Embed Size (px)
Citation preview

Vitamin D and CalciumNew Research – New Recommendations?
will begin at the top of the hourAudio for today’s presentation is being broadcast over your computer speakers, so be sure they are turned on and the
volume is upToday’s presentation in handout form can be
downloaded from: http://bit.ly/handout-11-05-15 (type in your browser)
NUTRI-BITES®
Webinar Series

November 5, 2015
Presenter:
Robert P. Heaney, MD, FACP, FASNJohn A. Creighton University Professor
& Professor of MedicineCreighton University Osteoporosis Research Center
Moderator:James M. Rippe, MD – Leading cardiologist, Founder and Director,
Rippe Lifestyle Institute
Approved for 1 CPE (Level 2) by the Commission on Dietetic Registration, credentialing agency for the Academy of Nutrition and Dietetics.
NUTRI-BITES®
Webinar Series
Vitamin D and CalciumNew Research - New Recommendations?

ConAgra Foods Science Institute With a mission of:
Promoting dietary and related choices affecting wellness
by linking evidence-based understanding
with practice

Webinar logistics CEUs – a link to obtain your Continuing Education Credit
certificate will be emailed and available on this webinar’s page at www.ConAgraFoodsScienceInstitute.com within 2 days.
A recording of today’s webinar, slides as a PDF, and summary PowerPoint will be available to download within 2 days at: www.ConAgraFoodsScienceInstitute.com
The presenter will answer questions at the end of this webinar. Please submit questions by using the ‘Chat’ dialogue box on your computer screen.

Today’s Faculty
Robert P. Heaney, MD, FACP, FASNJohn A. Creighton University Professor
& Professor of MedicineCreighton University Osteoporosis Research Center
Moderator:James M. Rippe, MD – Leading cardiologist, Founder and Director, Rippe Lifestyle Institute

Learning Objectives Recall the principal roles vitamin D and calcium serve in the
human body Describe how nutrients – and vitamin D in particular – are
like preventive maintenance of a complex machine Describe some of the consequences of inadequate intake of
each nutrient List the principal sources of vitamin D and calcium Recall the optimal intake/input of each nutrient, with
emphasis on differing needs at different life stages
NUTRI-BITES®
Webinar SeriesVitamin D and Calcium: New Research-New Recommendations

VITAMIN D AND CALCIUM
New Research –New Recommendations ?
Robert P. Heaney, MD, FACP, FASN
Creighton University Osteoporosis Research Center

Two fundamentally different ways of approaching nutrients:
micro-nutrients macro-nutrients

Two fundamentally different ways of approaching nutrients:
micro-nutrients macro-nutrients
needed for the proper running of the biochemical apparatus of all living cells; think: preventive maintenance

Two fundamentally different ways of approaching nutrients:
micro-nutrients macro-nutrients
needed for body structures;think: extracellular fluid
volume or bone mass
needed for the proper running of the biochemical apparatus of all living cells; think: preventive maintenance

Two fundamentally different ways of approaching nutrients:
micro-nutrients macro-nutrients
Vitamin D

Two fundamentally different ways of approaching nutrients:
micro-nutrients macro-nutrients
Calcium
Vitamin D
Two fundamentally different ways of approaching nutrients:
micro-nutrients macro-nutrientsexcept for the classical
deficiency diseases: don’t expect miracles don’t look for dramatic
disease cures

Two fundamentally different ways of approaching nutrients
micro-nutrients macro-nutrients
look instead for longer life expectancy better functional life

CU ORC
TWO FRAMEWORKS:The nutrient requirement
Risk assessment Physiology

CU ORC
THE NUTRIENT REQUIREMENT:
Two Frameworks
Risk assessment Physiology
Avoidance of some disease
outcome

CU ORC
THE NUTRIENT REQUIREMENT:Two Frameworks
Risk assessment Physiology
Avoidance of some disease
outcome
Support of cell function

The physiological approach must inevitably produce a higher estimate of the requirement than the disease avoidance approach:
the questions are different the goals are different the endpoints are different

CU ORC
THREE PHYSIOLOGICAL CRITERIA an example of a physiologically based
requirement would be an intake that: calls for the least day-to-day adaptation or
compensation

CU ORC
THREE PHYSIOLOGICAL CRITERIA examples of a physiologically based
requirement would be : an intake that calls for the least day-to-day
adaptation or compensation an intake to which the human body has been
adapted by natural selection

CU ORC
THREE PHYSIOLOGICAL CRITERIA examples of a physiologically based
requirement would be : an intake that calls for the least day-to-day
adaptation or compensation an intake to which the human body has been
adapted by natural selection an intake that is needed to support one or
more essential physiological functions

Vitamin D

CU ORC
RECOMMENDATION DISCORDANCE
Ages 51–70: IOM 2010 Endo Soc 2010 Am Ger Soc 2014 GrassrootsHealth

CU ORC
RECOMMENDATION DISCORDANCE
Ages 51–70: IOM 2010 Endo Soc 2010 Am Ger Soc 2014 GrassrootsHealth
Daily Input (IU)RDA/AI TUIL
600 4,0001,500–2,000 10,000
4,000 --4,000–5,000 ––

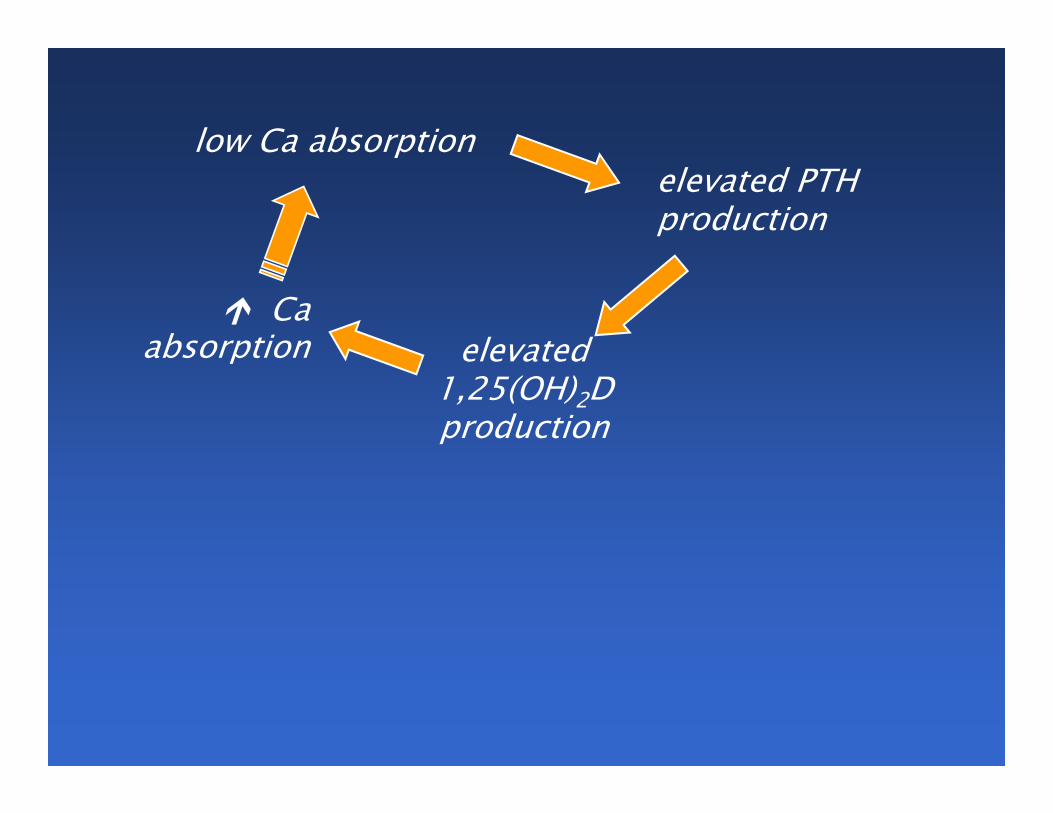
Minimizing the need for compensation

low Ca absorption

low Ca absorptionelevated PTH production

low Ca absorptionelevated PTH production
elevated1,25(OH)2Dproduction

low Ca absorptionelevated PTH production
elevated1,25(OH)2Dproduction
Ca absorption
low Ca absorptionelevated PTH production
elevated1,25(OH)2Dproduction
Ca absorption

low Ca absorptionelevated PTH production
elevated1,25(OH)2Dproduction
Ca absorption
Elevated PTH is an index of Ca and/or vitamin D inadequacy

low Ca absorptionelevated PTH production
elevated1,25(OH)2Dproduction
Ca absorption
Elevated PTH is an index of Ca and/or vitamin D inadequacy
The rise in PTH doesn’t cause us to consume more Ca, but it does cause us to absorb more, thus tending to close the loop

CU ORC
THE SETPOINT CRITERION
Serum 25(OH)D (ng/mL)0 10 20 30 40 50 60
Seru
m P
TH (pg
/mL)
0
20
40
60
80
100
120
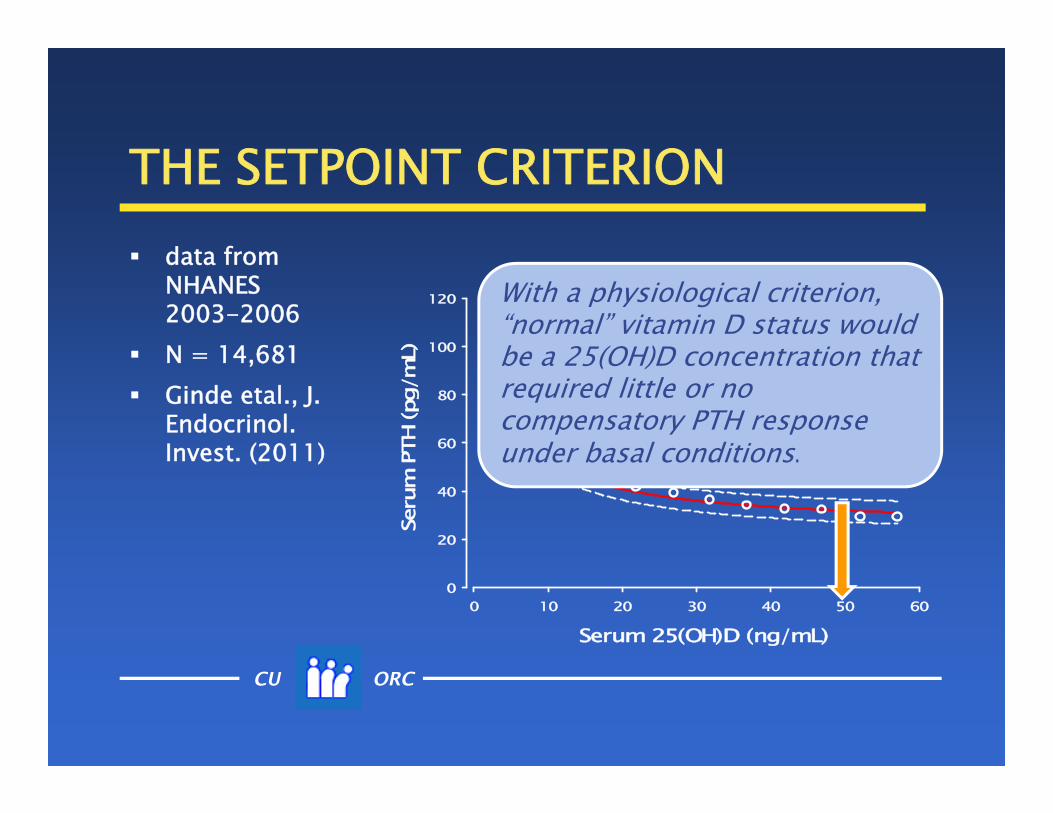
data from NHANES 2003-2006
N = 14,681 Ginde etal., J.
Endocrinol. Invest. (2011)

CU ORC
THE SETPOINT CRITERION
Serum 25(OH)D (ng/mL)0 10 20 30 40 50 60
Seru
m P
TH (pg
/mL)
0
20
40
60
80
100
120
data from NHANES 2003-2006
N = 14,681 Ginde etal., J.
Endocrinol. Invest. (2011)
CU ORC
THE SETPOINT CRITERION
Serum 25(OH)D (ng/mL)0 10 20 30 40 50 60
Seru
m P
TH (pg
/mL)
0
20
40
60
80
100
120 With a physiological criterion, “normal” vitamin D status would be a 25(OH)D concentration that required little or no compensatory PTH response under basal conditions.
data from NHANES 2003-2006
N = 14,681 Ginde etal., J.
Endocrinol. Invest. (2011)

Compensation is metabolically costly and often takes a toll in other organ systems.
Compensation is metabolically costly and often takes a toll in other organ systems.
Over the course of the evolution of human physiology, natural selection would have favored organisms that did not have to compensate for what the environment provided.

CU ORC
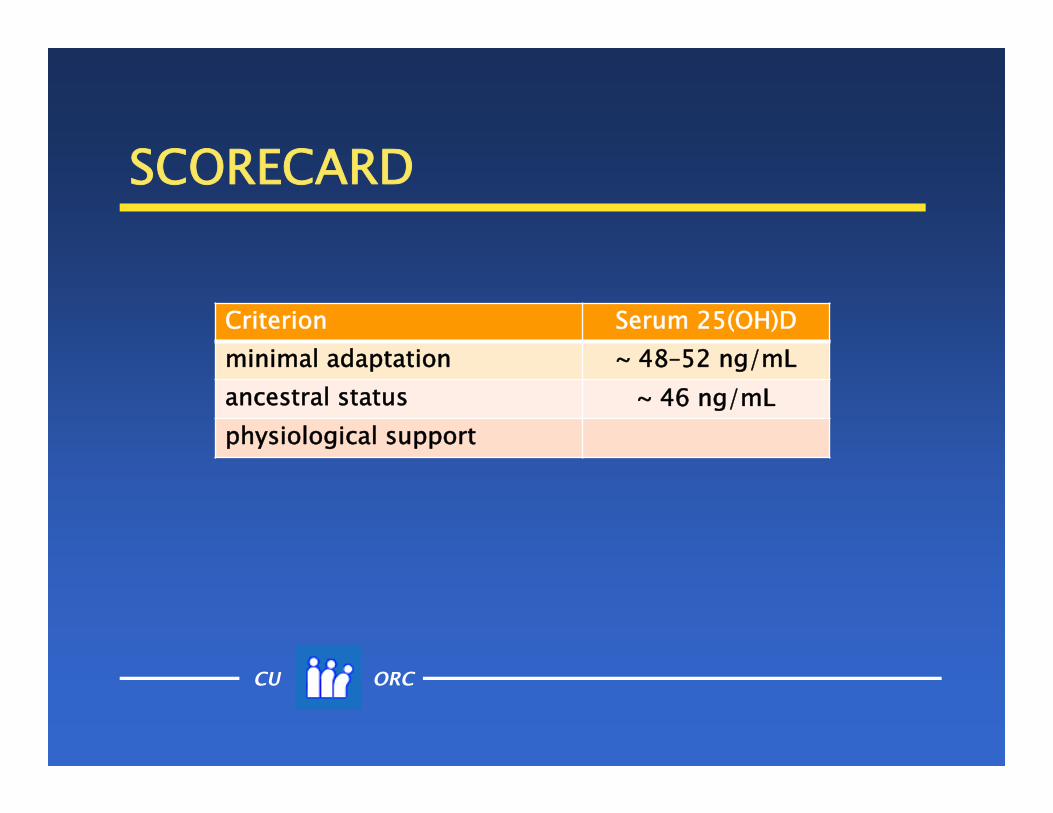
SCORECARD
Criterion Serum 25(OH)Dminimal adaptation ~ 48–52 ng/mLancestral statusphysiological support

Matching the ancestral intake

CU ORC
NATIVE AFRICANS* Masai
(pastoralists) Hadza (hunter-
gatherers)
* Luxwolda et al., BJN 2011
CU ORC
NATIVE AFRICANS* Masai (pastoralists) diet differs from the
ancestral, but latitude, skin pigmentation, and skin exposure are the same as ancestral
* Luxwolda et al., BJN 2011

CU ORC
NATIVE AFRICANS* Hadza (hunter-
gatherers) diet, latitude, skin
exposure, and skin pigmentation are all ancestral
they have been called “the last of the first”
* Luxwolda et al., BJN 2011

CU ORC
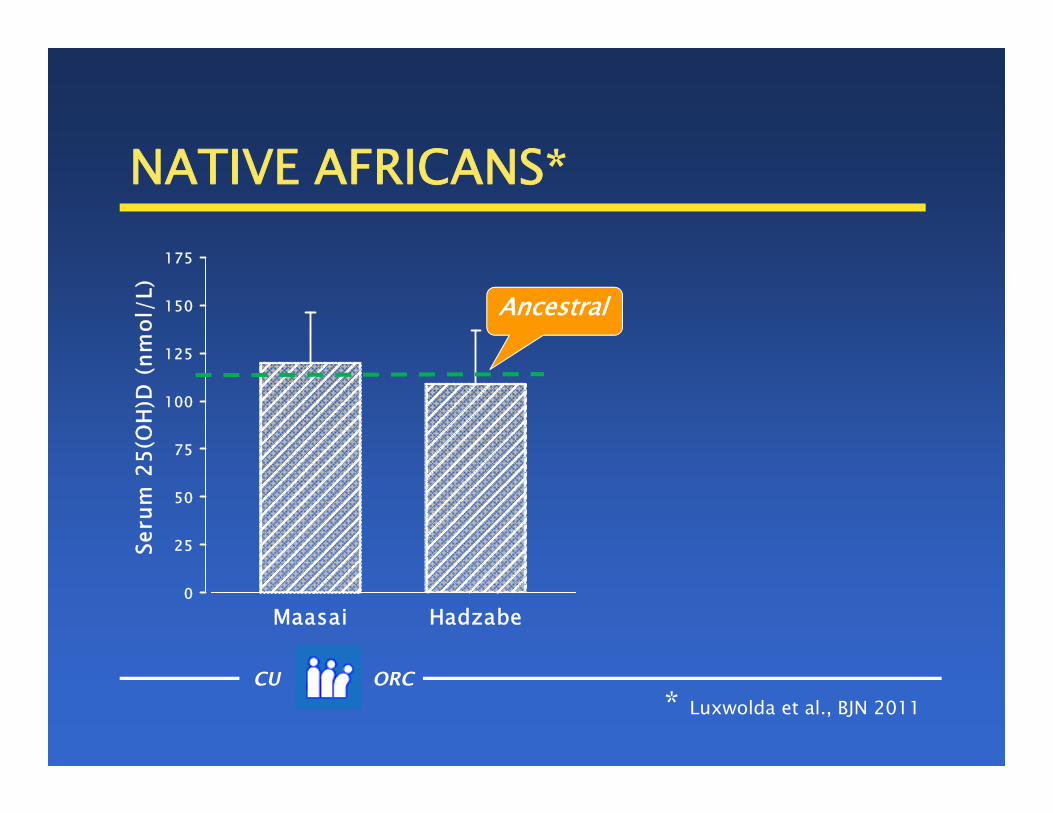
NATIVE AFRICANS*
Maasai Hadzabe
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
25
50
75
100
125
150
175
* Luxwolda et al., BJN 2011
CU ORC
NATIVE AFRICANS*
Maasai Hadzabe
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
25
50
75
100
125
150
175
* Luxwolda et al., BJN 2011
Ancestral
CU ORC
NATIVE AFRICANS*
Maasai Hadzabe
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
25
50
75
100
125
150
175
* Luxwolda et al., BJN 2011
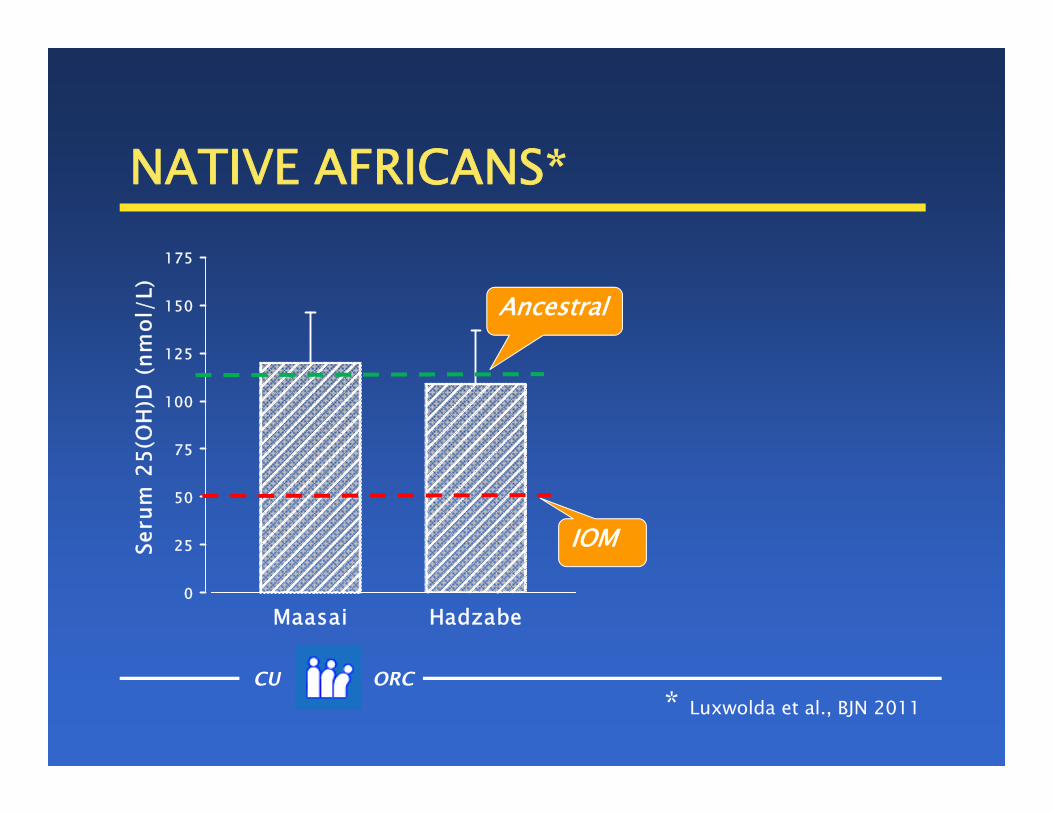
IOM
Ancestral

CU ORC
NATIVE AFRICANS*
Maasai Hadzabe
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
25
50
75
100
125
150
175
* Luxwolda et al., BJN 2011
IOM
Endocrine Society
Ancestral
CU ORC
SCORECARD
Criterion Serum 25(OH)Dminimal adaptation ~ 48–52 ng/mLancestral status ~ 46 ng/mLphysiological support

Just because ancestral humans averaged ~115 nmol/L doesn’t mean that modern humans need that much.

Just because ancestral humans averaged ~115 nmol/L doesn’t automatically mean that modern humans need that much.
But that’s the best starting point in determining the requirement, the burden of
proof should fall on those who say lower 25(OH)D values are adequate (and safe).
the question of adequacy must be: Will lower levels support critical physiological activities?
Supporting a critical physiological function

CU ORC
LACTATION FACTS human milk is capable of providing all the vitamin D
(cholecalciferol) an infant needs

CU ORC
LACTATION FACTS human milk is capable of providing all the vitamin D
(cholecalciferol) an infant needs but only if the mother has native vitamin D
(cholecalciferol) in her blood

CU ORC
LACTATION FACTS human milk is capable of providing all the vitamin D
(cholecalciferol) an infant needs but only if the mother has native vitamin D
(cholecalciferol) in her blood cholecalciferol crosses from the blood into the milk,
but 25(OH)D does not

CU ORC
LACTATION FACTS human milk is capable of providing all the vitamin D
(cholecalciferol) an infant needs but only if the mother has native vitamin D
(cholecalciferol) in her blood cholecalciferol crosses from the blood into the milk,
but 25(OH)D does not so maternal serum cholecalciferol is the key variable
CU ORC
LACTATION FACTS human milk is capable of providing all the vitamin D
(cholecalciferol) an infant needs but only if the mother has native vitamin D
(cholecalciferol) in her blood cholecalciferol crosses from the blood into the milk,
but 25(OH)D does not so serum cholecalciferol is the key variable its concentration begins to rise only after the hepatic
25-hydroxylase is approximately saturated, and that corresponds to a serum 25(OH)D above 100 nmol/L (40 ng/mL)

Serum Vitamin D3 (nmol/L)0 50 100 150 200 250
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
50
100
150
200
250
300
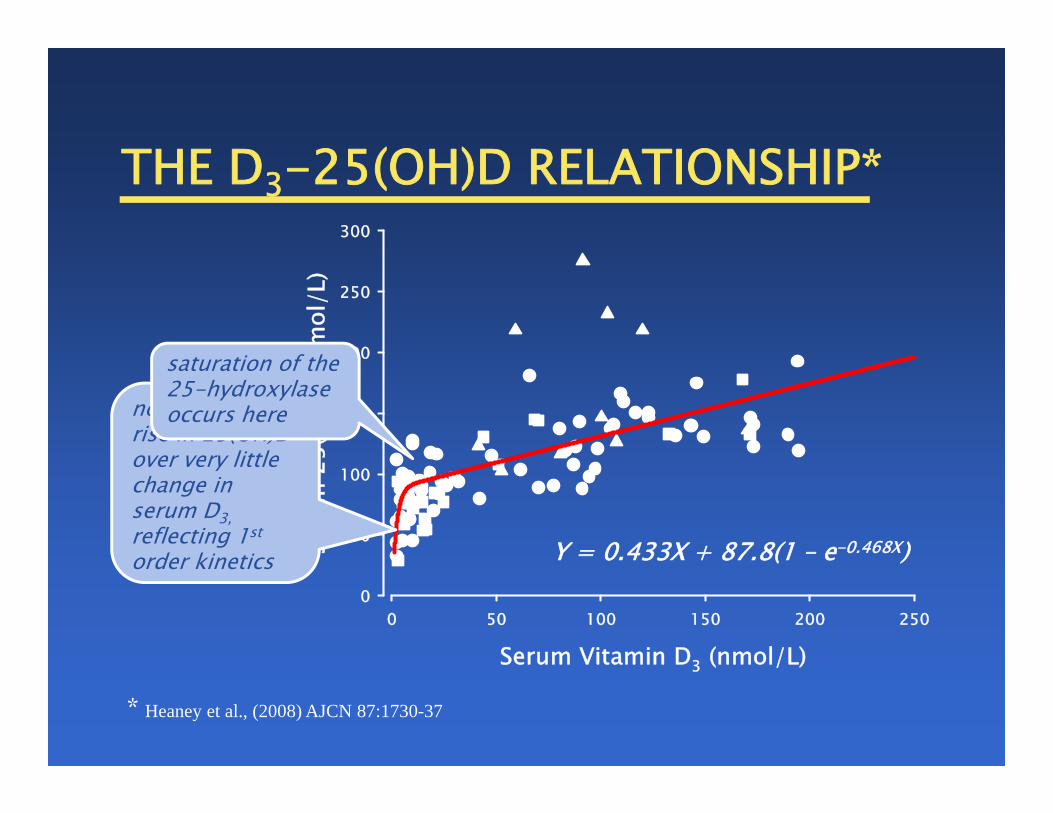
THE D3-25(OH)D RELATIONSHIP*
* Heaney et al., (2008) AJCN 87:1730-37
Y = 0.433X + 87.8(1 – e-0.468X)

Serum Vitamin D3 (nmol/L)0 50 100 150 200 250
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
50
100
150
200
250
300
THE D3-25(OH)D RELATIONSHIP*
* Heaney et al., (2008) AJCN 87:1730-37
Y = 0.433X + 87.8(1 – e-0.468X)
note the steep rise in 25(OH)D over very little change in serum D3,reflecting 1st
order kinetics
Serum Vitamin D3 (nmol/L)0 50 100 150 200 250
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
50
100
150
200
250
300
THE D3-25(OH)D RELATIONSHIP*
* Heaney et al., (2008) AJCN 87:1730-37
Y = 0.433X + 87.8(1 – e-0.468X)
note the steep rise in 25(OH)D over very little change in serum D3,reflecting 1st
order kinetics
saturation of the 25-hydroxylase occurs here

THE D3-25(OH)D RELATIONSHIP*
* Heaney et al., (2008) AJCN 87:1730-37
Y = 0.433X + 87.8(1 – e-0.468X)
Serum Vitamin D3 (nmol/L)0 50 100 150 200 250
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
50
100
150
200
250
300
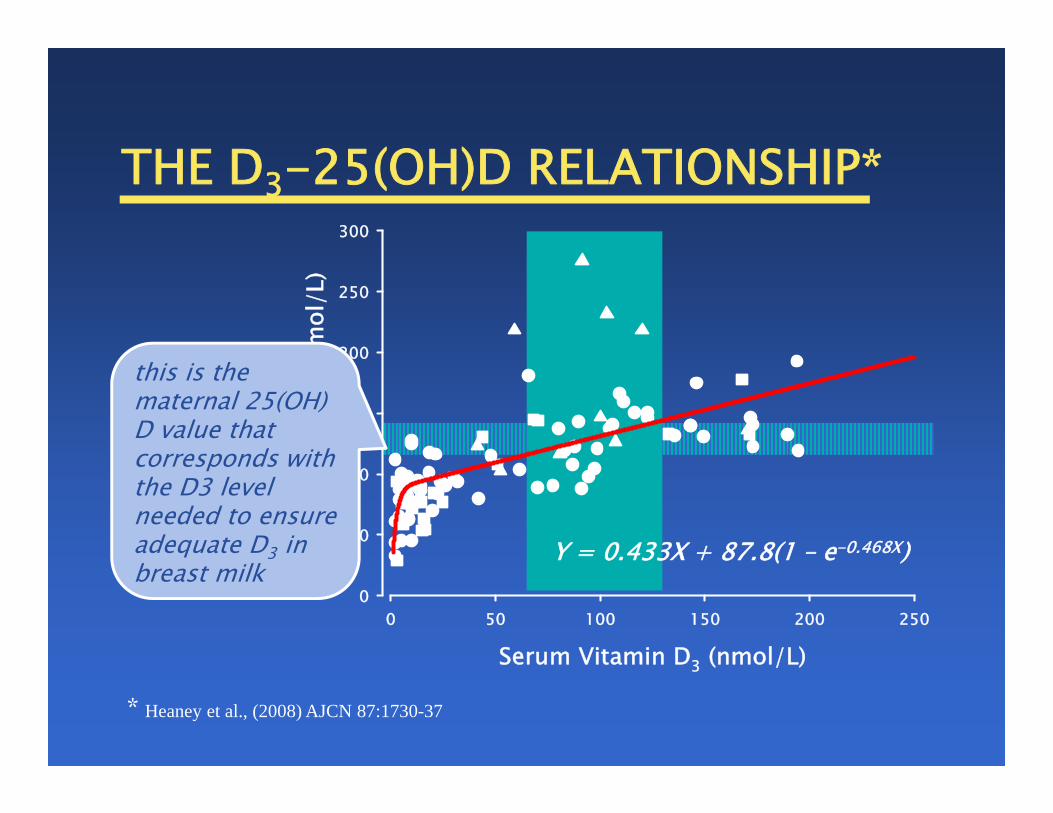
THE D3-25(OH)D RELATIONSHIP*
* Heaney et al., (2008) AJCN 87:1730-37
Y = 0.433X + 87.8(1 – e-0.468X)
Serum Vitamin D3 (nmol/L)0 50 100 150 200 250
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
50
100
150
200
250
300
this is the maternal 25(OH) D value that corresponds with the D3 level needed to ensure adequate D3 in breast milk

Serum Vitamin D3 (nmol/L)
0 20 40 60 80 100
Seru
m 2
5(O
H)D
(nm
ol/L
)
0
50
100
150
200
250
300
RELATIONSHIP OF D3 & 25D
this is the IOM value for adequacy; note that the D3concentration is too low to permit any transfer into milk
CU ORC
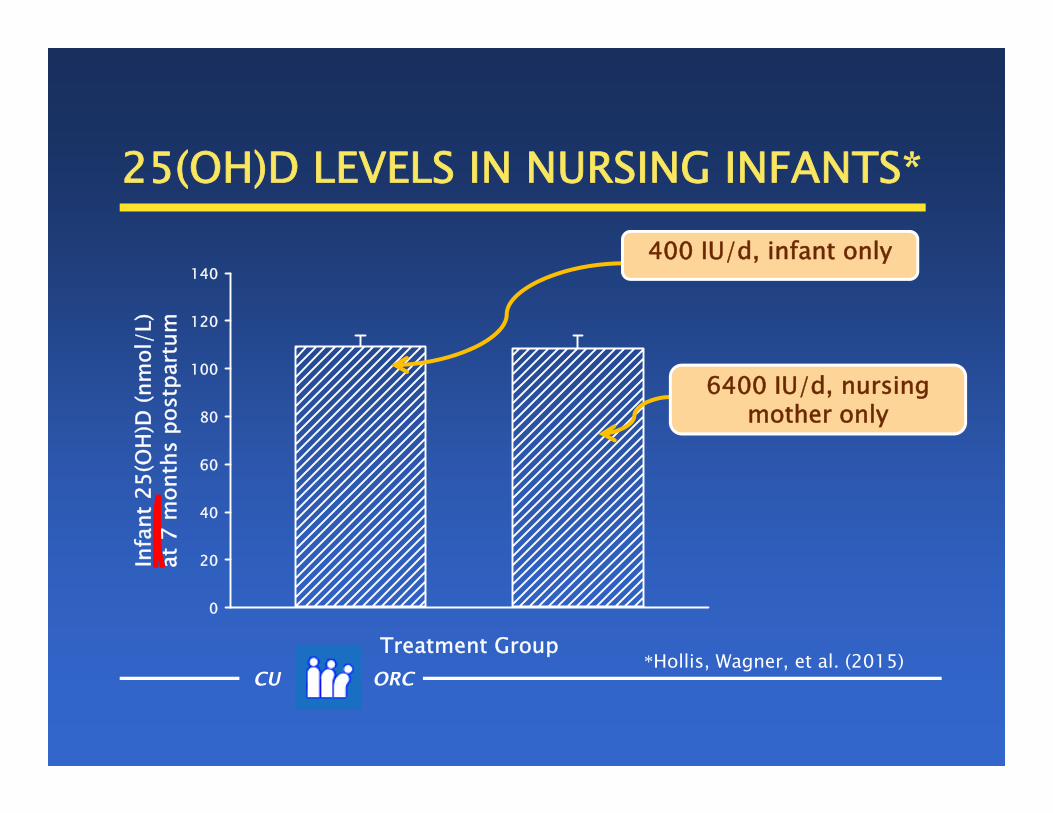
25(OH)D LEVELS IN NURSING INFANTS*
Treatment Group
Infa
nt 2
5(O
H)D
(nm
ol/L
) a
t 7 m
onth
s po
stpa
rtum
0
20
40
60
80
100
120
140400 IU/d, infant only
6400 IU/d, nursing mother only
*Hollis, Wagner, et al. (2015)

CU ORC
SUMMARY vitamin D remains a nutrient of concern
in pregnant women in babies in utero in infants
low perinatal vitamin D status leads to several late-life consequences
serum 25(OH)D levels should be maintained at 40 ng/mL or above

CU ORC
SCORECARD
Criterion Serum 25(OH)Dminimal adaptation ~ 48–52 ng/mLancestral status ~ 46 ng/mLphysiological support ~ 48–60 ng/mL

Calcium
Calcium&
Bone Health

Bone Health and OsteoporosisA Report of the Surgeon General
“Calcium has been singled out as a majorpublic health concern today because it is critically important to bone health and the average American consumes levels of calcium that are far below the amount recommended for optimal bone health.”
October 14, 2004
Bone Health and OsteoporosisA Report of the Surgeon General
“Calcium has been singled out as a majorpublic health concern today because it is critically important to bone health and the average American consumes levels of calcium that are far below the amount recommended for optimal bone health.”
October 14, 2004

Bone Health and OsteoporosisA Report of the Surgeon General
“Calcium has been singled out as a majorpublic health concern today because it is critically important to bone health and the average American consumes levels of calcium that are far below the amount recommended for optimal bone health.”
October 14, 2004
Bone Health and OsteoporosisA Report of the Surgeon General
“Calcium has been singled out as a majorpublic health concern today because it is critically important to bone health and the average American consumes levels of calcium that are far below the amount recommended for optimal bone health.”
October 14, 2004

CU ORC
CONSENSUS CONFERENCES
three NIH Consensus Development Conferences had specifically recommended Ca supplements: 1984 – Osteoporosis 1994 – Optimal Ca Intake 2000 – Osteoporosis

CU ORC
DANGERS WITH CALCIUM?
haven’t there been some papers suggesting increased CVD risk with Ca supplements?
Yes, but these papers have been thoroughly
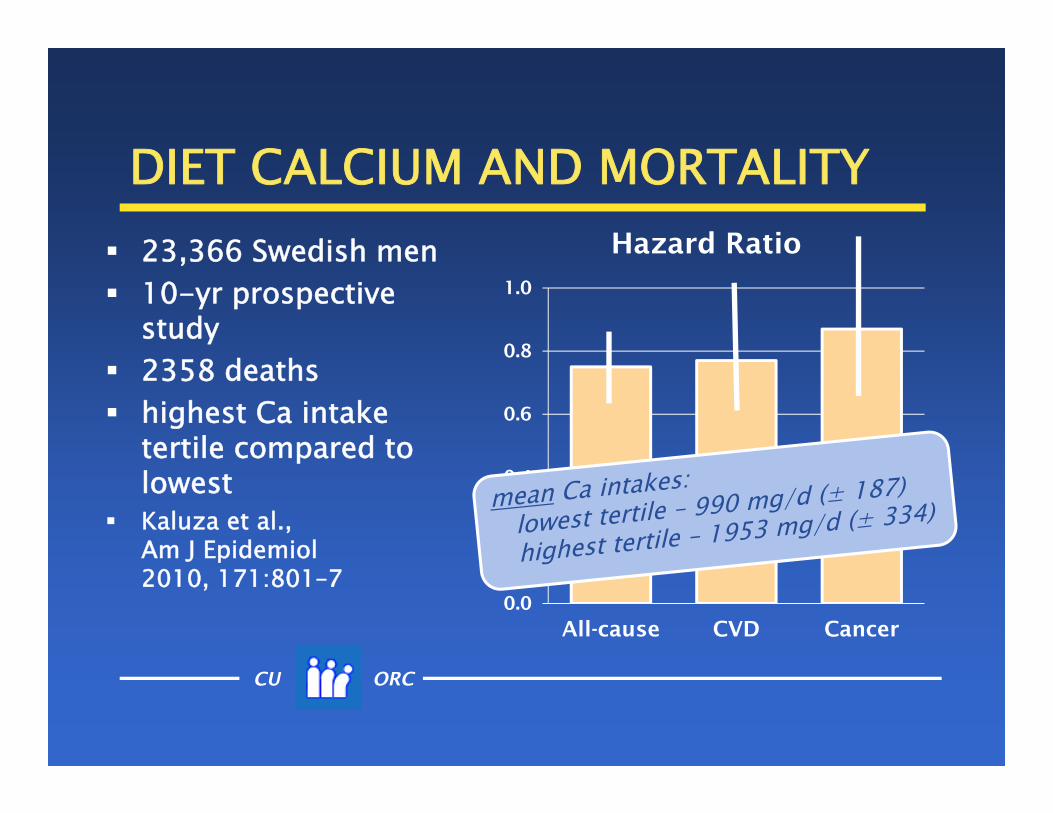
refuted and, as it turns out, high Ca intakes are actually associated with reduced all-cause mortality

CU ORC
DIET CALCIUM AND MORTALITY 23,366 Swedish men 10-yr prospective
study 2358 deaths highest Ca intake
tertile compared to lowest
Kaluza et al., Am J Epidemiol2010, 171:801–7

CU ORC
DIET CALCIUM AND MORTALITY 23,366 Swedish men 10-yr prospective
study 2358 deaths highest Ca intake
tertile compared to lowest
Kaluza et al., Am J Epidemiol2010, 171:801–7
0.0
0.2
0.4
0.6
0.8
1.0
All-cause CVD Cancer
Hazard Ratio
CU ORC
DIET CALCIUM AND MORTALITY 23,366 Swedish men 10-yr prospective
study 2358 deaths highest Ca intake
tertile compared to lowest
Kaluza et al., Am J Epidemiol2010, 171:801–7
0.0
0.2
0.4
0.6
0.8
1.0
All-cause CVD Cancer
Hazard Ratio

CU ORC
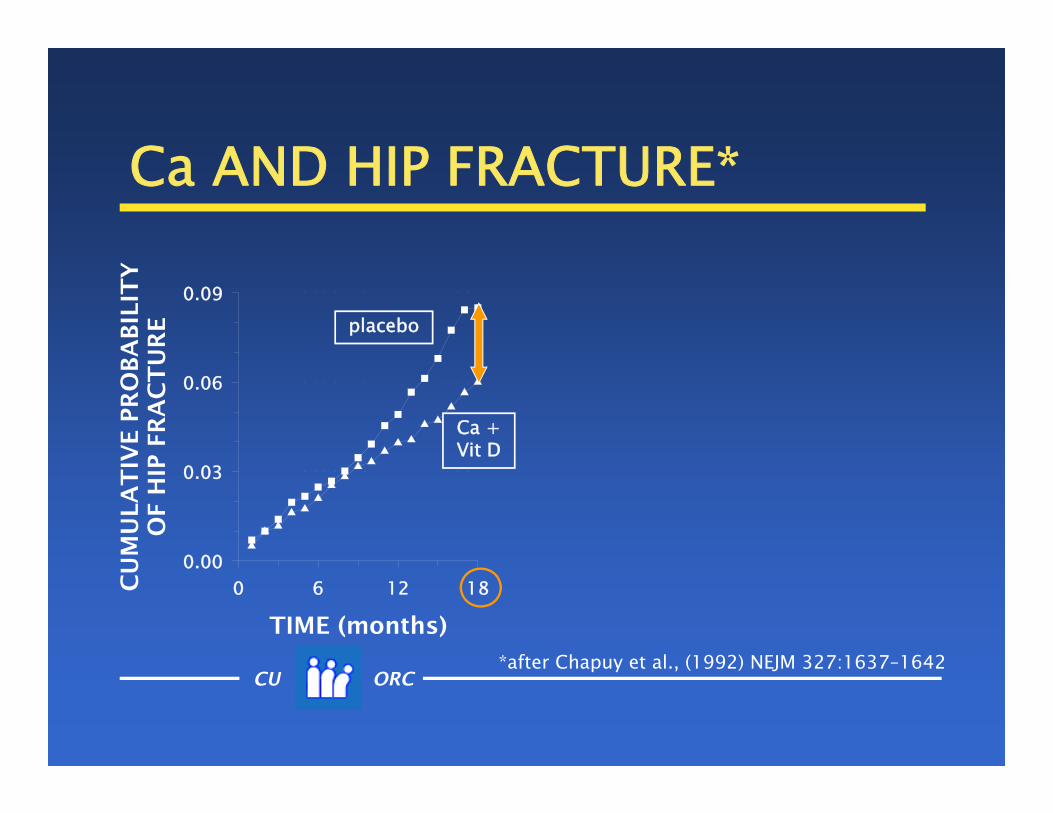
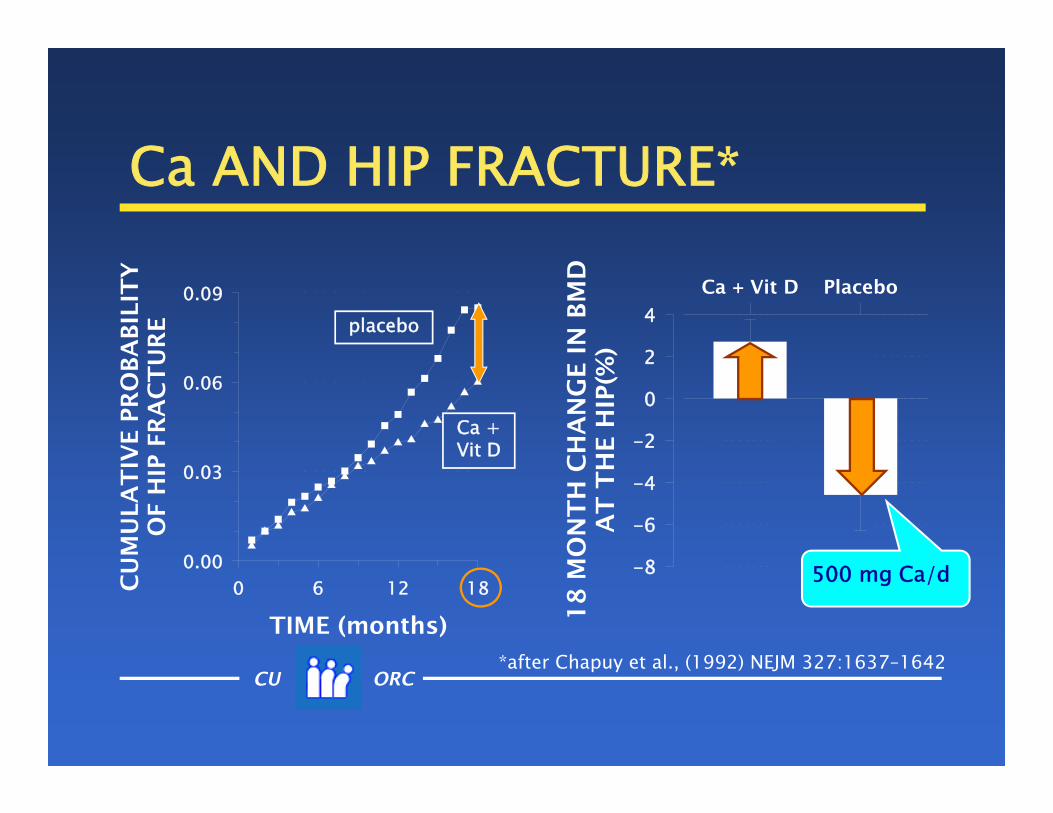
Ca AND HIP FRACTURE*
*after Chapuy et al., (1992) NEJM 327:1637–1642
TIME (months)
0 6 12 18CU
MU
LA
TIV
E P
RO
BA
BIL
ITY
OF H
IP F
RA
CT
UR
E
0.00
0.03
0.06
0.09placebo
Ca + Vit D
CU ORC
Ca AND HIP FRACTURE*
*after Chapuy et al., (1992) NEJM 327:1637–1642
TIME (months)
0 6 12 18CU
MU
LA
TIV
E P
RO
BA
BIL
ITY
OF H
IP F
RA
CT
UR
E
0.00
0.03
0.06
0.09placebo
Ca + Vit D
CU ORC
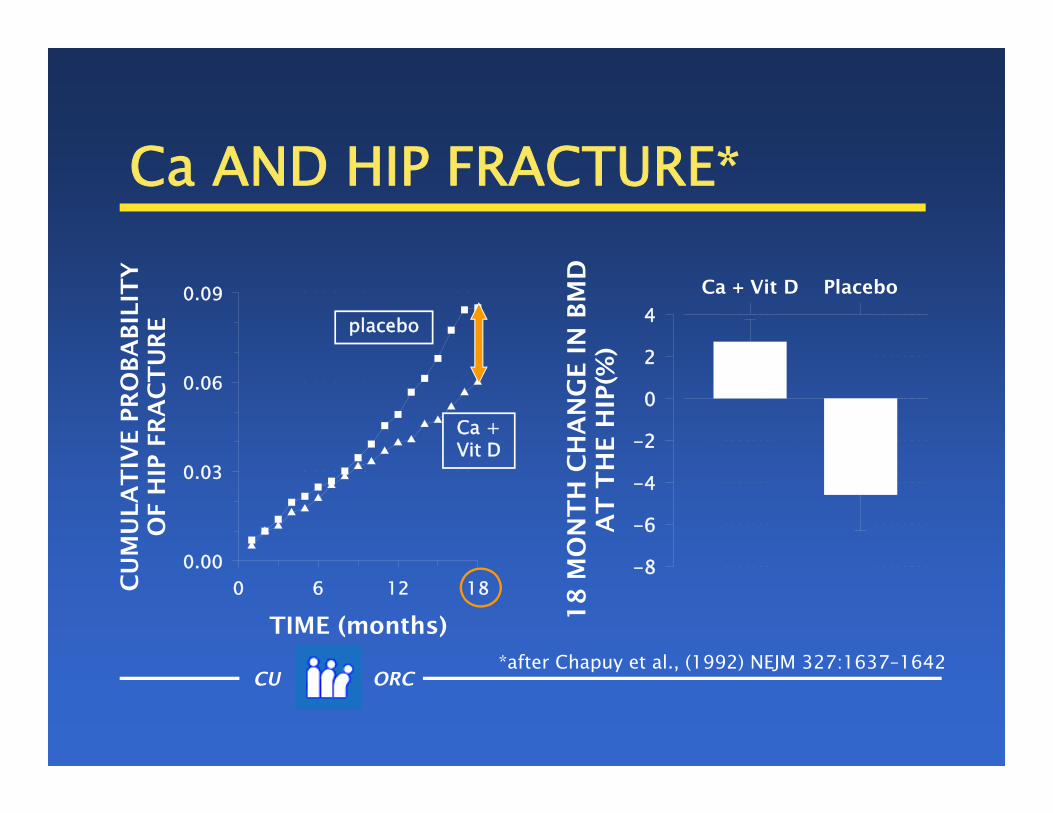
Ca AND HIP FRACTURE*
*after Chapuy et al., (1992) NEJM 327:1637–1642
Ca + Vit D Placebo
18
MO
NT
H C
HA
NG
E I
N B
MD
AT
TH
E H
IP(%
)
-8
-6
-4
-2
0
2
4
TIME (months)
0 6 12 18CU
MU
LA
TIV
E P
RO
BA
BIL
ITY
OF H
IP F
RA
CT
UR
E
0.00
0.03
0.06
0.09placebo
Ca + Vit D
CU ORC
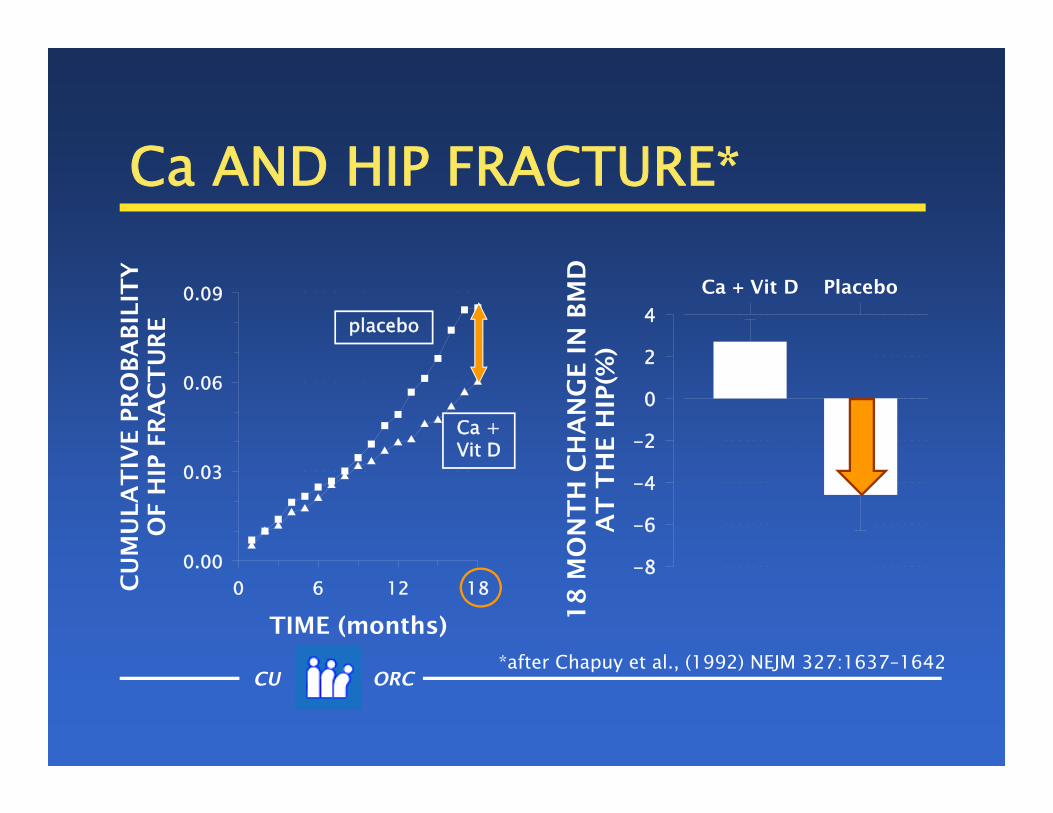
Ca AND HIP FRACTURE*
*after Chapuy et al., (1992) NEJM 327:1637–1642
Ca + Vit D Placebo
18
MO
NT
H C
HA
NG
E I
N B
MD
AT
TH
E H
IP(%
)
-8
-6
-4
-2
0
2
4
TIME (months)
0 6 12 18CU
MU
LA
TIV
E P
RO
BA
BIL
ITY
OF H
IP F
RA
CT
UR
E
0.00
0.03
0.06
0.09placebo
Ca + Vit D

CU ORC
Ca AND HIP FRACTURE*
*after Chapuy et al., (1992) NEJM 327:1637–1642
Ca + Vit D Placebo
18
MO
NT
H C
HA
NG
E I
N B
MD
AT
TH
E H
IP(%
)
-8
-6
-4
-2
0
2
4
TIME (months)
0 6 12 18CU
MU
LA
TIV
E P
RO
BA
BIL
ITY
OF H
IP F
RA
CT
UR
E
0.00
0.03
0.06
0.09placebo
Ca + Vit D
CU ORC
Ca AND HIP FRACTURE*
*after Chapuy et al., (1992) NEJM 327:1637–1642
Ca + Vit D Placebo
18
MO
NT
H C
HA
NG
E I
N B
MD
AT
TH
E H
IP(%
)
-8
-6
-4
-2
0
2
4
TIME (months)
0 6 12 18CU
MU
LA
TIV
E P
RO
BA
BIL
ITY
OF H
IP F
RA
CT
UR
E
0.00
0.03
0.06
0.09
500 mg Ca/d
placebo
Ca + Vit D

CU ORC
Ca AND HIP FRACTURE*
*after Chapuy et al., (1992) NEJM 327:1637–1642
Ca + Vit D Placebo
18
MO
NT
H C
HA
NG
E I
N B
MD
AT
TH
E H
IP(%
)
-8
-6
-4
-2
0
2
4
TIME (months)
0 6 12 18CU
MU
LA
TIV
E P
RO
BA
BIL
ITY
OF H
IP F
RA
CT
UR
E
0.00
0.03
0.06
0.09
1700 mg Ca/d
placebo
Ca + Vit D

CU ORC
CALCIUM, VIT D, & FRACTURE
TIME ON STUDY (months)
0 10 20 30FIRS
T N
ON
-VER
TEBR
AL F
RACT
URE
(Cum
ulat
ive
inci
denc
e –
%)0
2
4
6
8
10
12
14
*Dawson-Hughes et al., NEJM 1997:337:670-6
Ca + Vit D
placebo
176 men; 213women
ages > 65treatment:
Ca 500 mg + Vit D 700 iu

CU ORC
CALCIUM, VIT D, & FRACTURE
TIME ON STUDY (months)
0 10 20 30FIRS
T N
ON
-VER
TEBR
AL F
RACT
URE
(Cum
ulat
ive
inci
denc
e –
%)0
2
4
6
8
10
12
14
*Dawson-Hughes et al., NEJM 1997:337:670-6
Ca + Vit D
placebo –55%
176 men; 213women
ages > 65treatment:
Ca 500 mg + Vit D 700 iu

What is the mechanism by which calcium & vitamin D reduce fractures in these
studies?
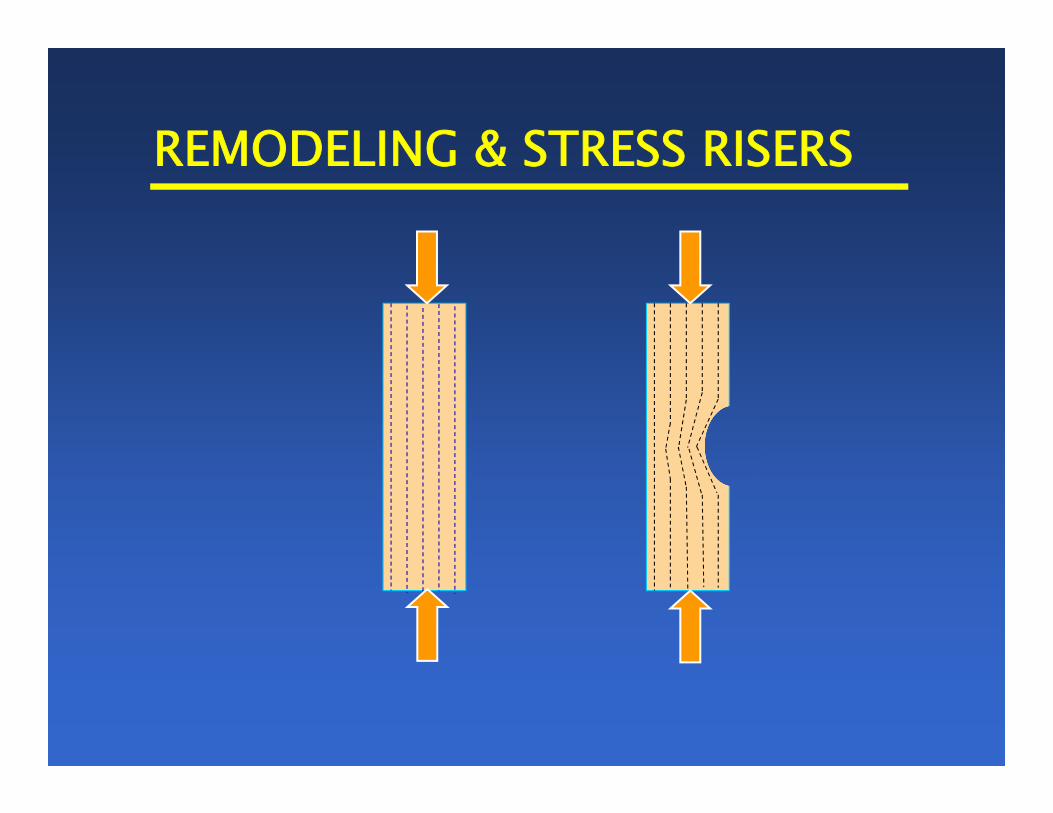
high bone remodeling activity makes bones fragile

high bone remodeling activity makes bones fragile
Calcium & vitamin D reduce fractures in these studies by
reducing the elevated rates of remodeling typically found in
post-menopausal women
CU ORC
RESTORING PRE-MENOPAUSAL RATES
the importance of restoring premenopausal rates of remodeling is shown by the fact that potent bisphosphonates produce the same reduction in fracture risk in patients who experience no change in BMD as in those who show an increase in BMD
CU ORC
RESTORING PRE-MENOPAUSAL RATES
the importance of restoring premenopausal rates of remodeling is shown by the fact that potent bisphosphonates produce the same reduction in fracture risk in patients who experience no change in BMD as in those who show an increase in BMD
the bone-sparing effect of bisphosphonates is of minor importance, despite the fact that bone sparing is generally considered the basis for their effect

CU ORC
RESTORING PRE-MENOPAUSAL RATES
the importance of restoring premenopausal rates of remodeling is shown by the fact that potent bisphosphonates produce the same reduction in fracture risk in patients who experience no change in BMD as in those who show an increase in BMD
the bone-sparing effect of bisphosphonates is of minor importance, despite the fact that bone sparing is generally considered the basis for their effect

REMODELING & STRESS RISERS
REMODELING & STRESS RISERS

REMODELING & STRESS RISERS
region of increased stress

REMODELING & FRAGILITY

REMODELING & FRAGILITY

REMODELING & FRAGILITY
CU ORC
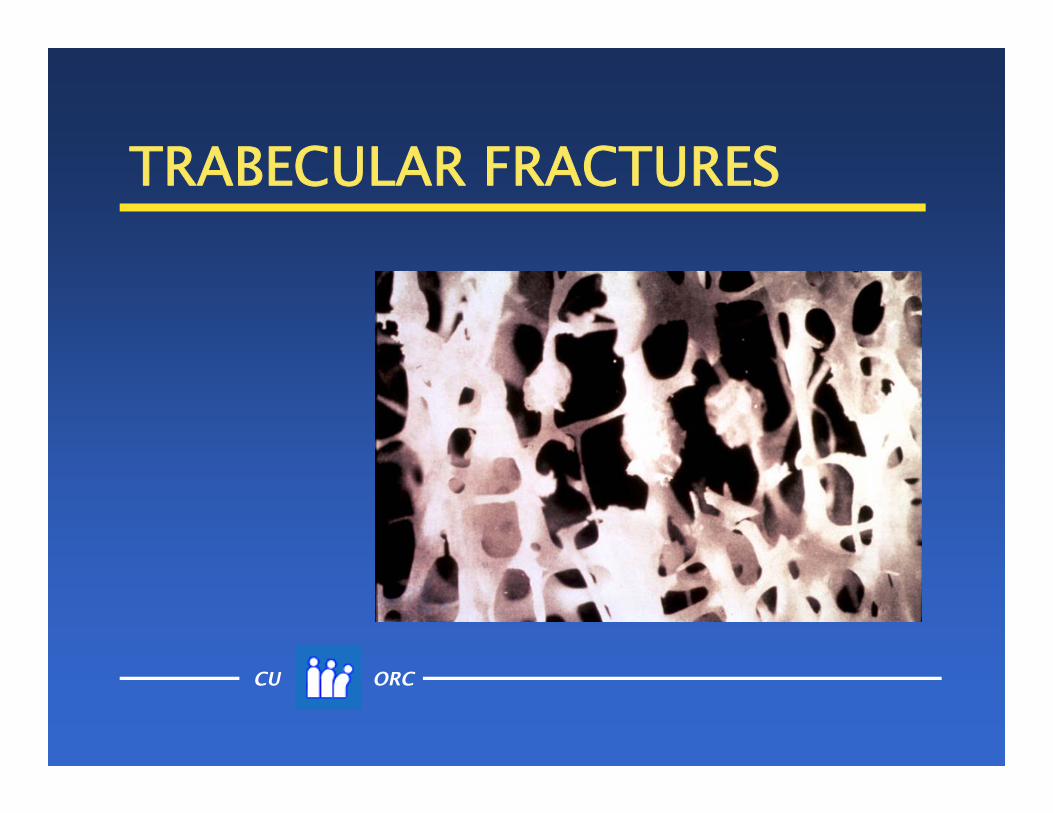
TRABECULAR FRACTURES

CU ORC
TRABECULAR FRACTURES

CU ORC
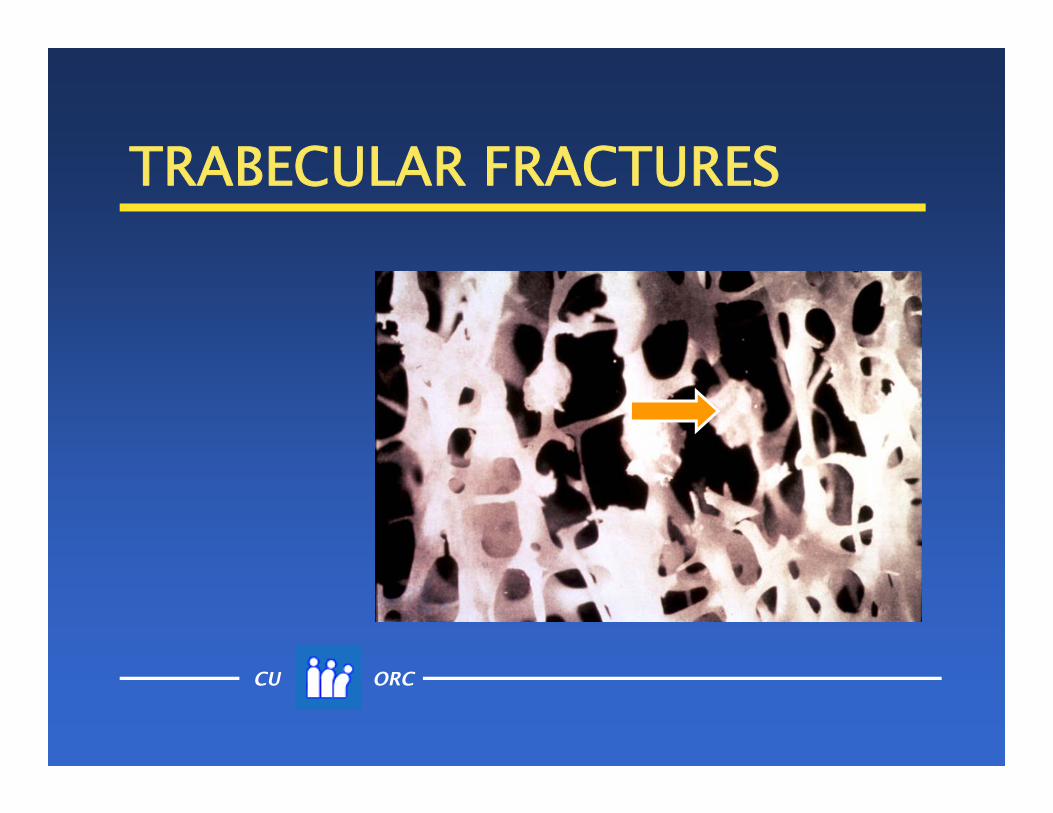
TRABECULAR FRACTURES
CU ORC
TRABECULAR FRACTURES

CU ORC
TRABECULAR FRACTURES
Healed or healing micro-fractures are painless. They can greatly reduce trabecular bone strength.

CU ORC
REMODELING REDUCERS nutrients
Ca (with vitamin D) endocrines
estrogen or estrogen agonists (e.g., genistein)
pharmaceuticals bisphosphonates RANK ligand antagonists & other resorption
inhibitors
CU ORC
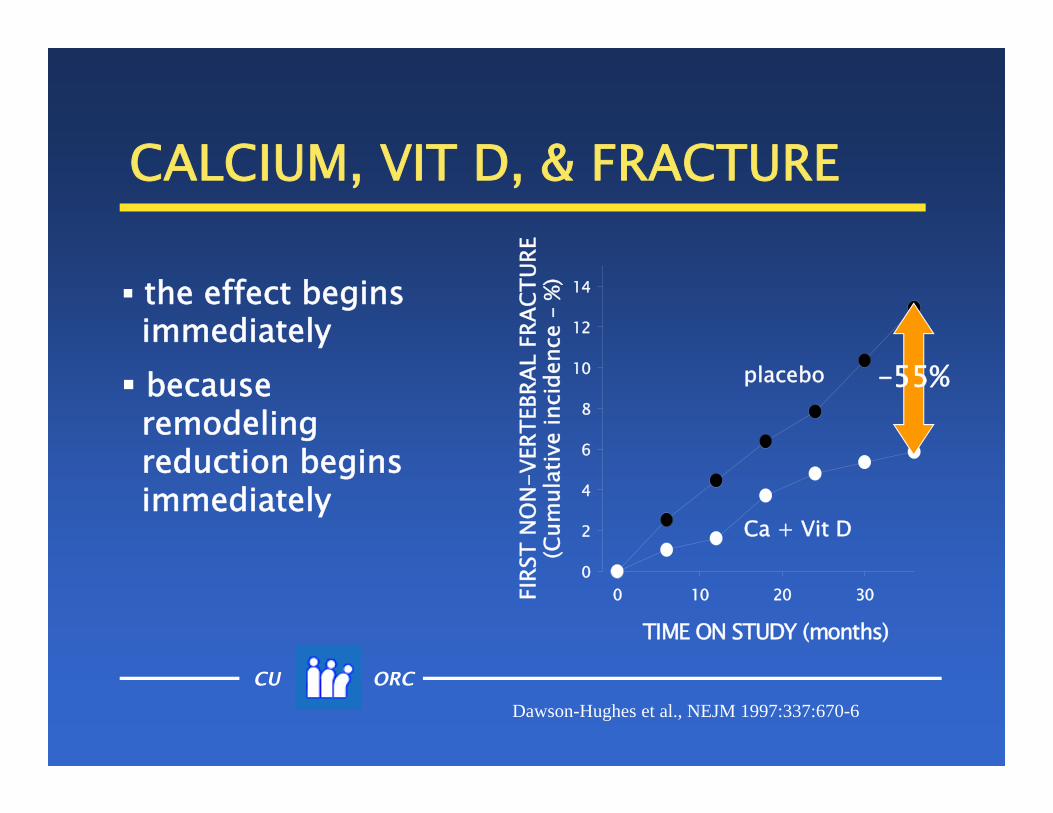
CALCIUM, VIT D, & FRACTURE
TIME ON STUDY (months)
0 10 20 30FIRS
T N
ON
-VER
TEBR
AL F
RACT
URE
(Cum
ulat
ive
inci
denc
e –
%)0
2
4
6
8
10
12
14
Dawson-Hughes et al., NEJM 1997:337:670-6
Ca + Vit D
placebo –55%
the effect beginsimmediately because
remodelingreduction beginsimmediately

CU ORC
CALCIUM, VIT D, & FRACTURE
TIME ON STUDY (months)
0 10 20 30FIRS
T N
ON
-VER
TEBR
AL F
RACT
URE
(Cum
ulat
ive
inci
denc
e –
%)0
2
4
6
8
10
12
14
Dawson-Hughes et al., NEJM 1997:337:670-6
Ca + Vit D
placebo –55%
the effect beginsimmediately because
remodelingreduction beginsimmediately

CU ORC
CALCIUM, VIT D, & FRACTURE
TIME ON STUDY (months)
0 10 20 30FIRS
T N
ON
-VER
TEBR
AL F
RACT
URE
(Cum
ulat
ive
inci
denc
e –
%)0
2
4
6
8
10
12
14
Dawson-Hughes et al., NEJM 1997:337:670-6
Ca + Vit D
placebo –55%
the effect beginsimmediately because
remodelingreduction beginsimmediately

CU ORC
SUMMARY – VITAMIN D vitamin D is essential for adequate
functioning of virtually all body systems inadequate vitamin D status predisposes
to various chronic diseases optimal status is achieved when serum
25(OH)D is between 40 and 60 ng/mL this requires an all-source input of
~5000 IU/d

SUMMARY – CALCIUM
Calcium is still important in 2015 optimal intake : 1200–1800 mg/d
preferably from dairy bone protection is due largely to
reduction of excess bone remodeling

CU ORC
Take away messages. . . .
Most Americans have inadequate intakes of both vitamin D and Ca.
Foods are the best sources for the needed Ca
But vitamin D needs can best be met by a combination of sun exposure and supplements

CU ORC
ADDITIONAL RESOURCES Vitamin D:
Baggerly C. et al. (2015) Sunlight & Vitamin D: Necessary for Public Health J Am Coll Nutr
Heaney RP & Armas LAG (2015) Quantifying the Vitamin D Economy. Nutr Rev
Calcium: Surgeon General’s Report: Bone Health &
Osteoporosis (2004) Heaney RP (2003) Is the paradigm shifting? Bone

Thank you . . .
Questions?

Based on this webinar the participant should be able to: Recall the principal roles vitamin D and calcium serve in the
human body Describe how nutrients – and vitamin D in particular – are
like preventive maintenance of a complex machine Describe some of the consequences of inadequate intake of
each nutrient List the principal sources of vitamin D and calcium Recall the optimal intake/input of each nutrient, with
emphasis on differing needs at different life stages
NUTRI-BITES®
Webinar SeriesVitamin D and Calcium: New Research-New Recommendations

ConAgra Foods Science Institute Nutri-Bites® Webinar details
A link to obtain your Continuing Education Credit certificate will be emailed within 2 days
Today’s webinar will be available to download within 2 days at: www.ConAgraFoodsScienceInstitute.com
For CPE information: [email protected]
Recent CEU webinars archived at the ConAgra Foods Science Institute website: Towards a Sustainable Food Supply: Myths and Realities Setting the Record Straight on Cholesterol, Saturated Fat, and Heart Disease Risk Nutrition Support for the Bariatric Patient Critical Evaluation of Nutrition Research Functional Foods: Phytochemicals – Hidden Nutrition Gems Sodium: Too much, too little or just right?

Dietary Supplements:Basics, Beliefs and Benefits
Johanna Dwyer, D.Sc., R.D.Professor of Medicine and Community Health
Tufts University School of Medicine and Professor of Nutrition
Friedman School of Nutrition Science and PolicyDate: February 4, 2016
2-3 pm EST/1-2 pm CST
www.ConAgraFoodsScienceInstitute.com
NextConAgra Foods Science Institute Nutri-Bites® Webinar

How are we doing?
Stay on the line for a brief survey about today’s ConAgra Foods Science Institute Nutri-Bites® webinar:
Thank you!
Vitamin D and Calcium: New Research-New Recommendations





























