Embed Size (px)
Citation preview

Journal of Clinical InvestigationVol. 42, No. 1, 1963
FIXED AND REPRODUCIBLEORTHOSTATICPROTEINURIA. III.EFFECT OF INDUCEDRENALHEMODYNAMICALTERA-
TIONS UPONURINARY PROTEIN EXCRETION*
By ROSCOER. ROBINSON, FRANKR. LECOCQ, PAUL J. PHILLIPPI,t ANDWILLIAM G. GLENN
(Fromi the Departments of Medicine, Duke University Medical Center and the Veterans Ad-ministration Hospital, Durham, N. C.; the Renal Unit, Department of Medicine,
USAFHospital, Lackland Air Force Base, Tex.; and the ImmunobiologySection, School of Aerospace Medicine, Brooks Air Force Base, Tex.)
(Submitted for publication July 3, 1962; accepted September 25, 1962)
Contrary to traditional opinion, recent observa-tions have suggested that nonhemodynamic fac-tors are the fundamental cause of "fixed and re-producible" orthostatic proteinuria (1-3). Im-portant findings have been the eventual appearanceof overt evidence of renal disease in many patientswith this disorder (3) and the description of acharacteristic pattern of glomerular alteration inrenal tissue from many such patients when bothconventional (1) and electron microscopy (4) wereused. Nevertheless, the renal circulatory responseto orthostasis may still play an important sec-ondary or modifying role in the pathogenesis ofthis form of orthostatic proteinuria. A basis forthis proposal is provided by previous observationsin patients with more advanced alterations of glo-merular anatomy due to obvious renal disease.Several observers have indicated that glomerularprotein transfer may be conditioned by intrarenalhemodynamic adjustments to the erect posture(5, 6).
The present study was undertaken to re-examinethe relative importance and contribution of uprightrenal circulatory adjustments to the occurrence offixed and reproducible orthostatic- proteinuria.Controlled changes of inulin and para-aminohip-purate clearance were produced in both the supineand upright posture by a variety of experimentalmaneuvers. A family of differing renal hemody-namic patterns was thus obtained, each of whichcould be related to its associated changes of uri-nary protein excretion in order to assess the rela-
* Supported in part by Research Contract 41(657) -368with the School of Aerospace Medicine, Brooks AirForce Base, Texas, and U. S. Public Health ServiceGrant No. 54-7370.
t Present address: Department of Medicine, USAFHospital, Travis Air Force Base, Calif.
tive importance of individual hemodynamic param-eters to the occurrence of proteinuria. Althoughnot conclusive, the results are compatible with thethesis that a normal reduction of renal blood flowduring orthostasis is the most important renalcirculatory determinant of upright proteinuria inthese patients.
All observations were limited to patients whoseorthostatic proteinuria was "fixed and reproduci-ble." No statement may be made regarding theirapplicability to patients with the much more com-mon "transient" type of orthostatic proteinuria(7).
METHODS
Fifty-five studies were carried out on 48 fasting pa-tients with "fixed and reproducible" orthostatic protein-uria. As outlined in a previous communication (1), casematerial for examination was selected from a large num-ber of Air Force recruits who had been hospitalized ona special ward for the particular evaluation of unclassi-fied proteinuria. All patients were asymptomatic andapparently healthy young men whose ages ranged be-tween 17 and 24 years (average: 19). With the ex-ception of proteinuria, no disturbances of renal functionwere demonstrable by either radiographic or routineclinical laboratory examination.
The presence of fixed and reproducible orthostaticproteinuria was established by the results of three or morecarefully supervised serial urine collection tests as de-scribed before (1). The test used has been found to bean adequate and reliable clinical means of classifying thevarious types of proteinuria by relating alterations ofurinary protein excretion to changes of body posture (7,8). Orthostatic proteinuria was termed "fixed and re-producible" if found consistently by repetitive examina-tion on different days. This type of orthostatic protein-uria is to be contrasted with the more common "transient"variety; the latter is variable and inconstant in its ap-pearance and cannot be detected reproducibly from dayto day. It cannot be emphasized too strongly that onlypatients with fixed and reproducible orthostatic protein-
100

RENAL HEMODYNAMICSIN FIXED AND REPRODUCIBLEORTHOSTATICPROTEINNURIA
uria were included in this study. This fact is of greatimportance, since it is quite possible that the two majorforms of orthostatic proteinuria ("transient" and "fixedreproducible") may provide entirely different etiologicand prognostic implications.
Glomerular filtration rate was measured as the inulinclearance, and effective renal plasma flow as the para-aminohippurate (PAH) clearance with standard renalclearance techniques (9). All patients were examined inthe early morning after they had been resting quietly inbed for at least 2 hours. Although some studies wereinitiated at a time when urine flow was low, most ex-periments were begun during a moderate water diuresis(5 to 8 ml per minute) produced by the oral ingestion of500 ml of tap water about 45 minutes prior to the test.In most studies, bladder urine was collected through anindwelling bladder catheter with the aid of an air wash-out. After three control clearance periods of 15 to 20minutes duration were obtained with the patient recum-bent, one of the four experimental plans listed below wasapplied in 54 experiments. In one study, clearance valueswere secured in the recumbent posture only.
Response to the upright posture. After completion ofthe last recumbent control clearance period, 23 patientswere asked to stand beside the bed in a relaxed and non-lordotic upright posture. While erect, three to four pe-riods of 10 to 15 minutes duration each were secured.Twelve of the 23 patients then returned to the supineposition in bed, and recovery clearance periods were ob-tained. In these and all other studies, the results of thefirst clearance period following a change of body posturewere not included in the final calculations.
A frequent and significant problem throughout theseexperiments was the occurrence of dizziness, or fainting,or both, while in the erect posture. This was particu-larly true during the studies described below in which avasoactive drug was administered. Many additional ex-periments were performed, but the appearance of eitherpresyncopal symptoms or actual fainting precluded ac-curate interpretation of the results. For this reason, noexperiments have been included which were complicatedby the appearance of recognizable vasomotor instability.In later studies, the incidence of syncope during ortho-stasis was lessened by instructing the patients to rest theirforearms upon a bedtable whose height had been adjustedconveniently and by then providing them with interestingreading material of their own preference.
Inflation of thigh tourniquets in the recumbent pos-hire. By the inflation of bilateral thigh tourniquets in 11patients, an attempt was made to produce a renal hemo-dynamic pattern during recumbency which resembledthat which occurred while standing. The lower ex-termities were first covered by a light blanket and thesupine control periods were obtained. Immediatelythereafter, high thigh tourniquets were inflated rapidlyto a cuff-pressure of 70 to 90 mmHg, and four sequen-tial periods of 10 to 15 minutes duration were secured.Recovery clearance periods were measured in 10 patientsafter tourniquet release. No undue discomfort was ex-perienced by the patients during tourniquet inflation.
Mllaintenzanice of positiVec pressure to the lower extremi-ties during the upright posture. These 12 experimentswere designed to either modify or obliterate the usualrenal circulatory response to standing. In 7 of the 12patients, sequential clearance periods were obtained firstduring recumbency, then during unmodified orthostasis,and then during recovery after the patients had returnedto the supine position in bed. Immediately after the lastrecumbent recovery period, a lower extremity, positive-pressure suit was inflated rapidly; the patients were thenrequested to stand upright while three to four clearanceperiods were obtained during the maintenance of positivepressure. The degree of pressurization was not standard-ized from patient to patient, although the suit pressurewas held steady throughout each individual experiment.In the remaining five patients, upright positive pressurewas applied immediately after the first supine control pe-riods, and erect control clearance periods without pres-sure application were not obtained.
Response to standing after prior administration ofhydralaZine.1 In eight experiments hydralazine was ad-ministered during recumbency in order to assess the sub-sequent effects of orthostasis upon urine protein excre-tion during the presence of renal hyperemia. Controlclearance periods were obtained sequentially during therecumbent, erect, and recumbent positions as describedbefore. After the last recumbent recovery period, in-travenous hydralizine hydrochloride (0.25 mg per kg)was administered, and two additional supine periods of15 minutes duration were obtained. The patients werethen asked to stand upright beside the bed while two tofour clearance periods were secured during the time ofnear maximal drug effect. Owing to the long duration ofthese experiments, supine recovery periods were notmeasured after completion of the upright posthydralazineperiods. Although syncope did not occur during any ofthe eight experiments reported here, one study was in-cluded in the final calculations which was terminated be-cause of a complaint of "giddiness' toward the end of thethird upright posthydralazine clearance period. Onlythe two upright periods which were unattended by vaso-motor instability were utilized.
Inulin was measured in urine and unyeasted plasma bythe resorcinol method of Roe as modified by Schreiner(10). Para-aminohippurate was determined by the pro-cedure of Selkurt (11). The peripheral venous hemato-crit was measured in duplicate by the Wintrobe tech-nique. Effective renal blood flow (ERBF) was calcu-lated from the PAH clearance and the venous hemato-crit. The renal extraction percentage of PAH was notdetermined.
The albumin concentration of unconcentrated urine wasquantified immunochemically by use of a double-diffusioncolumn method similar to that of Oakley and Fulthorpe(12) and Preer (13). This method required that thefraction-specific rabbit antihuman albumin serum be sepa-rated in the diffusion column from the urine perfusate by
1 Apresoline, Ciba Pharmaceutical Products, Inc., Sum-mit, N. J.
101

ROBINSON, LECOCQ, PHILLIPPI, AND GLENN
TABLE I
Average figures for renal hemodynamics and urinary proteinexcretion during the supine posture in patients with fixed
and reproducible orthostatic proteinuria*
Glomerular filtration rate (CO) t 121.0 +SD 17.4 ml/minEffective renal plasma flow (Cpah) t 614 4SD 123 mI/miEffective renal blood flow (ERBF) t 1117 ±SD 234 ml/minFiltration fraction (FF) t 20.2 dSD 3.0%Urinary albumin excretion (UalbV) $ 24.3 -SD 10.0 pg/minUrinary total protein excretion (Ut,,V) § 53.1 4SD 20.6 pg/min
* All values are corrected to 1.73 m2 BSA.t Fifty-five experiments; each figure represents the average of 174
clearance periods.$ Twenty-one experiments.§ Forty-one experiments.
10 mmof clear agar (13, 14). In this manner, urine al-bumin diffused downward, the antibody moved upward,and the position of the precipitin zone could be relatedto the albumin concentration of urine by reference to astandard curve. This was best accomplished by regres-sing the "P" value (ratio of the diffusion distance ofurine albumin to that of antialbumin) (13) onto the4albumin concentration of urine albumin standards pre-pared as follows: albumin was precipitated from a largepool of normal human urine by the use of 10 per cent tri-chloroacetic acid. The supernatant fraction from this pre-cipitation was found to be albumin-free when assayed insimple diffusion columns (15). Sufficient lyophilizedethanol-precipitated fraction V (albumin) was then tri-turated into the albumin-free substrate to give a con-centration of 100 mg per 100 ml. For accurate quanti-tation, it was essential that the standard concentrationsbe as similar as possible to those of the unknowns (16).All urine samples were analyzed in duplicate double-dif-fusion columns; appropriate standard solutions were al-lowed to react with antialbumin sera during each separaterun. Cathetometric measurement of the position of thealbumin-antialbumin precipitin system was made after 72hours at 30 ±.01° C (14). From such measurements,diffusivity ratios (13) could be calculated and substitutedinto the slope equation for the appropriate standard curve,and the albumin concentration of the unknown then calcu-lated. Statistical analysis of standard albumin curves(17) indicated that, on the average, urine albumin con-centration differences of 1.52 mg per 100 ml could be de-tected reliably at the 5 per cent probability level withinthe range of 0.782 to 25.0 mg per 100 ml. For purposes -ofthis study, any urine samples that contained less than 0.5mg of albumin per 100 ml were considered arbitrarily tobe "negative" for albumin. This method provides ac-curate quantitation only of that amount of urine albuminwhich is similar immunologically to that of normal pooledhuman serum.
Total urine protein was measured by a modification ofthe Folin-Ciocalteu procedure as described by Lowry(18). Because several constituents of normal urine mayreact with the Folin reagent, all urine samples were pre-pared as follows: a 10- to 20-ml portion of each samplewas lyophilized, reconstituted in 0.5 to 2.0 ml of water,precipitated with 10 per cent trichloroacetic acid, and
centrifuged. After centrifugation, the centrifuge tube wasinverted and the supernatant fraction allowed to drain;the precipitate was then dissolved in dilute alkali, and ap-propriate dilutions were made. The recovery of proteinadded to normal human urine averaged 94 per cent bythis procedure. The approximate concentration of urineglobulin was obtained from the difference between themeasured albumin and total protein concentrations.
RESULTS
Average values for renal hemodynamics andurinary protein excretion during all supine controlclearance periods are shown in Table I. Meas-urements of inulin and PAH clearance, effectiverenal blood flow, and filtration fraction were madeduring 55 experiments, and the average resultswere well within the range accepted as normal(19). The urinary excretion of total protein wasdetermined during recumbency in 41 studies andaveraged 53 ,ug per minute (Table I). Accuratequantitation of supine albumin excretion was se-cured in only 21 experiments because the rela-tively high urine flow during many supine controlperiods caused dilution of urine albumin to a levelbelow that measurable by our technique. In the21 experiments in which accurate measurementswere obtained, albumin excretion averaged 24 jugper minute (Table I) and accounted for an aver-age 45 per cent of the total urinary excretion ofprotein. These values are within the range ofthose reported by others (20, 21) for normal uri-nary protein excretion, although strict compari-son cannot be made because of methodologic dif-ferences and the fact that published normal figureshave been obtained from pooled 24-hour urine col-lections. It is not known what percentage of thenormal 24-hour excretion of protein is excretedduring the erect as contrasted to the supine pos-ture.
Response to the upright posture. Renal hemo-dynamic and urinary protein excretion values arepresented in Table II for those patients in whomboth supine and upright clearance measurementswere obtained. Patients have been listed accord-ing to descending figures for supine inulin clear-ance. In almost all patients, similar and significantchanges of renal hemodynamics and urinary pro-tein excretion were observed upon assumptionand maintenance of the upright posture. Inulinclearance fell in all but one patient (E. P.) and, onthe average, decreased to a value 28 per cent lower
102

RENAL HENMODYNAMICSIN FIXED AND REPRODUCIBLEORTHOSTATICPROTEINURIA 103
than the average supine figure (Table II; p=<.01). PAHclearance diminished in all patientsto an average figure which was 38 per cent lessthan that obtained during the control period (p =
<.01). As a result of the disproportionate reduc-tion of inulin and PAH clearance, filtration frac-tion increased significantly (average: 17 per cent;
p = <.01) in all but three patients (J. K., J. S.,and A. M.). During recumbent recovery periodsin 12 patients, inulin clearance averaged 125 18ml per minute, ERBF was 1,142 + 204 ml per
minute, and filtration fraction equaled 90.74.3 per cent. Although changes of the renal ex-
traction of PAH during orthostasis cannot be ex-
cluded, the associated reduction of filtration rate,the prompt return of clearance values to controlsupine levels, and the similarity of these altera-tions to those described in normal subjects (2, 19.22) upon standing suggest that the reduction ofPAH clearance was largely a consequence of a
reduced renal plasma flow.Although the order of magnitude varied widely,
values for both total protein and total albumin ex-
cretion rose in all subjects (Table II). On theaverage, urinary albumin excretion increased af-
ter standing to a value 555 per cent greater (p =
<.02) than the figure (22 6 /xg per minute)obtained for those 10 patients in whom albuminconcentrations could be determined accurately dur-ing recumbency. When compared to the averageurinary albumin excretion figure of all recumbentpatients (Table I), a percentage rise of similarmagnitude was found (500 per cent; p = <.01).
The urinary excretion of total protein rose, on
the average, to 362 per cent of the supine figure(Table II; p = <.01). Because the excretionrate of albumin rose to a greater degree than didthat of total protein, albumin contributed some-
what more to total protein excretion during stand-ing (59 per cent) than during the supine posture(42 per cent). No statistical correlation was
found between the magnitude of change exhibitedby the three hemodynamic parameters and that ofeither urinary albumin or total protein excretion.
Inflation of thigh totrniqulets in the recumibentposture. In 11 patients (Figure 1). thigh tourni-quet inflation produced an average 15.1 per centreduction of inulin clearance, from 116.9 16.3to 99.2 14.7 ml per minute (p = <.01). PAHclearance diminished proportionately (16.9 per
TABLE II
Renal hemodynaniics and urinary protein excretion during the upright posture in patientswith fixed and reproducible orthostatic proteinuria*
Supine Upright
Subject Age Cin Cpah ERBF FF UaIbV t UtpV Ci Cpah ERBF FF U. IV Ut-It
C-mi/mm mil/min ml/min %; jg/min ug/min ml/min ml/min mil/min C gmin/g:/minM.L. 17 146.6 769 1305 19.1 <40 40 96.0 401 730 23.9 103 174D.G. 18 142.4 848 1502 16.8 <53 73 86.5 408 741 21.2 74 127A.E. 17 142.1 631 1097 22.5 <46 56 86.1 347 603 24.8 79 139P.Z. 1 7 139.5 850 1603 16.4 34 85 101.2 389 749 26.0 433 575S.F. 17 129.0 700 1187 18.4 19 55 108.6 551 984 19.7 37 103N.M. 17 128.6 508 863 25.3 9 27 106.3 398 676 26.7 81 156D.H. 20 126.7 661 1212 19.2 12 29 78.4 338 669 23.2 126 254D.W. 17 126.6 500 847 25.6 <29 27 92.7 271 459 34.2 108 184J.K. 18 125.6 692 1473 18.2 <28 47 42.0 331 704 14.0 81L.A. 18 124.6 778 1441 16.0 11 63 92.0 541 1002 17.0 349 463R.H. 17 122.6 464 866 26.4 <43 48 116.4 424 785 27.5 96 186J.S. 19 121.8 532 1004 22.9 <37 77 68.2 320 639 21.3 121 167T.M. 19 119.1 570 1075 20.9 28 35 107.6 471 686 22.8 54 94F.D. 18 112.2 626 1129 17.9 21 56 81.1 304 548 26.7 154 231B.Y. 22 111.3 518 864 21.4 29 79 65.8 226 400 29.1 72 124C.D. 17 110.2 559 981 19.7 <35 77 89.1 368 658 24.2 162 369C. B. 18 109.8 563 954 19.5 33 62 81.4 361 644 22.6 96 207A.M. 17 108.9 447 812 24.4 <40 60 82.0 340 618 24.1 104 253M.S. 25 107.3 678 1190 15.8 <36 52 74.2 396 720 18.7 133 280S.M. 17 103.5 499 951 20.7 19 43 70.2 261 498 26.9 103 194J.M. 18 100.4 454 811 22.2 <40 63 92.3 372 664 24.8 115 211M.R. 19 97.5 500 894 19.5 <22 20 64.6 279 499 23.1 492 595E.P. 17 87.5 375 728 23.3 < 6 87.5 331 643 26.4 127 310
Average 18 119.3 597 1078 20.5 22 53 85.7 366 666 23.9 144 245
-+SD 15.4 132 250 3.1 6 19 17.1 80 142 4.2 117 141
* Supine values are the average of at least three clearance periods. Ipright values represent the average of two to three clearance determina-tions. All figures have been corrected to 1.73 m2 BSA. Abbreviations: Ci =inulin clearance; Cph =para-aminohippurate (PAH) clearance;ERBF=effective renal blood flow; FF =filtration fraction; UaibV =urinary albumin excretion; UtpV =urinary total protein excretion.
t Samples which were too dilute for accurate albumin analysis are preceded by a "less than" ( <) sign. Such figures represent the least amountof albumin which could have been detected accurately by our technique. Only those samples whose concentrations were actually measured areincluded in the average value.

ROBINSON, LECOCQ, PHILLIPPI, AND GLENN
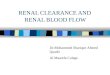
FIG. 1. EFFECT OF SUPINE, THIGH TOURNIQUETINFLATION UPONRENAL
HEMODYNAMICSAND URINARY PROTEIN EXCRETION IN 11 PATIENTS WITH
FIXED AND REPRODUCIBLEORTHOSTATICPROTEINURIA. Vertical bars repre-sent average values for the entire group. Standard deviation is indicatedby the brackets. Urine albumin was measured in only 3 patients duringthe supine control period.
cent) from an average supine figure of 562 + 108ml per minute to an average value of 467 + 60 mlper minute during tourniquet inflation (p = <.01).Filtration fraction increased in two patients, de-creased in four, and was essentialy unchanged dur-ing the remaining five studies. Because of theequal and parallel average reduction of inulin andPAH clearance, however, the average value forfiltration fraction did not change significantly(Figure 1; p = >.10). The hemodynamic re-sponse to tourniquet application resembled thatseen upon standing in that similar directionalchanges of inulin and PAH clearance occurred.The response differed in that the reduction ofthese clearances was of somewhat lesser magnitudeand it was unassociated with an average rise offiltration fraction. After tourniquet release, allhemodynamic values returned promptly to the ap-
proximate levels observed previously during thecontrol supine clearance periods (Figure 1).
These experiments are of interest because sig-nificant proteinuria occurred in all patients despitethe absence of an average rise of filtration frac-tion. Values for urinary albumin excretion in-creased from an average of 15 jug per minute dur-ing the control period (three patients only) to 50+ 23 Mtg per minute during tourniquet inflation(233 per cent increase). Although the paucity ofurine albumin measurements during the supinecontrol periods prevented an evaluation of sta-tistical significance within this group, compari-son of the figure for albumin excretion duringtourniquet inflation with that of the supine con-trol periods of all subjects (24.3 ± 10.0 ,mg perminute; Table I) revealed a significant difference(p = <.01). Similarly, total protein excretion in-
104

RENAL HEMODYNAMICSIN FIXED AND REPRODUCIBLEORTHOSTATICPROTEINTURIA 105
creased 220 per cent from an average value of33.2 + 12.7 Mug per minute during the control pe-riod to an average figure of 106.2 + 53.4 ug perminute during thigh tourniquet inflation (p = <.01). The relative contribution of albumin tototal protein excretion was unchanged both beforeand during tourniquet inflation (45 and 47 percent respectively). After tourniquet release, pro-tein excretion in all patients returned to the supinecontrol values (Figure 1). Again, no statisticalcorrelation was established between changes ofinulin or PAH clearance and the degree of pro-teinuria produced by tourniquet inflation.
Maintenance of positive pressure to the lo-wer
extremities during the upright posture. The ef-fects of positive pressure applied to the lowerextremities during the assumption and mainte-nance of the upright posture are shown in TableIII. Upright clearance periods were obtainedwith and without pressure-suit inflation in 7 ofthe 12 patients. The control hemodynamic re-sponses of these 7 patients to standing were simi-lar both qualitatively and quantitatively to thoseof other patients. During orthostasis with pres-sure suit inflation, however, a different type of re-sponse was observed in many of the 12 patients.Filtration rate was well maintained in all but 3patients (P. Z., D. D., and G. M.) and averaged
TABLE III
Effect of lower extremity positive pressure upon renal hemodynamics andurinary protein excretion during orthostasis*
Patient Posture Ci Cpah ERBF FF UaibV utpyr
S.F. SupineUprightSupineUpright-P t
C.D. SupineUprightSupineUpright-P
M.S. SupineUprightSupineUpright-P
D.G. SupineUprightSupineUpright-IP
M.L. SupineUprightSupineUpright-P
P.Z. SupineUprightSupineUpright-P
TM.N. SupineUprightSupineUpright-P
J.W. SupineUpright-P
R.G. SupineUpright-P
D.D. SupineUpright-P
D.E. SupineUpright-P
G.M. SupineUpright-P
Average Supine4SD Upright
SupineUpright-P
ml/min129109149132
11089
102108
10774
123122
14286
133144
14796
133135
140101133119
119108123130
122125
130136
128109
134129
10986
126 4 1395 4 12
128 i 13123 i 16
ml/min700551748611
559368494471
678396674615
848408709704
769401574555
850389666449
570471451500
555535
639598
616480
653552
447340
657 + 122426 ± 64644 i: 130534 ±t 95
ml/min1187984
12681075
981658882674
1190720
11841098
1502741
12671304
1305730989991
1603749
1293885
1075686835980
11111028
11831108
1082814
1156994
812618
1183 4 215753 4 99
1145 4 218964 + 190
.184
.197
.199
.216
.197
.242.206.230
.158.187.183.198
.168
.212
.187
.204
.191
.239
.232
.243
.164.260.199.264
.209
.228
.274
.260
.220
.233
.203
.228
.208
.228
.205
.233
.244
.252
.196 + .022
.224 4 .026
.204 + .036
.232 + .030
pig/min18.837.124.450.0
<35.0162.3
45.675.8
<36.3132.8
59.455.4
<53.273.739.482.0
<39.7103.2
31.473.1
34.1433.0
49.0119.0
28.354.334.232.6
27.285.2
14.679.7
<30.2102.6
43.153.2
<40.070.0
27.3 i 10.3142.3 i 135.438.1 4t 12.873.2 + 23.6
5sg/milt55.3
103.260.067.0
77.1368.6103.0154.0
52.1280.5
92.7116.1
73.4127.2
76.3141.7
39.6174.5
46.9149.2
85.2575.4
98.9186.2
35.293.654.051.6
41.3217.5
31.6138.2
56.7151.4
52.593.0
60.5112.7
55.0 ± 16.9246.1 i: 176.8
72.7 + 23.1131.6 + 47.1
* Eachtfigure represents the average of two to three clearance periods. All values are corrected to 1.73 m2 BSA. Abbreviations as in Table II.t "Upright-P" refers to those periods obtained while the patient maintained the upright posture during the application of positive pressure to
the lowver extremities.

ROBINSON, LECOCQ, PHILLIPPI, AND GLENN
TABLE IV
Effect of prior treatment with hydralazine upon renal circulatory adjustments and urinary protein excretionduring orthostasis in eight patients with fixed and reproducible orthostatic proteinuria*
Supine post- U~pright post-Supine Upright hydralazine hydralazinet
Determination Av. SD Av. SD Av. SD Av. SD
GlomerUlar filtration rate, 116 + 11 87 i 14 117 ± 15 92 ± 16ml/min
Effective renal plasma flow, 518 + 57 303 + 69 709 4+ 168 528 ± 80ml/min
Effective renal blood flow, 906 ±- 112 534 + 115 1265 i 319 892 i 115ml/min
Filtration fraction, %/0 22.7 + 2.9 29.2 i 3.9 17.0 i 3.1 17.5 ± 3.0Urine albumin excretion,t 27.1 + 10.2 107.1 i 28.7 28.7 i 12.6 44.9 i 14.6
jug/minUrine total protein excretion, 54.9 + 23.2 182.2 + 38.4 56.6 i 20.4 81.1 + 27.9
ig/min
* All figures are corrected to 1.73 m2 BSA. Two to three clearance periods were obtained during each change ofposture.
t Hydralazine, 0.25 mg per kg i.v., was administered to patients while supine, approximately 30 minutes beforestanding.
T Urine albumin could be measured during the control supine periods of four patients only.
only 3 per cent less than the average figure of thesupine control periods (Table III). This valuediffered significantly from that obtained when thepatients were standing upright without pressuresupport (p = <.01). Despite pressure-suit infla-tion, however, PAH clearance fell in all but 4 pa-tients (J. W., T. M., D. G., and R. G.) to an av-erage value 19 per cent lower than that observedwhile supine. Although this reduction of PAHclearance was not significantly different from theaverage supine control value of all 51 patients ex-amined (p = >.10), paired data analysis of thisgroup alone revealed it to be significantly differ-ent from the first supine control value (p = <.01)and the figure obtained during orthostasis withoutpressure-suit support (p = <.02). Because, onthe average, inulin clearance was maintained de-spite a modest reduction of PAH clearance, filtra-tion fraction rose 18 per cent when the patientswere standing erect during pressure-suit inflation(Table III). This hemodynamic response wasalways associated with the appearance of signifi-cant proteinuria. Albumin excretion rose, on theaverage, to a value of 168 per cent (p = <.01)higher than the first supine control value, and av-erage total protein excretion increased to 139 percent of the first supine figure (Table III). Thedegree of proteinuria, however, was not so markedas that observed when the patients were standing
upright without pressure-suit inflation (Tables IIand III).
Response to standing after prior administrationof hydralazine. The effect of prior treatment withhydralazine upon the usual renal circulatory ad-justment and change of protein excretion in re-sponse to standing is shown in Table IV. Inthese patients, the renal hemodynamic response tothe unmodified upright posture before hydralazineadministration was similar to that described before.After hydralazine administration, a significant (p= <.01) average rise of PAH clearance oc-curred in all subjects while in the recumbent pos-ture which was associated with maintenance ofinulin clearance and a fall of filtration fraction.The ability of this drug to increase the clearanceof PAH has been described previously (23).When the upright posture was assumed and main-tained during the time of maximal drug action,average inulin and PAHclearance values fell pro-portionately so that no significant change of fil-tration fraction occurred (Table IV). This pat-tern of response was similar to that seen duringthe application of thigh tourniquets in the supineposition. It differed perhaps accidentally, in thatthe absolute average figure for PAHclearance wasno different (p = >.10) from that of the supineperiod prior to hydralazine administration (TableIV). The average values for both inulin clear-
106

RENAL HEMODYNAMICSIN FIXED AND REPRODUCIBLEORTHOSTATICPROTEINURIA
ance andl filtration fraction, however, were sig-nificantly lower than those of the supine periods(21 and 23 per cent decreased, respectively; p =
<.01 and <.01). Thus, pretreatment with hy-dralazine appeared to prevent PAH clearancefrom falling during orthostasis to the absolutelower levels observed during periods of unmodifiedstanding prior to drug administration.
The average excretion of albumin and totalprotein during upright standing after hydralazineadministration was much less than that during theprehydralazine upright posture and only slightlyhigher than that of the supine control period(Table IV). Although albumin and total pro-
tein excretion rose 66 and 48 per cent, respec-
tivelv, from the control supine figure, these val-ues should be contrasted to increases of 295 per
cent for albumin excretion and 232 per cent fortotal protein excretion during unmodified stanid-ing.
DISCUSSION
The renal hemodynamic response to standing inthese patients was characterized by a moderatereduction of inulin and PAH clearance and an
elevation of filtration fraction. In almost all re-
spects, the character of this response resembledclosely that described by others in healthy, non-
proteinuric subjects (2, 19, 22). If, as seems
likely, the lowered clearance of PAH was theconsequence of a diminished renal plasma flow,then the rise of filtration fraction may be attributedto efferent arteriolar constriction as part of theusual asoconstrictive response to orthostasis.King and Baldwin (2) have reported similar find-ings in other patients with orthostatic proteinuriaand, on the basis of comparable control measure-
ments on normal subjects, first proposed that thepostural adjustments of inulin and PAH clear-ance in such patients were indistinguishable fromthe normal. The present results are in agreementwith this proposal, although the lack of similar ob-servations on normal subjects prevents its ftllconfirmation.
The demonstration of a normal postural re-
sponse of inulin and PAH clearance does not
necessarily exclude the coexistence of an abnormaladjustment of other hemodynamic variables. De-spite an apparently normal filtration fraction, dis-
turbances of intraglomerular pressure may stillexist, since there is some question as to the validityof this measurement as an index of glomerularhydrostatic pressure under all conditions (19).Complete acceptance of the normalcy of total re-nal circulatory function in this disorder must awaitthe measurement of such variables as renal ve-nous pressure, cardiac output, and mean arterialblood pressure. Although not excluded, the pres-ence of other hemodvnamic alterations would seemunlikely, however, since vascular alterations ofsufficient intensity to affect protein transfer at theglomerulus would logically be expected to produceassociated disturbances of either filtration rate,renal plasma flow, or filtration fraction. Conse-quently, the present findings, although not con-clusive, must be regarded as additional support tothe recent proposal that factors of a nonhemodv-namic nature are of primary etiologic importanceto fixed and reproducible orthostatic proteinuria(1, 2).
A typical histologic pattern of glomerular al-teration in renal tisstue from patients with this typeof orthostatic proteinuria has been described (1,4). The possible causes and clinical significanceof this histologic finding have been the subject ofprevious communications (1, 4). Although thepossibility remains that it is the secondary effectof an underlying hemodynamic alteration, presentconsiderations best support the concept that thestructural defect itself is the primary cause of fixedand reproducible orthostatic proteinuria. Thisopinion rests on the histologic nature of the glo-merular defect, the presumptive normalcy of fil-tration rate, renal plasma flow, and filtration frac-tion during orthostasis, and the observation thatmany patients with this disorder eventually de-velop overt evidence of renal disease (3).
Assuming that a fixed and underlying defect ofthe glomerular capillary wall is the primary causeof this disorder, even a normal circulatory adjust-ment to orthostasis may be of the appropriate na-ture and magnitude to effect an increased trans-fer of protein through a glomerular structure whichis already defective. A similar concept appearsapplicable to patients with early but definite re-nal disease (6). Although still of importance. he-modynamic factors may then be relegated to a"permissive" rather than a primary role in thegenesis of fixed and reproducible orthostatic pro-
107

ROBINSON, LECOCQ, PHILLIPPI, AND GLENN
teinuria. If valid, such a proposal offers thedistinct advantage of combining the demonstrationof an anatomic defect and a presumably normalvascular response to orthostasis into a singlepathogenetic concept.
Regardless of whether vascular adjustments inthis condition are normal or abnormal, severalobservers have emphasized their contribution tourinary protein excretion in both patients with or-thostatic proteinuria and with overt forms of renaldisease (5, 6, 24, 25). General agreement has notbeen reached as to which renal hemodynamicparameter is of most importance in this regard.Factors such as the rate and velocity of glomerularblood flow, filtration rate, and intraglomerular orrenal venous hydrostatic pressure have all beenconsidered of varying relative importance. Kinghas proposed that the normal filtration fractionelevation of orthostasis is most causally related tothe appearance of orthostatic proteinuria (7).Others have suggested that filtration rate and re-nal blood flow are of equal or greater importancein other forms of proteinuria (24, 26). Althoughonly limited conclusions are permitted by the pres-ent observations, diminished renal blood flow ap-pears to be of most hemodynamic importance tothe occurrence of fixed and reproducible ortho-static proteinuria.
Neither filtration rate nor filtration fractionseems of first order importance to the initiation ofproteinuria in view of filtration fraction stabilityduring thigh tourniquet inflation and the mainte-nance of filtration rate during pressure-suit infla-tion. Despite the constancy of these two variables,significant proteinuria occurred during both ex-perimental procedures. By exclusion then, a re-duced renal blood flow seems to be the most im-portant circulatory determinant of proteinuria be-cause an average moderate reduction of PAHclearance occurred during both pressure-suit andtourniquet inflation. Since proteinuria was some-what less during these two maneuvers than dur-ing unmodified orthostasis, however, both filtra-tion fraction and filtration rate may still contributeto either its initiation or maintenance. On theother hand, these factors may be of little or noimportance, and the lower rate of protein excre-tion during tourniquet and pressure-suit inflationmay be related solely to the less reduced renalblood flow.
Further evidence that the reduction of renalblood flow is of first importance is provided by theresults of the hydralazine experiments. In thesepatients, maintenance of the average PAH clear-ance value during orthostasis at a level approxi-mating that of the supine posture was associatedwith the occurrence of only minimal proteinuria.It is reasonable to suspect that the relative reduc-tion of blood flow which did occur upon standingwas not only of insufficient magnitude to effect alarge increase of glomerular protein transfer, butthat a certain critical flow level must first bereached in each patient before the proteinuria ap-pears. The oral ingestion of another, less potentvasodilator drug (caffeine citrate) has also beenreported to depress the intensity of exercise pro-teinuria (27).
Considered together, these experiments implythat the upright reduction of renal blood flow isthe most important hemodynamic determinant ofglomerular protein transfer for the following rea-sons: 1) significant proteinuria occurred regularlyin the absence of changes of either filtration rateor filtration fraction; 2) proteinuria was rarelyobserved without an associated reduction of PAHclearance; and 3) maintenance of PAHclearanceduring orthostasis at an absolute average levelequal to that of recumbency was attended by asignificant depression of upright proteinuria.Nevertheless, lesser contributions of filtration rate,or intraglomerular pressure to postural protein-uria, or both, have not been rigidly excluded, andthe absence of statistical correlation betweenchaniges of protein excretion and those of any he-modynamic variable prevents the formation ofdefinite conclusions on the exact role of circula-tory factors in this disorder.
No explanation is available for the mechanismby which a reduction of blood flow might increasethe glomerular transfer of protein. Its exactdefinition must await better knowledge of thefundamental process responsible for the passageof protein molecules across capillary walls, aproblem which has been the subject of several re-cent communications (24, 26, 28). In studies ofpatients with obvious renal disease, Lathem dem-onstrated a correlation between the relative fallof PAH clearance and the rise of protein clear-ance during the administration of catecholamines
108

REN-AL HEMODYNAMICSIN FIXED AND REPRODUCIBLEORTHOSTATICPROTEINTURIA
(24). He suggested tentatively that a diminishedglomerular blood flow might permit an increasedtransfer of protein across the capillary wall bylengthening the exposure time of protein mole-cules to the endothelial surfaces of the glomerularcapillaries. As in the present study, he concludedthat changes of filtration rate and filtration frac-tion were not the major hemodynamic determi-nants of an increased glomerular passage of pro-tein (24).
Throughout these experiments it has been as-sumed that altered glomerular function is the pri-mary cause of orthostatic proteinuria. The oc-currence of diminished tubular reabsorption ofprotein during orthostasis, however, has not beenexcluded. In fact, varying degrees of tubular re-absorptive activity among patients could explainthe lack of quantitative correlation between pos-tural hemodvnamiic responses and protein excre-tion in these experiments. Other observers havealso noted a similar lack of correlation betweenvarious circulatory responses and the minute ex-cretion rate of protein in urine (6). Albumin ortotal protein clearance values, if available, mighthave permitted the appearance of such a corre-lation.
The production of recumbent proteinuria (thightourniquet inflation) in patients with this disorderis an important finding that deserves brief com-ment. Since tourniquet inflation fails to producerecumbent proteinuria in normal individuals (7),and since there is nio reason to believe that thecirculatory response to this maneuver is differentin patients with orthostatic proteinuria, the pro-duction of supine proteinuria as described heremay be interpreted as further indirect evidence ofthe underlying importance of nonhemodynamicfactors. In addition, this observation implies thatneither the erect posture nor other anatomic fac-tors such as upright hepatic compression of the in-ferior vena cava (29) are essential to the appear-ance of this type of proteinuria. Nevertheless, asimilar but nonmechanical elevation of renal ve-nous pressure induced by, tourniquet inflation it-self cannot be ruled out explicitly without a di-rect estimation of renal venous pressure. Lastly,the appearance of recumbent proteinuria in thesepatients does not exclude a contributory role ofupright anatomic factors to the production of
"transient" orthostatic proteinuria, a variety oforthostatic proteinuria that is much more preva-lent than the "fixed and reproducible" type con-sidered in this report (7).
SUMMARY
1. The effects of induced renal hemodynamicalterationis upon urinary albumin and total pro-tein excretion were studied in patients with fixedand reproducible orthostatic proteinuria. Differ-ing types of renal circulatory patterns were pro-duced by unmodified orthostasis, recumbentthigh tourniquet inflation, application of positivepressure to the lower extremities during stand-ing. and by ortlhostasis after the prior admniniistra-tion of hydralazine.
2. Recumbent values for inulin and para-amino-hippurate (PAH) clearance and filtration fractionwere normal. Upon standing, a disproportionatereduction of inulin and PAH clearance occurred,filtration fraction rose, and urinary protein excre-tion increased significantly. The circulatory re-sponse to standing was of the same nature andmagnitude as that described by others in healthy,nonproteiniuric subjects.
3. Supine, thigh tourniquet inflation was as-sociated with reduced inulin and PAH clearancebut no change of filtration fraction, and uprightpressure support to the lower extremities was at-tended by maintenance of filtration rate and amodest average reduction of PAH clearance andrise of filtration fraction. Despite filtration frac-tion stability during thigh tourniquet inflation andthe maintenance of filtration rate during the ap-plication of lower extremity positive pressure. eachof these experimental maneuvers was accompaniedby proteinuria.
4. Prior treatment with hydralazine during re-cumbency prevented the usual average reductionof PAH clearance upon standing, and the smallrise of protein excretion that occurred was muchless than that observed before drug treatment.
5. As in other patients with more severe glo-merular defects, this combination of findings iscompatible with the proposal that a normal reduc-tion of renal blood flow during standing is the mainhemodynamic determinant of upright protein ex-cretion in patients with fixed and reproducibleorthostatic proteinuria.
109

ROBINSON, LECOCQ, PHILLIPPI, AND GLENN
ACKNOWLEDGMENTS
The authors wish to thank Mr. Robert N. Graham,A 1/c Chandler R. Monk, and Mrs. Nancy Langleyfor their technical assistance; Mr. Alton Rahe for hisstatistical aid with the albumin analyses; and Lt. Col.Wilbur L. Kenoyer for his advice and support throughoutthe study.
REFERENCES
1. Robinson, R. R., Glover, S. N., Phillippi, P. J.,Lecocq, F. R., and Langelier, P. R. Fixed andreproducible orthostatic proteinuria. I. Light mi-croscopic studies of the kidney. Amer. J. Path.1961, 39, 291.
2. King, S. E., and Baldwin, D. S. Renal hemodynam-ics during erect lordosis in normal man and sub-jects with orthostatic proteinuria. Proc. Soc. exp.
Biol. (N. Y.) 1954, 86, 634.3. King, S. E. Albuminuria (proteinuria) in renal dis-
eases. II. Preliminary observations on the clini-cal course of patients with orthostatic albuminuria.New York med. J. 1959, 59, 825.
4. Robinson, R. R., Ashworth, C. T., Glover, S. N.,Phillippi, P. J., Lecocq, F. R., and Langelier,P. R. Fixed and reproducible orthostatic protein-uria. II. Electron microscopy of renal biopsy speci-mens from five cases. Amer. J. Path. 1961, 39, 405.
5. Lathem, W., Roof, B. S., Nickel, J. F., and Bradley,S. E. Urinary protein excretion and renal hemo-dynamic adjustments during orthostasis in pa-
tients with acute and chronic renal diseases. J.clin. Invest. 1954, 33, 1457.
6. King, S. E. Postural adjustments and protein excre-
tion by the kidney in renal disease. Ann. intern.Med. 1957, 46, 360.
7. King, S. E . Patterns of protein excretion by thekidneys. Ann. intern. Med. 1955, 42, 296.
8. Derow, H. A. The diagnostic value of serial meas-
urements of albuminuria in ambulatory patients.New Engl. J. Med. 1942, 227, 827.
9. Goldring, W., and Chasis, H. Hypertension andHypertensive Disease. Cambridge, Mass., HarvardUniversity Press, 1944.
10. Schreiner, G. E. Determination of inulin by means
of resorcinol. Proc. Soc. exp. Biol. (N. Y.) 1950,74, 117.
11. Selkurt, E. E. VII. Measurement of renal bloodflow. Meth. med. Res. 1947, 1, 191.
12. Oakley, C. L., and Fulthorpe, A. J. Antigenic analy-sis by diffusion. J. Path. Bact. 1953, 65, 49.
13. Preer, J. R., Jr. A quantitative study of a techniqueof double diffusion in agar. J. Immunol. 1956,77, 52.
14. Glenn, W. G. Quantitative analyses by diffusioncolumn reactions. I. Variations in diffusion meas-urements. J. Immunol. 1962, 88, 535.
15. Oudin, J. Specific precipitation in gels and its ap-plication to immunochemical analysis. Meth. med.Res. 1952, 5, 335.
16. Oudin, J. Antigen-antibody precipitation in gels.Non-specific effect on the displacement of thezone. Discussions Faraday Soc., 1954. 18, 351.
17. Glenn, W. G. Quantitative analysis by diffusioncolumn reactions. III. Antigen and antiserumconcentration differences from diffusion measure-ments of simple homologous reactions. J. Im-munol. 1962, 88, 545.
18. Lowry, 0. H., Rosebrough, N. J., Farr. A. L., andRandall, R. J. Protein measurement with theFolin phenol reagent. J. biol. Chem. 1951, 193,265.
19. Smith, H. W. The Kidney, Structure and Functionin Health and Disease. New York, Oxford Univ.Press, 1951.
20. Rigas, D. A., and Heller, C. G. The amount andnature of urinary proteins in normal human sub-jects. J. clin. Invest. 1951, 30, 853.
21. Webb, T., Rose, B., and Sehon, A. H. Biocolloids innormal human urine. I. Amount and electropho-retic characteristics. Canad. J. Biochem. 1958, 36,1159.
22. Brun, C., Knudsen, E. 0. E., and Raaschou, F. Theinfluence of posture on the kidney function. II.Glomerular dynamics in the passive erect pos-ture. Acta med. scand. 1945, 122, 332.
23. Reubi, F. C. Renal hyperemia induced in man by anew phthalazine derivative. Proc. Soc. exp. Biol.(N. Y.) 1950, 73, 102.
24. Lathem, W. Renal circulatory dynamics and urinaryprotein excretion during infusions of 1-norepineph-rine and l-epinephrine in patients with renal dis-ease. J. clin. Invest. 1956, 35, 1277.
25. King, S. E., and Baldwin, D. S. Production of re-nal ischemia and proteinuria in man by the adrenalmedullary hormones. Amer. J. Med. 1956, 20,217.
26. Pappenheimer, J. R. Passage of molecules throughcapillary walls. Physiol. Rev. 1953, 33, 387.
27. Taylor, A. Some characteristics of exercise pro-teinuria. Clin. Sci. 1960, 19, 209.
28. Chinard, F. P. Possible mechanisms of formation ofglomerular fluid in Trans. Third Conf. on RenalFunction, Josiah Macy Foundation, 1951.
29. Bull, G. M. Postural proteinuria. Clin. Sci. 1948, 7,77.
110