Embed Size (px)
Citation preview

Visual Composition
Easiest Bill to Understand
August 8, 2016

Financial Summary: You owe $175.00. On July 25th, you had an office visit with your heart doctor, Dr. Levi. Upon arrival, you paid a $25 copay with your Visa ending in 4639. On 7/25 we billed your insurance $1825. On 7/28 we received a payment of $1725. The total amount you will owe for this visit is $100, minus your copayment of $25. Therefore the total amount owed for this visit is $75. Please note, you have an outstanding balance of $100. You owe $175.00.
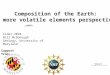
Patient Name: Wendy SmithPerson Responsible: Wendy SmithName of Provider: John Levi, MDDate of Service: 7/25/2016Single Account Number: 123456Primary Insurance: Hometown HealthSecondary Insurance: None
FINANCIAL STATEMENT
YOU OWE: $175.00
Due: 8/25/2016Statement Date: 8/1/2016
Code Description Insurance You Owe
90656 Flu Shot $75.00 $0.00
74176 CT-Scan $1025.00 $75.00
85610 Lab Work $400.00 $0.00
99204 Office Visit $225.00 $25.00
TOTAL $1725.00 $100.00
7/28 – Insurance Payment -$1725.00
7/25 - Copayment -$25.00
This Visit Balance $75.00
Previous Balance $100.00
You Owe $175.00
VISIT CHARGES
Insurance
You Owe
Copay
DEDUCTIBLE
LabOffice Visits
Hospital
$1,056 $1,942 $2,200
$1,300
$3,000
$4,000
2016 Spend
$5,1982016 Deductible
$9,500
PAYMENT OPTIONS
EASY PAYMENT PLAN:
Full Amount (10% Discount)
Monthly for 3 Months
Monthly for 6 Months
Monthly for 12 Months
Call to Discuss: 866-691-0284
Paperless Statements: YES NO
Billing Questions, Financial Assistance and Payment Plans: 866-691-0284
Online: Renown.org/PayNow Checks Payable to: Renown Health, PO BOX 844134
Los Angeles, CA 90084-4134 Credit: Visa MasterCard Disc Amex
Amount:
Name:
Card Number:
Exp Date: CVC:
Signature:
Health Summary: On July 25th, 2016 you had an office visit with your heart doctor, Dr. Levi. Dr. Levi assessed you in the clinic, performed an echocardiogram and CT-Scan to understand the health of your heart, adjusted your medications, and ordered lab tests to ensure your medications were working as planned.
EMAIL YOUR PROVIDER: MyChart.Renown.org HEALTHY LIVING TIPS: BestMedicineNews.org
REASON FOR VISIT:Visit Renown.org for interactive map
Heart Visit
WELLNESS CHECKLIST:Can we call you to schedule this? Yes No - Mammogram (Due 8/15) Yes No - A1c Lab Test (Due 9/1) Yes No - Colonoscopy (Due 10/1) Yes No - Eye Exam (Due 10/15)
CARE PROVIDED: Office Visit (7/25) Flu Shot (7/25) CT-Scan (7/25) Echocardiogram (7/26) Blood Work (7/28)
MYCHART VISIT VITALS: Weight: 130 BMI: 22 Blood Pressure: 120/80 Pulse: 80
VISIT INFORMATION: Provider: Dr. Levi Dates: 7/25 Location: 75 Pringle Number of Visits Included: 1
Patient Name: Wendy SmithPerson Responsible: Wendy SmithName of Provider: John Levi, MDDate of Service: 7/25/2016Single Account Number: 123456Primary Insurance: Hometown HealthSecondary Insurance: None
HEALTHCARESUMMARY

PREGUNTAS ACERCA DE SU BIL O PLANES DE PAGO: 866-691-0284
RESUMEN FINANCIERO: El 25 de Julio, usted tuvo una visita con su cardiologo el
Doctor Levi. A su llegada, usted pago una cuota de $25 dolares con su tarjeta
VISA terminando en 4639. Le mandamos un bil a su seguransa de $1420.
Recibimos un pago de $1350 el dia 7/28. El total restante que usted deve por
esta visita es $75.00 dolares. Tome encuenta, que usted tiene un balance de
$100 dolares devidos anteriormente. La cantidad que usted debe $175.00
Nombre Del Paciente: Wendy Smith
Fecha De Nacimiento: 9/15/1951
Dia de Servicio: 7/25/2016
Numero de Cuenta : 123456
Estado Financiero
$175.00Usted Deve:
Fecha De Pago: 8/25/2016
Vacuna de influenza $0.00
Ecocardiograma,
Eco, Tomografia$75.00
Analysis $0.00
Visita de oficina $0.00
TOTAL $75.00
Pago de Asegurnasa $1350.00
Balanse Anterior $100.00
Esta Visita $75.00
Usted Debe $175.00
RESPONSABILIDAD POR ESTA VISITA
PAGO
En Linia: Renown.org/PayNow
Pago de Checke: Renown Health, PO BOX 844134 Los
Angeles, CA 90084-4134
Credito: Visa MasterCard Disc Amex
Numero de Tarjetar:
Fecha de
Vencimiento:CVC :
Firma :
GASTO DE ANO ASTA LA FECHA
$1,056
$1,942
$2,200
Analysis Visitas de
OficinaHospital
2016 Total Gastado
$5,1982016 Maximo
$9,500
SEPARACION DEL BIL
El dia 7/28 Su Aseguransa Pago : $250
Resposabilidaddel Paciente
(Usted Deve): $75
El dia 7/25 su cuota
pagada fue : $25

Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
FINANCIAL STATEMENT
BILLING QUESTIONS & PAYMENT PLANS: 866-691-0284
FINANCIAL SUMMARY: On July 25th, you had an office visit with your heart
doctor, Dr. Levi. Upon arrival, you paid a $25 copayment via your Visa ending in
4639. We billed your insurance $1420. We received a payment of $1350 on 7/28.
The total remaining amount you will owe for this visit is $75.00. Please note, you
also have an outstanding balance of $100. Total amount owed is $175.00
DUE: 8/25/2016
PAGO
En Linia: Renown.org/Paga Ahora
Checks Payable to:
Renown Health, PO BOX 844134
Los Angeles, CA 90084-4134
YEAR-TO-DATE SPENDING
$1,056
$1,942
$2,200
Lab Office Visits Hospital
2016 Total Spend
$5,1982016 Maximum
$9,500ServicioPorcion de
AsegursaUsted Deve
Vacuna de Influenza $75.00 $0.00
Ecocardiograma,
Echo, CT-Scan$1025.00 $75.00
Lab Work $400 $0.00
Office Visit $250.00 $0.00
TOTAL $1350.00 $75.00
7/28 – Pago de Aseguransa $1350.00
Balance Anterior $100.00
Esta Visita $75.00
Usted Deve $175.00
RESPONSABILIDAD POR ESTA VISITA

Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
FINANCIAL STATEMENT
BILLING QUESTIONS & PAYMENT PLANS: 866-691-0284
$175.00YOU OWE:
DUE: 8/25/2016
ServiceCharged
Amount
Discounted
Amount
Insurance
PortionYou Owe
Flu Shot $150.00 $75.00 $75.00 $0.00
EKG, Echo, CT-Scan $2000.00 $1100.00 $1025.00 $75.00
Lab Work $0.00 $0.00 $400 $0.00
Office Visit $400.00 $250.00 $250.00 $0.00
TOTAL $2550.00 $1420.00 $1350.00 $75.00
7/28 - Insurance Payment $1350.00
Previous Balance $100.00
This Visit $75.00
Your Responsibility $175.00
RESPONSIBILITY FOR THIS VISIT
FINANCIAL SUMMARY: On July 25th, you had an office visit with your heart
doctor, Dr. Levi. Upon arrival, you paid a $25 copayment via your Visa ending in
4639. We billed your insurance $1420. We received a payment of $1350 on 7/28.
The total remaining amount you will owe for this visit is $75.00. Please note, you
also have an outstanding balance of $100. Total amount owed is $175.00
PAYMENT
Online: Renown.org/PayNow
Checks Payable to: Renown Health, PO BOX
844134 Los Angeles, CA 90084-4134
Credit: Visa MasterCard Disc Amex
Card Number:
Exp Date: CVC Code:
Signature:
2016 Total Spend
$5,198
YEAR-TO-DATE SPENDINGOut-of-Pocket at Hometown Health
2016 Maximum
$9,500

LEVEL 1 - SUMMARY
LEVEL 2 – DETAIL
LEVEL 3 – FULL INFORMATION
PAYMENT INFO
Online: Renown.org/PayNow
Checks Payable to: Renown Health, PO BOX 844134 Los
Angeles, CA 90084-4134
Credit: Visa MasterCard Disc Amex
Name:
Card Number:
Exp Date: CVC Code:
Signature:
PAYMENT INFO
Online: Renown.org/PayNow
PAYMENT INFO
EASY PAYMENT PLAN:
Full Amount (10% Discount)
Monthly for 3 Months
Monthly for 6 Months
Monthly for 12 Months
Call to Discuss: 866-691-0284
Paperless Statements YES NO
Name:
Card Number:
Exp Date: CVC Code:
Signature:
Online: Renown.org/PayNow
Checks Payable to: Renown Health, PO BOX
844134 Los Angeles, CA 90084-4134
Credit: Visa MasterCard Disc Amex

BILLING BREAKDOWN
ON 7/28 YOUR INSURANCE COMPANY PAID: $250
PATIENT RESPONSIBILITY(YOU OWE): $75
ON 7/25 YOUR COPAY PAID: $25
BILLING BREAKDOWN
Insurance
You Owe
Copay
BILLING BREAKDOWN
INSURANCE PAID: $250 YOU PREVIOUSLY PAID: $25 YOU OWE: $75
LEVEL 1 - SUMMARY
LEVEL 2 – DETAIL
LEVEL 3 – FULL INFORMATION

LEVEL 1 - SUMMARY
LEVEL 2 – DETAIL
LEVEL 3 –FULL INFORMATION
2016 Total Spend
$5,198
YEAR-TO-DATE SPENDINGOut-of-Pocket at Hometown Health
2016 Maximum
$9,500
YEAR-TO-DATE SPENDING
$1,056
$1,942
$2,200
Lab Office Visits Hospital
LabOffice
VisitsHospital
YEAR-TO-DATE SPENDING
$1,056
$1,942
$2,200
$1,300
$3,000
$4,000
2016 Total Spend
$5,1982016 Maximum
$9,500
2016 Total Spend
$5,1982016 Maximum
$9,500

ServiceCharged
Amount
Discounted
Amount
Insurance
PortionYou Owe
Flu Shot $150.00 $75.00 $75.00 $0.00
EKG, Echo, CT-Scan $2000.00 $1100.00 $1025.00 $75.00
Lab Work $0.00 $0.00 $400 $0.00
Office Visit $400.00 $250.00 $250.00 $0.00
TOTAL $2550.00 $1420.00 $1350.00 $75.00
7/28 - Insurance Payment $1350.00
Previous Balance $100.00
This Visit $75.00
Your Responsibility $75.00
RESPONSIBILITY FOR THIS VISIT
Flu Shot $0.00
EKG, Echo, CT-Scan $75.00
Lab Work $0.00
Office Visit $0.00
TOTAL $75.00
Insurance Payment $1350.00
Previous Balance $100.00
This Visit $75.00
You Owe $175.00
RESPONSIBILITY FOR THIS VISIT
LEVEL 1 – SUMMARY LEVEL 2 – DETAIL
LEVEL 3 – FULL INFO
ServiceInsurance
PortionYou Owe
Flu Shot $75.00 $0.00
EKG, Echo, CT-Scan $1025.00 $75.00
Lab Work $400 $0.00
Office Visit $250.00 $0.00
TOTAL $1350.00 $75.00
7/28 – Insurance Payment $1350.00
Previous Balance $100.00
This Visit $75.00
You Owe $175.00
RESPONSIBILITY FOR THIS VISIT

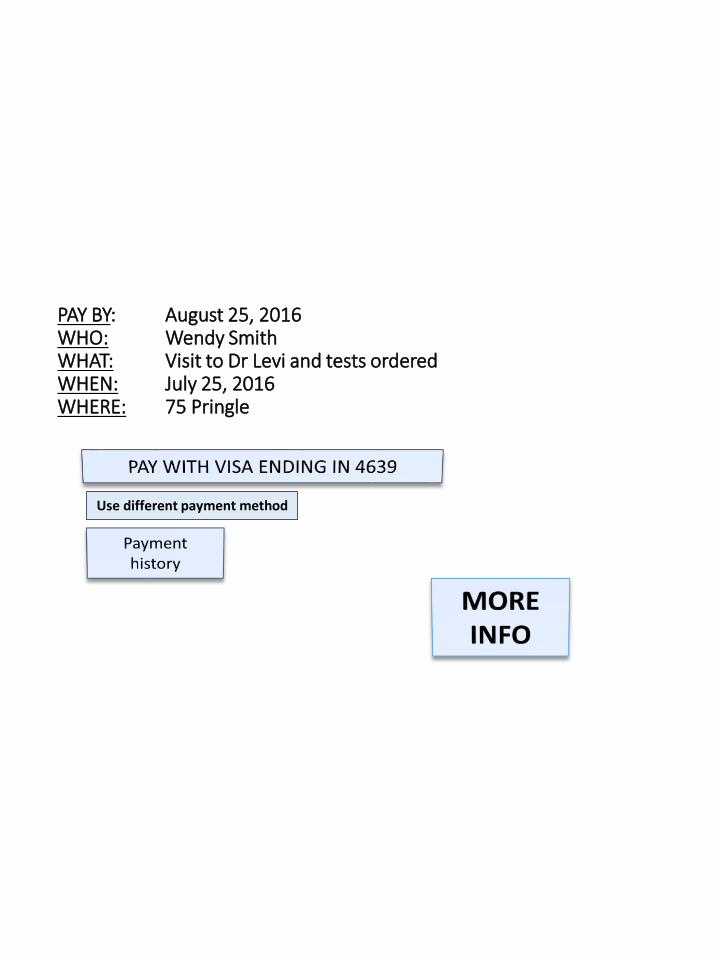
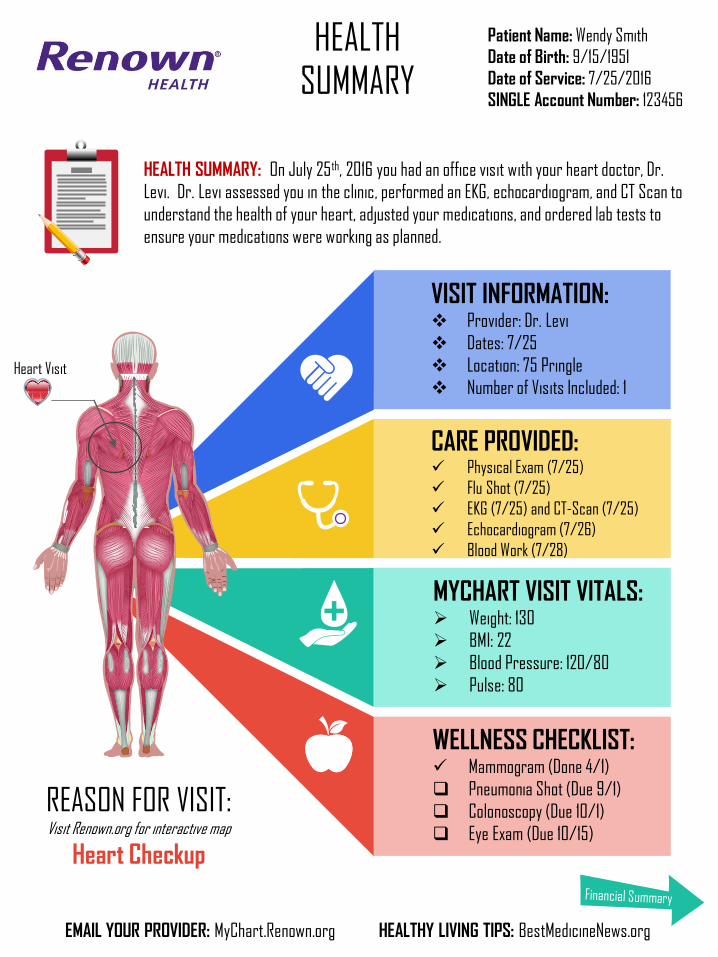
HEALTH SUMMARY: On July 25th, 2016 you had an office visit with your heart doctor, Dr.
Levi. Dr. Levi assessed you in the clinic, performed an EKG, echocardiogram, and CT Scan to
understand the health of your heart, adjusted your medications, and ordered lab tests to
ensure your medications were working as planned.
EMAIL YOUR PROVIDER: MyChart.Renown.org HEALTHY LIVING TIPS: BestMedicineNews.org
REASON FOR VISIT:Visit Renown.org for interactive map
Heart Checkup
WELLNESS CHECKLIST: Mammogram (Done 4/1)
Pneumonia Shot (Due 9/1)
Colonoscopy (Due 10/1)
Eye Exam (Due 10/15)
CARE PROVIDED: Physical Exam (7/25)
Flu Shot (7/25)
EKG (7/25) and CT-Scan (7/25)
Echocardiogram (7/26)
Blood Work (7/28)
MYCHART VISIT VITALS: Weight: 130
BMI: 22
Blood Pressure: 120/80
Pulse: 80
VISIT INFORMATION: Provider: Dr. Levi
Dates: 7/25
Location: 75 Pringle
Number of Visits Included: 1
Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
HEALTH SUMMARY
Heart Visit


Subject: Hi Wendy, your healthcare statement is ready for review
Wendy, you received services at Renown Health
PAY BY: August 25, 2016WHO: Wendy SmithWHAT: Visit to Dr Levi and tests orderedWHEN: July 25, 2016WHERE: 75 Pringle
Use different payment method


Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
PAYMENT
FINANCIAL STATEMENT
BILLING QUESTIONS & PAYMENT PLANS: 866-691-0284
FINANCIAL SUMMARY: On July 25th, you had an office visit with your heart doctor, Dr. Levi. Upon
arrival, you paid a $25 copayment via your Visa ending in 4639. We billed your insurance $1420. We
received a payment of $1350 on 7/28. The total remaining amount you will owe for this visit is
$75.00. Please note, you also have an outstanding balance of $100. Total amount owed is $175.00
Service
$1420.00TOTAL
Charged
Amount
EKG, Echo, CT-scan $1100.00
Lab Work $0.00
Office Visit $250.00
Flu Shot $75.00
RESPONSIBILITY FOR THIS VISIT
Insurance
Responsibility
$1025.00
$0.00
$250.00
$75.00
You Owe
$75.00
$0.00
$0.00
$0.00
$1350.00 $75.00
Online: Renown.org/PayNow
Checks Payable to: Renown Health, PO BOX 844134 Los
Angeles, CA 90084-4134
Credit: Visa MasterCard Disc Amex
Card Number:
Exp Date: CVC Code:
Signature:
This is your bill
STATEMENTS
$175.00YOU OWE:
DUE: 8/25/2016
DATE NOTES PAID AMOUNT
6/8 Prev Balance NO $100.00
7/25 New Balance NO $75.00
2016 Out of Pocket Renown Spend
$5,198
YEAR-TO-DATE SPENDING
$1,056
$1,942
$2,200
Lab Office Visits Hospital

Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
PAYMENT
FINANCIAL STATEMENT
STATEMENTS
BILLING QUESTIONS & PAYMENT PLANS: 866-691-0284
2016 Total Spend
$5,198
YEAR-TO-DATE SPENDINGOut-of-Pocket at Hometown Health
$175.00YOU OWE:
FINANCIAL SUMMARY: On July 25th, you had an office visit with your heart doctor, Dr. Levi. Upon
arrival, you paid a $25 copayment via your Visa ending in 4639. We billed your insurance $1420. We
received a payment of $1350 on 7/28. The total remaining amount you will owe for this visit is
$75.00. Please note, you also have an outstanding balance of $100. Total amount owed is $175.00
Service
$1420.00TOTAL
Charged
Amount
EKG, Echo, CT-scan $1100.00
Lab Work $0.00
Office Visit $250.00
Flu Shot $75.00
RESPONSIBILITY FOR THIS VISIT
Insurance
Responsibility
$1025.00
$0.00
$250.00
$75.00
You Owe
$75.00
$0.00
$0.00
$0.00
$1350.00 $75.00
DUE: 8/25/2016
Online: Renown.org/PayNow
Checks Payable to: Renown Health, PO BOX 844134 Los
Angeles, CA 90084-4134
Credit: Visa MasterCard Disc Amex
Card Number:
Exp Date: CVC Code:
Signature:
This is your bill
7/25 Copayment
7/31 $75.00
DATE NOTES PAID AMOUNT
7/31 $1350.00
6/8 Prev Balance NO
$25.00
$100.00
YES
NO
YES
7/25 New Balance NO $75.00
YourResponsibility
7/25 Charged $1420.00YES
InsurancePayment
2016 Maximum
$9,500

HEALTH SUMMARY: On July 25th, 2016 you had an office visit with your heart doctor, Dr.
Levi. Dr. Levi assessed you in the clinic, performed an EKG, echocardiogram, and CT Scan to
understand the health of your heart, adjusted your medications, and ordered lab tests to
ensure your medications were working as planned.
EMAIL YOUR PROVIDER: MyChart.Renown.org HEALTHY LIVING TIPS: BestMedicineNews.org
REASON FOR VISIT:Visit Renown.org for interactive map
Heart Checkup
WELLNESS CHECKLIST: Mammogram (Done 4/1)
Pneumonia Shot (Due 9/1)
Colonoscopy (Due 10/1)
Eye Exam (Due 10/15)
CARE PROVIDED: Physical Exam (7/25)
Flu Shot (7/25)
EKG (7/25) and CT-Scan (7/25)
Echocardiogram (7/26)
Blood Work (7/28)
MYCHART VISIT VITALS: Weight: 130
BMI: 22
Blood Pressure: 120/80
Pulse: 80
VISIT INFORMATION: Provider: Dr. Levi
Dates: 7/25
Location: 75 Pringle
Number of Visits Included: 1
Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
HEALTH SUMMARY
Heart Visit

Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
PAYMENT
FINANCIAL SUMMARY
BALANCE
BILLING QUESTIONS & PAYMENT PLANS: 866-691-0284
2016 Total Spend
$5,198
YEAR-TO-DATE SPENDINGOut-of-Pocket at Hometown Health
$175.00YOU OWE:
FINANCIAL SUMMARY: On July 25th, you had an office visit with your heart doctor, Dr. Levi. Upon
arrival, you paid a $25 copayment via your Visa ending in 4639. We billed your insurance $1420
and received a payment of $1350 on 7/28. The total remaining amount you will owe for this visit
is $75.00. Please note, you also have an outstanding balance of $100. Total amount owed is
$175.00
Services
$1420.00TOTAL
Total Fee
EKG, Echo, CT-scan $1100.00
Lab Work $0.00
Office Visit $250.00
Flu Shot $75.00
PATIENT RESPONSIBILITY
Insurance
Responsibility
$1025.00
$0.00
$250.00
$75.00
You Owe
$75.00
$0.00
$0.00
$0.00
$1350.00 $75.00
DUE: 8/25/2016
Online: Renown.org/PayNow
Checks Payable to: Renown Health, PO BOX 844134 Los
Angeles, CA 90084-4134
Credit: Visa MasterCard Disc Amex
Card Number:
Exp Date: CVC Code:
Signature:
7/25 $75.00CURRENT
DUE
6/1 $1350.00INSURANCE
3/14 $25.00YOU PAID
Yes Wendy, this is your bill.
6/15 $100.00PREVIOUS BALANCE
HEALTH SUMMARY: On July 25th, 2016 you had an office visit with your heart doctor, Dr.
Levi. Dr. Levi assessed you in the clinic, performed an EKG, echocardiogram, and CT Scan to
understand the health of your heart, adjusted your medications, and ordered lab tests to
ensure your medications were working as planned.
EMAIL YOUR PROVIDER: MyChart.Renown.org HEALTHY LIVING TIPS: BestMedicineNews.org
REASON FOR VISIT:Visit Renown.org for interactive map
Heart Checkup
WELLNESS CHECKLIST: Mammogram (Done 4/1)
Pneumonia Shot (Due 9/1)
Colonoscopy (Due 10/1)
Eye Exam (Due 10/15)
CARE PROVIDED: Physical Exam (7/25)
Flu Shot (7/25)
EKG (7/25) and CT-Scan (7/25)
Echocardiogram (7/26)
Blood Work (7/28)
MYCHART VISIT VITALS: Weight: 130
BMI: 22
Blood Pressure: 120/80
Pulse: 80
VISIT INFORMATION: Provider: Dr. Levi
Dates: 7/25
Location: 75 Pringle
Number of Visits Included: 1
Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
HEALTH SUMMARY
Heart Visit
Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
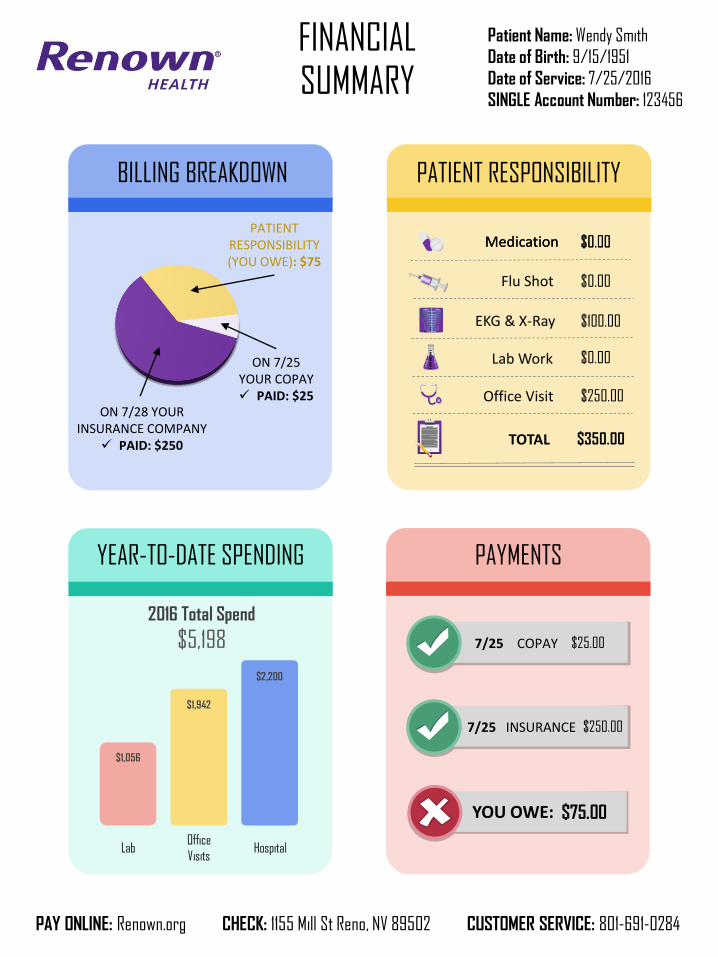
BILLING BREAKDOWN
ON 7/28 YOUR INSURANCE COMPANY PAID: $250
PATIENT RESPONSIBILITY(YOU OWE): $75
ON 7/25 YOUR COPAY PAID: $25
FINANCIAL SUMMARY
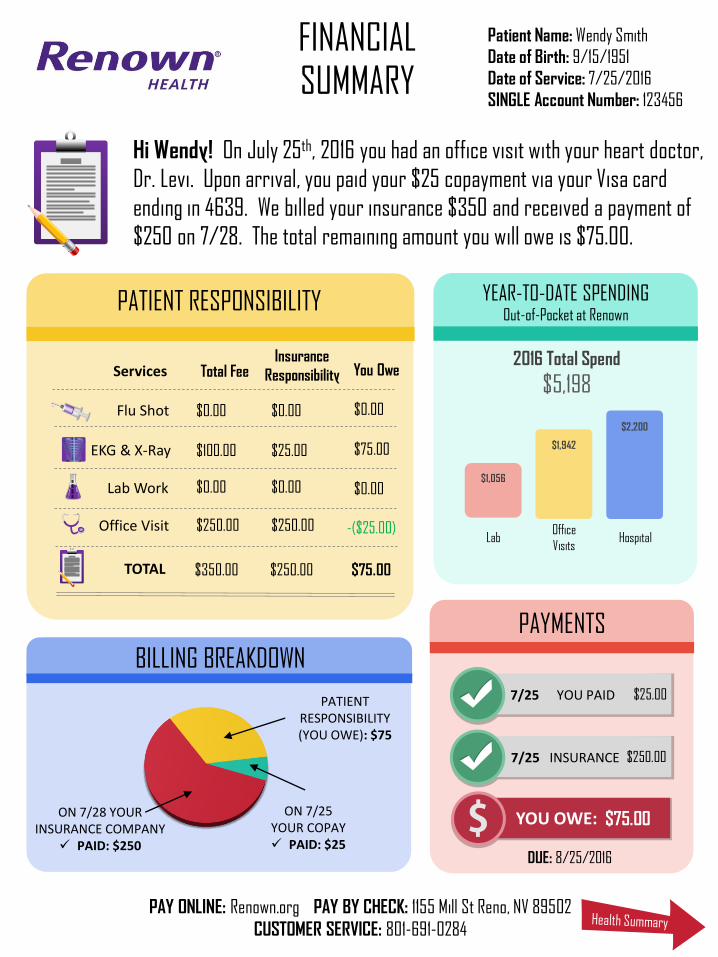
PAYMENTS
7/25 $25.00YOU PAID
7/25 $250.00INSURANCE
PAY ONLINE: Renown.org PAY BY CHECK: 1155 Mill St Reno, NV 89502
CUSTOMER SERVICE: 801-691-0284
$1,056
$1,942
$2,200
LabOffice
VisitsHospital
2016 Total Spend
$5,198
YEAR-TO-DATE SPENDINGOut-of-Pocket at Renown
$75.00YOU OWE:
Hi Wendy! On July 25th, 2016 you had an office visit with your heart doctor,
Dr. Levi. Upon arrival, you paid your $25 copayment via your Visa card
ending in 4639. We billed your insurance $350 and received a payment of
$250 on 7/28. The total remaining amount you will owe is $75.00.
Services
$350.00TOTAL
Total Fee
EKG & X-Ray $100.00
Lab Work $0.00
Office Visit $250.00
Flu Shot $0.00
PATIENT RESPONSIBILITY
Insurance
Responsibility
$25.00
$0.00
$250.00
$0.00
You Owe
$75.00
$0.00
-($25.00)
$0.00
$250.00 $75.00
DUE: 8/25/2016

Hi Wendy! On July 25th, 2016 you had an office visit with your heart
doctor, Dr. Levi. Dr. Levi assessed you in the clinic, performed an EKG to
understand the health of your heart, adjusted your medications, and
ordered lab tests to ensure your medications were working as planned.
MYCHART.RENOWN.ORG BESTMEDICINENEWS.ORG
REASON FOR VISIT:Visit Renown.org for interactive map
Heart Checkup
WELLNESS CHECKLIST: Mammogram (Done 4/1)
Pnemonia Shot (Due 9/1)
Colonoscopy (Due 10/1)
Eye Exam (Due 10/15)
CARE PROVIDED: Physical Exam
Flu Shot
EKG and X-Ray
Blood Work
TRACK MY VITALS: Weight: 130
BMI: 22
Blood Pressure: 120/80
Pulse: 80
VISIT INFORMATION: Provider: Dr. Levi
Dates: 7/25
Location: 75 Pringle
Number of Visits Included: 1
Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
HEALTH SUMMARY
Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
BILLING BREAKDOWN
Medication
$350.00TOTAL
$0.00
EKG & X-Ray $100.00
Lab Work $0.00
Office Visit $250.00
Flu Shot $0.00
PATIENT RESPONSIBILITY
ON 7/28 YOUR INSURANCE COMPANY PAID: $250
PATIENT RESPONSIBILITY(YOU OWE): $75
ON 7/25 YOUR COPAY PAID: $25
FINANCIAL SUMMARY
Medication $0.00
PAYMENTS
7/25 $25.00COPAY
7/25 $250.00INSURANCE
$75.00YOU OWE:
PAY ONLINE: Renown.org CHECK: 1155 Mill St Reno, NV 89502 CUSTOMER SERVICE: 801-691-0284
$1,056
$1,942
$2,200
LabOffice
VisitsHospital
2016 Total Spend
$5,198
YEAR-TO-DATE SPENDING

Hi Wendy! On July 25th, 2016 you had an office visit with your heart
doctor, Dr. Levi. Dr. Levi assessed you in the clinic, performed an EKG to
understand the health of your heart, adjusted your medications, and
ordered lab tests to ensure your medications were working as planned.
MYCHART.RENOWN.ORG BESTMEDICINENEWS.ORG
REASON FOR VISIT:Visit Renown.org for interactive map
Heart Checkup
WELLNESS CHECKLIST: Mammogram (Done 4/1)
Flu Shot (Due 9/1)
Colonoscopy (Due 10/1)
Eye Exam (Due 10/15)
CARE PROVIDED: Physical Exam
Flu Shot
EKG and X-Ray
Blood Work
TRACK MY VITALS: Weight: 130
BMI: 22
Blood Pressure: 120/80
Pulse: 80
VISIT INFORMATION Provider: Dr. Levi
Dates: 7/25
Location: 75 Pringle
Number of Visits Included: 1
Patient Name: Wendy Smith
Date of Birth: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
HEALTH SUMMARY

FINANCIAL SUMMARY
NAME: John Smith
DOB: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456
DUE DATE: Aug 25th, 2016
YOUR INSURANCE
COMPANY HAS PAID: $250
YOU OWE: $75
BILLING BREAKDOWN:
YOU PREVIOUSLY PAID: $25
RENOWN
CUSTOMER SERVICE:
866-691-0284
PATIENT RESPONSIBILITY:Based Upon Hometown Health Insurance:
$0.00
$0.00
$100.00
$0.00
($25.00) -Paid
Medication Reconciliation
Flu Shot
EKG and X-Ray
Blood Work
Office Visit
ANNUAL SUMMARY:What You’ve Actually Paid Renown
Office Visits: $2,500
Hospital: $1,800
Lab Services: $1,500 PAY NOW:
Online: Renown.org/PayNow
Check: 1155 Mill St Reno, NV 89502
YOU OWE:
PREVIOUS BALANCE:
$75.00AMOUNT
OWED FOR THIS SERVICE
$125.00
$200.00

Series 2WENDY’S WELLNESS LIST:
HEALTHSUMMARY
CARE PROVIDED:
Medication Reconciliation (7/25)
Flu Shot (7/25)
Vitals, EKG, Chest X-Ray (7/26)
Blood Work (7/26)
Physical Exam (7/25)
REASON FOR VISIT:Visit Renown.org for interactive map
2016 Mammogram (Done 4/1)
Flu Shot (Due 9/1)
Colonoscopy (Due 10/1)
Eye Exam (Due 10/15)
Heart Visit
Hi Wendy! On July 25th, 2016 you had an office visit with your heart
doctor, Dr. Levi. Dr. Levi assessed you in the clinic, performed an EKG to
understand the health of your heart, adjusted your medications, and
ordered lab tests to ensure your medications were working as planned.
ACCOUNT SUMMARY:Turn Page for Additional Detail
DUE DATE: Aug 25th, 2016
YOU OWE:
PREVIOUS BALANCE:
$75.00AMOUNT
OWED FOR THIS SERVICE
$125.00
$200.00
NAME: John Smith
DOB: 9/15/1951
Date of Service: 7/25/2016
SINGLE Account Number: 123456

Information, Layout and Aesthetic of Patient BillFront Page
Balance, Due Date and Statement Date are at the top, clear and prominent
Patient Information and what was done is at the top, in
bullets, and is easily understood
Visit Charges, Patient Balance, and Account Status, detailing only absolutely necessary
information, is displayed. Insurance
payment, copayment, previous balance, and
current patient balance are detailed, with most
important numbers highlighted
Patient Deductible, based upon insurance benefits, and current
annual healthcare spend YTD, are outlined giving the patient up-to-date information as to the
status of out-of-pocket spend. Visuals make the
information easy to understand
Payment Options, with easy to follow
instructions and payment plans, clearly outline actions needed
Prominent Contact Us information is outlined in the event of billing questions, financial assistance needs, and payment arrangements
A summary narrative, written in common language, explains
exactly what has been billed, paid and is still
owed

Information, Layout and Aesthetic of Patient BillBack Page
Patient Information and what was done is at the top, in
bullets, and is easily understood
A summary narrative, written in common language, explains
exactly the care that was provided and the tests that were performed
Visit Information, outlined in bullet points, defines the episode of care that the patient
received
Wellness Checklist, outlining all of the
patients overdue health maintenance gaps in
care, is listed and will be sent in with payment. Requests can be made
for Renown Patient Outreach to contact the patient for scheduling.
Prominent Contact Us information is outlined in the event of non-urgent medical questions, or the desire for healthy living tips.
Because patients receive care from many
providers, Care Provided, lists all care
that the patient received
MyChart Visit Vitals are detailed For patient tracking, and for a
reminder to log into Renown’s Patient Portal
An outline of the human body, with the area of focus for the patient’s
visit, is clearly and visually outlined.

Notification Email
The Pay Now button allows the patient to pay their bill
immediately without requesting additional information.
The View Statement button allows the patient to view a
detailed version of their Healthcare Statement
The Visit Charges section outlines a very basic
summary of their current and past due balance
A very simple and inviting email body makes it clear
as to what the email is requesting.

PAYMENT OPTIONS
Design A Bill YOU Can Understand at Renown Health
Summary Detail Full Information
BILLING BREAKDOWN
Summary Detail Full Information
DEDUCTIBLE
Summary Detail Full Information
VISIT CHARGES
Summary Detail Full Information
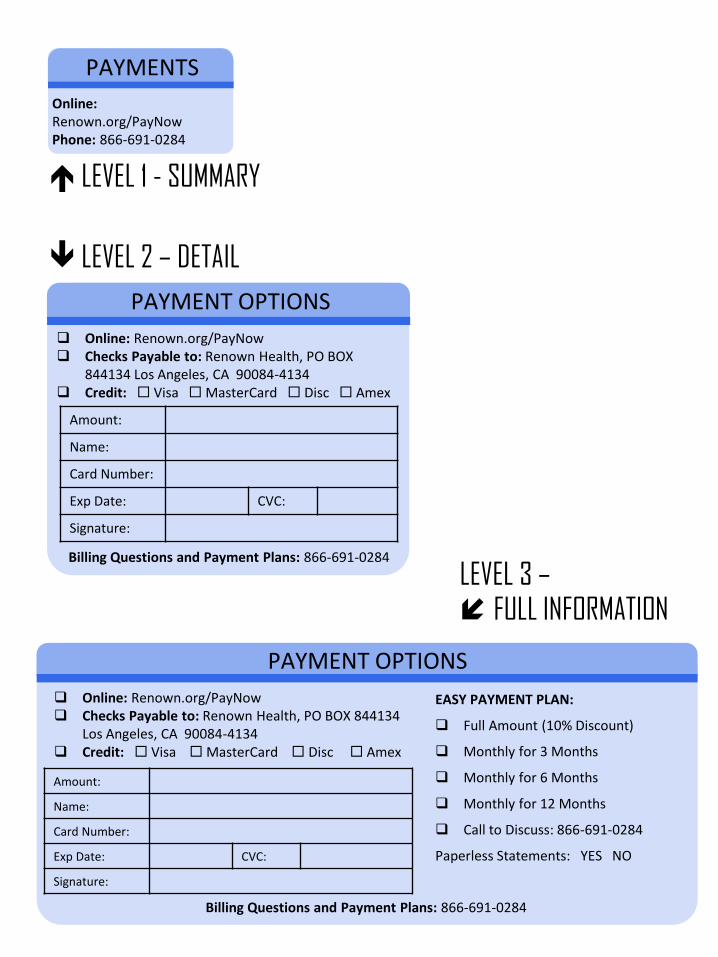
LEVEL 1 - SUMMARY
LEVEL 2 – DETAIL
LEVEL 3 – FULL INFORMATION
PAYMENTS
Online: Renown.org/PayNowPhone: 866-691-0284
PAYMENT OPTIONS
Online: Renown.org/PayNow Checks Payable to: Renown Health, PO BOX
844134 Los Angeles, CA 90084-4134 Credit: Visa MasterCard Disc Amex
Amount:
Name:
Card Number:
Exp Date: CVC:
Signature:
Billing Questions and Payment Plans: 866-691-0284
PAYMENT OPTIONS
EASY PAYMENT PLAN:
Full Amount (10% Discount)
Monthly for 3 Months
Monthly for 6 Months
Monthly for 12 Months
Call to Discuss: 866-691-0284
Paperless Statements: YES NO
Billing Questions and Payment Plans: 866-691-0284
Online: Renown.org/PayNow Checks Payable to: Renown Health, PO BOX 844134
Los Angeles, CA 90084-4134 Credit: Visa MasterCard Disc Amex
Amount:
Name:
Card Number:
Exp Date: CVC:
Signature:

BILLING BREAKDOWN
ON 7/28 YOUR INSURANCE COMPANY PAID: $1725
PATIENT RESPONSIBILITY(YOU OWE): $75
ON 7/25 YOUR COPAY PAID:
$25
BILLING BREAKDOWN
Insurance
You Owe
Copay
BILLING BREAKDOWN
INSURANCE PAID: $1725 COPAYMENT PAID: $25 PREVIOUS BALANCE: $100 YOU OWE: $175
LEVEL 1 - SUMMARY
LEVEL 2 – DETAIL
LEVEL 3 – FULL INFORMATION

LEVEL 1 -SUMMARY
LEVEL 2 –DETAIL
LEVEL 3 – FULL INFORMATION
2016 Total Spend
$5,198
DEDUCTIBLE
2016 Deductible
$9,500
DEDUCTIBLE
DEDUCTIBLE
LabOffic
e Visits
Hospital
$1,056 $1,942 $2,200
$1,300
$3,000
$4,000
2016 Total Spend
$5,1982016 Deductible
$9,500
2016 Total Spend
$5,1982016 Deductible
$9,500
Lab Office Visits
Hospital
$1,056 $1,942 $2,200
$1,300
$3,000$4,000
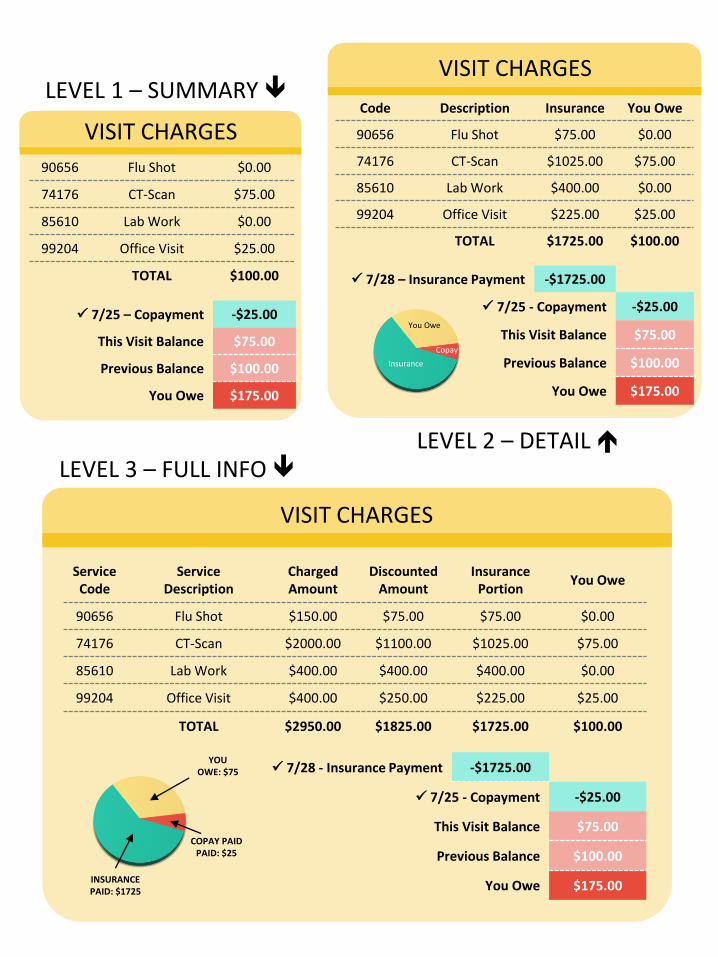
ServiceCode
Service Description
ChargedAmount
Discounted Amount
Insurance Portion
You Owe
90656 Flu Shot $150.00 $75.00 $75.00 $0.00
74176 CT-Scan $2000.00 $1100.00 $1025.00 $75.00
85610 Lab Work $400.00 $400.00 $400.00 $0.00
99204 Office Visit $400.00 $250.00 $225.00 $25.00
TOTAL $2950.00 $1825.00 $1725.00 $100.00
7/28 - Insurance Payment -$1725.00
7/25 - Copayment -$25.00
This Visit Balance $75.00
Previous Balance $100.00
You Owe $175.00
VISIT CHARGES
LEVEL 1 – SUMMARY
LEVEL 2 – DETAIL LEVEL 3 – FULL INFO
Code Description Insurance You Owe
90656 Flu Shot $75.00 $0.00
74176 CT-Scan $1025.00 $75.00
85610 Lab Work $400.00 $0.00
99204 Office Visit $225.00 $25.00
TOTAL $1725.00 $100.00
7/28 – Insurance Payment -$1725.00
7/25 - Copayment -$25.00
This Visit Balance $75.00
Previous Balance $100.00
You Owe $175.00
VISIT CHARGES
90656 Flu Shot $0.00
74176 CT-Scan $75.00
85610 Lab Work $0.00
99204 Office Visit $25.00
TOTAL $100.00
7/25 – Copayment -$25.00
This Visit Balance $75.00
Previous Balance $100.00
You Owe $175.00
VISIT CHARGES
INSURANCE PAID: $1725
YOU OWE: $75
COPAY PAIDPAID: $25
Insurance
You Owe
Copay