Embed Size (px)
Citation preview



www.heartpartners.com 3
features
ContentsVolume 1 • Issue 1HeartLines:TRENDS IN HEART ANDVASCULAR DISEASE
departments
DIAGNOSTICS AND TREATMENT
Going Beyond the HeartStent and Angioplasty Procedures Provide Global Vascular Benefits ..................7
Advancing TreatmentsThe Changing Paradigm in Coronary Artery Disease ................................................8
HEALTH CARE PRINCIPLES
Getting to the Heart of ThingsCardiology Center Focuses on All Aspects of Cardiovascular Care .................13
Know the Law Examining Critical Regulations Governing Medical Practices ..............................19
REPORTS
Heart Failure Guidelines Update Offers Effective Treatments ...............................................................................24
The Future of Medical Care Electronic Medical Records Benefit Both Patient and Physician ........................26
Evaluating SyncopeEtiology, Diagnosis, and Treatment ................................................................................10
Proper Application of Pacer TechnologyExploring New Paradigms in Cardiac Pacing..............................................................14
New Treatment Options for Venous DiseaseEvaluating Varicose Veins and Venous Insufficiency .................................................22
HeartLines: Trends in Heart and Vascular Disease is published by QuestCorp Media Group, Inc., 885 E. Collins Blvd., Ste. 102, Richardson, TX 75081. Phone (972) 447-0910 or (888) 860-2442, fax (972) 447-0911,www.qcmedia.com. QuestCorp specializes in creating and publishing corporate magazines for businesses. Inquiries: Victor Horne, [email protected]. Editorial comments: Brandi Hatley, [email protected]. Pleasecall or fax for a new subscription, change of address, or single copy. Single copies: $5.95. This publication may not be reproduced in part or in whole without the express written permission of QuestCorp Media Group, Inc.QC Creative is a full-service graphic design firm, www.qccreative.com. Creative services inquiries: Todd Hagler, [email protected].
10 24

HeartLines Trends in Heart and Vascular Disease4
Judah Friedman, MEd, MBA:Chief Executive Officer
Tracie Santana:Director of Administration
Jorge Diaz-Kropman, BSIT:Director of Medical Information Systems
Michelle Crowley:Office Manager
HeartLines:TRENDS IN HEART ANDVASCULAR DISEASE
Welcome
HeartLines is an educational magazinepublished by Cardiovascular Consul-tants of South Florida to introduce ourstaff and facilities as well as com-municate educational news and trendsinvolving cardiovascular diseases andtreatments as well as other articles ofinterest. The biannual publication is aimedat physicians throughout South Florida,as well as employer groups and otherinfluential members of our community.
LOCATIONS:
Corporate Office3335 N. University Dr., Ste. 8Davie, FL 33024(954) 965-4900
Hollywood1150 N. 35th Ave., Ste. 605Hollywood, FL 33021(954) 981-3331 • (954) 981-4659 Fax
Pembroke Pines603 N. Flamingo Rd., Ste. 225Pembroke Pines, FL 33028(954) 437-9116 • (954) 433-9734 Fax
Weston1855 N. Corporate Lakes Blvd.Weston, FL 33326(954) 981-3331 • (954) 981-4659 Fax
Aventura21150 Biscayne Blvd., Ste. 106Aventura, FL 33180(305) 933-2121
www.heartpartners.com
A publication fromt gives us great pleasure to welcome you to the inaugural issue ofHeartLines: Trends in Heart and Vascular Disease. Since our groupformed 10 years ago, our name has remained South Broward Cardi-
ology Consultants, and we have continued to provide premier cardio-vascular medical services to Broward County. In reality, however,we have a following all over South Florida, where we have taken thelead in vascular disease interventions. To reflect this expansion, we are
changing our name to Cardiovascular Consultants of South Florida (CCSF). With 16 full-time physicians, including noninvasive and invasive cardiologists, elec-
trophysiologists, and vascular medicine specialists, we are one of the largest cardio-vascular groups in Florida. Many of our physicians have practiced here for years. Infact, our invasive cardiologists have performed more than 25,000 procedures atMemorial Regional Cardiac Catheterization Laboratory since it opened under ourdirection more than a decade ago.
Because it makes sense to consider the heart and blood vessels as one system, ourcenter recently incorporated a vascular program that emphasizes the nonsurgicaltreatment of peripheral vascular disease. Our registered vascular technicians use thenewest in vascular diagnostic equipment, providing diagnostic testing for carotid,abdominal, and extremity disorders.
Our recent additions to the group include Raul Mitrani, MD, cardiac electrophysiol-ogist, former associate professor at University of Miami School of Medicine,and Director of the Arrhythmia and Syncope Center at Jackson Memorial Hospital.Also joining us is Juan Pastor-Cervantes, MD, cardiac and vascular interventionalist,who completed a post-fellowship in peripheral vascular interventions at the renownedCardiovascular Institute of the South. He joined us last year after spending a yearon the University of Miami School of Medicine faculty. Dr. Pastor-Cervantes was alsorecently named National Spokesperson for Cordis’s Healthy from the Heart program.Susan B. Fox, DO, vascular medicine specialist, was fellowship trained at The ClevelandClinic and is board certified in vascular medicine. She joined our group this year, alongwith John Cogan, MD, who is board certified in cardiac electrophysiology.
Members of our staff have worked as chiefs of cardiology and medicine. At this time,Howard Berlin, President of CCSF, serves on the Institutional Review Board forMemorial Regional Hospital. Dr. Mitrani is Director of Electrophysiology for theMemorial Healthcare System. Jose Guzman, MD, is Chief of Medicine at MemorialMiramar, and Michael Braun, MD, sits on the Medical Executive Committee atAventura Hospital.
In the past, our group distributed a Heartlines newsletter to all our patients with afocus on varying topics in cardiovascular disease. Last year’s newsletter is available forviewing and download at www.heartpartners.com. This year, we decided to start amagazine for physicians in our area, highlighting important topics we hope you willfind informative. We welcome your comments and questions. Feel free to e-mailHeartLines Editor Dr. Raul Mitrani with feedback at [email protected].
We thank the organizations that have partnered with us to make this publicationpossible. Each one is actively involved on some level with our group and was chosento join us on this project.
Enjoy!
Judah Friedman, MEd, MBA, Chief Executive Officer
I

www.heartpartners.com 5

HeartLines Trends in Heart and Vascular Disease6

www.heartpartners.com 7
DIAGNOSTICS AND TREATMENTBY JUAN A. PASTOR-CERVANTES, MD
ver the last 50 years, technologicaladvances in treating cardiovasculardiseases have allowed patients to
live longer and better lives. In the mid-1960s, for example, researchers developeda revolutionary concept — the coronarybypass — for patients with severe coro-nary disease. The advent of this techniquemarked a huge step forward in caring forthese individuals. In the mid-1970s,another landmark breakthrough hap-pened: the balloon angioplasty procedure.
Today, after years of hard work anddedication developing new techniques,physicians use minimally invasive cardio-vascular interventions to treat mostpatients, shifting away from the old stan-dard of performing surgery to correct coro-nary or peripheral artery blockages. Nowmore than one million coronary angioplas-ties are performed annually in the UnitedStates, compared to 300,000 surgeries, toimprove blood flow to the heart muscle.
Coronary Stent Advances
Over the last 15 years, physicians haveused coronary stents to improve outcomesfor coronary angioplasties. But moreimportantly, over the last two years, wehave begun implanting medicated stents,better known as drug-eluting stents. Thisadvance has improved results so less thanone in 10 patients returns for further treat-ments in the area of the stent implant.
Studies comparing the use of angioplastyand medicated coronary stents to coronarybypass surgery have found in favor of thecoronary stent technique. Patients receiv-ing the stents were much less likely to sufferdebilitating or fatal heart attacks or strokesin the first year after their procedures. Alsowith the stents and angioplasty, only threepatients in 100 returned in the first year forcorrection of a reblocked artery.
Stent and Angioplasty Success inOther Areas
Physicians have demonstrated similarsuccess using angioplasty and stentsto treat carotid arteries. Traditionally,carotid artery endarterectomy is the firstchoice to treat blockages in these vessels.Over the last few years, however, it wasproven that carotid artery stenting withembolic protection devices (filters thattrap clots during the stent implantation) isthe best way to treat high-risk surgical
patients. Soon we hope to show thisapproach is the best choice for all patientswith carotid artery problems.
Stents have allowed patients to avoidother high-risk surgeries, such as subcla-vian artery bypass, abdominal aorticaneurysm resection, renal artery bypass,and celiac trunk or mesenteric arterybypasses. These lower-risk procedurestypically produce better results andrequire shorter hospital stays (usually lessthan 24 hours).
Intermittent claudication is another areawhere stents and angioplasties are beingused more commonly. With this condition,patients have blockages of the arteries thatprovide blood to the legs. The incapaci-tating disease can gradually decrease bloodflow to such a degree that the limb needs tobe removed. Severely diminished circula-tion to the extremities is responsible formore than 150,000 amputations in ourcountry every year. Sadly, fewer than 30%of these patients return to their normalfunctioning after the amputation. The useof stents and angioplasties, however, canhelp restore blood flow and reduce the inci-dence of amputation in many instances.
Moving Ahead
As a physician, I am a firm advocate ofensuring my patients clearly understandtheir conditions and the possible coursesthey may take. I am also a firm believer inmaking patients aware of all treatmentoptions available to them, including thelatest advances in medical techniques andtechnology. Physicians are continuallyworking to develop devices, like the med-icated stents, and procedures, like balloonangioplasties, that achieve better out-comes with less risk, less pain, and shorterrecovery times for patients. The encourag-ing results for stents and angioplasties arejust one example of how the search forthe best treatment approach is movingforward every day. ■
Juan A. Pastor-Cervantes, MD, FACC, is a gradu-ate of Universidad La Salla School of Medicine,Mexico City, Mexico. He completed an internship,a residency, and cardiology and interventionalcardiology fellowships at the University ofMiami’s Jackson Memorial Hospital. Dr. Pastor-Cervantes has worked as an interventional cardi-ologist and a peripheral vascular interventionalist,as well as Assistant Professor of Medicine at theUniversity of Miami School of Medicine.
O
Going Beyond the HeartStent and Angioplasty Procedures Provide Global Vascular Benefits
More than one million coronary angioplasties areperformed annually in the United States, com-pared to 300,000 surgeries, to improve bloodflow to the heart muscle.

HeartLines Trends in Heart and Vascular Disease8
DIAGNOSTICS AND TREATMENT
here are many exciting new advan-ces in the diagnosis and treatment ofcoronary artery disease (CAD),
which is also known as atherosclerosis(“hardening”) of the coronary arteries.These arteries supply blood back to theheart muscle. The past 25 years have seenmajor advances from the days of difficultdiagnosis and very little treatment ofthis disease.
For instance, there is the recognitionof much lower limits of “normal” bloodpressure and serum cholesterol with infor-mation obtained from the FraminghamHeart Study. The ongoing Framinghamstudy follows numerous parameters such asblood pressure and cholesterol levelsof the population of Framingham,Massachusetts, over several decades.
Defining Normal Pressure
Normal blood pressure is no longerconsidered a patient’s age plus 100. Today,normal blood pressure is considered less
than 120/80 (systolic/diastolic). In addition,it is now recognized that both the systolicand diastolic pressures are important.Prehypertension is now defined as a systolicpressure 120 to 139 or a diastolic pressure80 to 89.
Total cholesterol was previously consid-ered normal up to 300. It is now knownthat ideal total cholesterol is less than200; and there are many important frac-tions of the total cholesterol that weneed to evaluate, including high-density
lipoprotein (HDL, the good cholesterol)and low-density lipoprotein (LDL, thebad cholesterol). High cholesterol is animportant CAD risk factor. However,80% of patients who develop CAD havethe same cholesterol values as those whodo not develop the disease.
Now physicians can look not only attotal cholesterol, HDL, LDL, and triglyc-erides, but with information from theBerkeley HeartLab, we can also evaluatesubfractions of HDL and LDL, Lp(a), and
T
BY FRANK J. PEARL, MD, FACC, FCCP, FACP
Advancing TreatmentsThe Changing Paradigm in Coronary Artery Disease
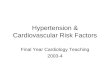
Cardiac catheterization, shown in this image withtwo typical entry points — popliteal and femoral,is no longer used just for diagnosis.
In the Forefront of Advanced TechniquesCholesterol Tests Lead to Better CAD Diagnosis
For decades, cholesterol has been arecognized major risk factor for coronaryartery disease (CAD). Millions of Americanswatch their diets, exercise, or take choles-terol-lowering medications to reduce therisk of life-threatening heart attacks. How-ever, approximately half of the 1.5 millionheart attacks occurring each year affectpeople with “normal” cholesterol tests.
Fortunately, new refined diagnostic toolsare becoming available in South Floridathat can provide a more accurate assess-ment of an individual’s heart attack risk.
“The average cholesterol profile todaydoesn’t adequately address risk issues,”says Frank J. Pearl, MD, FACC, FCCP,FACP, a board-certified cardiologist withCardiovascular Consultants of SouthFlorida. “It takes more sophisticated labo-ratory testing and new diagnostic tools.”
Dr. Pearl notes that hypertension (highblood pressure) and cholesterol areamong the key risk factors for heartattacks, along with smoking and geneticfactors. The big news is the release of newstudies that foster advanced medicalunderstanding of cholesterol’s role.
The lowering of low-density lipoprotein(LDL) cholesterol with statins reduces car-diovascular events by 30% to 40%. Whatabout the other 60% to 70%? One inthree senior men and one in five post-menopausal women have LDL “PatternB,” with extra small particles of LDL intheir blood, which increases the risk ofheart disease by as much as 300% com-pared to patients with LDL “Pattern A,”with larger particles. “Fortunately, treat-ment with niacin-based drugs and/orfibrates increases LDL size, reducing therisk, provided the pattern is identifiedin time,” says Dr. Pearl. In addition, theimportance of raising high-density lipo-protein (HDL) cholesterol and loweringtriglycerides is receiving a great deal ofattention. These goals are also achievedwith the use of niacin and fibrates.
By finding atherosclerosis at an early(asymptomatic) stage, before the develop-ment of a positive stress test, angina, or aheart attack, proper treatment can beinstituted that will stop progression, possi-bly achieve regression, and keep thepatient asymptomatic and “healthy.”

www.heartpartners.com 9
homocysteine, as well as a number ofinflammatory markers.
Improved Testing Accuracy
Testing for CAD has evolved from themaster’s two-step (walking up and downa two-step platform) to computerizedtreadmill exercise testing and sophisticatednuclear scanning of the heart’s bloodsupply and function. Such testing allows forboth improved sensitivity and specificity.
Unfortunately, a patient will not have apositive stress test until he or she has atleast a 50% blockage in a coronaryartery. Recently, electron beam comput-erized tomography (EBCT) arrived on thescene. This technology allows for visuali-zation and quantification of coronarycalcification. The greater the amountof calcification, the more coronaryplaque present.
The presence of plaque does not neces-sarily equate to hemodynamically signifi-cant blockage, however. Once coronarycalcification is determined as present,
stress testing can determine its physiologicsignificance.
Aggressive Treatment
In addition, treatment modalities haveevolved on several fronts. There are nowmultiple categories of medication to treatCAD aggressively, as well as the hyperten-sion and high cholesterol that exacerbateit. Cardiac catheterization is no longerused just for diagnosis. Percutaneoustransluminal coronary angioplasty (PTCA),or balloon angioplasty, can be used toopen blocked coronary arteries; and the
combined use of stents keeps the openedarteries patent.
From the surgical standpoint, aorto-coronary bypass surgery has now maturedto the point that the routine bypass patientis discharged from the hospital within fiveto seven days. Moreover, in the comingdecade, there is an excellent chance genetherapy will become available.
Given all the current options, it isimportant to identify any coronary prob-lem so it can be found and treated beforeit finds us. ■
Frank J. Pearl, MD, FACC, FCCP, FACP, earnedhis medical degree from Jefferson Medical College,Philadelphia, in 1974. An internship and resi-dency were completed at University of Miami,Jackson Memorial Hospital. Dr. Pearl completedhis fellowship in cardiology at Jefferson MedicalCollege and Temple University Health SciencesCenter. He is board certified in internalmedicine, cardiovascular disease, and critical caremedicine. He is a Voluntary Associate Professorof Medicine at the University of Miami and aClinical Assistant Professor of Medicine at NovaSoutheastern University.
Balloon angioplasty is used toopen blocked coronary arteries.

HeartLines Trends in Heart and Vascular Disease10
here are many causes of syncope. Some of them arebenign, while others may represent a malignant arr-hythmia capable of causing sudden death. Even benigncauses of syncope can produce injury, substantial anxi-
ety, and disability.According to the Framingham Heart Study data and pooled
data from five other studies, the most common causes for syn-cope are neurocardiogenic (“vasovagal,” 18%), cardiac (18%),neurologic (10%), orthostatic (8%), “situational” (5%), andmedication induced (3%).
Syncope Etiology
The etiology of syncope depends on the patient’s age. In theyounger population, neurocardiogenic syncope (NCS), situa-tional, and psychiatric causes are the most common and are usu-ally benign. Causes for cardiac syncope in younger patients thatare infrequent but important to diagnose since they are poten-tially life threatening include the long QT syndrome, Brugadasyndrome, Wolff-Parkinson-White syndrome, arrhythmogenicright ventricular dysplasia, and hypertrophic cardiomyopathy.
NCS is less prevalent in the older population than in theyounger set, although carotid hypersensitivity, a form of neurallymediated syncope, becomes more common. Orthostatic hypoten-sion, medication-induced syncope, cardiac syncope, or multi-factorial etiologies also become more prevalent in the elderly.
The most common causes of cardiac syncope include tach-yarrhythmias (ventricular fibrillation/tachycardia, torsades depointes, hypotensive supraventricular tachycardia) and brad-yarrhythmias (heart block, sick sinus syndrome, carotid hyper-sensitivity). Conditions associated with these arrhythmiasinclude VT/VF post myocardial infarction, hypertrophic car-diomyopathy, dilated cardiomyopathy, long QT syndrome,Brugada syndrome, anomalous coronary arteries, and right ven-tricular dysplasia.
The mortality related to syncope is clearly related to its etiolo-gy. NCS has the same mortality as the general population, where-as cardiac, neurologic, or even unknown causes for syncope havea greater mortality at one or two years than age-matched popu-lation. From several studies, it is clear that cardiac causes for
Syncope, or the transient loss of consciousness and postural tonewith spontaneous recovery, is one of the most common reasons foremergency room visits (3.5%), and one-third of those patients areadmitted to the hospital.
BY JOHN COGAN, MD
Evaluating SyncopeEtiology, Diagnosis, and Treatment
Evaluating SyncopeEtiology, Diagnosis, and Treatment
T

www.heartpartners.com 11
syncope are associated with a 20% to 30% mortality in oneyear if left untreated. Patients with syncope in the setting ofmoderate to severely depressed ejection fraction have a mor-tality rate as high as 40% in one year. It is now recommendedto refer this subgroup of patients for evaluation for a defibril-lator implantation.
Diagnosis
Finding the etiology of syncope is challenging. The diagnosticwork-up begins with a careful history and physical examina-tion, with all the details on frequency and circumstances on eachevent (including prodromal symptoms and precipitating fac-tors), the complete family history, past medical history, and his-tory from witnesses of these episodes. The physical exam canreveal clues on the etiology of syncope, including heart murmursand neurologic signs.
A 12-lead electrocardiogram (ECG) should be performed rou-tinely in almost all cases of syncope (with careful attention to
rhythm, QT duration, bundle branch blocks, and evidence ofischemia or hypertrophy). An echocardiogram should be per-formed in patients in whom there exists any question as towhether he or she has structural heart disease.
Diagnostic tools for the work-up syncope may include tilt tabletesting (TTT), Holter monitor, event recorder, echocardiogram,and an electrophysiologic study (EPS). Further work-up (forexample, magnetic resonance imaging [MRI] or electroen-cephalogram [EEG] in neurologic cases) is often necessary if theinitial history and physical examination point to other diagnoses.
The work-up and treatment of patients with syncope dependson the initial assessment and impression.
Patients with suspected NCS would likely require TTT. It isthe best method for confirming the diagnosis of neurocardio-genic syncope. Indications for TTT include unexplained recur-rent syncope in patients with normal hearts or a single episodeassociated with injury or in settings that pose a high risk ofinjury (for example, while driving a car). It is also indicated forpatients with organic heart disease in whom other causes of syn-cope are ruled out or patients with a clear history of NCS inwhom the test may alter the treatment.
Other indications include trying to differentiate convulsivesyncope from epilepsy, assessment of recurrent falls, or recur-rent near-syncope. A positive test is one that reproduces thepatient’s symptoms with a hypotensive/bradycardic episode.TTT can also help distinguish other etiologies for syncope,including postural orthostatic tachycardia syndrome (POTS),inappropriate sinus tachycardia, and autonomic insufficiency.
In cases where bradyarrhythmias or tachyarrhythmias aresuspected, Holter and event monitors can be diagnostic. A rel-atively new modality of event monitor is the implantable looprecorder (ILR). It is a small recording device that is implantedin the subcutaneous tissue in the chest. It can store up to 45minutes of retrospective ECG recording (without noisy chan-nels, as often seen in the Holter monitors or event recorders),
and the battery lasts for up to 18 months. It can record auto-matically (triggered by a slow or fast heart rate) or be activat-ed by the patient with a small remote control after a syncopalspell. In cases where the usual work-up has revealed no diag-nosis, the ILR yields 25% to 40% of diagnoses in eightto 10 months.
The EPS is of relatively low yield in patients with normalhearts and normal electrocardiograms but is often helpful inpatients with depressed ejection fraction, a history of coronaryartery disease, or some ECG abnormalities. In cases where theEPS shows a clear abnormality, treatment is often provided,including ablation (in cases of supraventricular tachycardia orselected ventricular tachycardias) and pacemaker and defibrilla-tor implantation.
Treatment
Treatment for syncope depends on the etiology. Patients withdiagnosed NCS are often treated with lifestyle modification
(hydration, exercises, salt repletion, learning about their owntriggers, and prodromal symptoms, etc.) without the need formedications. In patients who fail lifestyle modifications, medica-tions are indicated. There are several medications used for NCSbut only limited randomized controlled data.
Beta-blockers are the traditional first-line agents and havebeen used successfully for many years. Five of seven different tri-als regarding beta-blocker use in NCS showed no benefit, how-ever. There are many methodological limitations and patient-selection problems with these trials.
Fludrocortisone appeared effective in uncontrolled studies. Ina randomized trial, it was compared to atenolol and showed nosignificant difference (although no placebo was used).
Vasoconstrictors were evaluated as well. Midodrine (a directalpha-1 agonist) was studied in a randomized, double-blind,crossover study for one month. Results showed patients had lesssyncope than with placebo. It was also compared to salt and fluidtherapy for six months, where midodrine was superior. An uncon-trolled study of methylphenidate suggested it may be an alterna-tive. Etilefrine was no better than placebo in a randomized trial.
Selective serotonin-reuptake inhibitors (SSRIs) were proposedas a potential therapy, and in one randomized trial, 82% ofpatients on paroxetine were free of syncope at 25 months com-pared to 53% on placebo (P<.001). These medications maybecome first-line therapy if results are duplicated.
Cardiac pacing has been proposed as a treatment for NCS formany years, especially using the rate-drop response algorithm.Initial trials showed benefit, but they had no comparison group(patients received a pacemaker or no therapy), so the benefitmay have been a placebo effect of the pacemaker. Later, twopublished trials compared patients with pacemakers eitherturned on or off (to avoid the placebo effect). These trialsshowed no benefit for pacemakers.
At present, pacers are not recommended as first-line therapy.Pacemakers, however, are often used in patients who have little
There are many causes of syncope. Some of them are benign, while othersmay represent a malignant arrhythmia capable of causing sudden death. “ ”

Heartlines Trends in Heart and Vascular Disease12
or no prodrome or who fail other therapyand experience profound bradycardia orasystole during their syncope. In thesepatients, cardiac pacing may alleviate symp-toms and provide time for patients to takeevasive action (for example, to lie down).
Patients with other causes of cardiacsyncope should be treated based on the pre-cise etiology. Patients with the long QTsyndrome are treatable with beta-blockers,pacemakers, and/or defibrillators. Patientswith the Brugada syndrome often require adefibrillator in the setting of syncope.
Patients with syncope and the Wolff-Parkinson-White syndrome or other supra-ventricular arrhythmias should be referredfor EPS and ablation. Patients with hyper-trophic cardiomyopathy and syncope mayneed beta-blockers and a defibrillator.Patients with bradyarrhythmias or carotidhypersensitivity (a group of neurally medi-ated syncope that benefits of pacing) need apacemaker. Patients with low ejection frac-tion and syncope should also be referred forelectrophysiology evaluation.
In summary, patients presenting with syn-cope need a detailed history and physicalexamination and an ECG to categorize theevent, followed by the appropriate tests to getthe correct diagnosis and begin treatment. ■
John Cogan, MD, earned his medical degree fromUniversidad Peruana Cayetano Heredia in Lima,Peru. He completed his internal medicine residencyat University of Texas Southwestern Medical Schoolin Dallas, Texas, where he was appointed chief med-ical resident. Dr. Cogan’s training includes all facetsof diagnosis and treatment of heart rhythm disor-ders, including radiofrequency ablation of complexcardiac arrhythmias and implantation of pacers,defibrillators, and biventricular cardiac devices.
A 12-lead electrocardiogram should be performedroutinely in almost all cases of syncope.

www.heartpartners.com 13
ccording to the American HeartAssociation, cardiovascular dis-eases are still “America’s number-
one killer.” In fact, 73 million people inthe United States have some form ofcardiovascular disease, and Americanswill spend more than $400 billion in2006 on medical and disability costsrelated to these diseases. These numberspoint to the ever-increasing need for high-quality cardiovascular care concentratingon treatment and prevention.
The cardiologists at CardiovascularConsultants of South Florida (CCSF)know these numbers by heart. CCSF isone of the largest cardiovascular groups inFlorida. Each day, these physicians and thehighly skilled staff that supports themdedicate themselves to providing the bestmedical care to patients.
Quality Care through ClinicalResearch
One of the primary ways CCSF guaran-tees its patients the most innovative, pro-gressive cardiovascular care is through itsenthusiastic support of and participationin clinical research. By taking part in clin-ical studies sponsored by pharmaceuticaland medical device companies, the practicehelps push medicine forward and bringsthe most advanced drugs available in themarketplace to patients.
CCSF has conducted invasive and non-invasive, Phase II, III, and IV, inpatientand outpatient clinical trials. The grouptakes pride in its research record, especial-ly in the fact that it often succeeds insurpassing enrollment goals for studies inareas such as hyperlipidemia, arrhythmias,hypertension, myocardial infarctions, andcongestive heart failure.
Patients who participate in the CCSFtrials receive investigational products at
no cost. All clinical research trials at CCSFstrictly follow established protocols tomaintain quality control and patient safety.
Convenient Offices, CaringProfessionals
CCSF’s easily accessible office locationsin Hollywood, Pembroke Pines, Aventura,and Weston are staffed with skilled andcompassionate full-time technologists,nurses, and other support personnel. Theoffices are equipped with state-of-the-artequipment, such as new digital single pho-ton emission computed tomography(SPECT) cameras for highly sophisticatednuclear imaging and new digital ultra-sound equipment for accurate imaging ofthe heart and blood vessels. These factorsmake it possible for CCSF to provide themost comprehensive cardiac and vascularevaluation and treatment available inSouth Florida. ■
ACardiovascular Consultantsof South FloridaPhysicians and Physician Extenders:
Howard F. Berlin, MD, FACC, President Kashmira P. Bhadha, FACCMichael Braun, MD, FACCTroy Elmstrom, PA-CMichael Entenberg, MD, FACCCheryl Greenberg, ARNPJose A. Guzman, MD, FACCBarry Harris, MD, FACCRalph M. Levy, MD, FACCDaniel G. Norberg, MD, FACCFrank Jay Pearl, MD, FACC, FCCP, FACPLawrence M. Reiss, MD, FACCBernard E. Shair, MD, FACCEthan Daniel Siev, MD, FACC, FCCP
Interventional Cardiologyand Vascular Medicine:
Juan Pastor-Cervantes, MD, FACCSusan B. Fox, DOAnn Robblee, PA-C
Cardiac Electrophysiology:
Raul D. Mitrani, MD, FACCJohn Cogan, MD, FACCBernice Jones, ARNP
Administrator/CEO:
Judah Friedman, MEd, MBA
HeartLines Fact
AstraZeneca, a major international phar-maceutical company engaged in theresearch, development, manufacture,and marketing of prescription pharma-ceuticals and the supply of health careservices, recently chose CardiovascularConsultants of South Florida as oneof eight Centers of Excellence in theUnited States.
HEALTH CARE PRINCIPLES
Getting to the Heart of ThingsCardiology Center Focuses on All Aspects of Cardiovascular Care

HeartLines Trends in Heart and Vascular Disease14
he concept for bradycardia pacemakers originated inthe 1950s. Initial units were bulky, required frequentbattery changes, and had no programmability. Untilthe 1980s, single-chamber ventricular pacing was the
predominant mode; and even through the early 1990s, dual-chamber atrioventricular (AV) pacers had limited programma-bility and functionality.
The modern pacemaker generator now weighs 25 to 35 grams.It is capable of fully programmable dual chamber and biventric-ular pacing and rates response to activity. It also has transtele-phonic capability for telemetry of all pacing parameters down-loadable to the Internet, incorporates algorithms to respond tochanges in intrinsic rhythms, and can store details of patients’arrhythmic events. Because of the complexities of types of pac-ers, programmed parameters, and drug interactions with thesecardiac devices, cardiac electrophysiologists have become thepredominant specialists managing and implanting these devices.
The initial pacers (single and dual chamber) were designed toprovide right ventricular (RV) pacing in the event of asystole,generally due to AV block. In the early days of pacing, mostpatients presented with high-degree AV block. At present in theUnited States, however, approximately two-thirds of patientsrequiring pacing have an indication of sick sinus syndrome orone of its variants. These patients generally require atrial pacingbackup, which the dual-chamber pacers can reliably provide.
However, standard dual-chamber pacers with traditional pro-gramming of the DDD mode are designed to provide backup RVpacing. Therefore, the DDD pacing mode may inadvertentlystimulate the RV, which can lead to desynchronization of ven-tricular function.
Complications
The problem with inadvertent RV pacing is often exacerbatedby rate-slowing drugs (beta-blockers, calcium blockers, digox-in), which are often used in patients with sick sinus syndromebecause these patients also tend to have atrial fibrillation. Thesedrugs are used appropriately to slow the heart rate duringparoxysms of atrial fibrillation; however, these drugs also pro-long the patient’s intrinsic AV conduction (PR interval). In thisscenario, a prolonged PR interval is more likely to lead to moreRV pacing.
Another common problem involves the use of rate-responsivepacing (DDDR). The premise of DDDR includes pacing theatria and ventricle at a faster rate (driven by the pacer sensor) inorder to provide appropriate heart-rate response during activity.This faster atrial rate causes a physiologic delay in patients’intrinsic AV conduction (PR interval). The pacer AV intervalstays the same or actually shortens during DDDR, which againwould lead to inadvertent RV pacing. Unfortunately, manypatients have inappropriate DDDR, which leads to RV pacing.
The concept of inappropriate RV pacing was developed onlyover the past five years. Based on various studies, it is now rec-ognized that RV pacing leads to abnormal electrical activationof the left ventricle (LV) similar to patients having an intrinsicleft bundle branch block (LBBB). In certain patients, thiscondition desynchronizes LV systolic function, leading to leftventricular dysfunction and congestive heart failure. In fact,biventricular pacing was developed in order to resynchronize LVsystolic function in patients with congestive heart failure (CHF),low ejection fraction, and LV dyssynchrony due to LBBB orabnormal electrical activation.
The DAVID Study (see Figure 1) followed patients withimplantable defibrillators designed to compare backup VVI pac-ing at 40 to aggressive DDDR pacing at 70. The hypothesis wasthat DDDR pacing at 70 would lead to less ventricular tachycar-dia, better quality of life, and better outcomes. To the authors’surprise and as shown in the graph, the patients with VVI pac-ing at 40 fared better. The reason is that DDDR pacing led toLV desynchronization and worsening CHF, despite the fact thatthese patients were paced at faster heart rates than patientstreated with VVI pacing at backup rate 40.
The percent of RV pacing was examined and compared withoutcomes of CHF in the MOST trial (Circulation. 2003;107:2932). As shown in Figure 2, those patients with DDD pacing(Figure 2A) or VVI pacing (Figure 2B) with ventricular pacing
Proper Application of
PacerTechnology
ExploringNew Paradigms
in Cardiac Pacing
BY RAUL D. MITRANI, MD, FACC
T

www.heartpartners.com 15
less than 40% or less than 80%, respectively, had lower inci-dence of hospitalization for heart failure compared withpatients with higher percentages of ventricular pacing.
Inappropriate RV pacing has also led to higher incidence ofatrial fibrillation. This condition can lead to higher incidenceof thromboembolic complications.
Improved Patient Outcomes
Current strategies to prevent pacing-induced desynchroniza-tion involve programming DDD mode with excessively long AVintervals. This type of programming can lead to other problems,including pacemaker mediated tachycardia. DDI pacing modemay be used in this setting as long as the patient does not haveany form of second- or third-degree AV block.
Recently, some pacer companies have developed complexalgorithms involving AAI pacing (atrial pacing only) with back-up DDD pacing, should the patient go into advanced AV block.The purpose of all these algorithms is to provide appropriateatrial pacing backup response and allow for PR interval, which,in the presence of normal QRS width, is preferable to havingthe RV pacing.
In sum, there are new paradigms in pacer selection, program-ming, and follow-up in patients requiring pacer therapy. Theinitial evaluation of patients considered for pacing therapyshould include evaluation of the patient’s underlying rhythm,heart function, symptoms, and indication for the pacer. It shouldbe determined whether the patient requires placement of an LVlead for cardiac resynchronization and whether a backup defibrilla-tor as part of the pacer system should be used. Programming ofthese devices is often quite complex and needs to consider the
patient’s intrinsic AV conduction, intraventricular conductiondefects, and hemodynamic function.
The appropriate pacer algorithm (DDD, DDI, AAI with back-up DDD, search AV hysteresis algorithms) can make a signifi-cant difference in long-term cardiac function and quality of life.Follow-up of these patients involves assessment of frequency ofpacing in the different cardiac chambers and determiningwhether the various programming parameters (rate, AV interval,VV interval, etc.) are optimal for the patient’s overall hemody-
namic function. Fortunately, proper pacer programming andfollow-up leads to improved patient outcomes. ■
Raul D. Mitrani, MD, FACC, completed his internship and residency atCase Western Reserve University following graduation from ColumbiaCollege and medical school at Columbia University College of Physiciansand Surgeons. He then completed his cardiovascular fellowship at IndianaUniversity and cardiac electrophysiology fellowships at Indiana and CaseWestern Universities. He is a Diplomate and is board certified in cardiovas-cular disease and clinical cardiac electrophysiology. He has authored 17 bookchapters, 35 refereed journal articles, and 37 refereed abstracts. Dr. Mitranihas served as a consultant for many local hospitals and is a past associateprofessor of medicine at the University of Miami School of Medicine anddirector of the Arrhythmia and Pacemaker Center, Jackson MemorialHospital. Currently, he serves as Director of Electrophysiology for MemorialRegional Hospital and Director of Cardiovascular Consultants of SouthFlorida’s cardiac electrophysiology practice. He is also Director of FloridaArrhythmia and Syncope Center at CCSF.
FIGURE 1 FIGURES 2A & 2B
The initial evaluation of patients considered for pacing therapyshould include evaluation of the patient’s underlying rhythm,
heart function, symptoms, and indication for the pacer.“
”

HeartLines Trends in Heart and Vascular Disease16

www.heartpartners.com 17

HeartLines Trends in Heart and Vascular Disease18

www.heartpartners.com 19
HEALTH CARE PRINCIPLESBY JUDAH FRIEDMAN, CEO, CARDIOVASCULAR CONSULTANTS OF SOUTH FLORIDA
EDITED BY MIKE SEGAL, ESQ., BROAD AND CASSEL
hen I talk with physicians abouthealth care regulations, their eyesroll back into their sockets and
they immediately tune me out. Health careis one of the most regulated industries inour economy. Physicians spend years inmedical school, residencies, and fellow-ship programs training to provide qualitymedical care to their patients. They spendlittle time thinking about the practicalaspects of running a practice and, inmost cases, no time on the myriad federaland state regulations governing the prac-tice of medicine.
Medicare provides a template for cod-ing the services that each of you provideto your patients. Medicare sends out bul-letins every month, notifying you ofchanges in the regulations. It is essentialthat you read these bulletins so you arecoding properly for your services. If youfind there is not enough time, subscribeto a national service or contract with alocal consultant.
OSHA Standards
A number of pieces of legislation thathave passed in the last 35 years have hadmajor impacts on medical practices. In1970, the federal government enacted theOccupational Safety and Health Act (OSHAct). This program was established toensure every man and woman in the nationis working in safe, healthful conditions.
The Occupational Safety and HealthAdministration (OSHA) sets strict stan-dards for medical practices. As an exam-ple, all employees who have patient con-tact must receive certification stating theyhave the required knowledge to handleblood and other pathogens safely. OSHAhas the right to enter a facility withoutprior warning, and if it finds the standardsare below “national consensus standards,”it can shut the facility down.
Anti-Kickback and Stark Laws
It is also critical for you to have a famil-iarity with the federal Anti-kickback andStark laws, as well the Florida Patient Self-Referral law. The federal Anti-kickbacklaw has existed since 1972. Initially acriminal law, it is extremely expansive,prohibiting the payment or acceptance ofkickbacks (bribes) of any kind in exchangefor referrals.
In 1987, the law was modified toinclude civil penalties, including fines anda Medicare “death penalty” — termina-tion from the Medicare (and Medicaid)program. To address complaints that thestatute was too broad in scope, the gov-ernment also modified the law to includeexceptions, or “safe harbors” — safetynets that allow health care providers com-fort that potentially violative transactionswill comply with the law. A problem isthat many transactions only meet some —but not all — the safe harbors.
In 1992, Congress enacted the Stark lawin honor of the congressman who spon-sored the bill. Stark prohibits any physi-cian and members of his or her familyfrom referring certain defined ancillaryservices (known as designated health serv-ices, or DHS) that are reimbursable underMedicare or Medicaid to a business inwhich he or she has a financial interest.There are many exceptions to that rule(such as the exception for certain grouppractices) and voluminous regulationsinterpreting the law.
The Anti-kickback and Stark laws differgreatly in many aspects, including theirapplications. While the Anti-kickback lawhas many shades of gray, the Stark law isblack and white — either the law is satis-fied or it is not.
Baby Stark
In 1992, Florida enacted its own versionof the Stark law — the Florida Patient
W
Know the Law Examining Critical Regulations Governing Medical Practices
Ensure you understand the laws and their consequences. At the end of the day, you are held respon-sible, not your office manager.

HeartLines Trends in Heart and Vascular Disease20
Self-Referral law, often referred to as “BabyStark.” Similar to the Stark law’s prohibitionon referrals, Baby Stark contains a generalprohibition against a physician referring toan entity in which he or she owns an inter-est. In addition, like the Stark law, BabyStark contains many exceptions to the gener-al rule, including an exception for referralswithin group practices.
The laws also differ in many aspects, how-ever. DHS is defined differently in BabyStark. Although the Stark law includes 11services within its definition of DHS, BabyStark only consists of four general categoriesof DHS. Also, Baby Stark applies to DHSwhere the service is not reimbursable byMedicare or Medicaid.
Finally, whereas the Stark law limits physi-cian ownership of an entity to which thephysician refers, Baby Stark restricts physi-cian ownership of a medically related entity,even where no DHS is involved. With BabyStark, unless a physician meets certainrequirements, such ownership is prohibited.
Lesson Learned
The lesson here is for you to ensure youunderstand the laws and their consequen-ces. At the end of the day, you are heldresponsible, not your office manager.
And for those who believe “this too shallpass,” I hate to burst your bubble. Takingall three parts of Medicare together, it isprojected that the total Medicare debt forthe current generation will reach $29.2 tril-lion; and future generations will add $32.5trillion to this obligation. Clearly, the feder-al government will look for as many waysas possible to reduce this debt, either byincreasing taxes or reducing costs. No doubtthe easiest path is to reduce costs by elimi-nating fraud and abuse and promoting moreefficiency through Medicare HMOs. ■
Judah Friedman, CEO of Cardiovascular Consul-tants of South Florida (CCSF), has had a long anddistinguished career in health care administration.Prior to joining CCSF, Mr. Friedman served as aca-demic administrator at Albert Einstein College ofMedicine, Jacobi Hosptial, and Mount Sinai MedicalCenter in New York. Thereafter, he spent three yearsdeveloping a multispecialty medical practice in BocaRaton. Mr. Friedman was instrumental in the growthof CCSF as well as in developing new programs, suchas the first freestanding cardiac catheterization inSouth Florida, and in implementing an electronicmedical records program that allows physiciansinstant access to patient charts and improvesthe data quality. In 2003, Mr. Friedman was namedBest Practice Administrator at the 14th AnnualMedical Business Awards presented by FloridaMedical Business.

www.heartpartners.com 21

HeartLines Trends in Heart and Vascular Disease22
aphenofemoral incompetence causing reflux in thegreater saphenous vein is the most common cause ofVI. If left untreated, approximately half of the patientswill develop venous hypertension and symptoms of
chronic VI.2 With progressive degrees of reflux, patients candevelop leg pain, swelling, venous hemorrhage, venous eczema,stasis dermatitis, atrophie blanche, lipodermatosclerosis, andulcerations. Venous stasis ulcers are the most common cause oflower extremity ulceration in the world.
Diagnosing Venous Insufficiency
Since VI is a common problem, it is important to notice thesigns and symptoms associated with the condition. A thoroughhistory and physical, as well as looking for leg swelling, varicoseveins, venous stasis changes, hemosiderin deposition, andvenous eczema are important. Clinical tests are sometimes usedto diagnose VI. These tests, however, are relatively insensitiveand unreliable. The gold standard is a duplex ultrasound calleda valvular incompetency study.
Conservative Treatment
If the pedal pulses are normal, patients should receive a pre-scription for medical-grade, graduated compression hose andencouragement to elevate their legs. They should moisturizetheir legs and maintain good foot care to prevent skin break-down, infections, and ulcer development.
Definitive Treatment
Conventional therapy for VI is ligation of the saphenofemoraljunction, with or without vein stripping. High ligation with veinstripping is more successful than high ligation alone. Ligationplus stripping has an immediate success rate of 86% but apatient satisfaction rate of only 62%.3 Even when performed bya surgeon skilled in treating venous disease, there is still a highrate of recurrence.
The most common complications of vein stripping involvethose associated with general anesthesia. Other complicationsinclude postoperative pain, saphenous nerve injuries, infections,
New Treatment Options for
VenousDisease
Evaluating Varicose Veins and Venous Insufficiency
BY SUSAN B. FOX, DO
Venous disease affects an estimated 80 millionAmericans and ranges from spider veins to increasingdegrees of venous insufficiency (VI). In one U.S. healthsurvey, varicose veins were found to be the seventhmost common reason for medical referral. By theapproximate age of 60, 72% of women and 40% ofmen are affected by VI.1
S

www.heartpartners.com 23
neovascularization, hematomas, and thromboses. Neovascularreconnection that occurs in about half of these patients andpersistently abnormal venous physiology are considered theprimary causes of recurrence.4 Postoperative morbidity of veinstripping is high. As a result, newer, less invasive treatments arebecoming the standard of care. These include VNUS closure andendovenous laser vein ablation.
VNUS closure, approved in the United States in 1999,involves threading a radiofrequency catheter into the vein underultrasound guidance. The probe contacts the venous endo-thelium, heating it to 85˚C and causing the vein to seal shut.Tumescent anesthesia injected between the skin and the veinlimits surrounding tissue damage.
The procedure can be performed on veins 2 mm to 12 mm indiameter. It has a 92% to 98% success rate and a 10% recur-rence rate at two years.5, 6, 7 Two other studies by vein specialistsreported success rates of only 68% and 73%, however.8, 9 Theprocedure is frequently performed in the operating room.
Drawbacks and complications include the relative size limita-tions, some neovascularization, potential nerve injuries, infec-tions, skin burns, thromboses, and hematomas. Recovery time isshort, and people can return to their regular activities within afew days. The average time off work was 6.5 days with VNUSand 15.6 days with stripping. Patients had less pain and weremore satisfied with VNUS closure than vein stripping. Eventhough the procedure costs more, it appears cost-saving to
society because of the decreasein lost wages, even though40% of the patients studiedwere retired.10
Endovenous laser ablation,approved by the Food and Drug
Administration (FDA) in 2002, isthe newest technique to treat VI.The procedure is often performedin an outpatient setting. Using a mod-ified Seldinger technique, a laser isinserted into the vein under ultra-sound guidance. Once access is ob-tained, tumescent anesthesia is injected
between the skin and the vein. The tumescent anesthesia numbsthe area, contracts the vein around the catheter, and dissipatesheat from the laser. The entire procedure takes 45 minutes.Patients usually have only mild bruising and a temporarypulling sensation along the course of the vein.
Complications include minor skin burns, hematomas, infec-tions, nerve injuries, and thromboses. The benefits are that theprocedure is performed under local anesthesia, there is no limi-tation to the size of veins that are treatable, and recovery isshort, so people can return to work almost immediately. Severalreports have documented a success rate of 94% to 100%, witha two-year recurrence at less than 4%.11,12,13,14 As many as 99.8%of patients surveyed were satisfied with their results and wouldrefer a friend for endovenous laser ablation.15 ■
After earning her medical degree from Nova Southeastern College ofOsteopathic Medicine, Susan B. Fox, DO, completed her residency in inter-nal medicine and her fellowship in vascular medicine at The ClevelandClinic in Cleveland, Ohio. Before moving to Florida, she practiced as a veinand vascular expert at University Hospitals of Cleveland and was on theteaching faculty at Case Western Reserve University. Dr. Fox specializes inthe nonsurgical treatment of varicose and spider veins using state-of-the-art,minimally invasive therapy for large varicose veins and venous insufficiency.Dr. Fox was featured on several news programs and in articles and haslectured extensively on varicose veins.
Veins become varicose dueto weak one-way valves thatallow blood to leak and col-lect in the vein.
References:1 Callam, MJ. 1994 Epidemiology of varicose veins. BR J Surg., 81;167-173.
2 Widmer, L.K., Malland, T.H., Martin, H. 1974 Epidemiology and Social Medical Importanceof Disease of the Veins. Munch Med. Wochenschr., 116: 1421-1426.
3 Noppeney, T. Results of Standard Varicose Vein Surgery. Zentralbl Chir. 2002:127:748-51.
4 Lefeebvre-Vilardebo, M., Lemasle, P. Postsurgical Inguinal Neovascularization is notsystemically a cause of varicose recurrence. UIP World Chapter Meeting, Aug. 27-31,2003.(abstract A-128).
5 Weiss, R.A., Weiss, M.A. 2002 Endovenous RF occlusion for treatment of saphenous reluxand associated varicose veins: Long Term results at 3 years experience. 16th Annual CongAm Coll Phleb, Nov. 7-10 (abstract).
6 Weiss, R., Weiss, M.A. 2002 Controlled radio frequency endovenous occlusion using aradio frequency catheter under duple guidance to eliminate saphenous varicose veinreflux: A 2 year follow-up. Dermatol. Surg, 28:38-42.
7 Morrison, N., Nehardt, D. 2002 Radio frequency closure treatment of greater saphenousvein reflux utilizing increased heat and an increased pull back rate. 16th Ann Cong AmColl Phlebectomy, Nov. 7-10 (abstract).
8 Goldman, M.P., Amiry, S. 2002 Closure of the greater saphenous vein with endoluminalradio frequency thermal heating of the vein wall in combination with ambulatory phlebec-tomy: 50 patients with more than 6 month follow-up. Dermatol. Surg. 28: 29-31.
9 Rautio, T.T., Perala, J.M., Wiik, H.T., Juvonene, T.S., Haukipuro, K.A. 2002. Endovenousobliteration with radio frequency-resistive heating for greater saphenous vein insufficiency.A Feasible Study. J Vasc Interv Radiol. 13: 569-575.
10 Rautio, T. Endovenous obliteration versus conventional stripping operation in the treat-ment of varicose veins: A randomized controlled trial with comparison of the costs. J VascSurg. 2002 35: 958-65.
11 Navarro, L., Min, R.J., Bone, C. 2001 Endovenous laser: A new minimally invasivemethod of treatment for varicose veins-preliminary observations using an 810 nm diodelaser. Dermatol Surg. 27: 117-122.
12 Mackat, E. 2002 Transcatheter greater saphenous vein ablation with endovenous laserand ultrasound guided perivenous tumescent anesthesia. 16th Ann Cong Am CollPhlebology, Nov. 7-10. ( abstract).
13 Min, R.J., Khilnani, N. 2003 Endovenous laser treatment of saphenous vein reflux. Two-year follow-up results. J Vasc Interv Radiol. (Suppl).14: s35.
14 Prebstle, T.M., Guel, D., Lehr, H.A., Knop, J. 2003 Early recanalization of the greatersaphenous vein after endovenous laser treatment. 17th Ann United Internatl. PhlebologyWorld Cong. Aug. 27-31. (abstract) p A-170.
15 Min, R.J., Khilnani, N., Zimmet, S.E. 2003. Endovenous laser treatment of saphenousvein reflux: long-term results. J Vasc Interv Radiol., 14: 991-996.

HeartLines Trends in Heart and Vascular Disease24
REPORTSBY HOWARD F. BERLIN, MD, FACC
new updated version of theACC/AHA Clinical PerformanceMeasures for Adults With Chronic
Heart Failure was released in September2005. This third release since 1995 wascalled for due to the magnitude of newdata since the last guideline in 2001. Theguideline is available in its entirety atwww.acc.org.
This article highlights some of the impor-tant data presented in this latest review.
Justification
The new guidelines develop a stagingsystem similar to that used in cancer stag-ing. It is not meant to replace the NewYork Heart Association functional classifi-cation that is a symptoms guide. The newstaging system recognizes that heart fail-ure is a result of structural changes andthat symptoms can vary during a shortperiod of time, but the underlying struc-tural changes usually remain unchanged.
Neurohormonal System
Left ventricular dysfunction begins withsome injury to or stress on the myocardi-um, resulting in failure of inflow (diastolicdysfunction) or outflow (systolic dysfunc-tion). There is usually a change in thegeometry and structure of the left ventric-ular that follows. The left ventricularchamber dilates and/or hypertrophies andbecomes more spherical, which is termedcardiac remodeling.
It is apparent that the activation of theneurohormonal system plays an importantrole in these changes. Patients with heartfailure have elevated circulating or tissuelevels of epinephrine, angiotensin II, aldos-terone, endothelin, vasopressin, andcytokines that are regulated by the neuro-hormonal system. Treatment of heart fail-ure has improved immensely with the use
of drugs that interfere with the neurohor-monal system — angiotensin-convertingenzyme (ACE) inhibitors, angiotensinreceptor blockers (ARBs), beta-blockers,and aldosterone antagonists.
Staging and Interventions
The guidelines recognize that heart fail-ure is usually progressive once there arestructural changes in the myocardium. Themost effective treatment is to prevent theinitial structural changes. Stage A address-es the category of patients who have onlyrisk factors (hypertension, hyperlipidemia,diabetes mellitus, a family history of heartfailure, obesity, atherosclerotic cardiovas-cular disease, or metabolic syndrome) butno structural heart disease. Aggressive riskfactor intervention is suggested at thisstage, with the use of ACE inhibitorsencouraged in appropriate patients.
Stage B patients have structural changes(myocardial infarction, left ventricularhypertrophy, low ejection fraction, or
asymptomatic valvular disease) but arewithout symptoms of heart failure.
Drugs at this stage should includeACE inhibitors or ARBs, beta-blockers,and devices in selected patients. Devi-ces (implanted cardioverter/defibrillator)should be considered in patients with anejection fraction of less than 35%.Consider cardiac resynchronous therapy(BiV ICD) for symptomatic heart failuredespite stable optimal medical therapywith a QRS greater than 120 ms and anejection fraction of less than 35%.
Stage C patients have the structuralchanges of Stage B patients but also haveor have had symptoms of heart failure.ACE inhibitors and/or ARBs should beused in all appropriate patients. Beta-block-ers are to be initiated and, specifically,should be one of the currently approveddrugs — metoprolol succinate (not meto-prolol tartrate), carvedilol, or bisoprolol. Inselected patients, aldosterone antagonists(spironolactone and eplerenone), ARBs,
A
Heart Failure Guidelines Update Offers Effective Treatments
This anterior view of the left chamber of the heart shows the mitral and aortic valves with blood cells.Left ventricular dysfunction begins with some injury to or stress on the myocardium, resulting in fail-ure of inflow or outflow.

www.heartpartners.com 25
digitalis, or hydralazine/nitrates should be initiated. Devices inselect patients as mentioned above should also be utilized.
Stage D patients have refractory heart failure requiring special-ized interventions. These patients require a decision on compas-sionate end-of-life care. Extraordinary measures may includeheart transplant, chronic inotropes, mechanical support, experi-mental surgery, or experimental drug therapy.
The most effective treatment of heart failure is in preventionbecause heart failure is usually a progressive disorder. Physiciansmust be steadfast in their treatment of risk factors to achievepublished guidelines.
Heart-failure patients are growing in numbers, with a currentdirect and indirect cost of $27.9 billion per year. Only $3 billionper year are for drug costs. There are more than 550,000 newpatients per year diagnosed with heart failure, and the currentaffected population tops five million.
I hope many of you will take the time to read the new guide-lines or at least keep a copy of the pocket version to use in yourtreatment of heart-failure patients. ■
Howard F. Berlin, MD, FACC, earned his medical degree from JeffersonMedical College in 1975. He completed his internship and residency atAbington Memorial Hospital, Philadelphia, and a cardiology fellowship at theUniversity of Miami, Jackson Memorial Hospital. Dr. Berlin was honored bythe Hobert Amory Hare Honor Medical Society, Jefferson Medical College.He is board certified in internal medicine and cardiovascular disease.
1. Do not delay the use of beta-blocker therapy despite the inabil-ity to achieve the desired level of ACE inhibitor or ARB doses.
2. If coronary artery ischemia is suspected, cardiac catheterizationshould be undertaken early in an attempt to revascularize anischemic ventricle.
3. Screen for sleep apnea if suspected in obese individuals.
4. Keep in mind hemochromatosis, HIV, rheumatologic diseases,amyloid, and pheochromocytoma as less frequent but treat-able causes of heart failure.
5. Avoid the combination of an ACE inhibitor, ARB, and aldos-terone antagonist because of the risk of hyperkalemia.
6. Digoxin is not to be used in patients with sinus rhythm, lowejection fraction, and no heart-failure symptoms. Digoxin didreduce hospitalizations in patients with a reduced ejectionfraction and symptoms of heart failure.
7. Calcium channel blockers with negative inotropic effects maybe harmful in patients with low ejection fractions and symp-toms of heart failure post myocardial infarction.
8. Avoid nonsteroidal anti-inflammatory agents.
9. Add a nitrate/hydralazine combination if the patient is sympto-matic on ACE inhibitor and beta-blocker or if drug intolerant,hypotensive, or renal insufficient.
10. Do not use an aldosterone antagonist if creatinine is greateror equal to 2.5 mg/dL in men and 2.0 mg/dL in women or ifpotassium is greater than 5.0.
11. Long-term infusion of an inotrope may be harmful except aspalliation for end-stage heart failure.
12. Nutritional supplements are not indicated for the treatment ofheart failure at any stage.
Brief Suggestions and Concepts

HeartLines Trends in Heart and Vascular Disease26
REPORTSBY DANIEL G. NORBERG, MD, FACC
magine a world where your patients’medical information was readily avail-able to send to health care providers
anywhere in the world, was updated contin-uously, and was safely stored and securelymanaged on a mainframe computer.
Electronic medical records (EMRs) arehere and provide significant benefits toboth physicians and patients. EMR is aterm used to describe computer-basedpatient medical records. As more medicalservice providers convert to “paperless,”electronic systems, medical informationcould follow patients through patient-consented, secure Internet access.
Accurate and Accessible
EMR allows rapid access and trans-ferring of medical information. Considerthe possibility that your patient becomesill while out of town or while his or herregular physician is not on call. WithEMRs, the treating physician is able toaccess the relevant medical record andobtain important information for patient
care. The use of EMRs facilitates qualityand efficiency of patient care.
The system links multiple offices, allow-ing access to patient data at any providerlocation. There are no charts to transport,store, or maintain. Complete medical datais available anywhere in the network andis continuously updated.
In addition to maintaining a currentlist of patient medications and medicalproblems, it automatically checks for druginteractions and allergies. Accurate andaccessible EMRs greatly assist in provid-ing quality and affordable medical care.
Improving Efficiency
Economically, EMRs improve efficiencythrough several methods. A paperlesssystem is environmentally friendly anddecreases the long-term cost of producingand maintaining charted medical records.Since the information is complete, there isa decrease in duplication of services andneedless overutilization of resources.
Scheduling is completely automated andlinked to the patients through a phonereminder system. Billing cost and confu-sion are decreased through electronicclaims submissions to insurance compa-nies and patients. Maintaining recordselectronically allows for instant availabili-ty of entire records from hard-drive stor-age, which is continuously backed up toprotect information loss.
Electronic transmission of medical datais performed in a secure environment. TheEMR system information is securedthrough 128-bit encryption. Encryption isthe conversion of data into a form thatis not easily understood by unauthorizedindividuals. The EMR system complies
with the Health Insurance Portability andAccountability Act (HIPAA) and onlyallows access by health care professionalswith secure provider access. Medicalprofessionals maintain and update patientmedical records in one integrated system.The EMR system is capable of generatingtimely clinical notes, printing prescrip-tions, linking laboratory information,updating medications, storing procedure/operative reports, and preliminarily evalu-ating and comparing electrocardiograms.Reports generated at outside facilities orhospitals and previous patient medicalinformation are easily scanned, stored,and maintained through one system.
The future of medical care is availableelectronically at Cardiovascular Consul-tants of South Florida, where electronicmedical records are in place. Our comput-ers are linked to local hospitals, insuranceproviders, and laboratories and providefacsimile support for referring physiciansand pharmacies. We have invested signifi-cant time, effort, and capital to create apaperless electronic medical informationsystem that offers the most up-to-datetools for excellence in patient care. Webelieve accurate and accessible medicalrecords are essential to providing qualitymedical care to our patients. ■
Daniel G. Norberg, MD, FACC, earned his med-ical degree from the University of Florida Collegeof Medicine in 1991 and completed his internshipand residency at the University of Miami School ofMedicine, Jackson Memorial Hospital. He com-pleted a fellowship at the University of FloridaCollege of Medicine, Shands Hospital MedicalCenter. A Diplomate of the American Boardof Internal Medicine in cardiovascular disease,Dr. Norberg is certified in nuclear cardiology.
I
The Future of Medical Care Electronic Medical Records Benefit Both Patient and Physician
A paperless system is environmentally friendly and decreases the long-term cost of producing andmaintaining charted medical records.

www.heartpartners.com 27

Cardiovascular Consultantsof South Florida3335 N. University Dr., Ste. 8Davie, FL 33024