Embed Size (px)
Citation preview

Voiding Dysfunction 2009
Block lecture, 5th year student.
Choosak Pripatnanont, Department of Surgery, PSU.

Objectives
• Understand and explain physiologic function and dysfunction of lower urinary tract.
• Evaluation patient with LUTS
• Primary management /investigation
• Give primary management of BPH







Storage phase
Emptying phase
Bladder
pressure
Storage phase
Micturition cycle
Detrusorrelaxes
+
Urethracontracts
+Pelvic floorcontracts
Bladder filling
Normal desire to voidDetrusorcontracts
+
Urethra relaxes
+Pelvic floorrelaxes
MICTURITION
First sensation
to voidDetrusorrelaxes
+Urethra
contractionincreases
+Pelvic floorcontracts
First sensation
to voidDetrusorrelaxes
+Urethra
contractionincreases
+Pelvic floorcontracts
Bladder filling
Detrusorrelaxes
+
Urethracontracts
+Pelvic floorcontracts
Bladder filling
Detrusorrelaxes
+
Urethracontracts
+Pelvic floorcontracts
Normal desire to voidDetrusorcontracts
+
Urethra relaxes
+Pelvic floorrelaxes
MICTURITION


Normal voiding
Bladder filling and urine storage require:
1. Accommodation of increasing volumes of urine at a low intravesical pressureand with appropriate sensation.
2. A bladder outlet that is closed at rest and during increases in intra-abdominal pressure.
3. Absence of involuntary bladder contractions.

Bladder emptying requires:
1. A coordinated contraction of the bladder smooth musculature of adequate magnitude.
2. A concomitant lowering of resistance at the level of the smooth and striated sphincter.
3. Absence of anatomic (as opposed to functional) obstruction.
Normal voiding

Functional classification of voiding dysfunction
Failure to store
• Because of the bladder
• Because of the outlet
Failure to empty
• Because of the bladder
• Because of the outlet



Symptomatology:
Irritative bladder symptom: storage symptom
Suprapubic areaPain
the ultimate sign of storage failure, associated with urgency, frequency, or nocturia
Time per day, pads per day
Stress, total, overflow
Incontinence
infection, BOO, or neurogenicbladder.
Time per day, degree of leakage
Urgency
Infection, Insomnia, infection, drinking before bed.
how many times the patient awakes from sleep to urinate
Nocturia
functionally reduced bladder capacity, infection, tumor, stone, outlet obstruction, neurogenicbladder, or foreign body
how many hours between voiding
Frequency
Causes How to measureSymptom

Symptomatology:Obstructive symptoms
Residual urine (cath, ultrasound)Feeling of incomplete emptying
DiscomfortTerminal dribbling
BPH, BOO, CBN, stricture urethra, prostate cancer
Cath.cc.Acute urinary retention
UTI, urethritisDiscomfort ,burning in urethraDysuria
Flowmetry (instrument)Poor stream
Discomfort Straining to void
BPH, BOO, CBN, stricture urethra, prostate cancer
Seconds, IPSShesitancy
Causes How to measureSymptom

Different type of incontinence

Differential diagnosis of voiding dysfunction
Overactive bladder dysfunctionOther
Diuretics, sympathomimetics, anticholinergic, decongestants.Pharmacological
Polydipsia, excessive alcohol or caffeine consumption.Behavioral
Ureteral and bladder stoneAnatomical
Post prostatectomy, Cystectomy, traumatic stricture, radiation cystitis.
Iatrogenic
Poorly controlled DM, Diabetes Insipidus, CHF, hypercalcemia, Obstructive sleep apnea.
Medical
Spinal cord injury, cauda equina syndrome, Parkinsonism, Diabetic autonomic neuropathy, Multiple sclerosis, Alzheimer disease.
Neurologic
Prostatitis, Urethritis, STDInfections
Adenocarcinoma of prostate ,TCC of Bladder ,Squamous cell CA of Penis
Malignant disease
Cause of LUTSCondition

Diseases usually cause voiding dysfunction
pediatrics or congenital voiding dysfunction:
• posterior urethral valve
• phimosis ?
• meatal stricture
• fistula ; ectopic ureteralopening, hypospadias,

Hypospadias

• The most common form of infection found in female.
• Caused by gram-negative bacteria colonized in vaginal introitus.
• Symptoms : irritative bladder dysfunction
• Simple bacterial cystitis is always easy to treat with oral form antibiotic
Cystitisdisease usually cause voiding dysfunction

Type of cystitiswhen investigation needed.
• simple bacterial cystitisrecurrent cystitis
unresolved cystitispersistent cystitishoneymoon cystitis
• complicated cystitisanatomic abnormalities : post RT, contracted bladder, stricture
urethraphysiologic disorder: neurogenic, DMrare type bacteria; TB, granulamatousinterstitial cystitisstone hemorrhagic cystitis

Lower UTI in the male
less common than female, ascending infection usually end up as :
• urethritis
• orchitis
• epididymo-orchitis
• prostatitis
Cystitis is uncommon in male!!

Overactive bladder (OAB)detrusor overactivity (DO)
• Urgency with or without incontinence
• Frequency with low volume of urine
• Psychological and emotional involvement
• Normal urine analysis without pyuria and bacteriuria

Neurogenic bladder
Hyperreflexic bladder dysfunction.
CVA , high cord lesion, Pakinsonism etc.
voiding with reflex activity
irritative bladder dysfunction
low residual urine
urinary dribbling, wettingHyporeflexic bladder dysfunction
Sacral cord lesion, DM with neuropathy, myelomeningocoel
no reflex voiding activity
high residual urine ,
recurrence infection
overflow incontinence

Drugs to Facilitate Storage
Drugs to Facilitate Storage: Decrease Bladder Contractility
PropanthelineOxybutyninTolterodine tartrateFlavoxate (Urispas) Trospium (Sanctura) is a balanced M3/M2 selective anticholinergic.Darifenacin (Enablex) is an M3 selective anticholinergic..Solifenacin (VESIcare) is an antimuscarinic with smooth muscle relaxing
properties.Imipramine : dosage: 25 mg PO tid/qid.Hyoscyamine sulfate
Increase Outlet ResistanceEphedrine Estrogens

Drugs to Facilitate Emptying
Increase Bladder ContractilityBethanechol chloride (Urecholine)
Decrease Outlet ResistancePhenoxybenzamine (Dibenzyline) Prazosin (Minipress) Terazosin (Hytrin) Doxazosin (Cardura) Tamsulosin (Flomax) Alfuzosin (Xatral)

Bladder outlet obstructionBPH is the most common disease
Microscopic BPH : histologic evidence of cellular proliferation of the prostate.
Macroscopic BPH : enlargement of the prostate resulting from microscopic BPH.
Clinical BPH : the LUTS, bladder dysfunction, hematuria, and UTI resulting from macroscopic BPH.
Abrams (1994) has suggested using the more clinically descriptive terms benign prostaticenlargement (BPE), BOO, and LUTS to replace BPH.

Histologic BPH

Clinical BPH (with LUTS)

Not all LUTS is BPHLUTS is not disease specific
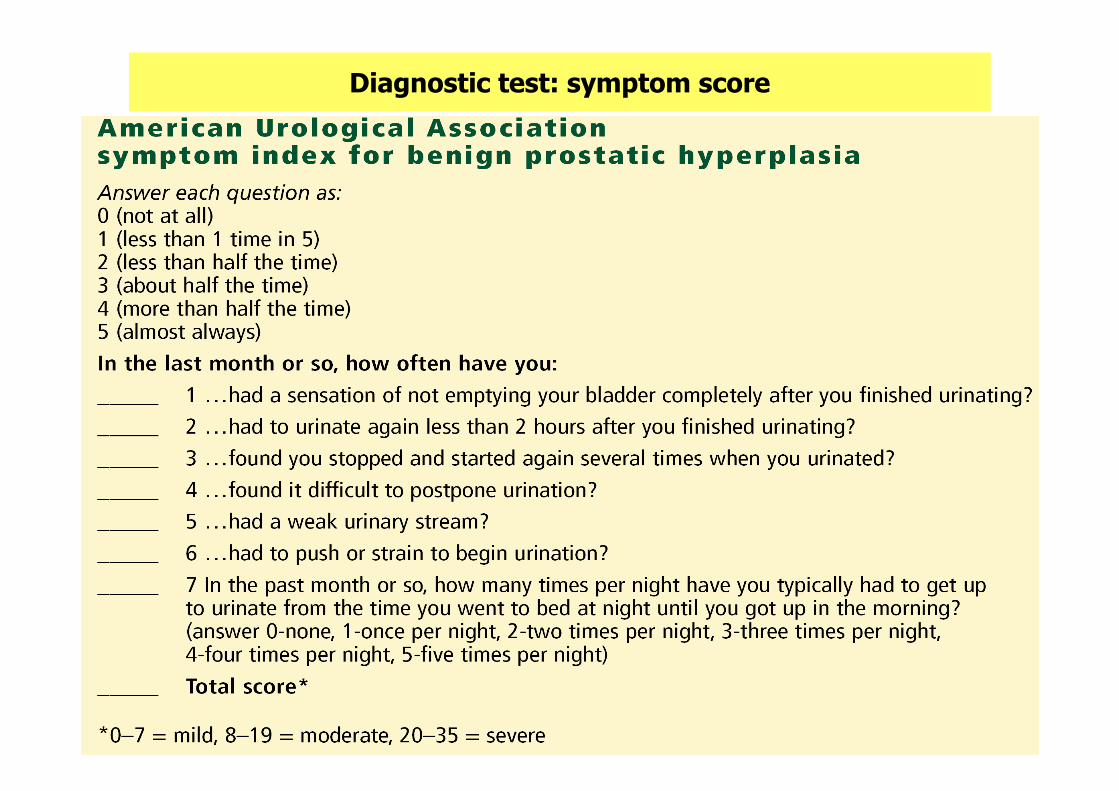
Diagnostic test: symptom score

Digital rectal examination (DRE)
• Size
• Consistency:
slight pressure over the surface to detect whether:
– smooth or elastic – normal
– hard or woody – may indicate cancer
– tender – suggests prostatitis
• Mobility: A malignant gland may be fixed to adjacent tissue
• Anatomical limits: seminal vesicles should be impalpable; induration of these suggests malignancy
Kirby R et al (Eds). Shared Care for Prostatic Diseases 1995

Lab test
• urinalysis, should be normal
• PSA, screen or not screen?
-may be unnecessary for pts less than 10 yrs. life expectancy.
-must accompany DRE
-beware of confounding
������������>70
������������60-70
������������<60
DRE suspectedDRE positiveDRE negativeage range, yrs


Objective measure of urine flow rate, Uroflowmetry : Qmax



Treatment goals for LUTS/BPHin clinical practice
Primary goals :
• Fast symptomatic relief of bothering LUTS.
• Improvement in quality of life (QoL).
• Potentially an increase of maximum flow rate (Qmax)
Secondary goals :
• Reducing in long-term worsening of symptoms.
• Preventing serious complication : AUR

Treatment of BPH
Watchful waitng : suitable for• mildly symptomatic
• not bothersome
• laboratory test is normal
• patient choose not to treatment
Medical treatment :• Moderate symptoms and patient agree to treat.
Surgical treatment• Severe symptom , failure medical treatment
• AUR

Drug use for possible shrinkage of prostate 5 alpha reductase inhibitor (Finasteride)
Drugs use for symptomatic relieve of LUTSalpha 1 blocker
• Doxazosin,
• Tamsulosin,
• Alfuzosin,
• Terazosin
Medical treatment


BPH – a progressive condition
Progression of BPH can be defined in
• increase in prostate volume
• worsening of LUTS, bother, interference with daily activities and quality of life
• deterioration in urinary flow rate
• increased risk of acute urinary retention (AUR)
• increased risk of surgery

Patterns of prostate growth (untreated BPH) (PLESS study)
Patterns of prostate growth (untreated BPH) (PLESS study)
McConnell JD et al. N Engl J Med 1998; 38: 557–63
BaselineYears
Prostate volume (mean % change from baseline)
20
10
–20
0
–10
1 2 3 4

Risk factors for acute urinary retention. J Urol 1997;158:481-487.

Current indications for surgery
• Fail medical treatment
• AUR
• Problems with compliance
• Side effect from medication
• Progressive enlargement of prostate
• Hematuria

Objectives, Do you copy?
• Understand and explain physiologic function and dysfunction of lower urinary tract.
• Evaluation patient with LUTS
• Primary management /investigation
• Give primary management of BPH





























