Embed Size (px)
Citation preview

Review
DEPRESSION AND ANXIETY 27 : 933–944 (2010)
VIRTUAL REALITY EXPOSURE THERAPY IN ANXIETYDISORDERS: A SYSTEMATIC REVIEW
OF PROCESS-AND-OUTCOME STUDIES
Katharina Meyerbroker, M.Sc.� and Paul M.G. Emmelkamp, Ph.D.
In recent years, virtual reality exposure therapy (VRET) has become aninteresting alternative for the treatment of anxiety disorders. Research hasfocused on the efficacy of VRET in treating anxiety disorders: phobias, panicdisorder, and posttraumatic stress disorder. In this systematic review, strictmethodological criteria are used to give an overview of the controlled trialsregarding the efficacy of VRET in patients with anxiety disorders. Furthermore,research into process variables such as the therapeutic alliance and cognitionsand enhancement of therapy effects through cognitive enhancers is discussed.The implications for implementation into clinical practice are considered.Depression and Anxiety 27:933–944, 2010. rr 2010 Wiley-Liss, Inc.
Key words: virtual reality exposure therapy; anxiety; exposure; efficacy;mechanisms
In the past 10 years, virtual reality exposure therapy(VRET) has become an interesting alternative forexposure in vivo in treating anxiety disorders, morespecifically in treating specific phobias.[1,2] VRET isregarded as a natural extension of the systematicexposure component of behavior therapy.[3] Especiallyin specific phobias VRET has been found to be at leastas effective as the state-of-the-art treatment exposurein vivo.[1] Although a number of studies has investi-gated the outcome and to a lesser extent the process ofVRET, not all studies meet stringent methodologicalcriteria and are externally valid.[4] Moreover, most ofthe randomized controlled trials (RCTs) within thisresearch field have been limited to subjects withacrophobia and fear of flying. Research concerningthe efficacy of VRET in other (anxiety) disorders is stillin its infancy.
Quite little is known about therapeutic processesinvolved in VRET. Very few studies have addressedemotional processing, cognitive processes, or psycho-physiology during VRET. Another important aspect,which still has been neglected in this field, is the role ofthe therapeutic alliance in VRET. Although thetherapeutic alliance has been the most studied variablein other psychological interventions,[5] only one studyexplicitly addressed the role of the therapeutic alliancein VRET.[6] The first aim of this article is to provide anoverview of studies into the efficacy of VRET; we limitourselves to the discussion of studies with high
methodological criteria and validity. For an overviewabout the technical possibilities we refer to Krijn andcolleagues, who provided a solid survey of the differentsystems of VRET.[7] A second objective of this review isto give an overview of research that investigatesmechanisms of VRET, including cognitive processes,psychophysiology, and the therapeutic alliance.
THE EFFICACY OF VRETAlthough a lot of research has been published on the
efficacy of VRETwe will confine our discussion to thecontrolled studies in this field. To ensure a systematicoverview, the following search strategy was applied.
Published online 23 August 2010 in Wiley Online Library
(wileyonlinelibrary.com).
DOI 10.1002/da.20734
Received for publication 2 April 2010; Revised 30 June 2010;
Accepted 1 July 2010
�Correspondence to: Katharina Meyerbroker, Department of Clinical
Psychology, University of Amsterdam, Roetersstraat 15, 1018 WB
Amsterdam, The Netherlands. E-mail: [email protected]
The authors report they have no financial relationships within the past
3 year to disclose.
Department of Clinical Psychology, University of Amsterdam,
Amsterdam, The Netherlands
rr 2010 Wiley-Liss, Inc.
A computer-assisted search of the databases PsychInfo,Pubmed, Web of Science, and Academic SearchPremier was conducted with the following searchterms: ‘‘VRET’’ alone AND in combination with‘‘efficacy, effectiveness, specific phobias, panic disorder,social phobia, agoraphobia, generalized anxiety dis-order, obsessive compulsive disorder, posttraumaticstress disorder (PTSD), process, mechanism ofchange, underlying mechanism, mechanism, therapeu-tic process.’’
The search was continued by using the ‘‘snowballmethod.’’ All studies retrieved were analyzed by bothauthors. To enhance a high quality of clinically relevantand methodologically well conducted studies, thefollowing inclusion criteria were applied:
* Studies should focus on the efficacy or effectivenessor process of VRET.
* Only studies with at least two different conditionswill be included (experimental group vs. controlcondition). The control group existed either ofanother type of intervention or a waitlist control.
* Only studies, which report original empirical find-ings, and those that are published in a peer-reviewedjournal or proceedings will be included.
* Only articles written in English will be included.
Studies were excluded, if they:
* Assess effectiveness or efficacy of VRET in a non-clinical population, whose subjects are not sufferingfrom an anxiety disorder at the time of the study(e.g. college students).
* Case-studies.* Data reported based on relatively small sample size
(Nr10) in the VRET condition.
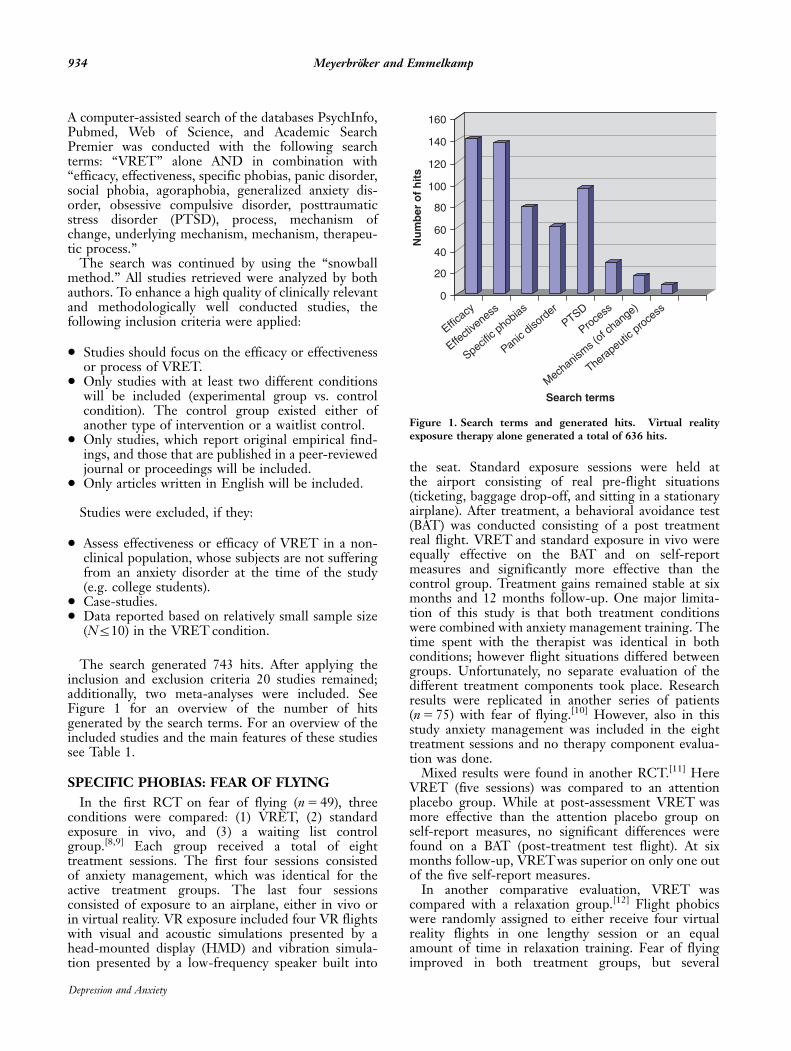
The search generated 743 hits. After applying theinclusion and exclusion criteria 20 studies remained;additionally, two meta-analyses were included. SeeFigure 1 for an overview of the number of hitsgenerated by the search terms. For an overview of theincluded studies and the main features of these studiessee Table 1.
SPECIFIC PHOBIAS: FEAR OF FLYING
In the first RCT on fear of flying (n 5 49), threeconditions were compared: (1) VRET, (2) standardexposure in vivo, and (3) a waiting list controlgroup.[8,9] Each group received a total of eighttreatment sessions. The first four sessions consistedof anxiety management, which was identical for theactive treatment groups. The last four sessionsconsisted of exposure to an airplane, either in vivo orin virtual reality. VR exposure included four VR flightswith visual and acoustic simulations presented by ahead-mounted display (HMD) and vibration simula-tion presented by a low-frequency speaker built into
the seat. Standard exposure sessions were held atthe airport consisting of real pre-flight situations(ticketing, baggage drop-off, and sitting in a stationaryairplane). After treatment, a behavioral avoidance test(BAT) was conducted consisting of a post treatmentreal flight. VRET and standard exposure in vivo wereequally effective on the BAT and on self-reportmeasures and significantly more effective than thecontrol group. Treatment gains remained stable at sixmonths and 12 months follow-up. One major limita-tion of this study is that both treatment conditionswere combined with anxiety management training. Thetime spent with the therapist was identical in bothconditions; however flight situations differed betweengroups. Unfortunately, no separate evaluation of thedifferent treatment components took place. Researchresults were replicated in another series of patients(n 5 75) with fear of flying.[10] However, also in thisstudy anxiety management was included in the eighttreatment sessions and no therapy component evalua-tion was done.
Mixed results were found in another RCT.[11] HereVRET (five sessions) was compared to an attentionplacebo group. While at post-assessment VRET wasmore effective than the attention placebo group onself-report measures, no significant differences werefound on a BAT (post-treatment test flight). At sixmonths follow-up, VRETwas superior on only one outof the five self-report measures.
In another comparative evaluation, VRET wascompared with a relaxation group.[12] Flight phobicswere randomly assigned to either receive four virtualreality flights in one lengthy session or an equalamount of time in relaxation training. Fear of flyingimproved in both treatment groups, but several
0
20
40
60
80
100
120
140
160
Nu
mb
er o
f h
its
Efficacy
Effecti
veness
Specific
phobias
Panic diso
rder
PTSD
Process
Mechanism
s (of c
hange)
Therapeutic proce
ss
Search terms
Figure 1. Search terms and generated hits. �Virtual realityexposure therapy alone generated a total of 636 hits.
934 Meyerbroker and Emmelkamp
Depression and Anxiety
outcome measures indicated greater effects in the VRcondition than in the relaxation condition includingself-ratings of fear of flying and avoidance of flying andphysiological fear responses.
In a study on one-session treatment of fear of flying,a combination of cognitive behavior therapy (CBT plusVRET with or without motion simulation) was super-ior to CBT.[13] Results of the combination treatmentwere superior to results of a non-randomized controlgroup; results of CBT alone were not superior. Motionsimulation did not enhance efficacy of VRET. Resultsremained stable at six-month follow-up. However,group differences in self-initiated flights during thefollow-up period did not reach significance. Limita-tions of this study include substantial difference in thetime spent with the therapist: in the combinedcondition, subjects spent approximately 140 min withtheir therapist, while in the CBT conditions subjectsspent only 60 min with their therapist. Time in therapyand the attention received by the therapist during thistime may distort results in favor of the combinedgroup. Another limitation is that the allocation to thecontrol group was not randomized, which makesresults difficult to interpret.
Another study evaluated the long-term effects ofonly one treatment session.[14] During a test flightafter treatment subjects were either accompanied by atherapist or not. All subjects (n 5 30) received onesession of VRET (four successive VR flights of 18 mineach). These results indicate that the attention or thepresence of a therapist during a test flight did notenhance the capability of clients to fly. Results werestable at 12-months follow-up. Seventy seven percentof the whole group was able to take the graduationflight after only one treatment session; there were nodifferences between both conditions.
In a comparison of VRETwith imaginal exposure, itwas found that eight sessions of VRET were moreeffective than eight sessions of imaginal exposure.[15]
Further, VRET plus biofeedback (feedback based onphysiological monitoring) was more effective thanVRET without biofeedback.[16] Finally, four sessionsof VRET were compared with four sessions of CBT,and with bibliotherapy over a five-week period.[17] Allsubjects received a psycho-educative book about fear offlying. At the intermediate test, both VRET and CBTwere superior to bibliotherapy. All participants receivedin addition a two-day CBT program in groups of fiveto eight participants, including exposure in vivoconsisting of a real flight from Amsterdam to Italy.Although at the intermediate test, no differencesbetween VRET and CBT were found, results at thepost-test indicated that CBT plus group interventionwas superior to VRET plus groups intervention.Unfortunately, the number of drop-outs was very high,especially in the VRET condition. However, intent totreat analyses did not show different patterns than thecompleters analyses. Post hoc analyses revealed thatindividual CBT and bibliotherapy enhanced positive
cognitions about flying while VRET and the groupintervention lessened negative cognitions.
SPECIFIC PHOBIAS: ACROPHOBIA
The first clinical trial on VRET with acrophobiainvolved a within group design.[18] Ten patients werefirst treated with two sessions of VRET followed bytwo sessions of exposure in vivo. Virtual realityexposure was found to be at least as effective asexposure in vivo on anxiety and avoidance. In afollowing study by the same research group, VRETand exposure in vivo were compared in a RCT.[19] Toenhance the comparability of the exposure conditions,virtual environments and real life situations wereidentical. Subjects (n 5 33) were randomly assigned toeither three sessions of VRET or three sessions ofexposure in vivo. Measures also included a BAT at postassessment. Results indicated that both treatmentswere equally effective and that practicing in a virtualenvironment did generalize to the real world asassessed with a BAT. Results were maintained at six-months follow-up.
In another study done by this group, the effectivenessof different VRET systems was investigated.[20] Sub-jects (n 5 37) with acrophobia were randomly assignedto either VRET administered by a HMD, or acomputer animated virtual environment (CAVE), or awaitlist control group. Subjects in the active treatmentconditions received three sessions of one hour each.After the waiting period, subjects were randomlyassigned to one of the active treatment conditions.Results showed no differences between the activetreatment conditions on any of the measures. However,in the CAVE condition, subjects experienced morepresence than in the HMD condition, but that did notinfluence the effectiveness of the therapy.
In a following study, the role of cognitive self-statements was investigated.[21] In a cross-over design,subjects with acrophobia (n 5 26) were randomlyassigned to either (1) two sessions of VRET followedby two sessions of VRETwith cognitive self-statementsor (2) two sessions of VRET with cognitive self-statements followed by VRET. Thus, all subjectsreceived a total of four sessions. Results showed thatthe addition of cognitive self-statements did notenhance the effectiveness of VRET.
SOCIAL PHOBIA
While in studies done with subjects with fear offlying or acrophobia, the treatment focus is only onfeared situations, in more complex phobias such associal anxiety different aspects have to be taken intoaccount as well. In social anxiety, not only the phobicsituation plays an important role but also how thesubject is evaluated by others participating in thesituation (e.g. giving a presentation is anxiety provok-ing, but also the (negative) evaluation from otherscauses anxiety). Given the complexity of social phobia,
935Review: Virtual Reality Exposure Therapy
Depression and Anxiety

TA
BL
E1.
Ove
rvie
wo
utc
om
est
ud
ies
VR
ET
Stu
dy
NC
lin
ical
sam
ple
Des
ign
Co
nd
itio
n(N
)N
o.
sess
ion
sP
rim
ary
ou
tco
me
mea
sure
Po
stas
sess
men
tF
oll
ow
-up
Spe
cifi
cph
obia
sE
mm
elka
mp
10A
cro
ph
ob
iaW
ith
in-s
ub
ject
sV
RE
T(N
510
)2
AQ
VR
ET
5In
Viv
oa
No
etal
.[18]
des
ign
InV
ivo
Exp
osu
re(N
510
)2
AT
HQ
Em
mel
kam
p33
Acr
op
ho
bia
RC
TV
RE
T(N
517
)3
BA
TV
RE
T5
InV
ivo
6m
on
ths,
stab
leet
al.[1
9]
InV
ivo
Exp
osu
re(N
516
)3
AQ
AT
HQ
Kri
jnet
al.[7
]37
Acr
op
ho
bia
RC
TV
RE
T:
HM
D(N
510
)3
BA
TH
MD
5C
AV
E4
WL
b6
mo
nth
s,st
able
VR
ET
:C
AV
E(N
514
)3
AQ
WL
-co
ntr
ol
(N5
11)
AT
HQ
Kri
jnet
al.[2
1]
26A
cro
ph
ob
iaC
ross
ove
rd
esig
nV
RE
T1
VR
ET
CS
S(N
514
)4
AQ
VR
ET
5V
RE
TC
SS
6m
on
ths,
stab
leV
RE
TC
SS
1V
RE
T(N
512
)4
AT
HQ
Kri
jnet
al.[1
7]
59F
ear
of
flyi
ng
RC
TV
RE
T(N
530
)4
FA
SV
RE
T5
CB
TN
oC
BT
(N5
23)
2–4
FA
MV
RE
T4
Bib
Bib
lio
ther
apy
(N5
19)
CB
T4
Bib
Mal
tby
etal
.[11]
45F
ear
of
flyi
ng
RC
TV
RE
T(N
520
)5
BA
TV
RE
T4
AP
GT
6m
on
ths,
resu
lts
Att
enti
on
pla
ceb
o(N
523
)5
FA
Sw
ere
no
tst
able
,F
AM
VR
ET4
AP
GT
on
FH
Fo
nly
on
em
easu
reM
uh
lber
ger
30F
ear
of
flyi
ng
RC
TV
RE
T(N
515
)1
FF
SV
RE
T5
Rel
axat
ion
No
etal
.[12]
Rel
axat
ion
(N5
15)
1G
FF
QM
uh
lber
ger
45F
ear
of
flyi
ng
RC
TV
RC
BT
1M
S(N
513
)1
BA
TV
RC
BT4
CB
T,
6m
on
ths,
stab
lefo
ret
al.[1
3]
VR
CB
T�
MS
(N5
13)
1F
FS
MS
5n
oV
RC
BT
CB
T(N
511
)1
GF
FQ
dif
fere
nce4
WL
WL
-co
ntr
ol
(10)
Mu
hlb
erge
ret
al.[1
4]
30F
ear
of
flyi
ng
RC
TF
ligh
t1
year
foll
ow
-up
alo
ne
(N5
15)
1 1B
AT
FF
SV
RE
Tal
on
e5
VR
ET
acc
12
mo
nth
s,st
able
Fli
ght
1ye
arfo
llo
w-u
pw
ith
ther
apis
t(N
515
)G
FF
Q
Ro
thb
aum
49F
ear
of
flyi
ng
RC
TV
RE
T(N
515
)8
BA
TV
RE
T5
SE
,V
RE
T4
WL
,6
and
12
mo
nth
s,st
able
etal
.[8,9
]st
and
ard
exp
osu
re(N
515
)8
QA
TF
SE4
WL
WL
-co
ntr
ol
(N5
15)
FF
IR
oth
bau
m75
Fea
ro
ffl
yin
gR
CT
VR
ET
(N5
32)
8B
AT
VR
ET
5S
E,
VR
ET4
WL
,6
–12
mo
nth
s,st
able
etal
.[10]
stan
dar
dex
po
sure
(N5
34)
8Q
AT
FS
E4
WL
WL
-co
ntr
ol
(N5
25)
FF
IW
ied
erh
old
and
30F
ear
of
flyi
ng
RC
TV
RE
T(N
510
)c8
EE
GV
RE
T1
bio
feed
bac
k43
year
s,st
able
Wie
der
ho
ld[1
5]
VR
ET
1b
iofe
edb
ack
(N5
10)c
8B
WM
VR
ET4
IET
Imag
inal
exp
osu
re(N
510
)c8
RR
SR
HR
ST
936 Meyerbroker and Emmelkamp
Depression and Anxiety

Soc
ial
phob
ia
Kli
nge
ret
al.[2
2]
36S
oci
alp
ho
bia
RC
TIn
div
idu
alV
RE
T(N
518
)12
LS
AS
VR
ET
5C
BT
No
Gro
up
sC
BT
(N5
18)
Wal
lach
etal
.[24]
88F
ear
of
pu
bli
cR
CT
VR
CB
T(N
528
)12
BA
TV
RC
BT
5C
BT4
WL
No
tye
t;st
ill
in
spea
kin
gC
BT
(N5
30)
12L
SA
Sp
rogre
ss
WL
(N5
30)
SS
PS
FN
E
Pan
icdi
sord
er
Bo
tell
aet
al.[2
8]
37P
anic
dis
ord
erR
CT
VR
ET
(N5
12)
9P
DS
SV
RE
T5
Invi
vo12
mo
nth
,st
able
Invi
voex
po
sure
(N5
12)
9A
SI
exp
osu
re4
WL
WL
-co
ntr
ol
(N5
13)
FQ
Ch
oi
etal
.[26]
40P
anic
dis
ord
erR
CT
Gro
up
exp
erie
nti
alco
gnit
ive
ther
apy
(ExC
T;
N5
20)
Pan
icco
ntr
ol
pro
gram
(PC
P;
N5
20)
4 12
PB
QA
CQ
BS
QE
xCT
5P
CP
6m
on
ths,
stab
leo
nm
ain
ou
tco
me;
med
icat
ion
dis
con
tin
uat
ion
hig
her
inth
eP
CP
Pen
ate
etal
.[29]
27P
anic
dis
ord
erM
atch
edb
etw
een
VR
ET
(N5
15)
11A
Q(1
)V
RE
T5
CB
T3
mo
nth
s,st
able
sub
ject
sd
esig
nC
BT
(N5
13)
11A
CQ
mat
ched
wit
han
anti
dep
ress
ant
BS
Q
BA
T
Pit
tiet
al.[3
0]
28P
anic
dis
ord
erM
atch
edb
etw
een
VR
ET
(N5
18)
11A
IV
RE
T5
CB
T
sub
ject
sd
esig
nC
BT
(N5
9)11
AC
Q
mat
ched
wit
han
anti
dep
ress
ant
BS
Q
PT
SD
Rea
dy
etal
.[32]
14P
TS
DO
pen
tria
lV
RE
T(N
514
)F
lexi
ble
up
toC
AP
SS
ign
ific
ant
pre
-po
stch
ange
s6
mo
nth
s,st
able
and
20se
ssio
ns
IES
furt
her
sym
pto
mre
du
ctio
n
Dif
ede
etal
.[31]
21P
TS
DQ
uas
i-ex
per
imen
tal
VR
ET
(N5
13)
Fle
xib
leu
pto
CA
PS
VR
ET4
WL
No
des
ign
WL
-co
ntr
ol
(N5
8)14
sess
ion
sB
DI
a Tre
atm
ent
Ais
equ
ally
effe
ctiv
eas
trea
tmen
tB
.bT
reat
men
tA
issu
per
ior
totr
eatm
ent
B.
c Np
erco
nd
itio
nes
tim
ated
;VR
CB
T,v
irtu
alre
alit
yco
gnit
ive
beh
avio
rth
erap
y;M
S,m
oti
on
sim
ula
tio
n;A
PG
T,a
tten
tio
np
lace
bo
gro
up
sth
erap
y;W
L-c
on
tro
l,w
aiti
ng
list
con
tro
l;F
U,f
oll
ow
-u
p;V
RE
TC
SS
,vir
tual
real
ity
exp
osu
reth
erap
yp
lus
cogn
itiv
ese
lf-s
tate
men
ts;A
Q,A
cro
ph
ob
iaQ
ues
tio
nn
aire
;AT
HQ
,att
itu
de
tow
ard
sH
eigh
tsQ
ues
tio
nn
aire
;BA
T,b
ehav
iora
lavo
idan
cete
st;
FA
S,F
ligh
tA
nxi
ety
Sit
uat
ion
sQ
ues
tio
nn
aire
;FA
M,F
ligh
tA
nxi
ety
Mo
dal
ity
Qu
esti
on
nai
re;F
HF,
flyi
ng
his
tory
form
;FF
S,F
ear
of
Fly
ing
Sca
le;G
FF
Q,G
ener
alF
ear
of
Fly
ing
Qu
esti
on
nai
re;
QA
TF,
Qu
esti
on
nai
reA
ttit
ud
eT
ow
ard
sF
lyin
g;L
SA
S,
Lie
bo
wit
zS
oci
alA
nxi
ety
Sca
le;
SS
PS
,S
elf-
Sta
tem
ent
Qu
esti
on
nai
red
uri
ng
Pu
bli
cS
pea
kin
g;F
NE
,fe
aro
fn
egat
ive
eval
uat
ion
;P
DS
S,
Pan
icD
iso
rder
Sev
erit
yS
cale
;A
SI,
An
xiet
yS
ensi
tivi
tyIn
dex
;F
Q,
Fea
rQ
ues
tio
nn
aire
(Ago
rap
ho
bia
Su
bsc
ale)
;P
BQ
,P
anic
Bel
ief
Qu
esti
on
nai
re;
AC
Q,
Ago
rap
ho
bic
Co
gnit
ion
sQ
ues
tio
nn
aire
;B
SQ
,B
od
ily
Sen
sati
on
Qu
esti
on
nai
re;
AQ
(1),
Ago
rap
ho
bia
Qu
esti
on
nai
re;
AI,
Ago
rap
ho
bia
Ind
ex;
CA
PS
,C
lin
icia
nA
dm
inis
tere
dP
ost
trau
mat
icS
tres
sD
iso
rder
Sca
le;
IES
,Im
pac
to
fE
ven
tS
cale
;B
DI,
Bec
kD
epre
ssio
nIn
ven
tory
;E
EG
,el
ectr
oen
cep
hal
ogr
aph
;B
WM
,b
rain
wav
em
easu
rem
ents
;R
R,
resp
irat
ion
rate
;S
R,
skin
resi
stan
ce;
HR
,h
eart
rate
;S
T,
skin
tem
per
atu
re.
937Review: Virtual Reality Exposure Therapy
Depression and Anxiety

treatment often consists of group therapy, which inturn might be too aversive for socially anxious patients.
A study investigating the effects of VRET for socialphobia compared individual VRET to group CBT.[22]
All subjects (n 5 36) received 12 sessions of therapy.Patients were not randomized, but allocation tocondition was based on matching for age and gender.No BAT was included so results are based on self-report measures only. Although results indicated thatdifferences in outcome between the two treatmentgroups were trivial, no real control condition for theeffect of time (e.g. waitlist control) was added, whichmakes the clinical effects achieved difficult to evaluate.In addition, a possible confound is the comparison ofan individual treatment (VRET) with a group treat-ment. Especially in the treatment of social phobiawhere social contact in the context of participation in agroup can be interpreted as exposure in vivo to a fearedstimulus, group treatment may confound the effects ofCBT per se.
One subcategory of social anxiety is fear of publicspeaking. Often, the state-of-the-art treatment (CBTincluding exposure in vivo) is quite difficult to organizeand too aversive for the patient. In a first open trial(n 5 10) four sessions VRET were combined with foursessions of anxiety management training.[23] Resultsindicated significant improvement on specific fear ofpublic speaking measures. In the first RCT with aclinical sample of subjects (n 5 88) with fear of publicspeaking, the following three conditions were com-pared: CBT vs. CBT plus VRET vs. a waitlist controlgroup.[24] Both treatment protocols consisted ofcognitive and behavioral components (respectivelye.g. working with the cognitive model of social phobiaand a presentation of the cognitive model in virtualreality or in imagination). All subjects received 12individual therapy sessions. Results indicated that CBTplus VRETwas equally effective as CBTand both weresuperior to the control condition on anxiety measuresand on a BAT. Although CBT was as effective as CBTplus VRET, twice as many subjects dropped out ofCBT (significant difference) and therefore the origin-ally planned randomized design was changed to aweighted assignment. This non-random assignment isa major limitation of this study. However, conclusionsare quite firm concerning generalization to the realworld and the much lower drop out rates in the CBTplus VRET group are promising.
PANIC DISORDER
In a more complex anxiety disorder such as panicdisorder with agoraphobia, few RCTs have beenreported. Treatment has to focus on panic as well ason agoraphobic avoidance behavior.[25] Exposure toagoraphobic avoidance behavior consists of exposingindividuals to a variety of situations which they fear—this can be easily done in virtual environments.
Four clinical trials, which investigated the effects ofVRET in subjects with panic disorder, have beenpublished. The first study compared group experientialcognitive therapy (including VRET) to a panic controlprogram in a between subjects design.[26] Subjects(n 5 40) received either four sessions of experientialcognitive therapy (consisting of psycho-education,relaxation training, interoceptive exposure, and VRexposure) or 12 sessions of a panic control program(based on Craske and Barlow).[27] All treatments weregiven in groups except for the VR exposure compo-nent. At post-assessment both treatment conditionswere equally effective. However, results were notmaintained at six-months follow-up, where the paniccontrol program obtained a higher end-state function-ing than the other treatment group. A major limitationof this study is that both treatment conditions receivedan unequal amount of treatment sessions. Interestingly,the experiential cognitive therapy achieved at postassessment the same results with less therapy sessionsthan the panic control program. This aspect and themulti component treatment (components were notevaluated separately) makes generalization difficult.Unfortunately, no BAT was included to control forgeneralization to the real world.
In a RCT done by Botella, Garcia-Palacios, Villa,Banos, Quero, Alcaniz et al. stricter methodologicalcriteria were applied.[28] Subjects (n 5 37) were ran-domly assigned to either nine treatment sessions ofCBT plus VRET, or nine sessions of CBT plusexposure in vivo, or to a waiting list control condition.Results indicated that there were no differences ineffectiveness between the two active treatment condi-tions. Both active treatment conditions were superiorto waitlist controls. The results remained stable at12-months follow-up. Also in this study no BAT wasincluded.
In the third clinical trial done by Penate, Pitti,Bethencourt, de la Fuente, and Gracia,[29] a matchedbetween subjects design was used to compare VRET toCBT in subjects with panic disorder. Subjects (n 5 28)received either 11 sessions of CBT or of a combinedtreatment of CBT and VR. CBT included exposure invivo. Additionally, all subjects received antidepressantmedication. A BATwas conducted at post assessment toinvestigate generalization. CBT and the combinedVRET-CBT program were found to be equallyeffective at post-test, and at three-months follow-up.In a RCT done by the same research group, 27 subjectswith a diagnosis of panic disorder and agoraphobiareceived either CBT (including exposure in vivo) or acombination of CBT and VRET.[30] All subjectsreceived antidepressant medication. There was anoverlap of subjects in the medication condition in thestudies from Penate et al. and Pitti et al. (personalcommunication, 02–20–2010). No significant differ-ences between groups were reported. However, a slighttrend in favor of the combined condition was found.Results of these studies are difficult to interpret
938 Meyerbroker and Emmelkamp
Depression and Anxiety

because of the overlap in subjects and because in thecombined condition, patients also received a number ofexposure in vivo sessions.
In summary, the results of pure VRET have hardlybeen investigated in panic disorder and agoraphobia.Only Botella et al.[28] compared VRET and in vivoexposure directly and found both components equallyeffective.
PTSD
To date, only one comparative treatment outcomestudy was published on VRET in PTSD. In a quasi-experimental (matched) design VRETwas compared toa waitlist control group.[31] Subjects (n 5 21) under-went a flexible amount of exposure sessions, with amaximum of 14 sessions. At post assessment, theVRET group improved significantly on specific PTSDmeasures, whereas the control group did not: thisdifference between groups was significant. Thus,preliminary results indicate that VRET could be auseful intervention in subjects with PTSD at least insome cases. These data are also supported in an opentrial study.[32,33] In this study veterans diagnosed withPTSD underwent VRET. Subjects improved signifi-cantly on specific PTSD measures, with stable resultsat follow-up three and six months later. Possibleproblems in patients with PTSD are that traumas aretoo idiosyncratic to be treated with standard virtualenvironments and that it often will be impossible tocreate virtual environments that are realistic (e.g. childabuse and rape).
META-ANALYSES
Two meta-analyses have been reported concerningthe effectiveness of VRET in anxiety disorders.[1,2] Inboth studies VRETwas found to be equally effective orsuperior to a variety of control groups. In one meta-analysis,[1] 13 studies (n 5 397) were included. Studieswere excluded that involved case reports, multiplecomponents of treatment conditions, and unequalamount of treatment sessions in the treatmentscompared. Between group effect sizes varied from 0.85until 1.67 (Cohen’s d: small: 0.2; medium: 0.5; andlarge: 0.8). There was a small effect size (d 5 0.35)favoring VRETover exposure in vivo. Generally, effectsizes of VRETwere large to very large, but most of thestudies involved specific phobias. In the other meta-analysis less strict criteria were applied and 21 studies(n 5 300) were included in the analysis.[2] The averagewithin group effect sizes varied from 0.87 until 1.79:PTSD 5 0.87; social phobia 5 0.96; acrophobia 5 0.93;panic disorder with agoraphobia 5 1.97; fear offlying 5 1.59. Unfortunately, also case reports wereincluded, which makes comparability with RCTs ratherdifficult, especially given the different anxiety disordersinvestigated, and the different amount of treatmentsessions in the studies compared, which was notcontrolled for in the analyses.
CONCLUDING REMARKS
Applying strict methodological criteria concerningresearch into the effects of treatment of anxietydisorders with virtual reality exposure, this reviewgives a more sobering look on the state-of-the-art ofresearch in this area and compared to earlier reviews(e.g.[7]). Although the two meta-analyses reportedreport promising effect sizes for VRET in general[2]
and in comparison with exposure in vivo,[1] general-ization across anxiety disorders is hardly possible. Onlyin two specific phobias (fear of flying and acropho-bia[8–11,13–15,17–21]) more or less systematic research hasbeen done to be able to state that VRET indeed iseffective in comparison with the state-of-the-art CBTtreatment and controlled for the effect of time. Resultsof VRETon behavioral measures at post-treatment areimpressive, suggesting that the results of VRET indeedgeneralize to the real world. Given the high rate oftreatment refusal and high drop-out rates of exposurein vivo, results of the studies discussed here suggestthat treatment refusal and drop-out rates[34,35] may belower in a treatment protocol using VR for exposure toagoraphobic situations.[28] With respect to otherphobias and PTSD hardly any comparative outcomestudy has been reported, which make any conclusionwith respect to clinical relevance of VRET for thesedisorders premature. Results concerning the treatmentof panic disorder are promising, but definite conclu-sions are precluded since the effects of the VRETcomponent in the package cannot be established inmost of these studies.
PROCESS OF VRETAlthough VRET is regarded as a natural extension of
the systematic exposure component of (cognitive)behavior therapy,[3] to date hardly any research hasexamined the underlying mechanisms of change inVRET. According to the emotional processing theoryof Foa and Kozak, two conditions within therapysessions have to be met for successful emotionalprocessing.[36,37] The fear structure has to be activatedand information incompatible with this existing struc-ture has to be presented and incorporated. In thissection, research concerning cognitive, physiological,or other therapeutic variables associated with VRETwill be discussed.
COGNITIVE MECHANISMS IN VRET
To analyze cognitive mechanisms during VRETdifferent approaches have been used, including auto-matic processing of threatening stimuli,[38,39] andcognitive change as assessed by perceived self-efficacyand self-statements.[6,21]
The first study investigating automatic processingduring VRETwas done with subjects (n 5 28) sufferingfrom arachnophobia.[38] Subjects received an exposure-based virtual reality treatment consisting of five
939Review: Virtual Reality Exposure Therapy
Depression and Anxiety

sessions of 60 min weekly. Pre- and post-treatmentsubjects were assessed with an emotional Stroop task.The Stroop task was done with a series of color-filteredpictures (each category consisted of eight pictures) andsubjects had to push the button with the correspondingcolor as quickly as possible. For positive emotionalcontent a rabbit was chosen, for the neutral emotionalcontent a cow was chosen, and a spider was chosen forthe negative emotional content. Results showed asignificant difference between pre- and post-treatment,indicating that threat interference reduced significantlywhile the response time for positive interference didnot. The authors conclude tentatively that treatmenthad a significant impact on information processing.
In another publication based on the same subjects,[39]
the perceived self-efficacy and threat-related beliefs ofsubjects were analyzed. Results indicated that generalimprovement on self-report measures was only sig-nificantly predicted by changes in self-efficacy, butchanges in threat-related beliefs were nonpredictive forgeneral improvement. A reverse pattern was observedfor improvement on the BAT. Changes in dysfunctionalthreat-related beliefs were the only significant pre-dictor of an increased performance on the BAT. Thus,perceived self-efficacy and threat-related beliefs play animportant but distinct role during VRET.
It is of some interest to analyze self-efficacy also incontext of other cognitive variables as for examplepositive and negative thoughts one has about him orherself. Positive self-statements can also be interpretedin a sense of coping mastery while negative self-statements may promote avoidance behavior.[40] In aprocess study involving subjects with fear of flying(n 5 14) or acrophobia (n 5 20) self-efficacy andnegative self-statements were assessed over the courseof treatment.[6] Subjects received four weekly exposuresessions each of 50 min in a virtual environment.Although cognitions were not directly addressedduring VRET, results indicated that self-statementschanged significantly during VRET: four sessions ofVRET led to a significant reduction in anxiety,enhanced self-efficacy, and a decrease in negative self-statements.
The steady increase in self-efficacy over the course offour VRET sessions is in line with a study in which itwas found that VRET led to a linear increase in self-efficacy in subjects (n 5 26) with acrophobia..[21] In thisstudy subjects were randomly assigned to two sessionsof VRET followed by two sessions of VRET pluscoping self-statements, or the other way around. Asdiscussed already above, results indicated that theaddition of coping self-statements did not influencethe effectiveness of treatment. Given the cross-overdesign used no conclusion can be drawn on the changeof cognitions during VRET as stand-alone treatment.
In summary, results into cognitive change duringVRET are still in its infancy. The few studiesaddressing cognitions during the process of VRETuse a variety of approaches, which shed some light on
cognitive processes, but are not yet conclusive.Although there is some evidence that VRET may leadto change on implicit measures,[38] it is still question-able whether the Stroop task used provides a reliableindication of automatic processing.[41,42] More promis-ing results were revealed with respect to changes inself-efficacy and self-statements over the course ofVRET.[6,17] There is a clear need for process researchfocusing on designs to analyze possible cognitivemediators and moderators and to determine temporalprecedence in mechanisms of cognitive change inVRET.
THERAPEUTIC ALLIANCE ANDEXPECTANCY OF THERAPEUTIC GAINS
A central process aspect concerning therapy outcomeis the therapeutic alliance between therapist and client.Since Freud’s[43] emphasis on the role of the client–therapist relationship, the importance of the relation-ship between client and therapist is being recognizedwithin nearly all schools of psychotherapy. Because ofits modest but stable ability to predict treatmentoutcome, the therapeutic alliance has become one ofthe most studied process variables in psychotherapyresearch.[44] Although the therapeutic alliance is anestablished predictor of psychotherapy outcome, alli-ance research in technology-based psychological treat-ment has been neglected.[45]
In a recent study the mediating role of thetherapeutic alliance was investigated in subjects withfear of flying (n 5 14) or acrophobia (n 5 20).[6] One ofthe aims of that study was to examine whether thequality of the therapeutic alliance predicted successfuloutcome in VRET in terms of anxiety reduction.Results indicated that the quality of the therapeuticalliance as assessed with the Working Alliance In-ventory[46] was positively related to treatment outcomein the fear of flying group but not in the acrophobiagroup. The discrepancy with respect to the predictivevalue of the therapeutic relationship between the twogroups might be related to differences in challengeswithin the exposure sessions, which differed for the twogroups. In the fear of flying patients exposure wasstandardized for all patients eliciting moderate anxiety,while exposure in the patients with acrophobia wasmore challenging in that therapists pushed the patientmore to do more difficult exercises. There is a clearneed for further studies into the mediating role of thetherapeutic relationship in VRET.
Further, there is some evidence that positiveexpectancy of patients with respect to outcome ofVRET may enhance improvement. In a study withsubjects with fear of flying (n 5 72) higher expectanciesfor treatment outcome of VRET led to strongersymptom reduction on self-report measures.[47]
In summary, research into the role of expectancyof therapeutic gains and the therapeutic alliance inVRET is still in its infancy. So far, only two studies
940 Meyerbroker and Emmelkamp
Depression and Anxiety

investigating different therapeutic mechanisms (i.e. thetherapeutic alliance and treatment outcome expectan-cies) have been reported and give only first notions inwhich direction future research should develop.
PSYCHOPHYSIOLOGY IN THE PROCESSOF VRET
More extensive research has been done with psycho-physiological measures into the process of VRET.Different physiological measures as heart rate, heartrate variability, or galvanic skin conductance have beenused to analyze physiological arousal and habituationprocesses in VRET.
A study investigating whether during VRET adifferent motivational system is activated than duringexposure in vivo was done with 20 subjects categorizedinto high- and low-anxious group.[48] The behavioralactivation system (BAS) and the behavioral inhibitionsystem (BIS) are considered differentially responsiblefor treatment effects with exposure in vivo versusVRET. Monitoring anxiety by different physiologicalmeasures (heart rate, which reflects activity of BAS) andskin conductance (which reflects activity of the BIS)may help to determine whether the same processesunderlie virtual exposure and exposure in vivo. Resultsindicated possible underlying physiological differencesbetween the process of VRET and in vivo exposure.Selective activity of BIS as assessed with skin con-ductance was registered during VRET but no activityof BAS (changes in heart rate) was observed. Althoughthese differences were found between in vivo exposureand VRET, results have to be interpreted with cautiongiven that heart rate did not distinguish exposure frombaseline in both groups, while large effect sizes werefound for skin conductance.
The results of the above-mentioned study[48] corro-borate earlier findings in a small study.[49] In this studynonphobic subjects (n 5 9) were immersed in agor-aphobic environments to investigate the pattern ofchange during exposure to virtual environments. Heartrate and skin conductance were registered duringexposure time to four different virtual environments.Results indicated no significant changes in heart rateduring exposure to virtual environments. These resultshave to be interpreted with caution since in such asmall sample size one outlier can distort results.Additionally, skin conductance is very sensitive tobodily movements.
Heart rate was also found not to discriminate in acomparison of exposure to a virtual flight betweenphobic (n 5 33) and nonphobic subjects (n 5 22).[16]
Also here significant differences between groups werefound on skin resistance. Whether the differencesbetween the groups found on skin resistance can beattributed to a VRET specific arousal in the phobicgroup as Wilhelm et al. propose cannot be concluded.Stricter methodological criteria (e.g. controlling forbody movements) should be applied to investigate
whether specific physiological arousal is associatedwith VRET. Further, the same subjects should beexposed to different exposure situations (VRET versusin vivo).
In a quasi-experimental design, a comparison wasmade between high-anxious subjects (n 5 15; fearful oftunnels) and matched controls (n 5 15) on physiologi-cal measures during VRET.[50] Subjects highly fearfulof tunnels underwent exposure to three different virtualenvironments, varying in degree of anxiety provoca-tion. Results indicated differences in heart rate only inthe high-anxious group for the most anxiety evokingvirtual environment, but not for the other environ-ments. Further, no significant results were found onskin conductance. Thus, physiological reactions (heartrate) varied between virtual environments only in thehigh-anxious group, but not in matched controls, thusresults are not in line with the results of earlierresearch,[16,48,49] in which a reverse pattern was found.
In studies by Cote and Bouchard[38,39] physiologicalreactions were observed on heart rate variability(HRV). Results indicated that the cardiac responsemeasured with HRV was the best predictor of changein behavioral avoidance. A significant decrease ininterbeat intervals was found when subjects wereconfronted to exposure situations,[38] indicating higheranxiety. Additionally, it was found that the cardiacresponse measured by HRV was best predicted bychanges in perceived self-efficacy and dysfunctionalbeliefs.[39]
Firm conclusions about a pattern of physiologicalarousal during VRET cannot be drawn since nocoherent pattern was found in the various studiesdiscussed. Overall in none of the studies, consistentsupport was found for the emotional processing theoryas indicated by changes in heart rate. More support wasfound for changes in skin conductance duringVRET,[16,48,49] but this was not corroborated inanother study;[50] all three studies, which foundsupport, lacked sufficient statistical power. Studies withmore sophisticated research designs, making a directcomparison between VRET and exposure in vivo whilekeeping all other variables constant, would be avaluable contribution.
ENHANCEMENT OF THERAPY EFFECTSTHROUGH COGNITIVE ENHANCERS
Another increasingly important area of researchconcerns the enhancement of extinction processesduring (virtual) exposure therapy. Extinction can bedescribed as a form of learning, indicated by a declinein frequency and magnitude of the anxious response.[51]
Experimental animal research has revealed that cogni-tive enhancers can augment the process of exposure[52]
and therefore be a valuable contribution in futureexposure-based treatments. A few studies with healthyhumans[53,54] and clinical samples have supported the
941Review: Virtual Reality Exposure Therapy
Depression and Anxiety

notion that pharmacological agents can enhanceexposure treatment[55] (for a review see[56]).
In a first study combining VRET with a cognitiveenhancer subjects (n 5 28) with acrophobia underwentVRET combined with D-cycloserine (DCS) or VRETcombined with placebo.[57] In this double blind RCT,subjects were treated with two sessions of VRET.Single doses of placebo or DCS were administeredbefore each exposure treatment. Subjects were assessedone week after treatment termination and three monthsafter treatment termination. Results indicated thatVRET plus DCS resulted in significantly largerreduction of acrophobia on all outcome measuresthan VRET plus placebo. The results remained stableat three months follow-up. Thus, there is somesupport that emotional learning during VRET can beaugmented using cognitive enhancers. However, dif-ferent doses of DCS were administered (50 or 500 mg),but no differences between doses were found for theprimary outcome measures of acrophobia, which makesresults difficult to interpret.
CONCLUDING REMARKSThis systematic review gives a sobering look on the
current status of research in this field. Only in fear offlying and acrophobia is there considerable evidencethat VRET indeed is effective. In more complexanxiety disorders as panic disorder and social phobia,which form the core clinical groups, first results ofVRET are promising,[24,28] but more and bettercontrolled studies are needed before the status ofempirically supported treatment is reached. Moresevere cases of panic disorder with agoraphobia andsocial phobia are often not reached with existingtreatments. Such patients are too scared to come intotreatment because they have to leave their ‘‘safe/securezone/circle’’ for that. To better reach this core clinicalgroup, a future aim of research could be to investigatewhether initial sessions can be conducted at home viaan Internet port, where patients can login and start firsttreatment sessions in virtual reality.
In the field of treatment of PTSD until now, onlytwo open studies support the notion that patientssuffering from PTSD are improving with VRET.[31,32]
But the question remains in how far PTSD can besuccessfully treated with virtual reality. Treatment forPTSD with virtual reality seems possible and realisticfor veterans who have been traumatized in more or lesscomparable (war) situations. Other traumatic events/incidents are often too idiosyncratic to be rebuild invirtual environments. The treatment of PTSD withVRET in veterans can be very relevant, though, giventhat stereotype virtual environments for war situationscan be used. Other traumatic incidents might be easierand better treated with other state-of–the-art treat-ments for PTSD.
A general remark is that in outcome researchof VRET often multiple components are mixed in
treatment protocols. First, these combined treatmentsare not always based on the state-of-the-art treatmentfor these specific disorders, which on its own makesstudies on the efficacy of VRET difficult to interpret.Further, given that virtual reality exposure is oftencombined with other techniques, dismantling researchmethodology is needed to separate the contribution ofthe various components. Finally, a last remark on studiesin this area is that often no BAT is included, in whichcase conclusions about generalization to real life cannotbe made; generalization to the real world remains ofcourse the ultimate measure for this treatment form.
Process studies could shed more light on mediatingvariables of the outcome of VRET. There is a clearneed of studies investigating the cognitive and physio-logical processes presumed to underlie VRET. Further,research into the role of the therapeutic alliance duringVRET is scarce. Research into another technology-based treatment (internet-based treatment) for post-traumatic stress suggests that such technology does nothave to interfere with treatment outcome. For example,when patients did not see the therapist at all face-to-face in an internet treatment, a substantial correla-tion was found between the quality of the therapeuticalliance as assessed with the Working Alliance In-ventory[46] and treatment outcome. Thus, there wereno indications that technology-based psychologicaltreatment interfered with the therapeutic process.[58]
Another valuable contribution that is possiblethrough sophisticated use of VRET is research intounderstanding contributing factors of specific disor-ders. In a review of the triggers of acrophobic behaviorit was concluded that motion combined with heightrather than height on its own triggers phobicresponses.[59] In this sense VRET can help in thefuture understanding treatment processes but alsoprocesses related to fear itself.
In summary, it would be a valuable addition whenresearch into VRET would not only focus on outcomebut also on the underlying processes. Understandingthe processes would help implementing VRET intoclinical practice given that treatment outcome wouldbe better predictable.
Acknowledgments. This study was supported bythe Royal Netherlands Academy of Arts and Sciences(Academy professorship awarded to Paul Emmelkamp).
REFERENCES1. Powers MB, Emmelkamp PMG. Virtual reality exposure therapy
for anxiety disorders: a meta-analysis. J Anxiety Disord 2008;22:561–569.
2. Parsons TD, Rizzo AA. Affective outcomes of virtual realityexposure therapy for anxiety and specific phobias: a meta-analysis. J Behav Ther Exp Psychiatry 2008;39:250–261
3. Emmelkamp PMG. Behavior therapy with adults. In: Lambert M,editor. Bergin & Garfield’s Handbook of Behavior Therapy andBehavior Change. New York: Wiley; 2004:396–448.
942 Meyerbroker and Emmelkamp
Depression and Anxiety

4. Cote S, Bouchard S. Virtual reality exposure for phobias:a critical review. J CyberTher Rehabil 2008;1:75–91.
5. Shelef K, Diamond GM. Short form of the revised vanderbilttherapeutic alliance scale: development, reliability, and validity.Psychother Res 2008;18:433–443.
6. Meyerbroker K, Emmelkamp PMG. Therapeutic processes invirtual reality exposure therapy: the role of cognitions and thetherapeutic alliance. J CyberTher Rehabil 2008;1:247–257.
7. Krijn M, Emmelkamp PMG, Olafsson RP, Biemond R. Virtualreality exposure therapy of anxiety disorders: a review. ClinPsychol Rev 2004;24:259–281.
8. Rothbaum BO, Hodges L, Smith S, Lee JH. A controlled studyof virtual reality exposure therapy for fear of flying. J ConsultClin Psychol 2000;68:1020–1026.
9. Rothbaum BO, Hodges L, Anderson P, Price L, Smith S.Twelve-months follow-up of virtual reality and standard exposuretherapies for fear of flying. J Consult Clin Psychol 2002;70:428–432.
10. Rothbaum BO, Zimand E, Hodges L, Lang D, Wilson J. Virtualreality exposure therapy and standard (in vivo) exposure therapyin the treatment of fear of flying. Behav Ther 2006;37:80–90.
11. Maltby N, Kirsch I, Mayers M, Allen GJ. Virtual reality exposuretherapy for the treatment of fear of flying: a controlledinvestigation. J Consult Clin Psychol 2002;70:1112–1118.
12. Muhlberger A, Herrmann MJ, Wiedemann G, Ellgring H,Pauli P. Repeated exposure of flight phobics to flights in virtualreality. Behav Res Ther 2001;39:1033–1050.
13. Muhlberger A, Wiedemann G, Pauli P. Efficacy of a one-sessionvirtual reality exposure treatment for fear of flying. PsychotherRes 2003;13:323–336.
14. Muhlberger A, Weik A, Pauli P, Wiedemann G. One-sessionvirtual reality exposure treatment for fear of flying: 1-year follow-up and graduation flight accompaniment effects. Psychother Res2006;16:26–40.
15. Wiederhold BK, Wiederhold MD. Three year follow-up forvirtual reality exposure for fear of flying. Cyberpsychol Behav2003;6:441–445.
16. Wiederhold BK, Jang DP, Kim SI, Wiederhold MD. Physiolo-gical monitoring as an objective tool in virtual reality therapy.CyberPsychol Behav 2002;5:77–82.
17. Krijn M, Emmelkamp PMG, Olafsson RP, et al. Fear of flyingtreatment methods: virtual reality exposure vs. cognitive beha-vioral therapy. Aviat Space Environ Med 2007;78:121–128.
18. Emmelkamp PMG, Bruynzeel M, Drost L, van der Mast CPAG.Virtual reality treatment in acrophobia: a comparison withexposure in vivo. CyberPsychol Behav 2001;4:335–339.
19. Emmelkamp PMG, Krijn M, Hulsbosch AM, De Vries S,Schuemie MJ, Van der Mast CAPG. Virtual reality treatmentversus exposure in vivo: a comparative evaluation in acrophobia.Behav Res Ther 2002;40:509–516.
20. Krijn M, Emmelkamp PMG, Biemond R, De Wilde de Ligny C,Schuemie MJ, Van der Mast CAPG. Treatment of acrophobia invirtual reality: the role of immersion and presence. Behav ResTher 2004;42:229–239.
21. Krijn M, Emmelkamp PMG, Olafsson RP, Schuemie MJ, van derMast CAPG. Do self-statements enhance the effectiveness ofvirtual reality exposure therapy? A comparative evaluation inacrophobia. CyberPsychol Behav 2007;10:362–370.
22. Klinger E, Bouchard S, Legeron P, et al. Virtual reality therapyversus cognitive behavior therapy for social phobia: a preliminarycontrolled study. CyberPsychol Behav 2005;8:76–88.
23. Anderson PL, Zimand E, Hodges LF, Rothbaum BO. Cognitivebehavioural therapy for public-speaking anxiety using virtualreality for exposure. Depress Anxiety 2005;22:156–158.
24. Wallach HS, Safir MP, Bar-Zvi M. Virtual reality cognitivebehavior therapy for public speaking anxiety; a randomizedclinical trial. Behav Modif 2009;33:314–338.
25. Emmelkamp PMG, Powers MB. Agoraphobia. In: Thomas J,Hersen M, editors. Handbook of Clinical Psychology Compe-tencies. New York: Springer; 2010:723–758.
26. Choi YH, Vincelli F, Riva G, Wiederhold BK, Lee JH, Park KH.Effects of group experiential cognitive therapy for the treatmentof panic disorder with agoraphobia. CyberPsychol Behav 2005;8:387–393.
27. Craske MG, Barlow DH. Mastery of Your Anxiety and Panic, II.Albany, NY: Graywind, 1994
28. Botella C, Garcia-Palacios A, Villa H, et al. Virtual realityexposure in the treatment of panic disorder and agoraphobia:a controlled study. Clin Psychol Psychother 2007;14:164–175.
29. Penate W, Pitti CT, Bethencourt JM, de la Fuente J, Gracia R.The effects of a treatment based on the use of virtual realityexposure and cognitive-behavioral therapy applied to patientswith agoraphobia. Int J Clin Health Psychol 2008;8:5–22.
30. Pitti CT, Penate W, de la Fuente J, et al. Agoraphobia: combinedtreatment and virtual reality. Preliminary results. Actas EspPsiquiatra 2008;36:94–101.
31. Difede J, Cukor J, Jayasinghe N, et al. Virtual reality exposuretherapy for the treatment of posttraumatic stress disorderfollowing September 11, 2001. J Clin Psychiatry 2007;68:1639–1647.
32. Ready DJ, Pollack S, Rothbaum BO, Alarcon RD. Virtual realityexposure for veterans with posttraumatic stress disorder.J Aggress Maltreat Trauma 2006;12:199–220.
33. Rothbaum BO, Hodges L, Ready DJ, Graap K, Alarcon RD.Virtual reality exposure therapy for Vietnam veterans withposttraumatic stress disorder. J Clin Psychiatry 2001;62:617–622.
34. Garcia-Palacios A, Botella C, Hoffman H, Fabregat S. Compar-ing acceptance and refusal rates of virtual reality exposure vs. invivo exposure by patients with specific phobias. CyberPsycholBehav 2007;10:722–724.
35. Garcia-Palacios A, Hoffman H, Kwong See S, Tsai A, Botella C.Redefining therapeutic success with virtual reality exposuretherapy. CyberPsychol Behav 2001;4:341–348.
36. Foa E, Kozak MJ. Emotional processing of fear: exposure tocorrective information. Psychol Bull 1986;99:20–35.
37. Foa E, McNally RJ. Mechanisms of change in exposure therapy.In: Rapee RM, editor. Current Controversies in the AnxietyDisorders. New York: Guilford Press; 1996:214–227.
38. Cote S, Bouchard S. Documenting the efficacy of virtual realityexposure with psychophysiological and information processingmeasures. Appl Psychophysiol Biofeedback 2005;30:217–232.
39. Cote S, Bouchard S. Cognitive mechanisms underlying virtualreality exposure. CyberPsychol Behav 2009;12:121–129.
40. van Hout WJPJ, Emmelkamp PMG, Koopmans PC, Bogels SM,Bouman TK. Assessment of self-statements in agoraphobicsituations construction and psychometric evaluation of theagoraphobic self-statements questionnaire (ASQ). J Anxiety Disord2001;15:183–201.
41. Olatunji BO, Sawchuk CN, Lee TC, Lohr JM, Tolin DF.Information processing biases in spider phobia: application of theStroop and ‘‘White Noise’’ paradigm. J Behav Ther ExpPsychiatry 2008;39:187–200.
42. Wiers RW, Teachman BA, De Houwer J. Implicit cognitiveprocesses in psychopathology: an introduction. J Behav Ther ExpPsychiatry 2007;38:95–104.
43. Freud S. The dynamics of transference. In: Strachey J, et al.,editors. The Standard Edition of the Complete Works ofSigmund Freud, vol. 12. London: Hogarth Press; 1912/1958;44.
943Review: Virtual Reality Exposure Therapy
Depression and Anxiety

44. Martin D, Garske JP, Davis MK. Relation of the therapeuticalliance with outcome and other variables: a meta-analytic review.J Consult Clin Psychol 2000;68:438–450.
45. Emmelkamp PMG. Technological innovations in clinical assess-ment and psychotherapy. Psychother Psychosom 2005;74:336–343.
46. Horvath AO, Greenberg LS. Development and validation of theWorking Alliance Inventory. J Couns Psychol 1989;36:223–233.
47. Price M, Anderson P, Henrich CC, Rothbaum BO. Greaterexpectations: using hierarchical linear modeling to examineexpectancy for treatment outcome as a predictor of treatmentresponse. Behav Ther 2008;39:398–405.
48. Wilhelm FH, Pfaltz MC, Gross JJ, Mauss IB, Kim SI,Wiederhold B. Mechanisms of virtual reality exposure therapy:the role of the behavioural activation and behavioral inhibitionsystems. Appl Psychophysiol Biofeedback 2005;30:271–284.
49. Moore K, Wiederhold BK, Wiederhold MD, Riva G. Panic andagoraphobia in a virtual world. CyberPsychol Behav 2002;5:197–202.
50. Muhlberger A, Bulthoff HH, Wiedemann G, Pauli P. Virtualreality for the psychophysiological assessment of phobic fear:responses during virtual driving. Psychol Assess 2007;19:340–346.
51. McNally RJ. Mechanisms of exposure therapy: how neurosciencecan improve psychological treatments for anxiety disorders. ClinPsychol Rev 2007;27:750–759.
52. Cain CK, Blouin AM, Barad M. Adrenergic transmissionfacilitates extinction of conditional fear in mice. Learn Mem2004;11:179–187.
53. O’Carroll RE, Drysdale E, Cahill L, Shajahan P, Ebmeier KP.Stimulation of the noradrenergic system enhances and blockadereduces memory for emotional material in man. Psychol Med1999;29:1083–1088.
54. Southwick SM, Davis M, Horner B, et al. Relationship ofenhanced norepinephrine activity during memory consolidationto enhanced long-term memory in humans. Am J Psychiatry2002;159:1420–1422.
55. Powers MB, Smits JAJ, Otto MW, Sanders C, Emmelkamp PMG.Facilitation of fear extinction in phobic participants witha novel cognitive enhancer: a randomized placebo controlledtrial of yohimbine augmentation. J Anxiety Disord 2009;23:350–356.
56. Davis M, Myers KM, Chhatwal J, Ressler KJ. Pharmacologicaltreatments that facilitate extinction of fear: relevance topsychotherapy. J Am Soc Exp NeuroTher 2006;3:82–96.
57. Ressler KJ, Rothbaum BO, Tannenbaum L, et al. Cognitiveenhancers as adjuncts to psychotherapy. Arch Gen Psychiatry2004;61:1136–1144.
58. Knaevelsrud C, Maercker A. Internet-based treatment for PTSDreduces distress and facilitates the development of a strongtherapeutic alliance: a randomized controlled clinical trial. BMCPsychiatry 2007;7:1–10.
59. Coelho CM, Waters AM, Hine T, Wallis G. The use of virtualreality in acrophobia research and treatment. J Anxiety Disord2009;23:563–574.
944 Meyerbroker and Emmelkamp
Depression and Anxiety




![Genomic Predictors of Outcome in Prostate Cancer · outcome after surgery [19,21,22,24,27,29]. In one 1 – Preferred Reporting Items for Systematic Reviews and Meta-analysis flow](https://img.dokumen.tips/doc/110x75/5f8870ec69b94e4fa748fb1d/genomic-predictors-of-outcome-in-prostate-cancer-outcome-after-surgery-192122242729.jpg)
























