Embed Size (px)
Citation preview

BritishJournal ofOphthalmology, 1991,75,280-283
Visual assessment of infants: vernier targets for theCatford drum
Bryan Hopkisson, Pamela Arnold, Barbara Billinghlam, Marilyn McGarrigle, Philip Entwistle
AbstractTargets comprising a horizontal black line 5'thick offset by 1' were printed on strips to stickto the drums of the Catford Visual AcuityApparatus. The 'vernier' targets so producedcorresponded to the different sizes of Snellenletters from 6/6 to 2/60 when presented at 50cm. Twenty-five children between the ages of3and 12 years with known amblyopia (mostlystrabismic) were tested in a double blind trialto compare the visibility of the vernier targetswith subjective Snellen acuity. All vernierresults, both for better and ambfyopic eye,were within one line of Snellen acuity. Onehundred and twenty normal preverbal infantswith normal eyes under the age of 2½ yearswere tested with the vernier strips. Normalinfants under the age of 6 months recorded avision of 6/60-2/60; normal infants aged 6 to 12months recorded 6/24-6/36, and infantsbetween the ages of 1 and 2½ years recorded6/12-6/18.
Catford and Oliver' described an instrument forthe objective determination of visual acuity. Itconsisted of a motor driven drum which coulddisplay black dots of various sizes in oscillatorymotion against a white background. Acuitieswere determined by finding the smallest dotwhich could be fixed and followed by the patient.The drum dot targets were criticised becausethey subtended five' of arc and were contrasttargets, testing merely visibility, thereby giving amarked overestimate of acuity.' The drummethod was also criticised because it used amoving target which was presumed to have asynergistic effect by simultaneously exciting anew area of retina while leaving an inhibitoryarea.3The forced-choice preferential looking (FPL)
method is also used as a means of estimatingacuity and other visual detection performance ininfants."8 However, there is often a poorrelationship between Snellen letter acuity and
measures of resolution such as grating acuity.9 10Teller acuity cards do not reliably detectstrabismic amblyopia. Ii The method can be timeconsuming, variable in older infants, and difficultto interpret in the clinical situation.
Shimojo et all" described a motor sound displayto measure vernier acuity. In this display a pair ofstriped patterns was presented, one of whichcontained horizontal vernier offsets on its edges.The displacement of the vernier offsets gave theimpression of intermittent motion of a targetwhich was defined by these offsets. The motionwas perceived only when the vernier offsets weredetected. Vernier acuity, defined as the inverseofthe smallest detectable misalignment ofedges,gives a resolving power of the order of 4" of arcfor the contour break and 0-5" of arc for theline.'3 It has therefore been termed a type ofhyperacuity,'4 which may be considered an out-come of central visual processing.
Atkinson et aP' stated that in principle theybelieve the use of an ocular following response torepetitive movement of a discrete target asproposed by Catford and Oliver is a robustmethod. It offers one of the best chances of rapidand reliable acuity assessment in children agedbetween 6 months and 21/2 years if a better targetcould be found. Since vernier acuity is known tobe less than grating acuity in neonates' and instrabismic amblyopes,'5-'7 we developed targetswith vernier offsets for attachment to the Catfordmachine so that we might compare the visibilityof them with subjective Snellen acuity for agroup of amblyopic children whose acuitiescould be reliably subjectively tested. We alsorecorded the vernier vision of 120 normal pre-verbal infants with the same vernier targets.
ApparatusA black horizontal line on a white backgroundmoving horizontally is not perceived to move ifthe ends of the line are concealed. If the line hasa vernier offset and the offset is perceived, theeye may fix and follow it. If targets of decreasing
Eye Department,Northampton GeneralHospitalB HopkissonP ArnoldB BillinghamM McGarrigle
Nene College,NorthamptonP EntwistleCorrespondence to:B Hopkisson, FRCS, EyeDepartment, NorthamptonGeneral Hospital,Northampton NN1 5BD.Accepted for publication26 October 1990
1 MIN
5MINS
Figure I Snellen and vernier targets.
1 MN
5 MINS
280
on March 15, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.75.5.280 on 1 M
ay 1991. Dow
nloaded from
281Visual assessment ofinfants: vernier targetsfor the Catford drum
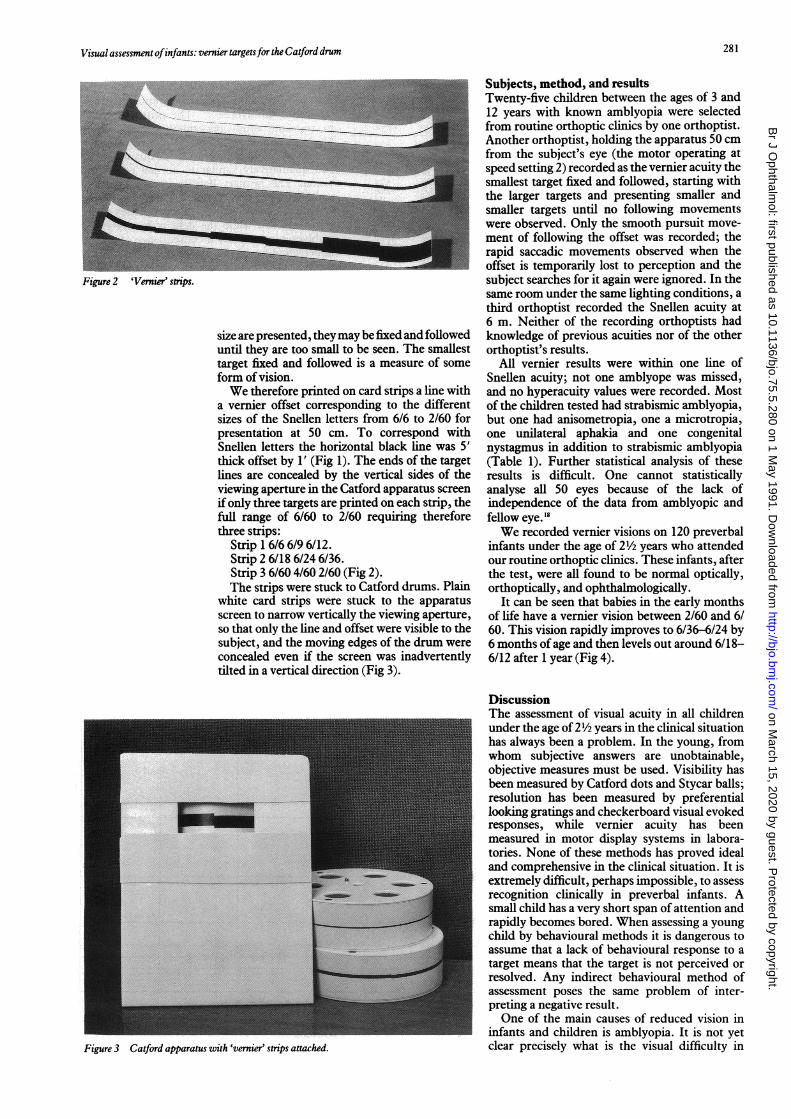
Figure 2 'Vernier' strips.
size are presented, theymay be fixed and followeduntil they are too small to be seen. The smallesttarget fixed and followed is a measure of someform of vision.
We therefore printed on card strips a line witha vernier offset corresponding to the differentsizes of the Snellen letters from 6/6 to 2/60 forpresentation at 50 cm. To correspond withSnellen letters the horizontal black line was 5'thick offset by 1' (Fig 1). The ends of the targetlines are concealed by the vertical sides of theviewing aperture in the Catford apparatus screen
ifonly three targets are printed on each strip, thefull range of 6/60 to 2/60 requiring thereforethree strips:
Strip 1 6/6 6/9 6/12.Strip 2 6/18 6/24 6/36.Strip 3 6/60 4/60 2/60 (Fig 2).The strips were stuck to Catford drums. Plain
white card strips were stuck to the apparatusscreen to narrow vertically the viewing aperture,so that only the line and offset were visible to thesubject, and the moving edges of the drum wereconcealed even if the screen was inadvertentlytilted in a vertical direction (Fig 3).
Figure 3 Catford apparatus with 'vernier' strips attached.
Subjects, method, and resultsTwenty-five children between the ages of 3 and12 years with known amblyopia were selectedfrom routine orthoptic clinics by one orthoptist.Another orthoptist, holding the apparatus 50 cmfrom the subject's eye (the motor operating atspeed setting 2) recorded as the vernier acuity thesmallest target fixed and followed, starting withthe larger targets and presenting smaller andsmaller targets until no following movementswere observed. Only the smooth pursuit move-ment of following the offset was recorded; therapid saccadic movements observed when theoffset is temporarily lost to perception and thesubject searches for it again were ignored. In thesame room under the same lighting conditions, athird orthoptist recorded the Snellen acuity at6 m. Neither of the recording orthoptists hadknowledge of previous acuities nor of the otherorthoptist's results.
All vernier results were within one line ofSnellen acuity; not one amblyope was missed,and no hyperacuity values were recorded. Mostof the children tested had strabismic amblyopia,but one had anisometropia, one a microtropia,one unilateral aphakia and one congenitalnystagmus in addition to strabismic amblyopia(Table 1). Further statistical analysis of theseresults is difficult. One cannot statisticallyanalyse all 50 eyes because of the lack ofindependence of the data from amblyopic andfellow eye. 18We recorded vernier visions on 120 preverbal
infants under the age of 2½yearss who attendedour routine orthoptic clinics. These infants, afterthe test, were all found to be normal optically,orthoptically, and ophthalmologically.
It can be seen that babies in the early monthsof life have a vernier vision between 2/60 and 6/60. This vision rapidly improves to 6/36-6/24 by6 months of age and then levels out around 6/18-6/12 after 1 year (Fig 4).
DiscussionThe assessment of visual acuity in all childrenunder the age of 21/2years in the clinical situationhas always been a problem. In the young, fromwhom subjective answers are unobtainable,objective measures must be used. Visibility hasbeen measured by Catford dots and Stycar balls;resolution has been measured by preferentiallooking gratings and checkerboard visual evokedresponses, while vernier acuity has beenmeasured in motor display systems in labora-tories. None of these methods has proved idealand comprehensive in the clinical situation. It isextremely difficult, perhaps impossible, to assessrecognition clinically in preverbal infants. Asmall child has a very short span of attention andrapidly becomes bored. When assessing a youngchild by behavioural methods it is dangerous toassume that a lack of behavioural response to atarget means that the target is not perceived orresolved. Any indirect behavioural method ofassessment poses the same problem of inter-preting a negative result.One of the main causes of reduced vision in
infants and children is amblyopia. It is not yetclear precisely what is the visual difficulty in
on March 15, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.75.5.280 on 1 M
ay 1991. Dow
nloaded from

282~~~~~~~~~~~~~~~~~~~~~~Hopkisson,Arnold, Billingham, McGarrigle, Entwistle
Table I Comparison ofacuities. Vernier strip and Snellen in 25 amblyopic children
Subject Age (years) Diagnosis Better eye Amblyopic eye
Snellen Vernier Snellen Vernier
1 11 LDS 6/6 6/6 6/18 6/182 6 RCS 6/6 6/6 6/36 6/603 5 RCS 6/6 6/6 6/24 6/244 4 LCS 6/9 6/12 6/36 6/605 4 LCS 6/6 6/9 6/36 6/246 6 LCS 6/9 6/12 4/60 2/607 12 RCS 6/6 6/6 6/18 6/188 5 RCSCongenital 6/18 6/18 2/60 2/60
nystagmus9 6 Left aphakia cCL 6/6 6/6 6/36 6/3610 5 LCS 6/6 6/6 <1/60 <2/6011 6 RCS 6/9 6/12 6/18 6/2412 7 LCS 6/6 6/9 6/18 6/2413 6 LCS 6/6 6/9 6/18 6/1214 6 RCS 6/6 6/6 6/18 6/2415 5 Left microtropia 6/9 6/9 6/18 6/1816 4 Left anisometropia 6/9 6/9 6/60 6/3617 6 LCS 6/9 6/9 6/18 6/1818 4 LCS UR 6/6 6/9 2/60 <2/6019 6 LCS 6/6 6/9 6/12 6/1220 6 LCS 6/6 6/9 6/36 6/2421 5 LCS 6/6 6/9 6/18 6/2422 3 RCS 6/12 6/18 6/60 6/3623 5 RCS 6/6 6/9 6/24 6/1824 8 LCS 6/6 6/9 6/24 6/1825 3 RCS 6/9 6/9 6/18 6/18
LDS=left divergent squint. LGS=left convergent squint. RCS=right convergent squint.c CL with contact lens. UJR left over right.
amblyopia, but there is considerable evidencethat it is not simply blurring of the image.""'1Strabismic amblyopes, and neonates both behavesimilarly when faced with vernier targets.'21-1
Grating acuity may depend on the smallest sizeof receptor field that shows functionally effectivecontrast sensitivity.7' Vernier acuity requiresdetection of offsets and may depend more on thedensity of receptor fields than on the size ofthem.20 It deteriorates two to three times fasterthan grating acuity in the normal retinal peni-
2/60
VERNIERVISION
4/60
6/60
6/36
6/24
6/18
6/12d6/96/6
phery as a function of retinal eccentricity,'72'1 andit is also degraded more than grating acuity instrabismic amblyopia.'"'7 The primary deficitsin strabismic amblyopia cannot be mimicked byblur and cannot be explained solely by filteringproperties. Rather they are both quantitativelyand qualitatively similar to normal peripheralvision. The primary deficits in anisometropicamblyopia can be accounted for by the spatialfiltering and contrast response properties of thevisual system, while the deficits in strabismicamblyopia are mainly a consequence of spatialundersampling as in neonatal vision.'7 Sincevernier and grating acuities reflect differentaspects of visual sampling and early processing,the comparison between them within individualinfants may serve as a significant critical testduring the first year of life.20 Because of theundersampling coificept perhaps our vernier typetargets may be more clinically useful in earlyinfancy and strabismic amblyopia than preferen-tial looking gratings.Our targets cannot possibly be measuring true
vernier hyperacuity, as no gross hyperacuityvalues are obtained in comparison with Snellenacuity in amblyopic children. There appears tobe no overestimate of vision produced by ourmoving targets. Indeed it has been shown thatthere is no significant difference between visualacuities with static and phase alternated targets.22The drum method of vision testing has been
recognised as offering one of the best chances ofrapid and reliable assessment of vision in smallchildren if a better target could be devised. Weknow that the Catford apparatus is robust andhas stood the test oftime in mechanical reliability.
1 2 3 4 5 6 7 a 9 10 I1I1 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
AGE IN MONTHS* BINOCMtARo MONOCULAR
Figure 4 120 normal infants: development of 'vernier' vision.
282
on March 15, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.75.5.280 on 1 M
ay 1991. Dow
nloaded from

Visual assessment ofinfants: vernier targetsfor the Catforddrum
We know that most orthoptists are familiar withthe apparatus and find it simple, quick, and easyto use in the clinical situation. We believe that wehave developed a target for the Catford drumwhich gives a clinically good and useful visualvalue in young children and indeed in olderchildren who cannot be formally tested by otherquick, easy methods in the clinical situation. Thestrips are cheap and replaceable when soiled;they are easily attached to the drums by doublesided sticky tape or glue.We have found a knowledge of our vernier
vision in normal babies, in babies with squint, inanisometropia and some pathological conditionsis clinically useful. We can certainly record theimprovement in vision in the amblyopic eye ofpreverbal children after occlusive therapy, andwe are confidently able to discharge from follow-up children with pseudosquint who have beenfound to have equally good vision in each eyemuch earlier than previously.We are sure that there will be exceptions and
difficult cases to assess with our targets, especiallysome cases with ocular motility problems, but wehave certainly been able to record accuratevisions of some children with congenitalnystagmus.We do not pretend to understand fully the
physiological reasons for our targets giving aclinically reasonable correlation with Snellentargets, but we believe this method of visualassessment warrants further investigation toestablish the true extent of its potential.
We thank Mr G V Catford for his help and encouragement in this
project.
1 Catford GV, Oliver A. Development of visual acuity. Arch DisChild 1973; 48: 47-50.
2 Atkinson J, Braddick 0, Pimm-Smith E, Ayling L, Sawyer R.Does the Catford drum give an accurate assessment ofacuity? BrJ Ophthalmol 1981; 65: 652-6.
3 Khan SG, Chen KF, Frenkel M: Subjective and objectivevisual acuity testing techniques. Arch Ophthalmol 1976; 94:2086-91.
4 Teller DY, Morse R, Borton R, Regal D. Visual acuity forvertical and diagonal gratings in human infants. Vision Res1974; 14: 1433-9.
5 Teller DY. The forced-choice preferential looking procedure:a psychophysical technique for use with human infants.Infant BehavDev 1979; 2:135-53.
6 Atkinson J, Braddick 0, Moar K. Development of contrastsensitivity over the first 3 months of life in the human infant.Vision Res 1977; 17: 1037-44.
7 Banks MS, Salapatek P. Acuity and contrast sensitivity in 1-,2-, and 3-month-old human infants. Invest Ophthalmol VisSci 1978; 17: 361-5.
8 Gwiazda J, Brill S, Mohindra I, Held R. Infant visual acuityand its meridional variation. Vision Res 1978; 18: 1557-64.
9 Hess RF, Cambell FW, Greenhalgh T. On the nature of theneural abnormality in human amblyopia; neural aberrationsand neural sensitivity loss. Pflugers Arch 1978; 377: 201-7.
10 Hess RF, Jenkins S. Amblyopia cannot be explained byconsidering only detection thresholds. Perception 1980; 9:569-76.
11 Katz B, Sireteanu R. Teller acuity card test. Klin MonatsblAugenheilkd 1989; 195: 17-22.
12 Shimojo S, Birch EE, Gwiazda J, Held R. Development ofvernier acuity in infants. Vision Res 1984; 24: 721-8.
13 Davson H. Physiology of the eye.2nd ed. London: Churchill1963:168.
14 Westheimer G. The spatial sense of the eye. Invest OphthalmolVisSci 1979; 18: 893-912.
15 Levi DM, Klein SA. Hyperacuity and amblyopia. Nature1982; 298: 268-70.
16 Levi DM, Klein SA. Differences in vernier discrimination forgratings between strabismic and anisometropic amblyopes.Invest Ophthalmol Vis Sci 1982; 23: 398-407.
17 Levi DM, Klein SA. Vernier acuity, crowding and amblyopia.Vision Res 1985; 25: 979-91.
18 Ray WA, O'Day DM. Statistical analysis of multi-eye data inophthalmic research Invest Ophthalmol Vis Sci 1985; 26:1186-8.
19 Atkinson J, Braddick 0, Braddick F. Acuity and contrastsensitivity of infant vision. Nature 1974; 247: 403.
20 Shimojo S, Held R. Vernier acuity is less than grating acuity in2- and 3-month-olds. Vision Res 1987; 27: 77-86.
21 Westheimer G. The spatial grain of the perifoveal visual field.Vision Res 1982; 22: 157-62.
22 Dobson V, Teller DY, Belgum J. Visual acuity in humaninfants assessed with stationary stripes and phase-alternatedcheckerboards. Vision Res 1978; 18: 1233-8.
283
on March 15, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.75.5.280 on 1 M
ay 1991. Dow
nloaded from


























![[Drum] Bob Moses - Drum Wisdom](https://img.dokumen.tips/doc/110x75/577cbfd31a28aba7118e36ec/drum-bob-moses-drum-wisdom.jpg)
![[Drum] Colin Bailey - Bass Drum Control](https://img.dokumen.tips/doc/110x75/5571f30449795947648d5ee9/drum-colin-bailey-bass-drum-control.jpg)

