Embed Size (px)
Citation preview

IJGDBPIndian Journal on Growth, Development and Behavioral PediatricsOfficial Journal of IAP Chapter on Growth, Development and Behavioral Pediatrics
Vol. 6 : 2010
Editor-in-ChiefJaydeep ChoudhuryExecutive EditorMonidipa BanerjeeAdvisory BoardK N AgarwalDilip MukherjeeMKC NairSukanta ChatterjeeKsh Chourjit SinghShabina AhmedMadhuri KulkarniRanjana ChatterjeeMembers, Editorial BoardAnjana A ThadaniAnju SethSaheli MisraSuchit TamboliZafar MeenaiEx OfficioS N ParidaChairperson of the ChapterJaydeb RaySecretary of the Chapter
Secretariat98 Ballygunge Place, Kolkata 700 019Email : [email protected]
Editorial OfficeJaydeep Choudhury95/2 Ballygunge Place, Kolkata 700 019Mobile : 98311 91020Email : [email protected]
THE IND
IAN
A
CADEMY OF PE
DIA
TRICS
Content
EditorialJaydeep Choudhury ................................... 1
Issues in Linear Growth in ChildrenJaydeb Ray ................................................. 3
Predictrs of Outcome in High RiskNeonatesSuchit Tamboli .......................................... 11
Transient Tachypnea of Newborn :A Preventable Impediment forNeonatal Growth andDevelopmentRaktima Chakrabarti ................................ 18
Developmentally Supportive Carefor Premature BabySantosh Nimbalkar ................................... 24
Genetic Counseling in AutismMonidipa Banerjee ................................... 28
Breaking NewsJaydeep Choudhury ................................. 34
This journal is supported by “Glaxo Nutrition Foundation”


Editorial
The year 2010 was a landmark year for IAP chapter on Growth,Development and Behavioral Pediatrics. On 18 June 2010 at the Instituteof Child Health, Kolkata the four modules on Growth Monitoring,Developmental Screening, Autism and Behavioral Problems were giventhe final shape. It started in 2008 when the chapter took the initiative todevelop modules on four important issues related to growth, developmentand behavioral pediatrics. Subsequently a task force was formed andtwo sessions were held in 2008 and 2009 as the preliminary steps todevelop the modules. Finally the task force came together and gavefinal shape to the modules. The main purpose behind development ofthese modules was to orient and train the members and post graduatestudents in important issues related to growth monitoring, developmentalscreening, autism and common behavioral problems. Dr Dilip Mukherjee,Dr K N Agarwal, Dr Ksh Chourjit Singh, Dr M K C Nair, Dr NandiniMundkur and Dr Sukanta Chatterjee are the advisors of these modules.The members are Dr Anjana Thadhani, Dr Anju Seth, Dr Jaydeb Ray,Dr Jaydeep Choudhury, Dr Madhuri Kulkarni, Dr Monideepa Banerjee,Dr Ranjana Chatterjee, Dr S N Parida, Dr Sabina Ahmed, Dr SuchitTamboli, Dr Swapna Mittal and Dr Zafar Meenai. President of CentralIAP 2010, Dr Deepak Ugra, President Central IAP 2011, Dr T USukumaran and Secretary General, Dr Tanmay Amladi are the Ex-officiomembers.
The module on Growth Monitoring focuses on growth assessment,anthropometric measures of weight, length, height and headcircumference, pitfalls in measurement and assessment of puberty. Italso highlights on interpretation of anthropometric data, growth chart,concept of centiles, Z score, SD, BMI, types and plotting on charts,interpretation, prediction of adult height based upon current growthcalculation of genetic potential and comparing whether a child’s growthis commensurate with it understanding the significance of bone age,differentiate between various normal and pathological growth patterns.
IJGDBP 1

The module on Developmental Screening demonstrates on identifyingthe neonates, infants and children at risk for developmental delay,recognize the flag signs of development delay, understand theetiological factors and co-morbidities in developmental delay, assessthe developmental delay in various domains, plan management ofdevelopmental delay and understand the preventive aspects ofdevelopmental delay.
The module on Autism stresses on identifying children at risk for autism,identify the red flags in autism and speech delay, recognize the deviantfeatures in development in autism, diagnose a child with autism, makeappropriate referrals, emphasize the need for early detection and earlyintervention.
The module on Behavioral Problems deals with childhooddevelopmental disorders including pervasive developmental disorders,attention-deficit and disruptive behavior disorders, eating disorders,habit disorders, somatoform disorders, psychotic disorders, substancemisuse, emotional disorders like phobias, school phobia, OCD,anxiety states, separation anxiety, panic disorders and selectivemutism and conduct disorders like stealing, defiance, aggression andanti-social behavior.
The plan is to conduct small workshops on these modules at variousplaces. The sincere efforts of the committee will be successful only ifthe message is passed on many members and then utilized in day today practice.
Jaydeep ChoudhuryEditor-in-Chief
2 Vol 6 : 2010

Growth is the sole indicator of health.Growth is influenced by nutrition,illnessand environment. Approximately10% of children may present with growthproblems.
Growth disorders may be due to ofexcessive shortness (short stature),excessive tallness (Tall stature), fatness(obesity), thinness and problems ofpuberty. Thus growth disorders may beclassified according to the following.
1.Stature – Short or tall
2.Weight – Obesity or thinness
3.Puberty – Delayed, early or secondarycharacters.
Short Stature
A short stature is defined as
(i) Height less than 2 StandardDeviations (2SD), or
(ii) Height is less than 3rd percentile ofstandard for child’s age and MPH(Mid-parental height) or
(iii) Growth velocity is low (< 5-6 cm/year from age of 3 years till onset ofpuber ty) based heightmeasurements (if measurementslikely to be accurate, and are over aperiod of at least 6-12 months).
Diagnosis of the child who is short andgrowing slowly comprises the whole of
Issues in Linear Growth in Children
Jaydeb RayProfessor, Department of Pediatrics, Institute of Child Health, Kolkata
pediatrics and is not just confined toendocrinal disorder. So it is a very vastfield. The parents would be worried aboutthe child’s height when,
(i) The child is too short for his parents(ie, below 2SD).
(ii) Growth prediction is too low (by mid-parental height [boys= (father +mother +12)/2; girls= (father -12+mother)/2]), the predicted height =mid-parental height ± 8 cm. TheMPH should be plotted on the properpercentile and this will be the centilethe child is likely to follow.
(iii) History does not account for thepresent situation.
(iv) Abnormal body proportion (abnormalupper/lower segment ratio or span/height ratio).
(v) Deceleration of the growth velocity.
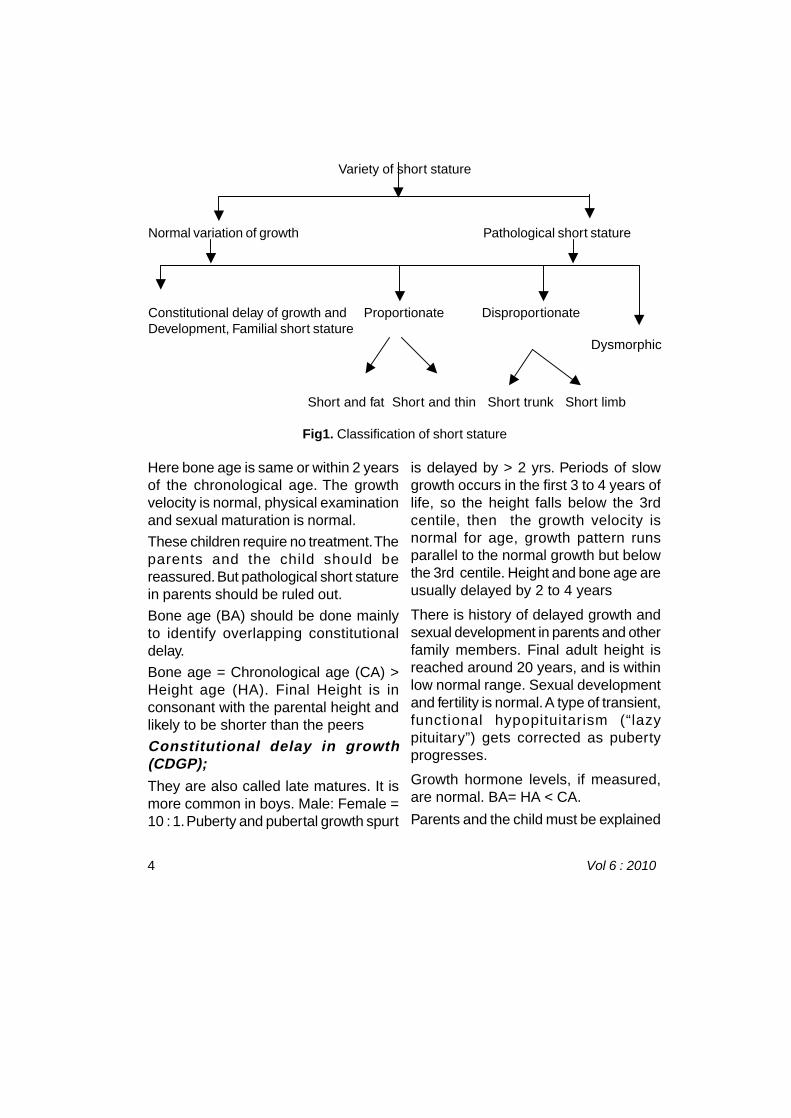
Short stature is classified as shown infigure1.
Normal Variations of Growth
Familial genetic short stature:
It is the most common cause of shortstature is due to low geneticendowment. Here the parents and/orclose relatives are shor t. Child’sprojected adult height falls within 2 SDof the MPH.
IJGDBP 3
Here bone age is same or within 2 yearsof the chronological age. The growthvelocity is normal, physical examinationand sexual maturation is normal.
These children require no treatment. Theparents and the child should bereassured. But pathological short staturein parents should be ruled out.
Bone age (BA) should be done mainlyto identify overlapping constitutionaldelay.
Bone age = Chronological age (CA) >Height age (HA). Final Height is inconsonant with the parental height andlikely to be shorter than the peers
Constitutional delay in growth(CDGP);
They are also called late matures. It ismore common in boys. Male: Female =10 : 1. Puberty and pubertal growth spurt
is delayed by > 2 yrs. Periods of slowgrowth occurs in the first 3 to 4 years oflife, so the height falls below the 3rdcentile, then the growth velocity isnormal for age, growth pattern runsparallel to the normal growth but belowthe 3rd centile. Height and bone age areusually delayed by 2 to 4 years
There is history of delayed growth andsexual development in parents and otherfamily members. Final adult height isreached around 20 years, and is withinlow normal range. Sexual developmentand fertility is normal. A type of transient,functional hypopituitarism (“lazypituitary”) gets corrected as pubertyprogresses.
Growth hormone levels, if measured,are normal. BA= HA < CA.
Parents and the child must be explained
Variety of short stature
Normal variation of growth Pathological short stature
Constitutional delay of growth and Proportionate DisproportionateDevelopment, Familial short stature Dysmorphic
Short and fat Short and thin Short trunk Short limb
Fig1. Classification of short stature
4 Vol 6 : 2010

that the child would continue to grow fora longer period than usual and ultimatelywill reach normal adult height.Testosterone can be used in older boyswhen delay in puber ty becomespsychologically unbearable.
Pathological Short Stature
Proportionate and heavy:
Generally endocrinal etiology is present.
(i) Congenital GH deficiency (?midlinedefects, perinatal asphyxia).
(ii) Acquired GH def. (tumors, trauma,post-infectious).
(iii) Hypothyroidism.
(iv) Cushing syndrome
Investigations according to the cause.TSH, FT4, IGF-1 and IGFBP3, boneage determination. For Cushing’ssyndrome consider overnightdexamethasone suppression test or 24hour urinary cortisol.
Proportionate and thin:
The list is endless.
(i) GI loss – Malabsorbtion, IBD, celiacdisease.
(ii) Renal – RTA, nephrogenic DI,chronic renal failure.
(iii) Cardiovascular –Shunts, failure.
(iv) Endocrinal – Diabetes mellitus,diabetes insipidus.
(v) Pulmonary – Cystic fibrosis,asthma.
Disproportionate short stature:
An abnormal upper/lower segment ratio
or span/height ratio indicatesdisproportionate short stature. Skeletaldysplasia is one of the impor tantinvestigations in this group.
Short trunk – In short-trunk dwarfism(Mucopolysaccaridosis etc), span isgreater than height, and US/LS ratio isdecreased
Short limb – In short-limbed dwarfism(Achondroplasia etc), the height isgreater than arm-span, and US: LS ratiois high.
Dysmorphic:
These are generally syndromic. Turnersyndrome, Down syndrome, etc.Karotyping and geneticist help isneeded.
During the assessment of a short childthe following thing has to be taken
(i) Full medical and social history
(ii) Accurate measurement of height ofchild and parents (for accurateheight, growth velocity and midparental height).
(iii) Good observation and thoroughclinical examination andinvestigation
(iv) Bone age, chronological age, heightage and body propor tionassessments((upper / lowersegment ratio and arm-span / heightratio)
(v) Karyotyping in specific cases
(vi) Specific investigation according tothe systemic disease.
IJGDBP 5

(vii)Biochemical investigation and
(viii)Endocrinal tests accordingly.
Outcome and treatment:
The outcome and treatment of the shortstature will depend upon the cause.
(i) Familial genetic shor t stature,constitutional delay in growth(CDGP) and most causes ofintrauterine growth retardation – Nospecific treatment, onlyreassurance.
(ii) Skeletal dysplasias – Limblengthening with limited benefit.
(iii) Specific therapy for chronicsystemic disorder, emotionaldeprivation is associated good catchup.
(iv) Growth hormone is indicated inchildren with growth hormonedefiency.
(v) Hypothyroidism should be managedwith replacement by thyroxin. .
Prognosis:
(i) Normal and short – Do not needtreatment.
(ii) Short due to intrinsic causes –Cannot be treated.
(iii) Remediable cause of short stature/growth failure – Can benefit fromtreatment.
Tall Stature
Tall stature and excessive overgrowthsyndromes represent physical
development in excess of 2 standarddeviations (SD) above the mean for theperson’s age and gender. The incidencevaries greatly depending on theetiologies. Following are the causes oftall stature.
Normal variation:(i) Familial tall stature
(ii) Increased caloric intake
Pathologic:(i) Marfan syndrome
(ii) Homocystinuria
(iii) Klinefelter syndrome
(iv) Precocious puberty
(v) Cerebral gigantism (Soto’ssyndrome)
(vi) Pituitary gigantism and acromegaly
Approach to tall stature withoutabnormal featuresIf growth velocity is normal, withadvanced bone age it may be due tofamilial tall stature, or due to increasedcaloric intake. Normal look, increasedgrowth velocity and without sign ofpubertal growth could have growthhormone excess or hyperthyroidism.Approach to tall stature withoutabnormal features is shown in figure 2.
Familial tall stature:
Familial tall stature is the commonestcause of excessive height. Height ofthese individuals is usually aboveninety-fifth percentile since earlychildhood, and their height velocity iswithin normal limits. Physical
6 Vol 6 : 2010

TALL STATURE
without abnormal feature
Growth velocity
Normal Increased
Familial tall stature Increased caloric intake (obesity)
Is there any sign of puberty?
NO YES Growth hormone excess or
hyperthyroidism.
Investigate
examination and bone age are normal.One or both parents are usually tall.Diagnosis can be made from historyincluding family history, normal physicalexamination and bone age, and growthrecord.
Increased caloric intake:
Many children who are overweight
Fig 2.Approach to tall stature without abnormal features
because of increased caloric intake alsohave height that is more than ninety-fifthpercentile for age and gender. In thiscircumstance, increased caloric intakecontributes to increased height.
Without abnormal feature withincreased growth velocity:
Precocious puberty – In children with
IJGDBP 7

precocious sexual development,excessive androgen or estrogensecretion causes accelerated growthand evidence of either virilization orfeminization. Bone age is advanced.Although accelerated growth results intall stature in childhood, prematureclosure of epiphyses limits growthperiod, producing attenuation of finaladult height
Approach to tall stature with abnormalfeatures is shown in figure 3.
Approach to tall stature withabnormal features not dispropor-tionate
Cerebral gigantism (Soto’sSyndrome):
Autosomal-dominant disorder, birthlength is typically above ninetiethpercentile. Characteristic findingsinclude macrocephaly, prominentforehead and jaw, hypertelorism, downslanting palpebralfissures, high-archedpalate, developmental delay, seizures,and mental retardation. Although growthmay be accelerated in first years of life,final height may not be excessive.Growth hormone secretion and othertests of endocrine function are normal.Physical findings and growth patternconfirm diagnosis.
Pituitary gigantism and Acromegaly:
Pituitary tumors (usually eosinophilic orchromophobe adenomas) andeosinophilic hyperplasia withoutadenoma produce excessive amountsof growth hormone, which cause
gigantism. Final height is 213–275 cm(83–108 in.). Acral changes includecoarse facial features with enlargementof nose, ears, and jaw; soft tissueswelling; and striking increases in sizeof hands and feet. Screening test forgrowth hormone excess is increasedserum concentration of insulin-likegrowth factor-1. CT or MRI defineslocation and extent of lesion. Histologicdiagnosis is definitive.
Approach to tall stature withabnormal features disproportionate
Marfan syndrome:
Autosomal-dominant disorder causedby mutations in fibrillin-1 gene locatedon chromosome15. Most importantclinical features are in skeletal,cardiovascular, and ocular systems.Skeletal features include increasedheight, disproportionately long limbs anddigits, joint laxity, scoliosis, thoraciclordosis, pectus excavatum orcarinatum, and narrow high-archedpalate. Cardiovascular findings includemitralvalve prolapse, mitral regurgitation,aor tic root dilatation, and aor ticregurgitation. Subluxation of lens(usually upward) and myopia arecharacteristic ocular findings. Clinicalfindings and positive family history whenavailable confirm diagnosis.
Homocystinuria:
Most common form of this autosomal-recessive disorder is due to decreasedactivity of enzyme cystathionine beta-synthase, which catalyzes formation of
8 Vol 6 : 2010

cystathionine from homocysteine andserine. Gene locus has been mappedto chromosome21q22.3. Clinicalfeatures include long limbs, narrowhands with long fingers, limited jointmobility, subluxation of lens (usuallydownward), osteoporosis, thrombosesof arteries and veins, and develop-mental delay. Some children with thisdisorder are taller than average.Increased serum concentrations ofhomocysteine and methionine arediagnostic. Enzyme assay of culturedfibroblasts is confirmatory.
Klinefelter syndrome:
Underlying defect in Klinefelter
syndrome is presence of extra Xchromosome in a boy. Diagnosis isusually made after the time of expectedpuberty. These individuals have smalltestes, decreased facial and axillaryhair, and often gynecomastia.Karyotype 47, XXY is diagnostic.
Diagnostic approach to tall stature
History and examination:
1. Family history
2. Parents’ heights and puberty agesto judge child’s growth relative togenetic potential (midparental targetheight); family history of chronicdisease or endocrinopathy.
TALL STATURE
With abnormal features
DISPROPORTIONATE WITHOUT DISPROPORTIONATE
Pituitary gigantism and acromegaly
Cerebral gigantism (Soto’s Marfan syndrome Klinefelter syndrome Homocystinuria
Fig 3. Approach to tall stature with abnormal features.
IJGDBP 9

3. History of pubertal signs.
4. Signs of tumor – Headache,behavioral, visual problems.
5. Symptoms of impaired secretion ofgonadotropins and thyrotropincorticotropin, or hyperprolactinemia.
6. Vital signs,
7. Anthropometry (height, weight,sitting height)
8. Features of acromegaly – Coarseface, broad nose, separate teeth,increased mandible growth, dorsalkyphosis, enlarging hands and feetwith thickening fingers and toes,visual field defects
9. Tanner staging for puber talassessment.
Laboratory tests:
1. Bone age X-ray to predict finalheight.
2. IGF-I is most sensitive screen forGH excess.
3. Karyotype in male patients.
4. Thyroid function tests.
5. Gonadotropins and sex hormonelevels if puberty abnormal.
6. Glucose suppression test –Suppress serum GH to <5 ng/dLafter 1.75 g/kg oral glucosechallenge, gold standard for verifyingGH excess.
7. MRI evaluation of pituitarymandatory if evidence of GHexcess
1. Behrman RE, et al., eds. Nelson Textbookof Pediatrics, 16th ed. Philadelphia: WBSaunders, 2000.
2. CDC Growth Charts: United States.Hyattsville, MD:US Department of Healthand Human Services, Centers for DiseaseControl and Prevention, National Center forHealth Statistics, Division of Data Services,2001. World Wide Web URL: http://www.cdc.gov/growthcharts.
3. Jones KL. Smith’s Recognizable Patternsof Human Malformation, 5th ed. Philadel-phia: WB Saunders, 1997.
4. Online Mendelian Inheritance in Man(OMIM). McKusick-NathansInstitute for Ge-netic Medicine, Johns Hopkins University(Baltimore,MD) and National Center for Bio-technology Information, NationalLibrary ofMedicine (Bethesda, MD), 2000. World Wide
Web URL: http://www.ncbi.nlm.nih.gov/omim.
5. Reiter EO. The “too tall” child.Pediatr Rev1983; 5: 119-26.
6. Rudolph AM, ed. Rudolph’s pediatrics,20thed, Stamford, CT: Appleton & Lange,1996.
7. Sotos JF, et al. Cerebral gigantism in child-hood: asyndrome of excessively rapidgrowth with acromegalic features andanonprogressive neurologic disorder. N EnglJ Med 1964;271:109-16.
8. Sperling MA, ed. Pediatric endocrinology.Philadelphia:WB Saunders, 1996.
9. Tanner JM, Davies PSW. Clinical longitudi-nal standardsfor height and height velocityfor North American children. JPediatr1985;107:317-29.
10 Vol 6 : 2010

Predictrs of Outcome in High Risk Neonates
Suchit TamboliDevelopmental Pediatrician, Ahmednagar
More and more smaller and sickerneonates are surviving over the pastthree decades with improved treatmentmodalities. Concurrent advances inreproductive technology have resultedin increasing numbers of preterm andmultiple births. These high risk neonatesaccount for infant mortality and morbidityand evidence shows that despite theneonatal interventions very low birthweight (VLBW) remain at a substantialrisk for long-term morbidity includingcerebral palsy, mental retardation,developmental delay, school problems,behavioral issues, growth failure andoverall poor health status1.
Outcome refers not only to initial 2 yearsbut also includes school age,adolescence and adult life. Focus ismoving from very VLBW to extremelylow birth (EBLW) and now to extremelyimmature infants (< 25 weeks gestation)because with decreasing birth weightand gestational age more severe anddifferent morbidities have becomeapparent2.
Last two decades have seentremendous interest in neonatalintensive care all over India but sadlyvery little attention has been paid to lessglamorous care such as systematicfollow up of high risk infants. Some of
the most elegantly done follow up studiesin India are ‘Pune Children’s Studies’ byChaudhari et al on children born in lateeighties3. However neonatology in Indiahas taken great strides in last 10 yearsand hence there is a need to continueto correlate neonatal risk factors andinterventions with long term outcomesto help us improve our strategies andalso understand cost-efficacy of thisexpensive care. This article is anoverview of predictors of long termoutcome of a high risk neonate who isexposed to perinatal stress.
Antenatal Predictors
Ultrasound and Doppler examina-tion:
Abdominal circumference below fifthpercentile predicts immediate outcome.The best antenatal predictor of pooroutcome was abnormal venous flow,based on the DV Doppler. At five yearsof age 54% of children born after raisedumbilical / cerebral or U/C ratio werefunctioning below the expected level,compared to 20 % of children born withnormal U / C ratio. There is associationbetween abnormalities in the fetal aortaDoppler studies and minor neurologicaldisability4.
Maternal diseases and antenatal
IJGDBP 11

steroids:
Preterm born to mother withpreeclampsia do better because theyhave less IVH and PVL but in contrastpreterm infant exposed to chronicchoriamniotis and elevated pro-inflamatory cytokines in amniotic fluidhave increased risk of PVL and CerebralPalsy5. Single dose of antenatal steroidsis well known to prevent RDS howeverfetal exposure to multiple / weeklycourses of steroids is known to resultinto smaller head size6. Multiple prenatalfactors like infection, metabolic, anoxia,toxic, genetic, infarction etc may resultinto spastic Cerebral Palsy.
Natal Predictors
Birth asphyxia:
Drage et al. found that 5 minutes Apgarscore gave a better prediction forneurological abnormality later on andpost asphyxial encephalopathy grade IIIcould predict significant morbidity andsequelae among survivors. Aninteresting finding from a largeprospective NCPP study at USA andcase control study done at westernAustralia have conclusively shown thatnot more than 10% of cerebral palsycases were at best related to birthasphyxia. Sigmund Freud whosuggested that the baby may haveasphyxia primarily because of a prenatalstructural or metabolic insult to the baby‘s brain and that asphyxia is only amiddle episode of a long drama startingwith intrauterine asphyxia and
presenting with a low Apgar score andneurological deficit later on7.
Postnatal Predictors
Birth weight:
Birth weight > 800 grams seems to beone of the good predictors of intactsurvival. However the developmentaloutcome of ELBW infant is determinedby a complex interaction of medical andenvironmental factors acting on thedevelopmentally vulnerable prematurebrain. 7-17 % has neuro sensoryimpairment and 13-37 % delays incognitive function and also quite highrate of behavioral problems. Since 2000there is net increase in survivors withoutimpairment however the rates ofsubnormal cognitive function continue toremain unchanged1. VLBW and ELBWchildren have more respiratory illnessesleading to hospital readmissions andother health problems in initial years1 butthose extremely premature enteringadulthood showed no significantdifferences between the ELBW adultsand term-born controls with regards torates of high school graduation, collegeenrollment permanent employment andindependent living status2.
Prematurity:
The greater the immaturity and the lowerthe birth weight, the greater the likelihoodof intellectual and neurologic deficit. 50%of 500-750g infants have a significantneurodevelopmental impairment(blindness, deafness, mentalretardation, cerebral palsy.)
12 Vol 6 : 2010

With increasing gestational age, survivalrates increase to approximately 15% at23 week , 56% at 24 week , and 79% at25%. The survival of infants <24weekgestation, weighing <750g with a 1- minApgar score <3 is 30% . These infantsare also at risk for poorneurodevelopmental outcome . Birth-weight – specific neonatal diseasessuch as grade III IVH , severe group Bstreprococcal pneumonia , andpulmonary hypoplasia also contribute toa poor outcome10.
Cerebral palsy :
Children with ‘transient dystonia’ had anexcess of school problems at a meanage of 6.7 years8.
The developmental outcome of ELBWinfant is determined by a complexinteraction of medical and environmentalfactors acting on the developmentallyvulnerable premature brain. 7-17 % hasneuro sensory impairment and 13-37 %delays in cognitive function. Disabilityrate as high as 49 % is reported1.Spastic diplegia is most commonlyassociated with pre-term birth.
Cerebral Palsy is caused by not onlyprematurity or low birth weight but aseries of life threatening medical events.Spastic Cerebral Palsy is caused byprenatal factors like infection, metabolic,anoxia, toxic, genetic, infarction .Ataxiccerebral palsy is caused by perinatalcause such as anoxia. Atonic cerebralpalsy is caused by post natal factorssuch as toxin ,trauma, infection.(7)
Many surviving LBW infants havehypotonia before 8 mo corrected age,which improves by the time they are 8mo-1yr old. This transient hypotonia isnot a poor prognostic sign10.
School age outcome of prematurechildren consists of significantly poorerintelligence, achievement and higherrates of behavioral problem. Thesescores are directly proportional to thedegree of immaturity. Problems can bepoor vocabulary skill, significant delayin reading, spelling and mathematics.The problems that appear to be relatedto academic failures include deficits inattention; memory and behavior areaffected in preterm, ELBW babies1.
Hypoxic ischemic encephalopathy:
Ataxic cerebral palsy is caused byperinatal cause such as anoxia. Itcauses severe motor disability. Theyhave poor score on cognitive,neuropsychological, educational andbehavioral assessments even with nofunctional motor deficit; memory andattention or executive functions wereimpaired in severe groups. There isdifficulty with language, spelling, letterrecognition, visual and short termmemory. ELBWchildren perform poorlyon tests of visual- motor performancebut are closer to controls on measuresof language9.
Hearing impairment:
Hypoxia damages the hair cells of thecochlea and hearing impairment is oftendue to hypoxia ischemia9.
IJGDBP 13

Seizures:
HIE grade III is associated with seizuresand is a bad prognostic factor for longterm intact neurology.
IVH, PVL:
Although incidence of periventricularhemorrhage has decreased, the ratesof PVL remained unchanged thusleading to adverse neurologicaloutcome. Isolated visual impairment canrarely be seen as a consequence ofPVL.
RDS, BPD, PDA :
Complications of RDS like asphyxia,cardiac arrest affect neurodvelopmentaloutcome. RDS may be associated withPDA. Delayed closure of the PDA isassociated with hypoxia, acidosis,increased pulmonary pressuresecondary to vasoconstriction,systemic hypotension, immaturity, andlocal release of prostaglandins, whichdilate ductus. There is a relationshipbetween early adrenal insufficiency,ductal patency , airway inflammationand the development of BPD. VLBWinfants with PDA are at increased riskof more prolonged and more severeRDS , bronchopulmonary dysplasia anddeath due to progressive respiratoryfailure. Although 85 to 90 % of all infantssurviving RDS after requiring ventilatorysupport with respirators are normal , theoutlook is much better for thoseweighing more than 1500 gm. The longterm prognosis for normal pulmonaryfunction in most infants surviving RDS
is excellent. Survivors of severeneonatal respiratory may havesignificant pulmonary andneurodelopmental impairment10.Somehow pulmonary hemorrhage doesnot seem to be associated withincreased long term morbidity.
NEC:
Premature infants with NEC who requiresurgical intervention or who haveconcomitant bacterimia are at increasedrisk for adverse growth andneurodevelopmental outcome10.
Hyperbilirubinemia:
Disruption of the blood brain barrier bydisease, asphyxia, and maturationalchanges in blood brain barrierpermeability affect risk. The preciseblood level above which free bilirubin istoxic for an individual infant isunpredictable ,the duration of exposureneeded to produce toxic effects isunknown .The more the preterm theinfant the greater the susceptibility tokernicterus. The commonest outcomeknown is athetoid cerebral palsy10.
Renal injury in asphyxiated newborn:
Oliguria in the perinatal period is asensitive indicator of infants at risk forlong term neurologic deficits. Oliguriawas significantly associated with clinicalsigns of HIE, including seizures, deathand long term neurological deficits.
Sepsis:
There is association between infectionand brain injury, including severe
14 Vol 6 : 2010

intraventricular hemorrhage andperiventricular leukomalacia. This leadsto poor neurodevelopmental outcome.Elevated peripheral neutrophil counts inthe first 96 h of life in term infants withHIE may contribute to abnormalneurodevelopmental outcome. Neonatalinfections among ELBW infants areassociated with poor neuro-developmental and growth outcomes inearly childhood11. Atonic cerebral palsyis caused by post natal factors such astoxin ,trauma, infection7.
Hypoglycemia:
Both premature and full term infants areat risk for serious neurodevelopmentaldeficits from equally low glucose levels.The risk is related to the depth andduration of hypoglycemia.Earlydiagnosis and treatment of neonatalhypoglycemia is crucial to prevent futureneurological sequelae. Even in theabsence of gross hypoglycemicencephalopathy it can be cause ofepilepsy even in full term babies due todelayed feeding which has beenelegantly described by Udani et alAggressive correction of hypoglycemiais more impor tant in presence ofadditional perinatal risk factors12,13.
Treatment Modalities in a High RiskNeonate
Surfactant treatment:
In surfactant treated neonates moderateand severe pulmonary haemorrhage isassociated with an increased risk ofdeath and short term morbidity. Long
term morbidity not affected.
Role of ventilation:
The prognosis of ELBW with ‘protectedlong term’ Ventilation remains grim.Those intubated have diminishedsurvival and high rates of impairment.Parents of these infants should beinformed of changes in prognosis as thetime of ventilation increases.Severehyperoxaemia and severe hypocapniawere associated with adverse outcomein infants with post-asphyxial HIE.During the first hours of life, oxygensupplementation and ventilation shouldbe rigorously controlled14.
Early HFOV when used with a lungrecruitment strategy in combinationwith surfactant replacement mayameliorate acute neonatal lung injurythat predisposes some preterm infantsto develop chronic lung diseases15.
Role of inhaled nitric oxide:
The results of NO inhalation are verypromising. Use of NO has improvedneurodevelopmantal outcomes at twoyears of age. Inhaled nitric oxidedecrease the risk of chronic lungdisease and death, as well as of severeintraventricular hemorrhage orperiventricular leukomalacia16.
Hyperoxia:
Exposure to the extra uterineenvironment to high inspired oxygenconcentrations produces cellulardamage due to free radicle release andis a well known cause of retinopathy of
IJGDBP 15

prematurity (ROP), however lower thegestational age, lower the birth weight,and the sicker the infant add to the riskis for ROP10.
Environment, socioeconomic status,parental education and nutrition, aspredictors of outcome:
While under nutrition is harmful, overnutrition seems to harm lower birthweight in adult life. Studies all oversuggest, that environment certainlycontributes in the long run which hasbeen shown by Dr Chaudhari et al in her“Pune children Studies- Biology vsEnvironment”1. Bavdekar et al from Punehave shown that a combination of smallsize at birth, followed by acceleratedweight gain during childhood appearedto be responsible for an increased riskof insulin resistance in prepubertalchildren consistent with earlier findingsby Barker et al4. Combination of perinatalrisk factors and non optimal rearingconditions can lead to poordevelopmental outcome, where as goodrearing conditions can ameliorate therisk. Low social class is a frequentlyused index of non optimal rearingenvironment because of the associatedsocial and economic disadvantages.Poor social class is powerfuldeterminant of intellectual status inpreterm infants.
Conclusion
Short term outcome and 2 yearsoutcome are predicted by combination
of BPD, PDA, IVH, PVL, RDS, NECetc. The more the diagnoses an infanthas the more severe those diagnosesthe more likely that infant show adverseresponse on assessment at 18 to 24months. Early outcomes do not reliablypredict school age performance,behavioral problems, specific learningdisabilities etc and studies have shownadverse outcomes have remainedunchanged over last 2 decades.Therefore the need for a multidisciplinaryfollow up clinic under guidance of aneonatologist cannot beoveremphasized which should beexplained to the parents duringdischarge planning from NICU. Earlyinterventions in such clinics are aimedat minimum disability and canrehabilitate the child but can not givecure. Therefore enhancing therecognition of high risk pregnancies,developing strategies to prevent pretermbirths, increasing maternal transports tolevel III prenatal centers, improvingneonatal transport facilities to ensureprevention of hypoxemia andhypoglycemia and broadening thescope and availability of prenatal careto periphery will lead to better neonatallong term outcome. More attention maybe paid to hypo/hyper oxemia and alsohypocarbia and better infection control.Areas of research include usage of nitricoxide, optimal nutrition and earlyintervention programs for rehabilitationof children with adverse outcomes.
16 Vol 6 : 2010

1. Wilson–Costello d. Is there evidence thatlong term outcomes have improved withintensive care?; Seminars in Fetal andNeonatal Medicine2007; 12, 344-54.
2. Saigal S, Rosenbaum P. What matters inthe long term : Reflections on the context ofadult outcomes versus detailed measuresin childhood ; Seminars in Fetal andNeonatal Medicine 2007;12, 415-22.
3. Chaudhari S, Otiv M, Chitale A,HogeM,Pandit A, Mote A. Pune Low Birth WeightStudy – Cognitive Abilities and EducationalPerformance at Twelve years; Indian Pediatr2004: 41:12.
4. Breeze ACG, Lees CC. Prediction andperinatal outcomes of fetal growthrestriction; Seminars in Fetal and neonatalMedicine 2007; 12, 383-97.
5. Editorials. Predictors of outcomes in preterminfants: Which ones and when? ; J PediatrFeb.2001;138(2):153-5.
6. Bonanno C, Fuchs K. Wapner RJ. ; Singleversus repeat courses of antenatal steroidsto improve neonatal outcomes : risks andbenefits; Obstet Gynecol Surv. 200762(4):261-71.
7. Nair MKC,Pejavar RK.Birth asphyxia andcerebral palsy;Child development 2000 andbeyond; Prism Books ;2000;9-14.
8. Fawke J. Neurological outcomes followingpreterm birth; Seminars in Fetal andNeonatal Medicine2007; 12:374-82.
9. Rennie JM, Cornelia F, Hagmann NJ.
Robertson; outcome after intrapartumhypoxic ischaemia at term; Seminars inFetal and Neonatal Medicine 2007;12: 398-407.
10. Kliegman.Beherman.Jenson.Stanton; Thenew born infant; Nelson Textbook ofPediatrics ; Elsevier 2007; (1) 679-713.G.
11. Adams-CI, Stoll BJ. Neonatal infection andlong-term neurodevelopmental outcome inthe preterm infant; Curr Opin Infect Dis.2006; 19(3):290-7.
12. YalnizogluD,HaliloguG, Turanli G.Neurological outcome in patients with MRIpattern of damage typical for neonatalhypoglycemia ;Brain development 2007; 29(5) : 285-92.
13. Udani V.Pediatr ic epilepsy-an Indianperspective; Indian J Pediatr.2005;72(4):309-13
14. Beyene KJ, Shah P, Periman M. Dohyperoxaemia and hypocapnia add to therisk of brain injury after intrapartumasphyxia? Arch. Dis. Child. Fetal NeonatalEd. 2005;90:49-52.
15. Gerstmann DR, Wood K, Miller A et al.Childhood Outcome After Early High –Frequency Oscillatory Ventilation forNeonatal Respiratory Distress Syndrome ;Pediatr 2001,108 (3):617-623
16. Mestan AKL, Marks JD , Hecox K, Huo D,Schreiber MD. NeurodevelopmentalOutcomes of premature infants treated withinhaled nitric oxide ; N. Engl J Med 2005 ;353:23:32.
IJGDBP 17

Transient Tachypnea of Newborn : A Preventable Impediment forNeonatal Growth and Development
Raktima ChakrabartiFellow, Department of Neonatology, University Children’s Hospital,Friedrich-AlexanderUniversity at Erlangen-Nürnberg,Germany.
Introduction
There are multiple factors responsiblefor the growth of human during neonatalperiod. This period is of immenseimportance with respect to the growthand development at later life. Neonatalgrowth is dependent on prenatal growthwhich in turn depends on maternalnutrition, maternal anthropometry, insulinand insulin like growth factor-2 andnormal placental function1. Duringpostnatal period it is dependent onthyroid hormone, growth hormone,insulin like growth factor-1, nutritionalfactor, energy expenditure, neonatalcare etc2. Neonates are prone to differenttype of morbidities which influence theirenergy expenditure and growth. Whenbabies are delivered normally at fullterm, there is very less risk of sufferingfrom any unwanted phenomena. Butnowadays there is an increasing trendof elective cesarean section; sometimesit is due to obstetrician’s decision andsometimes according to the choice ofthe prospective mothers and families. Inmany cases, this method of delivery canbe avoided which can lead to smootherneonatal and infantile course. In thisarticle, I want to report three full termneonates, delivered by electivecesarean section, had stormy neonatallife due to transient tachypnea of new
born (TTN). Normally this problem doesnot create much problem and lasts onlyfor 48-72 hours3, but that is not theuniversal rule and an unexpecteddisease course was experienced inthese present cases. Moreover, in thesecases, there was no other diagnosedgenetic or maturational problem, birthasphyxia, metabolic disorder, maternaldiabetes or any other ailments which canbe blamed for giving rise to suchcircumstances. They were required toget admitted in neonatal intensive careunit (NICU) with symptoms of TTN withsevere respiratory distress and neededto be mechanically ventilated.Mechanical ventilation itself is a riskfactor for developmental delay and alsoother morbidities which independentlyhampers neonatal and infantile growthand development4. So in these cases theunwanted outcome could be avoided justby allowing the babies to be deliverednormally. But these cases can act aseye opener to learn to prevent such typeof upshot.
Case Presentations
Case 1:
One male full term newborn wasdelivered by elective caesarean sectionand on the first day of life only, developedincreasing respiratory insufficiency with
18 Vol 6 : 2010

severe tachy-dyspnoea. He was shiftedto NICU. After a brief treatment attemptwith continuous positive airwaypressure (CPAP), endotrachealintubation was imminent. On the secondday of life his chest X-ray revealed apicture similar as respiratory distresssyndrome grade II (withairbronchogram). The necessity of highpressure ventilation (PIP-30 mm hg) andpoor oxygenation indicated the therapywith surfactant (curosurf @ 200 mg/kg).After the application of surfactant andhigh frequency oscillatory ventilation(HFOV) [Initial setting: Mean airwaypressure 16, amplitude 28, frequency10Hz, FiO2 40%] the respiratorysituation improved gradually. On the 12thday of life he was extubated to CPAPbut within 2 days he required to be re-intubated as his requirement of FiO2increased gradually and respiratorydistress was visible. Blood gas was alsoshowing acidotic picture. He was putunder synchronized intermittentmandatory ventilation (SIMV) with mildsetting and required to be mechanicallyventilated 3 more days. Ultimately duringthe 3rd week of life he could besuccessfully extubated and the repeatchest X-ray showed a normalized view.On the 25th day of life he wasdischarged from NICU without anyfurther problem.
Case 2:
The second baby was a full term femalenewborn presented with respiratoryinsufficiency shortly after birth. She was
shifted to NICU and chest X-ray wasdone which showed a mediastinal andapical pneumothorax of the left lung anda picture similar to respiratory distresssyndrome grade I. By applying CPAPher condition did not improve. Ultimatelyafter endotracheal intubation,mechanical ventilation (SIMV) andapplication of surfactant the situationimproved (initial setting PIP - 22, PEEP– 7, Flow 10, FiO2 30%, rate – 60/min,Ti – 0.33 sec., Te – 0.67 sec.). Thepneumothorax was reabsorbedspontaneously. She could be extubatedby 10th day of life. Later her clinicalcourse was problem free.
Case 3:This mature male newborn developed asevere respiratory distress syndromedirectly after birth. He was shifted toNICU for respiratory assistance.Endotracheal intubation was necessaryas he was non responsive to CPAP. Afterintroduction of conventional mechanicalventilation (SIMV) his respiratorycondition improved for a short period butdeteriorated again demanding highfrequency ventilation. The chest x-rayshowed fluffy opacities all over the lungs.Some areas of lungs were hyper aeratedwith prominent vascular marking aroundthe hila. Ultimately he improved withHFOV. On the 7th day of life he could beextubated without any fur thercomplication.
These three cases showed the exampleof extreme end of the picture of transienttachypnea of the newborn.
IJGDBP 19

Discussion
TTN is also known as delayed clearanceof fetal lung fluid. It was first describedby Avery and co-workers in 19665. In thissituation, lungs are filled with fluid (20-30ml/kg body weight) instead of air andthis fluid is quite distinctive from amnioticfluid or plasma6.
In order to the fetus to complete thetransition from intrauterine to extrauterine life, the lungs must clear this fluidsoon after birth. The process of clearingliquid from the lungs actually begins 2-3days prior to birth with a decrease in therate of secretion of fetal lung fluid.However, the lung-liquid begins to clearin earnest with the onset of labor7. It wasreported from previous study that nearlytwo third of the total clearance of liquidthat occurs during transition fromintrauterine to extra uterine life, occursduring labor. With the onset of labor, thepulmonary epithelium changes from achloride secreting membrane to asodium absorbing membrane, withreversal of the direction of flow of lungliquids. This change is an activemetabolic process involving increasedsodium potassium adenosinetriphosphatase (Na+- K+- ATPase)activity in the epithelial cells and servesto drive liquid from the lung lumen intothe interstitium and also mediated inlarge part by transepithelial sodium (Na)reabsorption through amiloride-sensitiveNa channels in the alveolar epithelialcells, with some contribution frommechanical factors and Starling forces8.
In addition, as lung liquid contains verylittle protein, oncotic pressure alsofavours the movement of water from theair space back into the interstitium andfrom there into the vascularcompartment9-12.
Greater likelihood of caesarean sectionhas been associated with TTN. Alongwith that, risk of respiratory distresssecondary to TTN, surfactantdeficiency, and pulmonary hypertensionis also increased8. Previous reportsshowed that infants not exposed tovaginal compression, have excessivelyhigh volumes of interstitial and alveolarfluid for the first few hours, thoughthoracic volume remains within normalrange; - i.e. liquid volume is increasedwhereas gaseous component isdecreased after caesarean section13. Soinfants born without labor do not havethe opportunity for early lung liquidclearance and begin their extra uterinelife with excess water in their lungs.
Newborn babies with TTN often arehypoproteinemic and decreased plasmaoncotic pressure may delay the directabsorption of water into the bloodvessels14. Babies with this diagnosiscan have elevated pulmonary vascularpressure and ventricular dysfunctionwhich again can raise central venouspressure and impair thoracic ductfunction and also the removal ofinterstitial water by lymphatics. Increaseof pulmonary vascular pressure givesrise to a decrease in cardiac out put. Asthe accumulated liquid compresses the
20 Vol 6 : 2010

compliant airways and causeobstruction, the infants developrespiratory distress. In TTN, on chest X-ray, some par ts of lungs showhyperaeration due to gas trapping as aresult of airway obstruction. The babiesdevelop hypoxia due to continuedperfusion of poorly ventilated lung units;also hypercarbia develops frommechanical interference with alveolarventilation and from central nervoussystem depression. Blood gas analysisreveals respiratory acidosis whichsupports the presence of hypercarbia.
Though generally this condition does notlast for longer time, but in some casesrespiratory assistance in the form ofCPAP, SIMV or HFOV is required.Sometimes surfactant is also requiredto treat the emergency situation ofrespiratory distress. Though initially itwas speculated that structural mutationof surfactant protein B (polymorphismsof intron 4 and heterozygous 121 ins 2mutation) is associated with thiscondition, no such relation was found butrelation with caesarean section and maleinfants were established15. So,surfactant washout or surfactantinactivation is responsible for therespiratory distress and exogenoussurfactant administration leads to asuccessful treatment outcome.
Some of the babies with this conditionrequire mechanical ventilation. A numberof respiratory and non respiratorycomplications stem out of this treatmentmodality. Among the respiratory
complications, airway injury, chronicpulmonary disorders, air leak arenoteworthy. Mechanical ventilation alsocan give rise to infection, feedingintolerance, intraventricularhaemorrhage, developmental delay. It ispostulated that standard technique ofapplying positive pressure ventilationmay itself lead to impaired alveolargrowth, although the effect is enhancedby concomitant respiratory distress16.Again newborn infants’ energyexpenditure increases greatly bydifferent co morbidities and to someextent by mechanical ventilation17. Fornormal growth, a full term infant’srequirement increases gradually till theend of the second week of life andreaches to an optimum level of 100-120kcal/kg/day18. With infection, increasedrespiratory work during distress andventilation this requisite becomesseveral fold higher but at the same timethese situations give rise to feedintolerance. So for appropriate nutritionaldelivery, central venous line placementbecomes essential which again is oneof the route causes of infection. Soultimately a vicious cycle develops.
Long term follow-up study showedlearning and school performanceproblem, growth and neuro-developmental delay in those childrenwho were under mechanical ventilationfor long time or developed broncho-pulmonary-dysplasia19. Delayed onsetof regular respiration is also a risk factorfor cerebral palsy, mortality and growth
IJGDBP 21

delay20.
So it can be said that frequentcaesarean section which are performednowadays can give rise to suchunwanted and preventablecomplications which can act as ahindrance for normal development ofthose term neonates.
To be more precise, caesarean sectionis often performed without any strictmedical indication. This is a clear riskfactor for development of transitorytachy-dyspnoea with respiratorydistress in mature babies. Severe
pneumothorax can also occur in thosecases due to strong shear forces.
But all these ailments are preventable.So it needs to be emphasized, that therisks of caesarean section have to becarefully discussed with the parents anda stringent guideline for its realindications has to be defined. Probablythis can prevent the NICU admissionafter caesarean section “without medicalindication”. This policy can improve thegrowth and development of normal fullterm neonates without posingunnecessary impediment.
1. Rudolf M. Growth: normal and abnormal, in:MRCPCH master course volume 1, 1stedition, Churchill Livingstone Elsevier. 235-261.
2. Rose SR. Thyroid Disorder, in: Fanaroff andMartin’s Neonatal Perinatal Medicine-Diseases of the Fetus and Infant, volume 2,8th edition, Elsevier Mosby. 1523-1550.
3. Miller MJ, Avroy A. Fanaroff, Martin RJ.Respiratory Disorders in Preterm and TermInfants. In: Fanaroff and Martin’s NeonatalPerinatal Medicine-Diseases of the Fetusand Infant, volume 2, 8th edition, ElsevierMosby. 1122-1146.
4. Spitzer AR, Greenspan JS, Fox WW.Positive-pressure Ventilation: Pressure-limited and time-cycled Ventilation. In:Assisted Ventilation of the Neonates, 4thedition, Saunders Elsevier. 149-169.
5. Avery ME, Gatewood OB, Brumley G.Transient tachypnea of newborn. Possibledelayed resorption of fluid at birth. Am J DisChild. 1966 Apr; 111(4):380-5.
6. Adamson TM, Boyd RD, Platt HS, Strang
LB. Composition of alveolar liquid in thefoetal lamb. J Physiol. 1969 Sep;204(1):159-68.
7. Welty S, Hansen TN, Corbet A. Respiratorydistress in the Preterm Infant, in: Avery’sDiseases of the Newborn. 8th edition,Elsevier. 687-703.
8. Jain L, Dudell GG. Respiratory transition ininfants delivered by cesarean section.Semin Perinatol. 2006; 30(5):296-304.
9. Berthiaume Y, Staub NC, Matthay MA. Beta-adrenergic agonists increase lung liquidclearance in anesthetized sheep. J ClinInvest. 1987;79(2):335-43.
10. Bland RD. Lung liquid clearance before andafter birth. Semin Perinatol. 1988; 12(2):124-33.
11. Bland RD, Nielson DW. Developmentalchanges in lung epithelial ion transport andliquid movement. Annu Rev Physiol. 1992;54:373-94.
12. Barker PM, Olver RE. Invited review:Clearance of lung liquid during the perinatalperiod. J Appl Physiol. 2002; 93(4):1542-8.
22 Vol 6 : 2010

13. Milner AD, Saunders RA, Hopkin IE. Effectsof delivery by caesarean section on lungmechanics and lung volume in the humanneonate. Arch Dis Child. 1978; 53(7):545-8.
14. Cummings JJ, Carlton DP, Poulain FR, RajJU, Bland RD. Hypoproteinemia slows lungliquid clearance in young lambs. J ApplPhysiol. 1993; 74(1):153-60.
15. Tutdibi E, Hospes B, Landmann E, GortnerL, Satar M, Yurdakök M, DellagrammaticasH, Ors R, Ilikkan B, Ovali F, Sarman G,Kumral A, Arslanoglu S, Koc H, Yildiran A.Transient tachypnea of the newborn (TTN):a role for polymorphisms of surfactantprotein B (SP-B) encoding gene? KlinPadiatr. 2003; 215(5):248-52.
16. Hislop AA, Wigglesworth JS, Desai R, AberV. The effects of preterm delivery andmechanical ventilation on human lunggrowth. Early Hum Dev. 1987; 15(3):147-64.
17. DeMarie MP, Hoffenberg A, Biggerstaff SL,
Jeffers BW, Hay WW Jr, Thureen PJ.terminants of energy expenditure inventilated preterm infants. J Perinat Med.1999;27(6):465-72
18. Scott C. Denne, Brenda B. Poindexter,Catherine A Leitch, udith A. Ernst, PamelaK. Lemon, James A. Lemon. EnteralNutrition, in: Fanaroff and Martin’s NeonatalPerinatal Medicine-Diseases of the Fetusand Infant, volume 2, 8th edition, ElsevierMosby. 661-679.
19. Robertson CM, Etches PC, Goldson E, KyleJM. Eight-year school performance,neurodevelopmental, and growth outcomeof neonates with bronchopulmonarydysplasia: a comparative study. Pediatrics.1992; 89(3):365-72.
20. Peters TJ, Golding J, Lawrence CJ, FryerJG, Chamberlain GV, Butler NR. Delayedonset of regular respiration andsubsequent development. Early Hum Dev.1984; 9(3):225-39.
IJGDBP 23
Members are requested to submitoriginal articles, review articles, case scenerios
for
Indian Journal ofGrowth, Development and Behavioral Pediatrics
Contact
Dr Jaydeep Choudhury, Editor-in-chief, [email protected]
Mobile 0931191020

Developmentally Supportive Care for Premature Baby
Santosh NimbalkarDevelopmental Pediatrician, Samwad Child Development Centre, Kolhapur. Niramay Instituteof Child Health, Satara. Bharati Vidyapith’s Medical College, Sangli. Maharashtra.
Although a baby may need to be in thehospital nursery,it is not always a verycomfor table or a restful place tobe.Lights are on 24 hrs a day, machinery,alarms, people, telephones and radioscan create a lot of noise andthatnecessary medical procedures areoften painful. Even routine caretakingactivities can be tiring and disruptive.
Boston psychologist Dr Heidi Als andothers have researched and developedways of making nurseries and neonatalcare more “baby friendly”.They haverecommended changes in the waysnurseries operate to help lessen thenegative effects the hospital careprovides and minimize the stress babiesexperience.In addition they recommendthat the care each baby receives beadjusted to best fit that childs needs andcoping abilities.This approach known asindividualized developmental care ( orformally, NIDCAP-Newborn Individua-lised Developmental Care andAssessment Program ),is designed toprovide an environment in which apremies development can continue asnormally as possible despite his earlybirth.
Research into its effects has shown thatbabies who are cared for using theindividualized developmental care
approach have fewer medicalcomplications,shorter stays in thehospital, better weight gain,and fewerdays on respirators.There may be longterm effects of this approach,aswell.Some of the early research hasindicated that babies cared for with theNIDCAP approach may show moreorganized behaviour and betterdevelopment in their first year of life.Asa result of this work, many nurserieshave made modifications in the nurseryenvironment and to the way in whichthey provide care.For eg,medical andcaregiving procedures are oftenclustered so that the baby can sleepundisturbed for several hours at atime.In addition during invasive oruncomfortable procedures,variouscomforting methods may be used to helpbabies stay calm.These includecholding a baby in a curled position withhands or swaddling giving the babysomething to grasp,or a pacifier to suck.Nursery may have a staff member-usually a nurse who has been trained inNIDCAP method.She will observe yourbaby, help plan his care and advice youand the staff on the best ways ofhandling him.
As a parent you can provide comfortand support to your growing baby in a
24 Vol 6 : 2010

number of ways.These may includemaking modifications to your baby’ssurrounding to minimize stress fromnoise and lights,as well as learning howbest to hold and interact with your babyas he grows and matures
Observe the baby’s environment andtry to minimize unnecessary noiseand light
(i) There are a number of simpleadjustments you can make in yourbaby’s surrounding to help reducethe amount of disruptive stimulationthat he receives.Make sure yourbaby is shielded from light either byadjusting the amount of light shiningdirectly on him or by putting a blanketor other covering over his incubatoror bassinet.Always close the doorsto his incubator quietly instead ofsnapping them shut.
(ii) If the nursery seems particularlynoisy because of a radio playing orphones ringing,talk to the staff aboutyour concerns.They may be able tomake adjustments to lessen thenoise or move your baby to a quieterlocation.
(iii) Keep voices low around your babyparticulary when he is sleeping ormove away from his bedside forconversations.
(iv) If your baby’s bed is located in anarea of the nursery where there is agreat deal of activity or foottraffic,see that he be relocated toquieter place.
(v) If your baby is on a respirator makesure that the water that accumulatesin the tubing is emptied regularly.
Hold the baby in a flexed position andprovide boundaries around him whilehe sleeps
Premies,like all newborn babies feelmore secure they are swaddledsecurely in a blanket with their legshooked up, arms bent, and handsbrought together in front of them.Whenthey sleep,they prefer to be touching orlying against something and will movein the incubator until they are against thewall or the bottom of the enclosure.Bypositioning your baby in a curled positionand providing boundaries for him whenhe sleeps, you are not only helping himfeel calm and comfortable but alsoencourage the development of the curledup position that babies naturally assumein the womb.Preemies with their lack ofmuscle strength ,have a hard timemaintaining this position by themselvesand if left alone, will lie spread eagledwith straight arms and legs on therelatively hard, flat surfaces of theirnursery beds.
To provide comfort to your baby andsupport his physical development, trythe following measures.
(i) Swaddle your baby in a blanket withhis arms and legs bent and handsbrought together in front of him or tohis face.
(ii) When you hold your baby, keep himin a slightly curled position with his
IJGDBP 25
legs tucked up and his handsbrought forward in front of him.
(iii) Create a nest for your baby to sleepin.wool blankets or cloth diapers andplace them around your baby to helpkeep his legs tucked.
(iv) If your baby must sleep on hisback,provide rolls along his sides tokeep his arms bent and handsbrought together in front of him andanother roll under his knees to keephis legs tucked up.
(v) In the hospital,babies sometimessleep on artificial lambskins or waterbeds to soften the surface on thebed.Artificial lamb skins and waterbeds are recommended for use onlyin the hospital where your baby iscontinuously monitored.Theyshouldn’t be used at home as theyare associated with higher risk ofSudden Infant Death Syndrome(SIDS).
Learn to read babies cues and paceyour activities with him accordingly.
As discussed earlier in thischapter,premature babies tend toexpress themselves through physicalchanges and behavior .As you spendmore time with your baby and as hematures you will begin to recognize howhe signals that he is gettingtired or upsetand the things he does to calmhimself.The following technique mayhelp your child stay calm or regainequilibrium if he has become upset.
(i) Provide one form of stimulation at a
time.If you rock him,don’t talk;if yourfeeding him, try not to look him in theeye,while your holding shield hiseyes from strong light.Add moretypes of stimulation slowly ,watching your baby for signs ofstress.
(ii) When your baby signals that he isgetting tired and needs some timeout give him a rest period by cuttingback on some of the stimulation heis receiving.For eg if you are rockingand looking at him, look away andjust hold him quietly,perhapsshading his eyes from light until herelaxes again or decrease theintensity of the stimulation by talkingsoftly,or rocking more slowly.Ifthese approaches don’t work, yourbaby may simply need to be placedback in his incubator or bassinet torest and sleep.
(iii) Help your child bring his hands tohis face or mouth,or offer him yourlittle finger or a pacifier to suck on.
(iv) Handle and move him slowly andgently.
(v) If your baby must be unwrappedfrom his blankets during certainprocedures,use your hands to keephis arms and legs tucked and createboundaries around him.This willcomfort him and help him feel moresecure.
(vi) Apply gentle but firm pressure onyour baby’s back or chest with youropen hands.This will help him to
26 Vol 6 : 2010

block out other stimulus,calm down
1. Harrison H;The principles of family centredneonatal care, Pediatrics,1993; 92(5):643-50.
2. Developmental care for very low birth weightpremature infants.Clinical Pediatr,1995;
34:523-9.
3. www.prematurity.org/baby/suppor tivecare.html.
4. The preemie parents companion’. MaddenSL.
Please Be A MemberAll members of Indian Academy of Pediatrics can be a life member of IAP Chapter onGrowth, Development and Behavioral Pediatrics. We request the members of IAP in variousStates to kindly be a member of this chapter by filling the following form and deposit it inthe address of the secretary with a DD of Rs.550/- in favour of “IAP Chapter on Growthand Development” payable at Kolkata. Membership Form Send it to Dr Jaydeb Ray, TheSecretary, IAP GDBP Chapter, 98 Ballygunge Place, Kolkata 700 019.
Membership Form of IAP Chapter on Growth, Development and Behavioral Pediatrics
1. Name :Surname....................……….Firstname.....................................………Middlename.................... (use Block Letter)
2. Male : Female : 3. Central IAP Membership No...........……………................... 4. IAP Non Member (Phychiatrist/Phychologist/Counselor/Teacher) :…………………………………
5. Corresponding Address :………………………………………………………………………………….
6. Designation in Institute with its Name (If any) ...………………………………………………………..
7. Academic Qualification (s) :……………………………………………………………………………..
8. Phone No. Residence :………………………………….Office/Chamber :…………………………..
9. Fax No. :……………………………10. Email :…………………………………………………………
11. Date of Birth :………………………………..
12. Bank Draft/Cheque No.:………………………… Name of Bank…………………………………..
Branch………………………………………………….Amount…………………………………………..
Date Signature
and organize himself.
IJGDBP 27

Genetic Counseling in Autism
Monidipa BanerjeeConsultant Pediatrician, Peerless Hospital and Institute of Child Health, Kolkata.
Objective:
This is a study through parentalinterviews, on the experiences ofparents going for a second child, afterhaving their first child diagnosed asautistic. The idea is to bring out theawareness of genetic predisposition inautism, and availability of adequatecounseling services.
The second part of the study looks atthe awareness among obstetricianswhen dealing with this population ofpatients.
Method
14 families were identified for theinterviews. Each of these families hadgone for a second child after having theirfirst child diagnosed as autistic. Theprofiles of the 14 families were as
follows:
(i) Father :
Aged between 30 – 50 years,average age- 39.5 years.
Occupation – Service 8, law 1,doctor 2, business 3.
Highest educational qualification – 7were graduates and 7 were postgraduates.
(ii) Mother :
Aged between 25 – 45 years,average age- 35 years
Occupation – House Wife 9, law 1,doctor 1, service 1, teacher 2.
Highest educational qualification –12 were graduates and 2 were postgraduates.
(iii) Age of first child (autistic) when
Abstract
With increasing incidence of autism (1 in 150), families with an affected memberhave a right to know regarding their risk of having another autistic child. 5-10%cases of autism have an identifiable medical disorder. Remaining 90% of cases ofautism, there is no identifiable cause (idiopathic). This is a study through parentalinterviews, on the experiences of parents going for a second child, after havingtheir first child diagnosed as autistic. The second part of the study, looks at theawareness among obstetricians when dealing with this population of patients.
The concerns of families need to be addressed by professionals with knowledgeof autism. Since obstetricians and pediatricians are most likely to face these ques-tions, there should be some guidelines on this issue.
28 Vol 6 : 2010

second child was born :
3 to 8 years, (average age - 4.8years)
(iv) Average monthly family income :5 had a family income of 10,000 to20,000/per month and 9 had a familyincome of >20,000/ per month.
(v) Family :
13 stayed in nuclear families andone belonged to an extended family.
(vi) Place of residence :
12 families were city based while 2were from towns.
The following questions were discussedwith either or both parents on a one toone basis by a single interviewer:
1. Why do/did you want a secondchild? (tick one or more)
(a) Want to experience a normalbaby ? (b) Want a babywhatsoever. (c) Somebody to lookafter the 1st child. (d) others(specify)
2. What/ who motivated you? (tick oneor more)a. Familyb. friend/peerc. Self Husband/Wifed. Unplanned pregnancye. Professional
3. Why do you think it happened? (Firstchild having autism)
4. Any history of similar problems in thefamily?
5. Did you know autism has a geneticpredisposition?
6. Did you go for counseling beforeconceiving or giving birth to yoursecond child?
7. If yes, to whom?
8. What were you told?
9. Did you tell your Obstetrician aboutyour first child? What did he/shesay?
10. What tests were done antenatally?
11. Did you think of the possibility thatthe second child may be autistic?
12. Did you want a boy or a girl secondtime? Why?
Father- ageoccupation highest educationalqualification
Mother- ageoccupation highest educationalqualification
Sibling – age sex
Average monthly family income
Family – nuclear/extended
Place of residence- city /town /village
contact no.
The following data were obtained:
1. Why did you want a second child?
Four couples want a babywhatsoever, 5 couples wanted asibling to look after the first child, and
IJGDBP 29

in 5 cases the pregnancies wereunplanned.
2. What/ who motivated you?Seven couples took the decisionthemselves, jointly. 5 pregnanciesas mentioned were unplanned. 2couples were influenced byprofessionals, into having a secondchild.
Further questionnaire
1. Why did you want a second child?Want a baby whatsoever - 4
Somebody to look after the first child- 5
Unplanned pregnancy - 5
2. What/whom motivated you ?Self H/W - 7
Unplanned pregnancy - 5
Professional - 2
3. Why do you think it happened?(1st child born with autism)
Nine said Don’t know – 9(64%) while5 (36%) had different thoughts oftheir own.
The different explanations givenwere:
Child fell & fainted at 1 yrs 3 months– 1; Child fell at 2 yrs – 1; Geneticpredisposition – 1; Lack of oxygenat bir th – 1; Multiple USG/polyhydramnios - 1.
4. Are there history of similarproblems in the family ?
No - 12(85%) yes - 2(15%) (Border
phenotye, MR)
5. Did you know autism has agenetic predisposition ?No - 11(78%). Yes - 3 (22%)
6. Did you go for geneticcounseling?No – 11(78%), yes – 3(22%)
7. To whom?Of the 3 who went for geneticcounseling, 2 went to thepediatrician, and 1 went to a referralinstitute.
8. What were you told?All 3 were advised that no antenataltests were available, and they hada higher risk of having another childwith autism than general population.
9. Did you tell your Obstetricianabout your first child?Yes – 13(93%) no - 1
What did he/she say?
They received the followinganswers:
don’t know – 1may not be repeated – 2your decision – 4continue your pregnancy – 2did not comment – 2leave it to God – 1have to take a chance - 1
10. What tests were doneantenatally?
TORCH, Triple test, USG were donein 7 cases and USG only in the
30 Vol 6 : 2010

other 7 cases.
11. Have you thought of thepossibility that the 2nd child maybe autistic ?
Yes - 13(93%). No 1(7%)
12. Did you want a boy or a girlsecond time ?
Anything - 13(93%). Girl - 1 (7%)
13. Why a autism is less in girl ?
Results:
Summarizing the above data it was seenthat,
(i) 36%(5) - wanted a 2nd child to lookafter the 1st child
(ii) 85%(12) – it was a Self decision bycouples
(iii) 85%(12) – there was no familyhistory
(iv) 29%(4) – Blamed autism on factorsin and around birth
(v) 78%(11) - Did not know autism hasa genetic predisposition
(vi) 22%(3) - Thought of geneticcounseling before having the secondchild
(vii)93%(13)- Told their obstetriciansabout their first child
(viii)93%(13) - Thought the 2nd childcould be autistic
Method
The second half of the study looked atawareness among obstetricians whendealing with this population ofpatients. 20 Obstetricians were
identified, all of whom werepostgraduates in their field. They wereall city based practitioners. They wereasked to fill up a questionnaire consistingof 5 questions.
Questionnaire
1. What is autism? (tick one or more)
Developmental delay
Psychiatric illness
Childhood schizophrenia
Neurodevelopmental disorder
Mental retardation
2. What causes autism? (tick one ormore)
Hereditary disorder (Mendelian)
Chromosomal disorder
Genetic disorder Familial factors
Environmental factors
Multifactorial
3. Write 3 most important features ofautism.
4. Incidence of autism in recent years?
5. A couple whose 1st child is autistic,comes to you for advice regardingsecond pregnancy
What would you advice?
The following data were obtained:
1. What is autism ?
Dev. delay - 6. Psychillness - 1
ND disorder - 10. MR 3
2. What causes autism ?
Genetic disorder -2
IJGDBP 31

Multifactorial - 18
3. Write 3 most important featuresof autism.
The following answers were obtained:
(i) Hyperactivity, attention deficit
(ii) Child can’t think, can’t mix with otherchildren
(iii) Developmental problem, low IQ level
(iv) MR, motor dysfunction, co-ordination problem
(v) Delayed speech, irritable
(vi) Unsocial
(vii)6 wrote, no idea
4. Incidence of autism in recentyears?
(i) Don’t know - 12
(ii) Increased - 4(20%)
(iii) Decreased - 3
(iv) 2-5%-1
5. A couple whose first child isautistic, comes to you for adviceregarding second pregnancyWhat would you advice?
(i) Counseling and further advice- 4(20%)
(ii) Refer to a pediatrician – 2 (10%)
(iii) No idea – 6 (30%)
(iv) Chance of repeat minimal – 2 (10%)
(v) Go for 2nd pregnancy – 4 (20%)
(vi) Ask for Karyotyping of both parents-1 (5%)
(vii)Whole battery of tests including
Chorionic Villus Sampling -1(5%)
Results
Summarizing the above data it was seenthat,
(i) 50% thought autism was aneurodevelopmental disorder
(ii) 90% thought cause of autism to bemultifactorial
(iii) Only 20% was aware of increasedincidence of autism in recent years
(iv) 30% had no idea about autism
(v) There was no clear cut idearegarding advice for next pregnancy
Discussion
With increasing incidence of autism (1in 150), families with an affectedmember have a right to know regardingtheir risk of having another child withautism. The concerns are not limited toparents only. It may extend to siblingsand cousins of autistic individuals. Withincreasing awareness of the importanceof genetic influences on autism, there isnow a demand from families with anaffected member for advice regardingtheir risk of having an autistic child.
5-10% cases of autism have anidentifiable medical disorder. Remaining90% of cases of autism, there is noidentifiable cause (idiopathic).Inheritance is likely multifactorial (genesplus environment). Exciting progress isbeing made in the journey towarddiscovery of genes conferring risk forautism and autism spectrum disorders.
32 Vol 6 : 2010

Current research evidence availablegives families empirical recurrence risksonly. There are no prenatal or carrierstate diagnostic tests.
Genetic counseling is a consultativeservice. Before counseling parents it isimpor tant to know what parents’expectations from the consultation are.It is important to first assess mainconcerns of parents. One also needs toassess their knowledge of diagnosis.This gives an idea as to what they hopeto gain from the session.
The study shows that in 85% of casesthere was no family history of autism.Almost 80% of the couples did not knowthat autism had a genetic predisposition,and 1/3rd blamed autism on factors inand around birth. Because of lack ofawareness only 3 out of 14 thought ofgenetic counseling. However almost allof them confided in their obstetricianregarding their first child, and feared thatthe second child could be autistic aswell.
The concerns of families requestinggenetic counseling need to beaddressed by professionals withknowledge of autism. There is a need togive information regarding recurrencerisks not only for autism but also for the
broader phenotype. In addition, couplesmay have other issues they wish todiscuss, which may influence theirreproductive decisions.
Geneticists are available in selectcenters only. Under thesecircumstances obstetricians andpediatricians are best placed to guideparents.
The study shows that obstetricians didnot have clear guidelines regardingadvice for next pregnancy. They alsohad limited knowledge on autism. Sinceobstetricians and pediatricians are mostlikely to face these questions, thereshould be some guidelines on this issue.Appropriate referrals should always bemade wherever possible.
Conclusion
With increasing incidence of autism (1in 150), families with an affectedmember have a right to know regardingtheir risk of having another autistic child.The concerns of families need to beaddressed by professionals withknowledge of autism. Sinceobstetricians and pediatricians are mostlikely to face these questions, thereshould be some guidelines on this issue.Appropriate referrals should always bemade wherever possible.
1. Simonoff E. Genetic counseling in autismand pervasive developmental disorders. JAutism Dev Disorders. 1998 ;28:447-56.
2. McMahon WM, Baty BJ, Botkin J. Utah.Genetic counseling and ethical issues for
autism. Am J Med Genet C Semin MedGenet. 2006;142:52-7.
3. Muhle R, Trentacoste SV. The Genetics ofAutism. Rebecca. Pediatr 2004; 113: 472-86.
IJGDBP 33

Breaking News
Jaydeep ChoudhuryAssistant Professor, Department of Pediatrics, Institute of Child Health, Kolkata
That medicine is not just a science andits practice requires art and tact is mostevident when a doctor has to breaknews. A bad news cannot be convertedto good news. Knowledge of normalpsychology will help inform and makethe process easier. Specific skills canbe learned and applied. Thus goodcommunication is the key. But thefoundation is empathy. Breaking newsis not like giving an update, one must befocused and understand the situationfrom “inside”. The approach should bewith caring. It is a complexcommunication task – requires expertverbal and non-verbal skills. Poordelivery can create seriousmiscommunications regardingprognosis of illness or purpose of care.The experience may stay in the mindlong after the initial shock has been dealtwith. The way a doctor or other health orsocial care professional delivers badnews places an indelible mark on thedoctor/professional-patient relationship.
The person who delivers news mayhave to cope with some difficulties. Likethe savior complex, where a physicianfeels that he is a savior and shouldalways come out with positive results.Perspective of disability and limitationsof the physician is another issue. Onehas to realize that certain situations are
beyond control. Then there may bediscomfort with negative emotions.
What is bad news?
Bad news can mean different things todifferent people. Bad news may be “anyinformation, which adversely andseriously affects an individuals view ofhis or her future” or, in situations wherethere is either a feeling of no hope, athreat to a person’s mental or physicalwell-being, risk of upsetting anestablished lifestyle, or where amessage is given which conveys to anindividual fewer choices in his or her life1.
The common denominator is that badnews is a message, which has thepotential to shatter hopes and dreamsleading to very different lifestyles andfutures.
Withholding bad news from patients wascommonly practiced until recently2.Hippocrates advised Concealing mostthings from the patient while you areattending to him. Give necessary orderswith cheerfulness and serenitycrevealing nothing of the patients futureor present condition. For many patientschave taken a turn for the worse byforecast of what is to come. In 1847,the American Medical Association firstcode of medical ethics stated, The lifeof a sick person can be shortened not
34 Vol 6 : 2010

only by the acts, but also by the wordsor the manner of a physician. It is,therefore, a sacred duty to guard himcarefully in this respect, and to avoid allthings which have a tendency todiscourage the patient and to depresshis spirits. A 1961 survey of 193physicians revealed that 169 (88%)routinely withheld cancer diagnoses.Fur thermore, they often usedeuphemisms such as “growth” todescribe cancer. The policy was “to tellas little as possible in the most generalterms consistent with maintainingcooperation and treatment.” However,the same study found that most patientsdesired the truth regarding theirdiagnosis.
In recent decades, this model of patientcare has been replaced by one thatemphasizes patient autonomy and fulldisclosure. Honest disclosure ofdiagnoses, prognoses, and treatmentoptions allows patients to make informedhealthcare decisions that are consistentwith their goals and values3,4.
Conveying Information to Patients
One should not break news in a hurry.The following is the Girgis and Sanson-Fisher guidelines on conveyinginformation to patients about seriousdisease or death5.
1. Ensuring privacy,
2. Allowing adequate time,
3. Assessing patients’ understanding,
4. Giving information about diagnosis
and prognosis simply and honestly,avoiding euphemisms,
5. Encouraging patients to expressfeelings,
6. Being empathic,
7. Giving a broad but realistic time-frame concerning prognosis,
8. Arranging a review.
The bottomline is that parents want theirdoctor to be honest, compassionate,caring, hopeful and informative.
Six Step Protocol for Breaking News
Robert Buckman has outlined a six stepprotocol for breaking bad news6. Thesteps are:
1. Getting started:
The meeting should be held in aprivate setting with both physicianand parent comfortably seated. It ishelpful to start with some questionsto indicate to the parent that thisconversation will be a two-wayaffair.
2. Finding out how much the patientknows:
By asking a question such as,“What have you already been toldabout the illness?” one can begin tounderstand what the parent hasalready been told, or how much theparent understood about what’sbeen said, the parents level oftechnical sophistication, and theparent’s emotional state.
3. Finding out how much the patient
IJGDBP 35

wants to know:
It is useful to ask parents what levelof detail they wish to cover Parentswant additional information regardingthe diagnosis, chances of cure, theside effects of therapy and a realisticestimate of recovery.
4. Sharing the information:
Decide on the agenda before sittingdown with the parents, so that onehas the relevant information at hand.The topics to consider in planning anagenda are: diagnosis, treatment,prognosis, and support or coping.However, an appropriate agenda willusually focus on one or two topics.Long lectures are overwhelming andconfusing. Medical terms should betranslated into English.
5. Responding to the patientsfeelings:
If the parent’s reaction is notunderstood, it will leave a lot ofunfinished business, and one willmiss an opportunity to be a caringphysician. Learning to identify andacknowledge a parent’s reaction issomething that definitely improveswith experience?
6. Planning and follow-through:
At this point one needs to synthesizethe parent’s concerns and themedical issues into a concrete planthat can be carried out in the parent’ssystem of health care. Outline astep-by-step plan, explain it to the
parent, and contract about the nextstep. Be explicit about your nextcontact with the parent or the factthat you won’t see the parent. Givethe parent a phone number or a wayto contact the relevant medicalcaregiver if something arises beforethe next planned contact.
Providing a Plan
Planning and follow-through is veryimportant. The doctor should synthesizethe parent’s concerns and the medicalissues into a concrete plan that can becarried out. Patients who have a clearplan for the future are less likely to feelanxious and uncertain. It may be helpfulif the patient has the option to speak tothe professional delivering the bad newsat a later stage.
Some phrases and questions that helpin good conversation are:
(i) “I wish I had better news” (asopposed to “I’m sorry, I have badnews”),
(ii) “I admire your courage,”
(iii) “I will be here for you,”
(iv) “What gives you hope andstrength?”
Some statements which may be avoidedinclude the following:
(i) “It could be worse,”
(ii) “We all die,”
(iii) “I understand how you feel,”
(iv) “Nothing more can be done.”
36 Vol 6 : 2010

Things go Wrong
Things go wrong when we try to escape,we react in anger or we dilute thesituation.
We try to escape:
We try to escape by inappropriatedelegation. The senior most member ofthe unit should break the news.Distraction, intellectualization,minimization and empty reassuranceshould be avoided.
React in anger:
Denial, idealization, rehearsal of thestory by the parents, some“unreasonable” demands, anger,frustration and blame may be naturalreactions of the parents. A physicianshould not react in anger under suchcircumstances.
Dilute the agenda:
It is not wise to dilute the agenda. It isimproper to discuss about billing,practical arrangements or try to distractwith trivial comments. After all a badnews is a bad news and it is a seriousmatter to the parents.
What is the importance ofdocumentation?
It is important that accurate records aremaintained of the conversation and theinformation and details exchanged.These will assist in the future care of thepatient and enhance communication
within the multidisciplinary team includingthe patient’s General Practitioner.
What if the parent starts to cry whilebreaking news?
It is always better to wait for the personto recover and stop crying. If it seemsappropriate, one can acknowledge andsuggest a temporary break till the parentrecovers. Most parents are somewhatembarrassed if they begin to cry and willnot continue for long. The doctor mustnot try to act as if tears are anemergency that must be stopped. Heshould not run out of the room. Oneshould show the willingness to deal withanything that comes up7,8.
When another Doctor has Conveyedthe Message in an Insensitive Way
Physician should try to understand theparents feeling and response, andanalyze what went wrong with theprevious encounter. One should notslander the insensitive caregiver.
What is the impact on you as a healthcare professional?
Breaking bad news can be extremelystressful for the doctor or professionalinvolved. The evidence suggests thatthe bearer of bad news experiencesstrong emotions such as anxiety, aburden of responsibility for the news andfear of a negative response. This stresscan result in a reluctance to deliver badnews9,10.
IJGDBP 37

1. Breaking Bad News.....Regional Guidelines.Department of Health, Social Services &Public Safety. Developed from Partnershipsin Caring (2000) DHSSPS, 2003. URL: http://www.dhsspsni.gov.uk/breaking_bad_news.pdf. Accessed on 29 December 2010.
2. Vandekieft G K. Breaking Bad News. AmFamily Phys 2001; 64: 12. URL:www.aafp.org/afp. Accessed on 29 Decem-ber 2010.
3. Taylor SE. Health Psychology, 1995. 3rd Ed.New York. NY: McGraw-Hill Book Company.
4. Buckman R. Breaking Bad News: A Guidefor Health Care Professionals 1992. Balti-more: Johns Hopkins University Press.
5. Girgis A, Sanson-Fisher R W. Breaking badnews: Consensus guidelines for medicalpractitioners. J Clin Oncol 1995; 13: 2449-56.
6. Breaking Bad News. University of Wash-ington School of Medicine. Ethics in Medi-cine. URL: http://depts.washington.edu/bioethx/topics/badnws.html. Accessed on29 December 2010.
7. Miyaji N. The Power of Compassion: TruthTelling Among American Doctors in theCare of Dying Patients. Soc Sci Med 1993;36:249-64.
8. Siminoff AL, Fetting JH, Abeloff MD. Doc-tor-Patient Communication about BreastCancer Adjuvant Therapy. J Clin Oncol1989; 7:1192-200.
9. Maguire P. Barriers of Psychological Careto the Dying. British Medical Journal 1985;291:1711-3.
10. Ptacek JT, Eberhardt TL. Breaking BadNews. A Review of Literature. JAMA 1996;276: 496-502.
38 Vol 6 : 2010
Visit Website of IAP Chapter on Growth, Development and
Behavioral Pediatrics
www.iapgdbp.orgGive your valuable opinion and suggestions to
Dr Jaydeb Ray, Secretary of the Chapterin his email ([email protected]),
or mobile (9831054552)















![Untitled-2 [] · Dr. Akshay Dr. Gade Dr. pratiksha Pat" Dr. Suresh Dr. AmitRajput Bensley Dr. Shefali Karkhanis Dr. Patil Dr. S Mulay Dr. Kamini Lakhiani Dr. Shah Dr. Jaydeep Rev](https://img.dokumen.tips/doc/110x75/5adee08b7f8b9a8f298c298a/untitled-2-akshay-dr-gade-dr-pratiksha-pat-dr-suresh-dr-amitrajput-bensley.jpg)












