycemic control was found tohave effects that persist well beyond the course oftreatment. The DCCT and UKPDS established optimizingmetabolic control as a priority and led to the suggestionthat it should be implemented early and maintained for aslong as is safely possible. Although, the intensive controlarm of the Action to Control Cardiovascular Risk inDiabetes (ACCORD) study was stopped because ofincreased all-cause mortality in people whose glucose wasextremely tightly controlled with insulin and multiple oralagents.
Modifying hypertension
Hypertension is a major risk factor for DR and DME. TheUKPDS demonstrated that control of blood pressure(systolic blood pressure <150 mmHg) led to a reduction in
the progression of diabetic retinopathy and reduced needfor laser treatment in the tight blood pressure control groupcompared with the less tight control group41. More intensiveblood pressure control resulted in a 37% reduction in themicrovascular complications of DM.
Lipid lowering agent
Lipid lowering agents may decrease the risk of vision lossin patients with DR. The Fenofibrate Intervention and EventLowering in Diabetes (FIELD) study on the effects of long-term fenofibrate on cardiovascular events in patients withtype 2 diabetes found beneficial effects on microvascularcomplications that included DR. There were significantbenefits in terms of the requirement for first laser anddevelopment of DME42. The ACCORD-Eye study confirmedthe results of the FIELD study. In ACCORD-Eye, theaddition of fenofibrate to basal statin therapy resulted in asignificant reduction in the progression of retinopathy, in asimilar manner to that observed with intensifying bloodglucose control, but with a good safety profile and withoutincreasing the risk of hypoglycemia43.
Ocular therapy for diabetic macular edema
Laser therapy
The ETDRS study was designed to evaluate the effects ofargon laser photocoagulation for macular edema in aprospective, randomized, multicentre clinical trial. At 3years, eyes with mild or moderate NPDR with macularedema at baseline treated with immediate focal/grid laserphotocoagulation showed an approximately 50% decreasein the rate of moderate vision loss3. Study done byDRCR.net compared the efficacy of modified ETDRS gridwith mild macular grid in DME44. In mild macular grid mildwidely placed burns throughout the macula, both in thethickened and non thickened areas. At 12 months aftertreatment, the MMG technique is less effective at reducingOCT measured retinal thickening than the more extensivelyevaluated current modified ETDRS laser photocoagulationapproach. However, the visual acuity outcome with bothapproaches is not substantially different. Since the adventof anti VEGFs the role of focal laser in DME is decreasingalthough the efficacy of modified ETDRS grid in non centralinvolving DME had been studied by DRCR.net. Focal/gridlaser in these non-CI eyes was associated with relativelystable visual acuity and retinal thickness measurements,and decreased fluorescein leakage area at 1 year45. Focalor grid laser can cause a scotoma within 20o of the centralfixation, choroidal neovascularisation and subsequentfibrosis.
DME ReviewDME ReviewDME ReviewDME ReviewDME ReviewVolume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH 7
Pharmacotherapy for DME
Although it has been the mainstay of DME treatment fordecades, laser monotherapy has some importantlimitations. Intravitreal injections of anti-VEGF agents haverecently replaced ETDRS-style macular laser as the choicefor initial treatment of center-involving DME, likely basedon the results of several well-controlled randomized clinicaltrials. In recent DRCR.net reports, treatment with modifiedETDRS laser resulted in stable or improved vision in amajority of patients, but close to 20% of patients lost >10letters of visual acuity46,47. The efficacy of anti VEGF likeranibizumab, bevacizumab and aflibercept has beenstudied in different studies done by DRCR.net.
(a) Ranizumab
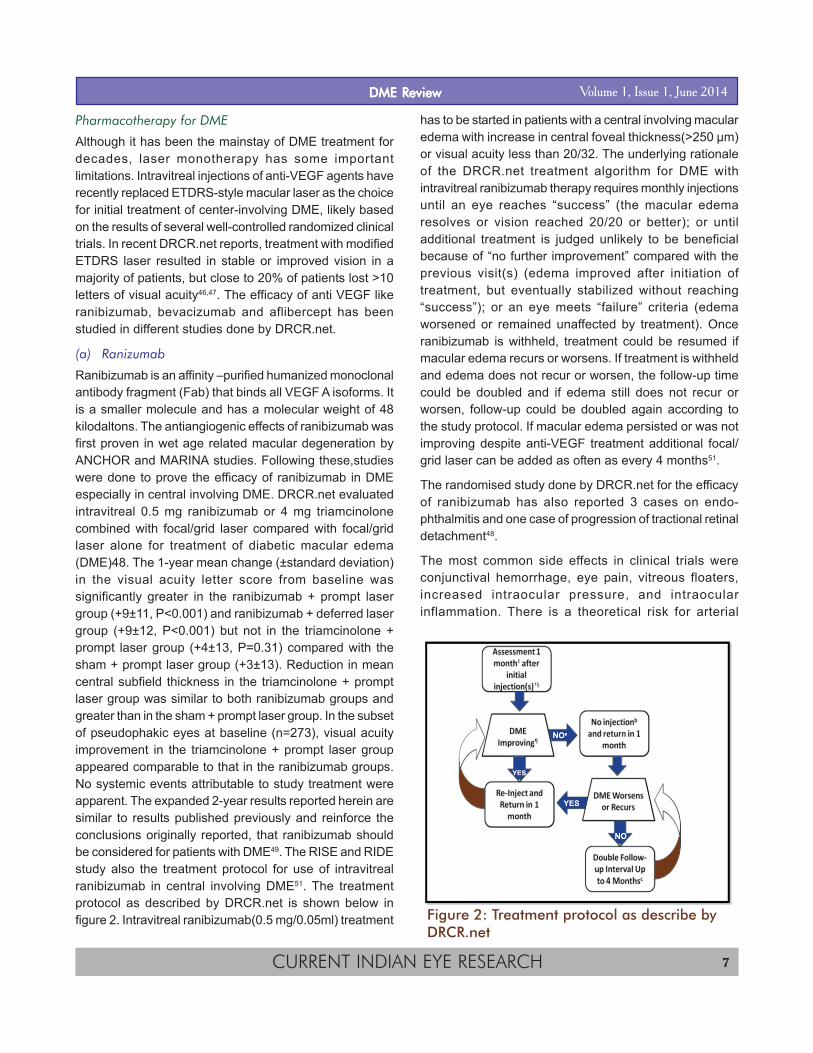
Ranibizumab is an affinity –purified humanized monoclonalantibody fragment (Fab) that binds all VEGF A isoforms. Itis a smaller molecule and has a molecular weight of 48kilodaltons. The antiangiogenic effects of ranibizumab wasfirst proven in wet age related macular degeneration byANCHOR and MARINA studies. Following these,studieswere done to prove the efficacy of ranibizumab in DMEespecially in central involving DME. DRCR.net evaluatedintravitreal 0.5 mg ranibizumab or 4 mg triamcinolonecombined with focal/grid laser compared with focal/gridlaser alone for treatment of diabetic macular edema(DME)48. The 1-year mean change (±standard deviation)in the visual acuity letter score from baseline wassignificantly greater in the ranibizumab + prompt lasergroup (+9±11, P<0.001) and ranibizumab + deferred lasergroup (+9±12, P<0.001) but not in the triamcinolone +prompt laser group (+4±13, P=0.31) compared with thesham + prompt laser group (+3±13). Reduction in meancentral subfield thickness in the triamcinolone + promptlaser group was similar to both ranibizumab groups andgreater than in the sham + prompt laser group. In the subsetof pseudophakic eyes at baseline (n=273), visual acuityimprovement in the triamcinolone + prompt laser groupappeared comparable to that in the ranibizumab groups.No systemic events attributable to study treatment wereapparent. The expanded 2-year results reported herein aresimilar to results published previously and reinforce theconclusions originally reported, that ranibizumab shouldbe considered for patients with DME49. The RISE and RIDEstudy also the treatment protocol for use of intravitrealranibizumab in central involving DME51. The treatmentprotocol as described by DRCR.net is shown below infigure 2. Intravitreal ranibizumab(0.5 mg/0.05ml) treatment
has to be started in patients with a central involving macularedema with increase in central foveal thickness(>250 µm)or visual acuity less than 20/32. The underlying rationaleof the DRCR.net treatment algorithm for DME withintravitreal ranibizumab therapy requires monthly injectionsuntil an eye reaches “success” (the macular edemaresolves or vision reached 20/20 or better); or untiladditional treatment is judged unlikely to be beneficialbecause of “no further improvement” compared with theprevious visit(s) (edema improved after initiation oftreatment, but eventually stabilized without reaching“success”); or an eye meets “failure” criteria (edemaworsened or remained unaffected by treatment). Onceranibizumab is withheld, treatment could be resumed ifmacular edema recurs or worsens. If treatment is withheldand edema does not recur or worsen, the follow-up timecould be doubled and if edema still does not recur orworsen, follow-up could be doubled again according tothe study protocol. If macular edema persisted or was notimproving despite anti-VEGF treatment additional focal/grid laser can be added as often as every 4 months51.
The randomised study done by DRCR.net for the efficacyof ranibizumab has also reported 3 cases on endo-phthalmitis and one case of progression of tractional retinaldetachment48.
The most common side effects in clinical trials wereconjunctival hemorrhage, eye pain, vitreous floaters,increased intraocular pressure, and intraocularinflammation. There is a theoretical risk for arterial
Figure 2: Treatment protocol as describe byDRCR.net
DME ReviewDME ReviewDME ReviewDME ReviewDME Review Volume 1, Issue 1, June 2014

CURRENT INDIAN EYE RESEARCH8
thromboembolic events in patients receiving VEGF-inhibitors by intravitreal injection.
(b) Bevacizumab
Bevacizumab is a full length humanised monoclonalantibody that binds all VEGF-A isoforms and is FDAapproved for colorectal carcinoma, but is used off label inthe eye. Compared to ranibizumab it is a larger moleculeand has a molecular weight of 149 kilodalton. A phase 2trial done by DRCR.net to provide data on the short-termeffect of intravitreal bevacizumab for diabetic macularedema (DME)52. The results demonstrate that intravitrealbevacizumab can reduce DME in some eyes, but the studywas not designed to determine whether treatment isbeneficial. A phase 3 trial would be needed for that purpose.The BOLT study demonstrates that at 12 months of followup the patients treated with intravitreal bevacizumab hasa significantly better mean change in visual acuity than inthe laser group53.
The adverse affects are similar to ranibizumab althoughas per CATT trial some nonfatal adverse effects like GIbleeding were more in cases of bevacizumab54.
(c) Aflibercept
Vascular Endothelial Growth Factor Trap-Eye is a 115-kDArecombinant fusion protein comprising the key VEGFbinding domains of human VEGF receptors 1 and 2 fusedto the Fc domain of human immunoglobulin G155. VascularEndothelial Growth Factor Trap-Eye is a panisoform VEGF-A inhibitor whose binding affinity to VEGF is substantiallygreater than that of either bevacizumab or ranibizumab55,leading to a mathematical model predicting it could havesubstantially longer duration of action in the eye56. Inaddition, VEGF Trap-Eye binds placental growth factors 1and 2, which have been shown to contribute to excessivevascular permeability and retinal neo-vascularization57.
The DA VINCI trial was done to show the efficacy, dosingand dosing schedule of aflibercept in DME58. In this phase2 clinical trial, all VEGF Trap-Eye doses and dosingregimens were found to be superior to macular laserphotocoagulation for the treatment of DME over the courseof 52 weeks and produced similar results in terms ofpreserving and improving visual acuity. Patients whoreceived VEGF Trap-Eye benefited from significantlygreater increases in mean visual acuity at 1 year (9.7 to13.1 letters of improvement) compared with laser treatmentalone (1.3 letters change). The average number of lasertreatments administered to eyes randomized to VEGF Trap-
Eye was fewer than 1 (of a maximum of 2 possible lasers),with most patients not requiring laser photocoagulation,indicating that the visual acuity and anatomic benefitsachieved were the result of VEGF Trap-Eye and not lasertreatment. The 2 mg dose of VEGF Trap-Eye almostcompletely eliminated vision loss at all dosing intervals. Aprolongation of the retreatment interval from 4 to 8 weeksbased on this data and the rationale of the improved bindingproperties of VEGF Trap-Eye represents an opportunity topotentially reduce the treatment and monitoring burden inanti-angiogenic therapy for DME59.
(d) Combination therapy
As proven by the studies done by DRCR.net monotherapywith corticosteroids does not have much advantage overfocal laser alone, several recent trials have provided goodevidence to support combined treatment modalities for thetreatment of DME. The RESTORE study was done tocompare injection ranibizumab with laser treatment vsranibizumab injection with sham laser vs laser alone60.Although the visual gain and the improvement of macularthickness was more in both the ranibizumab groups thanthe only laser group, it failed to show an outright advantageof combination therapy over ranibizumab monotherapy. TheREAD 2 study also had similar results like RESTORE61. At2 years although both monotherapy and combinationtherapy with laser showed similar visual outcomes, thecombination group required fewer treatments. Entry criteriafor READ 2 were similar to the RESTORE study, but theREAD 2 investigators chose to give injections every twomonths in the ranibizumab group. Importantly, in thecombination group, patients received focal laser a weekafter injection, which differs from the RESTORE trial, whichapplied combined treatment on the same day. TheDRCR.net's Protocol I study also investigated combinationtherapy involving ranibizumab or triamcinolone with focallaser62. By three years, VA scores had improved more inthe ranibizumab plus deferred laser group compared toprompt laser (9.7 letters vs 6.8 letters)63.
(e) Intravitreal steroids
Corticosteroids have immune modulatory andantiangogenic properties and have been utilised for themanagement of DME. The major side effects of usingintravitreal steroids are IOP rise and cataract formation.DRCR.net evaluated the efficacy and safety of 1 mg and 4mg doses of preservative-free intravitreal triamcinolone incomparison with focal/grid photocoagulation for thetreatment of diabetic macular edema (DME)64. At 4 months,
DME ReviewDME ReviewDME ReviewDME ReviewDME ReviewVolume 1, Issue 1, June 2014

CURRENT INDIAN EYE RESEARCH 9
a greater positive treatment response on visual acuity wasseen in the 4 mg triamcinolone group compared with theother two groups. However, by 1 year, there was littledifference in visual acuity between the groups, and at thetime of the two-year primary outcome assessment, visualacuity and safety (with respect to intraocular pressure andcataract) were significantly better in the laser group thanin either the 4 mg triamcinolone or 1 mg triamcinolonegroups. There was no significant difference between the 1mg triamcinolone and 4 mg triamcinolone groups in visualacuity at 2 years. Treatment group differences in thechange in retinal thickening generally mirrored the effecton visual acuity, with initially a greater reduction in the 4mg triam-cinolone group, an eventual greater reduction inthe laser group, and no difference between the twotriamcinolone groups at 2 years. Results in a subset ofrandomized subjects who completed the 3-year follow-upare consistent with previously published 2-year results anddo not indicate a long-term benefit of intravitrealtriamcinolone relative to focal/grid photocoagulation inpatients with diabetic macular edema similar to thosestudied in this clinical trial65. Thus 1st line intravitreal triam-cilonone is not recommended.
(f) Posterior subtenon triamcinolone:
DRCR.net also provided the pilot data on the safety andefficacy of anterior and posterior subtenon injections oftriamcinolone either alone or in combination with focalphotocoagulation in the treatment of mild diabetic macularedema (DME)66. No clinically important effects on centralretinal thickness or visual acuity were found with peribulbarinjections of triamcinolone with or without follow-up focalphotocoagulation in comparison with focal photo-coagulation alone.
(g) Sustained release implants
Steroids offer the potential advantage of longer durationof action. Rather than repeated bolus delivery of steroid,sustained-delivery devices have undergone developmentand testing for treatment of macular edema.
In the FAME trial, investigators used fluocinolone acetonidevitreous inserts (Iluvien, Alimera Sciences, Alpharetta, GA)to treat subjects with center-involving DME who had failedat least one prior macular laser67. The investigatorscompared two doses of steroid (0.2 and 0.5 µg/day) tosham injections. Both treatment groups showed largergains in VA compared to the sham group, with 4.4 and 5.4letters gained at two years in the low and high-dose groups,respectively, compared to a gain of 1.7 letters in the
controls. The differences were more pronounced in favorof the steroid group in patients with chronic DME of morethan three years' duration. Cataract progression wassignificant among steroid-treated patients.
The CHAMPLAIN and PLACID study demonstrates theefficacy of dexamethasone implant in refractory diabeticmacular edema. In the CHAMPLAIN study, theinvestigators administered a single dexa-methasoneinjectable implant (Ozurdex, Allergan, Irvine, CA) in a cohortof patients with refractory DME and prior vitrectomy68. ThePLACID study randomized eyes with central diffuse DMEto treatment with dexamethasone implant combined withmacular laser or to sham injection with macular laser69.
Poor responders and treatment failure
Definite worsening or treatment failure is defined aspersistent edema along with 10 or more letter worseningfrom baseline at any visit, or, after at least 1 year oftreatment, there was no improvement from baseline incentral subfield thickness or visual acuity in the setting of“complete” laser. “Complete” laser was defined as directtreatment to all micro-aneurysms within areas of macularedema and grid treatment already applied to all other areasof macular edema. Once “failure” criteria were met, anti-VEGF treatment could be discontinued and any alternativetreatment (such as intravitreal corticosteroids) along withfocal laser could be performed51.
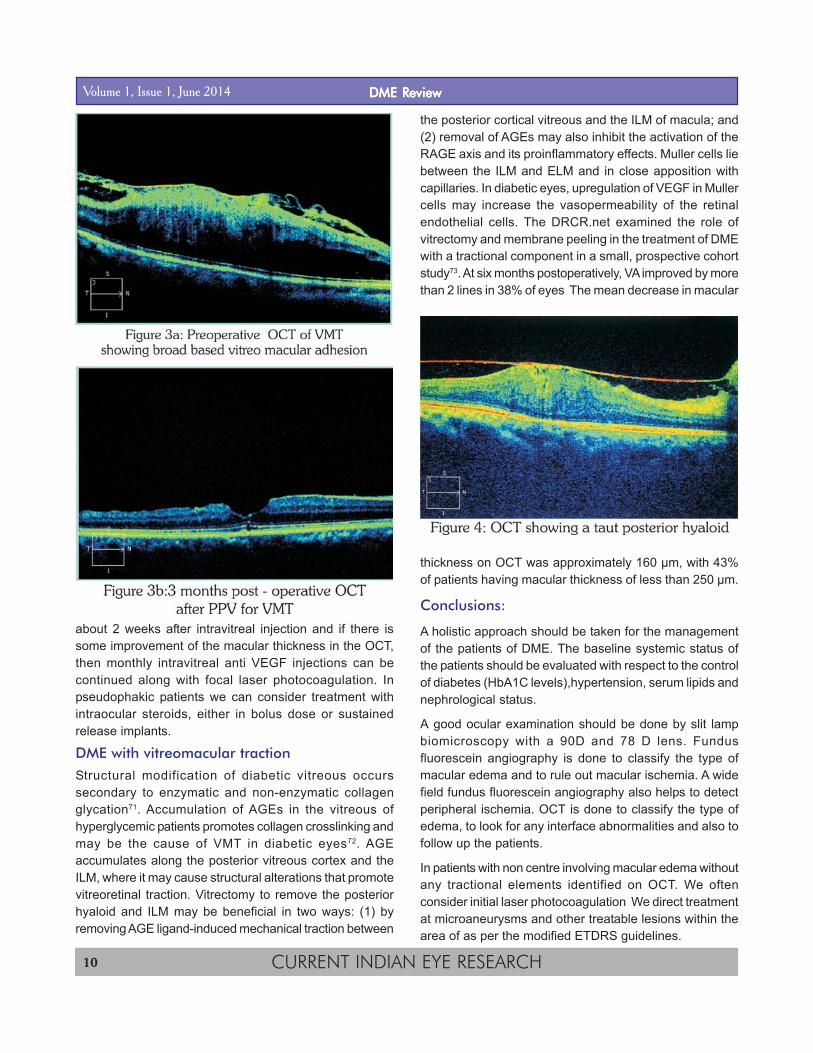
In cases of treatment failure we obtain wide fieldangiography to assess peripheral and macularnonperfusion. Based on anecdotal evidence of peripheralischemia driving persistent DME, we consider targeted PRPto areas of nonperfusion to reduce the ischemic burden.In those cases that remain refractory to treatment, the nextstep in the therapeutic algorithm is PPV with ILM removal.In eyes with, significant ERM, or vitreous adhesion andVMT (figure-3a), refractory edema and taut hyaloid (figure-4), we often consider vitrectomy with peeling early in thecourse of treatment with adequate intravitrealpharmacotherapy in the perioperative period (Fig 3b). Studydone by A. Kumar et al showed PPV with ILM peeling wasbeneficial by inducing a statistically significant reductionof macular thickness and macular volume. Visual acuityalso demonstrated a trend towards improvement in boththe ILM peel group and the grid laser group; however, thecomparative VA outcome analysis between the two groupswas not significantly different70.
For poorly responsive patients, they should be evaluated
DME ReviewDME ReviewDME ReviewDME ReviewDME Review Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH10
about 2 weeks after intravitreal injection and if there issome improvement of the macular thickness in the OCT,then monthly intravitreal anti VEGF injections can becontinued along with focal laser photocoagulation. Inpseudophakic patients we can consider treatment withintraocular steroids, either in bolus dose or sustainedrelease implants.
DME with vitreomacular tractionStructural modification of diabetic vitreous occurssecondary to enzymatic and non-enzymatic collagenglycation71. Accumulation of AGEs in the vitreous ofhyperglycemic patients promotes collagen crosslinking andmay be the cause of VMT in diabetic eyes72. AGEaccumulates along the posterior vitreous cortex and theILM, where it may cause structural alterations that promotevitreoretinal traction. Vitrectomy to remove the posteriorhyaloid and ILM may be beneficial in two ways: (1) byremoving AGE ligand-induced mechanical traction between
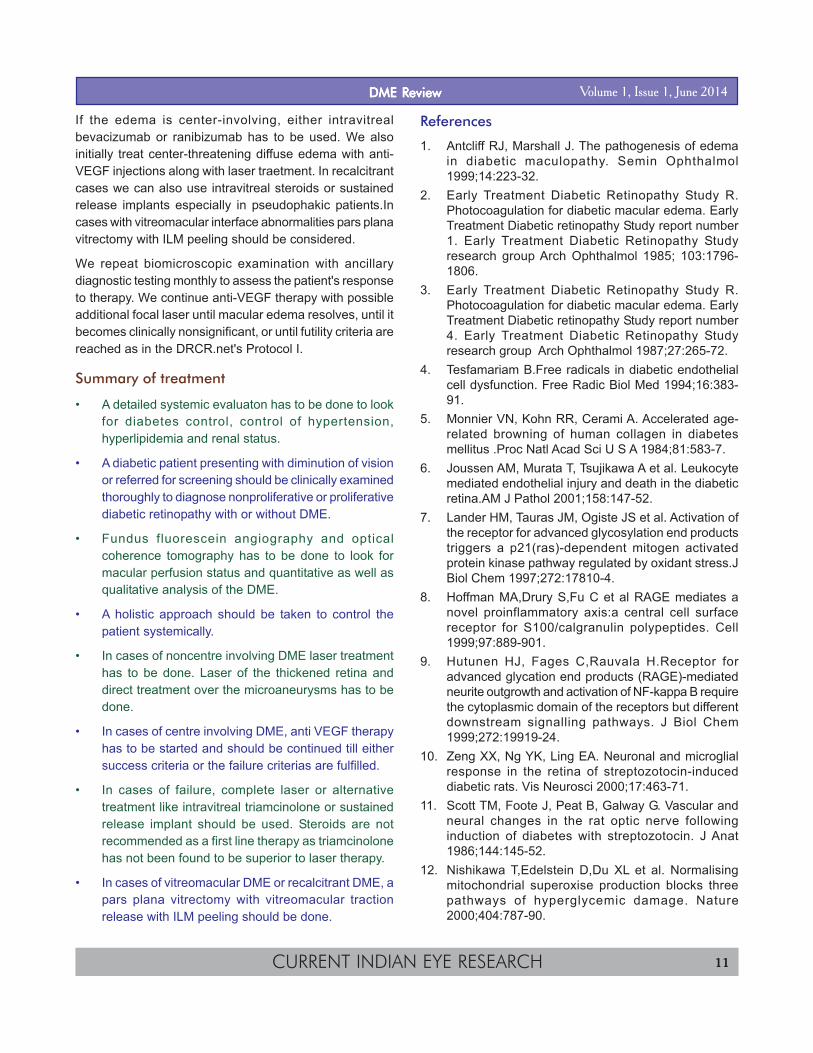
the posterior cortical vitreous and the ILM of macula; and(2) removal of AGEs may also inhibit the activation of theRAGE axis and its proinflammatory effects. Muller cells liebetween the ILM and ELM and in close apposition withcapillaries. In diabetic eyes, upregulation of VEGF in Mullercells may increase the vasopermeability of the retinalendothelial cells. The DRCR.net examined the role ofvitrectomy and membrane peeling in the treatment of DMEwith a tractional component in a small, prospective cohortstudy73. At six months postoperatively, VA improved by morethan 2 lines in 38% of eyes The mean decrease in macular
thickness on OCT was approximately 160 µm, with 43%of patients having macular thickness of less than 250 µm.
Conclusions:
A holistic approach should be taken for the managementof the patients of DME. The baseline systemic status ofthe patients should be evaluated with respect to the controlof diabetes (HbA1C levels),hypertension, serum lipids andnephrological status.
A good ocular examination should be done by slit lampbiomicroscopy with a 90D and 78 D lens. Fundusfluorescein angiography is done to classify the type ofmacular edema and to rule out macular ischemia. A widefield fundus fluorescein angiography also helps to detectperipheral ischemia. OCT is done to classify the type ofedema, to look for any interface abnormalities and also tofollow up the patients.
In patients with non centre involving macular edema withoutany tractional elements identified on OCT. We oftenconsider initial laser photocoagulation We direct treatmentat microaneurysms and other treatable lesions within thearea of as per the modified ETDRS guidelines.
DME ReviewDME ReviewDME ReviewDME ReviewDME ReviewVolume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH 11
If the edema is center-involving, either intravitrealbevacizumab or ranibizumab has to be used. We alsoinitially treat center-threatening diffuse edema with anti-VEGF injections along with laser traetment. In recalcitrantcases we can also use intravitreal steroids or sustainedrelease implants especially in pseudophakic patients.Incases with vitreomacular interface abnormalities pars planavitrectomy with ILM peeling should be considered.
We repeat biomicroscopic examination with ancillarydiagnostic testing monthly to assess the patient's responseto therapy. We continue anti-VEGF therapy with possibleadditional focal laser until macular edema resolves, until itbecomes clinically nonsignificant, or until futility criteria arereached as in the DRCR.net's Protocol I.
Summary of treatment
• A detailed systemic evaluaton has to be done to lookfor diabetes control, control of hypertension,hyperlipidemia and renal status.
• A diabetic patient presenting with diminution of visionor referred for screening should be clinically examinedthoroughly to diagnose nonproliferative or proliferativediabetic retinopathy with or without DME.
• Fundus fluorescein angiography and opticalcoherence tomography has to be done to look formacular perfusion status and quantitative as well asqualitative analysis of the DME.
• A holistic approach should be taken to control thepatient systemically.
• In cases of noncentre involving DME laser treatmenthas to be done. Laser of the thickened retina anddirect treatment over the microaneurysms has to bedone.
• In cases of centre involving DME, anti VEGF therapyhas to be started and should be continued till eithersuccess criteria or the failure criterias are fulfilled.
• In cases of failure, complete laser or alternativetreatment like intravitreal triamcinolone or sustainedrelease implant should be used. Steroids are notrecommended as a first line therapy as triamcinolonehas not been found to be superior to laser therapy.
• In cases of vitreomacular DME or recalcitrant DME, apars plana vitrectomy with vitreomacular tractionrelease with ILM peeling should be done.
References
1. Antcliff RJ, Marshall J. The pathogenesis of edemain diabetic maculopathy. Semin Ophthalmol1999;14:223-32.
2. Early Treatment Diabetic Retinopathy Study R.Photocoagulation for diabetic macular edema. EarlyTreatment Diabetic retinopathy Study report number1. Early Treatment Diabetic Retinopathy Studyresearch group Arch Ophthalmol 1985; 103:1796-1806.
3. Early Treatment Diabetic Retinopathy Study R.Photocoagulation for diabetic macular edema. EarlyTreatment Diabetic retinopathy Study report number4. Early Treatment Diabetic Retinopathy Studyresearch group Arch Ophthalmol 1987;27:265-72.
4. Tesfamariam B.Free radicals in diabetic endothelialcell dysfunction. Free Radic Biol Med 1994;16:383-91.
5. Monnier VN, Kohn RR, Cerami A. Accelerated age-related browning of human collagen in diabetesmellitus .Proc Natl Acad Sci U S A 1984;81:583-7.
6. Joussen AM, Murata T, Tsujikawa A et al. Leukocytemediated endothelial injury and death in the diabeticretina.AM J Pathol 2001;158:147-52.
7. Lander HM, Tauras JM, Ogiste JS et al. Activation ofthe receptor for advanced glycosylation end productstriggers a p21(ras)-dependent mitogen activatedprotein kinase pathway regulated by oxidant stress.JBiol Chem 1997;272:17810-4.
8. Hoffman MA,Drury S,Fu C et al RAGE mediates anovel proinflammatory axis:a central cell surfacereceptor for S100/calgranulin polypeptides. Cell1999;97:889-901.
9. Hutunen HJ, Fages C,Rauvala H.Receptor foradvanced glycation end products (RAGE)-mediatedneurite outgrowth and activation of NF-kappa B requirethe cytoplasmic domain of the receptors but differentdownstream signalling pathways. J Biol Chem1999;272:19919-24.
10. Zeng XX, Ng YK, Ling EA. Neuronal and microglialresponse in the retina of streptozotocin-induceddiabetic rats. Vis Neurosci 2000;17:463-71.
11. Scott TM, Foote J, Peat B, Galway G. Vascular andneural changes in the rat optic nerve followinginduction of diabetes with streptozotocin. J Anat1986;144:145-52.
12. Nishikawa T,Edelstein D,Du XL et al. Normalisingmitochondrial superoxise production blocks threepathways of hyperglycemic damage. Nature2000;404:787-90.
DME ReviewDME ReviewDME ReviewDME ReviewDME Review Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH12
13. Giugliano G, Ceriello A,Paolisso G. Oxidative stressand diabetic vascular complications. Diabetes Care1996;19:257-67.
14. Nagpala PG, Malik AB, Vuong PT, Lum H. Proteinkinase C beta 1 overexpression augments phorbolester-induced increase in endothelial permeability. JCell Physiol 1996;166:249—55.
15. Aiello LP, Bursell S-E, Clermont A, et al. Vascularendothelial growth factor-induced retinal permeabilityis mediated by protein kinase C in vivo andsuppressed by an orally effective beta isoformselective inhibitor. Diabetes1997;46:1473-80.
16. Kumagai AK, Glasgow BJ, Pardridge WM. GLUT 1glucose transpoeter expression in the diabetic andnondiabetic human eye.Invest Ophthalmol Vis Sci1994;35:2887-94.
17. Mantych GJ, Hageman GS, Devaskar SU.Characterization of glucose transporter isoforms inthe adult and developing human eye. Endocrinology1993;133:600-7.
18. Olsson AK, Dimberg A, Kreuger J, Claesson-WelshL. VEGF receptor signalling-in control of vascularfunction. Nat Rev Mol Cell Biol 2006;7:359-71.
19. Collins PD, Connolly DT, Williams TJ. Characterizationof the increase in vascular permeability induced byvascular permeability factor in vivo. Br J Pharmacol1993; 109:195-9.
20. Murata T, Ishibashi T, Khalil A, et al. Vascularendothelial growth factor plays a role inhyperpermiability of diabetic retinal vessels.Ophthalmic Res 1995;27:48-52.
21. Funatsu H, Yamashita H, Ikeda T, et al. Angiotensin IIand vascular endothelial growth factor in the vitreousfluid of patients with diabetic macular edema and otherretinal disorders. Am J Ophthalmol 2002; 133:537-43.
22. Jin M, Kashiwagi K, Iizuka Y, et al. Matrixmetalloproteinases in human diabetic and nondiabeticvitreous. Retina 2001;21:28-31.
23. Ogata N, Tombran-Tink J, Nishikawa M, et al. Pigmentepithelium-derived factor in the vitreous is low indiabetic retinopathy and high in rhegmatogenousretinal detachment. Am J Ophthalmol 2001;132:378-82.
24. Yamagishi S, Nakamura K, Takenaka K, et al. Pigmentepithelium-derived factor (PEDF) promotes growth ofpericytes through autocrine production of platelet-derived growth factor-B. Microvasc Res 2005;69:128-34.
25. Montesano R, Vassalli JD, Baird A, et al. Basicfibroblast growth factor induces angiogenesis in vitro.Proc Natl Acad Sci USA. 1986;83:7297-301.
26. Shepro D, Morel NM, Pericyte physiology. FASEB J1993;7:1031-8.
27. Aiello LP,Cavallerano J,Bursell SE.Diabetic eyedisease. Endocrinol Metab Clin North Am1996;25:271-91.
28. Robison Jr WG,Kador PF,Kinoshita JH.Retinalcapillaries:basement membrane thickening bygalactosemia prevented with aldose reductaseinhibitor .Science 1983;221:1177-9.
29. Robison Jr WG,Kador PF,Akagi Y, et al. Prevention ofbasement membrane thickening in retinal caoillariesby a novel aldose reductase inhibitors, tolrestat.Diabetes 1986;35:295-9.
30. Brownlee M,Cerami A.The biochemistry of thecomplications of diabetes mellitus.Annu rev Biochem1981;50:385-432.
31. Daneman D, Drash A,Lobes LA,et al. Progressiveretinopathy with improved control in diabeticdwarfism(Maurian's syndrome).Diabetes Care1981;4:360-5.
32. Jeppsen P,Aalkjaer C,Bek T.Bradykinin relaxation insmall porcine retinal arterioles.Invest Ophthalmol VisSci 2002;43: 1891-6.
33. Harbour JW, Smiddy WE, Flynn HWJ, RubsamenPE.Vitrectomy for diabetic macular edema associatedwith a thickened and taut posterior hyaloid membrane.Am J Ophthalmol 1996;121:405-13.
34. Lewis H, Abrams GW, Blumenkranz MS, CampoRV.Vitrectomy for diabetic macular traction and edemaassociated with posterior hyaloidal traction.Ophthalmology1992; 99:753-9.
35. Bresnik GH. Diabetic macular edema: a review.Ophthalmology 1986;93:989-97.
36. Bresnik GH. Diabetic maculopathy; a critical reviewhighlighting diffuse macular edema. Ophthalmology1983;90:1301-17.
37. Kang SW, Park CY, Ham DI. The correlation betweenfluorescein angiographic and optical coherencetomographic features in clinically significant diabeticmacular edema. Am J Ophthalmol 2004; 137:313-22.
38. Chan A, Duker JS. A standartized method for reportingchanges in macular thickening using opticalcoherence tomography. Arch ophthalmol2005;123:939-43.
39. Diabetes Control and Complications Trial ResearchGroup. The effect of intensive treatment of diabeteson the development and progression of long-termcomplications in insulin-dependent diabetes mellitus.N Engl J Med 1993;329:977-86.
DME ReviewDME ReviewDME ReviewDME ReviewDME ReviewVolume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH 13
40. UK Prospective Diabetes Study Group. Intensiveblood glucose control with sulphonylureas or insulincompared with conventional treatment and risk ofcomplications in patients with type 2 diabetes: UKPDS33. Lancet 1998;352:837-53.
41. UK Prospective Diabetes Study Group. Tight bloodpressure control and risk of macrovascular andmicrovascular complications in type 2 diabetes:UKPDS 38. Br Med J 1998;317:703-13.
42. Keech AC, Mitchell P, Summanen PA, et al. Effect offeno?brate on the need for laser treatment for diabeticretinopathy (FIELD study): a randomised controlledtrial. Lancet 2007;370:1687-97.
43. Scheen AJ, Van Gaal LF. Clinical study of the month.Accord lipid and accord-eye: towards a newpositioning of fenofibrate in the management of type2 diabetes. Rev Med Liege 2010;65:533-9.
44. Fong DS, Strauber SF, Aiello LP, Beck RW, CallananDG, Danis RP, Davis MD, Feman SS, Ferris F,Friedman SM, Garcia CA, Glassman AR, Han DP, LeD, Kollman C, Lauer AK, Recchia FM, Solomon SD.Comparison of the modified Early Treatment DiabeticRetinopathy Study and mild macular grid laserphotocoagulation strategies for diabetic macularedema. Arch Ophthalmol 2007 ;125:469-80.
45. Scott IU, Danis RP, Bressler SB, Bressler NM,Browning DJ, Qin H; Diabetic Retinopathy ClinicalResearch Network. Effect of focal/gridphotocoagulation on visual acuity and retinalthickening in eyes with non-center-involved diabeticmacular edema. Retina 2009;29:613-7.
46. Aiello LP, Edwards AR, Beck RW, et al; DiabeticRetinopathy Clinical Research Network. Factorsassociated with improvement and worsening of visualacuity 2 years after focal/grid photocoagulation fordiabetic macular edema. Ophthalmology 2010;117:946-53.
47. Fong DS, Strauber SF, Aiello LP, et al. Comparison ofthe modified Early Treatment Diabetic RetinopathyStudy and mild macular grid laser photocoagulationstrategies for diabetic macular edema. ArchOphthalmol 2007; 125: 469-80.
48. Diabetic Retinopathy Clinical Research Network.Randomized trial evaluating ranibizumab plus promptor deferred laser or triamcinolone plus prompt laserfor diabetic macular edema. Ophthalmology2010;117:1064-77.e35.
49. Diabetic Retinopathy Clinical Research Network.Expanded 2-year Follow-up of Ranibizumab PlusPrompt or Deferred Laser or Triamcinolone PlusPrompt Laser for Diabetic Macular Edema.Ophthalmology 2011; 118: 609-14.
50. Brown DM, Nguyen QD, Marcus DM, et al. Long-termoutcomes of ranibizumab therapy for diabetic macularedema: the 36-month results from two phase III trials:RISE and RIDE. Ophthalmology 2013 ; 120:2013-22.
51. The Diabetic Retinopathy Clinical Research Network.Rationale for the Diabetic Retinopathy ClinicalResearch Network Intravitreal Anti-VEGF Treatmentand Follow-up Protocol for Center-involved DiabeticMacular Edema. Ophthalmology 2011 ;118:e5-e14.
52. Diabetic Retinopathy Clinical Research Network, ScottIU, Edwards AR, Beck RW, Bressler NM, Chan CK,Elman MJ, Friedman SM, Greven CM, Maturi RK,Pieramici DJ, Shami M, Singerman LJ, Stockdale CR.A phase II randomized clinical trial of intravitrealbevacizumab for diabetic macular edema.Ophthalmology 2007;114:1860-7.
53. Michaelides M, Kaines A, Hamilton RD, et al. Aprospective randomized trial of intravitrealbevacizumab or laser therapy in the management ofdiabetic macular edema (BOLT study) 12-month data:report 2. Ophthalmology 2010;117: 1078-86 e2.
54. Comparison of Age-related Macular DegenerationTreatments Trials (CATT) Research Group, Martin DF,Maguire MG, Fine SL, , et al. Ranibizumab andbevacizumab for treatment of neovascular age-relatedmacular degeneration: two year results. Oph-thalmology 2012;119:1388-98.
55. Holash J, Davis S, Papadopoulos N, et al. VEGF-Trap: a VEGF blocker with potent antitumor effects.Proc Natl Acad SciUSA2002;99:11393–8.
56. Stewart MW, Rosenfeld PJ. Predicted biologicalactivity of intravitreal VEGF Trap. Br J Ophthalmol2008; 92: 667– 8.
57. Rakic JM, Lambert V, Devy L, et al. Placental growthfactor, a member of the VEGF family, contributes tothe development of choroidal neovascularization.Invest Ophthalmol Vis Sci 2003; 44: 3186 –93.
58. Do DV, Schmidt-Erfurth U, Gonzalez VH, et al. TheDA VINCI Study: phase 2 primary results of VEGFTrap-Eye in patients with diabetic macular edema.Ophthalmology 2011; 118: 1819-26.
59. Do DV, Nguyen QD, Boyer D et al. One-year outcomesof the DA VINCI Study of VEGF Trap-Eye in eyes withdiabetic macular edema. Ophthalmology2012;119:1658-65.
60. Mitchell P, Bandello F, Schmidt-Erfurth U, et al. TheRESTORE study: ranibizumab monotherapy orcombined with laser versus laser monotherapy fordiabetic macular edema. Ophthalmology2011; 118:615-25.
61. Nguyen QD, Shah SM, Heier JS, et al. Primary endpoint (six months) results of the Ranibizumab for
DME ReviewDME ReviewDME ReviewDME ReviewDME Review Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH14
Edema of the mAcula in diabetes (READ-2) study.Ophthalmology 2009;116:2175-81 e1.
62. Elman MJ, Aiello LP, Beck RW, et al. Randomizedtrial evaluating ranibizumab plus prompt or deferredlaser or triamcinolone plus prompt laser for diabeticmacular edema. Ophthalmology 2010; 117: 1064-77,e35.
63. Elman MJ, Qin H, Aiello LP, et al. Intravitrealranibizumab for diabetic macular edema with promptversus deferred laser treatment: three-yearrandomized trial results. Ophthalmology 2012; 119:2312-18.
64. Diabetic Retinopathy Clinical Reasearch Network. Arandomised trial comparing intravitreal triamcinoloneacetonide and focal/grid photocoagulation for diabeticmacular edema. Ophthalmology 2008;115:1447-9,9e1-10.
65. Beck RW, Edwards AR, Aiello LP, et al. Three yearfollow up of a randomised trial comparing focal/gridphotocoagulation and intravitreal triamcinolone fordiabetic macular edema.Arch Ophthalmol2009;127:245-51.
66. Diabetic Retinopathy Clinical Research Network, ChewE, Strauber S, Beck R et al. Randomized trial ofperibulbar triamcinolone acetonide with and withoutfocal photocoagulation for mild diabetic macular edema:a pilot study. Ophthalmology 2007;114:1190-6.
67. Campochiaro PA, Brown DM, Pearson A, et al. Long-term benefit of sustained-delivery fluocinolone
acetonide vitreous inserts for diabetic macular edema.Ophthalmology 2011;118: 626-635 e2.
68. Boyer DS, Faber D, Gupta S, et al. OzurdexCHAMPLAIN Study Group. Dexamethasoneintravitreal implant for treatment of diabetic macularedema in vitrectomized patients. Retina 2011;31: 915-23.
69. Callanan DG, Gupta S, Boyer DS, et al; OzurdexPLACID Study Group. Dexamethasone intravitrealimplant in combination with laser photocoagulationfor the treatment of diffuse diabetic macular edema.Ophthalmology 2013 ; 120:1843-51.
70. Kumar A, Sinha S, Azad R, Sharma YR, Vohra R.Comparative evaluation of vitrectomy and dye-enhanced ILM peel with grid laser in diffuse diabeticmacular edema. Graefes Arch Clin Exp Ophthalmol2007 ;245:360-8.
71. Sebag J, Nie S, Reiser K, et al. Raman spectroscopyof human vitreous in proliferative diabetic retinopathy.Invest Ophthalmol Vis Sci1994;35:2976-80.
72. Barile GR, Pachydaki SI, Tari SR, et al. The RAGEaxis in early diabetic retinopathy. Invest OphthalmolVis Sci 2005;46:2916-24.
73. Haller JA, Qin H, Apte RS, et al. Vitrectomy outcomesin eyes with diabetic macular edema andvitreomacular traction. Ophthalmology 2010;117:1087-93e3.
DME ReviewDME ReviewDME ReviewDME ReviewDME ReviewVolume 1, Issue 1, June 2014

CURRENT INDIAN EYE RESEARCH 15
ANNOUNCEMENT
ORG Award 2014
For Young Researchers (PG)
Most of the works by the post-graduate trainees in India end unpublished.
In order to create an environment where the post-graduate trainees (MS/ MD/ DNB)would try to showcase their hard work in a proper peer-reviewed scientific forum, ascientific paper writing competition is announced.
8 articles (two fr8 articles (two fr8 articles (two fr8 articles (two fr8 articles (two from each grom each grom each grom each grom each group) will be selectedoup) will be selectedoup) will be selectedoup) will be selectedoup) will be selected
First Prize: A citation/certificate and a cash prize of Rs. 50,000/
Second Prize: A citation/certificate and a cash prize of Rs. 20,000/-.
The award-winning articles will be published free after peer review in CurCurCurCurCurrrrrrent Indianent Indianent Indianent Indianent IndianEye ResearEye ResearEye ResearEye ResearEye Research, ch, ch, ch, ch, a peer reviewed open access journal.
Group A: Cornea, Refractive surgery, Ocular surface.
Group B: Retina-vitreous, Uvea.
Group C: Cataract, Glaucoma
Group D: Pediatric ophthalmology, Orbit, Lacrimal apparatus, Oculoplasty.
The last date for submission of the articles is 31st of October, 2014.
The panel of judges will consist of eminent post-graduate teachers from different teachinginstitutions and their decision regarding the awards will be final.
Eligibility: Post-graduate trainees in Ophthalmology (present trainees and also who havepassed out in the last two years)
Article type: Unpublished original article
Word limit: 250 words structured abstract, 3-5 key words, Maximum 3000 words(excluding maximum 50 references), maximum three tables/figures (b/w).
For further details please visit www.ophthalmicresearch.in
Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH16
Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH 17
Xeno-Free Autologous Cultivated Oral Mucosal EpithelialTransplantation for Bilateral Ocular Surface Burns: Clinical Outcomesand Immunohistochemical AnalysisSubhash Gaddipati1, Sayan Basu1,2, Geeta K Vemuganti1, Muralidhar Ramappa2, Savitri Maddileti1,Virender S Sangwan1,2
1 Sudhakar and Sreekanth Ravi Stem Cell Biology Laboratory, 2 Cornea and Anterior Segment Services, L V Prasad Eye Institute,Hyderabad, India.Corresponding Author : Dr. Virender S Sangwan, E-mail:[email protected] on : 28/06/2014, Accepted on : 11/07/2014Funded by the Department of Biotechnology, New Delhi, India; Champalimaud Foundation, Lisbon; Portugal, and the Hyderabad Eye ResearchFoundation, Hyderabad, India. None of these had any role in the design, collection, analysis and interpretation of the data.Conflict of Interest : None, Financial Disclosure : None
Abstract
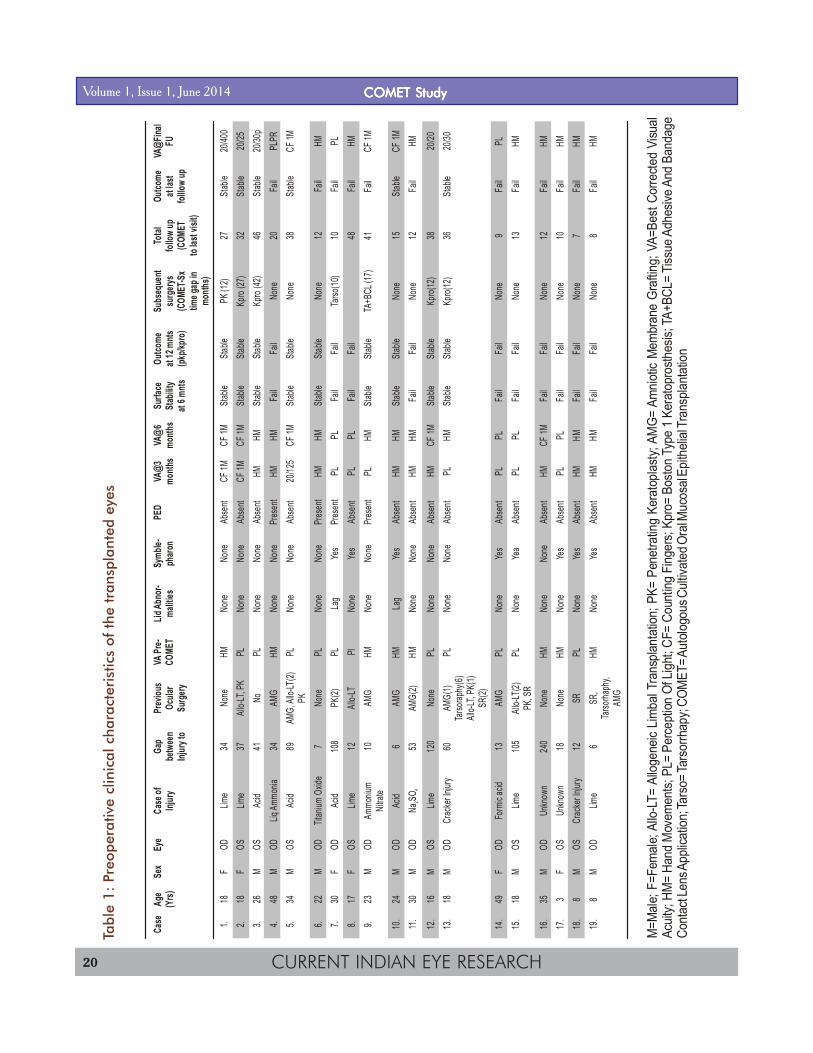
Purpose: To report the clinical and phenotypic findings following autologous cultivated oral mucosal epithelial transplantation ineyes with ocular surface burns in a retrospective case series. Methods: This study included 19 eyes of 18 patients with bilaterallimbal stem cell deficiency following ocular burns treated between 2007 and 2010. All patients underwent an oral mucosalbiopsy, following which the oral epithelium was cultivated on de-epithelized human amniotic membrane using a xeno-free explantculture technique. A monolayer of cultivated oral epithelium was transplanted onto the patient's ocular surface. Post-operativeocular surface stability, corneal avascularity and visual improvement were assessed. From five eyes that subsequently underwentkeratoplasty or keratoprosthesis surgery, the excised corneal tissue was subjected to histopathology and immunohistochemicalanalysis. Results: The mean follow-up was 22.3 months. All transplanted eyes showed superficial corneal vascularization by 3months. A stable ocular surface was seen in 7 (37%) eyes at the end of one year. Vision did not improve in 12 (63%) eyes, visionimproved from hand motions to counting fingers in 6 (32%) eyes and to 20/125 in one (5%) eye. Histopathology of excisedcorneal tissue showed six to eight layers of epithelial stratification and absence of goblet cells. Immunohistochemical analysis of thetransplanted epithelium showed expression of p75, p63, suprabasal K19 and K3 and absence of K12, K14. Conclusions:Clinical outcomes of autologous cultivated oral mucosal epithelial transplantation in eyes with ocular surface burns were poor andthe transplanted cells maintained the oral phenotype on the corneal surface.
Limbal stem cell deficiency (LSCD) is a rare cause ofcorneal blindness which results from physical,
chemical or immunological damage to the corneal epithelialstem cells located at the limbus1,2. In unilateral cases LSCDcan be treated by either conventional or cultivatedautologous limbal transplantation from the unaffected felloweye3,4. However, in bilateral cases there is no autologoussource for limbal stem cells and either a living or a cadavericallogeneic donor is required5. An alternative to allogeneiclimbal grafting, which necessitates long-term systemicimmuno-suppression, is transplantation of autologousepithelium from non-ocular sources.
The possibility of oral mucosa being used as a substitutefor limbal epithelium was considered because of thephenotypic semblance between the two epithelial
lineages6,7. Animal trials and preliminary human trials alsodemonstrated that the ex-vivo cultivated oral mucosa couldbe a suitable therapeutic alternative to limbal epitheliumin eyes with LSCD8-13. However the cell culture protocolsdescribed for cultivating oral mucosal cells for humantransplantation utilized various animal derived or xeno-biotic materials9-19. Use of xeno-biotic materials in cellculture for clinical use is undesirable as it carries the riskof transmitting known or unknown infections to thetransplant recipient20. To avoid xeno-biotic usage, wedeveloped a xeno-free technique of culturing oral mucosalcells,6 adopted from our standardized protocol for limbalepithelial cultivation21, which has been used successfullyto treat over 500 eyes with unilateral LSCD22-24. In this studywe report the clinical outcomes and immunohistochemicalfindings in eyes with LSCD following ocular surface burns,
Original ArticleOriginal ArticleOriginal ArticleOriginal ArticleOriginal Article

CURRENT INDIAN EYE RESEARCH18
treated by xeno-free autologous cultivated oral mucosalepithelial transplantation (COMET).
Methods:
Patients: At the L V Prasad Eye Institute, Hyderabad, Indiaautologous COMET was offered as an alternative toallogeneic cultivated limbal epithelial trans-plantation,between October 1, 2007 and November 1, 2010, topatients with bilateral and total LSCD (defined clinically as360o superficial corneal vascularization, diffuse fluoresceinstaining of the corneal surface with or without persistentepithelial defects, conjunctivalization of the corneal surfaceand absence of limbal palisades of Vogt) following ocularsurface burns. The Institutional Review Board approvedof this pilot study for 20 eyes (LEC 06003) andrecommended the following exclusion criteria to be appliedbefore enrolment: (a) patients with LSCD due to unknowncauses or causes other than ocular surface burns; (b)patients who had bilateral but partial LSCD; (c) patientswith total LSCD, but with dry eye disease (Schirmer's testwithout anesthesia of <10 mm at 5 minutes) orkeratinisation of the ocular surface epithelium; (d) patientswith no visual potential as determined by clinicalexamination and electrophysiological testing (flash visualevoked potential and flash electroretinogram); (e) patientswith untreated concurrent ocular problems, such asglaucoma and infection.
Data Collection: The data retrieved from the medicalrecords included age and sex of the patient, type and dateof injury, details of prior ocular procedures, Snellen's bestspectacle corrected visual acuity (BCVA) and at eachfollow-up visit, presence or absence of lid abnormalities,dry eye disease, symblepharon, degree of limbalinvolvement, intra-operative surgical details, post-operativecomplications, duration of follow-up and status of ocularsurface at each visit (slit-lamp findings including fluoresceinstaining).
Surgical Technique of Oral Mucosal Biopsy: All patientsunderwent an oral examination by a physician to rule outany contraindications to a mucosal biopsy. The patientswere advised 5% povidone-iodine mouth wash twice dailyfor 3 consecutive days prior to the biopsy. After confirmingsatisfactory oral hygiene, an oral mucosal biopsy of 3 x 3mm was obtained under local anesthesia (2% xylocainesub-mucosal infiltration) from the inner surface of thepatient's lower lip. The biopsied area was left bare and thepatient was advised to continue the mouth wash for one
week following the biopsy. The oral biopsies wereperformed by one surgeon (MR).
Technique of Oral Mucosal Epithelial Cultivation: The tissuewas transported to the laboratory in human cornealepithelium (HCE) medium, which has been describedpreviously.21-24 Briefly, HCE medium composed ofminimal essential Eagle's medium (Sigma, cat. no. M0644)with alpha modification/Nutrient mixture (Sigma, cat. no.I2643), HAM's F12 medium (1:1) containing 2 mM L-glutamine (Sigma, cat. no. G6392), 100 U/mL penicillin,100 µg/mL streptomycin (Sigma, cat. no. P4333), 2.5 µg/mL amphotericin B (Sigma, cat. no. A2942), 10 ng/mLhuman recombinant epidermal growth factor (Sigma, cat.no. E9644) and 5 µg/mL human recombinant insulin(Sigma, cat. no. I2643) along with 10% (vol/vol) autologousserum. Under strict aseptic conditions, human amnioticmembrane (hAM) was prepared and preserved by our eyebank, measuring 3 x 4 cm was de-epithelialised usingTrypLE (Invitrogen, cat. no. 12604) and 0.25% EDTA(Sigma, cat. No. E5134) solution after incubating at 37ºCfor 30 minutes. The patient's oral mucosal tissue wasdivided into small pieces after separation from theunderlying connective and minor salivary glands. Thetissue bits were explanted over the de-epithelized hAM,epithelial side-up. A similar parallel culture was alsoprepared as a backup. A submerged explant culture systemwithout a feeder cell layer was used. The culture wasincubated at 37ºC with 5% CO2 and 95% air in HCE media(Thermo Fisher Scientifc, model: 371). The growth wasmonitored daily under an inverted phase contrastmicroscope (Olympus, CX40) and the HCE medium waschanged every other day. The culture was transplantedwhen a monolayer of the cells growing from the explantsbecame confluent, typically in 15 to 19 days. The laboratorycultures were performed by one experienced cell biologist(SG).
Technique of Cultured Oral Mucosal EpithelialTransplantation: Any symblepharon which preventedadequate separation of the lids was released to permit theinsertion of a wire speculum (no additional surgery to treatthe symblepharon was performed). A peritomy wasperformed and the corneal fibrovascular pannus wasexcised, fixed in 10% formaldehyde solution and sent forhistopathological analysis. The hAM and monolayer ofcultivated oral mucosal epithelial cells was spread overthe cornea, epithelial side up. Using a sutureless techniquethe graft was secured to underlying ocular surface withfibrin glue (TISSEEL™ Kit from Baxter AG, Austria) and
Volume 1, Issue 1, June 2014 COMET StudyCOMET StudyCOMET StudyCOMET StudyCOMET Study

CURRENT INDIAN EYE RESEARCH 19
the margins of the graft were tucked under the surroundingconjunctival edge. Bandage contact lenses were notapplied at the end of surgery. The transplantations wereperformed by the one experienced ocular surface surgeon(VSS).
Postoperative Treatment Regimen: All the recipient eyesreceived topical prednisolone acetate 1% eye drops 8 timesdaily, tapered gradually based on the level of inflammationand ciprofloxacin 0.3% eye drops 4 times daily in the firstpost-operative week or until complete epithelization wasnoted.
Follow-up Schedule: All patients were seen on post-operative day one, at one week, at six weeks, andthereafter every six to eight weeks. Each examinationincluded a complete history, including any new ocular orsystemic symptoms, a complete ocular examinationincluding fluorescein staining, and any signs ofneovascularization or surface instability. The post-operativeclinical assessment was performed by one ocular surfacespecialist (SB).
Primary and Secondary Outcome Measures: Based on theclinical appearance of the corneal surface an impressionof success or failure of therapy was made. Success wasdefined as a totally epithelized, stable and avascularcorneal surface. Failure was defined as appearance of anysuperficial corneal vascularization (even if the cornealsurface was epithelized and stable), epithelial defectslasting more than two weeks and conjunctival overgrowthon the cornea (conjunctivalization). The secondary clinicaloutcomes were improvement in BCVA from baseline andocular and oral complications.
Additional Surgery: Either penetrating keratoplasty (PK)or Boston Type 1 keratoprosthesis was performed in eyeswith a stable ocular surface (irrespective of superficialvascularization) but poor visual improvement attributed tocorneal stromal scarring. The corneal tissue excised duringPK or keratoprosthesis surgery was fixed in 10%formaldehyde and processed for histopathology andimmnuohistochemistry analysis as described below.Hematoxylin-Eosin, Periodic Acid Schiff (PAS) staining: Thepannus excised at the time of COMET, the unused back-up culture and the corneal button excised at the time ofkeratoplasty/ keratoprosthesis were fixed in 10% bufferedformalin, embedded in paraffin and serial sections of 5 µmthickness were taken on silane-coated glass slides.Sections were deparaffinized, rehydrated with distilledwater and stained with hematoxylin and eosin and Schiff'sreagent and observed under light microscope.
Immunohistochemistry: The primary antibodies, anti-K3/12, anti-K14 and anti-K19 were procured from Chemicon,anti-p75 from Abcam, anti-p63 from Thermo Scientific, anti-Ki67 from Dako, while the anti-K19 andimmunohistochemistry (IHC) developing reagents werepurchased from BioGenex. The serial sections of theunused back-up culture and the excised corneal tissuewere de-paraffinized and rehydrated, blocked forendogenous peroxidase using 3% H2O2 in methanol.Antigen retrieval was done using citrate buffer (pH-6.0) ina microwave for 15 minutes and allowed to cool to roomtemperature. Blocking was done using 2.5% bovine serumalbumin in 1x phosphate buffered saline (PBS) beforeprimary antibody incubation at room temperature for onehour. HRP-conjugated secondary antibody incubations andIHC developing was done as per manufacturer'sinstructions (BioGenex). The samples were counterstainedwith hematoxylin, mounted in a resinous mounting mediumand observed under a light microscope. Cadaveric humanconjunctival and corneal tissue obtained from the eye bankand oral mucosal tissue obtained from voluntary humandonors (SG, SB, MR, GKV, VSS) were used as controls.The histopathology and immuno-histochemical analysiswas performed and interpreted by one experienced ocularpathologist (GKV).
Result:
Demographics: During the entire study period 19 eyes of18 patients with bilateral and total LSCD following ocularsurface burns underwent autologous COMET. The meanage at the time of surgery was 23.7± (12.5) years withmale to female ratio of 2.8:1. The median time periodbetween the initial injury and autologous COMET was 34months (range: 6 to 240) months. Other pre-operativeclinical characteristics of the transplanted eyes areprovided in Table 1.Biopsy, Ex-vivo Cultivation and Transplantation: Threepatients underwent biopsy and trans-plantation undergeneral anaesthesia, whereas others were operated underlocal anaesthesias. No anaesthetic or intra-operativecomplications occurred during either biopsy ortransplantation. Following the biopsy no donor sitecomplications were noted. The mucosal defect created onthe lower lip following the oral biopsy completely healedby one week. In the laboratory, a confluent monolayer ofcells formed on the denuded-hAM in a mean duration of19.3 days (range 15 to 27 days). No cultures showedmicrobial contamination or inadequate growth.
Volume 1, Issue 1, June 2014COMET StudyCOMET StudyCOMET StudyCOMET StudyCOMET Study
CURRENT INDIAN EYE RESEARCH20
Tabl
e 1:
Preo
pera
tive
clin
ical
cha
ract
eris
tics
of t
he t
rans
plan
ted
eyes
Case
Age
Sex
Eye
Case
ofGa
pPr
eviou
sVA
Pre-
Lid Ab
nor-
Symb
le-PE
DVA
@3VA
@6
Surfa
ceOu
tcome
Subs
eque
ntTo
talOu
tcome
VA@F
inal
(Yrs)
Injur
ybe
twee
nOc
ular
COME
Tma
lities
pharo
nmo
nths
month
sSt
abilit
yat
12 m
ntssu
rgery
sfol
low up
at las
tFU
Injur
y to
Surg
eryat
6 mnts
(pkp/k
pro)
(COM
ET-S
x(C
OMET
folllo
w up
time g
ap in
to las
t visi
t)mo
nths)
1.18
FOD
Lime
34No
neHM
None
None
Abse
ntCF
1MCF
1MSta
bleSta
blePK
(12)
27Sta
ble20
/400
2.18
FOS
Lime
37All
o-LT,
PKPL
None
None
Abse
ntCF
1MCF
1MSta
bleSta
bleKp
ro (27
)32
Stable
20/25
3.26
MOS
Acid
41No
PLNo
neNo
neAb
sent
HMHM
Stable
Stable
Kpro
(42)
46Sta
ble20
/30p
4.48
MOD
Liq Am
monia
34AM
GHM
None
None
Pres
ent
HMHM
Fail
Fail
None
20Fa
ilPL
PR5.
34M
OSAc
id89
AMG,
Allo-
LT(2)
PLNo
neNo
neAb
sent
20/12
5CF
1MSta
bleSta
bleNo
ne38
Stable
CF 1M
PK6.
22M
ODTit
anium
Oxid
e7
None
PLNo
neNo
nePr
esen
tHM
HMSta
bleSta
bleNo
ne12
Fail
HM7.
30F
ODAc
id10
8PK
(2)PL
Lag
Yes
Pres
ent
PLPL
Fail
Fail
Tarso
(10)
10Fa
ilPL
8.17
FOS
Lime
12All
o-LT
PlNo
neYe
sAb
sent
PLPL
Fail
Fail
48Fa
ilHM
9.23
MOD
Ammo
nium
10AM
GHM
None
None
Pres
ent
PLHM
Stable
Stable
TA+B
CL (1
7)41
Fail
CF 1M
Nitrat
e10
.24
MOD
Acid
6AM
GHM
Lag
Yes
Abse
ntHM
HMSta
bleSta
bleNo
ne15
Stable
CF 1M
11.
30M
ODNa
SO53
AMG(
2)HM
None
None
Abse
ntHM
HMFa
ilFa
ilNo
ne12
Fail
HM
12.
16M
OSLim
e12
0No
nePL
None
None
Abse
ntHM
CF 1M
Stable
Stable
Kpro(
12)
3820
/2013
.18
MOD
Crac
ker In
jury
60AM
G(1)
PLNo
neNo
neAb
sent
PLHM
Stable
Stable
Kpro(
12)
36Sta
ble20
/30Ta
rsorap
hy(6)
Allo-L
T, PK
(1)SR
(2)14
.49
FOD
Form
ic ac
id13
AMG
PLNo
neYe
sAb
sent
PLPL
Fail
Fail
None
9Fa
ilPL
15.
18M
OSLim
e10
5All
o-LT(2
)PL
None
Yea
Abse
ntPL
PLFa
ilFa
ilNo
ne13
Fail
HMPK
, SR
16.
35M
ODUn
know
n24
0No
neHM
None
None
Abse
ntHM
CF 1M
Fail
Fail
None
12Fa
ilHM
17.
3F
OSUn
know
n18
None
HMNo
neYe
sAb
sent
PLPL
Fail
Fail
None
10Fa
ilHM
18.
8M
OSCr
acke
r Injur
y12
SRPL
None
Yes
Abse
ntHM
HMFa
ilFa
ilNo
ne7
Fail
HM19
.8
MOD
Lime
6SR
,HM
None
Yes
Abse
ntHM
HMFa
ilFa
ilNo
ne8
Fail
HMTa
rsorha
phy,
AMG
24
M=M
ale;
F=F
emal
e; A
llo-L
T= A
lloge
neic
Lim
bal T
rans
plant
ation
; PK=
Pen
etra
ting
Kera
topl
asty;
AM
G= A
mni
otic
Mem
bran
e G
raftin
g; V
A=Be
st Co
rrecte
d Vi
sual
Ac
uity;
HM
= Ha
nd M
ovem
ents;
PL=
Per
cept
ion O
f Lig
ht; C
F= C
ount
ing F
inger
s; K
pro=
Bos
ton
Type
1 K
erat
opro
sthes
is; T
A+BC
L= T
issue
Adh
esive
And
Ban
dage
Co
ntac
t Len
s App
licat
ion; T
arso
= Tar
sorrh
apy;
COM
ET= A
utolo
gous
Cult
ivate
d Ora
l Muc
osal
Epith
elial
Tran
splan
tatio
n
Volume 1, Issue 1, June 2014 COMET StudyCOMET StudyCOMET StudyCOMET StudyCOMET Study

CURRENT INDIAN EYE RESEARCH 21
Primary Outcome: The mean follow-up was 22.3 (range: 7to 48) months. Post-operatively on day one and at oneweek, fluorescein staining was negative over the graftedarea and no folding or loosening of the hAM was noted. Atsix weeks all the grafted eyes had a completely epithelizedand stable corneal surface but absence of peripheralsuperficial corneal vascularization noted in 16 (84%) of 19eyes. However, peripheral superficial cornealvascularization was seen in all eyes by three months.Therefore none of eyes met the clinical criteria of successat 3 months and thereafter. In 7 (36.8%) eyes the peripheralvascularization did not progress and the corneal surfacewas completely epithelized and stable at 12 months afterCOMET. In the remaining 12 (63.2%) eyes the centralcornea became progressively vascularized or developedpersistent epithelial defects with recurrence or worseningof symblepharon between 3 and 9 months of COMET.
Visual Outcomes: Prior to COMET the BCVA ranged fromhand movements to perception of light in all eyes. On thelast date of follow-up or before undergoing keratoplasty orkeratoprosthesis surgery the BCVA had not improved in12 (63%) eyes, had improved to counting fingers in 6 (32%)eyes and to 20/125 (5%) in one eye.
Additional Surgery: Of the 7 eyes with a stable ocularsurface, one eye underwent PK and four eyes underwentBoston type 1 keratoprosthesis surgery for visualimprovement. Following PK the corneal graft developedrepeated epithelial defects and a permanent tarsorrhaphyhad to be performed three months later. Three years afterPK the BCVA with an intact tarsorrhaphy was handmovements. The final BCVA in the four eyes that underwentBoston type 1 keratoprosthesis ranged from 20/20 to 20/30 with a maximum follow-up of 26 months.
Histopathology: (a) hematoxylin and eosin and PASstaining of the pannus excised during COMET showedeight to ten layer thick stratified columnar epithelium withpresence of goblet cells and underlying loose fibrovascularstromal tissue. These findings were consistent the clinicalimpression of LSCD. (b) hematoxylin and eosin and PASstaining of the unused back-up oral mucosal cultureshowed a monolayer of epithelium on a thick eosinophilicmembrane. (c) hematoxylin and eosin staining of thecorneal buttons excised during keratoplasty orkeratoprosthesis surgery following COMET showed a sixto eight cell stratified epithelium with basement membrane.No remnants of the hAM were seen. Goblet cells were notobserved in PAS staining. A few sub-epithelial blood
vessels were also seen in close proximity to the basementmembrane both at the periphery and at the centre.Bowman's membrane was absent and variable stromalscarring was noted. The Descemet's and endothelialcomplex was noted to be normal in all eyes.
Immunohistochemistry: (a) Immunohistochemicalexamination of the unused back-up culture showed: (1)Cytoplasmic K3/K12 expression was seen in all cells; (2)p63 expression was seen in all cells; (b)Immunohistochemical examination of the post-COMETcorneal tissues and control corneal and conjunctivalspecimens showed: (1) K19 being expressed in the basallayer of the epithelial cells of post-COMET corneas, in thebasal layer of the limbal epithelium in control corneas, inall layers of the conjunctiva and in the basal cells of theoral mucosa; (2) expression of K14 was absent in post-COMET corneas, absent in control corneas, present in thebasal cells of conjunctiva, absent in oral mucosa; (3)Cytoplasmic K3/K12 expression was seen in all epitheliallayers of post-COMET corneas, control corneas and oralmucosa but absent in conjunctiva; (4) Cytoplasmic K12staining was seen only in the control corneal epitheliumand was absent in oral, conjunctival and post-COMETepithelium; (5) Ki-67 expression was seen in the supra-basal layer of all specimens;(6) p63 expression was seenin basal and supra-basal layers of the post-COMETcorneas, control corneas, conjunctiva and oral mucosa;(7) p75 expression was seen in basal epithelial cells ofpost-COMET corneas, basal epithelial cells of the limbusin control corneas, basal cells of conjunctiva as well asoral mucosa; (8) CD31 and CD34 expression was seen insub-epithelial layers of the central and peripheral post-COMET corneas.
Discussion:
COMET emerged with the promise of being an autologousalternative to allogeneic cell based therapy in eyes withbilateral and total LSCD. Based on the experience withex-vivo cultivation of limbal epithelial cells21-24, wedeveloped an efficient xeno-free explant culture techniqueof expanding the oral mucosal cells into a transplantableepithelial sheet on denuded hAM6. We also noted that thecultivated oral mucosal epithelium had certain phenotypicsimilarities to limbal as opposed to conjunctival epithelium6.These results along with the promising clinical outcomesof COMET reported by other groups9-14 encouraged us toattempt this present clinical study in 2007. However, as
Volume 1, Issue 1, June 2014COMET StudyCOMET StudyCOMET StudyCOMET StudyCOMET Study

CURRENT INDIAN EYE RESEARCH22
elucidated in the results, the clinical experience withautologous COMET for the treatment of chronic ocularburns was extremely disappointing in terms of achievingocular surface stability, corneal clarity, avascularity andvisual improvement.
When we compare this study with the indications,laboratory techniques and clinical outcomes of previousstudies on autologous COMET with a sample size of 9 ormore eyes12-14, 17-19, it is note-worthy that: a) none of theprevious studies used a xeno-free culture technique; b)the indications for COMET varied widely among differentstudies; c) all studies used clinical criteria for assessingthe outcome of therapy; d) success rates with regards toocular surface stability ranged from 28.5% to 100% withmean follow-up durations ranging from 12 months to 55months; and e) all studies reported appearance ofperipheral superficial corneal vascularization after COMET.In the context of this heterogeneous data, ocular surfacestability achieved in our study (37% in 19 eyes) compareswell with that reported by Satake and associates (36% in11 eyes)18 and Burillon and associates (44% in 9 eyes)19
in eyes with ocular surface burns.
A comparison between this study and previous studies onCOMET with those on allogeneic limbal transplantation isagain difficult, because the indications and sample sizesvary among different studies. Indeed, there are nocomparable published studies (with a sample size of fiveeyes or more) of allogeneic cultivated limbal transplantationin eyes with ocular burns25,26. With regards to keratolimbalallografts, in two series of 16 and 17 eyes with ocular burnsamong other indications, Solomon and associates27 andMaruyama-Hosoi and associates28 reported long-termcorneal epithelial stability in 71.3% and 58.8% eyesrespectively. Similar to ocular surface stability, theproportion of patients who gained 20/200 or better vision,after keratolimbal allografting (43.5% to 44.6%)27,28 wasalso greater as compared to that after COMET (7% to 30%,Table 2)12-14,17-19. This limitation of COMET is particularlysignificant because unlike patients with unilateral LSCD,who usually have good vision in the unaffected eye andmay be satisfied with a stable and symptom free ocularsurface in the affected eye, the primary need of a patientwith bilateral blindness is improvement in vision. Thereforethe benefit of COMET of being an autologous therapy notrequiring immunosuppression does not outweigh its poorclinical outcomes. In view of these results, currently we donot offer COMET to patients with bilateral LSCD.
Other findings of our study were similar to Chen andassociates and Nakamura and associates who performedhistopathology and immuno-histochemical analysis in fourand six post-COMET eyes, respectively15,29. Onhistopathology, they found the transplanted epithelium tobe five to twelve layers thick without goblet cells or apicalmicrovilli. On immunohistochemistry, they also found thatK3 was present in all epithelial layers, K12 was presentoccasionally at the peripheral portion of corneal tissue,p63 and p75 was present in the basal epithelial layers.These findings along with ours suggest that thetransplanted oral mucosal epithelium maintains its originalphenotype without any trans-differentiation to the cornealphenotype. Additionally we showed expression of vascularendothelial markers CD31 and CD34 in the sub-epithelialregion of the post-COMET corneas to corroborate with theclinical findings of superficial vascularization.
This is the first report on transplantation of oral mucosalcells cultivated using a xeno-free technique of cell culture.Another strength of this study is the homogeneity of thepatient cohort; being the largest such study in cases withbilateral ocular burns. Unlike others we used an explantculture technique and transplanted at a monolayer stage,like we do for cultivated limbal epithelial transplan-tation21-24. It may be argued that these unconventionaltechniques of cultivation and transplantation may haveaffected the results. But similar poor outcomes of COMETin ocular burns have been reported with conventional cellculture protocols as well18,19. We also found that the oralepithelium does not convert to a corneal phenotype whentransplanted onto the ocular surface and because of theassociated vascularization, which is probably essential toits survival, a conjunctivalized ocular surface and onereconstructed after COMET are virtually indistinguishable.
In summary, the findings of our study suggest thattransplantation of autologous oral mucosal epitheliumcultivated using a xeno-free explant culture system, isunsuccessful in restoring a stable ocular surface andimproving vision in eyes with bilateral LSCD followingocular burns. However, our results do not apply to othercauses of LSCD or other cell-culture protocols.
Reference:
1. Schermer A, Galvin S, Sun TT. Differentiation-relatedexpression of a major 64K corneal keratin in vivo andin culture suggests limbal location of corneal epithelialstem cells. J Cell Biol 1986; 103: 49-62.
Volume 1, Issue 1, June 2014 COMET StudyCOMET StudyCOMET StudyCOMET StudyCOMET Study
CURRENT INDIAN EYE RESEARCH 23
2. Cotsarelis G, Cheng SZ, Dong G, Sun TT, Lavker RM.Existence of slow-cycling limbal epithelial basal cellsthat can be preferentially stimulated to proliferate:implications on epithelial stem cells. Cell 1989; 57:201-9.
3. Kenyon KR, Tseng SC. Limbal autografttransplantation for ocular surface disorders.Ophthalmology 1989; 96: 709-22.
4. Pellegrini G, Traverso CE, Franzi AT, Zingirian M,Cancedda R, De Luca M. Long-term restoration ofdamaged corneal surfaces with autologous cultivatedcorneal epithelium. Lancet 1997; 349 :990-3.
5. Fernandes M, Sangwan VS, Rao SK, Basti S, SridharMS, Bansal AK, Dua HS. Limbal stem celltransplantation. Indian J Ophthalmol 2004; 52:5-22.
6. Madhira SL, Vemuganti G, Bhaduri A, Gaddipati S,Sangwan VS, Ghanekar Y. Culture andcharacterization of oral mucosal epithelial cells onhuman amniotic membrane for ocular surfacereconstruction. Mol Vis 2008;14:189-96.
7. Krishnan S, Iyer GK, Krishnakumar S. Culture &characterisation of limbal epithelial cells & oralmucosal cells. Indian J Med Res 2010; 131: 422-8.
8. Gipson IK, Geggel HS, Spurr-Michaud SJ. Transplantof oral mucosal epithelium to rabbit ocular surfacewounds in vivo. Arch Ophthalmol 1986; 104: 1529-33.
9. Nakamura T, Endo K, Cooper LJ, et al. The successfulculture and autologous transplantation of rabbit oralmucosal epithelial cells on amniotic membrane. InvestOphthalmol Vis Sci 2003; 44: 106-16.
10. Hayashida Y, Nishida K, Yamato M, et al. Ocularsurface reconstruction using autologous rabbit oralmucosal epithelial sheets fabricated ex vivo on atemperature-responsive culture surface. InvestOphthalmol Vis Sci 2005;46:1632-9.
11. Nishida K, Yamato M, Hayashida Y, Watanabe K,Yamamoto K, Adachi E, et al. Corneal reconstructionwith tissue-engineered cell sheets composed ofautologous oral mucosal epithelium. N Engl J Med2004; 351: 1187-96.
12. Nakamura T, Inatomi T, Sotozono C, Amemiya T,Kanamura N, Kinoshita S. Transplantation of
cultivated autologous oral mucosal epithelial cells inpatients with severe ocular surface disorders. Br JOphthalmol 2004; 88: 1280-4.
13. Inatomi T, Nakamura T, Koizumi N, Sotozono C, YokoiN, Kinoshita S. Midterm results on ocular surfacereconstruction using cultivated autologous oralmucosal epithelial transplantation. Am J Ophthalmol2006;141:267-75.
14. Ang LP, Nakamura T, Inatomi T, Sotozono C, KoizumiN, Yokoi N, Kinoshita S. Autologous serum-derivedcultivated oral epithelial transplants for severe ocularsurface disease. Arch Ophthalmol 2006; 124: 1543-51.
15. Chen HC, Chen HL, Lai JY, et al. Persistence oftransplanted oral mucosal epithelial cells in humancornea. Invest Ophthalmol Vis Sci 2009; 50: 4660-8.
16. Ma DH, Kuo MT, Tsai YJ, et al. Transplantation ofcultivated oral mucosal epithelial cells for severecorneal burn. Eye 2009; 23: 1442-50.
17. Nakamura T, Takeda K, Inatomi T, Sotozono C,Kinoshita S. Long-term results of autologous cultivatedoral mucosal epithelial transplantation in the scarphase of severe ocular surface disorders. Br JOphthalmol 2011;95:942-6.
18. Satake Y, Higa K, Tsubota K, Shimazaki J. Long-termoutcome of cultivated oral mucosal epithelial sheettransplantation in treatment of total limbal stem celldeficiency. Ophthalmology 2011; 118: 1524-30.
19. Burillon C, Huot L, Justin V, et al. Cultured AutologousOral Mucosal Epithelial Cell-Sheet (CAOMECS)Transplantation for the Treatment of Corneal LimbalEpithelial Stem Cell Deficiency. Invest Ophthalmol VisSci 2012 ;53:1325-31
20. Schwab IR, Johnson NT, Harkin DG. Inherent risksassociated with manufacture of bioengineered ocularsurface tissue. Arch Ophthalmol 2006; 124: 1734-40.
21. Mariappan I, Maddileti S, Savy S, et al. In vitro cultureand expansion of human limbal epithelial cells. NatProtoc 2010; 5: 1470-9.
22. Sangwan VS, Basu S, Vemuganti GK, et al. Clinicaloutcomes of xeno-free autologous cultivated limbalepithelial transplantation: a 10-year study. Br JOphthalmol 2011; 95: 1525-9.
Volume 1, Issue 1, June 2014COMET StudyCOMET StudyCOMET StudyCOMET StudyCOMET Study

CURRENT INDIAN EYE RESEARCH24
23. Basu S, Mohamed A, Chaurasia S, Sejpal K,Vemuganti GK, Sangwan VS. Clinical outcomes ofpenetrating keratoplasty after autologous cultivatedlimbal epithelial transplantation for ocular surfaceburns. Am J Ophthalmol 2011; 152: 917-24.e1.
24. Basu S, Ali MH, Sangwan VS. Clinical Outcomes ofRepeat Autologous Cultivated Limbal EpithelialTransplantation for Ocular Surface Burns. Am JOphthalmol 2012 ;153:643-50, 650.e1-2
25. Shortt AJ, Tuft SJ, Daniels JT. Ex vivo cultured limbalepithelial transplantation. A clinical perspective. OculSurf 2010;8:80-90.
26. Baylis O, Figueiredo F, Henein C, Lako M, AhmadS.13 years of cultured limbal epithelial cell therapy:
A review of the outcomes. J Cell Biochem2011;112:993-1002.
27. Solomon A, Ellies P, Anderson DF, Touhami A, et al.Long-term outcome of keratolimbal allograft with orwithout penetrating keratoplasty for total limbal stemcell deficiency. Ophthalmology 2002; 109: 1159-66.
28. Maruyama-Hosoi F, Shimazaki J, Shimmura S,Tsubota K. Changes observed in keratolimbal allograft.Cornea 2006; 25: 377-82.
29. Nakamura T, Inatomi T, Cooper LJ, Rigby H, FullwoodNJ, Kinoshita S. Phenotypic investigation of humaneyes with transplanted autologous cultivated oralmucosal epithelial sheets for severe ocular surfacediseases. Ophthalmology 2007; 114: 1080-8.
DisclaimerCurrent Indian Eye Research (CIER) is the journal of Ophthalmic Research Group, which giveseditorial freedom to the editor of CIER. CIER follows guidelines of editorial independence proposedby World Association of Medical Editors and code of good publication practice of the Committee ofPublication Ethics.
CIER is intended for professionals associated with medical research and practice, without warranty,express or implied. Statements in the journal are responsibilities of the authors and advertisers and notthe author’s institution, publisher, editors or the Ophthalmic Research Group. Publication ofadvertisement does not imply endorsement.
Volume 1, Issue 1, June 2014 COMET StudyCOMET StudyCOMET StudyCOMET StudyCOMET Study
CURRENT INDIAN EYE RESEARCH 25
Original ArticleOriginal ArticleOriginal ArticleOriginal ArticleOriginal Article
Combination of Azathioprine and Corticosteroids in the Treatment ofSerpiginous ChoroiditisAneesha Lobo1, Prachir Agarwal1, Debmalya Das1, Manmath Das1, Rupak Roy1, Jyotirmay Biswas2
1. Shri Bhagwan Mahavir Vitreoretinal Services, 18, College Road, Sankara Nethralaya, Chennai-600 006, Tamil Nadu, India, 2. L and TDepartment of Ocular Pathology, Vision Research Foundation, Sankara Nethralaya, Chennai, India.Corresponding Author : Dr. Rupak Roy, E-mail: [email protected] on : 06/04/2014, Revision accepted on : 25/06/2014Conflict of Interest : None, Financial Disclosure : None
Abstract
Purpose: To evaluate the role and efficacy of combination of azathioprine and corticosteroids in the treatment of serpiginouschoroiditis. Methods: Medical records of all patients with serpiginous choroiditis those were treated with a combination regimenof azathioprine 2.5 mg/kg/body weight in 3 divided doses and prednisolone 1mg/ kg body weight for at least 6 months werereviewed. The patients were followed up every month for atleast 6 months or till the lesions showed clinical and angiographic signsof inactivity. Doses of both azathioprine (50 mg/ month) and prednisolone (10 mg/ week) were tapered as and when the lesionsbecame inactive. On subsequent follow-up visits, any episode of relapse was treated by resuming the therapy with both agents in thedoses described above with a more prolonged tapering. Blood counts were monitored every 15 days and liver function tests everymonth. Sight threatening serpiginous choroiditis was initially treated with 1 gram/day of intravenous methyl prednisolone for 3days, followed by the above mentioned regimen. Wilcoxon sign rank test was done to obtain the p value for comparison of pretreatment and post treatment visual acuity. Results: Medical records of 30 eyes of 19 patients were evaluated. All patients showeddisease regression having inactive lesion at the time of last follow-up. Only four out of the thirty eyes showed deterioration of visualacuity. Thirteen (43%) out of the thirty eyes maintained their pretreatment visual acuity and another thirteen (43%) eyes hadimprovement in visual acuity. (p = 0.023). Conclusion: Combination therapy of azathioprine and corticosteroids is an effectiveregimen for treatment of serpiginous choroiditis.
Key words: azathioprine, corticosteroids, immunosuppressive agents, intravenous methyl prednisolone, serpiginous choroiditis.
Serpiginous choroiditis is a chronic, visually debilitating,progressive condition of undetermined etiology. The
disease shows recurrent episodes of choroiditis involvingboth eyes primarily affecting the retinal pigment epithelium(RPE), the choriocapillaris and the choroid1. Apart fromthe typical peripapillary form of the disease, many differentforms have been described like macular serpiginouschoroiditis (predominantly involving the macular area) andampigenous choroiditis (which combines the signs ofserpiginous choroiditis and APMPPE) wherein the funduslesions involve the disc and the macula in a mutifocalpattern.
Many systemic diseases are reported to be associated withserpiginous choroiditis, but they are, merely an associationrather than the cause of the disease. Infections such astuberculosis and herpes have been associated withserpiginous choroiditis in India2. Approximately 25% of thepatients may develop choroidal neovascular membrane(CNVM) that leads to loss of central vision late in the course
of disease. The visual implications of serpiginouschoroiditis are, therefore, quite serious and about 75% ofpatients have a final visual acuity of less than or equal to6/603,4. The therapeutic options available for treatment aresystemic corticosteroids5, antimetabolites6 and immuno-suppressive agents7,8. A number of studies have been doneto find the optimum therapeutic regimen for serpiginouschoroiditis. Hooper and Kaplan have described triple agenttherapy for serpiginous choroiditis consisting ofcorticosteroids, azathioprine and cyclosporine9. Howeverthis therapeutic regimen exposes the patient to seriousside effects of two immunosuppressive agents andcorticosteroids. Therefore, in the present study, we havetried to explore the efficacy of treatment using a singleimmunosuppressive agent (azathioprine) along withsystemic corticosteroids.
Materials and Methods:
The medical records of all patients diagnosed as

CURRENT INDIAN EYE RESEARCH26
serpiginous choroiditis and treated with combinationtherapy of Azathioprine and Corticosteroids, in a tertiarycare centre in southern India between January 2000 toDecember 2008 were reviewed. Patients on any otherimmunosuppersive regimen were excluede from the study.The study was approved by the Institutional Review Boardand a written consent taken as per Helsinki Declaration.All patients received oral azathioprine 2.5 mg/kg bodyweight/day in three divided doses. Systemic corticosteroidswere given in a dose of 1 mg/ kg body weight/day orallywith 10 mg/ week tapering for a minimum period of 6months. Sight-threatening disease was treated initially withintravenous methyl prednisolone (IVMP) 1 gm/day for 3consecutive days followed by azathioprine and oralcorticosteroids10. Azathioprine was continued for at least6 months along with corticosteroids and the patients werereviewed every month for first 6 months.
A detailed ophthalmic examination including best-correctedvisual acuity (BCVA), applanation tonometry, slit-lampbiomicroscopy, fundus examination by noncontact +78Dlens and indirect ophthalmoscopy were performed at eachvisit. Fundus fluorescein angiogram was done as and whenfelt necessary. During each review, activity of the lesion,any drop in vision from the previous visit and side effectsof azathioprine and corticosteroids were noted.Azathioprine and corticosteroids were continued till thelesions showed clinical signs of regression. If required,fundus fluorescein angio-graphy was performed duringfollow up and the absence of late phase leakage from themargins of active lesions was considered as the evidenceof regression. If the lesions were found to be active, therapywas further continued till they became inactive.Corticosteroids were tapered at the first sign of inactivityat a rate of 10 mg per week and azathioprine in a dose of50 mg per month.
During follow up visits, development of new lesions and /or appearance of lesions adjacent to the previously inactivelesions were taken as signs of relapse, that were treatedby resuming the therapy with a more prolonged tapering.Total leukocyte count and total platelet count weremonitored every fortnight and liver function test wasrepeated at monthly interval.
Statistical analysis was performed using SPSS forWindows (version 14; SPSS, Inc., Chicago, IL). Diseaseactivity at final follow-up, visual acuity outcome, durationof azathioprine therapy and number of relapses wererecorded. Vision was recorded in Snellens and converted
into logMAR for statistical analysis. Pre and post treatmentvisual acuity were compared by Wilcoxon sign rank test.Significance was assessed at p 0.05 level for allparameters.
Results:
Thirty eyes of 19 patients were analyzed. Six (31.5%) werefemales and 13 (68.5%) were males. The mean age was36.16 years (range 16-63 years). Eleven (58%) patientshad bilateral disease. Mean duration of follow-up was 32.9months (range 6 to 79 months, S.D.18.15) and meanduration of azathioprine therapy was 6.5 months (range 3to 20 months, S.D. 5.7). All patients showed diseaseregression in the form of inactive lesion at the time of lastfollow-up. But three patients (5 eyes, 16.6 %) developedrecurrence once and one (2 eyes, 6.6 %) had two episodesof recurrence which were managed by increasing the dosesof oral corticosteroids and azathioprine. The mean initialBCVA was 0.33 LogMAR units. The mean final BCVA was0.15 LogMAR units (Mean visual acuity cannot becalculated in snellens as it is a non continuous parameterhence we have provided the mean logMAR value- Pleasemention snellen's VA) The improvement in the visual acuitybefore and after institution of combination therapy wasstatistically significant (p = 0.023, Wilcoxon sign rank test).Thirteen (43.3%) eyes had improvement in visual acuity,13 (43.3%) maintained the pretreatment visual acuity. Four(13.4%) eyes showed deterioration of visual acuity in spiteof disease remission clinically as a result of involvementof the center of fovea.
Discussion:
The pathogenesis of serpiginous choroiditis remainsunknown despite various studies done in the past to identifythe infectious, the immunological, and the vascular etiologyof the disease. Various infections such as tuberculosis andherpes virus have also been implicated in thepathogenesis2,10. The inflammatory nature of the diseaseis supported by histopathological findings such aslymphocytic infiltrates in the choroid and the vessel wall11.
A large number of immunosuppressive agents have beentried either alone or in combination to treat serpiginouschoroiditis (Table 1). Corticosteroids have both anti-inflammatory and immuno-suppressive actions. Thedifficulty with corticosteroid therapy alone is that it has noeffect on prevention of recurrences. Recurrences arecommon while tapering the dose or shortly afterdiscontinuation of the treatment. Gupta et al treated
Volume 1, Issue 1, June 2014 Serpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous Choroiditis
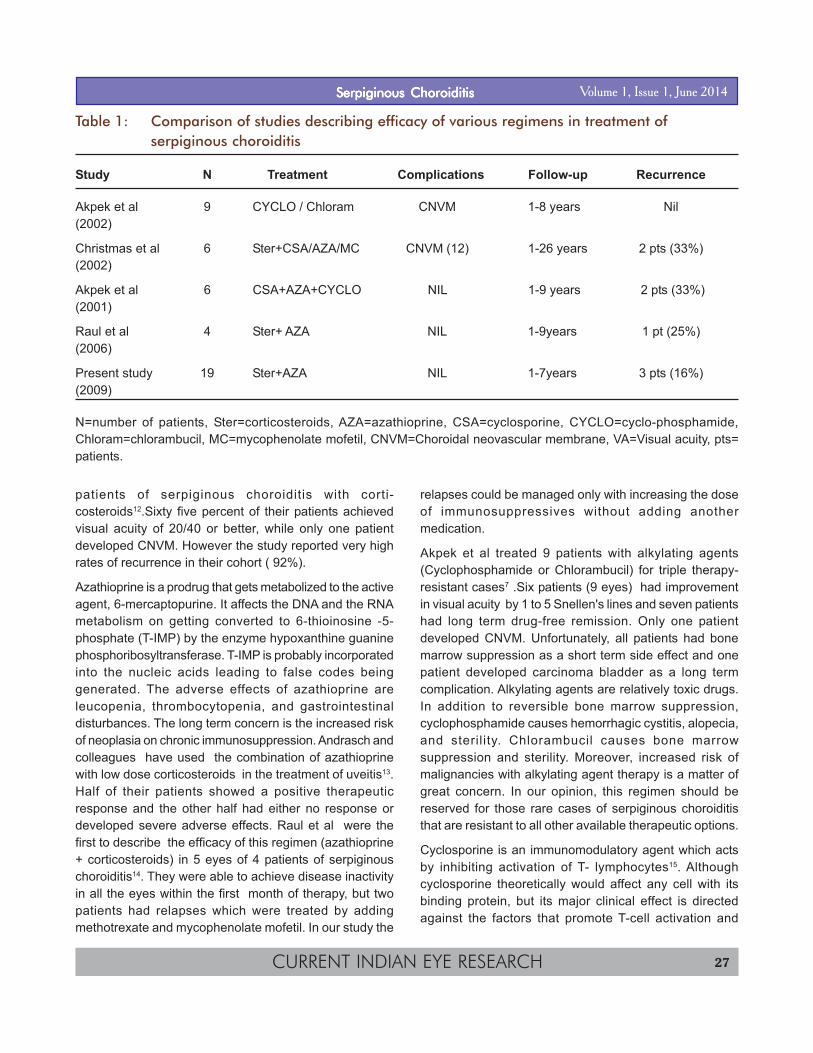
CURRENT INDIAN EYE RESEARCH 27
patients of serpiginous choroiditis with corti-costeroids12.Sixty five percent of their patients achievedvisual acuity of 20/40 or better, while only one patientdeveloped CNVM. However the study reported very highrates of recurrence in their cohort ( 92%).
Azathioprine is a prodrug that gets metabolized to the activeagent, 6-mercaptopurine. It affects the DNA and the RNAmetabolism on getting converted to 6-thioinosine -5-phosphate (T-IMP) by the enzyme hypoxanthine guaninephosphoribosyltransferase. T-IMP is probably incorporatedinto the nucleic acids leading to false codes beinggenerated. The adverse effects of azathioprine areleucopenia, thrombocytopenia, and gastrointestinaldisturbances. The long term concern is the increased riskof neoplasia on chronic immunosuppression. Andrasch andcolleagues have used the combination of azathioprinewith low dose corticosteroids in the treatment of uveitis13.Half of their patients showed a positive therapeuticresponse and the other half had either no response ordeveloped severe adverse effects. Raul et al were thefirst to describe the efficacy of this regimen (azathioprine+ corticosteroids) in 5 eyes of 4 patients of serpiginouschoroiditis14. They were able to achieve disease inactivityin all the eyes within the first month of therapy, but twopatients had relapses which were treated by addingmethotrexate and mycophenolate mofetil. In our study the
relapses could be managed only with increasing the doseof immunosuppressives without adding anothermedication.
Akpek et al treated 9 patients with alkylating agents(Cyclophosphamide or Chlorambucil) for triple therapy-resistant cases7 .Six patients (9 eyes) had improvementin visual acuity by 1 to 5 Snellen's lines and seven patientshad long term drug-free remission. Only one patientdeveloped CNVM. Unfortunately, all patients had bonemarrow suppression as a short term side effect and onepatient developed carcinoma bladder as a long termcomplication. Alkylating agents are relatively toxic drugs.In addition to reversible bone marrow suppression,cyclophosphamide causes hemorrhagic cystitis, alopecia,and sterility. Chlorambucil causes bone marrowsuppression and sterility. Moreover, increased risk ofmalignancies with alkylating agent therapy is a matter ofgreat concern. In our opinion, this regimen should bereserved for those rare cases of serpiginous choroiditisthat are resistant to all other available therapeutic options.
Cyclosporine is an immunomodulatory agent which actsby inhibiting activation of T- lymphocytes15. Althoughcyclosporine theoretically would affect any cell with itsbinding protein, but its major clinical effect is directedagainst the factors that promote T-cell activation and
Table 1: Comparison of studies describing efficacy of various regimens in treatment ofserpiginous choroiditis
Study N Treatment Complications Follow-up Recurrence
Akpek et al 9 CYCLO / Chloram CNVM 1-8 years Nil(2002)
Christmas et al 6 Ster+CSA/AZA/MC CNVM (12) 1-26 years 2 pts (33%)(2002)
Akpek et al 6 CSA+AZA+CYCLO NIL 1-9 years 2 pts (33%)(2001)
Raul et al 4 Ster+ AZA NIL 1-9years 1 pt (25%)(2006)
Present study 19 Ster+AZA NIL 1-7years 3 pts (16%)(2009)
N=number of patients, Ster=corticosteroids, AZA=azathioprine, CSA=cyclosporine, CYCLO=cyclo-phosphamide,Chloram=chlorambucil, MC=mycophenolate mofetil, CNVM=Choroidal neovascular membrane, VA=Visual acuity, pts=patients.
Volume 1, Issue 1, June 2014Serpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous Choroiditis

CURRENT INDIAN EYE RESEARCH28
recruitment. Its common side effects are nephrotoxicity,hypertension, and myelosuppression. Hooper and Kaplanhave reported triple agent immunosuppression9(combination of azathioprine, corticosteroids andcyclosporine) in the treatment of serpiginous choroiditis.They treated five patients of bilateral disease where threepatients had remission while being maintained on low dosetriple therapy and two had relapses. Christmas et al treated34 eyes of 17 patients with corticosteroids and variousimmunosuppressive agents16.Only 23-26% of their patientshad a final visual acuity of less than 20/200, but they hada higher rate of CNVM development (35%). Akpek et altreated 6 patients with different combinations ofimmunosuppressive agents, cyclosporine and azathioprinein 3 patients, cyclophosphamide in 2 patients andcyclosporine in 1 patient15. They reported visualimprovement in 10 eyes and recurrences in two. Araujo etal treated 14 eyes of 7 patients with corticosteroids andcyclosporine17. In addition, two patients receivedazathioprine and one had mycophenolate mofetil. Visionwas maintained in 10 eyes, 3 had improvement and onehad deterioration due to the formation of cataract.Laatikainen et al treated 15 patients with antituberculardrugs or corticosteroids18. They reported development ofCNVM in 2 eyes and their series did not report anyfavorable outcome at all. All these studies employingdifferent regimens did not show convincing evidence toprove one's superiority over another. Till date, ours is thelargest case series evaluating the efficacy of combinationtherapy of azathioprine and oral corticosteroids in thetreatment of serpiginous choroiditis.
In the present series, the patients in whom the final BCVAin the affected eye showed deterioration had involvementof fovea by the disease process. In fact the lesions becameinactive with the treatment and all the patients showedresolution of the disease. None of the patients reportedmajor side effects of either azathioprine or oralcorticosteroids. Two patients had one episode of relapseand one had two episodes of relapse that were managedby increasing the dose of immunosuppressive and by moreprolonged tapering of corticosteroids. The outcome of thisstudy as determined on analysis of 19 eyes of 30 patientswas that an improvement in visual acuity does occur withtreatment with azathioprine and corticosteroids.We reportstabilization or improvement in around 86% of the eyesand minimal recurrence.Limitations of this study areinherent to its retrospective, cross-sectional design andthat it lacked a comparator group. As a retrospective review,
the sample size and selection bias are likely significantfactors. Furthermore, the patients in this study were not ahomogenous group, and represent serpiginous choroiditisin various stages of disease. We recognize that there aresubjective limitations to fundus picture and angiograminterpretation. We suggest further prospective studies tooptimize treatment protocols.
We conclude that combination therapy employingazathioprine and corticosteroids is an equally effectivealternative to triple agent therapy in the treatment ofserpiginous choroiditis.
References:
1. Abrez H, Biswas J, Sudharshan S. Clinical Profile,Treatment, and Visual Outcome of SerpiginousChoroiditis Ocul Immunol Inflamm 2007;15, 325-35.
2 Gupta V, Gupta A, Arora S, Bambery P, Dogra M R,Agarwal A: Presumed tubercular serpiginouschoroiditis: clinical presentations and management.Ophthalmology 2003; 110:1744-49.
3. Lee DK,Augustin W,Buggage RR,Suhler EBSerpiginous choroidopathy presenting as choroidalneovascularisation Br J Ophthalmol 2003;87:1184-85.
4. Blumenkranz MS, Gass D, Clarkson JD. AtypicalSerpiginous Choroiditis Arch Ophthalmol 1982; 100:1773-5.
5. Weiss H, Annesley W H, Shields J A, Tomer T,Christopherson K. The clinical course of serpiginouschoroidopathy. Am J Ophthalmol 1979; 87:133- 42
6. Laatikainen L, Erkkila H. A follow-up study onserpiginous choroiditis. Acta Ophthalmol (copenh)1981; 59:707-18.
7. Akpek EK, Douglas A,J, Tessler HH, Joondeph CB.Successful treatment of serpiginous choroiditis withalkylating agents.Ophthal-mology2002;109:1506-13.
8. R H, Piorfsky B, Burns R P. Immuno-suppressivetherapy for severe chronic uveitis. Arch Ophthal 1978;96:247-51.
9. Hooper P L, Kaplan H J. Triple agent Immuno-suppression in Serpiginous Choroiditis.Ophthalmology 1991; 98:944-52..
10. Saraswathy S, Rao NA, Smith RE. TuberculousUveitis: Distribution of Mycobacterium tuberculosis inthe Retinal Pigment Epithelium. Arch Ophthamol.2006; 124:1777-9.
11. Nicholas J. Cutrufello, Petros C. Karakousis, JaneFishler, Thomas A. Albini Intraocular TuberculosisOcular Immunology and Inflammation 2010, 1: 281-91.
Volume 1, Issue 1, June 2014 Serpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous Choroiditis

CURRENT INDIAN EYE RESEARCH 29
12. Gupta V, Agarwal A, Gupta A, Bambery P, Narang S:Clinical characteristics of serpiginous choroidopathyin North India. Am J Ophthalmol 2002; 134:47-56.
13. Andrasch R H, Piorfsky B, Burns R P.Immunosuppressive therapy for severe chronicuveitis. Arch Ophthalmol 1978; 96:247-51.
14. Raul N G V, Ozdal P C, Deschenes J , Burnier M N.Combination of Azathioprine and Corticosteroids inthe treatment of serpiginous Choroiditis. Can JOphthalmol 2006; 41:183-9.
15. Akpek EK, Baltatzis S, Yang J, Foster CS. Long-term immunosuppressive treatment of serpiginouschoroiditis. Ocul Immunol and Inflammation 2001; 9 :153-67.
16. Christmas N J, Oh K T, Oh D M, Folk JC. Long termfollow-up of patients with serpiginous choroiditis.Retina 2002; 22:550-6.
17. Araujo AA,Wells AP,Dick AD,Forrester JV. Earlytreatment with cyclosporin in serpiginouschoroidopathy maintains remission and good visualoutcome Br J Ophthalmol 2000;84:979-82
18. Laatikainen L, Erkkila H. Serpiginous choroiditis. Br JOphthalmol 1974;58:777-83
19. Akpek EK, Baltatzis S, Yang J, Foster CS. Long-term immunosuppressive treatment of serpiginouschoroiditis. Ocul Immunol and Inflammation 2001; 9 :153-67.
Volume 1, Issue 1, June 2014Serpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous ChoroiditisSerpiginous Choroiditis

CURRENT INDIAN EYE RESEARCH30
Community Based Intervention for PreventingCorneal Injury from Paddy GrainAsim Kumar Sil
Abstract
Purpose: To assess community based intervention in preventing general injury from paddy grain. Method: Six villages wereselected. Educative materials were produced to propagate use of protective glass during the time of threshing. Interactive meetingswere organised. Plastic dark goggles and white goggles were promoted. Hospital records were stadied and compared with previousyear. Result: Not a single case of paddy grain injury was reported from these area. Conclusion: Campaign and availibity ofprotective goggles is helpful in preventing such injury.
The prevalence of ocular injury in agriculture-workersis unknown in India; but data from few studies suggest
that this is quite common1, 2. It varies from region to regionaccording to the nature of the crop. Injury from sugarcaneleaf is quite common in northern and western India, grapevine injury is common in central and south India. Paddygrain injury of cornea is very common in coastal India whererice is grown as main crop. In recent years the incidenceof paddy grain injury has gone up because mechanicalthreshers have replaced the practice of manual separationof grains by beating the plant against a hard platform. Thisarticle depicts the results of a community based interventionfor preventing corneal injury in a rural area of West Bengal,India.
Paddy grain and the eye: The age old practice of separationof paddy grains from the plant used to be hitting the tip ofthe plant against a bamboo platform. This process takeslonger time and involves more manpower. Since the speedof the grain during separation is less there is less chanceof eye injury by paddy. Now the process has been replacedby the use of mechanical threshers to do the same work inmuch shorter time and save manpower.
Rice is the main crop in major part of India. In some fertileareas of the country it is grown thrice a year. Naturallyfarmers engaged in paddy cultivation in those areas aremore exposed to the risk of corneal injury at the time ofharvesting. Plants grown in different seasons are not ofsame length. In Southern part of Bengal one high yielding
Netra Niramay Niketan, Vivekananda Mission Ashram, Chaitanyapur, Purba Medinipur, West BengalCorresponding Author : Dr. Asim Sil, E-mail: [email protected] on : 23/04/2014, Accepted on : 20/05/2014Conflict of Interest : None, Financial Disclosure : None
variety of rice is harvested during April-May. This plant isshortest in length and has much more number of grainsthan the other ones. That is why cases of corneal abrasionare much more reported during April-May.
During harvesting the entire family of a farmer is involvedin the work. Mechanical threshers are used usually by twogentlemen who operate the machine by feet and place thetip of the plant over the spin. Another person, usually alady constantly sweeps the ground to collect the grains atone place. Her face is usually closer to the machine andmore prone to injury. Anybody, even a child moving closeto the thresher may get injured.
Farmers have a habit of covering the head and face with apiece of cloth to avoid dust but leave the eyes open whilethreshing. This practice keeps the eyes unprotected. Thecommonest mode of injury is abrasion of cornea by rapidlymoving seed. The most unfortunate sequel of this injury isdevelopment of fungal keratitis. Paddy grain has fine hairlike structures over the outer coating. That is why the grainsget anchored to conjunctiva firmly. Sometimes the grainlodges inside the upper fornix and remain unnoticed. Eventhe plant may start growing inside the eye5. Treatment offungal keratitis is difficult in any peripheral location. Thecases report late and are often complicated by the use ofunknown eye drops and native medication. Fungal culturefacility is usually not available in the periphery andantifungal medications are used empirically. Applicationof too many drops often reduces the efficacy of antibiotics.
Original Article — Community OphthalmologyOriginal Article — Community OphthalmologyOriginal Article — Community OphthalmologyOriginal Article — Community OphthalmologyOriginal Article — Community Ophthalmology
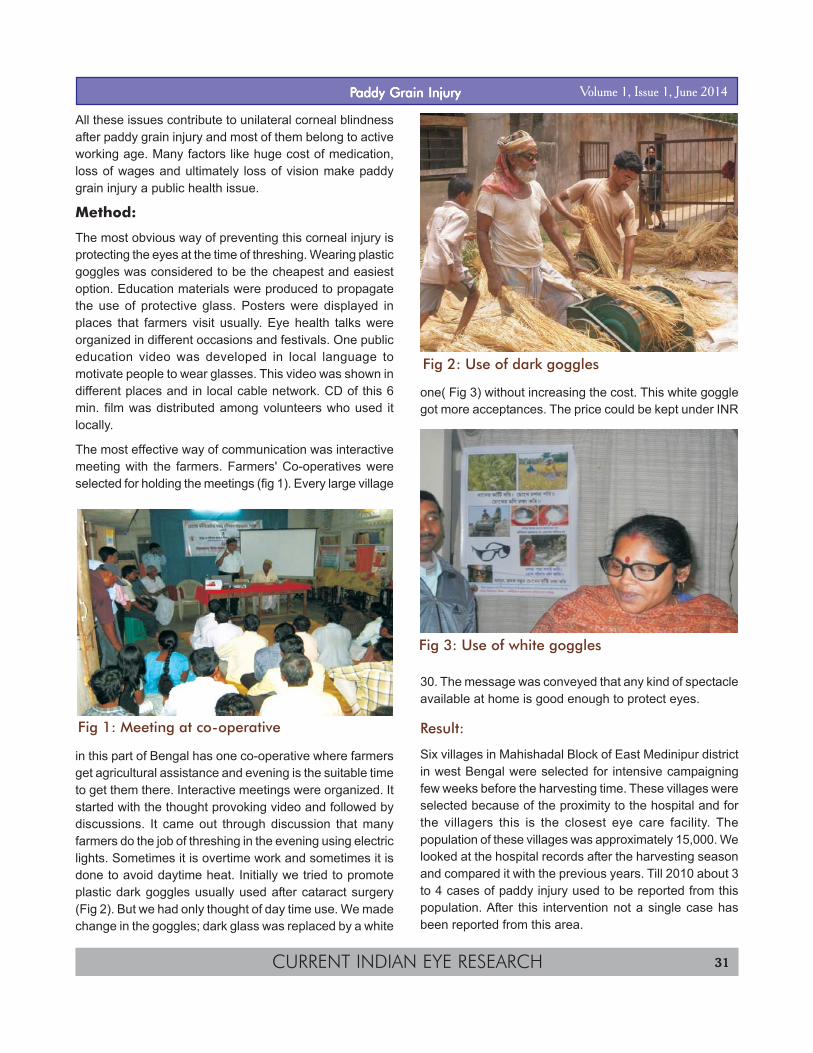
CURRENT INDIAN EYE RESEARCH 31
All these issues contribute to unilateral corneal blindnessafter paddy grain injury and most of them belong to activeworking age. Many factors like huge cost of medication,loss of wages and ultimately loss of vision make paddygrain injury a public health issue.
Method:
The most obvious way of preventing this corneal injury isprotecting the eyes at the time of threshing. Wearing plasticgoggles was considered to be the cheapest and easiestoption. Education materials were produced to propagatethe use of protective glass. Posters were displayed inplaces that farmers visit usually. Eye health talks wereorganized in different occasions and festivals. One publiceducation video was developed in local language tomotivate people to wear glasses. This video was shown indifferent places and in local cable network. CD of this 6min. film was distributed among volunteers who used itlocally.
The most effective way of communication was interactivemeeting with the farmers. Farmers' Co-operatives wereselected for holding the meetings (fig 1). Every large village
in this part of Bengal has one co-operative where farmersget agricultural assistance and evening is the suitable timeto get them there. Interactive meetings were organized. Itstarted with the thought provoking video and followed bydiscussions. It came out through discussion that manyfarmers do the job of threshing in the evening using electriclights. Sometimes it is overtime work and sometimes it isdone to avoid daytime heat. Initially we tried to promoteplastic dark goggles usually used after cataract surgery(Fig 2). But we had only thought of day time use. We madechange in the goggles; dark glass was replaced by a white
one( Fig 3) without increasing the cost. This white gogglegot more acceptances. The price could be kept under INR
30. The message was conveyed that any kind of spectacleavailable at home is good enough to protect eyes.
Result:
Six villages in Mahishadal Block of East Medinipur districtin west Bengal were selected for intensive campaigningfew weeks before the harvesting time. These villages wereselected because of the proximity to the hospital and forthe villagers this is the closest eye care facility. Thepopulation of these villages was approximately 15,000. Welooked at the hospital records after the harvesting seasonand compared it with the previous years. Till 2010 about 3to 4 cases of paddy injury used to be reported from thispopulation. After this intervention not a single case hasbeen reported from this area.
Fig 2: Use of dark goggles
Fig 3: Use of white goggles
Fig 1: Meeting at co-operative
Volume 1, Issue 1, June 2014PPPPPaddy Grain Injuryaddy Grain Injuryaddy Grain Injuryaddy Grain Injuryaddy Grain Injury

CURRENT INDIAN EYE RESEARCH32
Discussion:
There are always barriers in the usage of safety eyewearamongst workers. In one study4 from central India aboutthree-fourth of the workers reported using it all or most ofthe time during work. Despite knowing that protectiveeyewear devices offer safety from work-related injuriesworkers do not tend to use them for multiple reasons. Theseinclude some blurring of vision, discomfort, fogging,unusual appearance, people making fun of them, slippingof the goggles due to sweat and slowing work pace.
Prevention of ocular injuries in agriculture workers willindirectly reduce the incidence of microbial keratitisamongst them. Srinivasan et al had demonstrated thattreating corneal abrasions with antibiotic ointment by healthworkers at the village level significantly reduced theincidence of bacterial and fungal corneal ulcers3, butprimary prevention of injury is always the best. It is all aboutdeveloping the attitude of adopting safety measures.Constant effort of educating the community would resultin consciousness about eye safety and develop peerpressure to wear protective goggles. Providing protectivegoggles at an affordable cost should complement this effort.The manufactures of the threshers have great responsibilityin ensuring safety by modifying the design.
The current experience with a small defined populationencourages us to scale up the campaign involving all stakeholders and making the goggles available locally.
Acknowledgement: Dr. Samar K. Basak, Disha EyeHospitals, Barrackpore.
References:
1. Nirmalan PK, Katz J, Tielsch JM, Robin AL, ThulasirajRD, Krishnadas R, et al. Ocular trauma in rural southIndian population. The Aravind Comprehensive EyeSurvey. Ophthalmology 2004;111:1778-81.
2. Krishnaiah S, Nirmalan PK, Shamanna BR, SrinivasM, Rao GN, Thomas R. Ocular trauma in ruralpopulation of southern India: The Andhra Pradesh EyeDisease Study. Ophthalmolgy 2006;113: 1159-64.
3. Srinivasan M, Upadhyay B, Priyadarshini B, et al.Corneal ulceration in south-east Asia III: Preventionof fungal keratitis at the village level in south Indiausing topical antibiotics. Br J Ophthalmol 2006;90:1472-5.
4. Chatterjee S, Agrawal D, Sahu A, Dewangan D.Primary Prevention of Ocular Injury in AgriculturalWorkers with Safety Eye Wear. Proceedings of AIOC,2012.
5. Sil AK. Grain Found Growing in the Eye .CommunityEye Health 2000;13:32.
Volume 1, Issue 1, June 2014PPPPPaddy Grain Injuryaddy Grain Injuryaddy Grain Injuryaddy Grain Injuryaddy Grain Injury

CURRENT INDIAN EYE RESEARCH 33
Original Article — Ophthalmic ImagingOriginal Article — Ophthalmic ImagingOriginal Article — Ophthalmic ImagingOriginal Article — Ophthalmic ImagingOriginal Article — Ophthalmic Imaging
Retinal Vascular Caliber Measurement through Mahalanobis DistanceFunction based SegmentationSubhamoy Chatterjee1, Souvik Dasgupta2, Jyotirmoy Chatterjee3 , Sambuddha Ghosh2
1. Indian Institute of Astrophysics, Bangalore - 560 034, India; 2.Regional institute of Opthalmology, Kolkata -700 073, India. 3. Indian Instituteof Technology, Kharagpur-721 302, India.Corresponding Author : Dr. Subhamoy Chatterjee, E-mail: [email protected] on : 23/03/2014, Accepted on : 28/05/2014Conflict of Interest : None, Financial Disclosure : None
Abstract
Purpose: To measure retinal vascular caliber by image segmentation with training based on color image segmentation usingMahalanobis distance function. Method: cross-sectional observational study with 20 eyes of 10 normal individuals. Fundusphotographs were captured and processed for target feature segmentation using MATLAB R2008 a. Data matrices for all theclasses were built followed by calculation of mean and covariance matrix for respective classes. Subsequently, to segment outdifferent target classes from the fundus images, each pixel in the image was mapped to one of the classes giving minimum value ofMahalanobis distance. Optic disc was segmented out. Two circles were drawn at radial distances 0.5D (disc diameter)and 1Dfrom the boundary of the disc. Edge detection was performed through gradient calculation and vascular caliber was determinedusing two points marked on the walls of a vessel where they intersected the two concentric circles. Result: Average arterialdiameter was 147 ±16µm and average venous diameter was 168 ±22µm in our study population. Conclusion: Method usedin the present work relies on segmentation by manual marking of the pixels over different study classes to calculate their respectivecovariance matrices used in Mahalanobis distance function taking care of the correlation of different variables in the feature set.Thus the resulting segmentation determines the edges of the vessels properly which results in accurate computation of vessel width.
Computer image analysis involves segmentation inorder to detect objects to divide an image into regions
which can be considered homogeneous according to agiven criterion, such as shape, color, texture etc. Image isnot just a random compilation of pixels; it is a consequentialarrangement of regions and objects. Image segmentationinvolves dividing an image into different regions where eachregion is homogeneous. In retinal image processing forvasculature segmentation, there are algorithms forextraction of image ridges, which coincide approximatelywith vessel centerlines. Every line element comprises alocal coordinate frame for its corresponding patch andfeature vectors, for each pixel are calculated by propertiesof patches and line elements.
There are reports about other methods of image processinglike either 1-D or 2-D matched filters1, applied strategiesfor locating bifurcation, branches, estimating vesseldiameter and calculating angle geometry2, mathematicalmorphology and linear processing for vessel recognitionin noisy retinal images3, identification of bifurcation andretinal vasculature by both edges and regions4.
Mahalanobis Distance is a very useful way of determining
the similarity of a set of data points to an unknown. Itsadvantage over Euclidean distance is that it takes
b a
Fig. 1(a-b): Shows unlike Euclidean distance (1a) theMahalanobis distance (1b) takes care of the distributionof data. The (x1, x2) doublets are Gaussian distributed (graypatch) around mean vector (µ1, µ2) with standard deviation(σ1, σ2). The distribution can be expressed by f(x1,x2)=(1/(2*π* σ1* σ2))*exp[-0.5*{( x1 - µ1)/ σ1}^2-0.5*{(x2 -µ2)/ σ2}^2].Mahalanobis distance from (x1,x2) to class depicted by ((µ1,µ2), (σ1, σ2)) is given by twice the absolute value theexponent of the distribution i.e. {(x1 - µ1)/ σ1}^2+{( x2 -µ2)/σ2}^2 which is not same as Euclidean distance between(x1,x2) and (µ1, µ2) i.e. (x1- µ1) ^2+(x2 -µ2) ^2.Only samevalue of the distribution ensures same Mahalanobisdistances from respective points to class.

CURRENT INDIAN EYE RESEARCH34
distribution of the points (Fig. 1(a-b)) into account. It takesinto account not only the average value but also its varianceand the covariance of the variables measured. Itcompensates for interactions (covariance) betweenvariables. Also, it is dimensionless.
The aim of this study was to measure retinal vascularcaliber by image segmentation with training based on colorimage segmentation using Mahalanobis distance function.
Materials and Methods:
In this cross-sectional observational study betweenJanuary 2011 and June 2012, we studied for 20 eyes of10 normal individuals. Patients with refractive errors (> +2D or < -2 D ), hazy media, previous history of glaucomamedication and surgery, diabetes, hypertension, ischaemicheart disease, cerebrovascular accidents, peripheralvascular diseases, collagen vascular diseases,hyperlipidaemia, smoking habit and alcohol addiction wereexcluded from study. Fundus photographs were capturedby TRC 50 DX TOPCON camera at three angulations- 200,350 and 500. Fundus photographs were processed fortarget feature segmentation using MATLAB R2008 a.
Image segmentation: The preprocessed (histogramequalized) digital retinal fundus image was taken as input.The input image pixel RGB triplet was considered to bethe feature set for discrimination of four target classes inthe image viz. class 1 = optic disc(OD), class 2 = artery,class 3 = vein, class 4 = background. Using medical groundtruth, data matrices for all the classes were built followedby calculation of mean and covariance matrix for respectiveclasses. Subsequently, to segment out different targetclasses from the fundus images, each pixel in the imagewas mapped to one of the classes giving minimum valueof Mahalanobis distance (a statistical distance function:Di representing distance of data point x from ith class in 3-D RGB space) given by Di
2=(x-µi)TSi
-1(x-µi),where µi and Siwere the mean vector and covariance matrix for ith class;Si
-1 was the inverse of covariance matrix Si (a matrixconsisting of covariance of different pairs of variables alongoff diagonal positions and variances along diagonal).
OD was segmented out and its diameter (D) was measuredin terms of number of pixels using Euclidean distance (amathematical distance function which is used to calculatedistance between two points having n-dimensions inEuclidean space) between the OD centroid pixelcoordinates and boundary pixel coordinates i.e. optic discradius (D/2). Two circles were drawn at radial distances0.5D and 1D from the boundary of the disc. Segmentationof the background (i.e. class 4) was done and mergedwith OD segmented images. Edge detection was performed
through gradient calculation and vascular caliber wasdetermined using two points marked on the walls of avessel where they intersected the two concentric circles.Pixel to Pixel Euclidean Distance in mm = (D in mm/D no.of pixels)* Distance in no. of pixels, where D ~ 1.5mm.Usingartery and vein segmented images vessels of both kindswere identified on the OD and background merged images.Thereafter artery to vein caliber ratio was determined onthe mentioned circles.
Flow chart for image processing of retina
Segmentation of all four classes →Segmentation of class1and centre of optic disc was detected on that and discdiameter was measured→ Two circles were drawn at 0.5D and 1 D, radial distances from the boundary of the disc→Processing of the background (class 4) was completedand merged with optic disc images→ Edge detection donethrough gradient calculation→ Processed image is readyfor interpretation→The image result was opened withMATLAB R2008a Software for determination of vascularcaliber→ Two points were marked on two walls of a vessel,where they intersected by concentric circles→ Distance ismeasured in unit of pixel→ Pixel value is transformed in totrue diameter (in mm),by multiplying with converting factor.
Results:
Retinal images were segmented out using the abovementioned steps (Fig. 2a-c).
Average arterial diameter was 147 ±16µm and averagevenous diameter was 168 ±22µm in our study population.
Fig. 2a: Raw retinal image
Volume 1, Issue 1, June 2014 VVVVVasdcular Caliber Measurementasdcular Caliber Measurementasdcular Caliber Measurementasdcular Caliber Measurementasdcular Caliber Measurement
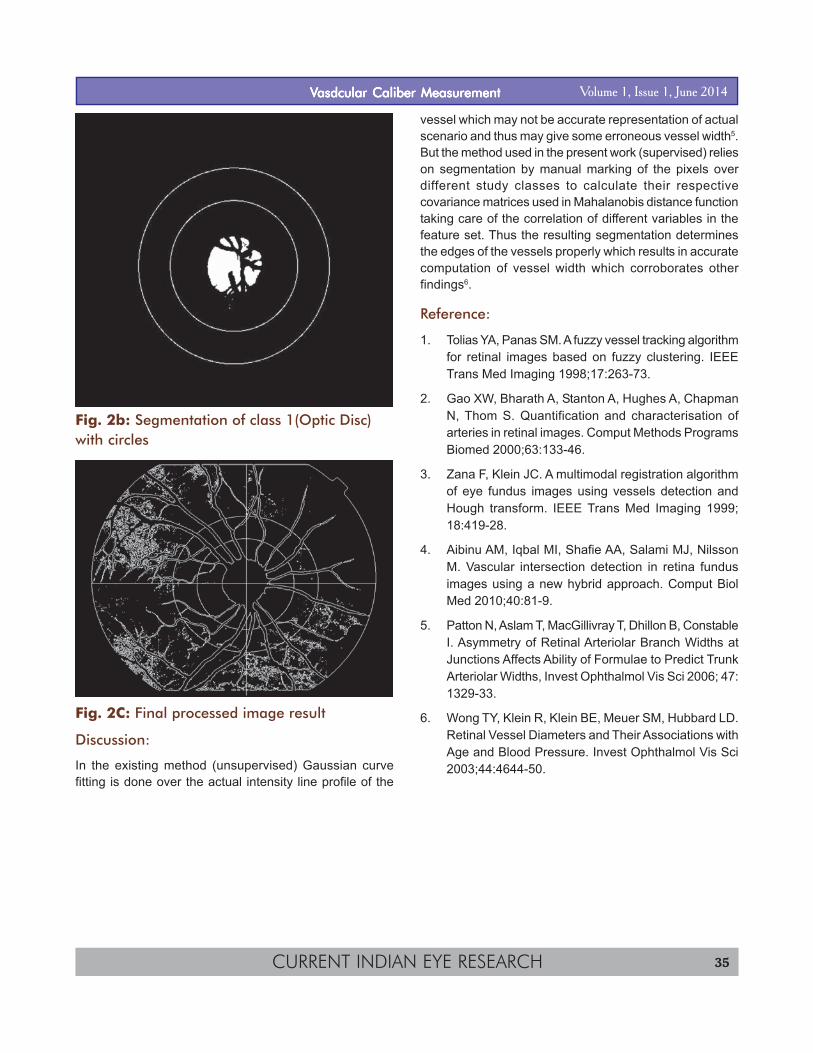
CURRENT INDIAN EYE RESEARCH 35
Fig. 2b: Segmentation of class 1(Optic Disc)with circles
Fig. 2C: Final processed image result
Discussion:
In the existing method (unsupervised) Gaussian curvefitting is done over the actual intensity line profile of the
vessel which may not be accurate representation of actualscenario and thus may give some erroneous vessel width5.But the method used in the present work (supervised) relieson segmentation by manual marking of the pixels overdifferent study classes to calculate their respectivecovariance matrices used in Mahalanobis distance functiontaking care of the correlation of different variables in thefeature set. Thus the resulting segmentation determinesthe edges of the vessels properly which results in accuratecomputation of vessel width which corroborates otherfindings6.
Reference:
1. Tolias YA, Panas SM. A fuzzy vessel tracking algorithmfor retinal images based on fuzzy clustering. IEEETrans Med Imaging 1998;17:263-73.
2. Gao XW, Bharath A, Stanton A, Hughes A, ChapmanN, Thom S. Quantification and characterisation ofarteries in retinal images. Comput Methods ProgramsBiomed 2000;63:133-46.
3. Zana F, Klein JC. A multimodal registration algorithmof eye fundus images using vessels detection andHough transform. IEEE Trans Med Imaging 1999;18:419-28.
4. Aibinu AM, Iqbal MI, Shafie AA, Salami MJ, NilssonM. Vascular intersection detection in retina fundusimages using a new hybrid approach. Comput BiolMed 2010;40:81-9.
5. Patton N, Aslam T, MacGillivray T, Dhillon B, ConstableI. Asymmetry of Retinal Arteriolar Branch Widths atJunctions Affects Ability of Formulae to Predict TrunkArteriolar Widths, Invest Ophthalmol Vis Sci 2006; 47:1329-33.
6. Wong TY, Klein R, Klein BE, Meuer SM, Hubbard LD.Retinal Vessel Diameters and Their Associations withAge and Blood Pressure. Invest Ophthalmol Vis Sci2003;44:4644-50.
Volume 1, Issue 1, June 2014VVVVVasdcular Caliber Measurementasdcular Caliber Measurementasdcular Caliber Measurementasdcular Caliber Measurementasdcular Caliber Measurement

CURRENT INDIAN EYE RESEARCH36
Case SeriesCase SeriesCase SeriesCase SeriesCase Series
Multilayered Amniotic Membrane Transplantation for Mooren's Ulcer –A Case Series of Ten PatientsJayanta Dutta1, Somnath Mukhopadhyay2, Himadri Datta1, Tamojit Chatterjee1
1. Regional Institute of Ophthalmology, Medical College, Kolkata, 88 College Street,West Bengal, India, Pin code: 700073, 2. Department ofOphthalmology, NRS Medical College, Kolkata, West Bengal, India.Corresponding Author : Dr. Jayanta Dutta, E-mail: [email protected] on : 24/02/2014, Revision Accepted on : 25/05/2014Conflict of Interest : None, Financial Disclosure : None
Abstract
Purpose: To examine the efficacy of amniotic membrane transplantation as a primary procedure in the treatment of Mooren'sulcer. Method: A total of 10 patients with primary Mooren's ulcer were treated by this method: none of the patients hadundergone any previous treatment for their ulcer. The ulcer in each of the 10 patients (10eyes) was treated with amniotic membranetransplantation. Separate amniotic membranes were transplanted (in lay) as material to fill the gap in the stromal layer (amnioticmembrane filling), as a basement membrane (amniotic membrane graft), and as a wound cover (amniotic membrane patch). In thepostoperative period all the patients were treated with topical antibiotics, topical steroids and artificial tear drops. Result: 7 eyes(70%)healed with epithelialization in (range,7 to 18 days) with 4 eyes showing corneal epithelialization and 3 eyes showingconjunctival epithelialization. 3 eyes showed persistent defect with no epithelialization and showed recurrence of ulcer on followup. Conclusion: Multilayered amniotic membrane transplantation is effective for treatment of deep ulceration of the cornea asoccurs in Mooren's ulcer.
Key words: Mooren’s ulcer, amniotic membrane, cyclosporine, keratoplasty
Mooren's ulcer is a chronic, painful, peripheralulcerative keratitis that was described as a clinical
entity by Mooren in 1867. It is characterised by progressive,crescentic, peripheral corneal ulceration that is slightlycentral to the corneoscleral limbus1. It is associated with acharacteristic extensive, undermined overhanging edge.It typically progresses with an anterior stromal yellowishinfiltrate at the advancing margin. An overlying epithelialdefect then develops followed by progressive stromalmelting. The ulcer progresses circumferentially andcentrally. The pathogenesis remains unknown but appearsto involve an autoimmune reaction against a specific targetmolecule in the corneal stroma which may occur ingenetically susceptible individuals. It is usually treated asa stepladder approach by local, systemic and surgicaltherapy. Local treatment includes topical steroids or topicalcyclosporin. Subconjunctival heparin injections and topicalcollagenase inhibitors have also been used2,3.
Systemic immunosuppresives are initiated if treatment withtopical therapy and conjunctival resection fails.
Surgical therapy include lamellar keratoplasty,epikeratoplasty, delimiting keratotomy, patch grafts ofperiosteum, fascia lata and amniotic membrane. Surgical
management for visual rehabilitation is a challenge;penetrating keratoplasty is usually associated with diseaserecurrence, graft rejection and melting4,5,6. In the presentseries we have used amniotic membrane transplantationas primary modality of treatment in all the 10 cases.
Amniotic membrane has long been used as a surgicalmaterial in this surgery. Amniotic membrane has a numberof indications, both as a graft to replace damaged ocularsurface stromal matrix and as a patch to decreaseinflammation.
Methods:
10 Patients (7 males and 3 females) with severe ulcerationof the cornea from Mooren's ulcer were treated withamniotic membrane transplantation. All the operations wereperformed by a single surgeon after obtaining informedconsent from the patient.
Amniotic membrane was obtained during caeserian sectionin donors who were sero-negative for hepatitis B, hepatitisC, syphilis and HIV. The amniotic membrane withunderlying chorion was washed in phosphate bufferedsaline containing 1mg/ml of dibekacin sulphate and bluntly
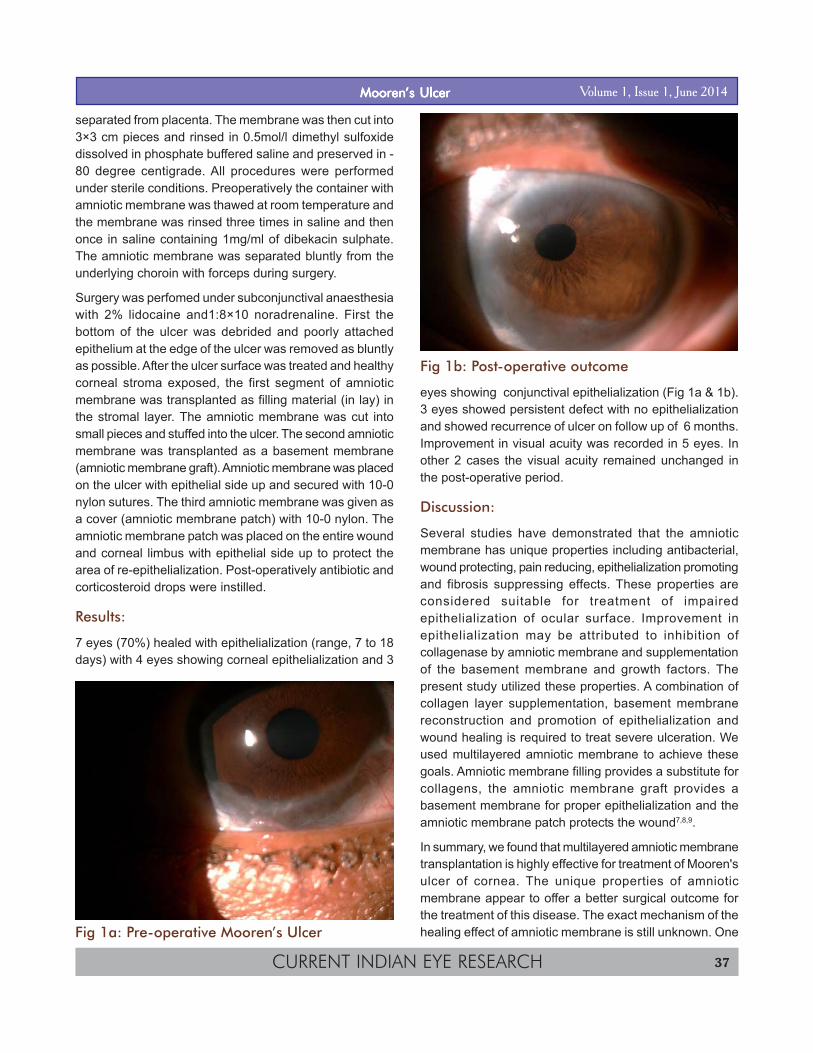
CURRENT INDIAN EYE RESEARCH 37
separated from placenta. The membrane was then cut into3×3 cm pieces and rinsed in 0.5mol/l dimethyl sulfoxidedissolved in phosphate buffered saline and preserved in -80 degree centigrade. All procedures were performedunder sterile conditions. Preoperatively the container withamniotic membrane was thawed at room temperature andthe membrane was rinsed three times in saline and thenonce in saline containing 1mg/ml of dibekacin sulphate.The amniotic membrane was separated bluntly from theunderlying choroin with forceps during surgery.
Surgery was perfomed under subconjunctival anaesthesiawith 2% lidocaine and1:8×10 noradrenaline. First thebottom of the ulcer was debrided and poorly attachedepithelium at the edge of the ulcer was removed as bluntlyas possible. After the ulcer surface was treated and healthycorneal stroma exposed, the first segment of amnioticmembrane was transplanted as filling material (in lay) inthe stromal layer. The amniotic membrane was cut intosmall pieces and stuffed into the ulcer. The second amnioticmembrane was transplanted as a basement membrane(amniotic membrane graft). Amniotic membrane was placedon the ulcer with epithelial side up and secured with 10-0nylon sutures. The third amniotic membrane was given asa cover (amniotic membrane patch) with 10-0 nylon. Theamniotic membrane patch was placed on the entire woundand corneal limbus with epithelial side up to protect thearea of re-epithelialization. Post-operatively antibiotic andcorticosteroid drops were instilled.
Results:
7 eyes (70%) healed with epithelialization (range, 7 to 18days) with 4 eyes showing corneal epithelialization and 3
eyes showing conjunctival epithelialization (Fig 1a & 1b).3 eyes showed persistent defect with no epithelializationand showed recurrence of ulcer on follow up of 6 months.Improvement in visual acuity was recorded in 5 eyes. Inother 2 cases the visual acuity remained unchanged inthe post-operative period.
Discussion:
Several studies have demonstrated that the amnioticmembrane has unique properties including antibacterial,wound protecting, pain reducing, epithelialization promotingand fibrosis suppressing effects. These properties areconsidered suitable for treatment of impairedepithelialization of ocular surface. Improvement inepithelialization may be attributed to inhibition ofcollagenase by amniotic membrane and supplementationof the basement membrane and growth factors. Thepresent study utilized these properties. A combination ofcollagen layer supplementation, basement membranereconstruction and promotion of epithelialization andwound healing is required to treat severe ulceration. Weused multilayered amniotic membrane to achieve thesegoals. Amniotic membrane filling provides a substitute forcollagens, the amniotic membrane graft provides abasement membrane for proper epithelialization and theamniotic membrane patch protects the wound7,8,9.
In summary, we found that multilayered amniotic membranetransplantation is highly effective for treatment of Mooren'sulcer of cornea. The unique properties of amnioticmembrane appear to offer a better surgical outcome forthe treatment of this disease. The exact mechanism of thehealing effect of amniotic membrane is still unknown. OneFig 1a: Pre-operative Mooren’s Ulcer
Fig 1b: Post-operative outcome
Volume 1, Issue 1, June 2014MoorenMoorenMoorenMoorenMooren’s Ulcer’s Ulcer’s Ulcer’s Ulcer’s Ulcer
CURRENT INDIAN EYE RESEARCH38
shortcoming of the present series is the lesser number ofpatients. Further studies with a larger number of patientsare needed to fully understand the mechanism of beneficialeffects of amniotic membrane in the treatment of Mooren'sulcer.
Reference:
1. Zaidman GW, Mondino BJ. Mooren's ulcer. In:KrachmerJH, Mannis MJ, Holland EJ, eds. CorneaText and Color Atlas CD-ROM. St. Louis: Mosby; 1998vol. II, V: 110.
2. Sangwan VS, Zafirakis P, Foster CS. Mooren'sulcer:current concepts in management. Ind JOphthalmol 1997; 45: 7-10.
3. Foster CS. Systemic immunosuppressive therapy forprogressive bilateral Mooren's ulcer. Ophthalmology1985; 92: 1436-9.
4. Martin NF, Stark WY, Maumenee AE. Treatment ofMooren's and Mooren's like ulcer by lamellar
keratectomy: report of six eyes and literature review.Ophthalmic Surg 1987; 18: 564-6.
5. Brown SI, Mondino BJ. Penetrating kerato-plasty inMooren's ulcer. Am J Ophthalmol 1980; 89: 255-8.
6. Lee SH, Tseng SCG. Amniotic membranetransplantation for persistent epithelial defects withulceration. Am J Ophthalmol 1997; 123: 303-12.
7. Solomon A, Meller D, Prabhasawat P, et al. Amnioticmembrane grafts for nontraumatic cornealperforations,descemetoceles, and deep ulcers.Ophthalmology 2002; 109: 694-703.
8. Prabhasawat P, Tesavibul N, Komolsuradej W. Singleand multilayer amniotic membrane transplantation forpersistent corneal epithelial defect with and withoutstromal thinning and perforation. Br J Ophthalmol2001; 85: 1455-63.
9. Chen KH, Hsu WM, Liang CK. Relapsing Mooren'sulcer after amniotic membrane trans-plantationcombined with conjunctival auto-grafting.Ophthalmology 2004;111:792-5.
Volume 1, Issue 1, June 2014 MoorenMoorenMoorenMoorenMooren’s Ulcer’s Ulcer’s Ulcer’s Ulcer’s Ulcer

CURRENT INDIAN EYE RESEARCH 39
Research MethodologyResearch MethodologyResearch MethodologyResearch MethodologyResearch Methodology
Multivariable AnalysisBijay Prasad Mukhopadhyay1
1. District Family Welfare Bureau, Darjeeling, West Bengal, India.Corresponding Author : Dr. Bijay Prasad Mukhopadhyay, E-mail: [email protected] on : 06/04/2014, Accepted on : 15/05/2014Conflict of Interest : None, Financial Disclosure : None
Is it absolutely essential to include multivariable analysisin one and all studies? The answer is “probably not”.
Here I have consciously excluded the term “certainly not”because there are many instances where multivariableanalysis helps a lot in analysis.
What is multivariable analysis? Multivariable analysis is atool to determine the relative contribution of different causesto a single cause. This, when I put in statistical term, Imention it as “simultaneously predicting a single outcome(dependant or response variable) from multiple factors(independent or predictor variables)”. This is importantbecause we live in multivariable world and most events,whether political, social or personal have multiple causes.Diseases also, as we know, are associated with multiplefactors. In fact any (pretty or large) event can be fit in thismodel of multiple factors versus single or multiple effector outcome (or response variable in statistical term).Though many researchers use multivariable andmultivariate analysis interchangeably, some hasreservation for using single outcome as multivariable andmultiple outcomes as multivariate analysis1.
Why multi variable analysis? Multi variable analysis isprobably a non absolute requirement in any analysis. It isso because we use this tool for addressing the third factor(which is also familiar by name “confounding”). There areother methods of tackling the third factors like stratification,randomization, matching and restriction besidemultivariable analysis. But every method has its ownadvantage and disadvantage and these choices are alsono exception. Stratification can not be done for a largenumber of variables (it gives huge number of permutationand combination tables which is difficult to digest, also topublish in journals). It is very useful to assess interaction(also known as effect modification). Randomization is anexcellent process for addressing the unknown confounders(in fact even in multivariable models also we can notaddress unknown confounders; but these are particularlyuseful in randomized controlled trials). In cases of serious
issues like use of anti-retroviral in post exposureprophylaxis, nobody would like to be randomized in nonanti retroviral group. Unless specially called for, unmatchedanalysis is easier and preferred; there may be some cryptomatching or over matching in some cases. Restriction isagain restricted to some individual consideration and thereis very little scope of including multiple variables at onetime.
One great advantage of multivariable analysis is that itunmasks the suppressive effects of any interaction andindicates an apparent insignificant association tosignificant. This was very clear in table provided by Hasdai,D. et al in table for comparison of bivariate and multivariableassociation between status and risk of death. Here abivariate analysis of smoking status and relative risk ofdeath2 were as follows (figures in the parenthesis 95%confidence interval): non smokers 1.0 ( ref), former smokers1.08 (0.92 – 1.26), recent quitters 0.56 (0.4 – 0.77) andpersistent smokers 0.74 (0.50 – 0.94). This apparently mayindicate that non smokers were at greater risk for deaththan other groups and smoking might had played aprotective role in prevention of death. But the actual factwas that, young age low BMI, low triglyceride levels, normalblood pressure etc all played the protective roles in thesmokers (suppressive interaction, in persistent smokersor in recent quitters where as non smokers and formersmokers were already at higher risk and probably leftsmoking because of those higher risks). When thosefactors were adjusted for known variables, the effect ofsmoking on risk of death was prominent: non smoker 1(ref), former smoker 1.34 (1.14 – 1.57), recent quitters 1.21(0.87 – 1.7) and persistent smoker 1.76 (1.37 – 2.26). Inrecent quitters risk included 1 in the confidence intervalsbut this could be due to wide confidence interval of a smallsample number in that sub strata. Similar effect could beseen in a study of Zidovudine use and sero conversion ofHIV infection in post exposure prophylaxis study wherethe interaction variable was the severity of injury. More

CURRENT INDIAN EYE RESEARCH40
seriously injured patients were more likely to useZidovudine and found it insignificant but when they areadjusted in the multivariable analysis model seroconversion becomes significant3.
What are the common uses of multivariable analysis?There may be variety of uses not only in the field of clinicalresearch but in other areas like marketing, sociology also.In clinical research there are four uses namely: (1)identification of prognostic factors while adjusting forpotential confounders like effect of low density lipoproteinon coronary artery diseases adjusting confounding effectsof other known risk factors of the same disease, (2) inadjusting base line characteristics variables inobservational studies (which is main type of study for mostof the public health post graduate students), (3) use inprognostic models which is particularly useful in estimatingsurvival periods of different lethal diseases like malignancy. There are some limitations and these models give validestimates of risk factors only in similar group of patientswhich in practice may not be same (biological variation).Similarly it may not be accurate in heterogeneous geneticmarker of cancer detections and (4) diagnostic modelthough scientifically sound, this is not favoured by cliniciansmainly because of uncertainty. The mathematicalexplanation is that all these models are based on probabilitycalculation and they are true only for a reasonably largenumber of trials. But in practice, we do not see that manysingle disease patients at a time. Moreover, the clinicianmay not like to accept even five percent failure in diagnosisfor a living human being, particularly in emergency.
What are the common types of multivariable analysis andwhere are they used? Are there any assumptions for aparticular type of multivariable analysis model to be true?Well, this is a vast matter to explain. In brief, there arethree types of analysis we commonly use: (1) Multiple linearregressions, (2) multiple logistic regressions and(3) proportional hazard analysis. In multiple linearregression, the outcome variable increases or decreasesin linear fashion (first order equation in index mathematicsor arithmetic progression) where as in multiple logisticregression, the logarithm of odds of outcome (odds meansprobability of an occurrence to the probability of nonoccurrence), also called 'logit', changes in linear fashionwith the independent variable. Like in any bacterial countstudy, the bacteriological count increase or decreases ingeometrical series pattern and it is then logarithmicallytreated to make the relationship linear. The proportionalhazard model has the similar logic like multiple regressions
where the logarithmic value of relative hazard (ratio of timeto outcome given a particular risk factor to the time tooutcome without the risk factor) changes in linear fashionwith unit change of interval independent variable. Hereone important consideration is tackling the censor cases(it is similar to tackling non responders in any study). Thereare several examples of studies which fit in these threemodels like diffuse linear association model showingassociation between Vitamin B12 level and pneumococcalantibody titer after pneumococcal vaccination, Z curves orS curve (or a simple Sine curve pattern and ultimatelylinear) association between skeletal muscle strength andpresence of cardiomyopathy among alcoholics. But onehas to remember, these are still models and the directionof the model at a particular point of time may not matchwith the ultimate direction of the model. Still these modelshave remarkable utility. It can be explained with one veryrelevant example. In a very lethal malignancy, ninetypercent patient may die within first two years with or withouttreatment. But after adjustment with multivariable model ifit is found that eighty percent die between one and halfand two years in the treatment group than only six monthsin the non treatment group it becomes very vital so far theindividual patients are concerned. Because one patientmay find very valuable time to arrange his / her daughter'smarriage or within that precious time gained; one may seethe smiling face of new born grand children. There are somany patterns of association found in these models likelogarithmic, anti logarithmic, U shaped, upside down Ushaped, J shaped, step ladder shaped etc. and theinterested readers are requested to look for referencebooks in the library or internet for that.
Some of the important issues which are to be taken intoconsideration for setting up multivariable model areestimation of sample size (it again depends on severalconsiderations like alpha error, beta error, dispersion withinpopulation or homogeneity of the population etc), selectionof the outcomes (preferably ten to twenty in some models),number of study subjects per each independent variable(preferably twenty or more), consideration of inclusion ofvariables (forward method), consideration of eliminationof variables (backwards method), omission of variables(depending on theory, measurement and experimentalmethods), combining multiple variables to single variablesor scale, consideration of the problems of factor analysisin the perspective of original variables (for example severalincome groups are lost to below median and above mediangroup in multiple logistic regression : some sorts of data
Volume 1, Issue 1, June 2014 Multivariable AnalysisMultivariable AnalysisMultivariable AnalysisMultivariable AnalysisMultivariable Analysis

CURRENT INDIAN EYE RESEARCH 41
loss). There are several methods of handling the missingvalues which are again beyond scope of this brief topic.Then there are considerations for calculation of cumulativesurvivals based on current survival or event rate (numberof outcome divided by the subjects at risk), conditionalprobability (1-event rate), loss to follow up, alternativeoutcome, withdraw etc.
Performing the analysis was critical in earlier days when abunch of formulae of “correlation, regression” were used.Now a days specially designed statistical or epidemiologicalsoftwares perform the analysis for the researcher.Nevertheless, when the researcher becomes familiar withthe concepts of multivariable analysis, not only that s/heunderstands the method in the computer but alsopossesses a grip to interpret the results so obtained throughthe software. The pleasure is like matching the correct
answer with a long struggling difficult problem solvinganswer in a puzzle. For these softwares, manuals are alsoavailable with the special softwares.
Reference:
1. Mitchell H K. In:Multivariable analysis: a practicalguide for linicians and public health researchers. 3rdEd. Cambridge University Press; 2011.pp2.
2. Hasdai D, Garratt KN, Grill DE, Lerman A, HolmesDR Jr. Effect of smoking status on the long termoutcome after successful percutaneous coronaryrevascularization. N Engl J Med 1997; 755-61.
3. Cardo DM, Culver DH, Ciesielski CA, et al. A case -control study of HIV sero conversion in health- careworkers after percutaneous exposure. N Eng J Med1997; 337:1485 – 90.
Volume 1, Issue 1, June 2014Multivariable AnalysisMultivariable AnalysisMultivariable AnalysisMultivariable AnalysisMultivariable Analysis

CURRENT INDIAN EYE RESEARCH42
CommentaryCommentaryCommentaryCommentaryCommentary
Ophthalmology beyond Ophthalmologists and Also IncludingOphthalmologistsGarga Chatterjee
Abstract
Ophthalmology stands in close relationship with other branches of medical science, but the linkages of ophthalmology have longbeen with disciplines beyond conventional medicine. Project Prakash in the department of Brain and Cognitive Sciences of theMassachusetts Institute of Technology identifies congenitally but curably blind children in India who have so far remained untreateddue to poor medical access. The Prakash studies have yielded evidence of significant adverse effects of congenital blindness onsome aspects of post-operative vision, but also impressive visual skill acquisition by those who gain their sight even after severalyears of blindness.
Keywords: ophthalmology ; vision science ; blindness
Computer Vision and Pattern Recognition Unit, Indian Statistical Institute, Kolkata 700108, West Bengal, India.Corresponding Author : Dr. Garga Chatterjee, E-mail: [email protected] on : 15/05/2014, Accepted on : 05/07/2014Conflict of Interest : None, Financial Disclosure : None
Clinical ophthalmology is a discipline with a long andglorious past that has served mankind admirably. The
implications of ophthalmological research are enormous;its translation potential has been life changing for much ofhumanity. Imagine life today in the absence of intra-ocularlenses (IOL) and we will appreciate what I am talking about.
However, ophthalmology today does not stand in isolationto other bodies of knowledge. I would argue, it never hasbeen in the case in the past either. It is obvious thatophthalmology stands in close relationship with otherbranches of medical science, but the linkages ofophthalmology have long been with disciplines beyondconventional medicine. Consider the IOL example providedabove. It could not have been developed without the closeinteraction between material science and ophthalmology.The demonstration of its efficacy needed epidemiologicalknowledge. Note that I did not mention specialists likeophthalmologists, material scientists, epidemiologists, etcbut disciplines like ophthalmology, material science,epidemiology and so on. I will return to the significance ofthis distinction.
Ophthalmology today closely interacts with vision sciencewhich cuts through various disciplines like “psychology(more specifically sensation and perception psychology,cognitive psychology and psychophysics), neuroscience,physics (specifically optics) and computer science (morespecifically computer vision, artificial intelligence, and
computer graphics), as well as practical applications suchas data visualization, user interface design, and humanfactors and ergonomics1.” With these kinds of interactions,certain kinds of collaborations and research have takenplace whose success bear testimony to the value of suchinterdisciplinary knowledge and methods. Let me illustratethis point using the example of a research initiative I havebeen personally involved with.
Project Prakash was born in the department of Brain andCognitive Sciences of the Massachusetts Institute ofTechnology and was conceived by a scientist (PawanSinha) whose original training was in Computer Scienceand Artificial Intelligence.
‘The Prakash initiative identifies congenitally but curablyblind children in India who have so far remained untreateddue to poor medical access2.’ The two major kinds oftreatable childhood blindness in India are cataracts andcorneal opacities. ‘By providing such children correctivesurgery, Project Prakash is creating a population of childrenacross a wide age range who are just learning how to see.Longitudinal studies of these unique children offer insightsinto how they develop visual skills. This approach combinesthe best of both worlds: it directly addresses the pressinghumanitarian need to treat curably blind children and, inthe process, illuminates fundamental questions regardingbrain plasticity and learning2. Till date, Project Prakash hasbeen able to screen over 40,000 children (primarily in rural

CURRENT INDIAN EYE RESEARCH 43
North India) and has provided surgical treatment to over400 of them as well as non-surgical care to over 1,400individuals.
What has been the research impact of this project? Toquote a recent paper summarizing its results -‘The Prakashstudies have yielded evidence of significant adverse effectsof congenital blindness on some aspects of post-operativevision, but also impressive visual skill acquisition by thosewho gain their sight even after several years of blindness.We have investigated how patients acquire many aspectsof visual function, including low-level attributes such asacuity and contrast sensitivity as well as high-levelfunctions such as object and face recognition and spatialimagery. This work has also demonstrated how motioninformation plays a crucial role in parsing the world intodistinct objects and, more importantly, in helping the visualsystem learn heuristics that can be used even with staticimages. The results have guided our studies of normallysighted individuals, as well as our computational modelingefforts. Complementing our behavioral studies, we havebegun to employ non-invasive brain imaging technology,specifically functional magnetic resonance imaging (fMRI),to examine the kinds of cortical changes that accompanythe very initial stages of human sensory development.These neuroimaging studies so far have revealed that theonset of patterned visual information results in rapidmodification of the visual cortex even in individuals whohave been congenitally blind for the first two decades oftheir lives2.’
The Project Prakash team consists of a variety ofindividuals which include ophthalmic surgeons specializingin paediatric ophthalmic surgery, optometrists withexperience in rural field testing, social workers with goodpublic relation skills, sensitive nursing staff, computerscientist who now is an world-acclaimed neuroscientist,
low vision researcher, medical doctor turned visionscientist, biomedical engineer turned vision scientist, andothers. Being one of the above-mentioned people, I cannow understand how each member is integral to theexecution of the project. It is also important howophthalmologists in the project are simply not ‘surgeryproviders’ or ‘diagnosis providers’ to the scientists butimportant part of the scientific conceptualization of theproject. In medical science, clinicians are often ‘serviceproviders’ or even worse, ‘sample’ or ‘patient’ providers.Clinicial scientist is quite a different idea. Project Prakashand various other such projects bring this idea to life.
Now let me return to the point that I had promised I wouldtake up. I had mentioned interacting disciplines and notpeople because the essence of collaborative science liesin people coming together with their core competenciesbut also learning what needs to be learned so that eachperson becomes a repository of interdisciplinaryknowledge. Thus, the ophthalmologist strives to understandin some depth the material science or the visualneuroscience or epidemiology. The idea is to become apart master of multiple trades with a core competency. Thisalso points to the direction of future ophthalmology wherethe advances will come not only from ophthalmologistsbut also from people trained originally in other disciplinesand from enthusiastic ophthalmologists who have thecourage and zeal to wear multiple hats.
References:
1. Palmer, S. E. (1999). Vision science photons tophenomenology. Cambridge, Mass.: MIT Press
2. Sinha P, Chatterjee G, Gandhi T, Kalia A. (2013).Restoring Vision through “Project Prakash”: TheOpportunities for Merging Science and Service. PLoSBiology, e1001741.
Volume 1, Issue 1, June 2014

CURRENT INDIAN EYE RESEARCH44
History of OphthalmologyHistory of OphthalmologyHistory of OphthalmologyHistory of OphthalmologyHistory of Ophthalmology
Famous Ophthalmologists Who Suffered from Eye DisordersDebmalya Das
Abstract
Ophthalmologists with eye disorders were many but they seldom came out in open or reported about their diseases to maintainprivacy and to maintain his /her practice in the society. However, these ocular conditions prompted them to experiment with variousmedicines or surgeries to counter the ill effects of the diseases often leading to discoveries of newer modes of management. Wereview three such famous ophthalmologists whose eye disorders were reported and were subjected intense debate in the ophthalmologyfraternity.
Key-words: Ophthalmologist, eye disease, glaucoma.
Ophthalmologists with eye disorders were many butthey seldom came out in open or reported about their
diseases. Most of the time an Ophthalmologist hid his /hersystemic and ocular problem to maintain privacy and tomaintain his /her practice in the society. However, theseocular conditions prompted them to experiment with variousmedicines or surgeries to counter the ill effects of thediseases often leading to discoveries of newer modes ofmanagement. Cataract, strabismus and refractive errorswere common amongst ophthalmologists but were seldomreported. Glaucoma, often angle closure, was the mostcommonly reported eye disease amongst ophthalmologistsas it forced an ophthalmologist to seek another's opinion,required a long term follow up and often surgicalintervention was necessary. We review three such famousophthalmologists whose eye disorders were reported andwere subjected intense debate in the ophthalmologyfraternity at that time.
One such was Alexander Pagenstecher (1828-1879),famous for introducing yellow mercury oxide ointment formanaging external eye diseases, which bears his name.His papers were mainly concerned with sympatheticophthalmia, the indications for enucleation, iridodesis,glaucoma and cataract. He was instrumental in introducingintracapsular cataract extraction as the primary treatmentof cataract having personally performed more than 2000cataract operations. In 1878, he had an acuteglaucomatous attack in the right eye and was immediatelyoperated on by his brother, Hermann, who performed a
Aditya Birla Sankara Nethralaya, 147, Mukundapur, E.M.Bypass, Kolkata-700 099, West Bengal, India.Corresponding Author : Dr. Debmalya Das, E-mail: [email protected] on : 05/05/2014, Accepted on : 30/06/2014Conflict of Interest : None, Financial Disclosure : None
complete iridectomy. No visual deficit remained. The longterm effect, however couldn't be ascertained asPagenstecher died shortly thereafter from an unusualhunting accident1.
Ludwig Laqueur (1837-1909) introduced physostigmine asa medical treatment for glaucoma. Since childhood he wasred-green color blind, was photophobic and suffered fromchronic recurrent conjunctivitis for which he used a 1.5%silver nitrate solution1. At the age of 30, prodromal signs ofan angle closure glaucomatous attack started. In his paper2,he vividly described these attacks and stated that theattacks were triggered by emotions or when in the theatreand resulted in cloudy visions. He also noticed that withPhysostigmine, a calabar bean extract, he was able torepeal the attack every time but recurrences were commonand became very frequent. Hence, total iridectomise wereperformed in both the eyes by Horner. Although, the surgeryprevented any further attack or progression of visual loss,the large surgical colobomas, which were visible to thenaked eye made Laqueur photophobic and extremely self-conscious1.
Louis-Emile Javal (1839-1907) is often called 'the Fatherof Orthoptics'3. His contribution to strabismus wasimmense. He was also instrumental in designing the Javal-Schiøtz ophthalmometer. He was earlier an engineer butbecame interested in strabismus because his father andsister both had squint. Since childhood, he had a highdegree of astigmatism, chronic conjunctivitis andheterochromia4. In 1881, he noticed the first attack of an
CURRENT INDIAN EYE RESEARCH 45
acute glaucoma in his right eye. However, treatment startedlate and he became legally blind in right eye in 1886. Thefirst prodromal signs in the left eye appeared 1885 andwas not operated till 1900. But the surgeries couldn't arrestthe disease progression and he became blind in left eye in1901. Right eye was enucleated in 1901. Too frequentchanging of ophthalmologists, non-compliance on part ofJaval, delaying necessary operations and too manysurgeries in a short span had been attributed to the loss ofvision in the left eye5. The blind Javal invented an armrestwith a cogwheel device advancing the writing paper by 1cm at the end of each line. This 'planchette scotographique'could be used by blind persons to write ordinary script.
References:
1. Blodi FC. Prominent ophthalmologists who sufferedfrom acute glaucoma Documenta Ophthalmologica1994; 86: 111-22,.
2. Laqueur L. Geschichte meiner Glauko-merkrankung.Klin. Monatsbl. f. Augenhk 1909; 47(1):639.
3. Revell MJ. Strabismus: A History of OrthopticTechniques. London: Barrie and Jenkins; 1971, p.15.
4. Roper-Hall G. Historical Vignette: Louis Émile Javal(1839–1907): The Father of Orthoptics. AmericanOrthoptic Journal 2007; 57: 131-6
5. Jacobson J. Briefe an Fachgenossen (MargaretheQuidde, editor), Königsberg 1899, p.10.
Ludwig Laqueur (1837-1909)Alexander Pagenstecher(1828-1879)
Louis-Emile Javal(1839-1907)
Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH46
AUTHOR GUIDELINES
Manuscripts must be prepared in accordance with "Uniformrequirements for Manuscripts submitted to BiomedicalJournals" developed by the International Committee ofMedical Journal Editors (October 2004).The manuscripts will be reviewed for possible publicationwith the understanding that they are being submitted toone journal at a time and have not been published,simultaneously submitted, or already accepted forpublication elsewhere.Manuscripts will be sent for peer review.Articles accepted would be copy edited for grammar,punctuation, print style, and format.
Types of manuscripts and limits
• Review article: The limit of text is up to 3500 wordsexcluding about 70 references and abstract.
• Original article: The limit of the text is up to 3000 wordsexcluding about 50 references and structured abstractup to 250 words. This section will publish clinical,experimental and community reports.
• Research methodology: This includes educativearticles related to the conduct of research with wordcount up to 2000 and references up to 30.
• Case report: The limit is up to 1000 words excludingreferences and abstract with a maximum of 10references.
• Letter to the Editor: up to 500 words and 5 references.
• History of Ophthalmology: Up to 1000 words and 10references
Authorship credit should be based only on substantialcontributions1. Conception and design or acquisition of data or
analysis and interpretation of data;2. Drafting the article or revising it critically for important
intellectual content;3. Final approval of the version to be published.When you submit an article, the following items must beincluded.1. The covering letter2. Article file: Use doc files. Do not zip the files. Do not
incorporate images in the file. The first page will beTitle Page. All information which can reveal youridentity should be hereProvide the highest degree andinstitution of each author, Phone number and email
address of corresponding author. Also includesource(s) of support, acknowledgement, if themanuscript was presented earlier.
3. Images: Preferably black and white images. Colorimages will be considered if absolutely necessary.Image format jpeg/tiff is acceptable. Do not zip thefiles.
4. Legends: Legends for the figures/images should beincluded at the end of the article file.
The language should be American English.The text should be divided into sections with the headings:Abstract, Key-words, Introduction, Material and Methods,Results, Discussion, References, Tables and Figurelegends. Use double spacing throughout. Number pagesconsecutively, beginning with the title page.The contributors' form has to be submitted with thesignatures of the corresponding author at the time ofsubmission via e-mail as a scanned image.Clearance from ethics committee should be mentioned inmethod section. When informed consent has beenobtained, it should be indicated in the article.
ReferencesReferences should be numbered consecutively in the orderin which they are first mentioned in the text (not inalphabetic order). Identify references in text, tables, andlegends by Arabic numerals in superscript before thepunctuation marks. The titles of journals should beabbreviated according to the style used in Index Medicus.Use complete name of the journal for non-indexed journals.Reference style:Journal article: Vinekar A, Dogra MR, Sangtam T, NarangA, Gupta A. Retinopathy of prematurity in Asian Indianbabies weighing greater than 1250 grams at birth: Ten yeardata from a tertiary care center in a developing country.Indian J Ophthalmol 2007;55:331-6.Incase of more than six authors, list the first threecontributors followed by et al.Chapter in a book: Phillips SJ, Whisnant JP. Hypertensionand stroke. In: Laragh JH, Brenner BM, editors.Hypertension: pathophysiology, diagnosis, andmanagement. 2nd ed. New York: Raven Press; 1995. pp.465-473.
Processing fee : NilArticle to be sent by email only to:
Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH 47
CONTRIBUTOR'S FORM
Manuscript Title: ...................................................................................................................
While submitting this article to Current Indian Eye Research for publication, I certifythat I/we have participated sufficiently in the intellectual content, conception and design ofthis work or the analysis and interpretation of the data (when applicable), as well as thewriting of the manuscript, to take public responsibility for it and have agreed to have my/ourname listed as a contributor. I/we believe the manuscript represents valid work. Neither thismanuscript nor one with substantially similar content under my/our authorship has beenpublished or is being considered for publication elsewhere. I certify that all the data collectedduring the study is presented in this manuscript and no data from the study has been or willbe published separately. I/we attest that, if requested by the editors, I/we will provide thedata/information or will cooperate fully in obtaining and providing the data/information onwhich the manuscript is based, for examination by the editors or their assignees. Financialinterests, direct or indirect, that exist or may be perceived to exist for individual contributors inconnection with the content of this paper have been disclosed .Corresponding author hasbeen assigned by the co authors to make necessary changes as per the request of the journal,do the rest of the correspondence.
All persons who have made substantial contributions to the work reported in the manuscript,but who are not contributors, are named in the Acknowledgment and have given me/us theirwritten permission to be named. If I/we do not include an Acknowledgment that means I/wehave not received substantial contributions from non-contributors and no contributor has beenomitted. The order of authors has been mutually agreed upon by all co authors.
Name Signature Date
(Corresponding author)
Volume 1, Issue 1, June 2014
CURRENT INDIAN EYE RESEARCH48
Volume 1, Issue 1, June 2014



























