Embed Size (px)
Citation preview

T e c h n i c a l R e p o R T s
744 VOLUME 17 | NUMBER 6 | JUNE 2011 naTuRe medicine
Transplant rejection involves a coordinated attack of the innate and the adaptive immune systems of the host. To investigate this dynamic process and the contributions of both donor and host cells, we developed an ear skin graft model suitable for intravital imaging. We found that donor dermal dendritic cells (DCs) migrated rapidly from the graft and were replaced by host CD11b+ mononuclear cells. The infiltrating host cells captured donor antigen, reached the draining lymph node and cross-primed graft-reactive CD8+ T cells. Furthermore, we defined the mechanisms by which host T cells target graft cells. We found that primed T cells entered the graft from the surrounding tissue and localized selectively at the dermis-epidermis junction. Later, CD8+ T cells disseminated throughout the graft and many became arrested. These results provide insights into the antigen presentation pathway and the stepwise progression of CD8+ T cell activity, thereby offering a framework for evaluating how immunotherapy might abrogate the key steps in allograft rejection.
Transplantation of solid organs triggers a complex immune reac-tion, comprising an inflammatory component subsequent to the surgery and ischemia-reperfusion process as well as an adaptive immune response1–3. During this process, the graft tissue is the site of dynamic cellular exchanges, in which donor cells leave while multiple subsets of recipient immune cells invade the graft. Central to the rejection of allografts is the activation of recipient CD4+ and CD8+ T cells by both donor and recipient DCs4–6. It has been pro-posed that donor DCs may promote acute rejection (through the direct pathway of antigen presentation), whereas recipient DCs may also contribute to chronic rejection through an indirect path-way1,7,8. Crucial aspects of each pathway of T cell activation remain to be elucidated. The ability of specific donor DC subsets to reach the draining lymph node (dLN) and to activate alloreactive T cells is unclear. The mechanism underlying the transfer of donor anti-gen from graft to host DCs with respect to an indirect antigen presentation pathway remains unknown. Donor cells that migrate to the dLN and subsequently die may provide a source of antigen
for indirect presentation6,9. This mechanism may be less relevant at later time points when the majority of migratory donor cells have already left the graft. Alternatively, recipient antigen-presenting cells (APCs) that infiltrate the graft may acquire antigen locally and subse-quently migrate to the dLN3. This scenario has, however, never been formally shown to occur after transplantation.
For both the direct and indirect pathways of T cell activation, the dLN has been shown to be the primary site for priming10–13. Nonetheless, there are data supporting direct activation of alloreac-tive T cells within the graft14–16. Finally, although CD8+ T cells are considered to have a major role in graft rejection17, we do not fully understand how they enter, disseminate and kill donor cells inside the graft.
Clearly, a better understanding of immune cell migration and of the interactions promoting transplant rejection is required to delineate new strategies for modulating the immune response to an alloge-neic transplant. To address these key subjects, we took advantage of two-photon imaging of a new model of ear skin transplantation. We provide evidence that migratory recipient APCs infiltrating the graft reach the dLN and cross-prime CD8+ T cells. We further show that tissue destruction is intrinsically linked to the spatiotemporal regulation of cytotoxic T lymphocyte (CTL) migration and activity in the graft.
RESULTSDonor Langerhans cells but not dermal DCs persist in the graftTo investigate immune cell migration and interactions regulating allo-graft rejection, we established an ear skin transplant model suitable for real-time in vivo two-photon imaging (Supplementary Fig. 1). Ear skin from C3H donor mice grafted onto C57BL/6 (B6) mice was rejected after 11–15 d. Rejection was delayed (rejection occurred 20–30 d after transplantation) in the context of male-to-female minor histo-compatibility antigen (mHA) mismatch (Supplementary Fig. 1).
We first investigated the persistence of donor DCs inside the graft. Ear skin from CD11c-YFP (expressing yellow fluorescent pro-tein (YFP) under the control of the mouse integrin α−x promoter (Itgax, also known as CD11c)) mice, backcrossed to a B6 or a C3H
Visualizing the innate and adaptive immune responses underlying allograft rejection by two-photon microscopySusanna Celli1,2, Matthew L Albert3,4 & Philippe Bousso1,2
1Institut Pasteur, Unité des Dynamiques des Réponses Immunes, Département d’Immunologie, Paris, France. 2Institut National de la Santé et de la Recherche Médicale (INSERM) U668, Paris, France. 3Institut Pasteur, Unité d’Immunobiologie des Cellules Dendritiques, Paris, France. 4INSERM U818, Paris, France. Correspondence should be addressed to P.B. ([email protected]).
Received 27 May 2010; accepted 19 January 2011; published online 15 May 2011; doi:10.1038/nm.2376
© 2
011
Nat
ure
Am
eric
a, In
c. A
ll ri
gh
ts r
eser
ved
.

T e c h n i c a l R e p o R T s
naTuRe medicine VOLUME 17 | NUMBER 6 | JUNE 2011 745
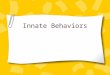
background, was transplanted onto B6 recipient mice. We did intravi-tal two-photon imaging of the grafts on day 6. As a control, we imaged the ear skin of a nontransplanted B6 CD11c-YFP mouse. In both iso-grafts (B6→B6) and allografts (C3H→B6), the network of Langerhans cells was well preserved, resembling that of nontransplanted skin (Fig. 1a). In contrast, the density of dermal DCs was drastically reduced in both isografts and allografts (Fig. 1a). Langerhans cells were largely immotile, whereas dermal DCs showed a small amount of crawling activity (Supplementary Video 1). Thus, dermal DCs but not Langerhans cells rapidly disappear from the graft in an anti-gen-independent manner; this possibly constitutes the first wave of APCs reaching the dLN. Later, in allografts (day 10), we noted altera-tions in the Langerhans cell network in the areas coinciding with the first macroscopic signs of tissue destruction, initially detected at the periphery and later at the center of the graft. These changes included decreased cell density and a less pronounced dendritic morphology, as seen in different pathological conditions18,19 (Fig. 1b).
To visualize donor DCs in the dLN, we imaged the lymph nodes of cyan fluorescent protein (CFP)-expressing mice draining a graft of CD11c-YFP mouse skin at day 1, 2 or 3 after the transplant. In the absence of antigenic mismatch, we occasionally observed live donor DCs (as suggested by dynamic shape changes, Supplementary Video 2). In contrast, fluorescent donor DCs detected in condi-tions of antigenic mismatch lacked membrane dynamics and had
the typical morphology of dead cells (Supplementary Video 2). This observation is consistent with a recent study that showed rapid killing of allogeneic DCs by natural killer cells in lymph nodes9. Additional mechanisms, including rapid T cell–mediated killing and short DC half-life, may also be involved. Thus, although we found that donor DCs could reach the lymph nodes, they did not remain alive for extended periods of time.
Dynamics of host CD11b+ cells infiltrating the graftAllograft transplantation results in a rapid infiltration of the graft by cells of the innate immune system. To clarify the dynam-ics of graft infiltration, we transplanted C3H or B6 mouse skin onto the ear of transgenic recipient mice ubiquitously express-ing GFP (B6 GFP). On day 3, the majority of infiltrating GFPhigh cells expressed CD11b (isograft: 75 ± 2.1%; allograft: 72 ± 7.2%) and comprised CD11b+Gr-1high neutrophils (isograft: 49% ± 18; allograft: 46% ± 24). They also included, to a lesser extent, CD11b+ Gr-1intermediate monocytes (isograft: 26 ± 14%; allograft: 26 ± 18%). By day 9, the relative contribution of monocytes and inflammatory DCs increased substantially in both the isograft and the allograft (Supplementary Fig. 2).
Using two-photon microscopy, we characterized the spatial organi-zation of the immune cell infiltrate in live, anesthetized mice. We used CD11c-YFP (C3H or B6) transgenic mice as donors, and we used the presence of Langerhans cells and collagen to identify the epider-mal and dermal skin layer, respectively. On day 3, we found GFP+ cells in the dermis (Fig. 2a,b) with a similar density for all the tested
ba Day 6
Control skin Isograft Allograft
Epidermis
Dermis
DC
den
sity
per
mm
2 500
300
100
LCDDC LC
DDC LCDDC
Day 10
Isograft Allograft
Center
Periphery
Isograft Allograft
LC d
ensi
type
r m
m2
800
Cente
r
Periph
ery
Cente
r
Periph
ery
400
0
Figure 1 Donor Langerhans cells but not dermal DCs persist in the graft. (a) Two-photon microscopic images of ear skin from C3H CD11c-YFP (allograft) or B6 CD11c-YFP (isograft) mice grafted onto B6 mice; images were obtained 6 d after transplant. We also imaged ear skin from nontransplanted B6 CD11c-YFP as a control. Representative images corresponding to the epidermal or the dermal layer of the skin are shown. Graphs depict the density of Langerhans cells and dermal DCs in the control skin, isograft and allograft. Cell densities were calculated from at least four images obtained in different experiments. (b) Representative images of the epidermal layer of the graft are shown for areas located in the center (top images) or at the periphery (bottom images) of the transplanted skin on day 10. Graphs show the density of Langerhans cells measured in different areas of isografts or allografts. Cell densities were calculated from at least four images obtained in different experiments. Scale bars, 20 µm. Error bars represent the means ± s.d.
a
Day 3y
x
xz0
Day 9
z = 0 µm z = 0 µm
z = 30 µmz = 30 µmDonor DC Collagen
LC Collagen
Recipient cells
30
b
c
Day 3 Day 9
Infil
trat
ing
cell
dens
ity p
er m
m2 Epidermis Dermis
B6m
HAM
HC B6m
HAM
HC
Day 3 Day 9
B6m
HAM
HC B6m
HAM
HC10,000
8,000
6,000
4,000
2,000
0
10,000
8,000
6,000
4,000
2,000
0
Day 3
Day 9
GFP+ cells Trajectories
Day 3 Day 9
Vel
ocity
(µm
per
min
) 16
12
8
4
0
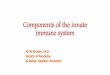
Figure 2 Spatiotemporal pattern of graft infiltration by host cells. (a) Visualization of the progressive infiltration of the graft by host cells. Two-photon microscopic images of ear skin from female C3H CD11c-YFP (allograft), female B6 CD11c-YFP (isograft), or male B6 CD11c-YFP (mHA-mismatched graft) mice grafted onto female B6 GFP or CFP transgenic recipients. We imaged grafts on days 3 and 9. The characteristic morphology of Langerhans cells (LC) and the presence of collagen were used to identify the epidermal and dermal layer of the skin, respectively. Representative images of the epidermis (top) and dermis (bottom) of a mHA mismatched graft. Scale bars, 50 µm. (b) For the various graft combinations tested, the densities of infiltrating GFP+ cells were quantified in the epidermal and dermal layers. Error bars represent the means ± s.d. (c) Representative images (left) and trajectories (right) of GFP+ infiltrating cells in the dermis of a mHA-mismatched graft on days 3 and 9. Scale bars, 20 µm. The graph shows the velocity of recipient infiltrating cells on days 3 and 9 after transplant. Each dot represents an individual cell. Results are representative of three independent experiments.
© 2
011
Nat
ure
Am
eric
a, In
c. A
ll ri
gh
ts r
eser
ved
.

T e c h n i c a l R e p o R T s
746 VOLUME 17 | NUMBER 6 | JUNE 2011 naTuRe medicine
Primary transplant onto B6 GFP
Retransplant onto B6 WTC3H
dLN??
GFP+ cells
GFP+ cells CD8+ T cells
a b
RetransplantedB2m–/– skindraining LN
Retransplanted B2m–/– mOVA skin
draining LN
RetransplantedB2m–/– mOVA skin
nondraining LN
CD
8
CFSE
3 18 1
B2m–/– mOVAor B2m–/–
Primary transplantonto B6 WT
Retransplant onto B2m–/– + OT-I T cells
combinations (allograft, isograft and mHA mismatch) (Fig. 2b). GFP+ infiltrating cells were motile (mean velocity 5 µm min−1), with a large subset of cells showing vigorous migration (mean velocity > 6 µm min−1) (Fig. 2c and Supplementary Video 3), a behavior consistent with neutrophil phenotype20,21. GFP+ infiltrating cells were absent from the epidermal layer, suggesting a selective exclusion (Fig. 2a,b). By day 9, the density of GFP+ cells infiltrating the dermis had substantially increased, independently of antigenic mismatch (Fig. 2a,b). Dynamic imaging revealed that infiltrating cells formed a sessile network between and along collagen fibers (mean velocity 1.6 µm min−1) (Fig. 2a–c and Supplementary Videos 3 and 4). Many of these infiltrating cells had dendritic morphology (Supplementary Fig. 3). In the epidermis, we detected GFP+ cells only in major histo-compatibility complex (MHC)- or mHA- mismatched grafts (Fig. 2a,b and Supplementary Video 4), and they were either sessile or showed very low motility (1–2 µm min−1) (Supplementary Fig. 4). Taken together, these observations indicate that the rapid graft infiltration by CD11b+ cells in the dermis is antigen independent and ultimately results in a dense network of immotile cells, including monocytes and inflammatory DCs. In contrast, infiltration of the epidermis is a late event and is strictly dependent on antigenic mismatch between donor and recipient.
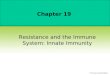
Host graft-infiltrating cells prime CD8+ T cells in the lymph nodes The massive graft infiltration by recipient CD11b+ cells suggests their potential role in stimulating T cells through an indirect antigen pre-sentation pathway. To address this possibility, we developed a two-step transplant procedure. We did a C3H skin transplant on a B6 GFP recipient mouse. After 6 d, we removed the graft containing recipient GFP+ infiltrating cells and retransplanted it onto a B6 host. After 3 d, we analyzed the graft and dLN from the second host by two-photon imaging for the presence of GFP+ cells; numerous GFP+ cells per-sisted in the graft after retransplantation (Fig. 3a and Supplementary Video 5). Most notably, we also detected GFP+ cells in T cell areas of the dLN, as identified by adoptively transferred fluorescent T cells (Fig. 3a and Supplementary Video 6). These findings strongly suggest that the graft is not a dead end for infiltrating CD11b+ cells; rather, CD11b+ cells do, in fact, have the ability to reach the dLN. Because these cells have resided in the graft, they may represent a relevant population for indirect presentation of donor antigens once they are in the lymph nodes. We applied our two-step grafting system to assess the ability of recipient infiltrating cells to cross-prime CD8+ T cells. We grafted skin from a β-2 microglobulin–knockout (B2m−/−) mouse
expressing a membrane-bound form of ovalbumin (mOVA) onto a wild-type B6 recipient mouse. We retransplanted the graft 3 d later onto a B2m−/− recipient mouse that had received carboxyfluorescein succinimidyl ester (CFSE)-labeled CD8+ T cells derived from OT-1 mice (OT-I CD8+). In this setting, direct presentation was excluded, and only infiltrating cells migrating from the first recipient could cross-present OVA (as these cells solely expressed MHC class I mol-ecules). Notably, we detected OT-I CD8+ T cell clonal expansion in the dLN (Fig. 3b). We did not see proliferation in the nondraining lymph nodes or when the initial graft did not express mOVA (Fig. 3b). To exclude the possibility that B2m−/− cells were somehow capable of priming OT-I T cells, we used B2m−/− mice as first recipients. In this case, we detected no OT-I T cell proliferation (Supplementary Fig. 5). Together, these results provide evidence that graft-infiltrating cells do contribute to an indirect pathway of CD8+ T cell activation.
Priming and graft infiltration of alloreactive CD8+ T cellsSecondary lymphoid organs have been shown to be primary sites for priming of alloreactive T cells, although the graft itself could partici-pate in the activation of T cells with a memory phenotype14,15. To determine the relative contribution of the lymph nodes and the graft to the priming of alloreactive CD8+ T cells, we imaged these sites in B6 mice grafted with C3H skin and adoptively transferred with polyclonal GFP-expressing CD8+ T cells. Virtually no GFP+CD8+ T cells could be detected in the graft at day 5 (Fig. 4a). By contrast, in the dLN, many GFP+ T cells showed blasting morphology at day 5 (Fig. 4a) and as early as day 2 (data not shown). We confirmed T cell activation in the dLN by flow cytometry (Supplementary Fig. 6). Next, we assessed how effector alloreactive CD8+ T cells enter the graft after lymph node egress. Skin grafts were revascularized on day 5, as shown by intravenous (i.v.) injection of fluorescent dextran (Supplementary Video 7), providing a potential port of entry for activated CD8+ T cells. However, at this time point, the first detect-able CD8+ T cells were located in the recipient skin surrounding the transplant and not inside the graft (Fig. 4b). On day 8, large numbers of CD8+ T cells had accumulated in the recipient skin in the vicinity of closed-end recipient vessels (Fig. 4b and Supplementary Video 8), and CTLs were readily detected within the graft (Fig. 4a). GFP-expressing CD4+ T cells showed a similar dynamic (Supplementary Video 9). Taken together, these observations indicate that the dLN is the primary site for priming alloreactive CD8+ T cells, and they strongly suggest that the graft edges represent a major point of entry for activated CD4+ and CD8+ T cells.
Figure 3 Recipient graft-infiltrating cells reach the dLN and cross-prime CD8+ T cells. (a) Experimental design. Ear skin from a C3H donor was transplanted onto a B6 GFP recipient. After 6 d, the graft was removed and retransplanted onto a B6 host that had received seminaphtharhodafluor-labeled CD8+ T cells. Representative two-photon microscopic (3 d after retransplantation) images showing that GFP+ cells are present in the dermal layer of the graft (left) and in T cell areas of the dLN (right). Scale bars, 50 µm. (b) We transplanted ear skin from a B2m−/− donor or a B2m−/− donor expressing mOVA onto a B6 recipient; 3 d later we retransplanted it onto a B2m−/− mouse that had been adoptively transferred with CFSE-labeled OT-I T cells. After 4 d, we assessed OT-I T cell proliferation in the dLN by flow cytometry. Profiles are gated on the CD8+Vβ5+CFSE+ cells. Numbers correspond to the percentage of divided cells. Data are representative of at least two independent experiments. LN, lymph node.
© 2
011
Nat
ure
Am
eric
a, In
c. A
ll ri
gh
ts r
eser
ved
.

T e c h n i c a l R e p o R T s
naTuRe medicine VOLUME 17 | NUMBER 6 | JUNE 2011 747
CD8+ T cell dynamics and the progression of tissue destructionOnce CD8+ T cells are in the graft, it is unknown when and where they exert their activity. We found that, on day 8, CD8+ and CD4+ T cells were not uniformly distributed throughout the skin layers; rather, they had accumulated at the dermis-epidermis junction (Fig. 4c, Supplementary Fig. 7 and Supplementary Video 10). To confirm this preferential localization, we imaged the allograft in recombination activating gene 2–deficient (Rag2−/−) mouse recipients that had been adoptively transferred with polyclonal GFP-expressing CD8+ T cells so that all graft-infiltrating T cells would be fluorescently labeled. In this model, graft rejection occurred within 12–15 d (Supplementary Fig. 1). T cells selectively accumulated at the dermis-epidermis junc-tion in this setting as well (Fig. 4c). To assess whether CD8+ T cells exerted cytotoxic activity at this stage, we imaged graft-infiltrating CTLs after i.v. injection of propidium iodide. In these experiments,
we grafted the same B6 recipient mouse with C3H and B6 skin, on the left and right ear respectively, and then adoptively transferred polyclonal GFP-expressing CD8+ T cells into it. We readily detected areas containing large numbers of propidium iodide–positive cells in allografts but not in isografts (Fig. 5a). These regions coincided with areas of CTL accumulation, and CTLs were often arrested in the vicin-ity of dead cells (Supplementary Videos 11–14). Other CTLs (~50%) maintained motile behavior within these areas (Supplementary Videos 11,12,14).
On days 9 and 10, CTLs had disseminated throughout the allograft, and we noted alterations in skin structure, including collagen fiber loss (Fig. 5b). At this stage, CTLs were arrested in allografts (showing low velocity), whereas control isograft CTLs remained motile (Fig. 5b and Supplementary Video 15). In allografts, a small subset of CD8+ T cells maintained high motility (Supplementary Video 15), thereby suggesting that CTL arrest is not the result of T cell migration impair-ment in tissue undergoing rejection. Together, these data reveal a two-step model for graft destruction, with an early phase of CTL killing in discrete areas located at the dermis-epidermis junction and a later phase of CTL dissemination and complete arrest.
Day 5
Day 5
z = 0 µm z = 27 µm z = 63 µm xyx
027
63
z
Day 8
Collagen
Collagen
Collagen
Vessels
Donor LC
CD8+ T cells
CD8+ T cells
CD8+ T cells
Recipient
Graft Graft
CD8+ T cells
* *
Day 8 Day 5dLNGraft dermisa
b
c
Figure 4 Priming and graft localization of CD8+ T cells in the early phase of rejection. (a) Representative two-photon microscopic images of B6 recipients grafted with C3H skin and transferred with GFP+ CD8+ T cells showing that T cells have not reached the graft on day 5 (left) but are detected on day 8 (middle). Scale bars, 50 µm. Right, representative image showing that numerous blastic T cells (arrows) are detected in the dLN on day 5 (right). Asterisks show nonblastic T cells for comparison. Scale bars, 30 µm. (b) Images from the graft edge obtained by intravital two-photon microscopy on days 5 (left) and on day 8 (middle, right). The right image shows CD8+ T cell accumulation around recipient vascular loops. We visualized blood vessels after injection of fluorescent dextran. Scale bars, 50 µm. (c) Images from an ear skin graft (day 9) from C3H CD11c-YFP donor onto a B6 Rag−/− mouse adoptively transferred with GFP+ CD8+ T cells. Images of the epidermis (left), dermis (right) and dermis-epidermis junction (middle) show preferential CD8+ T cell accumulation at the interface. Scale bar, 50 µm. Far left, a schematic of a skin section depicts Langerhans cells (LCs, red), collagen (green) and the depth of the three images presented. Data are representative of two independent experiments.
Dermis-epidermisa
b
Isograft
Allograft
Isograft
20 min
0 min
Allograft
CD8+ T cells Trajectories
Donor LC CD8+ T cells Pl+ cells
Collagen
Dermis
Isograft
CD
8+ T
cel
l vel
ocity
(µm
min
–1)
0
2
4
6
8
10
12
14
Allograft
*
Figure 5 CD8+ T cell dynamics and cytotoxic activity in the graft. (a) Images obtained by intravital two-photon microscopy of the skin from a B6 CD11c-YFP and a C3H CD11c-YFP donor grafted onto the same B6 recipient, on the left and right ears, respectively. Recipients were also adoptively transferred with GFP+ CD8+ T cells (yellow) at the time of transplant and injected with propidium iodide at the time of imaging to visualize dead cells (blue). Scale bars, 70 µm. Right, time-lapse images illustrate a stable interaction between a CD8+ T cell (yellow) and a dead cell (blue). Scale bar, 20 µm. (b) CD8+ T cells in the allograft showed reduced motility and increased confinement. Intravital two-photon imaging (on day 9) showing CD8+ T cell distribution and trajectories for the isograft and the allograft. Scale bar, 30 µm. The graph shows individual T cell velocity in the isograft and in the allograft; *P < 0.0001 (Wilcoxon-Mann-Whitney test). Data are representative of two independent experiments and are from 275 (isograft) and 765 (allograft) T cells. LC, Langerhans cell.
© 2
011
Nat
ure
Am
eric
a, In
c. A
ll ri
gh
ts r
eser
ved
.

T e c h n i c a l R e p o R T s
748 VOLUME 17 | NUMBER 6 | JUNE 2011 naTuRe medicine
DISCUSSIONTransplant rejection is the result of a complex immune response com-prising both an inflammatory and an antigen-specific component3,17. Multiple experimental approaches have helped to investigate these processes; however, they have only provided snapshots of a highly dynamic reaction22,23. In particular, we have only a poor understand-ing of how the immune response is organized in time and space, and of how the dynamics of the various cellular components influence the destruction of the graft. To gain insight into this process, we devel-oped an ear skin graft model for real-time intravital two-photon imag-ing. Two-photon imaging has already proven to be a powerful tool to resolve the orchestration of immune responses against infectious agents and tumors24,25. In the present report, we used intravital imag-ing to identify new checkpoints in the development of an immune response that culminates in allogeneic tissue destruction.
Through imaging donor DCs in transplanted skin, we revealed dif-ferent behaviors for distinct DC subsets. Dermal DCs rapidly disap-peared from the graft within 3–5 d, whereas Langerhans cells persisted until the onset of graft rejection. This phenomenon was independent of MHC disparities and is reminiscent of the different waves of skin DCs migrating to the dLN, as seen previously in other conditions26,27. These results also suggest that Langerhans cells do not contribute to the early activation of alloreactive T cells; this is in line with a recent study showing that Langerhans cells do not usually promote T cell response to skin antigen28. Langerhans cells may, however, have a role at later time points, perhaps by providing additional activation or regulatory signals to T cells, as was recently suggested29.
Using GFP-expressing recipient mice, we identified a massive anti-gen-independent infiltration of host CD11b+ cells within the graft. Neutrophils constituted the predominant population of the early infil-trate but were rapidly outnumbered by monocytes. These temporal changes resembled those observed in the skin after infection with the parasite Leishmania major20,30. Within 6 d, infiltrating cells consti-tuted a dense, immotile network in the dermis, with many cells having a dendritic morphology. Previous studies have shown the presence of inflammatory monocytes and DCs at sites of microbial infection31,32. The phenotype (CD11b+Gr1intermediateCD11clow) and morphological characteristics of the host cells repopulating the graft suggest that infiltration by inflammatory monocytes and DCs is a hallmark of organ transplantation.
The rapid disappearance of donor dermal DCs from the graft raised the question of which APCs activate alloreactive T cells at later time points. An indirect pathway of antigen presentation is believed to have an key role in chronic rejection1,33. A potential source of alloantigen for indirect presentation may include donor cells migrating and dying in the dLN3,9. Alternatively, recipient APCs infiltrating the graft may collect antigen and subsequently migrate to the dLN3. Although this possibility has been suggested by a recent study on inflamed skin34, it has never been formally shown during organ rejection. To address this issue, we have developed a two-step grafting procedure to restrict antigen presentation capacity to host graft-infiltrating APCs. With this strategy, it was possible to show that recipient infiltrating cells have the ability to reach the dLN and cross-prime CD8+ T lym-phocytes. Thus, host inflammatory monocytes and DCs within the graft may represent an important source of migrating APCs ferrying antigen from the graft to activate alloreactive T cells in the dLN via an indirect pathway. This mechanism may be involved in chronic graft rejection, in which T cell–mediated tissue destruction may favor sus-tained monocyte infiltration and differentiation. Therefore, blocking monocyte recruitment into allografts might offer an effective strategy
to disrupt ongoing chronic rejection. Indirectly primed CTLs may exert their effector functions in the skin graft, for instance, by target-ing host endothelial cells presenting donor antigen35.
Furthermore, we identify the microanatomy of CD8+ T cell infil-tration and activity within the graft. After priming within the dLN, CD8+ T cells begin to accumulate in recipient tissue surrounding the graft. This finding was notable, given that at this point, revascu-larization of the graft had been established, thereby providing direct access for infiltrating cells. Our data suggest that, at least in early time points, CD8+ T cell infiltration proceeded from the periphery to the center of the graft. In addition, graft-infiltrating CD8+ T cells initially accumulated selectively at the dermis–epidermis junction, where evi-dence for cytotoxic activity was first detected. Later, CD8+ T cells were found to be uniformly distributed throughout the graft, where they arrested, perhaps as the result of antigen recognition. Experiments in allophenic mice have indicated that T cell effector activity during skin graft rejection is antigen-specific36. Our results are consistent with this, and they support the idea that CTL cytotoxic activity in the skin is associated with the formation of long-lasting interactions with target cells, as was previously observed in solid tumors37,38.
In summary, we report here the development of a skin graft model suitable for intravital two-photon imaging. Using this model, we have characterized the spatiotemporal orchestration of the immune response leading to allograft rejection (Supplementary Fig. 8). We have shown how the inflammatory infiltrate in the graft contributes to an indirect pathway of T cell activation, and we have uncovered the spatial progres-sion of CD8+ T cell effector activity. In addition, our approach should offer new opportunities for studying how therapeutic intervention may finely tune the cellular mechanisms underlying graft rejection.
METHODSMethods and any associated references are available in the online version of the paper at http://www.nature.com/naturemedicine/.
Note: Supplementary information is available on the Nature Medicine website.
ACknowLedgMentSWe wish to thank H. Saklani and C. Auriau (Institut Pasteur) for providing B2m−/– mOVA mice and E. Robey and the members of the Bousso laboratory for comments on the manuscript. This work was supported by INSERM, Institut Pasteur and a Marie Curie Excellence grant.
AUtHoR ContRIBUtIonSS.C. designed and carried out the experiments, analyzed the data and wrote the manuscript; M.L.A. developed crucial reagents and participated in experimental design; and P.B. designed the experiments, analyzed the data and wrote the manuscript.
CoMPetIng FInAnCIAL InteReStSThe authors declare no competing financial interests.
Published online at http://www.nature.com/naturemedicine/. Reprints and permissions information is available online at http://www.nature.com/reprints/index.html.
1. Auchincloss, H. Jr. & Sultan, H. Antigen processing and presentation in transplantation. Curr. Opin. Immunol. 8, 681–687 (1996).
2. Rosenberg, A.S. & Singer, A. Cellular basis of skin allograft rejection: an in vivo model of immune-mediated tissue destruction. Annu. Rev. Immunol. 10, 333–358 (1992).
3. Ingulli, E. Mechanism of cellular rejection in transplantation. Pediatr. Nephrol. 25, 61–74 (2010).
4. Talmage, D.W., Dart, G., Radovich, J. & Lafferty, K.J. Activation of transplant immunity: effect of donor leukocytes on thyroid allograft rejection. Science 191, 385–388 (1976).
5. Richards, D.M. et al. Indirect minor histocompatibility antigen presentation by allograft recipient cells in the draining lymph node leads to the activation and clonal expansion of CD4+ T cells that cause obliterative airways disease. J. Immunol. 172, 3469–3479 (2004).
© 2
011
Nat
ure
Am
eric
a, In
c. A
ll ri
gh
ts r
eser
ved
.

T e c h n i c a l R e p o R T s
naTuRe medicine VOLUME 17 | NUMBER 6 | JUNE 2011 749
6. Ochando, J.C., Krieger, N.R. & Bromberg, J.S. Direct versus indirect allorecognition: Visualization of dendritic cell distribution and interactions during rejection and tolerization. Am. J. Transplant. 6, 2488–2496 (2006).
7. Larsen, C.P., Austyn, J.M. & Morris, P.J. The role of graft-derived dendritic leukocytes in the rejection of vascularized organ allograft. Recent findings on the migration and function of dendritic leukocytes after transplantation. Ann. Surg. 212, 308–315 (1990).
8. Valujskikh, A., Hartig, C. & Heeger, P.S. Indirectly primed CD8+ T cells are a prominent component of the allogeneic T-cell repertoire after skin graft rejection in mice. Transplantation 71, 418–421 (2001).
9. Garrod, K.R. et al. NK cell patrolling and elimination of donor-derived dendritic cells favor indirect alloreactivity. J. Immunol. 184, 2329–2336 (2010).
10. Lakkis, F.G., Arakelov, A., Konieczny, B.T. & Inoue, Y. Immunologic ‘ignorance’ of vascularized organ transplants in the absence of secondary lymphoid tissue. Nat. Med. 6, 686–688 (2000).
11. Zhou, P. et al. Secondary lymphoid organs are important but not absolutely required for allograft responses. Am. J. Transplant. 3, 259–266 (2003).
12. Barker, C.F. & Billingham, R.E. The role of afferent lymphatics in the rejection of skin homografts. J. Exp. Med. 128, 197–221 (1968).
13. Wang, J. et al. Donor lymphoid organs are a major site of alloreactive T-cell priming following intestinal transplantation. Am. J. Transplant. 6, 2563–2571 (2006).
14. Schenk, A.D., Nozaki, T., Rabant, M., Valujskikh, A. & Fairchild, R.L. Donor-reactive CD8 memory T cells infiltrate cardiac allografts within 24-h post-transplant in naive recipients. Am. J. Transplant. 8, 1652–1661 (2008).
15. Kreisel, D. et al. Non-hematopoietic allograft cells directly activate CD8+ T cells and trigger acute rejection: an alternative mechanism of allorecognition. Nat. Med. 8, 233–239 (2002).
16. Gelman, A.E. et al. Cutting edge: Acute lung allograft rejection is independent of secondary lymphoid organs. J. Immunol. 182, 3969–3973 (2009).
17. Rocha, P.N., Plumb, T.J., Crowley, S.D. & Coffman, T.M. Effector mechanisms in transplant rejection. Immunol. Rev. 196, 51–64 (2003).
18. Strid, J. et al. Acute upregulation of an NKG2D ligand promotes rapid reorganization of a local immune compartment with pleiotropic effects on carcinogenesis. Nat. Immunol. 9, 146–154 (2008).
19. Nishibu, A. et al. Behavioral responses of epidermal Langerhans cells in situ to local pathological stimuli. J. Invest. Dermatol. 126, 787–796 (2006).
20. Peters, N.C. et al. In vivo imaging reveals an essential role for neutrophils in leishmaniasis transmitted by sand flies. Science 321, 970–974 (2008).
21. Chtanova, T. et al. Dynamics of neutrophil migration in lymph nodes during infection. Immunity 29, 487–496 (2008).
22. Matsuo, S., Kurisaki, A., Sugino, H., Hashimoto, I. & Nakanishi, H. Analysis of skin graft survival using green fluorescent protein transgenic mice. J. Med. Invest. 54, 267–275 (2007).
23. Ehst, B.D., Ingulli, E. & Jenkins, M.K. Development of a novel transgenic mouse for the study of interactions between CD4 and CD8 T cells during graft rejection. Am. J. Transplant. 3, 1355–1362 (2003).
24. Konjufca, V. & Miller, M.J. Two-photon microscopy of host-pathogen interactions: acquiring a dynamic picture of infection in vivo. Cell. Microbiol. 11, 551–559 (2009).
25. Ng, L.G., Mrass, P., Kinjyo, I., Reiner, S.L. & Weninger, W. Two-photon imaging of effector T-cell behavior: lessons from a tumor model. Immunol. Rev. 221, 147–162 (2008).
26. Kissenpfennig, A. et al. Dynamics and function of Langerhans cells in vivo: dermal dendritic cells colonize lymph node areas distinct from slower migrating Langerhans cells. Immunity 22, 643–654 (2005).
27. Sen, D., Forrest, L., Kepler, T.B., Parker, I. & Cahalan, M.D. Selective and site-specific mobilization of dermal dendritic cells and Langerhans cells by TH1- and TH2-polarizing adjuvants. Proc. Natl. Acad. Sci. USA 107, 8334–8339 (2010).
28. Wang, L. et al. Langerin expressing cells promote skin immune responses under defined conditions. J. Immunol. 180, 4722–4727 (2008).
29. Obhrai, J.S. et al. Langerhans cells are not required for efficient skin graft rejection. J. Invest. Dermatol. 128, 1950–1955 (2008).
30. Beil, W.J., Meinardus-Hager, G., Neugebauer, D.C. & Sorg, C. Differences in the onset of the inflammatory response to cutaneous leishmaniasis in resistant and susceptible mice. J. Leukoc. Biol. 52, 135–142 (1992).
31. Léon, B., Lopez-Bravo, M. & Ardavin, C. Monocyte-derived dendritic cells formed at the infection site control the induction of protective T helper 1 responses against Leishmania. Immunity 26, 519–531 (2007).
32. Robben, P.M., LaRegina, M., Kuziel, W.A. & Sibley, L.D. Recruitment of Gr-1+ monocytes is essential for control of acute toxoplasmosis. J. Exp. Med. 201, 1761–1769 (2005).
33. Benichou, G., Valujskikh, A. & Heeger, P.S. Contributions of direct and indirect T cell alloreactivity during allograft rejection in mice. J. Immunol. 162, 352–358 (1999).
34. Le Borgne, M. et al. Dendritic cells rapidly recruited into epithelial tissues via CCR6/CCL20 are responsible for CD8+ T cell crosspriming in vivo. Immunity 24, 191–201 (2006).
35. Valujskikh, A., Lantz, O., Celli, S., Matzinger, P. & Heeger, P.S. Cross-primed CD8+ T cells mediate graft rejection via a distinct effector pathway. Nat. Immunol. 3, 844–851 (2002).
36. Rosenberg, A.S. & Singer, A. Evidence that the effector mechanism of skin allograft rejection is antigen-specific. Proc. Natl. Acad. Sci. USA 85, 7739–7742 (1988).
37. Breart, B., Lemaitre, F., Celli, S. & Bousso, P. Two-photon imaging of intratumoral CD8+ T cell cytotoxic activity during adoptive T cell therapy in mice. J. Clin. Invest. 118, 1390–1397 (2008).
38. Boissonnas, A., Fetler, L., Zeelenberg, I.S., Hugues, S. & Amigorena, S. In vivo imaging of cytotoxic T cell infiltration and elimination of a solid tumor. J. Exp. Med. 204, 345–356 (2007).
© 2
011
Nat
ure
Am
eric
a, In
c. A
ll ri
gh
ts r
eser
ved
.

naTuRe medicine doi:10.1038/nm.2376
ONLINE METHODSMice. We purchased male and female wild-type C57BL/6 (B6) and C3H/HeOuJ (C3H) mice from Charles River Laboratories. We bred CD11c-YFP transgenic mice bred into a B6 or C3H background, Rag−/− OT-I TCR transgenic mice, B6 Rag2−/−, B6 transgenic mice expressing GFP under the control of the ubiquitin C promoter and B6 B2m−/− mice in our animal facility. We crossed B6 B2m−/− mice to B6 mice expressing a mOVA under the chicken β-actin promoter (The Jackson Laboratory) to obtain B6 B2m−/− mOVA-expressing transgenic mice. All animal studies were approved by the Pasteur Institute Safety Committee in accordance with French and European guidelines.
Ear skin transplantation. We killed B6 or C3H donor mice and removed a 7 × 7 mm flap of skin comprising the epidermis and dermis, but not donor cartilage, from the ventral side of the ear and placed it in cold saline solution. We anesthetized recipients and replaced a 7 × 7 mm flap of skin (epidermis, dermis and cartilage) from the ventral side of the ear with donor skin. We applied four stitches (8/0 Dexon, Davis and Geck) to maintain the graft. In this model, the lymph node draining the graft corresponded to the superficial parotid lymph node, according to recent nomenclature39. This lymph node showed the most prominent size increase after ear skin transplant. For the two-step transplant experiments, we gently removed the first skin graft at day 3–6 and retransplanted it immediately into a new host.
Flow cytometry. We incubated skin grafts at 37 °C for 30 min in RPMI con-taining 1 mg ml−1 collagenase and 0.05 mg ml−1 DNase (Sigma). We then incubated cell suspensions with Fc-specific receptor (CD16/32, eBioscience, cat. no.14-0161-86) and stained them with phycoerythrin (PE)-conjugated CD11b-specific (BD Biosciences, cat. No. 553311), PE-Cy7–conjugated CD11c-specific (BD Biosciences, cat. no. 558079), APC-conjugated Gr1-specific (eBioscience, cat. no. 17-5931-82) and Alexa Fluor 750–conjugated CD8α-specific (eBioscience, cat. no. 47-0081-82) monoclonal antibodies. We incubated lymph node cells with a Fc-specific receptor and stained them with PE-Cy7–conjugated CD8α-specific (eBioscience, cat. no. 25-0081-82) and APC-conjugated CD44-specific (cat. no. 17-0441-83) monoclonal antibodies, or with APC-conjugated CD8α-specific (BD Bioscences, cat. no. 553035) and PE-conjugated Vβ-specific 5.1,5.2 antibodies (BD Bioscences, cat. no. 553190).
We acquired data with a FACSCanto II flow cytometer (BD Biosciences) and analyzed it with FlowJo software (TreeStar, version 8.8.2).
Cell purification and transfer. We purified CD8+ T cells by negative selection from lymph nodes and spleens of GFP-expressing transgenic mice using a CD8+ isolation kit and an autoMACS system (Miltenyi Biotec). Approximately 2 h before transplantation, we adoptively transferred 50 × 106 CD8+ T cells into recipient mice by i.v. injection. When Rag2−/− mice were used as recipients, we transferred 10 × 106 CD8+ T cells. We isolated OT-I CD8+ T cells from lymph nodes and spleens of Rag2−/− OT-I TCR mice and labeled them with 5 µM CFSE (Invitrogen) for 12 min at 37 °C.
Intravital two-photon imaging. We carried out lymph node imaging as previ-ously described40. For skin graft imaging, we anesthetized mice and placed them on a custom-designed heated stage. We placed a cover slip, onto which was glued a heated metal ring, on the mouse’s ear, and filled the ring with sufficient water to immerge a ×20/0.95NA dipping objective (Olympus). We did two-photon imaging using an upright microscope (DM6000B, Leica Microsystems) with excitation provided by a Ti-sapphire laser (Coherent) tuned at 900–950 nm. We detected fluorescence with four nondescanned detectors (Leica Microsystems). Typically, we collected images from 5 to 10 z-planes, spaced 5 µm apart, every 30 s for up to 30 min. We measured three-dimensional cell tracking and cell velocity with Imaris software (Bitplane).
For the detection of dead cells in vivo, we slowly injected 200 µl of PBS containing 1 mg ml−1 propidium iodide (Sigma) into the tail vein of an anes-thetized mouse. We started image acquisition by two-photon microscopy 15 min after the injection. To visualize the vasculature, we injected mice i.v. with 300 µl of PBS containing 10 mg ml−1 tetramethyl rhodamine isothiocyanate–dextran 150 kDa (Sigma) 15 min before imaging.
Statistical analyses. Statistical analyses were done using the Wilcoxon-Mann-Whitney test. A P value of < 0.05 was considered significant.
39. Van den Broeck, W., Derore, A. & Simoens, P. Anatomy and nomenclature of murine lymph nodes: Descriptive study and nomenclatory standardization in BALB/cAnNCrl mice. J. Immunol. Methods 312, 12–19 (2006).
40. Celli, S., Garcia, Z. & Bousso, P. CD4 T cells integrate signals delivered during successive DC encounters in vivo. J. Exp. Med. 202, 1271–1278 (2005).
© 2
011
Nat
ure
Am
eric
a, In
c. A
ll ri
gh
ts r
eser
ved
.