Embed Size (px)
Citation preview

INDOPOVNilanjana Mukherjee
Voices of the Poor:Making Services Work for the Poor in Indonesia

THE WORLD BANK OFFICE JAKARTA
Jakarta Stock Exchange Building Tower II/12th Fl.
Jl. Jend. Sudirman Kav. 52-53
Jakarta 12910
Tel: (6221) 5299-3000
Fax: (6221) 5299-3111
Website: www.worldbank.or.id
THE WORLD BANK
1818 H Street N.W.
Washington, D.C. 20433, U.S.A.
Tel: (202) 458-1876
Fax: (202) 522-1557/1560
Email: [email protected]
Website: www.worldbank.org
Printed in 2006.
This paper has not undergone the review accorded to offi cial World Bank publications. The fi ndings, interpretations,
and conclusions expressed herein are those of the author(s) and do not necessarily refl ect the views of the
International Bank for Reconstruction and Development / The World Bank and its affi liated organizations, or those of
the Executive Directors of The World Bank or the governments they represent.
The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors,
denominations, and other information shown on any map in this work do not imply any judgement on the part of
The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries.

Bank Dunia | The World Bank
East Asia and Pacifi c Region
Voices of the Poor:Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Nilanjana Mukherjee

Acknowledgements
Voices of the Poor is based upon fi eld work done by a team consisting of Nyoman Oka and Ratna Indrawati
Josodipoero, Co-fi eld team leaders, Wiji J. Santoso, Idul Fitriatun, Ketut Suarken, and Nur Khamid (East Java Team),
Purnama Sidi, Laksmini Sita, Herry Septiadi, and Ririn Fajri (West Java Team), Husnuzzoni, Khusairi, Nazmi Rahkman,
and Indraningsih (South Kalimantan Team), Titik Soeprijati, Irwan, Mochamad Rifai, and Ariati (West Nusa Tenggara
Team).
Field work and analysis for Voices of the Poor was supported by the Indonesia Poverty Analysis Program (INDOPOV),
a partnership program of the World Bank Indonesia led by Jehan Arulpragasam. The report is a qualitative study
intended to supplement the quantitative analysis “Making Services Work for the Poor in Indonesia.”
This work benefi ted from advice, discussion, and critique from members of the INDOPOV team, particularly Menno
Pradhan, Vicente Paqueo, Peter Heywood, and Ellen Tan. Suzanne Charles and Ellen Tan provided valuable editing
support. Claudia Surjadjaja provided health service assessment tools and briefi ng to the researchers. Consultations
with the poor were undertaken by the researchers drawn from several NGOs and academic institutions in
Indonesia.
Grateful thanks are due to the women and men consulted in the Java, Kalimantan, and West Nusa Tenggara
communities, who shared their assessments, experiences, insights, and knowledge to provide a human face and
voice to this study – which we hope will be heard by policy makers.
The author deeply appreciates the support of the management of the World Bank’s Water and Sanitation Program
(WSP), which made it possible for her to undertake this work. Specifi cally, thanks are due to Richard Pollard, the
Regional Team Leader for WSP - East Asia and Pacifi c, and Ede Jorge Ijjasz-Vasquez, the global Program Manager.
For any shortcomings and omissions in this report, the author claims responsibility

vMaking Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Table of Contents
ACKNOWLEDGEMENTS iv
TABLE OF CONTENTS v
LIST OF BOXES, FIGURES, & TABLES vi
GLOSSARY viii
EXECUTIVE SUMMARY x
1. POVERTY CHARACTERISTICS AND LOCAL INSTITUTIONS AT STUDY SITES 11. 1. Sample, Sites, Research Tools 11. 2. Identifying And Engaging With The Poor 21. 3. Local Well Being And Poverty Profi les 2
2. EDUCATION SERVICES USED BY THE POOR 42. 1. Primary Schools: Not Really Free – Despite Government Provisions 42. 2. Secondary School Education Services 62. 3. Quality Of Services - Providers’ Views 82. 4. Independent Observation Results And Conclusions 9
3. HEALTH CARE: PRENATAL, CHILDBIRTH, AND CHILD HEALTH SERVICES 143. 1. Prenatal Services: Preferences Vary With Geography 143. 2. Childbirth Assistance Services: Tba Still Reigns Supreme 163. 3. Curative Services For Young Children (< 5 Years): Public Services Are The Preferred Choice 173. 4. Quality Of Health Services Being Delivered To The Poor 183. 5. Independent Observation Results And Conclusions 21
4. “CLEAN” WATER SERVICES USED BY THE POOR 254. 1. Poor Lack Reasonable Access To Potable Water 254. 2. Water Use And Health Hazards 264. 3. The Poorest Pay The Highest Price For Water 274. 4. Observation Results: “Clean” Water Services 294. 5. Quality Of Services: Views Of The Poor 30
5. SANITATION FACILITIES USED BY THE POOR 315. 1. Observation Results: Sanitation Services 335. 2. Quality Of Services: Various Views 34
6. POOR HAVE LITTLE CLIENT POWER—BUT THEY WANT IT 356. 1. Lack Of Information-“We Don’t Know” 366. 2. “Who Will Hear Us?” 386. 3. Poor Treatment By Pro-poor Service Providers And Offi cials 396. 4. No Voice In Community Decisions And Service Provision 396. 5. Problems With The Participatory Process-“We Are Stepchildren” 40
7. RECOMMENDATIONS FOR POLICY AND STRATEGY 427. 1. For Basic Services In General 427. 2. For Health Services 437. 3. For Education Services 447. 4. For Clean Water And Sanitation Services 45

viMaking Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
List of Boxes
Box 1. No explanation of fees 6
Box 2. Married at 13, childbirth at 14 –the only option after primary school 7
Box 3. No clean water equals no schoolteachers and health workers 10
Box 4. 92 Enrolled but 29 Present 10
Box 5. Pregnancy danger signs unrecognized 17
Box 6. Repeated premature births, No ANC check ups 22
Box 7. No longer possessed by the devil 23
Box 8. Four days too late … 23
Box 9. How to feed my child when breast milk fails? 24
Box 10. Diarrheal death of an infant close to services in a mega city 25
Box 11. The poor pay 30 times PDAM tariff for water – but don’t realize it 27
Box 12. Held ransom by monopolistic water service 30
Box 13. “They give us no choice….” 36
Box 14. “Because i am poor, and therefore also stupid ” 38
Box 15. Kartu sehat users need patience and forbearance 39
List of FiguresFigure 1. Proportion of votes for choice of provider for primary education services 6
Figure 2. Proportion of votes for choice of provider for ANC services 15
Figure 3. Proportion of votes for choice of water services used 26
Figure 4. Proportion of votes for choice of sanitation facility used 32
List of TablesTable 1. Study sites 1
Table 2. Secondary school observations at diff erent sites 13
Table 3. Costs of clean water services and water use by the poor at 8 study sites 28
List of Annex Tables
Table 2.1. Paminggir - Remote, Forestry-dependent Rural Community, South Kalimantan 5
Table 2.2. Bajo Pulau - Island Fishing Community , West Nusa Tenggara 5
Table 2.3. Alas Kokon - Rural, Dryland Farming Community, Madura, East Java 6
Table 2.4. Kertajaya – Irrigated Rice-Farming Rural Community, West Java 7
Table 2.5. Antasari - Urban Kelurahan, South Kalimantan 8
Table 2.6. Jatibaru - Urban Poor Kelurahan on the Outskirts of Bima, West Nusa Tenggara 9
Table 2.7. Simokerto - Urban Low-Income Neighborhood and Squatters’ Settlement, Surabaya, East
Java
10

viiMaking Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Table 2.8. Soklat - Urban Poor Kelurahan in Subang, West Java 11
Table 3.1. Choice and Costs of Primary Education Services Reported by the Poor at 8 Sites 12
Table 3.2. Costs of secondary school education reported by the poor at 8 study sites 15
Table 3.3. Choice and Costs of ANC Services Used by the Poor at 8 Study Sites 19
Table 3.4. Cost of Childbirth Assistance Services Used by the Poor at 8 Study Sites 22
Table 3.5. Costs of One-time Use of Curative Care Services Most Used by the Poor for Their Children
under Five
26
List of Annex Figures
Figure 3.1 Benefi t and value perceptions for primary education services 13
Figure 3.2 Satisfaction Ratings for Primary Education Providers 14
Figure 3.3 Proportion of votes for provider of secondary school education services 16
Figure 3.4 Benefi t and value perceptions for secondary school education services 17
Figure 3.5 Satisfaction ratings for secondary school education providers 18
Figure 3.6 Benefi t and Value Perceptions for ANC Service Providers 20
Figure 3.7 Proportion of votes for choice of provider for Childbirth Assistance Services 21
Figure 3.8 Satisfaction Ratings for Childbirth Assistance Providers 23
Figure 3.9 Benefi t and Value Perceptions for Childbirth Assistance Providers 24
Figure 3.10 Proportion of votes for provider of Infant Health Care Services (2M – 5Y) 25
Figure 3.11 Proportion of votes for provider of Infant Health Care Services (0 - 2M) 25
Figure 3.12 Benefi t and Value Perceptions for Curative Services for Infants (0-2 months) 27
Figure 3.13 Satisfaction Ratings for Curative Care Providers for Infants (0-2 months) 28
Figure 3.14 Benefi t and Value Perceptions for Water Supply Option Used 29
Figure 3.15 Satisfaction ratings for water supply options 30
Figure 3.16 Benefi t and value perceptions for sanitation facilities 31
Figure 3.17 Satisfaction ratings for sanitation facilities 32

viiiMaking Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Glossary
ANC Antenatal Care
Arisan Saving & Credit Group
bidan desa Trained Village Midwife
BKKBN (Badan Koordinasi Keluarga
Berencana Nasional)
National Family Planning Coordinating Board
BOS (Biaya Operasional Sekolah) School Operation Costs
BPS (Badan Pusat Statistik) Central Bureau of Statistics
Dukun Local faith healer
Dusun Hamlet
GDS Governance and Decentralization Survey
GOI Government of Indonesia
Imunisasi TT (Tetanus Toxoid) TT (Tetanus Toxoid) immunization
Inpres Desa Tertinggal Presidential program for disadvantaged villages
Kangkung Leafy vegetable
Kantor Kelurahan Political District Offi ce
Kapuk Silk Cotton
Kartu Sehat Health Card
Kec./ Kecamatan Sub-district
Kelurahan Sections of the village/Urban district admistration unit
Kelurahan /Kantor Desa Political District Offi ce administered by Lurah (Village Chief )
Kepala Desa Village Chief
Kepala Dusun Hamlet Chief
Ketua RT Neighborhood Community Head
Madrasah Religious School, privately managed
Madrasah Ibtidaiyah Community-managed Islamic Schools (grades 1-6)
Madrasah Tsanawiyah Religious school, run by government (Department of Religious Aff airs), grades 6
– 8)
Mantri Paramedic
Menengah Middle/Suffi cient
MOE Ministry of Education
NGO Non Governmental Organization
PDAM (Perusahaan Daerah Air
Minum)
Regional Drinking Water Company
Pesantren Other Islamic Schools
PKK Women’s Family Welfare Program
PLN State Electricity Corporation
Polindes (Poliklinik Desa) Village Birthing Clinic
POSYANDU (Pos Pelayanan Terpadu) Integrated Services Post
Puskesmas Primary Health Centre/ Sub-district Public Health Centre
Pustu (Puskesmas pembantu) Sub-primary Health Centre (outreach facility)
Raskin (Beras Miskin) Cheap Rice

ixMaking Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
SANIMAS Community Sanitation Project piloted in 7 Indonesian cities during 2001-2003,
promoting community-based sanitation solutions for the urban poor
SD (Sekolah Dasar) Primary School (grades 1 – 6)
SDN (Sekolah Dasar Negeri) Government – run Primary School (grades 1 – 6)
SLTP (Sekolah Lanjutan Tingkat
Pertama)/ SMP (Sekolah Menengah
Pertama)
Junior High School or Secondary School, generally grades 7-9
SLTP Negeri/ SMP Negeri Government – run Junior High School
SSIP Small Scale Independent Water Providers
TBA Traditional Birth Attendant (Sando, Dukun Beranak/ Dukun Berobat, Dukun/Bidan
Kampung, Paraji)
UKS (Unit Kesehatan Sekolah) School Health Education Unit
*At the time of the study, 1 US dollar was equal to 9700 Indonesian Rupiah.

xMaking Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Executive Summary
In January 2001, Indonesia decentralized the delivery of most government services to the district level. The center of
gravity for innovation has thus shifted to the districts, where local governments now have signifi cant autonomy to
promote change, both positive and negative. In a country of about 2201 million people and 4402 districts and cities,
this shift has created tremendous potential for innovative local approaches for public sector service delivery.
The World Bank’s Making Services Work for the Poor in Indonesia initiative aims to provide analytical support for
the Indonesian Government’s eff orts to improve access to and quality of basic services for the poor in the wake of
decentralization. Its objectives are to summarize the state of basic service delivery for the poor, identify and analyze
key factors that have an impact on current outcomes, and propose an analytical framework and practical steps for
improving pro-poor service provision.3
None of the fairly extensive literature on decentralization has yet included an analysis of how the poor view the
delivery of public services. This report attempts to fi ll this gap. It tries to understand what constraints the poor
face, and the rationale for choices made by the rural and urban poor with respect to basic health, education, water
supply and sanitation services that they need. The report also describes policy recommendations to improve service
delivery for the poor on the basis of this analysis, and suggestions from the poor and service providers that could
help improve accountability and strengthen relationships among clients, service providers, and policy makers.
This study focused on eight types of key services:4
• antenatal services
• childbirth assistance
• curative services for 0 to 2 month old infants
• curative services for >2 months to 5 year old children
• primary schooling
• transition to secondary schooling
• clean water services
• sanitation facilities (excreta disposal)
These services are important elements in reaching the Millennium Development Goals. High malnutrition, maternal
and infant mortality, and low education can be directly traced back to failings in these services.
1 National Bureau of Statistics BPS, “Proyeksi Penduduk Indonesia, 2000-2005”, 2005
2 Ministry of Home Aff airs
3 For the full report, see the World Bank website, www.worldbank.or.id
4 For the purposes of this report, curative services have been combined. For specifi c results of 0 to 2 months and > 2 months to 5 years.
Please see Annex.

xiMaking Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
It is hoped that this synthesis, which pulls together commonalities and diff erences among eight localities, will be
useful to donors and government in Indonesia, as well as other countries interested in practical ideas for improving
government service delivery.
By participating in the delivery of services and pressuring policy makers and service providers, the poor have
the potential to improve the quality of services they receive. The study explored to what extent the poor do this
and whether they deem their eff orts to be eff ective. The study also sought their views on how they can draw
policymakers’ attention towards the aspirations of the poor and how to improve the accountability of the service
providers to serve poor consumers.
Generally, the policy response in Indonesia to lack of utilization of basic services by the poor, or disappointing
service outcomes, has been to use targeted price subsidies for public service provision, such as the health card and
scholarships programs. These policies presume that the public sector is the most effi cient way to deliver services to
the poor and that the poor do not use them when the fees are too high. This study was designed to take a fresh look
at this hypothesis, which has been driving policy in Indonesia, and to generate suggestions for alternative policies
that are more directly related to the constraints the poor face.
The following fi ndings represent the voices of the poor from eight selected locations in Indonesia. No claim is made
about their being completely representative of the country’s poor.
A number of key messages reverberate throughout the consultations:
1. Perceptions of the poor on service quality were often at variance with independent professional views on
quality.
• The poor perceived traditional birth attendants (TBAs) to be providing better quality service for childbirth
assistance than trained nurse midwives.
• Well water is perceived as clean, whereas river water is not. While the latter is mostly correct, the fi rst is often not.
2. The primary constraint to increasing the number of births assisted by trained service providers appears to be lack
of demand rather than lack of access. The poor do not demand trained midwives’ services because midwives
charge much more and serve their clients for much shorter periods than the TBAs do. Many poor clients were
not fully aware of the additional benefi ts of professionally assisted births. Those who were aware were not certain
the additional benefi ts are worth the high extra cost.
3. Programs for the poor, such as the health card, are highly valued, but researchers found that information about
policies for the poor is typically not available. Often, the public service provider or government offi cial was the sole
source of information about pro-poor services. Often these elites failed to give the poor complete information,
and sometimes they even misused their power, preventing the poor from accessing these services.

xiiMaking Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
4. Community elite—service providers and government offi cials— seldom listened to the poor when the poor
were stating their needs, their concerns, or ideas they have for improvements to service. The poor see themselves
as “stepchildren”; the elites consider the poor as “stupid” and do not want to interact with the poor or provide
them with information. The only way input from the poor is valued is when it is mediated through outside
partners.
5. Non-fee primary school expenses (such as uniforms, books, etc.) are a substantial burden for the poor. The recent
policy to abolish tuition fees for the poor does not address these signifi cant non-fee expenses.
6. Public perceptions about the poor being unable to aff ord quality water and sanitation services are not correct.
The poor in urban areas were buying water from private vendors at 15 to 30 times the tariff s of the district
drinking water companies (Perusahaan Daerah Air Minum, PDAM). While they could aff ord to buy water from
PDAMs at the PDAM tariff rates, they fail to obtain connections due to lack of tenure of lease or land ownership
and the high one-time cash costs of connections. Most of the urban poor could aff ord to build low-cost latrines,
but again lack of land ownership or tenure of residence stands in the way. Also, most are not aware of low-cost
latrine options, both in rural and urban areas.
7. On islands, the poor have little access to clean water, often because of the monopolistic manipulation of the
system by water vendors. This was also true in an urban slum.
8. There is a big diff erence in quality between urban providers serving slum areas and rural providers serving poor
areas. The latter are of much worse quality.
9. Particularly in rural areas, many children enrolled in school do not attend regularly. Their teachers are often
absent. High enrollment rates fail to capture non-attendance.
10. Teacher absenteeism in rural schools and the unavailability of paramedics in rural health outposts (Pustus) were
sometimes tied to the lack of basic infrastructure facilities such as water supply and sanitation facilities in rural
schools and health posts. Teachers were not willing to work in such conditions (although they were willing to be
paid).
11. When there is no secondary school in the village, such as seen in Madura, girls were married off and get pregnant
immediately after primary schooling. When there is a chance of attending junior high, such young marriages
do not occur as frequently. This emphasizes the need to improve girls’ access to junior high school for reasons
beyond educational attainment.

1Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
1. Poverty Characteristics and Local Institutions at Study Sites
1. 1. Sample, Sites, Research Tools
Eight localities were chosen based on BKKBN poverty criteria, inclusion in the Governance and Decentralization
Survey, Badan Pusat Statistik’s poverty maps and geography/locality. Communities chosen, both rural and urban,
had high poverty rates (30 to 80 percent). Social mapping was further used at each site to identify the poorest
neighborhoods for consultation. Half of the sites were chosen on Java, which houses the largest absolute number
of the country’s poor. Two other sites, West Nusa Tenggara and Kalimantan, were included to refl ect conditions
outside Java. The 2003 GDS results had shown high satisfaction rates with public services and popular perceptions
of improved services after decentralization. The quantitative GDS results neither explained why ratings were high,
nor whether the views of the poor diff ered from that of the non-poor. Poor people’s views about services in this
study were far less positive than the GDS results, possibly refl ecting the experience of the poorest segments.
Criteria for selection of rural sites included principal livelihoods (irrigated rice-growing farmers in West Java, an
island fi shing community in West Nusa Tenggara, a forestry-dependent upland agricultural community in South
Kalimantan, and a dry land agricultural community in Madura (see Table 1).
Table 1. Study Sites
JAVA OFF-JAVA
Rural Urban Rural Urban
Irrigated agriculture-based
livelihoods
Desa Kertajaya, District
Subang, West Java
Mega city slum
community
Kelurahan Simokerto,
Kecamatan Simokerto,
District Surabaya, East Java
Forestry and upland
agriculture livelihoods
Desa Paminggir,
Kecamatan Danau
Panggang, District Hulu
Sungai Utara, South
Kalimantan
Small town community
Kelurahan Antasari,
Kecamatan Amuntai
Tenggah, South
Kalimantan
Dry land agricultural
livelihoods
Desa Alaskokon,
Kecamatan Modung,
District Bangkalan,
Madura
Urban poor community
Kelurahan Soklat,
Kecamatan/Kota Subang,
West Java
Coastal fi shing
community
Desa Bajopulau, District
Sape, West Nusa Tenggara
Small town community
Kelurahan Jatibaru, Bima
City, West Nusa Tenggara

2Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Research methods included the use of participatory analysis tools and focus group discussions with poor men and
women, and in-depth interviews with individuals selected for case studies. A total of 450 people were consulted.
The views of four subdistrict health center doctors, six village midwives (bidan desa), two paramedics, four traditional
birth attendants, seven primary school teachers, and three secondary school teachers were incorporated into
fi ndings. Observations with service quality standard checklists were carried out at 16 primary school classes, eight
secondary school classes, homes of four TBAs and two bidan desas, six subdistrict health centers and two sub centers.
Water fi lling and supply facilities were observed for two Small Scale Independent Water Providers (SSIPs); 16 school
sanitation facilities and 23 household sanitation facilities were observed. Teams spent a total of 42 person-days in the
fi eld between October and November 2005.
1. 2. Identifying and Engaging with the Poor
It is easy to miss the real poor while carrying out community level consultations or research. The poor, who are
at the bottom of the social ladder, rarely attend community meetings. They cannot aff ord to take time off from
work and often they are not invited to meetings. From past experience, the poor have no reason to trust outsiders
and talk freely about their experiences, which are often very diff erent from the glossed-over versions repeated by
formal leaders. Researchers were equipped with a sequence of participatory analysis and qualitative research tools
(described in Annex 1, pg. 1-4) designed to address the communication barriers described above and gather views,
assessments and experiences of the poor.
Four research teams of four people each spent four to fi ve days in each community. Each team had two men and
women from NGOs or academia who held sessions with men and women’s groups. They explained the purpose of
the study, fi rst to the formal leaders of the communities and then to the poor.
The interest at each site was high. No one had asked the poor about their views regarding basic services before.
They were at fi rst surprised, and then expressive in their assessments and explanations. As work progressed, visual
analysis tools attracted participants and attendance grew. No incentives were off ered for participation and none was
needed. The group sessions resembled enjoyable social events which lasted late into the evening.
1. 3. Local Well Being and Poverty Profi les
For detailed information on sites and poverty, see Annex 2, pg. 5-12. It is particularly interesting to note diff erences
in who is considered poor by local standards compared to offi cial standards.
PAMINGGIR: Paminggir, a remote village of 333 households in kecamatan Danau Panggang, district Hulu Sunggai
Utara in South Kalimantan, is classifi ed as a “left behind village” by the GOI program Inpres Desa Tertinggal. Half of the
households are poor, by local standards. Well-being is measured in terms of one’s control over means of livelihoods,
i.e. boats, fi shing equipment, fi shponds, and buff aloes. The poor are defi ned, in contrast, by what they do not have.

3Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
The village is accessible only by boat, two to six hours away from the district capital. The community depends on the
river for its livelihood, fi shing, as well as transport. Land is swampy, unsuitable for crops. Rainfall is heavy and fl ooding
is frequent. The community has one public primary school, a secondary school and a sub-health center open two to
three days a week. The nearest bidan desa is six kilometers away, the nearest health center 14 kilometers and diffi cult
to reach. The village has no clean water source or sanitation facility. Paminggir received a state electricity corporation
(PLN) connection in 1999.
BAJO PULAU: Bajo Pulau is a small village with 380 households on a 91 hectare island off the coast of Sumbawa in
Kecamatan Sape, West Nusa Tenggara. Most households depend on fi shing. Two decades ago, they used explosives
and potassium cyanide to fi sh; since 1987 they have focused on lobster and pearl harvesting, which provides better
income. There is little infrastructure; there are no puskesmas or private doctors on the island. Clean water has to be
brought from another island. There are three run-down primary schools, which function two to three hours a day.
Schoolteachers and bidan desa do not live on the island; the Bidan is thus rarely available when needed.
ALAS KOKON: This village of 508 households is in district Bangkalan, Kecamatan Modung, on Madura island. It has a
high 46 percent poverty rate by the BPS poverty map and 80 percent poverty rate by BKKBN criteria. The community,
using local standards, puts the poverty rate at 67 percent. Households are dependent on seasonal dryland agriculture
(corn, soybean, chillies, legumes and seasonal crops such as mango, banana and silk cotton—kapuk). Alas Kokon has
one public and one private primary school. There is a Pustu/Polindes in the village; the Puskesmas is seven kilometers
away. Clean water supply in dugwells is limited in quantity and sanitation access is minimal.
KERTAJAYA: Farmers grow fi ve tons per hectare of rice in the fertile soil of the West Java village of Kertajaya in
Subang district, Kecamatan Binong. Of the 1159 households, only 197 households are land owners; none of the poor
(63 percent of the population) own land. The village has good access to markets and is connected to Subang, the
district town, by bus or motorbike taxis. Houses of the rich on the main road have PDAM water connections others,
including the poor, use dug wells. A puskesmas is fi ve kilometers away; a bidan desa lives in the village. Kertajaya has
two public and one private primary school.
ANTASARI: This urban kelurahan in Kecamatan Amuntai Tengah, district Hulu Sungai Utara, has poverty rates of
more than 30 percent (BKKBN). The population is a mix of people from various parts of Kalimantan and Java, Sumatra
and Sulawesi. The Kelurahan has 1,243 households engaged in a variety of trades and services. The poor in Antasari
are mostly wage laborers in markets, at construction sites, and seasonal fi shers in the river. Education and health is
accessible (two public primary schools, one public secondary school, a puskesmas). Although PDAM provides piped
water to homes of the better off , the poor are not connected.
JATIBARU: The urban kelurahan in Bima city in West Nusa Tenggara Province is located in a fl ood-prone area. The
livelihoods of 1,886 refl ect an urban/rural mix: in the agricultural season the poor are wage laborers in farmlands of
neighboring Bima city, in other seasons they collect and sell fuel wood or work as vendors or day laborers in brick

4Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
kilns and factories. Jatibaru has fi ve public primary schools, two public secondary schools, and one Pustu served by
three health workers; a Puskesmas and a public hospital are within two kilometers. The poor get their water from
unprotected dug wells and shallow bore wells; a piped water system built by CARE has fallen into disrepair: “The
community has no funds to repair” was the reported reason.
SIMOKERTO: Simokerto is an urban village in kecamatan Simokerto, district Surabaya, in East Java Province. The
village, 10 kilometers from Surabaya, situated in the middle of commercial and industrial areas, has a 90 percent
poverty rate (BKKBN). There is little social cohesion among the approximately 3,500 households: some live in a
squatter settlements on land owned by the state railways. The poor struggle to survive through a variety of work.
There are no health services in Simokerto, but Pustu and Puskesmas are nearby. Simokerto has eight public primary
schools, two private primary schools and a private high school. The nearest secondary school is three kilometers
away. A few rich have PDAM connections. The rest buy clean water from vendors. The poor mostly use dug well
water. Some houses have unimproved sanitation facilities that directly discharge into drains and black-colored
streams. Poor squatters have no sanitation access except one public toilet.
SOKLAT: Soklat is an urban village of 2,881 households. 54 percent of the households is poor (local criteria) in
kecamatan and district Subang, West Java Province, three kilometers from the Kecamatan capital. Though classifi ed
as urban, the region has irrigated rice cultivation and about 40 percent of poor households’ income is derived from
agricultural labor. Others work at construction sites, in shops, or pull carts as transportation laborers. A large proportion
of poor households send members overseas for wage labor. Agents regularly visit the village to recruit people and
provide loans for travel expenses, thus binding the recruited people into exploitative service agreements.
2. Education Services Used by the Poor
2. 1. Primary Schools: Not Really Free – Despite Government Provisions
Lack of education is a basic fact for the poor in Indonesia. At six of the eight sites, the poor cited one of the
characteristics of poverty as: “Children of poor households are often not enrolled in primary school/do not complete
primary school/just manage to fi nish primary school.”
In July 2005, the Indonesian government promised to provide nine years of free basic education for all school aged
children via Operational Aid for Schools (BOS) grants. Nonetheless, the poor still pay hefty entrance fees (sometimes
called building fees), particularly in Java (see Annex 3, Table 3.1).
Although students reportedly are no longer paying monthly tuition fees (which ranged from Rp.2,000 – 17,000
per month), cost of books, uniforms, fees for computers, examinations, and certifi cates can add up to Rp.100,00
– 150,000 per child per year. Additional “hidden” costs include shoes (required by some schools), school bags, snacks,
etc. (see Annex 3, Table 3.1).

5Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Top Choice: SDN
The poor prefer public schools. At most sites there was some choice among several government-run primary
schools (Sekolah Dasar Negeri or SDN), and in some cases also community-managed Islamic schools (Madrasah
Ibtidaiyah). At seven of the sites the primary school chosen by most of the poor was the SDN. The factors that the
poor mentioned in making this choice were:
• The SDN is near home; no transport costs; children can go alone; no need to cross main roads.
• SDN is free for the poor.
• Teachers are good; children learn many things in SDN. In Madrasah they get only religious teaching.
• Children fi nishing the SDN receive a certifi cate.
The only site where the Madrasah was preferred was Alas Kokon in Madura. Parents’ reasons for this choice:
• The Madrasah does not require costly uniforms.
• Teachers are more disciplined and regular at the Madrasah. The SDN teacher is often absent/not disciplined
• SDN only teaches children to read, write and count. At the Madrasah they also learn religious practices and
Qur’an reading.
Poor men and women generally think the benefi ts of primary education at public schools outweigh the costs (see
Figure 1 and Annex 3, Figures 3.1 and 3.2,). However, paying for that education, particularly when there are several
children, is a challenge.
Satisfaction ratings depend on the quality of individual teachers and the degree of transparency in the school’s
fi nancial dealings with parents (see Box 1).
The Burden of Additional Fees
The poor feel burdened by the cost of schools:
- “Why must books be changed every semester?”,
- “Why not have books that work for the whole year?”,
- “Why do school books cost so much?”,
- “Why are we charged for certifi cates?”
are recurrent questions. Unpaid entrance and certifi cation fees pile up. Schools increase the burden by withholding
passing certifi cates from defaulters, causing frustration and friction between poor parents and school authorities.
Even the kepala dusun (head of hamlet) of Simokerto had trouble paying the registration fee (typically kepala dusuns
are better off than the rest of their community). Only one of his three children received the school certifi cate after
full payment of the Rp750,000 (US$75) fee, roughly equivalent to three and a half months income of a local poor
household.

6Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 1. Proportion of votes for choice of provider for primary education services
86%
14%
SD Negeri Madrasah Ibtidaiyah
78%
22%
Women’s View Men’s View
Education costs at the SDN vary widely among the sites (see Annex 3, Table 3.1). In Paminggir (South Kalimantan),
school is almost free with only nominal enrollment and school completion certifi cate fees; in the Surabaya slum,
enrollment fees and books amount to Rp.830.000.5 At West Java sites, parents pay 10 to 15 times more than elsewhere
to obtain primary school completion certifi cates. At Soklat, the men’s group complained that despite having paid
Rp.68,000, they still had not received the certifi cate. (In comparison, the privately run Madrasah Ibtidaiyah costs only
Rp.5,000 – 10,000 per month).
Box 1. No Explanation of Fees“We heard that in SDN Cibarola, at the time of getting the certifi cate, all the parents were invited to a meeting and informed that it will cost
Rp. 60,000. They were also informed of details of the cost. But in SDN Ds. Samsi, we parents were never informed nor invited to any meetings. I
have contributed several times – the total comes to Rp. 68,000. Why is it more than in SDN Cibarola? I asked the school principal but I was not
heard. And the certifi cate is still not given. Every time I ask, the principal says – later, later”.
Father of a child fi nishing primary school, Soklat, West Java
2. 2. Secondary School Education Services
“Free? What free? We don’t have to pay monthly tuition now, but we have to buy books and uniforms and pay building
maintenance fees. In the past we just paid Rp.10,000 – 20,000 every month and nothing else. Now we have to spend
Rp.200,000 at the start of the year.”
- Vegetable vendor and mother of two school children in Jakarta
Reported in The Jakarta Post, July 17, 2005
5 Registration or building fees range from Rp. 50,000 – Rp.100,000 per child at the NTB urban and West Java rural sites. The fees, which may be paid in
installments, reportedly cause many students to drop out. In addition, recurrent costs other than tuition (books, computer fees, uniforms, bags and
shoes, etc.) added up to Rp.100,000 – 150,000 per year.

7Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Extra Fees a Problem, again
Public junior high school represents a major fi nancial burden for poor families. Poor households try to send at least
one child to junior high school—Sekolah Lanjutan Tingkat Pertama (SLTP) or Sekolah Menengah Pertama (SMP)—
but can rarely aff ord to send all.
Only three children from Kertajaya village go to secondary school — and that is an Islamic boarding school (Pesantren)
outside the village. Bajo Pulau has no secondary school and no children are sent to study outside the village.
At urban sites Jatibaru, Simokerto and Soklat, respondents enrolled at least one child in SMP or Madrasah, whichever
is available and not too far from home. They prefer the Madrasah as there are no entry or construction fees. Entrance,
registration, and building fees are not fi xed, ranging from Rp.200,000 – 600,000 (see Annex 3, Table 3.2). The schools
charge whatever they can, depending on their reputation and popularity—and justify the fees on the basis of extra
subjects or facilities off ered. Reportedly, such charges have no legal basis.6 A comment from the men of Kertajaya
sums up the parents’ frustration: “To enter SMP Negeri calls for at least Rp.1.5 million. On top of that, there are the costs of
transportation, food etc. Who can aff ord it?”
Public Schools Most Popular, but Islamic Schools are Important
Pesantren or other Islamic schools (Madrasah Tasanawiyah) were chosen over SMP by 37 percent of the men and
women in the study, and were the popular choice at two sites, Alas Kokon and Antasari (see Annex 3, Figure 3.3).
Kertajaya and Bajo Pulau have no secondary schools and the remaining four sites chose the SMP available in the
community.
In Alas Kokon and Antasari, parents who send children to the Madrasah Tsanawiyah (religious schools run by the
Government Department of Religious Aff airs) seem highly satisfi ed. In Alas Kokon, the school costs Rp.1,500 a
month; in Antasari, annual fees are Rp.100,000, but all children received fi nancial aid this year. It is a “model” school.
Its services are complete and parents consider it very good value for money.
The SMP in Paminggir (South Kalimantan) is free, but the quality of the school facilities and education are very low.
Costs of the SMPs in Java and NTB are much higher (Rp.400,000 –600,000) (see Annex 3, Table 3.2).
When fees are charged the poor think that the SMP Negeri does not off er suffi cient value for the cost, whereas the
Madrasah Tsanawiyah does. Women are particularly dissatisfi ed because (see Annex 3, Figures 3.4 and 3.5):
• The SMP is far from home – transportation costs are high / not on public transport route.
• SMP is expensive. On top of that, it costs another Rp.450,000 to get the completion certifi cate (Simokerto).
• The classrooms are shared with the primary school (Jatibaru).
6 According to the Director of Paramadina University Center for Education Reform, Hutomo Danangjaya, state schools need no additional building
maintenance funds because they already have well-maintained buildings. Jakarta Post, July 17, 2005.

8Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Lack of Secondary Schools Means Girls Must Marry
Girls’ lives are drastically changed when the secondary school is inaccessible either due to distance or cost. In these
cases, the girls are married off soon after primary school and become pregnant just after they enter puberty (see Box
2). Maternal and infant deaths and disabilities are common in such pregnancies.
Box 2. Married at 13, childbirth at 14 –the only option after primary schoolOn September 15, 2005 in Alas Kokon village on Madura, researchers met Nurhayati who is 14 years old. She had just given birth to her fi rst
child after three days and nights of diffi cult labor. She was fi rst assisted by the local TBA, but later the bidan desa had to be called to help. She
did not die—this time. In the absence of a secondary school in the village, every girl in the area is married off right after primary school; im-
mediate pregnancies are inevitable, death is a high probability. How can Nurhayati and other young girls be empowered to gain any control
of their bodies and lives?
Site Report, Alas Kokon, Madura
2. 3. Quality of Services - Providers’ Views
Primary School Teachers’ Views
At seven sites the researchers met and interviewed teachers at state primary schools. At Paminggir, the night
watchman was substituting for a habitually absent teacher.
Teachers at rural primary schools state that they are able to provide very little in terms of quality education. Schools
have only two or three classrooms serving six grades. School buildings are in disrepair, but reports to the education
department bring no results. Rural schools in remote places like Paminggir and Bajo Pulau island have trouble
keeping teachers in school because of lack of basic services such as clean water and sanitation.
The teachers say that children tend to drop out and work, once they gain basic literacy and numeric skills. Parents
see no value in further education for their children. Sometimes a school will provide incentives such as funds for
transport or second-hand uniforms to encourage the poor children to stay in school.
The outlook of urban primary school teachers is much brighter. They believe they are providing very good value for
cost to poor students. They recounted the many pro-poor measures in place in the schools such as scholarships and
fund raising drives to pay for poor students’ uniforms, writing materials, and extra-curricular activities. In Antasari
and Jatibaru they said that parents know about the quality of the school and the pro-poor measures. At two urban
primary schools the teachers said that poor students do not have textbooks and suggested that the school should
lend books to the poor students.
Educators’ and parents’ assessments sometimes are far apart. The principal of the primary school in Soklat exalted the
quality of his school as “200 percent.” He emphasized that school administrators frequently interacted with parents,

9Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
maintained transparency of funds, and allowed poor parents to pay fees in installments. Poor parents disagreed, and
complained that completion certifi cates were withheld and that information about waiver of tuition fees had not
been publicized.
Secondary School Teachers’ Views
The state secondary teachers interviewed were in Soklat, West Java and Antasari, South Kalimantan. In Paminggir,
rural Kalimantan, the village chief was serving as a volunteer teacher in place of the absentee state-paid teacher.
The teacher in Soklat argued that education could not be totally free, although the school does consider the
economic capacity of parents and allows them to pay the registration/building fee in installments. According to
him, the issue of education costs is over emphasized: “If they just smoke one cigarette less a day, it would be possible
to save enough to pay Rp. 15,000 a month for education.”
The principal of the Madrasah Tasanawiyah Model School in Antasari said government funds are suffi cient to cover all
fees and other study and extracurricular materials for students identifi ed as poor. Poor parents gave very high marks
for value and quality to this large school, which has seven to eight sections for each grade, totaling 23 classrooms.
This school is funded by the Department of Religious Aff airs.
2. 4. Independent Observation Results and Conclusions
Primary Schools- Quality of Service
Only state primary schools were observed. The four rural schools observed are in markedly poor condition, and
delivering signifi cantly lower quality services than the urban schools.
Although all primary schools are designed for Grades 1 through 6, rural schools had only two to three classrooms
necessitating grades to group together. None of the rural primary schools had clean water; half had no sanitation facilities.
Sanitation facilities at the other schools were present, but were damaged and unusable. None had electricity or a library.
Three had damaged roofs.
At the four rural schools attendance on the day of observation ranged from 28-92 percent. Classrooms were dusty
and littered, with damaged fl oors, but there were suffi cient chairs, adequate ventilation, and daylight. Wallboards
were the only classroom resources. No students’ work was displayed on walls. Frequently, students were left alone in
classrooms, without a teacher. Discipline levels were low.
Teachers did not live in the village but commuted from urban areas, and were often late or absent. Their reasons: lack
of clean water and sanitation services (Bajo Pulau, Paminggir, Alas Kokon), see also Box 3.

10Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Less than a quarter of the students in observed classes had textbooks and writing material. Teachers showed very
limited questioning skills and did not generate interactions with students. No student asked any questions in any of
the classes. Teacher displayed no gender bias in dealing with students, and used a mix of Indonesian and the local
language.
Box 3. No clean water equals no schoolteachers and health workers in the villagePak Sahrul, the school watchman/stand-in teacher at the Paminggir public primary school says government-employed teachers (Guru Negri)
are frequently absent.
“I enter the class and teach whatever I can when the teacher is not there,” he says. “It is better than letting the children waste their time.”
Sahrul says teachers live in towns, far away from the village, even though they have been provided free lodging. Paminggir has no clean water
supply and everyone has to use the river water for all purposes – cooking, drinking, washing, bathing, as well as defecation. The Guru Negeri
from the towns are not used to this. They return to the city to do their washing and are often late to report back to work.
Site report, Paminggir, South Kalimantan
Box 4, illustrates why students and parents do not value the education being provided at a rural primary school in
NTB.
Box 4. 92 Enrolled but 29 presentTison dropped out of primary school in grade fi ve to help his family by working as a ferry boat operator. He now earns around Rp.100,000 (US$
10) month, giving most of his earnings to his father.
When asked why he preferred work to attending school, Tison said he had already learned to read, write and count and wasn’t learning much
else. Teachers came from the mainland, arrived late at 9 and sent the children home at 11 a.m.. School dismissed at 11 a.m. Grades 2, 3, 4 and 5,
6 were grouped together, consequently they were unruly and too big to manage. Surroundings were dismal: no water or sanitation facilities,
not enough chairs, and leaks in the roof. On top of that, Tison was bored.
On the island boys generally drop out of school between the third and fi fth grade, leaving mostly girls enrolled in primary school. On the day
researchers visited the school, only 29 out of the 92 children were present.
Site Report, Bajo Pulau, NTB
Urban Primary Schools: In contrast the urban schools were markedly better than their rural counterparts in terms
of facilities as well as teaching processes.

11Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Illustration 1: The Urban/Rural Divide: Conditions are good at urban state primary schools, as exemplifi ed by the
class in Soklat, West Java (left) and the school in Simokerto, East Java (right), which has a library
All four urban primary schools (SDN) had a reliable clean water supply. Sanitation facilities, while present and
functional, were minimal, with only one or two toilets serving up to 200 children. All schools had electricity and
suffi cient classrooms, but only two had a library and a sports fi eld. Two claimed to off er computer classes. Classrooms
observed were clean, well ventilated, and in good condition. Basic classroom resources like blackboards and wall
charts were present and used whilst chairs and tables for students and teachers were suffi cient.
Student attendance rates on the day of observation were a high 87-100 percent. At two sites, there were signifi cantly
fewer girls than boys.
Less than a quarter of students in observed classes had textbooks, copybooks and writing materials. The one
exception was SDN Murungsari 2 in Antasari, South Kalimantan, where more than three quarters of the students
had and used these learning materials during the class
Teachers present in all classes were well prepared and skilled in asking questions and engaging students’ attention.
Students, however, asked questions at only two schools. The teachers used local languages combined with Bahasa
Indonesia, checked for student understanding, did not display gender bias, and controlled their classes well.
Secondary Schools: Quality of Service
Illustration 2: Classrooms in the rural state primary
school of Bajo Pulau devastated by storms and fl ooding
three years ago.
In general, the quality of facilities available and education
processes of state secondary schools were far superior to those
observed at state primary schools.
Secondary schools were available and observed at all four urban
sites, but only at one rural site (SMP Negeri in Soklat, Simokerto,
Jatibaru, Paminggir and Madrasah Tasanawiyah Negeri Model in
Antasari).

12Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
School buildings were permanent constructions; classrooms were in good condition, well ventilated, and adequately
lit with natural light. All urban schools had electricity and clean water supply available. Remote, rural Paminggir’s
school was supplied with river water pumped up to the school and generator-provided electricity. Two of fi ve
schools seen had libraries.
In three schools, two toilets were meant to serve 200-300 children and in all these cases the toilets were broken. In
two other schools six to eight toilets were well maintained. A separate toilet was allocated for teachers.
Illustration 3: Rural conditions are not conducive to
learning. At state primary school in Alas Kokon, grades
2, 3, and 4 are combined in one room. Children amuse
themselves—sometimes becoming quite rowdy—
because the teacher is absent.
The secondary schools had 6-23 classrooms at diff erent sites.
Except in Jatibaru (Bima) they were clean and in good condition.
On the day of observation, classes had upwards of 92 percent
attendance everywhere. Girls signifi cantly outnumbered boys
present (see Table 2). Reasons were not clear and warrant further
investigation.
Illustration 4: Urban state secondary school, Subang, West Java

13Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Table 2. Secondary school observations at diff erent sites
Present in observed classes
Girls Boys
Paminggir (South Kalimantan) 23 15
Antasari (South Kalimantan) 29 11
Jatibaru (NTB) 21 16
Simokerto (East Java) 35 8
Soklat (West Java) 21 23
More than three-quarters of the students were equipped with copybooks and pen or pencil, fewer than a quarter had
textbooks. Teachers appeared well prepared for their lessons. At two sites teachers taught only in Bahasa Indonesia.
At other sites they combined it with local languages.
Conclusions
1. Quality of primary education service in rural areas was observed to be very poor. The condition of the school
infrastructure was not conducive to learning.
2. Providing incentives to poor households for secondary schooling of girls or making it easier to send girls
to secondary schools can be a strategically important investment to delay teen pregnancies, give girls an
opportunity to gain control over their lives, and improve human development outcomes in Indonesia.
3. Teacher absenteeism was a key problem in rural areas that lacked clean water and sanitation—which reportedly
makes teachers from urban areas unwilling to stay in the villages. When they are absent, children are let out
of school, left in classes without teachers, or taught by teacher substitutes who have no training in teaching
methods and education levels no higher than secondary school. Most primary school students lacked textbooks
and writing materials, which lowered the quality of teaching and learning.
4. Lack of clean water and sanitation facilities in rural primary schools also made it impossible to inculcate basic
hygiene practices. Children observed had poor personal hygiene.
5. Urban state primary schools were better than rural schools in terms of basic infrastructure, except for sanitation.
Urban primary schools had teachers with adequate teaching skills. Most students lacked textbooks.
6. The quality of infrastructure and educational facilities, as well as the quality of teaching at the secondary schools
were far superior to those at the primary schools. This, however, made little diff erence to the poor since, according
to the study, children from poor households rarely progressed beyond primary school.

14Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
7. Out of all the schools observed, the state primary school (SDN Murung Sari 2) and the state secondary school
(Madrasah Tasanawiyah Negeri Model, Sungai Malang), both in Antasari, seem to stand out above the rest,
followed by SMP in rural Paminggir. Ironically, these schools were charging the lowest fees and off ering the most
scholarships for poor students. All three schools are located in South Kalimantan. Parents are highly satisfi ed with
these schools, probably because the local government in South Kalimantan seemed to have made a dedicated
eff ort to fund quality education for the poor with a higher per student budget allocation than at other sites.
3. Health Care: Prenatal, Childbirth, & Child Health Services
The availability and aff ordability of the services and poor people’s perceptions of value and quality determine the
choices they are making. Typically, women make decisions about providers; men are involved only when expenditures
rise above Rp.10, 000. Each choice is highly rational, based on weighing of benefi ts and costs as perceived by the
poor. Policies to improve service delivery to the poor can be eff ective only if they are cognizant of the ways and
reasons the poor make their choices.
During the 1990s trained nurse-midwives (bidan desas) were introduced all over Indonesia in an attempt to lower
high maternal mortality rates. A decade later, bidan desas do not seem to have caused a large shift in the poor
population’s preference away from the traditional birth attendants (TBAs) for obtaining childbirth assistance
services.
3. 1. Prenatal Services: Preferences Vary with Geography
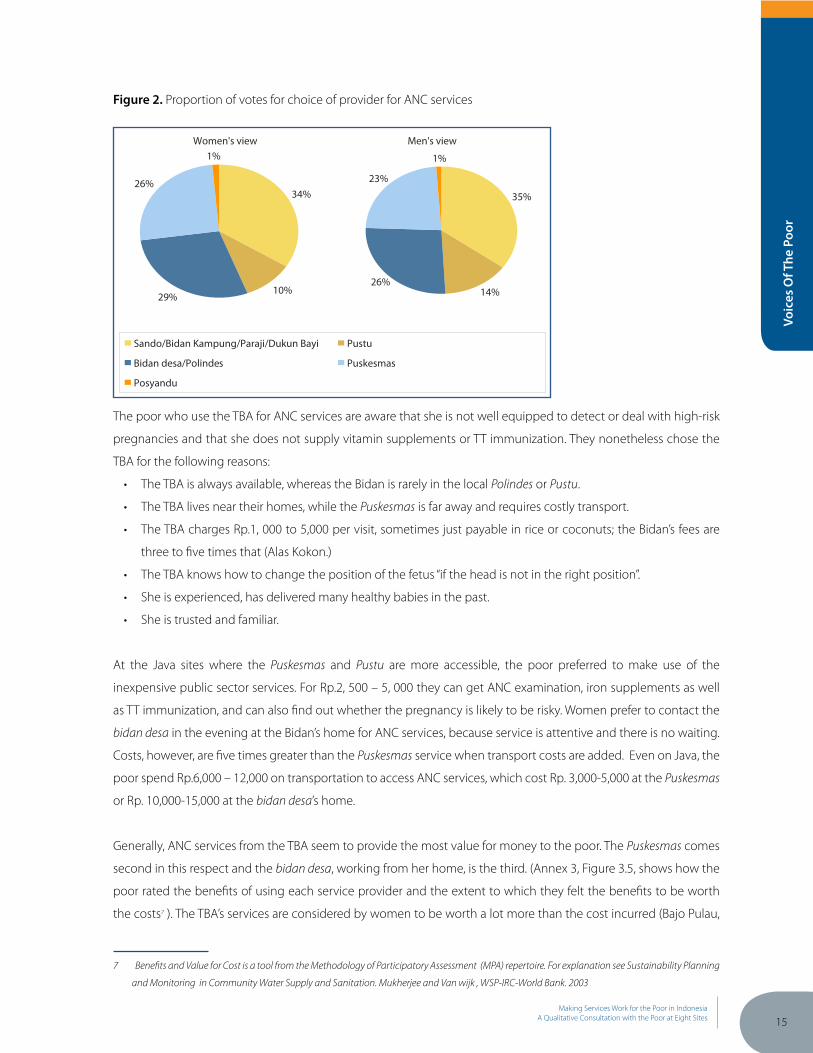
Approximately 65 percent of all the poor surveyed use public sector providers, i.e. the bidan desa, Puskesmas or Pustu,
while the remaining 35 percent use the traditional birth attendant known by various names such as dukun bayi,
dukun beranak, sando, paraji, bidan kampung (see Figure 2).
The TBA was the most popular choice at all sites outside Java. At the Java sites, both rural and urban, the bidan desa
or the Puskesmas/Pustu were preferred choices, except in Alas Kokon village on Madura.
Generally the pregnant woman or older female members of the household chose the ANC service provider. Costs of
the most used option and its closest comparators are shown in (see Annex 3, Table 3.3).
15Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 2. Proportion of votes for choice of provider for ANC services
Women's view Men's view
34%
10%29%
26%
1%
Sando/Bidan Kampung/Paraji/Dukun Bayi Pustu
Bidan desa/Polindes Puskesmas
Posyandu
35%
14%26%
23%
1%
The poor who use the TBA for ANC services are aware that she is not well equipped to detect or deal with high-risk
pregnancies and that she does not supply vitamin supplements or TT immunization. They nonetheless chose the
TBA for the following reasons:
• The TBA is always available, whereas the Bidan is rarely in the local Polindes or Pustu.
• The TBA lives near their homes, while the Puskesmas is far away and requires costly transport.
• The TBA charges Rp.1, 000 to 5,000 per visit, sometimes just payable in rice or coconuts; the Bidan’s fees are
three to fi ve times that (Alas Kokon.)
• The TBA knows how to change the position of the fetus “if the head is not in the right position”.
• She is experienced, has delivered many healthy babies in the past.
• She is trusted and familiar.
At the Java sites where the Puskesmas and Pustu are more accessible, the poor preferred to make use of the
inexpensive public sector services. For Rp.2, 500 – 5, 000 they can get ANC examination, iron supplements as well
as TT immunization, and can also fi nd out whether the pregnancy is likely to be risky. Women prefer to contact the
bidan desa in the evening at the Bidan’s home for ANC services, because service is attentive and there is no waiting.
Costs, however, are fi ve times greater than the Puskesmas service when transport costs are added. Even on Java, the
poor spend Rp.6,000 – 12,000 on transportation to access ANC services, which cost Rp. 3,000-5,000 at the Puskesmas
or Rp. 10,000-15,000 at the bidan desa’s home.
Generally, ANC services from the TBA seem to provide the most value for money to the poor. The Puskesmas comes
second in this respect and the bidan desa, working from her home, is the third. (Annex 3, Figure 3.5, shows how the
poor rated the benefi ts of using each service provider and the extent to which they felt the benefi ts to be worth
the costs7 ). The TBA’s services are considered by women to be worth a lot more than the cost incurred (Bajo Pulau,
7 Benefi ts and Value for Cost is a tool from the Methodology of Participatory Assessment (MPA) repertoire. For explanation see Sustainability Planning
and Monitoring in Community Water Supply and Sanitation. Mukherjee and Van wijk , WSP-IRC-World Bank. 2003

16Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Alas Kokon, Jatibaru). Yet, at least at all the Java mainland sites, the poor were choosing the Puskesmas or the bidan
desa for ANC services rather than the TBA. They did this in order to minimize the risks of complicated labor and large
unexpected expenses during childbirth – through timely detection of possible high-risk pregnancies.
3. 2. Childbirth Assistance Services: TBA Still Reigns Supreme
Fees per birth assisted: SOKLAT / West Java
Paraji (TBA):
Rp.50,000 - 100,000 or Rp.50,000 + 5 kg rice
Bidan Desa:
Rp.300,000 - 400,000
As long as the birth is expected to be normal, the TBA is the most
popular and obvious choice everywhere. Barring the big city
slum site of Simokerto, at every site the TBA was the fi rst choice
among women (76 percent) and men (64 percent). (See Annex
3, Figure 3.7) Although the most obvious reason seems to be the
diff erences in costs, there are several other factors favoring the TBA. The bidan desa’s services for childbirth cost more
than an average poor household’s monthly income, and have to be paid for in cash. In contrast, the TBA can be paid
fl exibly in cash plus in-kind, at a rate about one tenth to one fi fth of the Bidan’s rate. The TBA is also willing to accept
deferred and installment payments – as and when the family can pay (see Soklat and Annex 3, Table 3.4).
More importantly, the poor are better satisfi ed with TBA’s services and feel they receive value for their money (see
Annex 3, Figures 3.8 and 3.9). The TBA is reported to be more caring and patient than the Bidan, both during labor and
after childbirth. Poor women say the TBA would continue to serve for 10 - 44 days postpartum, lovingly pampering
the new mother and the baby. She takes on all the washing and cleaning up after birth, sparing the family members
and allowing the new mother to rest and recuperate. In contrast, the Bidan is said frequently to be unavailable when
needed or even unwilling to come when called (Bajo Pulau, Paminggir, Alaskokon, Jatibaru). When she does come,
she assists only up to the delivery of the baby and the placenta.
The poor recognize that the Bidan is better equipped to handle diffi cult deliveries, but at six of the eight sites, the
Bidan is called only when the TBA is unable to deliver due to complications during labor, a practice that often leads
to fatal delays.
Professional jealousies further threaten the health of the mother and baby. The poor report that the bidan desa is
often unwilling to respond if the family has previously used the TBA’s services, and instead tells the family to go to
the Puskesmas or the public hospital. In West Java, the bidan desa has made a condition that if people want help from
the Bidan, they must call both the TBA and the Bidan to attend childbirth so that the Bidan can control the process
from the start. This however implies that the household incurs double charges.
The poor are seldom aware of possible problems during pregnancy or childbirth (see Box 5). They depend on their
chosen service provider (most often the TBA) to take action or refer the pregnant women to better health facilities.
The health care system fails to alert the poor to the danger signs of pregnancy or childbirth and what actions to
take.

17Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
The public hospitals in Java and the Puskesmas are deemed to provide the most satisfying services (see Annex
3, Figure 3.8) but high costs keep the people away. The Puskesmas and the public hospital are used only in life-
threatening emergencies.
Box 5. Pregnancy danger signs unrecognizedTasiah, 36, fell down in her sixth month of pregnancy with her third child. She had visited the Posyandu and the TBA for ANC check up, but did
not report her fall and no one asked or reviewed risks. The baby was stillborn, dry and deformed at birth, and TBA said that there was no water
in the womb. The fall may have broken the amniotic sac long before birth, without the mother realizing it.
Site Report, Paminggir, South Kalimantan
3. 3. Curative Services for Young Children (< 5 Years): Public Services are the
Preferred Choice
At all the sites the poor tend to prefer public sector services for curative services for infants and under - fi ves. They
cite: better diagnosis, faster recovery, and aff ordability. From 80 to 85 percent choose public sector providers for
children’s’ health care mainly the bidan desa and Puskesmas (see Annex 3, Figure 3.10 and Figure 3.11). At urban sites,
the Puskesmas or the Pustu is the fi rst choice, at rural sites bidan desa or Pustu. Although private doctors are perceived
to provide better services, their fees are prohibitive (Soklat, Bajo Pulau).
Only the island community of Bajo Pulau, NTB, prefers the TBA. One reason is practical: the bidan desa was “never available
in the village”. Another relates to beliefs: according to local traditions, babies delivered by the sando (TBA) are considered
to belong to her for the fi rst 44 days of life and she takes care of them free of charge.
The poor consider a number of factors in choosing a health provider for their children under 5 years. Their most
important requirements echo their concerns regarding prenatal and childbirth services. The provider should:
• Be available when needed.
• Be close to home /no or low transportation costs.
• Prove aff ordable/good value for money (true mainly of the Puskesmas, since the bidan desa or mantri do not
accept Kartu Sehat outside the Puskesmas).
• Examine sick children thoroughly. When parents take the trouble to travel to the Puskesmas, their children
should get to see a doctor rather than paramedics.
• Only give medicines that are eff ective and clarify how long treatment is necessary before results can be seen.
• Explain to parents the nature of the illness and provide advice on how to care for the child (diagnosis,
prescription, medicines, immunization, supplements etc).
The poor consider their choices, and tend to make them by the degree of severity of the problem. They know that
the quality of service from the TBA is insuffi cient, but traditional healers are still consulted for minor ailments. The
comment of one parent was typical: “Traditional healers can only pray, off er massage, and herbal remedies, but can rarely
guarantee quick recovery.”

18Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
The poor say the costs of consulting traditional healers and Pustu or Puskesmas are comparable, however they note
transportation to the Pustu and Puskesmas can signifi cantly raise the cost of seeking Pustu or Puskesmas services (see
Annex 3, Table 3.5).
In the villages, the poor with a Kartu Sehat (Health card) are attracted to the Puskesmas or Pustu, where they only pay
a “registration” fee of Rp.2,500 to Rp.3,000 to access services and free medicines. In Simokerto the Pustu “registration”
fee costs Rp.5,000 according to the poor, but Rp.3,000 according to service providers.
The previous points out a big problem in health care delivery for the poor. By law, the poor with a Kartu Sehat should
receive services and drugs at the Puskesmas for free. By charging a “registration” fee, the Puskesmas are collecting fees
illegally. By lacking information about set fees, the poor are consistently overcharged.
Services from the bidan desa at her home are highly rated, although the charge is roughly double, Rp.15,000: “There
is no need to wait in long queue and the medicines are more eff ective.”
If the child is still not cured, parents next consult the paramedic (mantri), who charges Rp.25,000 - 50,000, or a private
doctor at an average cost of Rp.40,000 - 70,000 per consultation, in addition to the cost of prescribed drugs. The
private doctor was the most satisfying option: “He gives medicines that make babies recover fast. One visit to the private
doctor is enough to the cure the baby.”
(Annex 3 Figure 3.12, shows how the top choice among service providers at each site measured up in terms of
benefi ts versus costs, in the perceptions of the poor clients).
3. 4. Quality of Health Services Being Delivered to the Poor
Observations by the Poor
Predictably, considering the fact that women are more involved than men in the care of sick infants, there is a gender
divide in satisfaction ratings of various providers (see Annex 3, Figure 3.13). Women are less satisfi ed than men with
services of the bidan (Soklat, Kertajaya, Bajo Pulau), the Pustu (Paminggir), and the Puskesmas (Soklat). While men
tended not to explain their ratings, poor women had many insights to off er about their experience.
Concerns about the bidan:
• “Why pay more at the bidan’s house, when she is the same one providing service at the Puskesmas [where it is only
Rp.3,000]?”
• “More than two to three times the cost of the Puskesmas”
• “Ibu Bidan is never available when we need her.”

19Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Reasons for women’s low satisfaction with the Pustu:
• “Workers are often not available, without prior information.”
• “Medicines given are not eff ective.”
• “We have to wait long in queues, even with a seriously ill baby.”
• “The workers just write down prescriptions and don’t explain how to give the medicines.”
• “They don’t tell the parents what is the baby’s illness and how to take care of the baby at home. They are always in a
hurry to fi nish with one patient and go to the next.”
• “Paramedics often make only cursory examinations for less than fi ve minutes. Sometimes, they don’t examine the
child at all and simply prescribe medicines after asking parents about symptoms.”
Dissatisfaction with Puskesmas:
• “At the Puskesmas those who examine the baby are not doctors, they are either the bidan or the mantri. There is no
doctor specialized for anything at the Puskesmas.”
• “For all illnesses they just give the same medicine. Often for babies they just give us a powder. I ask ‘Doc, what is the
fever my baby has?’ He says ‘Many things, mixed up’.”
• “They never explain the illness, or the medicine given to the patient. ‘If not better, come again next week.’ But if I come
again – the medicine will be the same again.”
Traditional Birth Attendants’ Observations on Quality of Care
TBAs were interviewed in rural Paminggir, Alas Kokon, Kertajaya and urban Soklat regarding their opinions of the
quality of services they provide.
The TBAs feel they are providing high quality, aff ordable ANC and childbirth assistance services. They say their poor
clients are highly satisfi ed, and see no need to improve their service. The Paraji in Kertajaya summed it up: “Helping
childbirth is our sacred human duty. People pay us whatever and whenever they can – rice, coconut, sugar, money. We
provide service for 40 days after the birth, day and night. That is why the poor are so happy with us.” The respondents’
votes for choice of ANC and childbirth assistance in this study certainly confi rm the truth of her statement.
Two of the four TBAs interviewed had received training from Puskesmas doctors in 1990-91. They had found the
training and the birthing kit given with the training to be useful.
An indication of how tight funds are: the TBAs are still using the same instruments – namely a pair of surgical scissors
to cut the cord. They wondered why training was no longer available, and suggested that the government should
provide them new birthing kits and a scale to weigh newborns.
The other two TBAs (in NTB and Madura) had refused the training and birthing kit. “I am too old to learn new things and
I don’t want to carry books and bag”, said the TBA from Madura. “My experience and traditional knowledge are enough
for my job.”

20Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
This attitude probably refl ects the uneasy relationship between the TBAs who are old and respected members of
the community, and the bidan desa, a trained government employee from outside of the community, often younger
in age. Ideally the two should work collaboratively, but in reality, the TBA is reluctant to admit that the bidan desa is
better able to deal with diffi cult childbirths; consequently, references are sometimes tragically delayed.
Still, TBAs do see a need for improvements in the public health sector. The TBA in Paminggir said: “We need health
workers, Bidans and doctors who are willing to stay in the village, or at least visit the village on a defi nite weekly schedule.”
Bidan desa (Village Midwife) on Quality of Service
Bidan desas at six sites were asked their views about the issue. They said they were doing the best they can, but
observed that there is little demand for their services among the poor. Bidan Liliek in Kertajaya explained: “Some
of the poor choose my service because it is complete. I can detect pregnancy problems. I provide TT immunization and
vitamins. My ANC service fulfi lls standards.”
Bidan desas think they are charging fees commensurate with their services. They say that the poor unrealistically
consider them too high: “The poor expect miracles if they pay anything”, said Bidan Windarti of Alas Kokon. The Bidans
said they do adjust their fees to their clients’ ability to pay.
The bidan desas have several recommendations for service improvements that the government could make:
• More poor people need the Kartu Sehat or Askes insurance card. Often, when the Bidan refers the poor to the
hospital in an emergency, the clients do not have a health card.
• Increase the number and quality of drug supplies at the Puskesmas or Pustu, which the poor can access through
use of the Kartu Sehat.
Puskesmas/Pustu Bidan and Paramedics on Quality of Service
Urban Pustus (sub-health centers) may be losing customer bases. The Bidan in Simokerto said that only the poor
came to the Pustu, but even their attendance was falling. She suggested the center’s limited hours “might clash with
their working hours…. We used to serve up to 70 patients a day at this Pustu. Now it’s only 20 to -30 per day.”
Remote areas are more problematic: The mantri (paramedic) makes weekly visits to Bajo Pulau island to seek out
patients; people don’t visit the Pustu on the mainland. The mantri says people call him on his cell phone only if
someone is seriously ill.
Poor people can rarely fi nd the bidan or the mantri in the Pustu in Paminggir. The mantri said “I cannot stay in the
village as I have many tasks in the city.” The bidan desa, his substitute, doesn’t stay in the village either, because she is
reportedly preparing for the Haj. The villagers do not consider these reasons for their absence justifi able.

21Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Puskesmas Doctors’ Views of Quality of Service
Three Puskesmas doctors were interviewed in West and East Java (Madura) and NTB regarding services available and
their quality.
The doctors agree that the Puskesmas is valued by the poor mainly as a place to get free medicines and cheap
health services. They note that, in the past, medicines were in short supply, but now the Puskesmas is authorized to
buy medicine supplies using funds leftover from annual budgets. They worry that the poor have an impression that
generic medicines, which are sold or distributed without branded packaging, are less eff ective than the branded
ones.
The doctors were divided in their opinions about the quality of service provided by health workers to the poor. At
both the West Java sites they said the health workers provide good service at the Puskesmas; interact with poor
clients at Posyandus; and are trained in “quality assurance procedures”. According to them, one reason why the
poor are not fully satisfi ed with the clinics is because they are located far from their communities, which makes
transportation expensive.
All doctors state that the Kartu Sehat health cards have not been properly targeted at the poor. Many who have and
use it are well off , while a lot of the real poor still do not have Kartu Sehat or health insurance (Askes Card). Listing and
registration for Askes began in January 2005 and is not completed at the time of this study (October 2005). With fi xed
and inadequate quotas of clients per Puskesmas, Askes will not be available to all who need it.
The physician in the peri-urban Puskesmas in NTB said most of the outreach health workers were not providing good
quality services at the community level. To improve service quality he suggested the Depkes (Ministry of Health)
should:
• Establish practical performance indicators for health workers, which can be easily understood and verifi ed by
them and their clients.
• Institute rewards and sanctions for health workers as done in the private sector. Use standards like total patients
served per day.
• Deduct from health workers’ salaries when they are absent.
• Publicize the rights of the poor to health services through mass media.
3. 5. Independent Observation Results and Conclusions The study included an independent assessment of service quality and compared this with established norms. The
following conclusions draw upon assessments by the poor, by service providers, and the independent assessment
using observations guided by checklists.

22Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Ante Natal Care
The study reveals heavy use of the TBA for ANC and childbirth. This is not only because TBAs’ fees are low and they
are available, but also because the poor perceive the quality of their services to be high.
Poor men and women have little understanding about what constitutes good ANC services, and poor pregnant
women do not see periodic antenatal care as a priority. Their TBAs are generally not familiar with the pathological events
that may develop during pregnancy. The result is poor identifi cation and management of maternal complications or
risk factors, and a failure to benefi t from protective services like TT immunization and iron supplements. This leads to
elevated risks of maternal deaths, stillbirths, and neonatal deaths (See example in Box 6).
Box 6. Repeated premature births, no ANC check upsSri Wahyuni went into labor and delivered her fi rst child at only seven months of pregnancy. She was delivered at home by the local TBA. The
baby weighed only 2 kilograms, had diffi culty breathing, and the TBA could not clear her respiratory passages. The baby lived for only two
hours. Sri Wahyuni and her husband had no money for pregnancy check ups and had never gone to the Puskesmas for ANC examination.
The following year, Sri got pregnant again, did not go for ANC check ups, suff ered greatly from nausea during pregnancy and again went into
labor in the 7th month. The second baby was born alive, weighted only 1.4 kilograms and also did not survive.
Sri and her husband have given up trying to have a child. They don’t have money for pregnancy treatments, and are afraid of the mishap
repeating itself. Sri is using contraceptive injections every three months.
Site report, Simokerto, East Java
ANC by the TBA usually consisted only of determining the position of the fetus (with corrective massage if indicated).
Several undetected fetal deaths, maternal deaths, and stillbirths were attributed to this practice and the consequent
late referral for clinical intervention. TBAs lack of formally documented professional skills. For example, their level of
training does not allow them to make reliable estimates of delivery dates. The failure to follow standard care, e.g., not
giving tetanus toxoid immunization, results in infant deaths (Box 7).
The positive trend is that nearly two-thirds of the women and men interviewed reported using one out of three
other types of public service providers, i.e. going to the Puskesmas, Pustu or the village–based midwife. The need to
get the tetanus toxoid immunization for the pregnant mother was one reason they made at least one visit to public
service providers.
The observation checklists revealed that services provided by trained village midwives are relatively good. In general,
they follow the minimum standards. However, they tended to ignore the importance of health promotion/education.
During the initial evaluation of the patient, they tended not to ask about the profi le of the client, their obstetrical and
other health histories, and their socio-economic status. This could be due to the provider and the client knowing
each other as neighbors. Alarmingly, none of these providers washed their hands before examining clients. Physical
examination by the midwife consisted only of measuring the height of the uterus and the weight of the mother.

23Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
They did not check the breasts, extremities, head and neck. Midwives usually provided tetanus toxoid immunization
and iron tablets. However, the midwives usually had to resort to purchasing these supplies themselves and charge
costs to their clients, resulting in fees higher than those charged by the TBA.
Box 7. No longer possessed by the devilBetween 1990 and 1996, 16 babies died in Rancajaya village. People believed that the devil possessed them. All had the same symptoms – convulsions,
high fever, their bodies turning stiff and bending like a bow. All were delivered by the local traditional midwife, who used a bamboo knife to cut the
umbilical cord. None of the mothers had received TT injections nor had the babies been immunized. When the babies got sick their mothers took them
to the midwife who massaged the child and prayed for its recovery.
Ibu Rusmini lost 3 children in this way, at 9 months, 1 month and 2 weeks.
Today, in 2005, people are aware of tetanus and try to get TT immunization for pregnant mothers. They however still use the services of the TBA for
childbirth. The TBA still cuts cords with a sharp piece of bamboo, which she now boils before use.
Site report, Kertajaya, West Java
During ANC examinations by the village midwife at or outside health centers, no women were informed about
those set by danger signs during pregnancy, which should prompt them to seek immediate care from trained health
service providers.
Childbirth Assistance
The study showed that most people were keen to use TBAs, as their defi nitions of quality service diff er from those set
by medical standards. The primary shortcoming of this seemingly superb service is the failure of most TBAs to meet
minimal medical standards, such as using non-sterile practices, e.g. cutting the umbilical cord with a bamboo strip
and aspirating the newborn’s nasal passages by mouth.
The case histories of maternal and fetal deaths in this study illustrate what happens when the TBA fails to respond to
the danger signs during pregnancy and labor and delays referrals (see Box 8).
Box 8. Four days too late …On Bajo Pulau island off the Sumbawa coast, Zubaedah was pregnant with her second child when she experienced abdominal pain and bleeding
in her third trimester. According to the sando (TBA) it was still too early for labor and the bleeding was “nothing much to worry about.” The wife of
the head of the dusun (Sub-village habitation), a trained midwife, thought the baby was already dead and urged the family to take Zubaedah to the
hospital, but they refused.
After Zubaedah continued to bleed for two days, the family decided to contact the bidan desa. She arrived a day later and, after examining Zubaeda,
the Bidan referred her to the hospital. After the journey to Sape by boat and rented horse carriage, Zubaedah was examined by doctors, who decided
to operate to extract the baby which had died because the placenta was blocking its passage out of the uterus. Before the operation could begin,
Zubaedah, exhausted from four days of bleeding, died.
Site Report, Bajo Pulau, NTB

24Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Curative Treatment for Children Under 5
The health center (Puskesmas) is the preferred provider. People consider it inexpensive and reliable. Nonetheless,
convenience compels most of them to bring sick children fi rst to village midwives or paramedics available in the
village. When the poor take the time and incur expenses to go to the health center, they hope that their children
will be examined by doctors or even specialists, not just paramedics and the midwife. Examinations by the latter are
considered too rushed (confi rmed during independent observations using a checklist devised by a doctor).
Assessment and classifi cation: Observation results reveal that very few sick children seeking care at the health
center were fully assessed and correctly treated by the midwife and paramedics. None of these providers washed
their hands before examining a sick child. Moreover, the quality of assessment and classifi cation of illness when
measured against the IMCI standards was low. Only one health care provider checked for the three danger signs. This
was at the one center staff ed by a doctor, and even he only checked for two of the three standard signs.
Treatment: In the absence of defi nitive diagnoses as the basis of judging the quality of treatment, the data cannot
gauge the appropriateness of treatment in this study.
Advice and counseling given: The study reveals a pervasive absence of health education services at every level of
care encountered by pregnant women, new mothers, care givers of infants and sick children. Providers did not explain
their diagnoses nor did they advise parents/guardians about ways to care for the sick children. If an explanation was
given, it was hurried and one way. Before moving on to the next patient, they rapidly stated instructions about
medication to be given but did not check whether the explanation had been understood and whether the parents
were clear how long the medication should be given.
When health service providers fail to counsel poor parents about infant nutrition and the need for immediate
treatment for diarrheal dehydration, children’s lives are put at risk ( See Boxes 9 and 10).
Box 9. How to feed my child when breast milk fails?Parhan was born a healthy 3.5 kilos, the fi fth child of his 38 years old mother, Hoiriyah. Parhan is now 20 months old, and underweight, weighing only
6 kilograms. He is often sick, and cannot stand or walk.
Hoiriyah stopped producing breast milk seven days after Parhan’s birth. From then, he was fed water only until he was one month, when he was also
given boiled rice. His parents have taken him to the bidan desa often to cure diarrhea, for which she gives them ORALIT but no nutritional advice.
Parhan’s family still does now know how to feed the baby.
Health workers at the nearest health center mentioned that this is a frequent pattern in the region, but they have not devised corrective or preventive
approaches.
Site Report, Alas Kokon

25Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Box 10. Diarrheal death of infant - close to services in a mega citySix month old Keni suff ered a bout of sudden diarrea and vomitting. Her parents took her to the nearest Puskesmas , which was understaff ed due to
a national holiday. Keni waited a long time to be examined, by which time she was severely dehydrated . She was referred to the city hospital. No one
told Keni’s parents that delay in getting Keni to the hospital could be fatal.
Keni’s father did not have a health card. Afraid that the hospital will cost much money, he delayed taking Keni there. Instead he went home to contact
his neighborhood chief (Pak RT) to get a letter certifying that he was poor, which would get him free hospital treatment. By the time he got the letter
and Keni reached the hospital she was critical. After two days on an intravenous drip, Keni died.
Site report, Simokerto, East Java
None of the poor respondents in the study knew about an offi cial Health Ministry provision (Danareksa) by which
the bidan desa can provide services to the very poor needing her help in an emergency, and claim reimbursement of
her own fees/costs from the Puskesmas. If they had been informed, many of the poor could have been encouraged
to contact the bidan desa early; many of the deaths in complicated child births might have been avoided.
4. “Clean” Water Services Used by the Poor
Poor Indonesians do not have access to public water services and buy water at 15 to 33 times the utility’s water
tariff .
4. 1. Poor Lack Reasonable Access to Potable Water
In rural areas 40 percent of the poor were using unsafe water sources (unprotected dug wells and rivers) for drinking
and cooking (see Figure 3). Another 22 to 25 percent were buying water from vendors whose methods of carting are
often unhygienic. In Bajo Pulau, for instance, a vendor transports bore well water from another island in open drums
stowed in a boat hull lined with a dirty tarpaulin. In Simokerto water is sold in old, discolored plastic jerry cans.

26Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3. Proportion of votes for choice of Water Services used
Women's view Men's view
11%
32%
5%22%
10%
8%
13%
River (no clean water supply) Unprotected dugwell
Borewell with pump (neighbor's) Vendor reselling PDAM water/borewell water
Public handpump Buy PDAM water from neighbor
Protected dugwell
14%
26%
4%25%
11%
12%
8%
In urban areas, not a single poor household was connected to utility networks. The poor buy PDAM (District Water
Company) water from neighbors who are connected or from vendors and pay 15 to 33 times the rate PDAM charges
low-income customers. Because they must go through many middlemen for their water, the poor pay six to eight
times more than the most affl uent households in Indonesian cities pay.
The poor are typically not aware that they are paying exorbitant rates because they pay small sums for small,
incremental amounts of water. Poor people often believe that they cannot aff ord to connect to piped water supply,
which could be true given the connection fees and the fact that they often live far from the network feeders. But the
poor are certainly able to aff ord water consumption at PDAM rates, since they already pay many times more than
that rate (see Box 11).
4. 2. Water Use and Health Hazards
Potable water is a precious commodity for the poor, who reserve it for cooking and drinking. Washing and bathing in
clean water is a luxury they cannot aff ord. At all sites, poor people bathe and wash clothes in rivers, at unprotected
dug wells or even in seawater.
This has important health implications. The strong cultural preference for defecating in running water has led to
an ingrained habit of defecating in natural water bodies. Several participatory evaluations of water and sanitation
projects8 and the Baseline Survey for the WSLIC project conducted by the University of Indonesia in 2003 found
that: “Almost all people wash their clothes, take a bath and defecate at the river even though they have a well. Defecation
in the river is perceived as ‘clean’, as it does not create a bad smell, like defecating in a poorly ventilated toilet.” People also
often throw garbage in the river and use the same river to wash their livestock, clothes and motorcycles—as well
as themselves.
8 WSP-EAP , 1997, 1999, 2000

27Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Those who do not wash and bathe in rivers and streams use water from unprotected dug wells without boiling.
In the Surabaya slum, water is “reddish, brackish and smells bad”. In Soklat the wells had no cement platforms and
were surrounded by muddy, stagnant pools. In Jatibaru, the walls of the dug well are made of old metal drums
used for storing industrial chemicals. The wells are located next to stables and have no cement platforms to prevent
environmental pollutants from seeping in. Solid waste garbage has blocked existing drains so that wastewater
stagnates around wells.
In people’s minds, well water is “clean”, while river water is not. Thus, those who are able use well water to wash and
bathe consider themselves fortunate, regardless of the condition of the well. Levels of satisfaction with well water
tend to be high unless the water is visibly colored, has a bad odor or is brackish. (See Annex 3, Figures 3.14 and
3.15).
Box 11. The poor pay 30 times PDAM tariff for water – but don’t realize it
Perception:“Pak Ketua RT (the neighborhood head) says we can’t aff ord a house connection to the PDAM’s piped network because the connection cost Rp. 750,000
($75) is too high for us. What is more, now that PDAM’s tariff s have increased from Rp. 300 to Rp. 700 per cubic meter, the monthly costs of water
consumption will also be unaff ordable for us. We spend only Rp. 300 everyday to buy 30 liters for drinking and cooking. We buy it from our wealthier
neighbors in buckets, paying Rp.100 for 10 liters”
Kalimantan Women’s Focus Group, Antasari, South Kalimantan
“We can never hope to get a household water connection from the PDAM. It will cost at least Rp.3 to 5 million, because the pipeline will have to cross a
railway line, a highway and a market, to reach Simokerto where we live. Who can aff ord it? Moreover, we are not owners of this land we live on so we
can’t apply for water connection. This land belongs to the State Railway company (Perusahaan Jalan Kereta Api)”
Men’s Focus Group, Simokerto, Surabaya
Reality:
The poor in Antasari are paying their neighbors Rp. 100 for 10 liters of PDAM water. This implies a rate of Rp.10,000/cubic meter of water—more
than 13 times the PDAM tariff s of Rp. 700/cubic meters. The poor in Simokerto buy re-sold PDAM water from a vendor at Rp.1,400 per day for 50
liters of water delivered to homes (or Rp.700 per day for 50 liters if collected from the vendor’s outlet). This implies a rate of Rp.28,000 per cubic
meter of water delivered at home. The current PDAM tariff for household connection in Surabaya is only Rp. 850 per cubic meter
4. 3. The Poorest Pay the Highest Price for Water
Water is costly. The poorest households—which comprised between 51-73 percent of community households at
diff erent sites—spend from a low Rp.5,000 (Jatibaru) up to a high Rp.60,000 (Bajo Pulau, Antasari, Simokerto) a
month for water (see Table 3). This means that the poor can spend as much as 15 percent of their income for
drinking and cooking water (Bajo Pulau).
The costliest water is bought from vendors. The cheapest way for the poor to obtain clean water was to collect it
from the mosque or a well off neighbor. In rural areas, this is usually bore well water; the poor pay about Rp.5,000

28Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
a month to cover electricity costs of pumping it from wells. In the city, poor people collect PDAM water from
neighbors’ homes paying them about Rp.30,000 a month. In Soklat and Kertajaya, the poor spend about 30 hours a
month collecting dug well water from neighbors’ wells or public wells. Households in Alas Kokon spend 150 to 200
person hours a month hauling water for washing, cleaning and watering animals. Women in that village say it takes
them “two to three trips to the river to bring back water from the river, walking 1.5 kilometers each time”. Along with
washing and cleaning, “that adds up to more than three hours everyday”.
Table 3. Costs of clean water services and water use by poor household at 8 study sites
Rural Sites
Paminggir/S.Kalimantan
(River. No access to clean
water)
Bajopulau/NTB
(Bore well water from another
island, brought by boat by
vendor)
Alas Kokon/Madura
(protected public dug well)
Kertajaya/W.Java
(public handpump)
• Drink river water, after
sedimentation and boiling
• Bathe & wash in the river
• Defecate in the same river
• Rp.30,000 + 30 person hours/
month for 35 liters/day
• Buy water only for cooking &
drinking (Rp.30,000/month)
• Bathe & wash in the sea
• Defecate on the beach
• Quota 20 liters/day/
household,only for cooking &
drinking, time cost 8-10 hrs.
per person/house/month
• No payment
• Collect river water for other
purposes, using 210 person
hours/house/month
• Use simple pit latrines at/
near home
• 30 person hours per month &
Rp.5,000 for buying cooking
& drinking water from
mosque
• Bathe + wash in river
• Most also defecate in the
same river
Urban sites
Antasari/S.Kalimantan
(buy PDAM water from
neighbor)
Jatibaru/NTB
(buy water from neighbor’s
bore well with pump)
Simokerto/E.Java
(buy PDAM water from
vendor)
Soklat/W.Java
(neighbor’s dug well
– unprotected)
• Rp.30,000/month for 100
liters/day at Rp.100/10 liters,
only for cooking & drinking
(>13 times the PDAM rate in
the small town*)
• Bathe + wash in river
• Use unimproved pit latrines
at home
• Large % defecate in the same
river
• Rp.5,000/month for sharing
electricity cost. Collect about
120 liters bore well water/day
for cooking & drinking
• Bathe + wash at neighbor’s
unprotected well (no cost)
• Most defecate in the river
• Rp.42,000/month for 50
liters water delivered home
everyday, for drinking and
cooking (>30 times the
PDAM rate)
• Bathe + wash at public dug
well
• Defecate in pit latrines at
home/by railway line/ into
river/public toilets
• 30 person hrs./month per
household to collect water
for cooking and drinking. Boil
water for drinking
• Bathe + wash at well
• Half use sanitary latrines
shared with several
households
• Other half defecates in river
or pond
* Lowest PDAM tariff for house connections in Antasari = Rp. 700/cubic meter water.
Lowest PDAM tariff for house connections in Surabaya = Rp. 850/cubic meter of water

29Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
4. 4. Observation Results: “Clean” Water Services
It was not within the purview of this study to carry out bacteriological tests of water samples at the sites. Observations
included: a) checking for the nature of the water sources used, viz. improved or unimproved sources according to
global MDG monitoring defi nitions9 , b) condition of water sources, and c) possibilities for contamination.
Illustration 5: Urban slum poor buy PDAM water resold several times—each
time the price increases. Bulk water seller fi lling small-scale provider’s jerry cans
from PDAM water stored in drum.
By these criteria, the poor at half the sites had
no access to clean water. They were drinking
and cooking with water from unimproved
sources open to various forms of organic and
chemical pollution. At the other sites, water
from improved sources was available in very
limited quantities, due either to the capacity
of the source, or the price of water.
The poor pay the highest prices,but get
the lowest quality. Because of the high rates
of the water vendors, the poor bought water
at 15 to 33 times the rate consumers pay to
utility companies. Because of the costs, none
of the poor can wash and bathe in clean water. Rivers, lakes, and the sea are used for washing and bathing; clean
water is used for a scanty fi nal rinse.
Illustration 6: Unprotected dug well, lined
with an industrial drum, in urban Jatibaru,
NTB. Water from this well is used for all pur-
poses.
.
Water vendors are unregulated and monopolistic. They collect water from
supposedly clean sources such as utility (PDAM) connections or bore
wells. However, water passes from large and medium scale water re-sellers
to small scale vendors, who use a variety of unsanitary means (used
chemical and oil storage drums, rubber hoses, funnels, etc.) to transport
water. There are no regulations requiring regular cleaning and periodic
replacement of these containers or equipments.
Contamination levels of the water fi nally reaching poor consumers
through vendors are likely to be much higher than acceptable norms, but
would require a bacteriological examination to confi rm.
9 The WHO-UNICEF Joint Monitoring Program classifi es improved water sources as protected dug wells, protected springs, tube well/borehole; rain-
water collection; public tap/standpipe; piped water into dwelling/yard/plot; and bottled water only when there is a secondary source that is also
improved.

30Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
The poor consider dug well water to be clean. However, the physical conditions of dug wells and the surrounding
environments observed indicated that the water in all save one was and remains highly contaminated. Only Alas
Kokon had a protected dug well, but its capacity was limited. Poor users were allocated a quota of only 20 liters per
day per household, to be collected and stored once a week. This was used only for cooking and drinking.
Vendors have a vested interest in perpetuating their highly profi table, monopolistic hold on poor clients and have
been known to subvert other water supply options. Box 12 presents an example.
Box 12. Held to ransom by monopolistic water serviceBajo Pulau island has only one source of clean water – a private bore well three kilometers from the seaside hamlet of the poor. Because of the hilly ter-
rain, the poor cannot access that source. They survive by buying water for cooking and drinking from the vendor who transports bore well water from
another island. He sells the water at Rp.1,000 per 35-liter jerry can ( Rp.28,600 per cubic meter). The better off can buy three to fi ve jerry cans a day. The
poor buy one jerry can a day, aff ording 35 liters for a family of six to eight people. They bathe and wash in the sea, using the precious jerry can water
only for a scanty fi nal rinse.
The water is transported un-hygienically in the tarpaulin-lined hull of a boat and open drums. It is contaminated with dust and traces of oil. The water
vendor’s fi rst priority is to sell water to boats anchored at the port, and serve the poor community only with leftovers. Women often wait up to two hours
on the beach for the vendor to come. They can only helplessly curse the vendor if he fails to show up or runs out of water. They suspect that the vendor
intentionally damaged a government-built undersea water pipeline. Because the Public Works Department planned and built the pipeline without
involving the community, no local organization was established to manage and maintain it and it fell into disrepair.
Site Report, Bajo Pulau, NTB
4. 5. Quality of Services: Views of the Poor
Access to clean water is a prime determinant of quality of life. Having to depend on a water vendor’s whims frustrates
and angers poor women in Bajo Pulau: “We wait on the beach for the vendor’s boat. Sometimes we wait from the morning
and he comes as late as 2 in the afternoon. If his supply is fi nished serving the big boats in the harbor, we don’t get any. Just
wait for the day when he might need our help—then we’ll fi x him!”
Illustration 7: Water transported in boat’s hull to Bajo Pulau, a
rural island off Sumbawa coast, NTB
Urban poor who buy utility-supplied water from
vendors or neighbors (albeit at a high premium over
the utility rates) are highly satisfi ed with water quality
and price. According to the poor in Simokerto and
Antasari: “The PDAM water is clean, has no smell or color,
can be used without boiling, does not need to be pulled up
(from wells), and is aff ordable.”
This comment was surprising, considering the poor
were paying many times more than the PDAM rate per
cubic meter of water. It completely debunks the myth often stated by PDAMs that the poor are not profi table
customers because “they cannot pay cost-covering tariff rates.”

31Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
In fact, many of the local poor work as water vendors for the cartels that serve designated slums. These cartels decide
the selling price for water and do not allow competition that might bring down prices. There are designated fi lling
stations in each Kelurahan supplied with a PDAM connection; consumers may buy their water at the fi lling stations
or have the vendor deliver it to their homes at twice the cost.
Illustration 8: Water vendor’s boat, Bajo Pulau, NTB
Because of the high prices, the poor only buy
limited quantities of clean water—just enough
for cooking and drinking. They accept as a fact of
life having to use unsafe water from polluted
wells and surface water sources for all other
purposes. Consequently, they had no complaints
about unsafe river water when it was available
and free.
Nonetheless, others recognize the impacts this
“free” water has on people’s health. The Mantri
from the health outpost in Paminggir comments:
“This village needs a clean water supply more than
any other health service. Each year there are numerous cases of diarrhea and skin diseases because the people use the river
for drinking and cooking as well as for all bathing, washing and defecation.”
5. Sanitation Facilities Used by the Poor
Water availability, water use practices, and sanitation practices are intrinsically linked, as amply illustrated in the
previous section. Sanitation practices refl ect what people consider clean, convenient and comfortable—and what
is available.
Figure 4 shows that, except for a tiny minority in Soklat (West Java), poor men and women at all eight sites have no
access to any kind of “improved sanitation facilities.”10
10 “Improved sanitation facilities” are defi ned by the WHO-UNICEF Joint Monitoring Program (used for global monitoring of MDG targets) as: venti-
lated improved pit latrines, pour fl ush latrines, simple pit latrines with cover, or connections to septic or sewer systems. This defi nition excludes bucket
latrines, open pit latrines, public or shared latrines, and latrines discharging directly into water bodies.

32Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 4. Proportion of votes for choice of sanitation facility used
Women's view Men's view
44%
8%9%
10%
25%
4%
River (open defecation) Field (open defecation)
Beach (open defecation) Unimproved pit away from home
Unimproved pit household latrine Shared household latrine
41%
17%
16%
11%
14%
The coastal Bajo Pulau community defecates on the beach at night or before down, so that the tide can wash away
the feces. At six other sites people prefer to defecate in the river, while washing, bathing and brushing their teeth
in the same river water (see Table 3). Defecation in the water leaves no visible excreta or obvious smell, and is thus
considered “clean” and in fact a “healthier option” than the smelly, simple pit latrines and public toilets available to
them—this despite the decades of eff orts by health authorities to push the health benefi ts of latrines.
Women (61 percent) and men (74 percent) said that they defecated in the open in rivers and small streams, beaches,
ponds, rice paddies and bushes. The use of natural water bodies is free, whereas there are long lines and a Rp.200
charge at public latrines in the urban Java slum. Unsafe open pit household latrines are used by another 25 to 35
percent. These are no more than holes dug into the yard (Alas Kokon, Jatibaru), directly beneath the home on stilts
in swamp areas (in Antasari), or by the railway track embankment in the urban slum (Simokerto).
There are gender diff erences in sanitation behaviors (see Annex 3, Figures 3.16 and 3.17). Privacy was reported as the
most important rationale for sanitation behavior, in conjunction with convenience and “cleanliness” (natural running
water). Regardless of the quality of the latrine facility, a household facility is preferred over having to go out for
defecation – particularly where homes are not close to the river or the sea (Alas Kokon, Antasari, Soklat, Simokerto).
Women prefer the household facility more than men do.
Another major obstacle to poor people gaining access to improved sanitation is the widespread misconception
about sanitary latrines being an expensive luxury. The poor are under the impression that latrines cost a lot of money

33Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
(Rp.750,000 – 2,000,000, i.e. $75 – 200), and are therefore out of reach of poor households. In a country where half the
people live on less than $2 a day, such perceptions are rational. The misconception is born of poor people having
seen only expensive household toilets built by upper class households. Public Works departments have not helped,
by promoting only standardized engineering designs of high-cost options certifi ed as “hygienic”.
5. 1. Observation Results: Sanitation Services
The poor do not have basic sanitation services. This study found barriers to improving public sanitation to include:
1) public perceptions of open defecation into water bodies being a desirable practice; 2) widespread ignorance of
low-cost sanitation alternatives and misconceptions of sanitation being an expensive luxury; 3) lack of mechanisms
to eff ectively promote better sanitation and hygiene practices and low-cost sanitation improvement options.
In both rural and urban areas the poor use any natural water body available as the preferred sites for excreta disposal;
some do so even when they have latrines built at home through project- provided funds or subsidies, because of the
unpleasant and typically unsanitary conditions of the latrines. The result is a grossly under-recognized environmental
disaster that aff ects the living environment for the total population in Indonesia, both the poor and the non-poor
alike.
People use latrines when they are clean and convenient. At a Java peri-urban site, a small group of people had access
to sanitary household latrines built by a project. These latrines were reasonably well maintained and shared by four to
fi ve households. People were less inclined to use public toilets provided by an NGO, which were grossly inadequate
in number, poorly maintained despite a Rp.200 fee per use, and plagued with long queues in the morning.
Apart from these two instances, various forms of unimproved household toilets built by the poor were encountered
at half the sites. In the rural areas these were the bamboo poles or wooden slats over ponds or rivers, often temporarily
enclosed with fabric or makeshift wooden structures, or simply holes dug in the backyard.
Illustration 9: In Paminggir,
rural South Kalimantan, the
poor live on the river and use
it for everything: cooking,
drinking, washing, bathing and
defecating (right). Enclosure in
the background is a latrine.
In the urban areas these holes were
often cemented and incorporated
within dwelling units, but they
discharged raw feces directly into
urban drains or rivers. The poorest in
squatter and slum settlements do not
have even these holes. They seek out
public land with any semblance of
privacy for open defecation, or
defecate into urban rivers just as in villages.

34Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Illustration 10: Open pit household latrine in a backyard is
accessible to domestic animals, further expanding the chances
of the spread of diseases. Alas Kokon, Madura
Rural primary schools and half the urban primary schools
lacked functional sanitation facilities for students. The
urban and the secondary schools had functioning toilets
for students and teachers, but the ratios of students to
toilets were upwards of 100 to 1 at most sites, which
would preclude their use by all students.
The government has not dispelled the myth that sanitation
is expensive. The reality is that in most parts of inhabited
Indonesia today, it is possible to build low-cost sanitary
toilets using locally available materials and labor, at costs
ranging from Rp.100,000 – 300,000 (US$10 - $30)—within
the reach of the majority of the poor. However, there are
no programs to raise public awareness of the real costs
and consequences of poor sanitation, and to widely promote low-cost options for sanitation improvements.
5. 2. Quality of Services: Various Views
Illustration 11: Household toilets exist in urban poor
neighborhoods they typically discharge directly into rivers or
drains behind homes which fl ow into urban rivers. Simokerto.
The quality of sanitation services for the poor is abysmal.
There is no visible eff ort on the part of local or national
governments to provide the poor with solutions for this
basic need.
In rural areas, natural bodies of water become ad-hoc
toilets, imperiling the health of the community. The Pustu
paramedic in Paminggir said:
“The biggest health problem here is the river, which is the
principal life support for the villagers…. It’s used for all
purposes by the villagers, including bathing, washing, cooking
and drinking, as well as excreta and wastewater disposal.
Diarrhea and skin diseases occur frequently; annual fl oods turn them into epidemics. We can treat diseases with drugs, but
we can’t prevent them.”
The lack of basic sanitary services impacts other services such as education. In rural areas, teachers often refuse to
stay in the villages—and consequently often don’t show up to teach. The volunteering local teacher at the Paminggir
primary school explained that the trained teacher is seldom in the village (even though living quarters are provided)
because there are no sanitation facilities. The offi cial teacher goes back to the city “to wash clothes” and is usually late
returning to his duties in the village. Local teachers at Bajo Pulau echoed these views.

35Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Illustration 12: Natural bodies of water are the preferred places
to defecate, as illustrated by this toilet over a pond in peri-urban
Soklat, West Java
There seem to be no norms governing basic water and
sanitation facilities in the construction of school
buildings. Primary teachers in rural Kertajaya said their
school had been built without any water or sanitation
facilities. They later received one toilet from the
Kecamatan Development Program (KDP)—one toilet for
the entire school, which proved inadequate and soon
broke down.
Similarly, there seem to be no funds set aside in local
budgets for routine and regular maintenance. In urban
Soklat, after the students’ toilets broke, the teachers
allocated one of the two teachers’ toilets for the use of
female students. Repairs had to wait for the next annual
government allocation, many months away.
Public pay toilets are a fi nancial burden for the poor. In the Simokerto slum settlement, the money collector at the
public toilet says less than 30 people a day use the toilet, although the neighborhood (RW) has 300 households, many
of which are within 100 meters of the toilet. He believes the Rp. 200 charged per use is too much for the poor to
aff ord.
6. Poor Have Little Client Power—But They Want It
The poor are disempowered. At all eight sites, it was clear that the men and women had little concept of their own
power or their rights as clients. The top-down approaches of the New Order era and feudal societies have left a
heritage of unequal relationships which extends to the relationships between the poor and their service providers.

36Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Box 13. “They give us no choice….”About 15 years back, all married women in Rancajaya village were forced to accept the spiral (intra-uterine contraceptive device). Women were round-
ed up by government workers and taken by pick-up trucks to camps for insertion of the spiral. Not a single married woman could escape. Women who
hid were chased until found. Those who refused or ran away had their houses marked with red strips for follow up.
Many women who received the spiral suff ered for months from pain and bleeding. Husbands were scared for the health of their wives and tried many
things. Some had their wives spend hours sitting partly submerged in the river or water tanks, hoping that the spiral would fl oat out. Nothing worked.
All those women and their daughters—now married with children of their own—are so frightened of contraceptives that they avoid using any.
“Health workers never give us information about diff erent types of contraceptives and what are the benefi ts and disadvantages of each type. Don’t be
surprised if in the women’s group discussions you fi nd married women who have never seen a condom!”
As related to researchers by the men’s group in Kertajaya, West Java
6. 1. Lack of Information-“We Don’t Know”
Illustration 13: Lost opportunities: In the ANC examination room, Soklat, West
Java, posters show diagrams of labor and reproduction system. There is no
information for women about danger signs in pregnancy, or protective services
available.
Typically, the poor have no direct access to
information of programs directed at them and
so have little or no idea of their rights. The
researchers did not fi nd any public material
publicizing what services are available (such
as Kartu Sehat, Askes and scholarships) or
describing how those services could be
obtained. Service outlets—Pustu, Puskesmas,
schools, and village government offi ces
(Kantor desa/Kelurahan)—simply did not have
supporting literature. Poor women asked: “Why
is there no information about these measures on
radio and TV, in posters in Puskesmas?”
In their own eyes and in the eyes of service
providers, the poor are passive recipients of whatever services and information the service providers or community
leaders choose to make available. They must depend upon community leaders (Ketua RT or Kepala Desa) to list them
as “poor”, and then depend on Puskesmas workers to dole out the quota of Kartu Sehat/Askes cards, or upon school
principals to award scholarships. Typically, poor are also at the mercy of water distributors—when they will deliver
and how much they will charge.
Confusion Regarding Pro-poor Services Available
The poor do not know accurately what fees should be charged for pro-poor services—a very central issue in
the lives of the poor. Because of the lack of information, none of the poor in the study knew about an offi cial Health
Ministry provision (Danareksa) by which the bidan desa is reimbursed for providing emergency services to the very
poor. Residents at two sites did not know about health cards. The poor said it was never clear which medicines are
free for Kartu Sehat users (Simokarto, Soklat, Jatibaru) and which not.

37Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
At other sites the poor were aware of services such as cheap rice (Raskin) and health card. Information about school
fees being waived was well known at six sites, although they understood the school operation funds (BOS) program
to start as of September 2005 when in fact the date was July 2005. At Jatibaru (NTB) and Soklat (West Java), the poor
said they had found out late, from television. The primary school did not inform parents. In fact, in Soklat, parents
paid tuition fees for September 2005 before they learned that fees had been waived. The school has not returned
the money.
Frequently, the people were confused about what the pro-poor services provide and to whom. For instance,
at diff erent study sites quotas of cheap rice available to poor households per month ranged from 3 to 20 kilograms.
Many had questions about who was eligible for Kartu Sehat. They complained that few poor families received health
cards, while many non-poor did because they were related or close to the village chief (Soklat, Jatibaru, Antasari,
Paminggir).
The poor repeatedly said they didn’t know the duties of public sector service providers. This was particularly
true in reference to health workers manning the Puskesmas, the Pustu or outreach services.
It is not clear to the poor how decisions are made about services or who makes them. In Soklat, the poor
approached the Puskesmas to get Kartu Sehat, but most failed: “Everyone passes us on to someone else—no one gives
clear answers.” In Jatibaru, the poor asked the school about their children’s eligibility for scholarships. They were told
that recipients were “decided from above”.
6. 2. “Who Will Hear Us?”
What To Do About Bad Service?
Poor men and women are aware that they are often not served well, but don’t know what to do. Complaining to
local political leaders or the mass media is alien to most of them; they cannot imagine reaching such people nor
do they believe that these elites will pay attention. Residual memories of the harsh tactics of the Soeharto regime
stifl e most dissent. No one at any of the eight sites has ever seen or heard of a negligent service provider being
sanctioned in any way, regardless of the number of complaints. “We can’t even ask why we don’t get proper service, let
alone sanctioning anyone. We have no authority or power, even to ask questions,” commented women in Soklat, West
Java. The result is resignation: “The service provider has the authority to decide what services we can get,” was a typical
response in Jatibaru. Complaints might bring retribution. “If we complain, they will exclude us from distribution of things
like Kartu Sehat,” comments another from Simokerto.

38Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Fears About Complaining About Poor Services Abound
The poor are at the bottom of the community hierarchy. On densely populated Java where land is a highly prized
asset, the poor often do not own the land they live on, which creates a feeling of insecurity and fear of speaking
up. In Jati Baru, people claimed it was embarrassing (tidak enak) to complain about the Bidan and Pustu workers,
because they had family and social connections in the community; in Madura, the poor hesitated to go to the village
leader because “that will create more problems for us later”.
Some villagers did make attempts: In Kertajaya, West Java, the poor asked the village chief to require the bidan
desa to live in the Polindes (birthing clinic) built by the community. In South Kalimantan the villagers lodged formal
complaints with the local government (Dinas Pendidikan) about a primary school teacher who failed to show up for
classes, despite being given living quarters (Paminggir). None of these eff orts yielded any results. “The Bidan lives in
the town (Sape)”, noted women in Bajo Pulau. “If we call her she always has many excuses why she can’t come, including
even low tide! She won’t even get off the boat lest her feet get wet! But we are afraid to complain – she is related to the
Village Secretary, and he is powerful.”
The poor are not afraid of complaining about sanitation services—simply because there are no providers. The
poor do complaint about monopolistic water servers (SSIPs) in Bajo Pulau, but the complaints get them nowhere.
Urban SSIPs satisfy their customers—the exploitative price of the water is hidden by the fact that it is paid in daily
increments.
Community Elites Give Directions
Generally, the poor take directions from the people in charge—teachers, health workers, village leaders—regarding
pro-poor services (or the lack of them): “We keep quiet and do what they tell us to do”, said one resident of Soklat. “At
most we ask our Ketua RT (neighborhood head) if he can explain.”
Box 14. “Because I am poor, and therefore also stupid”Pak Yusuf has 13 children and earns a meager living working as a carpenter. Only one of his children has entered junior high; two others did not con-
tinue beyond primary school because of school fees and because they could not obtain a pass certifi cate from the primary school.
“I could not pay Rp.55,000 required for each certifi cate”, Pak Yusuf said, adding that he has pleaded with the school to reduce the rate, to no avail.
To get their child admitted to junior high school, Pak Yusuf and his wife off ered Rp.20,000 and their only valuable asset—a table fan—as registration
fee. He still wonders how to pay another Rp.50,000 for uniform and books. He never tried to obtain a letter from the local government certifying his
poverty, which could lead to fee waivers. He said: “I am only a poor man, and therefore also stupid. No one told me about this. I don’t know how to get
it although I do want to obtain this letter. My experience so far has always been that no one really wants to help me.”
Site report, Soklat, West Java
The Ketua RT is an important bridge between the government processes and structures and the people. In contrast,
the village chief, his assistants and the village governance apparatus are often too distant to be relevant to the lives
of the poor. The people of Bajo Pulau were particularly vehement about village offi cials: “The Kepala Desa doesn’t care

39Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
for us. He never comes to our hamlet, even when someone dies. Just throw him into the sea!”, “That Village Secretary just
eats village funds!”, “The Badan Perwakilan Desa (BPD, the village council) is just a formality—has nothing to do with us.”
6. 3. Poor Treatment by Pro-Poor Service Providers and Offi cials
“We feel like stepchildren in the family. Possibly because we don’t own the land we are living on and not paying land taxes
to the village government. We have no right to expect any services from them ….”
Poor women’s group, Kertajaya
Many health card users said they had to wait at the Puskesmas until paying customers had been served; at the Pustu
they were sometimes simply ignored. Women in Kertajaya and Jatibaru said that the bidan desa would only assist
them during childbirth if they had gone to her for ANC services previously.
When they are examined by public health service providers, it is cursory at best; sometimes drugs are given without
examination. The poor said that they get the public service provider’s attention only when they pay fees at a private
facility.
Residents of Bajo Pulau island have thrown away their Kartu Sehat, since it is too far and too costly to visit the
Puskesmas on the mainland.
Box 15. Kartu Sehat users need patience and forbearance“The doctor who works at the public hospital in Jereng also practices privately outside the hospital. My wife had been examined by him at his private
clinic during her pregnancy. At the time of childbirth, because I had no money, I took my pregnant wife to the public hospital in Jereng, which is the
nearest hospital that accepts my Kartu Sehat. When we reached the hospital I was asked to fi ll out forms with information about my wife. Soon after,
the doctor who had examined my wife before, arrived and started scolding me because I had not taken her to the private hospital which he had earlier
recommended. I said I cannot aff ord the expenses of the private hospital – but the doctor kept shouting at me and my wife…..”
Bapak Sobirin, Kampung Rancajaya, West Java
6. 4. No Voice in Community Decisions and Service Provision
According to both women and men, decisions regarding the use of public funds are made solely by government
functionaries together with the formal community leader.
“There has never been a public meeting or forum to inform us about plans for local development or government fund
allocations to provide services to our community. If there is a community meeting, the Kelurahan workers do not publicize
it.”
Poor Men’s Group, Simokerto

40Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Sometimes, this high-handed approach on the part of offi cials has forced the poor to act on their own and provide
supposedly public services with their own meager savings. “Even though the Ketua RT and community representatives
are members of the Badan Perwakilan Desa, we never get to know anything about fund allocation for basic services,”
noted the men from Kertajaya. “We have sent formal requests to the village government many times to give us an offi cial
electricity connection. Now we are spending our own money on cables to draw power from another kampong.”
.
6. 5. Problems with the Participatory Process-“We are Stepchildren”
While poor men feel they have no voice in community decisions in general, and in basic service provision in particular,
poor women are even more on the periphery: “Women in the Kelurahan, if involved in any activity, are only from the rich
households”, said women in the Antasari Focus Group.
The women from Soklat were even more outspoken, “They never call us for meetings and discussions because they think
we are stupid, because we don’t have money, because our eff orts/ initiatives are small scale, because we are considered
‘small people’ (poor).”
Despite the fact that Indonesia is one of the world’s largest democracies, these poor citizens do not feel as if they
are equal.
This state of aff airs distorts the quality of participatory processes and equity in outcomes of development projects
aimed at poverty reduction and empowerment of the poor. The following unsolicited comments, made during
focus groups about community-driven development projects (considered largely successful in Indonesia) illustrate
this point:
“We only came to know about the road-building work after laborers from outside the village were hired to build it, although
the road is meant for our community’s use, and the program was for providing wage income to our community.”
Poor men’s group, Antasari

41Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Illustration 14: The poor in places like Jatibaru, West Nusa Tenggara (left), and Paminggir, Kalimantan (below) claim that local elites will only
listen to their views through outside facilitators.
“The hand pump was installed entirely by project functionaries, starting from selecting the contractor and laborers until
construction. The result is a hand pump near the mosque, where the kepala desa wanted to put it. The water is salty. No one
uses it. The pump has broken down within one year of construction.”
Poor women’s group, Kertajaya
“We have never received any micro-credit services from the poverty reduction project. Those who did had some business
initiative of their own, and are the middle class people. The Badan Kerja Masyarakat (community management team for
the project) that decides the recipients is made up of people who are not poor. The poor people only get loan and saving
facilities from the private mobile banks that visit the community often.”
Poor women’s group, Soklat
Help Us Participate
Poor men and women did articulate that they can gain a voice in community life if outsiders support their eff orts.
The people of Alas Kokon explained their vision: Essentially, they believe they need facilitators from outside the
community who can organize meetings or create a forum for open discussion. These external facilitators must care
about the poor and they should have the skills to identify who the poor are in the community.
Residents of Alas Kokon were emphatic about the need for outside intervention: “Through government institutions/
workers, this kind of process facilitation is impossible. … Until now, we have not seen any government institutions that care
about the quality of services for the poor or about the aspirations of the poor.”

42Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
7. Recommendations for Policy and Strategy
Following are a series of recommendations for general and specifi c policy actions and strategies to improve service
delivery to the poor. They are drawn from the specifi c observations, complaints and assessments made by the poor
at all eight sites. Based on personal, real-life experiences, these suggestions off er unique insights into the ways poor
women and men poor believe services could be improved and form a complementary list of actions to be used
along with fi ndings from the quantitative analysis in the main report, Making Services Work for the Poor in Indonesia.
7. 1. For Basic Services in General
1. Establish procedures that allow the poor to seek and obtain pro-poor services on their own without having to
depend on community leaders or service providers for procedures to access.
2. Eliminate poor people’s dependency on service providers and community leaders for information that aff ects
their lives and health, e.g. basic services available, their standards and costs, special provisions for the poor,
where and how to get.
3. The paradigm of the poor passively and helplessly waiting to get listed/ certifi ed at the discretion of their formal
leaders needs to be reversed. Certifi cations and classifi cations of who is poor and who is not should become
more participatory and be done through collective assessment methods that make it fully transparent and allow
local-specifi c poverty characteristics to be identifi ed and taken into account.
4. Create coordinated information programs to alert the poor to the services that are available to them and to
make them aware of the benefi ts of these programs. There should also be information programs alerting the
poor to danger signs—common situations that can and should be addressed immediately by them to avoid
harm.
5. Communicate directly with the poor about all pro-poor services through mass and institutional media. Publicize
pro-poor services and how to access them, e.g. through radio, regional newspapers, visual publicity materials
at puskesmas, pustus, public hospitals, schools, mosques, banjars, village/kelurahan offi ces and public transport,
information handouts distributed to households through neighborhood heads (Ketua RT), men’s and women’s
groups (arisan, PKK) and the like. Set up information kiosks in districts and kecamatans where the poor can go
to fi nd out about all pro-poor services available in the region from all public and private sector sources. Publicize
the presence of such kiosks.
6. Empower the poor with information on service standards that they should expect from each type of provider,
and what action to take when those standards are not met. Publicize these prominently at all relevant public
service outlets and make their permanent display mandatory.

43Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
7. Establish mechanisms that make it easy and risk free for consumers to report on the performance of basic service
providers in comparison to the expected norms. The Kecamatan Development Program (KDP) in Indonesia has
fi elded several innovative methods of community reporting on corruption, which could be adapted for this
purpose. Develop ways for consumers to assess and report on performance of providers that do not require
consumer identities to be revealed, since social familiarity with the provider is often the constraint to reporting
on poor performance. Find ways to use the results of these consumer reports and link them directly to providers’
salaries and perks to create incentive for best practices in service.
8. Publicize these mechanisms and service standards widely through mass media and at all points of service.
9. Prominently publicize consequences of people’s use of such reporting mechanisms. Poor people will not come
forward to report poor service performance without concrete proof that it is worth their while to do so and that
it is risk free. Previous experiences have convinced them that seeking accountability is an exercise in futility.
7. 2. For Health Services
All of the above apply to Health Services. The following are additional specifi c recommendations:
1. Improve the transparency and fairness of procedures to identify the benefi ciaries of health cards or health
insurance (Kartu Sehat and Askes) using methods suggested in point 3 above.
2. Providing information can save lives. Galvanize the health service provision system to focus more on providing
life-saving information to empower the poor. Such information includes:
• Making benefi ts clear; sometimes the poor fail to use services because they are afraid of the expenses.
• Pregnancy danger signs that require immediate referral to a health center. The poor should not have to depend
on TBAs or other advisers to tell them when to take action.
• Comparison of ANC services at the TBA and the Puskesmas/Pustu in terms of life-protecting measures, such as
TT immunization, and better family-level preparation for potentially risky childbirths, e.g. counseling families to
be fi nancially and logistically prepared for emergency transportation to a health facility during labor when the
pregnancy has been identifi ed as a high-risk one.
• How to feed and care for infants when breastfeeding fails or during illness. (Information should go beyond
simple dispensing of drugs and oral rehydration salts).
3. Publicize measures available for the poor to make trained bidan desa’s services more aff ordable, e.g. Danareksa,
whereby the Puskesmas can reimburse the Bidan for her services to the poor. None of the poor men and women
in this study had heard about this.

44Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
7. 3. For Education Services
To improve the quality of primary education in villages, a variety of issues need to be addressed: causes underlying
teacher absenteeism and performance; aff ordability and availability of text books; hidden, additional costs putting
education out of the reach of the poor; poor quality of school infrastructure.
1. Teacher absenteeism was consistently reported in rural schools; the cases were closely linked to the absence of
basic infrastructure services in the village such as clean water supply, sanitation and, to a lesser extent, electricity.
Parents said the teachers mostly hail from urban areas and are unwilling to live in the village when basic facilities
are lacking. Clean water and sanitation are important not just for teachers but also for students – for whom
learning key hygiene behaviors is not possible in the absence of water supply and sanitation.
2. The Ministry of Education (MOE) should adopt a policy to construct schools only with an assured sustainable
supply of clean water and locally appropriate sanitary toilets at a ratio of not more than 50 students per toilet.
The school health education unit (UKS) should design programs to promote the use of these facilities and key
hygiene practices, such as excreta disposal only in toilets and hand washing with soap after defecation and
before eating.
3. The MOE’s construction policies regarding primary schools should be reviewed for anomalies that impair quality
education. Currently, many primary schools are built with only two or three classrooms, which means that two
or three diff erent grades will always be combined for teaching, resulting in a poor learning experience.
4. Establish ways for parents to monitor and report on teacher absenteeism and performance to authorities who
are responsible for the teachers and their salaries. The use of teacher attendance registers maintained by school
PTAs and annual assessments of teacher performance by all parents of students by simple secret ballot voting
procedures could be linked to teachers’ salaries and increment payments. The Ministry of Education should be
more directly involved with parents in monitoring teacher absenteeism and enforcing sanctions.
5. Make textbooks available to all poor students. Some possible solutions: schools could purchase the books
and lend them to poor students (if necessary, a small, refundable deposit could be required). If students must
purchase books, the school should buy back books at the end of the academic year. Parents also suggested that
books cover two consecutive years of education, extending their life and cutting costs.
6. Registration fees at secondary schools deter enrollment of poor students. There seems to be no fi xed fees;
schools charge whatever they can. It is recommended that the government establish reasonable entry fees and
publicize them, e.g. a limit no higher than the equivalent of 4-5 days of the local minimum wages.
7. Schools should be built on public transport routes. Students should be given free or subsidized monthly public

45Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
transportation passes. Private sector transportation providers should be obliged to off er concessional rates
to students if they make use of public sector-provided incentives to promote entrepreneurship, e.g. loans at
concessional rates to buy public transport vehicles.
7. 4. For Clean Water and Sanitation Services
Policymakers need to wake up to the fact that the poor are paying exorbitant prices for clean water—as much
as 30 times utility rates. None of the 424 poor men and women consulted had piped water connections and so
did not benefi t from the heavily subsidized utility water that is enjoyed by the non-poor. With no access to public
water utilities they are forced to buy water from neighbors or independent providers. The rural poor depend on
groundwater, access to which is limited in the dry season.
About half the population in Indonesia, both the poor and the non-poor, continue to use water from shallow and
deep wells, even when they are connected to utility networks. Typically the well water is not potable in urban
areas.
At all eight sites the poor had almost no access to sanitation. The situation is representative of conditions across the
nation. In both rural and urban areas of the study people were using the nearest natural water body for defecation
purposes. The failure to provide basic sanitation solutions for the millions of the urban and rural poor is creating an
environmental disaster that impacts all Indonesians. Policymakers need to open their eyes to this little-recognized
public health disaster and deal with its roots.
Recommendations on Ways to Supply Clean Water to the Poor
1. In urban areas, assess the real costs of Small Scale Independent Water Providers (SSIPs) operation against
profi ts they make through use of PDAM water. Set non-negotiable ceilings on the price SSIPs may charge, so all
consumers pay the same in the city. SSIPs should not be allowed to enjoy subsidized PDAM rates while charging
exploitative rates to the poor.
2. Policies and regulations should help ensure competition among water providers, at least in urban areas where
multiplicity of providers is economically feasible. Publicize the ceiling rates to educate consumers and encourage
the poor to report violations. PDAMs should recognize the market share of the SSIPs and enter into formal
contracts with them for supply at lower-than consumers’ tariff rates, with the understanding that re-selling prices
will not exceed PDAM’s tariff rates for direct customers. PDAMs should monitor the rates charged by SSIPs to
consumers and sever supplies to SSIPs who charge exploitative rates.
3. Recognize that the urban poor are able and willing to pay fair rates for clean water. Poor customers are not an
obstacle to PDAMs charging tariff s that cover costs as well as reasonable profi t that can make PDAMs viable.

46Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
The poor already pay the SSIPs a lot more than the actual production costs of PDAMs. The principal obstacles
to connecting the poor to PDAM networks, which need to be addressed creatively by service provision policies,
are: a) the high, one-time cash cost of connection that the poor typically cannot aff ord, and b) poor people’s lack
of tenurial status in their squatter settlements on public land – which at present does not allow them to seek a
legal water supply connection.
4. The rural poor were able to get reasonably clean ground water from protected dug wells or bore wells in
Java. Well water was not potable or suffi cient on the dry NTB island and in the swampy, riverine Kalimantan
village. Indonesia’s varied topographical and geo-hydrological conditions require various types of water supply
technologies that are geared to local conditions. A national approach to rural water supply should capitalize on
the rural population’s high demand for clean water services, and works with the poor to identify and develop
service options that meet local demands using technologies and water management arrangements that can be
sustained by the local population.
Recommendations to Improve Sanitation Services for the Poor
1. Scale up the application of approaches for rapid communitywide adoption of improved hygiene practices in
rural areas.11 Establish national policy and strategies for rural sanitation programs that will enable scaling up of
fi eld-tested best practices consistently across the country.
2. Scale up institutional capacity in local governments for promoting a range of locally appropriate low-cost
sanitation options so that sanitation is aff ordable by all. These could range from improved direct pit dry latrines
to more sophisticated off set-pit, composting, pour-fl ush and water-seal single or twin-pit latrines—all with
adaptations for cost-reduction using locally available materials.
3. Develop similar options for poor urban communities. A successful experiment in that direction was fi elded
through the SANIMAS12 project. The approach is currently being replicated by local governments. But because,
local governments and legislators do not yet understand the innovative process aspects of the SANIMAS
approach, its community mobilization and capacity building components are currently at a risk of being eroded.
Services created without adequate community capacity and ownership buildings are unlikely to be sustained.
4. Overarching the above is a larger problem, i.e. a policy and strategy vacuum with respect to sanitation services.
To address this vacuum,
11 An example is the Community-Led Total Sanitation (CLTS) approach propagated through selected large scale RWSS programs, which builds com-
munitywide movements and social pressure for all households to be free of open defecation within short time periods. Field trial results in Lumajang,
Sumbawa, Muara Enim, Muaro Jambi, and Sambas districts have been promising. For more information see CLTS–related papers in issues of the
PERCIK newsletter on the GOI website: www.ampl.or.id
12 Sanitation by Communities project piloted in seven Indonesian cities during 2001-2003, promoting community-based sanitation solutions for the
urban poor.

47Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
• Urban policymakers must better understand the real costs of inaction and what makes for sustained services
as these are both key to progress on the urban sanitation front. Sector analyses studies and formative research
into how policymakers and opinion leaders think about sanitation in Indonesia are needed to develop
targeted advocacy campaigns to generate public pressure for improved sanitation services, and an enabling
environment for sanitation investments that can benefi t the poor.
• Devise innovative ways to catalyze high-level political commitment to improving sanitation services for the
urban poor. The ongoing failure to do so has resulted in a widespread urban health and environmental crisis in
Indonesia – both for the poor and the non-poor, yet the issue remains invisible and low priority for politicians
and leaders. Raising the political profi le of the sanitation agenda could include, for instance, cross-sectoral
analysis assessing the economic and human development costs to the nation from poor sanitation, linking
potable water resources and sanitation management with strategies for poverty reduction and economic
growth; organizing high-level regional conferences to periodically compare progress among neighboring
countries regarding their commitments to the MDGs for sanitation; raising consumer and voter awareness
regarding the impact on the entire population stemming from the absence of basic sanitation services for the
poor.
5. Equipping primary schools with clean water and basic sanitation facilities is considered one of the most cost-
eff ective investments for human development. However, provision of these services needs to be directed by
policies for sustained functioning and use, e.g. ratios of toilets to students not exceeding 1:50; mandatory
hygiene education curricula to accompany service provision; incentives and sanctions in allocation of
operational budgets to schools (BOS) linked to funtionality of school water and sanitation facilities.

48Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r

1Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Annex 1: Study ToolsQualitative Research Sample and Sequence of Tools - Making Services Work for the Poor Study
INDICATIVE SEQUENCE AT EACH STUDY SITE
Respondents Research instrument Information targeted
1 Introductory meeting
with community
group
Mixed gender
and age groups,
possible presence of
community leader/s
Break into gender-
segregated groups.
• Introduction of researchers (important—
where are they from?)
• Explanation of purpose of meeting,
• Request for permission to research,
• Likely schedule of further discussions in the
community.
Welfare Classifi cation
Local Livelihoods pattern analysis—Have
both gender groups present results. Compare
and consolidate
Use available village/kelurahan map to identify
areas where most poor households are clustered
(using criteria from Welfare Classifi cation)
• Description of criteria locally
used to describe diff erent
levels of well being and
poverty
• Proportion of local
community “poor” by local
defi nitions.
• Pattern of major livelihood
activities, by gender.
• Proportion of average poor
hh’s. Income/earnings from
various sources.
2 Men, Women and
children met in
the course of the
walk through the
community
Transect walk (with copy of map, and
Environmental Healthwalk Observation
Checklist) to visit clusters of poor households,
explain purpose of visit, make appointments
for FGDs , observe environmental sanitation
conditions/ location of poor households vis-
à-vis public infrastructure facilities and health
and education service providers.
• Identifi cation of poor
households to contact for
setting up FGs
• Living environment and
facilities.

2Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
3 Focus Groups with
men and women
from identifi ed
“poor”households
2 groups by gender,
each group with an
equal mix of 2 age
groups:
Young women
(15 - 30)
Young men (15-30)
Older women
(>30 – 50)
Older men (>30-50)
FGD: MAPPING SERVICE PROVIDERS
a. Venn diagramming for service providers in
general (See Guidelines provided)
b. Pocket voting: Mapping of local basic
service providers, for the selected Health,
Education, Water and Sanitation services.
(See Guidelines provided)
c. Ranking and scoring of options preferred
for H/E/WS services
OR
For the most used option in each category:
d. Benefi ts and Value for Cost perceptions
(See Guidelines provided)
e. Rating scales for satisfaction with the most
chosen option in each category —- criteria
used for judging quality (See Guidelines
provided)
f. If public services included among those
not used or little used, , probe for reasons,
perceived value for cost and quality.
_____________________________________
FGD: VOICE & CLIENT POWER ISSUES
With Discussion guide regarding poor
people’s experience, ideas for strengthening
accountability of service providers and
policymakers to the poor—
Possible Case Studies identifi ed for pursuing
further.
An overall mapping of the
service-providing agencies/
persons who are important to
poor women and men, as well
as those irrelevant or less useful
to them. Probing of reasons why
considered useful/not so.
• What service options are
available?
• Who is providing?
• Extent of usage of available
options
• Perceived costs of diff erent
options, in cash/kind/ time/
eff ort
• Who in the household
decides/chooses each type
of service option to use ?
• Actual expenditures incurred
to avail of services- in cash
and kind, time and eff ort
(daily/weekly/monthly/one
time)
Poor men and women’s
• rationale for choice ,
• Perception of value for cost
• Perception of what
constitutes quality service
__________________________
Poor people’s opinions and
experience re.exercising
client power, client voice,
accountability seeking by the
poor.

3Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Identifi ed poor
women /Men for
case studies
In-depth individual interviews to explore
case studies of failures of basic services,
(With reference questions for basic health serv-
ices failures)
Tracing events leading to
• Maternal death/disability from
childbirth,
• Stillbirth/neonatal death,
• Infant death,
• Under-5 death.
• Severe child malnutrition
• Girl/Boy of primary school age
never enrolled.
• Girl/Boy dropped out of pri-
mary school
Observations with checklists/standards for
• Puskesmas/ bidan/ dukun/ private doctor’s
outlet/service provision session.
• Primary school, Junior Secondary school/
class activity.
• Inspection of public and household latrines,
school sanitation and water facilities,
• Inspection of clean water sources, Water
storage and transportation facilities/
practices of water vendors,
• Water quality testing kit for drinking water in
poor homes
• Quality of selected types of
services provided by each
provider/obtained by the
poor.
• Condition of service facilities
Selected health/
education/water
and sanitation
service providers
Interviews with selected Service providers,
in each category
Providers’ views re:
• Quality of (identifi ed specifi c)
services provided
• Preferences of the poor.
• Obstacles to improving
services for the poor
• What can help the poor
obtain better services.

4Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
The following participatory analysis tools13 were used to explore diff erent topics, mostly with men’s and
women’s groups separately.
Participatory Analysis Tools Description
Welfare Classifi cation* Tool to elicit local criteria by which people are classifi ed as poor, rich/
well off or in-between classes. This produced site- specifi c descriptions
of poverty, as well as the means to identify community households with
whom to engage in, for further research activities.
Social mapping* Activity to locate poor households in relation to other households,
infrastructure, and other basic services available in the community.
Health/environmental transect walk* Using the Social Map and a checklist for environmental observation,
researchers walked around the community to assess environmental,
health, and sanitation conditions, visit poorest clusters of households,
meet poor women and men, and set up appointments for group
discussions
Venn Diagramming This PRA tool was used to understand the institutions that are important
in poor people’s lives as well as those which are not relevant/unimportant
to them, and the poor people’s reasons for their assessments
Livelihoods analysis This PRA tool was used to rapidly map the major livelihoods –related
activities of poor women and men in the community, and the proportion
of total incomes derived from the various activities
Pocket Voting This was used to understand the choices available to the poor at each site
with respect to providers for diff erent types of services, and the extent to
which they were using each type
Rating scales* Graphic scales of standard length were used to elicit people’s satisfaction
levels with services. The two ends of the scale represented “No satisfaction
at all” and “Full satisfaction,” with mid-points and quarter points also
marked.
Benefi ts and Value for Cost* A quantitative participatory tool to obtain people’s assessment of the
extent to which their expectations are fulfi lled by the services available,
and the extent to which they think them to be worth the cost incurred to
obtain the services.
The sequence of tools was interspersed with focus group discussions covering several other aspects such as the
experiences of the poor in exercising voice in community decisions and in seeking accountability from service
providers. Site reports were produced by researchers for each site studied, in Indonesian, along with a documentation
of the results of each participatory analysis tool. Analysis was a collaborative exercise with most of the fi eld team
members. This consolidated report was written based on all of these outputs.
13 Fuller descriptions of the * marked MPA tools can be found in Sustainability Planning and Monitoring : A Guide to Methodology for Participatory
Assessment for Community-Driven Development Programs . Mukherjee, Nilanjana and Van wijk, Christine. Water and Sanitation Program, IRC
International water and Sanitation Centre and the World Bank. 2003..

5Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Annex 2: Village DescriptionsTable 2.1. Paminggir—Remote, Forestry-dependent Rural Community, South Kalimantan
Well being Indicator Rich (Kaya) In-between (Sederhana) Poor (Miskin)
Livelihood Own 10 fi sh ponds and
2-3 speedboats, successful
traders.
Fishers with 1 speedboat
and 2 fi sh ponds.
Wage laborers. No
fi shponds..
Diets Varied foods. Eat meat or
fi sh at every meal.
Can eat enough to fi ll
stomach.
Very simple meals,
sometimes quantity not
enough.
Clothes Many clothes, good
quality.
Enough for needs, but
average quality.
Few clothes, low quality.
Home ownership 20m x 8m size. High
quality timber (ulin) house,
tiled fl oor.
Medium quality timber
(Balangiran) house. Size
5-8m x 10m.
Low quality timber (katol)
house. Smaller than 5m
x 10m.
Livestock 30-40 buff aloes. 2-5 buff aloes. No livestock.
Health Services used Specialist doctors or city
hospital.
Health Center (Puskesmas). Traditional healer in
village/Pustu.
Income Rp.100,000/day. Between Rp.30,000-
Rp.100,000/day.
Rp.0-Rp.20,000/day.
Household assets All equipment, color TV
21” or bigger, refrigerator,
rice cooker, cupboard,
chairs + table of wood.
Some equipment, TV
14” or smaller. Cook with
kerosene, plastic or cane
chairs.
No TV. Cook with
fuelwood, 1 chair.
Contribution to Arisan
(saving + credit group)
Rp.50,000 / week. Rp.2,500-Rp.10,000/ week. Do not join arisan.
Proportion of
community households
16% 33% 51%
Table 2.2. Bajo Pulau - Island Fishing Community , West Nusa Tenggara
Well-being indicator Rich/able
(Aha mampu/kaya)
Middle/Suffi cient
(Cukuplah/Lung
satataba)
Poor
(Singsara/Tidak
mampu)
Livelihoods and livelihood
assets
Trade in lobster, pearls,
sea cucumber, marine
fi sh, own more than one
motorboat.
Sea fi shers, lobster and
pearl fi shers with own
motor boat.
Fishers with small sail
boat.
Income More than Rp.1 million/
day.
More than Rp.40,000/ day. Rp.10,000/ day.

6Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Children’s education High School. Primary – Secondary
School.
Do not complete primary
school.
Lighting facility Have generator. Get connection from
owners of generator.
Oil lamp.
Health service provider Specialist doctor in Bima
(city on mainland).
Puskesmas or private
doctor in Sape (town on
mainland).
TBA and traditional healer
in village.
Asset Stone-built house,
galvanized iron roofi ng,
on 12-20 stilts.
Tiled roof, plywood walls,
on 6-12 stilts.
Bamboo and thatch
roofed house, on 6 stilts.
Daily household
expenditure
Rp.50,000-Rp.100,000. Rp.25,000-Rp.40,000. Rp.8,000-Rp.9,000.
Daily expenditure to buy
water
Rp.10,000 (10 jerry cans x
35 liters).
Rp.5,000 (5 jerry cans x 35
liters).
Rp.1,000-Rp.2,000 (1-2
jerry cans x 35 liters).
Proportion of total
households
14% 42% 44%
Table 2.3. Alas Kokon - Rural, Dryland Farming Community, Madura, East Java
Well-being indicator Rich (Kaya) In-between (Sedang) Poor (Miskin)
House Permanent structure,
ceramic tile fl oor.
Simple house, self-
constructed.
Thatch house, dirt fl oor.
Livelihood Landowning farmers,
Government employees,
Fruit traders. Daily income
Rp.50,000 ++.
Laborers, some skilled. Unskilled laborers in
construction, agriculture,
transport.
Land ownership 2 or more hectares of
cropland.
0.5 to 2 hectares of
cropland.
No land owned. If owned,
only the land under the
house.
Livestock 3 or more cows or
buff aloes.
1-2 goats. Take care of
cattle owned by the rich.
Children education At the most complete
junior high school.
A few reach and complete
junior high school.
Only primary school. Many
drop out.
Health Services used Private doctor. Puskesmas and bidan desa. bidan desa or traditional
healer in village. If having
money, go to Puskesmas
(cost of transport).

7Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Water Supply Have own water storage
tank. Buy from water
truck.
• Dugwell, collect by
turn once/week.
• Buy from water truck
sometimes
• Bathe and wash in
river.
• Collect dugwell water
once/week by queuing
up, for cooking +
drinking
• Collect water for other
needs from river far
away. Many hours/
month used to collect
water.
Assets 4-wheel transport, TV,
tape recorder, refrigerator,
motorbike bought with
bank-loan.
Second-hand motorbike,
bough on credit.
No means of transport,
No TV.
Food Eat 3 times a day,
complete with meat or
fi sh and vegetables.
Simple meals, because
market is far.
Eat 2 times a day. Rice
with corn or cassava and a
little dried, salted fi sh.
Proportion of
community households
9% 24% 67%
Table 2.4. Kertajaya – Irrigated Rice-Farming Rural Community, West Java
Well-being indicator Rich (Sugih)In-between
(Pertengahan)
Poor (Ora duwe,
melarat, miskin)
House • Permanent structure,
ceramic tiled/marble
fl oor, on 0.5 hectare
land, iron fencing;
• Have own bathroom
and sanitary toilet.
• Walls half cement half
wood/thatch;
• Simple bathroom and
pit latrine. House on
own land + 150m2;
• Furniture simple,
plastic.
• Bamboo thatch
house—leaks during
rain;
• Dirt fl oor;
• House built on
someone else’s land;
• Furniture wooden—
but- self-made.
Crop land ownership Up to 70 hectares—
stretching to next village.
1,000m2 – 0.5 hectare
only within the village.
No land owned.
Livelihood • Own rice huller/ shop/
tractor for renting/
business;
• Manage own
farmlands.
• Work in government
or private sector in
Jakarta;
• Use wage-laborers for
farming.
• Agricultural or
construction laborers
• Cart/rickshaw pullers
in Jakarta, Bekasi,
Pamanukan.

8Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Transportation Car and motorbike. Motorbike. Bicycle.
Foods eaten daily Bread, milk, beef, chicken. Soybean cake, eggs
sometimes.
Rice, soybean cake,
kangkung (leafy
vegetable).
Children’s education Can go to college. Can complete high school. • Many children – all
cannot be educated;
• Some get primary
schooling, some never
enrolled.
Health Services Used • To private doctor in
Subang (district) or
Bandung (province
capital);
• Childbirth in hospital
• To Puskesmas Mantri or
doctor in village or in
Pamanukan (nearest
town);
• Childbirth with Bidan
desa
• If minor ailment – get
medicine from local
shop;
• If more serious – go to
Puskesmas with Kartu
Sehat or to Dukun (TBA).
Livestock Many goats – given to
poor people to maintain,
with sharing agreement
for off springs
Up to 10 goats Do now own. Take care of
goats of the rich.
Proportion of
Community households
13% 24% 63%
Table 2.5. Antasari—Urban Kelurahan , South Kalimantan
Well-being indicator Rich (Kaya) Middle (Sederhana) Poor (Miskin)
House Tiled roof, ceramic fl oor
tiles, cement and brick
walls.
Simpler home, galvanized
iron sheet roofi ng,
wooden board walls and
fl oor.
Thatched roof, thin board
walls, bamboo or board
fl oor.
Livelihood Trader, or government
employee level 3 or more.
Kiosk vendor, or
government employee
level 3 or lower.
Agricultural wage
laborers, construction
laborer, fi shers.
Mix with Mix only with the rich,
their own crowd.
Freely mix with both
richer and poorer than
themselves.
Avoid mixing with the
rich, feel embarrassed to.
Water Supply Drink bottled water.
Bathe, wash, cook in
water supplied by PDAM
connection.
Cook with and drink
PDAM water (own
connection). Wash +
bathe in dugwell water.
Drink and cook with
PDAM water (bought from
the rich). Bathe and wash
at dugwell or river.

9Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Sanitation Sanitary toilet—more
than 1, built inside house.
Household toilet, but
some not sanitary, only
one per house.
• Public toilet
• In plastic bags and
throw out of house/
into river;
• No household facility.
Clothes and jewelry Silk, pure gold, Rolex
watch
Cotton, clothes. Gold-
plated jewelry
Ordinary clothes
Household assets 21” or bigger TV, high
quality furniture,
refrigerator.
Simple furniture – smaller
TV.
nothing
Food • Nutritious always
• Can eat at restaurants.
• Sometimes nutritious;
• Can eat at warungs
(roadside foodstalls)
Eat whatever is available
at home
Means of transport Car/motorbike Motorbike bought on
credit
Sometimes have bicycle.
Proportion of
Community households
19% 37% 44%
Table 2.6. Jatibaru—Urban Poor Kelurahan on the Outskirts of Bima, West Nusa Tenggara
Well-being Indicator Rich / Able (Ntau wara)Middle / Suffi cient
(Nohi ru’u)
Poor
(Ncoki mori)
Livelihoods and
Livelihood Assets
Civil servant, traders in
brick/stone, farmers.
Carpenter, horse cart
driver, seller/vendor,
wage laborers.
Wage laborers in agriculture,
brick/tile production,
collecting and selling wood
Income More than Rp.1,000,000/
month
Approx. Rp.10,000/day
not regular
Approx. Rp.5,000/day.
Children Education University High school Primary school/do not
complete primary school
Health Service provider Doctor. Traditional healer. Traditional healer in village.
Water and Sanitation
Services
Own latrine and dugwell
(water source)
Public dugwell, Open
defecation in river.
Public dugwell, Open
defecation in river.

10Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Asset • own land (1 ha);
• permanent stone built
house with roof tile,
ceramic fl oor;
• Owner of cow/goat +
chicken (+ 10).
• Permanent (6-9
pillars) house, with
platform, cheap
rooftile, bamboo and
brick stone wall;
• Owner of goat,
chicken and duck;
• Own land (10 are)
Platform house (4 pillars),
cheap materials, bamboo
wall/fl oor.
Food Pattern 3 times per day, rice, fi sh,
vegetables, fruit.
2 times per day. Rice with
vegetables and small fi sh
(fresh) .
2 times per day. Rice with
salted dried fi sh, vegetables.
Proportion of
Community
households
18% 28% 54%
Table 2.7. Simokerto—Urban Low-Income Neighborhood and Squatters’ Settlement, Surabaya, East Java
Well-being indicator Well-off (orang mampu) In-between (sedang) Poor (tidak mampu)
House Permanent structure,
ceramic tiled fl oor, about
9m x 15m, Complete
facilities.
Simpler construction
about 5m x 8m.
Small 3m x 4m area,
Temporary structure of
ply-boards, tin roof, near
rail track. Live in parents’
house.
Water supply All have utility connection
– piped water. Drink, cook
+ bathe + wash with clean
water.
Some have utility
connections. Others buy
from vendor.
Dugwell water – poor
quality. Dries up in
summer. Forced to buy
expensive water from
vendor.
Sanitation Ceramic toilet pan, in
house sanitary toilet
Communal toilet. A few
have own simple toilet,
but not sanitary.
Open defecation in pits
on public land owned by
Railways corporation.
Livelihood Traders, shop owners,
permanent well-paid jobs,
salaried people.
Salaried people in public
or private sector.
Wage laborers, rickshaw
and cart-pullers, motor
garage workers, water
vendors. Unemployed
people.
Transportation Own car and motor bike. Own motorbike and cycle. Rickshaw or cart – but not
all have.

11Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Income Above Rp.2 million/
month
Between Rp.300,000
– Rp.350,000/month.
Less than Rp.200,000/
month.
Children’s education High school and college Usually just high school. Pass primary school at the
most.
Health Services used Private hospital or
specialist private doctor
Puskesmas or public
hospital.
Traditional medicine
sellers (Jamu) or healers.
Sometimes go to
Puskesmas.
Electronic Goods owned 21” color TV, VCD player,
refrigerator.
14” TV, radio/tape player. None.
Proportion of
community households
6% 22% 72%
Table 2.8. Soklat—Urban Poor Kelurahan in Subang, West Java
Well-being indicator Rich / Able (Benghar)Middle / Suffi cient
(Menegah/Cukup)Poor (Miskin)
Livelihoods and
Livelihood Assets
Doctor, civil servant,
trader, entrepreneur, own
shop, car repair shops.
Entrepreneur, car drivers,
teachers, share croppers.
Construction labor, farm
labor, service in a shop,
cart/rickshaw pullers
Daily household
expenditure
Big income. Enough to live on. Big expenditure but not
enough income.
Income More than Rp.3-4 million/
month. Can even be
Rp.50,000/ day
Rp.15,000-Rp.20,000/ day. Maximum Rp.10,000/ day.
Education University High school – Secondary
school.
Primary school only, or
do not even complete
primary school.
Health Service provider Doctor, private hospital,
mid wife in village.
Health Centre, bidan
desa, traditional healer in
village.
Massage, traditional
medicine. Buy drugs from
local kiosk.
House Clean, healthy, large
house, 2-3 storeys.
Ceramic fl oor, iron fencing.
Clean house, cement fl oor,
bamboo fence.
Poor quality house. Dirt
fl oor, roof tiles old, thatch
walls. No fence. Do not
own the land under the
house.

12Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Asset Own refrigerator, sofa,
motor car, TV, luxurious
house.
Own TV, radio, bicycle,
simple chairs, rickshaw/
becak, own latrine, electric
pump for water.
• Old bicycle, small radio,
simple kitchen set;
• Nothing
Proportion of
Community households
20% 26% 54%
Annex 3
Table 3.1. Choice and Costs of Primary Education Services Reported by the Poor at 8 Sites SITES Certifi cate
(upon
completing
school)
Enrollment/
Registration/
Construction*
Uniforms Tuition
(monthly)
Books
(per year)
Shoes/Bag
(yearly)
Snacks
(daily)
RURAL
PAMINGGIR/
S.Kalimantan
(SDN)
7,500 10,000 - - - - -
BAJOPULAU/ NTB
(SDN)- - 140,000 / yr N.M. 60,000 55,000 1,000
ALAS KOKON/ Madura
(Madrasah Ibtidaiyah)- - 5-10,000** 10,000 - -
KERTAJAYA/ W.Java
(SDN)65,000 – 100,000
30,000 / yr7,000**
12,000
-18,000- 1,000
URBAN
ANTASARI / S.Kalimantan
– (SDN)7,500 -
75,000 /
3 yrs2,000** 15,000 1,000
JATIBARU: NTB
(SDN)5,000 100,000-
65,000 /
3 yrs- 20,000 35,000 -
SIMOKERTO: E.Java
(SDN)- 750,000- -
17,000** +
10,000 for
computer +
copybooks
80,000 - -
SOKLAT: W.Java
(SDN)100,000 100,000- 30,000/yr 10,000** 60,000 - -
* Payable in instalments throughout primary school period ** All reported that these fees are not being charged since September 2005
NOTE:
• SDN – Government- run Primary School
• Madrasah Ibtidaiyah – Community managed Islamic School
Husband and wife choose the school together at all sites

13Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.1. Benefi t and value perceptions for primary education services
Value for cost score
most used by the poor at 8 study sites: WOMEN's perception
97.5
90 87.5 8892.5 91.4
65
80
100 100 100
26
95 94.3
62.5
82.2
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
SD Negeri SD Negeri Madrasah Ibtidaiyah SD Negeri SD Negeri SD Negeri SD Negeri SD Negeri
RURAL URBAN
rocSe
most used by the poor at 8 study sites: MEN's perception
80
100
57.5
100
82.5
74
86
100100 100 100 100 100
74
80
63
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
SD Negeri SD Negeri Madrasah Ibtidaiyah SD Negeri SD Negeri SD Negeri SD Negeri SD Negeri
RURAL URBAN
rocSe
Value for cost score
Notes:
SD Negeri = Government – run Primary School (grades 1 – 6)
Madrasah Ibtidaiyah = Religious school, also government – run (grades 1 – 6)

14Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.2. Satisfaction Ratings for Primary Education Providers
Paminggir
Bajopulau
Alas Kokon
Kertajaya
Antasari
Jatibaru
Simokerto
Soklat
Legends Women's Rating Men's Rating
SD Negeri
Madrasah Ibtidaiyah
Score 0 = No satisfaction at all Score 100 = Full satisfaction
50 27 88 5 100 80
50 0 100 60 70
100 0 25 50 75
0 100 50 75
0 100 50
60 0 100 50
25 0 100 50 80
0 100 50 75

15Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Tabl
e 3.
2. C
osts
of s
econ
dary
scho
ol e
duca
tion
repo
rted
by
the
poor
at 8
stud
y sit
es
RURA
L
BAJO
PU
LAU
No
SMP
on th
e isl
and.
No
child
ren
cont
inue
. Mos
t boy
s dro
pout
eve
n fro
m S
D to
wor
k an
d ea
rn o
n bo
ats
KERT
AJA
YA O
nly
3 ch
ildre
n fro
m th
e vi
llage
go
to Ju
nior
Hig
h sc
hool
, out
side
villa
ge. T
hey
are
from
the
uppe
r cla
ss h
ouse
hold
s. Th
e en
try
fee
Rp.1
.5 m
illio
n is
an u
nthi
nkab
le
amou
nt fo
r poo
r hou
seho
lds
Gov
ernm
ent-
run
SMP
Neg
eri /
SLT
PM
adra
sah
Tasa
naw
iyah
/ Pes
antr
en
PAM
ING
GIR
* fre
e
ALA
S KO
KON
*Rp.
15,0
00 /
mon
th
(Com
mun
ity-
ente
rpri
se.
Onl
y 8
enro
lled
)
URB
AN
AN
TASA
RI*
Rp.1
00,0
00 /
yea
r, .b
ut.
all
stud
ents
re
ceiv
e
scho
lars
hip
JATI
BARU
Regi
stra
tion
Rp.1
20,0
00 +
Cons
truc
tion
fee.
Uni
form
45,
000/
yrTu
ition
Rp.
15,0
00/m
on.-f
ree
now
Boo
ks/s
hoes
/bag
20,
000-
112,
000
/yea
r
SIM
OKE
RTO
Cons
truc
tion
fee
Rp
600,
000
Uni
form
30,
000/
yr.
Tuiti
on R
p.38
-42,
000/
mon
. Fre
e no
w.
Book
s 80,
000/
yr
SOKL
ATCo
nstr
uctio
n fe
e R
p. 4
00,0
00
– 60
0,00
0
Uni
form
30,
000/
yrTu
ition
fees
25,
000/
mon
.Fre
e no
w. B
ooks
60,
000/
yr
Mad
rasa
h Ta
sana
wiy
ah –
Fun
ded
by D
ept.
of R
elig
ious
Aff a
irs ;
SMP
Neg
eri –
Fun
ded
by D
ept o
f Edu
catio
n &
Cultu
re. I
n vi
ew o
f the
dat
a fro
m W
elfa
re C
lass
ifi ca
tion
belo
w ,
Seco
ndar
y Sc
hool
see
ms t
o be
a se
rvic
e lit
tle u
sed
by th
e po
orW
elfa
re C
lass
ifi ca
tion
data
fro
m 8
site
s re
gard
ing
char
acte
rist
ics
of lo
cal
poor
in
term
s of
“ed
ucat
ion
of c
hild
ren”
:An
tasa
ri - “
Child
ren’
s edu
catio
n” n
ot m
entio
ned
amon
g re
port
ed c
hara
cter
istic
s of t
he p
oor
Jatib
aru
- “P
oor c
hild
ren
may
enr
oll i
n SD
(prim
ary
scho
ol) ,
ofte
n th
ey d
on’t
fi nish
SD
(prim
ary
scho
ol)”
Sim
oker
to
- “ T
he p
oor o
nly
pass
SD
/Mad
rasa
h Ib
tidai
yah.
Don
’t at
tend
SM
P/SL
TP (j
unio
r hig
h sc
hool
)”So
klat
- “
The
poo
r can
man
age
only
up
to S
D p
ass”
Pam
ingg
ir - “
Child
ren’
s edu
catio
n” n
ot in
clud
ed a
mon
g re
port
ed c
hara
cter
istic
s of t
he p
oor
Bajo
Pul
au
- “Ch
ildre
n of
the
poor
do
not e
ven
pass
SD
”Al
as K
okon
- j
ust r
each
SD
, not
pas
s, dr
op o
utKe
rtaj
aya
- chi
ldre
n no
t enr
olle
d in
scho
ol –
or o
nly
in S
D

16Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.3 Proportion of votes for provider of secondary school education services
Women's view Men's view
63%
37%
SMP Negeri Madrasah Tsanawiyah/ Pesantren SMP Yayasan (private sector)
62%
37%
2%

17Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.4 Benefi t and value perceptions for secondary school education services
Secondary School Education Service Providers most used by the poor at 8 study sites: WOMEN's perception
93.390
92.5 91
80
87.593.3
10095 94
66
75
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
SMP Negeri - MadrasahTsanawiyah
- MadrasahTsanawiyah
SMP Negeri SMP Negeri SMP Negeri
RURAL URBAN
rocSe
e Value for cost score
loohcs oN
loohcs oN
Secondary School Education Service Providers most used bythe poor at 8 study sites: MEN's perception
90
67.5
93.3
74
92.586.67
100
87.5
100
74
62.568.3
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
SMP Negeri - MadrasahTsanawiyah
- MadrasahTsanawiyah
SMP Negeri SMP Negeri SMP Negeri
RURAL URBAN
e Value for cost score
oN
cslooh
oN
c sloo h
rocSe
Notes:
SMP Negeri = Government run junior high school (grades 6 – 8 or 7 – 9)
Madrasah Tsanawiyah = Religious school, run by government (Department of Religious Aff airs), grades 6 – 8)

18Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.5 Satisfaction ratings for secondary school education providers
Paminggir
Bajopulau
Alas Kokon
Kertajaya
Antasari
Jatibaru
Simokerto
Soklat
Legends Women's Ratings Men's Ratings
SMP Negeri
MTSn
SMP Yayasan
Score 0 = No satisfaction at all Score 100 = Full satisfaction
50 0 100
0 100 50
60 0 100 50
0 100 50 75
50 40 90 2 100 10
100 0 25 50 75 45
0 100 50 90 10
25 0 100 50 55

19Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Tabl
e 3.
3. C
hoic
e an
d Co
sts o
f AN
C Se
rvic
es U
sed
by th
e Po
or a
t 8 S
tudy
Site
s
RURA
L SI
TES
PAM
ING
GIR
/ S.
Kalim
anta
nBA
JOPU
LAU
/ N
TBA
LAS
KOKO
N /
Mad
ura
KERT
AJA
YA/ W
.Jav
a
Mos
t use
dBi
dan
Kam
pung
(TBA
)
Rp.3
-5,0
00 /
visit
Sand
o (T
BA)
Free
or 1
kg ri
ce
Duk
un (T
BA)
Rp.5
,000
/ exa
min
atio
n
bida
n de
sa, p
ract
icin
g at
hom
e
in th
e ev
enin
gs
Rp.2
5,00
0 (in
cl.R
p.10
,000
fo
r
tran
spor
t)
In c
ompa
rison
with
oth
er
choi
ce a
vaila
ble
If bi
dan
desa
ava
ilabl
e in
PUS
TU,
then
at P
USTU
Rp.3
-5,0
00/ e
xam
inat
ion
bida
n de
sa –
but n
ever
ava
ilabl
e
bida
n de
sa
• Rp
.15,
000/
exa
min
atio
n
Rp.2
5,00
0/ h
ome
visit
Duk
un (T
BA)
2-5
kg ri
ce
URB
AN
SIT
ES
AN
TARA
SARI
/ S.
Kalim
anta
nJA
TIBA
RU /
NTB
SIM
OKE
RTO
/ E.
Java
SOKL
AT /
W.J
ava
Mos
t use
dPu
skes
mas
Rp.3
,000
/visi
t
• Sa
ndo
(TBA
) acc
ordi
ng to
wom
en
Rp
.3-5
,000
+ 1
cup
rice
• Pu
skes
mas
– a
cc.to
Men
.
Rp.3
,000
/visi
t
Pust
u/ P
uske
smas
Rp.1
1,00
0 (in
clud
es R
p.6,
000
for
tran
spor
t)
• Pu
skes
mas
Rp.
12,5
00 (i
ncl.
Rp.1
0,00
0 fo
r tra
nspo
rt)
bida
n de
sa p
ract
ising
at
hom
e
Rp.3
5,00
0 (in
cl.
Rp.1
0,00
0 fo
r
tran
spor
t)
In c
ompa
rison
with
oth
er
choi
ce a
vaila
ble
Bida
n Ka
mpu
ng (T
BA)
Rp.5
,000
/ exa
min
atio
n
bida
n de
sa
Rp.1
0-15
,000
Duk
un (T
BA)
Rp.3
,000
Para
ji (T
BA)
Rp.
3-5,
000
NO
TE:
Wom
en g
ener
ally
cho
ose
the
ANC
serv
ice
prov
ider
. M
en a
re in
volv
ed in
dec
idin
g w
ith w
omen
if se
ekin
g AN
C se
rvic
es c
osts
cas
h m
ore
than
Rp.
10,
000.

20Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.6 Benefi t and Value Perceptions for ANC Service Providers
ANC service providersmost used by the poor at 8 study sites: WOMEN's perception
100
62.5
72
46.67
93.390
70
95
100
95
100
20
100 100
74
100
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
Bidan kampung
TBA
Sando (TBA) Dukun beranak
TBA
Bidan Puskesmas Puskesmas Sando
TBA
Bidan Puskesmas Puskesmas
RURAL URBAN
rocSe
Value for cost score
most used by the poor at 8 study sites: MEN's perception
9094
72.570
100
84 82 8283.33
94
100
76.67
100
84
100
82
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
Bidan kampung
TBA
Sando (TBA) Dukun beranak
TBA
Bidan Puskesmas Puskesmas Puskesmas Bidan Puskesmas Puskesmas
RURAL URBAN
rocSe
Value for cost score
Notes:
Dukun beranak/paraji/bidan kampung/sando = traditional birth attendant
Puskesmas = Primary Health Centre
Bidan Puskesmas = trained midwife at Primary Health Centre, government employee

21Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.7 Proportion of votes for choice of provider for Childbirth Assistance Services
Women's view Men's view
76%
14%
8% 2%
Sando/Bidan Kampung/Paraji/Dukun Bayi Bidan desa/Polindes
Puskesmas Public hospital
64%
15%
18%
3%

22Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Tabl
e 3.
4. C
ost o
f Chi
ldbi
rth
Assis
tanc
e Se
rvic
es U
sed
by th
e Po
or a
t 8 S
tudy
Site
s
RURA
L SI
TES
PAM
ING
GIR
/ S.
Kalim
anta
nBA
JOPU
LAU
/ N
TBA
LAS
KOKO
N /
Mad
ura
KERT
AJA
YA/ W
.Jav
a
Mos
t use
dBi
dan
Kam
pung
(TBA
)
Rp.2
5,00
0 -5
0,00
0 +
Ric
e 2k
g +
2 co
conu
ts
Sand
o (T
BA)
Rp.2
5,00
0 -5
0,00
0 +
rice
2kg
+ 1
coco
nut.
Afte
r 3 d
ays p
ost b
irth
anot
her
Rp.2
0,00
0, ri
ce+
coco
nut
Duk
un (T
BA)
Rp.5
0,00
0
Para
ji (T
BA)
Rp.5
0,00
0 -1
00,0
00 +
20k
g ric
e
Com
pare
d to
oth
er
avai
labl
e ch
oice
bida
n de
sa
Rp.2
00,0
00-4
00,0
00
No
othe
r op
tion.
bida
n de
sa n
ever
ava
ilabl
e w
hen
need
ed
bida
n de
sa
Rp.1
50,0
00 -2
00,0
00
bida
n de
sa
Rp.3
00,0
00 -4
00,0
00 +
Rp.1
0,00
0 fo
r tra
nspo
rt
URB
AN
SIT
ES
AN
TARA
SARI
/ S.
Kalim
anta
nJA
TIBA
RU /
NTB
SIM
OKE
RTO
/ E.
Java
SOKL
AT /
W.J
ava
Mos
t use
dBi
dan
Kam
pung
(TBA
)
Rp.5
0,00
0 -2
00,0
00 +
rice
,
coco
nut,
suga
r
Duk
un (T
BA)
Rp.1
0,00
0 +
1kg
rice
bida
n de
sa
Ro.3
00,0
00 +
Rp.
20,0
00 fo
r
tran
spor
t
Para
ji (T
BA)
Rp.5
0,00
0 -1
00,0
00 o
r
Rp.5
0,00
0 +
5 k
g ric
e
Com
pare
d to
oth
er
avai
labl
e ch
oice
bida
n de
sa
Rp.2
50,0
00 -5
00,0
00
depe
ndin
g on
leng
th +
com
plex
ity o
f lab
or
bida
n de
sa
Rp.3
00,0
00 -4
00,0
00
Duk
un (T
BA)
Not
use
d an
y m
ore
bida
n de
sa
Rp.3
00,0
00 -4
00,0
00
NO
TE: A
ccor
ding
to m
en, t
he h
usba
nd c
hoos
es th
e se
rvic
e pr
ovid
er, f
or c
hild
birt
h.
Acc
ordi
ng to
wom
en, h
usba
nd a
nd w
ife d
ecid
e to
geth
er.

23Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.8 Satisfaction Ratings for Childbirth Assistance Providers
Paminggir
Bajopulau
Alas Kokon
Kertajaya
Antasari
Jatibaru
Simokerto
Soklat
Legends Women's Ratings Men's Ratings
Public hospital
Bidan Desa
Posyandu
TBA
Puskesmas
Score 0 = No satisfaction at all Score 100 = Full satisfaction
50 0 100 10 70 90
45 75 0 100 50
50 30 3 70 100
100 0 45 50 75
0 100 50 25
0 100 50
0 100 50
0 100 50 75

24Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.9 Benefi t and Value Perceptions for Childbirth Assistance Providers
most used by the poor at 8 study sites: WOMEN's Perception
97
90
75
98 97.5
91.67
82
68.75
100 100 100 98 100 100
54
68.7
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
Bidan kampung Sando (TBA) Dukun beranak Paraji Bidan kampung Sando (TBA) Bidan Puskesmas Paraji
RURAL URBAN
rocSe
Value for cost score
most used by the poor at 8 study sites: MEN's perception
96.67
8588
9590
84
76
96.67100 100 100 100 100
84
90
100
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
Bidan kampung Sando (TBA) Dukun beranak Paraji Bidan kampung Puskesmas Puskesmas Paraji
RURAL URBAN
rocSe
e Value for cost score
Notes:
Dukun beranak/paraji/bidan kampung/sando = traditional birth attendant
Puskesmas = Primary Health Centre
Bidan desa = trained midwife, resident in village, government employee
Bidan Puskesmas = trained midwife at Primary Health Centre, government employee

25Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.10 Proportion of votes for provider of Infant Health Care Services (2M – 5Y)
Women's view Men's view
9%
8%
3%
17%
35%
23%
2% 4%
Sando/Bidan Kampung/Paraji/Dukun Bayi Sando/Dukun berobat
Dokter (Private practice) Pustu
Bidan desa/Polindes Puskesmas
Mantri (Paramedic) Public hospital
Posyandu
4%5%
6%
17%
21%
36%
7%2% 3%
Figure 3.11 Proportion of votes for provider of Infant Health Care Services (0 - 2M)
Women's view Men's view
12%
2%
5%
17%
33%
30%
0.5%
Sando/Bidan Kampung/Paraji/Dukun Bayi Sando/Dukun berobat
Dokter (Private practice) Pustu
Bidan desa/Polindes Puskesmas
Public hospital Posyandu
20%
2%
17%
28%
30%
1% 2%

26Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Tabl
e 3.
5. C
osts
of O
ne-t
ime
Use
of C
urat
ive
Care
Ser
vice
s Mos
t Use
d by
the
Poor
for T
heir
Child
ren
unde
r Fiv
e
RURA
L SI
TES
PUSK
ESM
ASPU
STU
TBA
/Tra
ditio
nal H
eale
rbi
dan
desa
PAM
ING
GIR
S.K
alim
anta
nRp
.5,0
00Rp
.5,0
00 -1
0,00
0
(if P
USTU
pro
vide
rs n
ot a
vaila
ble,
as
happ
ens f
requ
ently
)
BAJO
PULA
U
NTB
Free
(dur
ing
fi rst
44
days
the
baby
is
deem
ed to
bel
ong
to th
e TB
A w
ho
deliv
ered
it)
If TB
A ca
nnot
cur
e, n
ext c
hoic
e is
Man
tri
at R
p.20
-50,
000
ALAS
KOKO
N M
adur
aRp
.15,
000
(if n
ot c
ured
then
seco
nd c
hoic
e M
antr
i or K
yai
at R
p.25
000-
50,0
00)
KERT
AJA
YA W
.Java
Rp.1
5,00
0 +
Rp.
10,0
00 fo
r
tran
spor
t
URB
AN
SIT
ES
ANTA
SARI
S.K
alim
anta
nRp
.3,0
00
JATI
BARU
/ N
TBRp
.3,0
00 +
Rp.
3,00
0 fo
r tra
nspo
rt
SIM
OKE
RTO
E.Ja
vaRp
.5,0
00 +
Rp.
6,00
0
for t
rans
port
SOKL
AT
W.Ja
va
Rp.2
,500
(if t
his d
oes n
ot c
ure
then
next
to B
idan
- at
Rp.
25-3
0,00
0.
If Bi
dan
can’
t hel
p th
en p
rivat
e
doct
or a
t Rp.
40-7
0,00
0 +
cos
t of
med
icin
es)

27Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.12 Benefi t and Value Perceptions for Curative Services for Infants (0-2 months)
Met and Value for Cost forInfant (0 - 2 months old) Health Care Service Providers most used
by the poor at 8 study sites
92.5
76.67
64
85 8590
66
76
90
100
94
50
92.596.67
60
72
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
Puskesmaspembantu
Sando Bidan desa Bidan Puskesmas Puskesmas Puskesmas Puskesmaspembantu
Puskesmas
RURAL URBAN
rocSe
Value for cost score
Infant (0 - 2 months old) Health Care Service Providers most used bythe poor at 8 study sites
90
100
80
90
100
84
94 92.5
70
100
92.590
100
84
100 100
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
Puskesmaspembantu
Sando Bidan desa Puskesmas Puskesmas Puskesmas Puskesmaspembantu
Puskesmas
RURAL URBAN
rocSe
Value for cost score
Notes:
Pustu (Puskesmas pembantu) = Sub-primary Health Centre (outreach facility)
Puskesmas = Primary Health Centre
Bidan desa = trained midwife, resident in village, government employee
Bidan Puskesmas = trained midwife at Primary Health Centre, government employee
Sando = Traditional healer

28Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.13 Satisfaction Ratings for Curative Care Providers for Infants (0-2 months)
Paminggir
Bajo Pulau
Alas Kokon
Kertajaya
Antasari
Jatibaru
Simokerto
Soklat
Legends Women’s Rating Men’s Rating
Public hospital
Bidan Desa
Posyandu
Pustu
TBA
Puskesmas
Private doctor
Mantri
Trad. healer
Score 0 = No satisfaction at all Score 100 = Full satisfaction
0
0
0
10 0
0
0
0

29Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.14 Benefi t and Value Perceptions for Water Supply Option Used
Met and Value for Cost forWater Services most used by the poor at 8 study sites
100
8590
93.390
78
92 93.396.67
100 100 100
63.3
100
85
100
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
River Vendor from otherisland
Protected publicdugwell
Public handpump Buy PDAM waterfrom neighbor
Unprotected dugwell Vendor resellingPDAM water
Unprotected publicdugwell
RURAL URBAN
rocS
e
Value for cost score
xpectation Met and Value for Cost forWater Services most used by the poor at 8 study sites
90 90
100
83
100
81.67
93.3
100
93.3
100 100
86
100 100
91.67
100
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
River Vendor from otherisland
Protected publicdugwell
Public handpump Buy PDAM waterfrom neighbor
Unprotected dugwell Vendor resellingPDAM water
Unprotected publicdugwell
RURAL URBAN
rocS
e
Value for cost score

30Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.15 Satisfaction ratings for water supply options
Paminggir
Bajo Pulou
Alas Kokon
Kertajaya
Antasari
Jatibaru
Simokerto
Soklat
Legend Women’s Rating Men’s Rating
River
Dug welll
Dugwell with pump (sanyo)
Borewell with pump (sanyo)
Hand pump
Utility water resold by neighborVendor-sold PDAM / borewell water
Score 0 = No satisfaction at allScore 100 = Full satisfaction
0 63 90 1 00
0 100
0 25
0 10 100
0 100
0 100
0 50 75 100
0 85 100
40
10050
8050
50
60
50
30
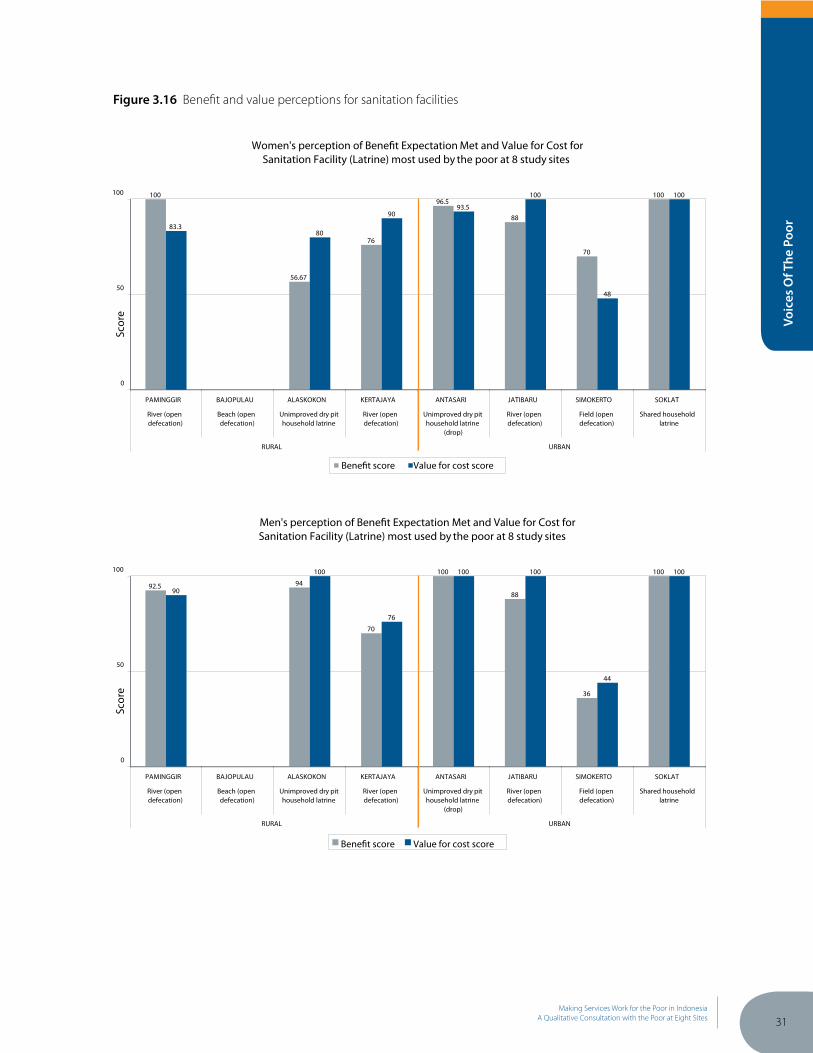
31Making Services Work for the Poor in Indonesia
A Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.16 Benefi t and value perceptions for sanitation facilities
Met and Value for Cost forSanitation Facility (Latrine) most used by the poor at 8 study sites
100
56.67
76
96.5
88
70
100
83.380
9093.5
100
48
100
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
River (opendefecation)
Beach (opendefecation)
Unimproved dry pithousehold latrine
River (opendefecation)
Unimproved dry pithousehold latrine
(drop)
River (opendefecation)
Field (opendefecation)
Shared householdlatrine
RURAL URBAN
rocSe
Value for cost score
Sanitation Facility (Latrine) most used by the poor at 8 study sites
92.5 94
70
100
88
36
100
90
100
76
100 100
44
100
0
50
100
PAMINGGIR BAJOPULAU ALASKOKON KERTAJAYA ANTASARI JATIBARU SIMOKERTO SOKLAT
River (opendefecation)
Beach (opendefecation)
Unimproved dry pithousehold latrine
River (opendefecation)
Unimproved dry pithousehold latrine
(drop)
River (opendefecation)
Field (opendefecation)
Shared householdlatrine
RURAL URBAN
rocSe
Value for cost score

32Making Services Work for the Poor in IndonesiaA Qualitative Consultation with the Poor at Eight Sites
Voic
es O
f The
Poo
r
Figure 3.17 Satisfaction ratings for sanitation facilities
Paminggir
Bajo Pulou
Alas Kokon
Kertajaya
Antasari
Jatibaru
Simokerto
Soklat
Legend Women’s Rating Men’s Rating
Shared household latrine
Public toilet
Open pit latrine at home
Open defecation in backyard
River/sea
Pond
Simple pits, away from home
Score 0 = No satisfaction at allScore 100 = Full satisfaction
0 80 90 100
0 100
0 25
0 5 100
0 10 25 100
0 50 75 100
0 50 75 100
0 30 85 100
25
10050
45 50
25
50 75




























![BBC VOICES RECORDINGS€¦ · BBC Voices Recordings) ) ) ) ‘’ -”) ” (‘)) ) ) *) , , , , ] , ,](https://img.dokumen.tips/doc/110x75/5f8978dc43c248099e03dd05/bbc-voices-recordings-bbc-voices-recordings-aa-a-a-a-.jpg)
